the shockwave lithoplasty concept: finally the … shockwave lithoplasty concept: finally the...
TRANSCRIPT

The Shockwave Lithoplasty Concept:
Finally the Solution for Calcified Lesions?
Andrew Holden, MBChB, FRANZCR

Disclosure
Speaker name:
Associate Professor Andrew Holden
I have the following potential conflicts of interest to report:
Consulting – Clinical Investigator for Shockwave
Employment in industry
Stockholder of a healthcare company
Owner of a healthcare company
Other(s)
I do not have any potential conflict of interest
X

Arterial Calcification
• Most endovascular devices do not cope well with
vessel calcification
• Significant calcification is a common exclusion
criteria for many device trials
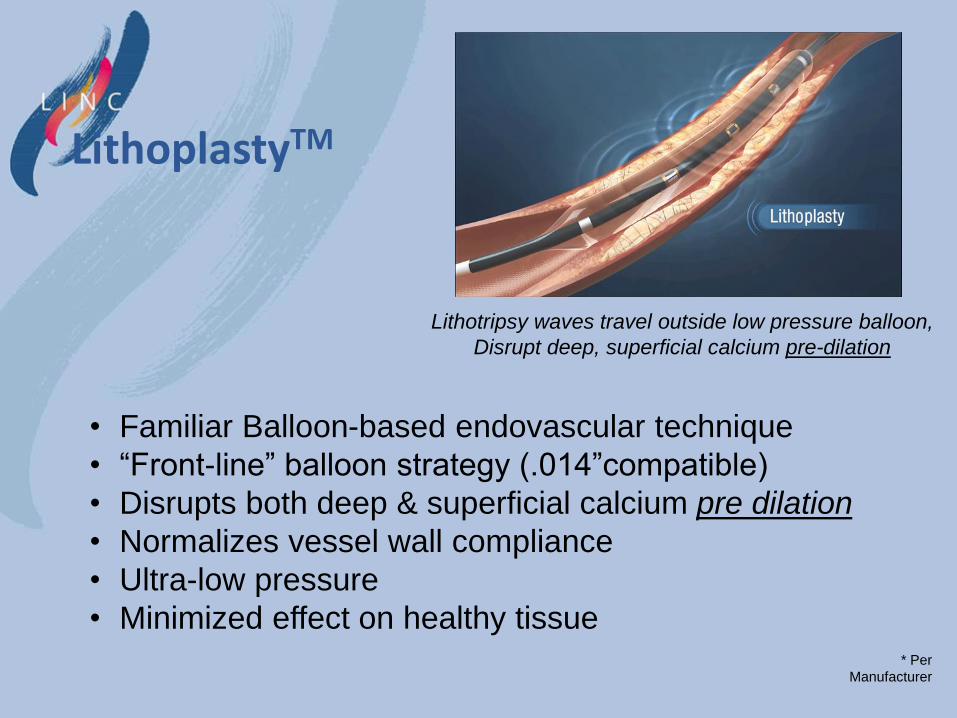
• Familiar Balloon-based endovascular technique
• “Front-line” balloon strategy (.014”compatible)
• Disrupts both deep & superficial calcium pre dilation
• Normalizes vessel wall compliance
• Ultra-low pressure
• Minimized effect on healthy tissue
Lithotripsy waves travel outside low pressure balloon,
Disrupt deep, superficial calcium pre-dilation
* Per
Manufacturer
LithoplastyTM

Lithotripsy disrupts calcium prior to low-pressure
dilation to reference vessel diameter

Inclusion Criteria
• Rutherford II-IV Intermittent Claudication (n= 35 Patients)
• ABI < 0.9
• Screen CT, MR, X-ray
• SFA/Popliteal Lesion > 70% stenosis, 3.3-7.0 mm, < 180 mm
• Angiographic Moderate/Severe Calcification
Procedure
• Lithoplasty 3.5 to 7.0 x 60 mm Multi-electrode Balloon
Endpoints
• Acute Angiographic Result-Core lab adjudicated
• Safety-30 day MAE-CEC Adjudicated
• Duplex Ultrasound 30 & 180 Days-Core lab adjudicated
• OCT Sub-study-Core lab adjudicated
DISRUPT PAD

Investigational Sites
Investigator Site Enrollment
Marianne Brodmann (PI)
Medizinische Universität Graz, Austria
23
Andrew Holden (co-PI)
Auckland City Hospital, New Zealand
7
Martin Werner Hanusch-Krankenhaus, Vienna, Austria
5
Total: 35

Core Labs
Angiography
• Alexandra Lansky, MD-Yale Cardiovascular Research Group
Duplex Ultrasound
• Michael Jaff, MD-Vascore (MGH)
Optical Coherence Tomography
• Case Western Reserve
Clinical Events Committee
Bill Gray MD (Chair)
• Columbia Presbyterian Medical Center- NY, NY
Nick Shammas MD
• Genesis Heart Center- Davenport, IA
Rob Lookstein MD
• Mt Sinai Medical Center- NY, NY
DISRUPT PAD

Clinical Baseline
Symptoms Total (N=35)
Rutherford Category, %(n/N)
0 0.0% ( 0/ 35)
1 0.0% ( 0/ 35)
2 40.0% ( 14/ 35)
3 57.1% ( 20/ 35)
4 2.9% ( 1/ 35)
5 0.0% ( 0/ 35)
6 0.0% ( 0/ 35)
ABI Resting (treated limb)
Mean ± SD (N) 0.7± 0.1 ( 31)
[95% Conf. Interval]¹ [ 0.7, 0.7]
Pain Scale
Mean ± SD (N) 3.6± 0.8 ( 35)
Median (Q1, Q3) 3.0 ( 3.0, 4.0)
Range (min, max) ( 2.0, 5.0)
[95% Conf. Interval]¹ [ 3.3, 3.9]
Pain Scale, %(n/N)
1 0.0% ( 0/ 35)
2 5.7% ( 2/ 35)
3 45.7% ( 16/ 35)
4 34.3% ( 12/ 35)
5 14.3% ( 5/ 35)

Lesion Characteristics (Core Lab) Angio Core Lab Baseline
N= 35 pts M=39 lesions
Morphology
Target Lesion Length (mm)
Mean ± SD (N) 61.5± 36.6 ( 39)
[95% Conf. Interval]¹ [ 49.6, 73.4]
Calcification, %(n/N)
None/Mild 0.0% ( 0/ 39)
Moderate 35.9% ( 14/ 39)
Severe 64.1% ( 25/ 39)
Total Length of Calcification (mm)
Mean ± SD (N) 80.3± 38.4 ( 39)
Median (Q1, Q3) 59.8 ( 55.7, 119.2)
Range (min, max) ( 28.6, 184.3)
[95% Conf. Interval]¹ [ 67.9, 92.7]
Thrombus Present
[95% Conf. Interval]² 0.0% ( 0/ 39) [ 0.0%, 9.0%]
Aneurysm Present
[95% Conf. Interval]² 7.7% ( 3/ 39)
[ 1.6%, 20.9%]
Distal Run-Off, %(n/N)
1 10.3% ( 4/ 39)
≥ 2 89.7% ( 35/ 39)

Primary Performance Endpoint < 50% residual stenosis
Lithoplasty with or without PTA Primary Performance Parameters
N=35 pts.
M= 39 lesions
Achieved < 50% DS
[95% Conf. Interval]²
100.0% ( 39/ 39)
[ 91.0%,100.0%]
Acute Gain (mm)
Mean ± SD (N)
Median (Q1, Q3)
Range (min, max)
[95% Conf. Interval]¹
2.9± 0.8 ( 39)
2.8 ( 2.4, 3.4)
( 1.4, 4.6)
[ 2.6, 3.1]
Percent Stenosis Reduction (%)
Mean ± SD (N)
Median (Q1, Q3)
Range (min, max)
[95% Conf. Interval]¹
68.7± 8.5 ( 39)
68.6 ( 62.0, 75.2)
( 48.2, 85.1)
[ 65.9, 71.4]
Adjunctive Angioplasty required in only 4 patients

DISRUPT PAD: Primary Performance Endpoint
Procedural Success: Residual diameter stenosis of <50% (with or without adjunctive PTA) of
moderate (36%) and severe (64%) calcified lesions assessed by quantitative angiography via
core lab evaluation.
Average Residual Stenosis 23%
Primary Endpoint
(<50%)
Exploratory Endpoint
(<30%)

Patency at 30 days
Follow up visit N <50% stenosis
30 days 38 100%
• Duplex Ultrasound at 30 days, core lab adjudicated results:

Patency – Matched Pairs • Duplex Ultrasound, core lab adjudicated
– Average PSVR at discharge: 1.40
– Average PSVR at 30 days: 1.21
*Core lab adjudicated
2
1,4
1,7
1,2 1,1
1,7
1,2 1,3
1
1,3
0,9
1,3
1,9
1,1 1,2
1,5
1,1
1,4 1,3 1,3
0,7
1,1
0,8
1,1
1,8
1,5
0,9
1,5
1,1
0,9
1,2 1,2
0,8 0,9
0,7
1,2 1,1 1,1 1,1
1,3
0,9
1,6
1,2 1,1
1,0
1,4
1,2
1,4
0
0,5
1
1,5
2
2,5
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Change in PSVR (Matched Pairs)
Discharge 30 Days
Is there continued remodeling of the vessel wall after Shockwave lithoplasty?

Subject AUC-007
Pre-procedure Post LB/ Final Lithoplasty Balloon Calcification

Subject AUC-007
Pre-procedure Pre-procedural OCT

Subject AUC-007
Post LB/ Final Post-procedural OCT

Subject AUC-007
Pre-procedure DUS
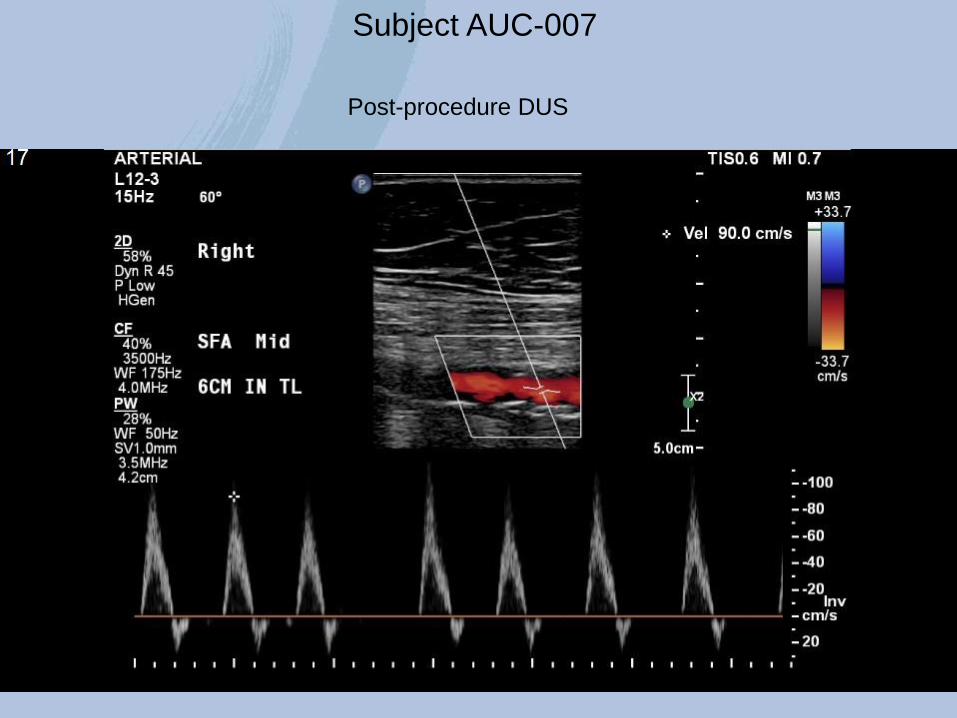
Subject AUC-007
Post-procedure DUS

ABI Scores - Change Summary by Visit for Matched Pairs
Visit N Baseline
Mean [95% CI]¹
Post-Proc Mean
[95% CI]¹
Δ from Baseline [95% CI]¹
P-value*
Discharge 31 0.7± 0.1 [ 0.7, 0.7]
1.0± 0.2 [ 0.9, 1.0]
0.3± 0.2 [ 0.2, 0.3]
< 0.0001
1 Month 31 0.7± 0.1 [ 0.7, 0.7]
1.0± 0.3 [ 0.9, 1.1]
0.3± 0.2 [ 0.2, 0.4]
< 0.0001

Heavily Calcified Superficial Femoral Artery Stenosis

Lithoplasty™

Active Lithoplasty™

Pre-procedure Post LB/ Final Lithoplasty Balloon Calcification
DS=100%
Lesion Length=76.5 mm Total Length of Ca=74.8 mm
Prox. RVD=5.50 mm
Dist. RVD=6.05 mm
Interpolated RVD=5.89 mm
MLD=4.59 MM
DS %=21.94%
27.5mm OL
Core Lab Residual: 22%

• 4 FIM cases treated at Auckland Hospital with 20mm long initial device – follow up > 2 years
• 2 cases treated with EU device pre-trial – follow up > 1 year
• No DUS evidence of restenosis
• No recurrent symptoms
• No re-interventions
Longer Term Follow Up

Post-Lithoplasty @ 0.5ATM Pre-treatment
Longer Term Follow Up

MRA Pre-treatment
Longer Term Follow Up
MRA @ 2 years

Conclusions • Lithoplasty is a novel balloon-based technology for treatment of
calcified vascular lesions
• The results of the DISRUPT PAD Trial demonstrate outstanding acute results for treatment of moderate and severe calcified SFA/Popliteal lesions
• The procedure was extremely well tolerated and had an excellent safety profile
• Patency determined by DUS at 30 days was 100 percent
• Clinical pain & walking scores at 30 days were excellent
• Peak velocity ratios suggest positive remodeling effects at 30 days that warrant further investigation
• Longer term vessel patency will be determined by DUS at 6 month follow-up

The Shockwave Lithoplasty Concept:
Finally the Solution for Calcified Lesions?
Andrew Holden, MBChB, FRANZCR