the significance of aberrant or heterotopic parotid
TRANSCRIPT
THE SIGNIFICANCE OF ABERRANT OR HETEROTOPIC PAROTID GLANDTISSUE IN'LYMPH NODES*
R. B. BROwN, CAPTAIN, MC, U. S. N., R. A. GAILLARD, COMMANDER, MC, U. S. N.J. A. TuRNER, COMMANDER, MC, U. S. N.
BETHESDA, MARYLAND
FROAI THE U. S. NAVAL HOSPITAL AND THE U. S. NAVAL MEDICAL SCHOOL, NATIONAL NAVAL MdEDICAL CENTER, BETHESDA, MARYLAND
INTEREST IN THIS subject was stimulatedby recent experience which may be sum-marized as follows. In several instancessmall tumors in or adjacent to the parotidsalivary gland were removed and on his-tological examination appeared to be nor-mal or enlarged lymph nodes containingnormal salivary tissue. This finding was atfirst accepted as rare and interesting, butprobably not clinically significant except asit complicated differential diagnosis oftumors in the parotid region.
Several months following the removalof one of these nodes, the patient returnedwith another tumor in the parotid region.This was removed by partial parotidec-tomy, and on microscopic examinationproved to be a muco-epidermoid carcinomaof the parotid gland. Needless to say thisstimulated a great deal of discussion andthought among the clinicians and patholo-gists involved. Was this benign-appearingsalivary tissue in lymph nodes in truthmetastatic from a primary unrecognizedtumor in the parotid in all instances; anal-ogous to the "lateral aberrant thyroid" or"benign metastasizing thyroid" in its rela-tionship to primary thyroid tumors? Orwas this combination of lymphoid andsalivary tissue in the region of the parotid
* The statements and conclusions publishedby the authors are the result of their own studiesand do not necessarily reflect the opinion or policyof the Navy Department. Submitted for publica-tion July, 1953.
a developmental or congenital anomaly,associated with a primary tumor in theparotid in one instance merely by chance?The literature was reviewed, postmortemmaterial examined, and our cases were re-studied, to provide an answer to thisproblem.
REVIEW OF THE LITERATURE
There are relatively few reports to befound in the medical literature on aberrantor heterotopic parotid tissue in lymphnodes. Those articles which are availabledeal with this topic primarily from theanatomic or histologic standpoint. Appar-ently the subject has received little atten-tion from the clinician.
Neisse3 (1898) consistently found gland-ular inclusions in the lymph nodes in andaround the parotid of 14 newborn infantsexamined at the postmortem table. He thencarried this study to fetuses of varioussizes, and came to the conclusion that par-otid tissue grows into, and is included in,the lymph nodes as they develop. Lowen-stein2 (1910) studied the parotid glandsof embryos and very young children, 40in all. In practically every case he foundparotid lobules in small lymph nodes asdescribed by Neisse. These parotid aciniand excretory ducts were scattered irreg-ularly throughout the nodes.
Nicholson4 (1922) reported two casespertinent to the subject. He found tubules
850
HETEROTOPIC PAROTID GLAND TISSUE IN LYMPH NODES
which had the same structure as thesmaller ducts of the parotid in a smalllymph node under the capsule of the par-
otid in a 25-year-old woman. Identicaltubules were seen in a tuberculous pre-
parotid lymph node in a child of 18months. The author stated that thesetubules had become separated from theparotid and enclosed by lymphoid tissueduring development, an abnormal blend-ing of tissues. In a subsequent article,5Nicholson presented two cases which hebelieved were instances of tumor forma-tion of the heterotopic salivary epithelium.This concept has been carried up to date indiscussions on the pathogenesis of the so-
called Warthin's tumor, but is not relevantto our problem.
Bairatil (1932) examined fetuses invarious stages of development, infants, andadults up to 83 years of age, and found,with absolute constancy, glandular ele-ments in the lymph nodes of the parotidregion. These glandular elements were
both ducts and acini, identical to thestructure of the parotid gland. The authordemonstrated that, at least in the firstyears of life, these excretory canals re-
mained in material continuity with theprincipal excretory system of the salivarygland. In subsequent years phenomena ofundifferentiation were observed, and theadenomeres and excretory canals lost theirspecific characteristics. However, in atleast some of the lymph nodes of all of thesubjects examined, numerous epithelialaccumulations with specific characteristicspersisted.Thompson and Bryant6 ( 1950), in an
investigation into the histogenesis of pap-
illary cystadenoma lymphomatosum of theparotid, contributed to the subject underdiscussion. They studied 18 human em-
bryos and in the older ones (over 14weeks), found lymph nodes containingsalivary gland ducts both inside and out-
side the capsular area of the parotid
gland. They also examined 100 presumablynormal salivary glands obtained at autopsy,
and in six cases, parotid gland ducts were
identified in lymph nodes. In all but one
of these latter cases the glands were fromadults. In commenting on these observa-tions, Thompson and Bryant stated thatlymph nodes containing salivary glandducts may be the seat of chronic hyper-plastic lymphadenitis secondary to some
inflammatory process about the head andneck. They felt that some of these may beconsidered erroneously as true adeno-lymphomas.
POSTMORTEM STUDY
A study to determine the incidence ofheterotopic salivary tissue in lymph nodeswas undertaken in our laboratory. Thisconsisted of the examination of totally ex-
cised parotid glands and adjacent lymphnodes, which limited our study to bodiesof newborn infants.At least one recognizable lymph node
containing salivary gland acini and ductshas been found in all of the newborn in-fants examined to date, a total of 19. Usu-ally more than one such lymph node was
found. No significant observations were
made on location of the lymph node. Somewere deep within the parotid gland whileothers were adjacent but extracapsular.The microscopic appearance varied froma loose intermingling of lymphoid and par-
otid tissue to almost complete inclusion ofa large mass of normal salivary glandtissue within a well-delineated lymph node.The study is being continued, but the
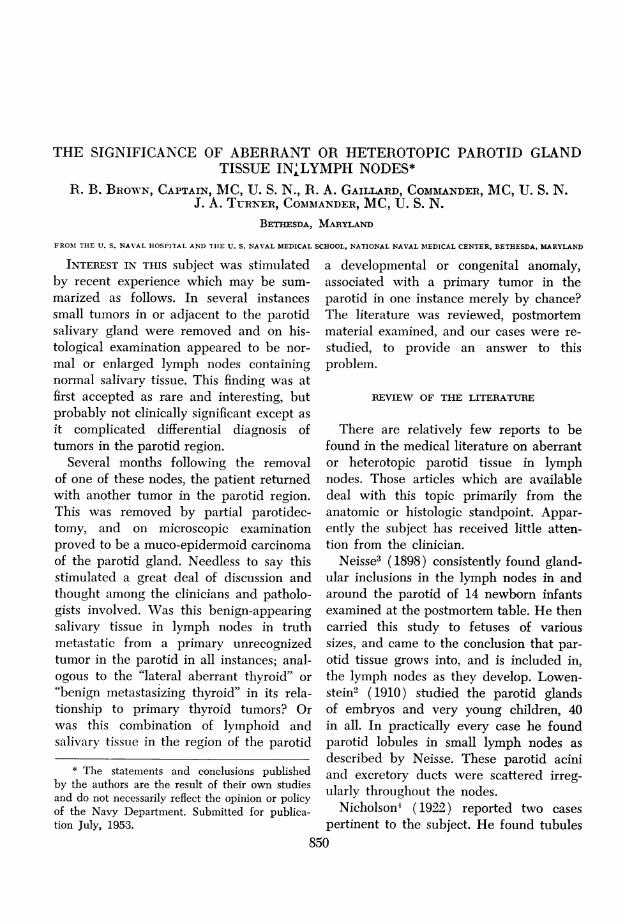
100 per cent incidence demonstrated thusfar verifies the observations cited. Sincepreviously published illustrations have
been almost entirely diagrams or draw-ings, an actual photomicrograph showingintermingling of parotid and lymphoid tis-
sues in the newborn is submitted (Fig. 1).851
Volume 138Number 6
BROWN, GAILLARD AND TURNER
CASE REPORTS
Case 1. This 28-year-old white man was ad-mitted to the hospital on September 26, 1951,with a diagnosis of malignant melanoma. Threeweeks previously he had been seen at another
FIG. I
On October 11, 1951, a wide excision of theprimary site of the melanoma, with radical neckdissection, was performed.
Pathology Report. No metastatic melanomawas found in any of the excised tissues. However,
FIG. 2
FIG. 3 Fic. 4
FIG. 1. Photomicrograph shows intermingling of salivary gland and lymphoid tissue withinthe parotid of a newborn. (Hematoxylin and eosin stain; x 38.)
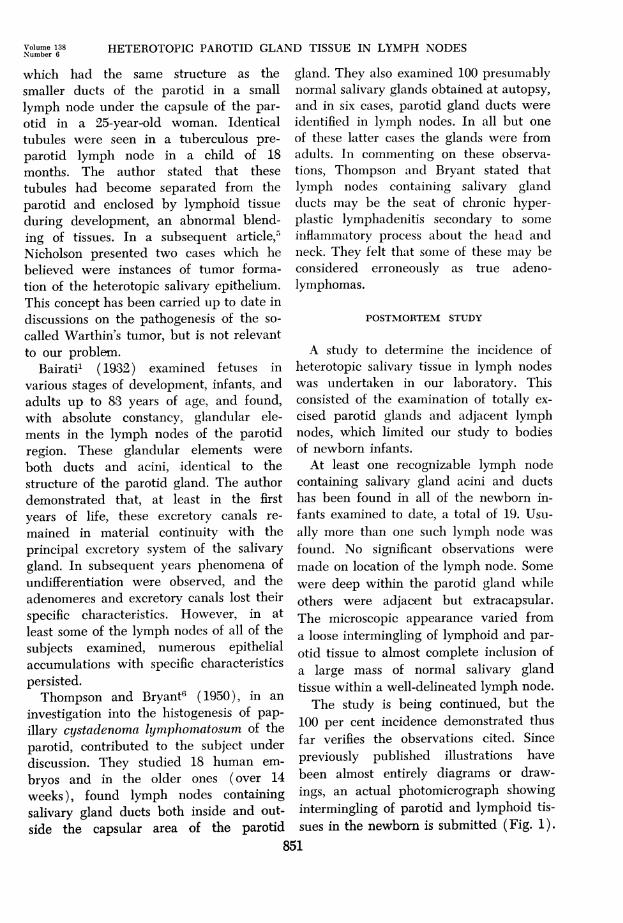
FIG. 2. (Case 1) Photomicrograph shows a large nodule of salivary ducts and acini par-tially surrounded by a well-delineated lymph node. At other levels, the lymph node com-pletely surrounded the salivary gland tissue. (Hematoxylin and eosin stain; x6.)
FIG. 3. (Case 1) Photomicrograph shows moderate distortion of the heterotopic salivarygland tissue. The very dark appearance of the acini is due to the heavy content of eosino-philic granules. Ductal structures are well preserved. Note moderate atrophy and replace-ment by adipose tissue. (Hematoxylin and eosin stain; x76.)
FIG. 4. (Case 2) Photomicrograph shows a thin rim of lymphoid tissue completely sur-rounding atrophic salivary gland tissue largely replaced by adipose tissue. (Hematoxylin andeosin stain; x12.)
hospital, where a small black skin lesion hadbeen excised from its location just posterior toand below the right ear lobe. The diagnosis ofmalignancy had been made by microscopic studyof the excised specimen.
The physical examination was essentially neg-
ative except for a well-healed, 2 cm. scar belowthe right ear lobe, a posterior cervical node 1 cm.
in diameter on the right, and bilateral, palpablesubmaxillary nodes. Routine laboratory studieswere noncontributory.
there was a large lymph node 2 cm. in diameterlocated -between the parotid gland and the ster-nomastoid muscle. Cut surfaces revealed a tannodule 1.5 cm. in diameter within this lymphnode. Figures 2 and 3 demonstrate the micro-scopic findings. Serial sections revealed that themass of salivary gland tissue was surrounded onthree sides by a well-delineated lymph node.There was moderate reticuloendothelial hyper-plasia of the lymphoid tissue and moderateatrophy of the salivary gland tissue with replace-
852
Annals of SurgeryDecember, 1 9 5 3
I II
"III
.r11VOf
i
d, ..
HETEROTOPIC PAROTID GLAND TISSUE IN LYMPH NODES
ment by adipose tissue. The pathologist's diag-nosis was "heterotopic salivary gland tissue incervical lymph node."
The patient was last seen for follow-up exam-
ination on January 6, 1953. At that time he hadno complaints. His wounds remained well-healedand there were no demonstrable local or nodal
FIG. 5
mandible on the right. The mass seemed to beattached to the parotid gland.
Dental examination, including roentgeno-grams, was negative for foci of infection in themouth. Ear, nose, and throat examinations were
likewise negative. Routine laboratory studies were
noncontributory.
FIG. 6
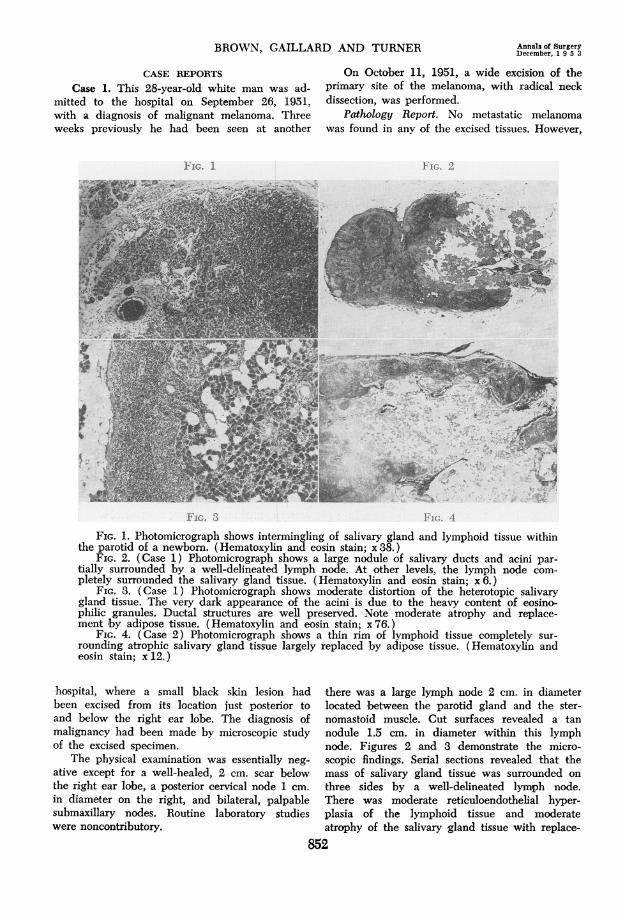
Fic. 7 Fir. 8FIG. 5. (Case 2) Photomicrograph of section stained for reticulum shows details at the
junction of salivary and lymphoid tissue in Figure 4. (Wilder's reticulum stain; x38.)FIG. 6. (Case 3) Photomicrograph shows salivary gland tissue on the left with ducts lying
within the capsule of the adjacent lymph node. (Hematoxylin and eosin stain; x 38.)FIG. 7. (Case 4) Photomicrograph shows a lobulated lymph node with fibrosis of medul-
lary portion. Figure 8 is a high-power photomicrograph of the area within the outlined rec-
tangle. (Hematoxylin and eosin stain; x8.)FIG. 8. (Case 4) Photomicrograph shows distorted salivary gland acini and ducts located
within the outlined rectangle in Figure 7. (Hematoxylin and eosin stain; x 76.)
recurrences in the neck. The lung fields were clearto roentgen examination.
Case 2. The patient, a 33-year-old white man,
was admitted to the hospital on November 28,1951, for repair of a left inguinal hernia. Systemreview was essentially negative, except that thepatient had noted a small lump at the angle ofthe jaw on the right. This had been present forsome time, was not tender, and had not increasedin size.
On physical examination a 2 x 1 cm. discretenodule was demonstrable at the angle of the
With a diagnosis of "probable mixed tumor ofthe parotid," an operation was performed on
December 4, 1951. The tumor was readily ex-
posed and its contiguity with the parotid glandwas demonstrated. The tumor was removed bysuperficial parotid lobectomy. Frozen sectiondiagnosis was "benign."
Pathology Report. The excised specimen con-
sisted of a portion of parotid gland and a lymphnode which measured 1.6 x 1 x 0.4 cm. Cut sur-
faces of the latter revealed a central nodule 0.6cm. in diameter, which differed from the sur-
85t3
Volume 138Number 6
BROWN, GAILLARD AND TURNER
rounding lymph node. Figures 4 and 5 demon-strate the microscopic findings. Serial sections re-vealed lymphoid tissue surrounding salivarygland tissue on three sides in the form of a"cap." There was extensive atrophy of the sali-vary tissue with replacement by adipose tissue.The pathologist's diagnosis was "heterotopic sal-ivary gland tissue in lymph node adjacent to theparotid gland."
The patient was last seen on December 23,1952, at which time there was no evidence ofrecurrence of the tumor in either the remainderof the parotid gland or its satellite nodes.
Case 3. This 38-year-old white female wasadmitted to the hospital on April 7, 1952, fordiagnosis and treatment of a nodule in the rightpreauricular region. The mass was first noticedabout three weeks prior to admission. It was notpainful or tender, and had not changed in sizesince it was discovered.
Examination revealed a well-circumscribed,non-tender, 1 x 1 cm., globular mass just anteriorto the ear in the right parotid region. It was notfixed to the skin and moved freely in the under-lying tissue. The remainder of the physical exam-ination was noncontributory.
Blood count showed a slight anemia, but wasotherwise normal. Urine examination and Kahntests were negative. The heart and lungs werenegative to roentgen examination.
The preoperative diagnosis was mixed tumor ofthe parotid or an enlarged parotid lymph node.Operation was performed on April 8, 1952. Thetumor nodule lay deep in the superficial lobe ofthe parotid gland and was not visualized untilthe lobe had been mobilized for resection. Themass had the gross appearance of a lymph node.
Pathology Report. The excised specimen con-sisted of a portion of parotid gland which meas-ured 5 x 3 x 1 cm. On one surface there was anodule 0.4 cm. in diameter which resembledlymph node. Figure 6 demonstrates the micro-scopic findings. There was a thin peripheral rimof salivary gland tissue about the lymph node. Atseveral points small ducts resembling those ofparotid gland were demonstrated within the cap-sule of the lymph node. There was extensivereticuloendothelial hyperplasia throughout thenode. The pathologist's diagnoses were "hetero-topic salivary gland ducts within lymph node"and "reticuloendothelial hyperplasia, lymph node."
Case 4. This 32-year-old white man was ad-mitted to the hospital on September 11, 1952,for excision of a small mass located at the angleof the jaw on the left. In May of 1951, the
patient had had a left hemithyroidectomy withexcision of adjacent lymph nodes for what provedto be an undifferentiated carcinoma of the thy-roid. In June of the same year, a left radical neckdissection had been performed and metastaseswere demonstrated in several of the removed cer-vical nodes. Convalescence had been uneventfuland periodic follow-up examinations, includingchest roentgenograms, had revealed no definiteevidence of local recurrence or distant metastases.However, the nodule at the angle of the jaw onthe side of the radical neck dissection had beennoted by the patient some months prior to ad-mission.
Examination revealed a well-healed scar ofthe previous thyroidectomy and left radical neckdissection. There was a soft, movable, non-tendermass 2 cm. in diameter, located at the tip of themastoid on the left. There was no demonstrableattachment of the tumor to the overlying skin.The remainder of the physical examination was
essentially negative. Routine laboratory studieswere noncontributory. On September 12, 1952, themass was excised.
Pathology Report. The excised specimen hadthe gross appearance of a lobulated lymph nodeand measured 1.4 x 0.5 x 0.5 cm. Figures 7 and8 demonstrate the microscopic findings. Withinthe medulla of the lymph node there were sev-eral small masses of fibrosed and distorted salivarygland tissue. There was marked fibrosis and mod-erate hyperplasia of follicles throughout the node.The pathologist's diagnoses were "heterotopicsalivary gland in lymph node adjacent to theparotid gland" and "chronic lymphadenitis."
Convalescence was uneventful. The patientwas last seen on February 5, 1953. At this time hehad no new complaints and there were no newnodules demonstrable in the neck or left parotidregion. Chest roentgenogram was negative.
Case 5. This 25-year-old white female wasfirst admitted to the hospital on October 11, 1951.During the year previous to admission she hadnoticed a firm, slowly enlarging, non-tender massat the angle of her mandible on the right.
Physical examination on admission was essen-
tially negative, except for a firm, movable masssituated beneath the skin overlying the right par-otid gland. Laboratory and roentgenographicstudies were essentially normal.
On October 12, 1951, operation was per-formed. The subeutaneous mass was found to beattached to the external parotid capsule. It wasexcised. The frozen tissue diagnosis was "benign."
Pathology Report. The mass excised from theexternal parotid capsule was firm, globular, and
854
Annals of SurgeryDecember, 1 9 5 3
HETEROTOPIC PAROTID GLAND TISSUE IN LYMPH NODE
measured 0.8 cm. in diameter. The microscopicappearance was that of a fibrosed and hyalinizedlymph node (Fig. 9) within which there were
remnants of distorted salivary gland ducts andacini (Fig. 10). At the periphery there was a
structure (Fig. 11) interpreted as a salivary ductwith metaplastic changes. The pathologist's diag-
FIG. 9
Physical examination, laboratory and roent-genologic studies were essentially normal exceptfor a rather fixed, firm mass in the same positionas the previously removed lesion.
A second operation was performed on October7, 1952, at which a 2 cm. firm, irregular, fibroticmass was noted with the mandibular and cer-
FIG. 10
;>. feX *
FIG. 12FIG. 11
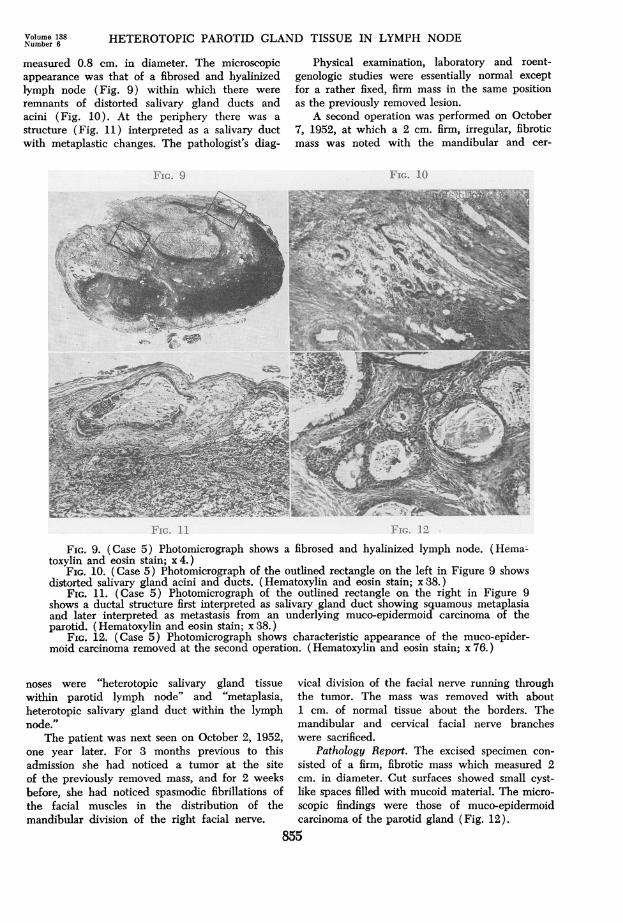
FIG. 9. (Case 5) Photomicrograph shows a fibrosed and hyalinized lymph node. (Hema-toxylin and eosin stain; x4.)
FIG. 10. (Case 5) Photomicrograph of the outlined rectangle on the left in Figure 9 showsdistorted salivary gland acini and ducts. (Hematoxylin and eosin stain; x 38.)
FIG. 11. (Case 5) Photomicrograph of the outlined rectangle on the right in Figure 9shows a ductal structure first interpreted as salivary gland duct showing squamous metaplasiaand later interpreted as metastasis from an underlying muco-epidermoid carcinoma of theparotid. (Hematoxylin and eosin stain; x 38.)
FIG. 12. (Case 5) Photomicrograph shows characteristic appearance of the muco-epider-moid carcinoma removed at the second operation. (Hematoxylin and eosin stain; x 76.)
noses were "heterotopic salivary gland tissuewithin parotid lymph node" and "metaplasia,heterotopic salivary gland duct within the lymphnode."
The patient was next seen on October 2, 1952,one year later. For 3 months previous to thisadmission she had noticed a tumor at the siteof the previously removed mass, and for 2 weeksbefore, she had noticed spasmodic fibrillations ofthe facial muscles in the distribution of themandibular division of the right facial nerve.
vical division of the facial nerve running throughthe tumor. The mass was removed with about1 cm. of normal tissue about the borders. Themandibular and cervical facial nerve brancheswere sacrificed.
Pathology Report. The excised specimen con-
sisted of a firm, fibrotic mass which measured 2cm. in diameter. Cut surfaces showed small cyst-like spaces filled with mucoid material. The micro-scopic findings were those of muco-epidermoidcarcinoma of the parotid gland (Fig. 12).
855
Volume 138Number 6
BROWN, GAILLARD AND TURNER Annals of SurgeryDecember, 1 9 5 3
With these new findings, the sections fromthe tissue removed at the first operation werereviewed and the structure originally interpretedas heterotopic salivary gland duct showing meta-plasia (Fig. 11) was, in retrospect, considered ametastasis from the muco-epidermoid carcinoma.The pathologist's diagnosis was "muco-epider-moid carcinoma of the parotid gland withmetastasis to a parotid lymph node."
On November 25, 1952, a wide excision of theremaining parotid and a neck dissection were per-formed. On pathologic examination, no additionalmalignancy was found.
Convalescence has been uneventful, and atthe present time there is no evidence of disease.
COMMENT
As a result of this review of the liter-ature, postmortem study, and re-examina-tion of the cases cited, we believe that thefollowing summarizing statements andconclusions are justified.
1. Previous reports have indicated thatheterotopic salivary gland tissue can befound in lymph nodes within or near theparotid gland in the human newborn in-fant; this condition persisting in the adultin some instances.
2. We have demonstrated such findingsin 100 per cent of 19 autopsied newborninfants in confirmation of these previouslycited observations.
3. Five cases have been presented inwhich lymph nodes containing heterotopicparotid tissue have assumed clinical sig-nificance in adults. This entity must beconsidered in the differential diagnosis oftumors in the parotid region.
4. The presence of parotid tissue in theselymph nodes in the adult is believed torepresent a persistence of the heterotopiacommon to newborns. No justification hasbeen found for drawing an analogy be-tween the relationship of parotid tissue inlymph nodes to primary parotid tumorsand "lateral aberrant thyroid" to primarythyroid tumors.
5. Case 5 is regarded as an example ofheterotopic parotid tissue within a lymphnode with concurrent metastasis to thislymph node from an underlying muco-epi-dermoid carcinoma of the parotid gland.
BIBLIOGRAPHY
Bairati, A.: Constante Concrescenza fra nodulilinfatici ed adenomeri delle ghiandole sali-vari nell'uomo durante lo sviluppo e nell'adulto. Arch. de Biol., Paris, 43: 415, 1932.
2 Lowenstein, C.: tYber atypische Epithelwuche-rungem und Tumoren der Speicheldriisen,besonders der Parotis. Frankfurt. Ztschr. f.Path., 4: 187, 1910.
3 Neisse, R.: Uber den Einschluss von Parotis-lappohen in Lymphknoten. AnatomischeHefte., 10: (part 1): 289, 1898.
4 Nicholson, G. W.: Studies on Tumour Forma-tion; Tissue Malformations, Anomalies ofPosition and Blending. Guy's Hosp. Rep., 72:333, 1922.
5 : Studies on Tumour Formation; TheImportance of Congenital Malformations inTumour Formation. Guy's Hosp. Rep., 73:37, 1923.
6 Thompson, A. S., and H. C. Bryant, Jr.: Histo-genesis of Papillary Cystadenoma Lympho-matosum (Warthin's Tumor) of the ParotidSalivary Gland. Am. J. Path., 26: 807, 1950.
856