the short term effects of non surgical periodontal therapy on il-6 and crp levels in chronic...
TRANSCRIPT
THE SHORT TERM EFFECTS OF NON-SURGICAL PERIODONTAL THERAPY ON THE CIRCULATING LEVELS OF IL-6 AND CRP IN PATIENTS WITH CHRONIC PERIODONTITIS
George AK, Janam P.Journal of Indian Society of Periodontology. Jan-Feb 2013:17(1):36-41.
Presented ByDr. Bibina GeorgeMDS Periodontics
Interleukin-6 and C- reactive protein
Interleukin-6• Proinflammatory cytokine• Synergistic with Il-1β • Induces synthesis of acute phase
proteins by liver
CRP• Tissue factor production
(+) coagulation pathway• (+) complement cascade
INTRODUCTION
Therapeutic oral manipulations or the inappropriate or absence of intervention of
progressing periodontitis could have a significant influence on the levels of systemic
inflammation.
AIM:
• The extent of “spill” of pro inflammatory cytokines like interleukin (IL)‑6 into the systemic
circulation
• The systemic inflammatory response generated due to severe chronic generalized
periodontitis by assessment of IL‑6 and C‑reactive protein (CRP) levels
• The changes in the systemic levels of cytokine IL‑6 and acute phase reactant CRP brought
about by non‑surgical periodontal therapy.
MATERIALS AND METHODS:
• SOURCE OF DATA:
Patients who attended the Department of Periodontics and Oral Implantology
Government Dental College, Thiruvananthapuram.
• Ethical clearance:
Reviewed and approved by Human Ethical Committee, Medical College,
Thiruvananthapuram.
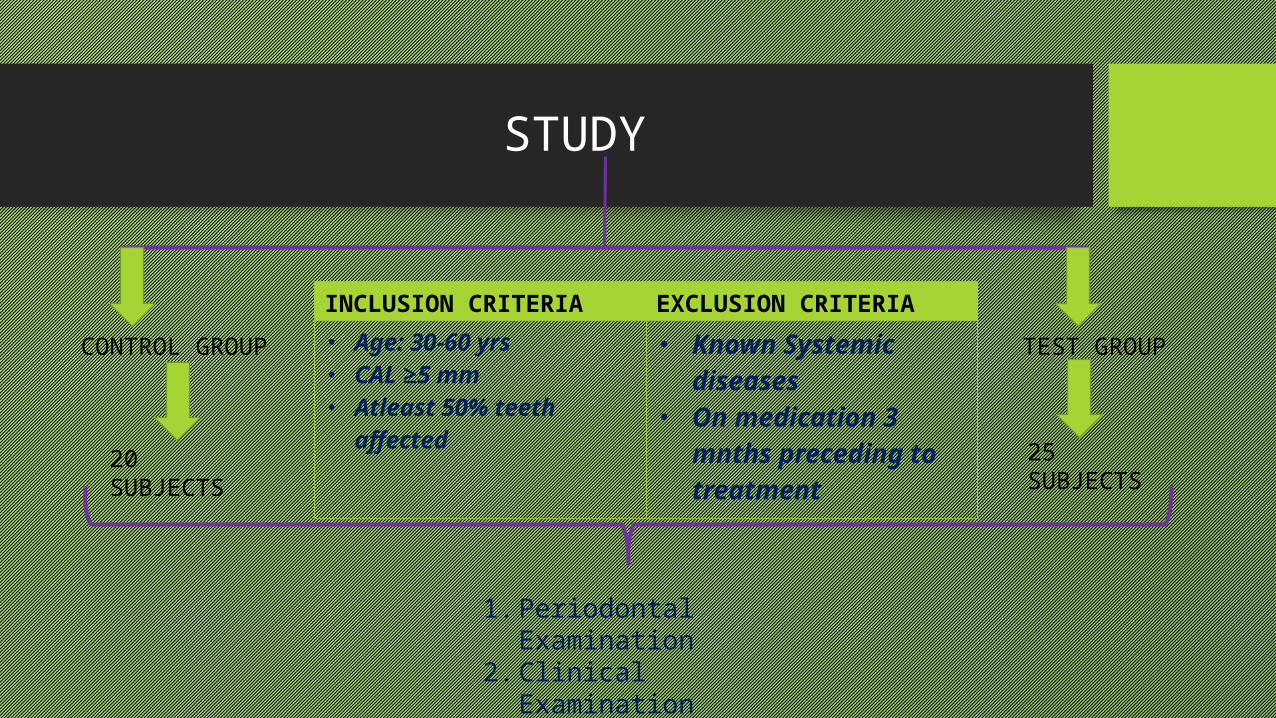
STUDY
CONTROL GROUP
TEST GROUP
25 SUBJECTS
20 SUBJECTS
INCLUSION CRITERIA EXCLUSION CRITERIA• Age: 30-60 yrs• CAL ≥5 mm• Atleast 50% teeth affected
• Known Systemic diseases
• On medication 3 mnths preceding to treatment
1. Periodontal Examination2. Clinical Examination3. Collection of blood sample
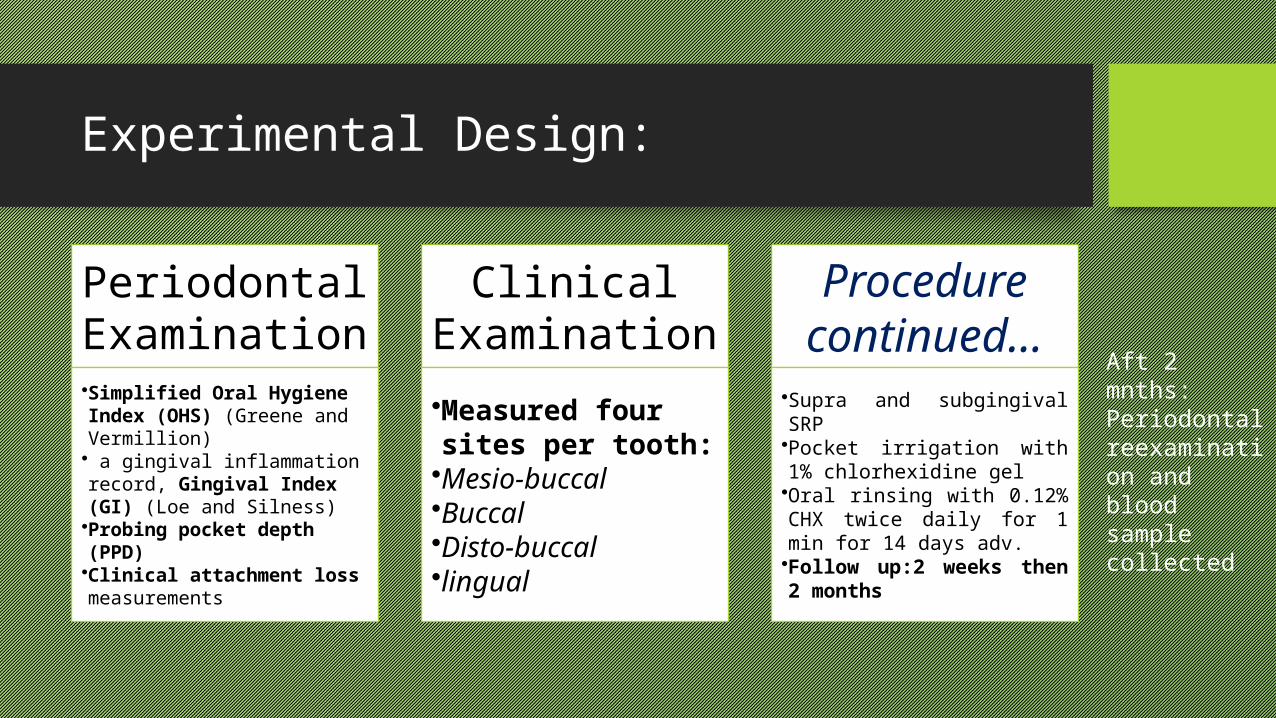
Experimental Design:
Periodontal Examination•Simplified Oral Hygiene Index (OHS) (Greene and Vermillion)• a gingival inflammation record, Gingival Index (GI) (Loe and Silness)•Probing pocket depth (PPD)•Clinical attachment loss measurements
Clinical Examination•Measured four sites per tooth:•Mesio‑buccal•Buccal•Disto‑buccal•lingual
Procedure continued…
•Supra and subgingival SRP•Pocket irrigation with 1% chlorhexidine gel•Oral rinsing with 0.12% CHX twice daily for 1 min for 14 days adv.•Follow up:2 weeks then 2 months
Aft 2 mnths:Periodontal reexamination and blood sample collected
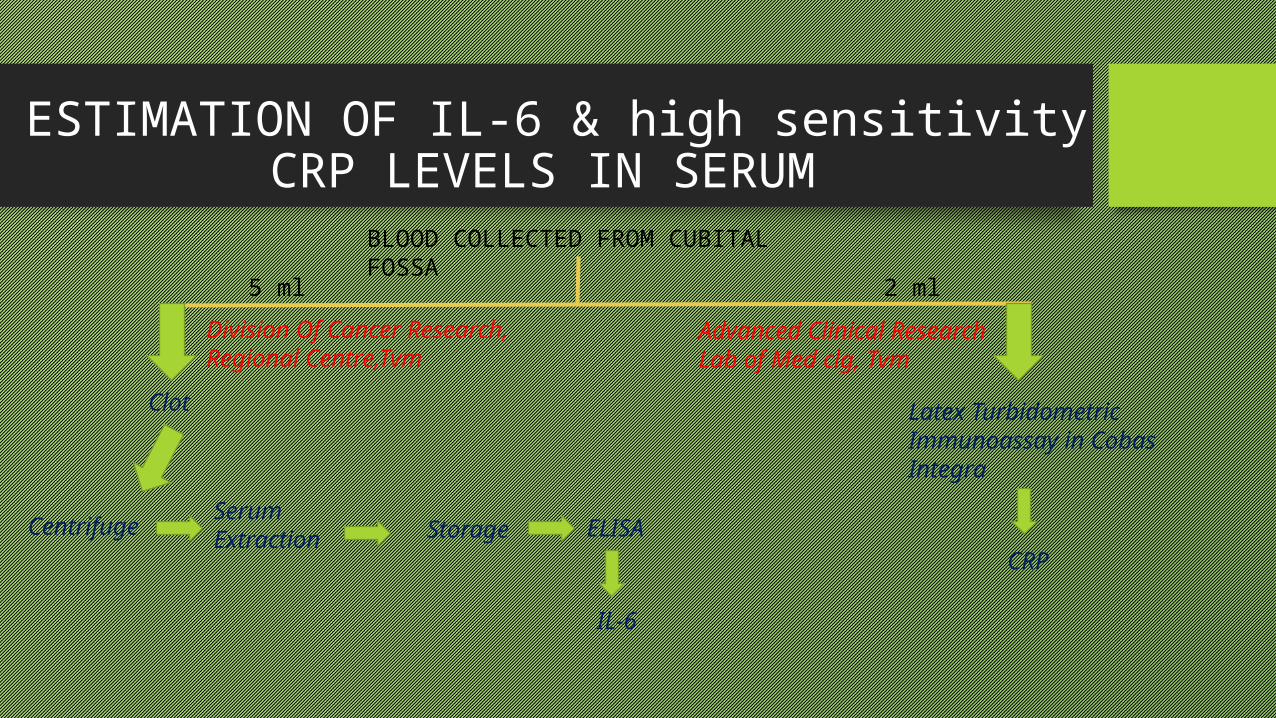
ESTIMATION OF IL-6 & high sensitivity CRP LEVELS IN SERUM
BLOOD COLLECTED FROM CUBITAL FOSSA5 ml 2 ml
Division Of Cancer Research, Regional Centre,Tvm
Advanced Clinical Research Lab of Med clg, Tvm
Latex Turbidometric Immunoassay in Cobas Integra
Centrifuge Serum Extraction
IL-6
Storage
ELISA
Clot
CRP

STATISTICAL ANALYSIS:
• Software: Statistical Package for Social Science version 10
• Tests: Chi square test
Student’s paired t test
• P value < 0.05 – Statistically significant

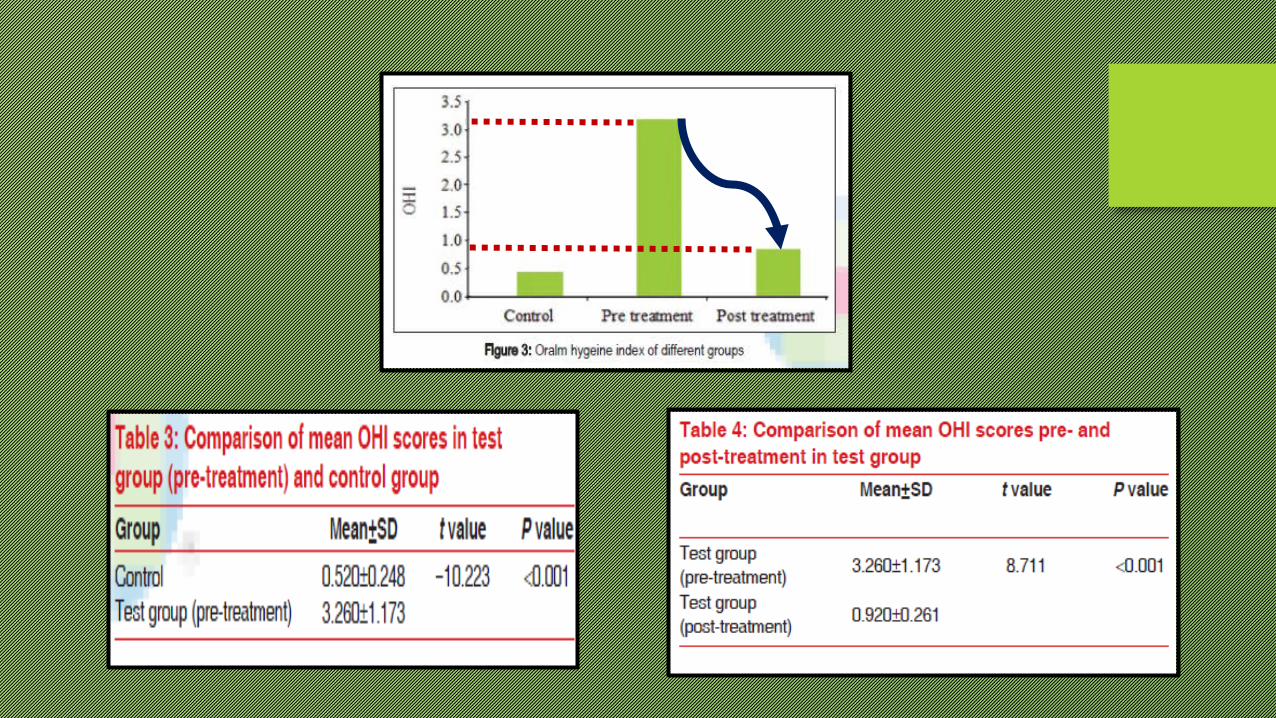
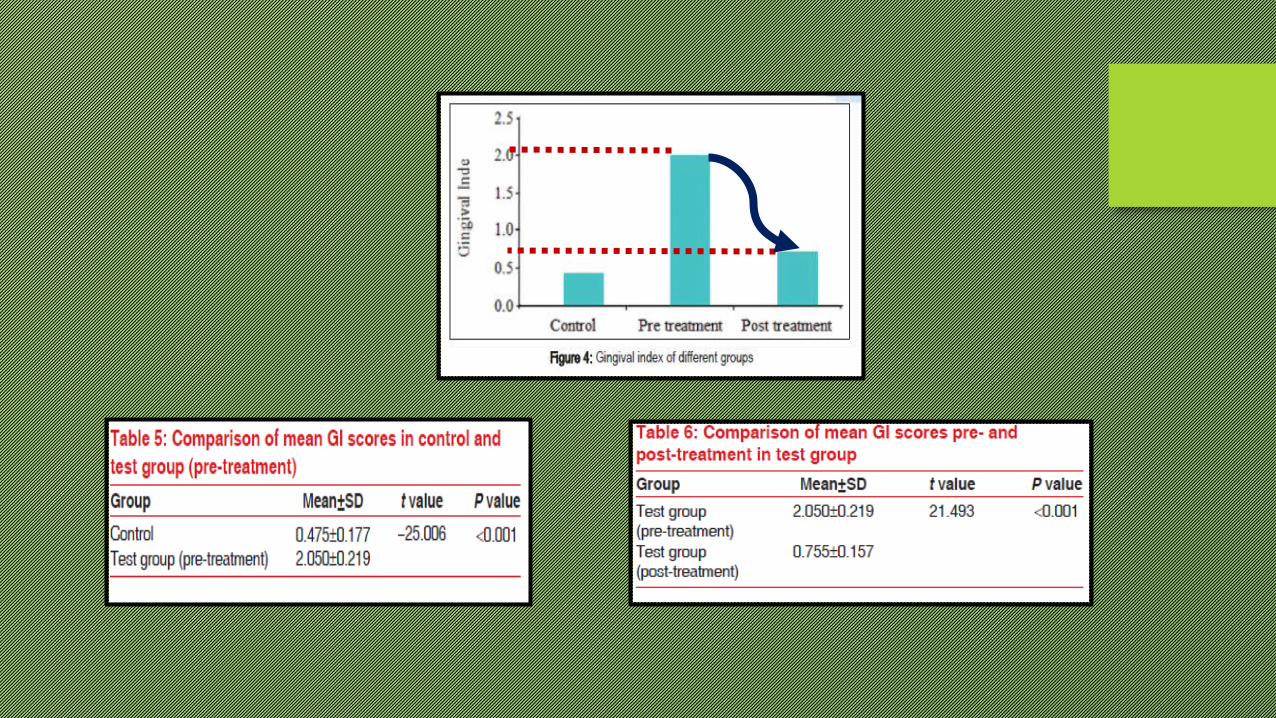
RESULTS:
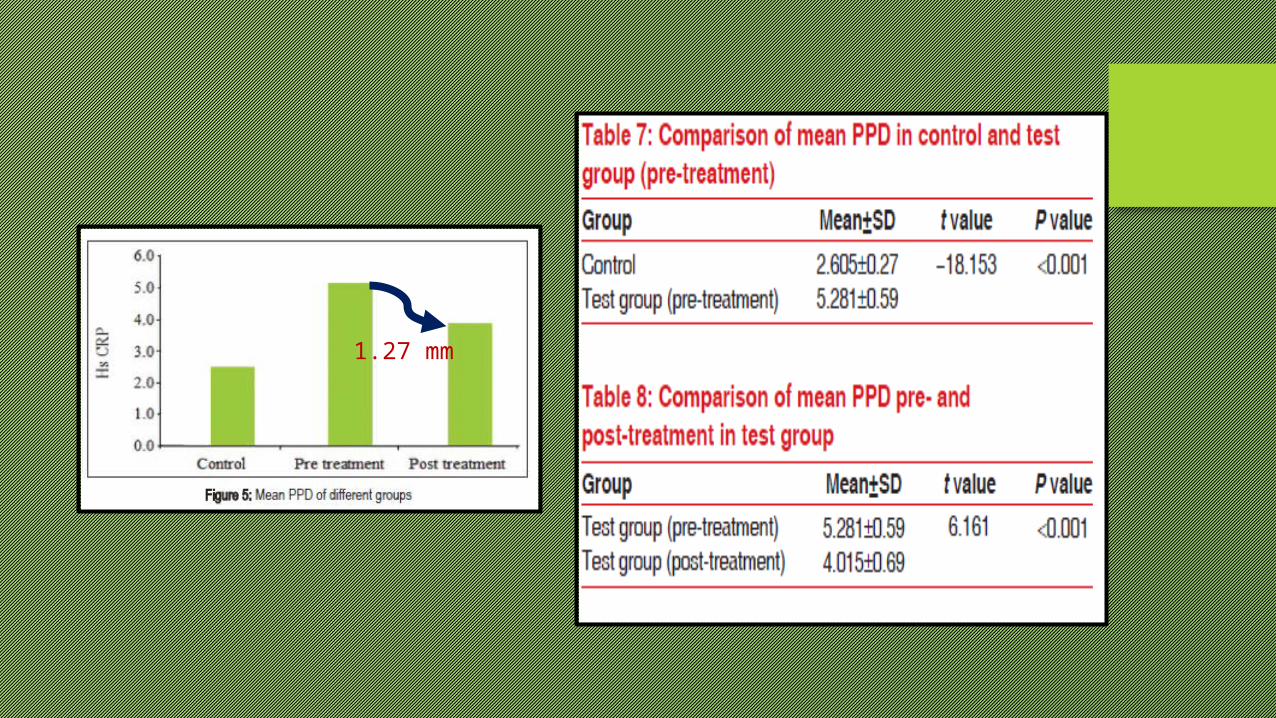
1.27 mm
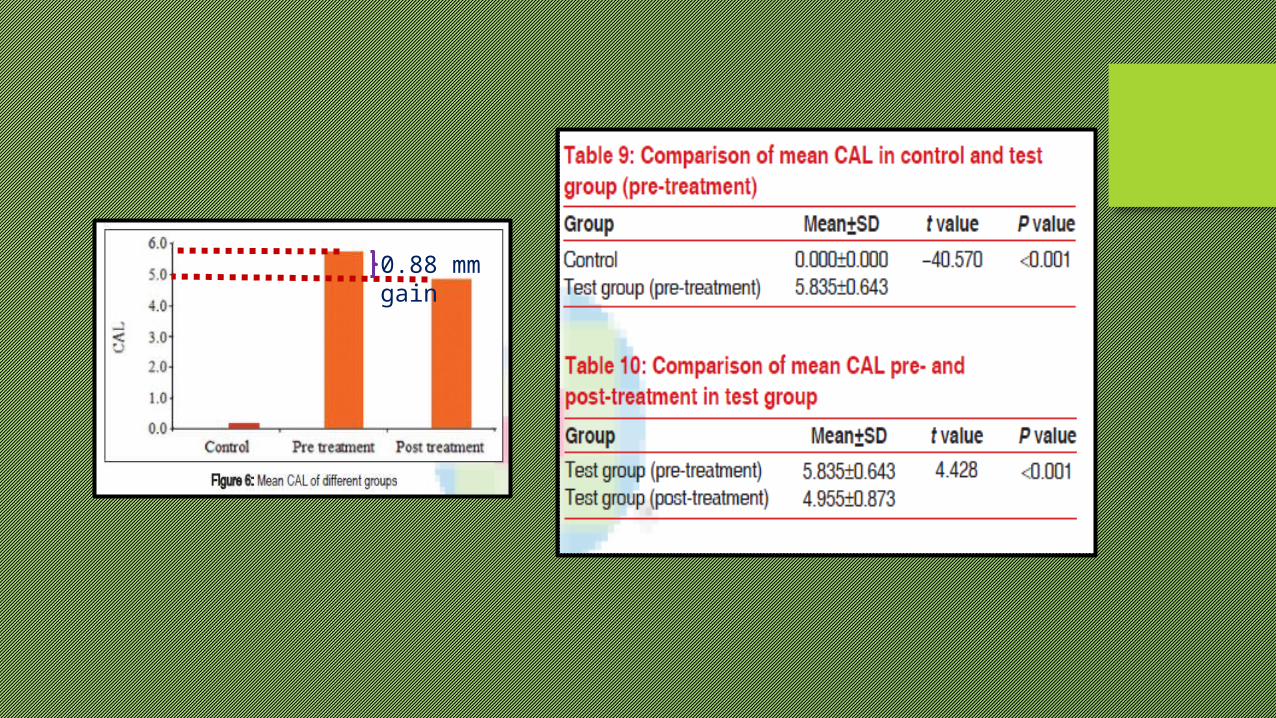
0.88 mm gain

7.43 pg/ml

DISCUSSION:
• The mean OHI score, mean GI score, and PPD were significantly higher for patients in the test group than
in the control group
• After non‑surgical periodontal therapy, there was a significant reduction of the OHI score, GI score, and
PPD, and a gain of attachment.
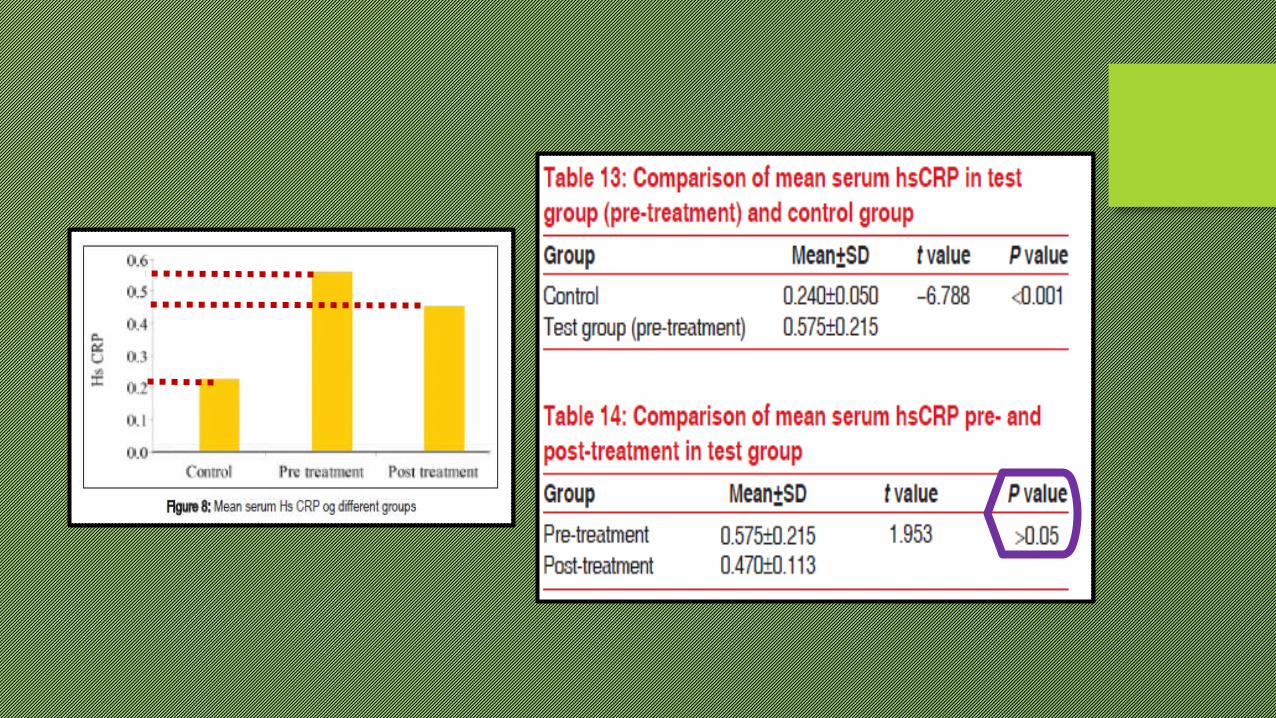
• IL- 6 was found to be decreasing following NSPT whereas there was no significant difference in hsCRP
levels

• Tonneti et al. Treatment of Periodontitis and Endothelial Function. N Engl J Med
2007;356: 911-20 report from their study that CRP and IL‑6 levels did decrease 6 months
after therapy in both treatment groups, standard periodontal therapy and intensive
periodontal therapy, but Tonetti and colleagues suggest that CRP and other markers might
not adequately reflect the relevant inflammatory pathways or that the long‑term
improvements were independent of the systemic inflammatory response.
Review of literature:
• D’ Aiuto et al. Control of the Local Infection is Associated with a reduction in
Serum Inflammatory Markers. J Dent Res 2005;84:156-60 conducted a pilot study
on 94 subjects and assessed serum CRP and IL‑6 levels at baseline and at 2 and 6
months following non‑surgical periodontal therapy. They found significant reductions in
CRP and IL‑6 serum levels, along with improvement in all clinical periodontal
parameters with therapy.

• Loos et al. Elevation of systemic markers related to cardiovascular diseases in the
peripheral blood of Periodontitis Patients. J Periodontol 2000; 71: 1528- 34 in his study
examined the levels of IL‑6 and CRP in the peripheral blood of periodontitis patients. They
found that CRP, IL‑6, and neutrophil levels were elevated in periodontitis patients. He found
IL‑6 to increase in a dose‑dependent manner. In general, patients with chronic severe
generalized periodontitis had much higher levels and were much more often positive for IL‑6
than the controls, because IL‑6 could not be measured in many controls.

• Sothern et al. Ircadian characteristics of circulating IL-6 in men. J Allergy Clin
Immunol 1995;95:1029-35 in their study found that the average IL-6 values ranged
from 1.66 to 5.38 pg/ml, with the lowest to highest values within 24 h ranging from 1.20
to 7.58 pg/ml between subjects.
CRITICAL APPRAISAL:
• Small Sample size
• The authors themselves mention that a few patients were lost to follow-ups
• The article does not assess the effects of hypertension, education, or cholesterol on
these findings.
Conclusion:
• Severe generalized periodontitis seems to contribute to systemic inflammation.
• Periodontal therapy can cause reductions in the serum levels of proinflammatory cytokines like IL‑6.
• The level of the acute phase reactant CRP did not show significant reduction 2 months after non‑surgical periodontal therapy.
• No periodontal treatment protocols are available that are specifically designed to improve systemic status.
• Further studies in this regard could lead to the emergence of novel therapeutic measures.
