the social context of public health
TRANSCRIPT
The social context of public healthDistrict Health Management
Community Research and Health Promotion
Session 2015-2016
Assoc Prof Dr Halyna Lugova
Content
1. Definitions of health: models of health
2. Evolution of public health
3. Approaches to health promotion
4. Health needs assessment

Definitions of Health(a) The medical model of health
‘Health is defined as the absence of disease’
(has dominated since Middle Ages in Western societies)
Human body like an intricate machine
Curative model, undermines prevention
Fails to accommodate social causes of diseases
(sanitation, overcrowding)
Subjective perceptions of ill-health disregarded by
health professionals
Medicine is a social enterprise closely linked with
exercise of professional power
Health is measured in terms of its absence:
o incidence, death rates
By studying and mastering the workings
(Physiology) of the parts (Anatomy), we
can understand the operation of the
whole. Simple.
When the parts start to malfunction
(Pathology), we can address them…cure
them…through medicines
(Pharmacology) and/or removal
(Surgery)
Definitions of Health
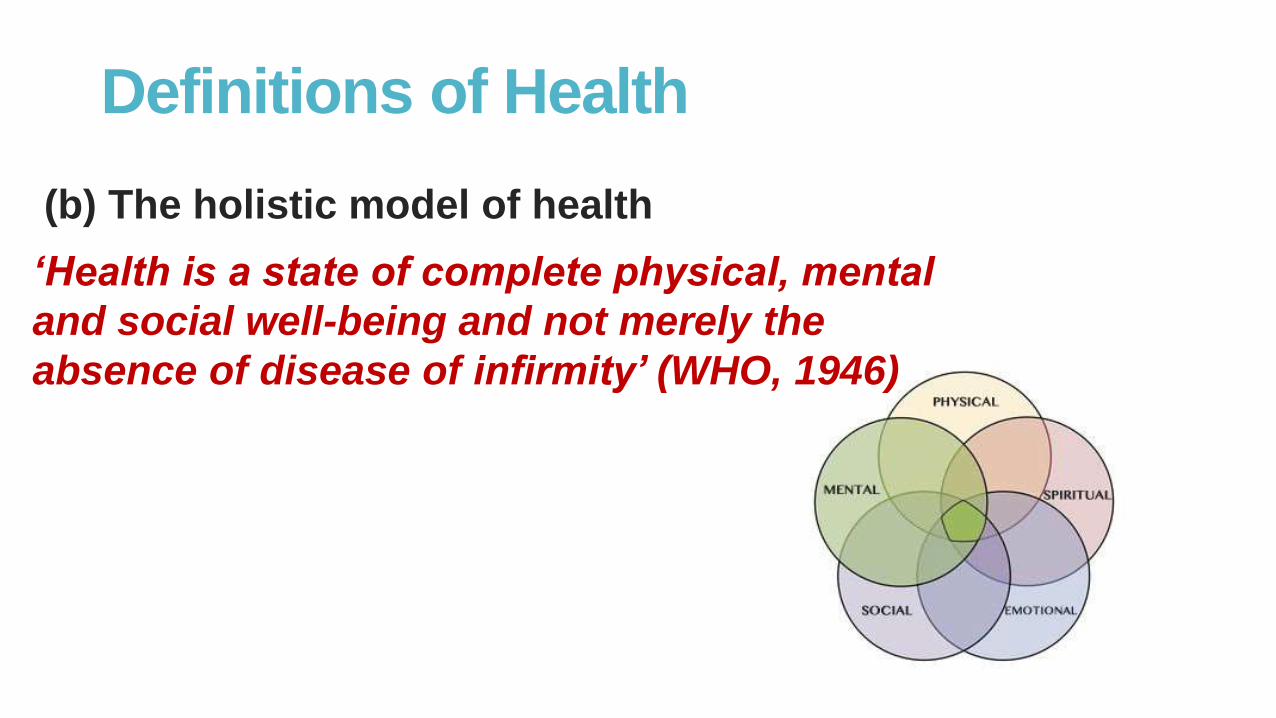
(b) The holistic model of health
‘Health is a state of complete physical, mental
and social well-being and not merely the
absence of disease of infirmity’ (WHO, 1946)
Definitions of Health
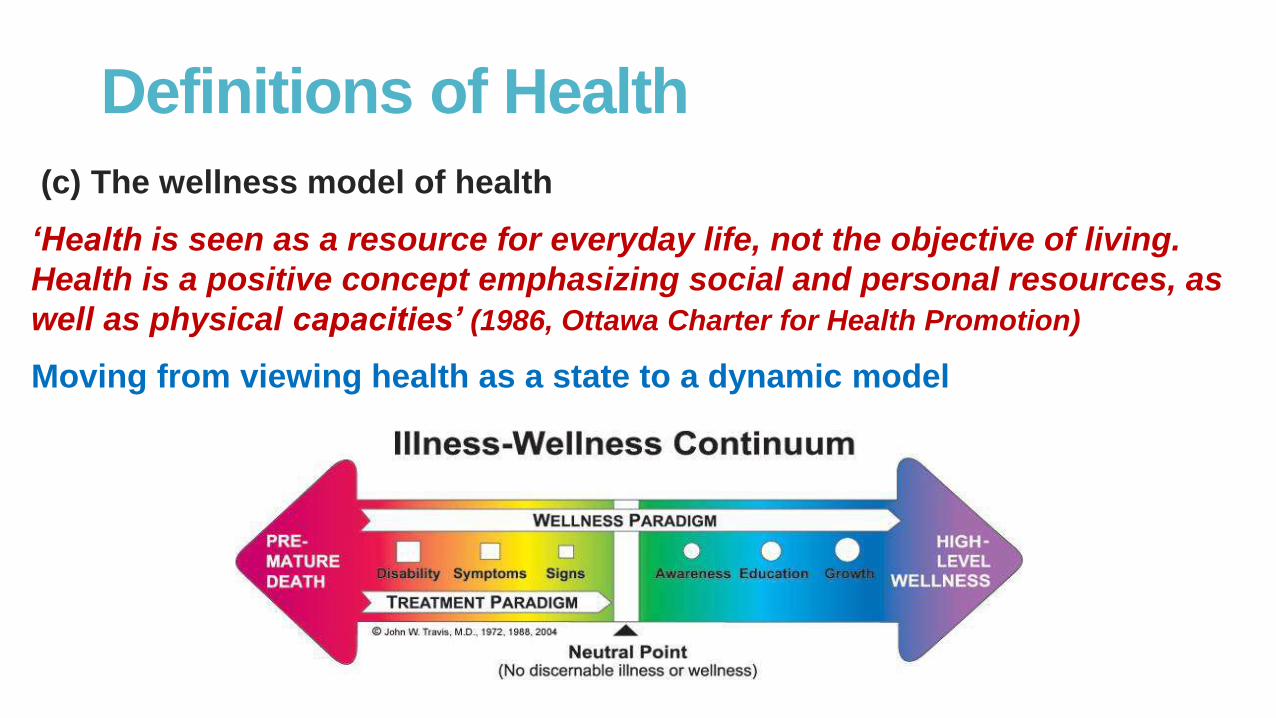
(c) The wellness model of health
‘Health is seen as a resource for everyday life, not the objective of living.
Health is a positive concept emphasizing social and personal resources, as
well as physical capacities’ (1986, Ottawa Charter for Health Promotion)
Moving from viewing health as a state to a dynamic model
(d) Salutogenesis and Quality of Life
Salutogenetic model:
‘Health is viewed in terms of resilience as the capability of individuals and
communities to cope successfully in the case of significant adversity or risk’
(A. Antonovsky, 1996)
Quality of Life model:
‘Health is not a condition that one introspectively feels in oneself. Rather, it
is condition of being involved, of being in the world, of being together with
one‘s fellow human beings, of active and rewarding engagement in one‘s
everyday tasks’ (Gadamer, 1986)
Definitions of Health
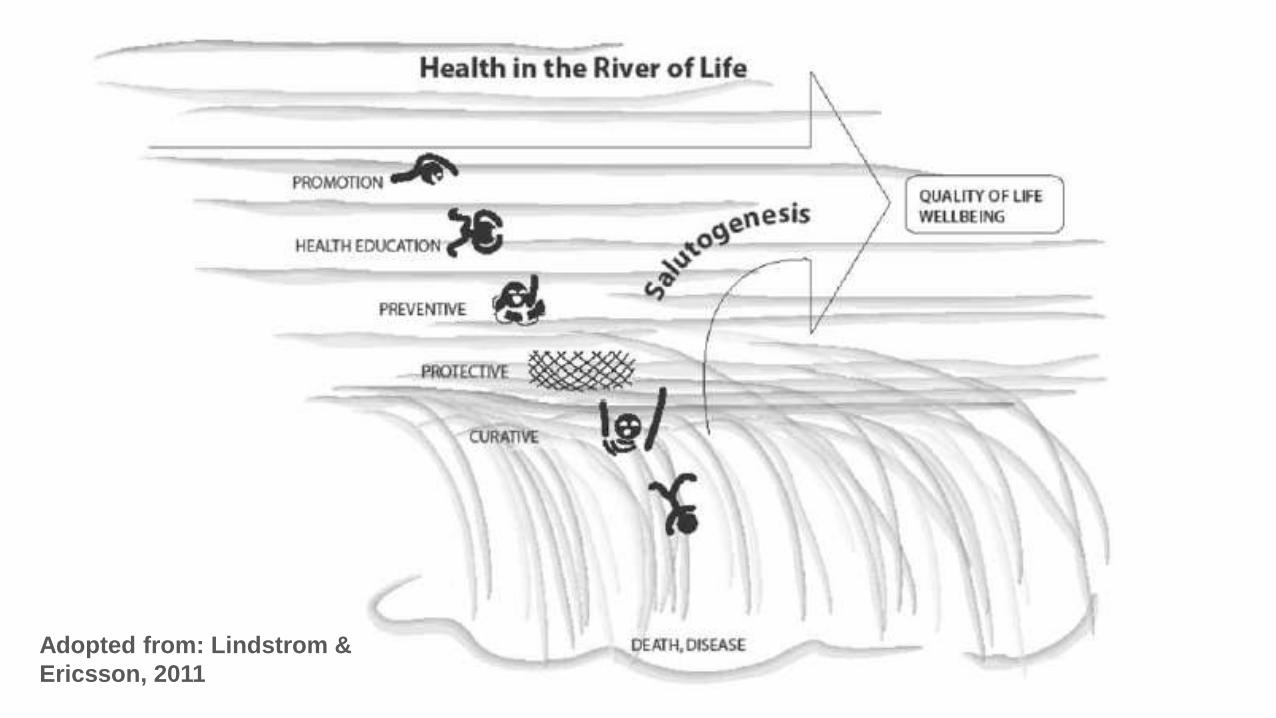
Adopted from: Lindstrom &
Ericsson, 2011
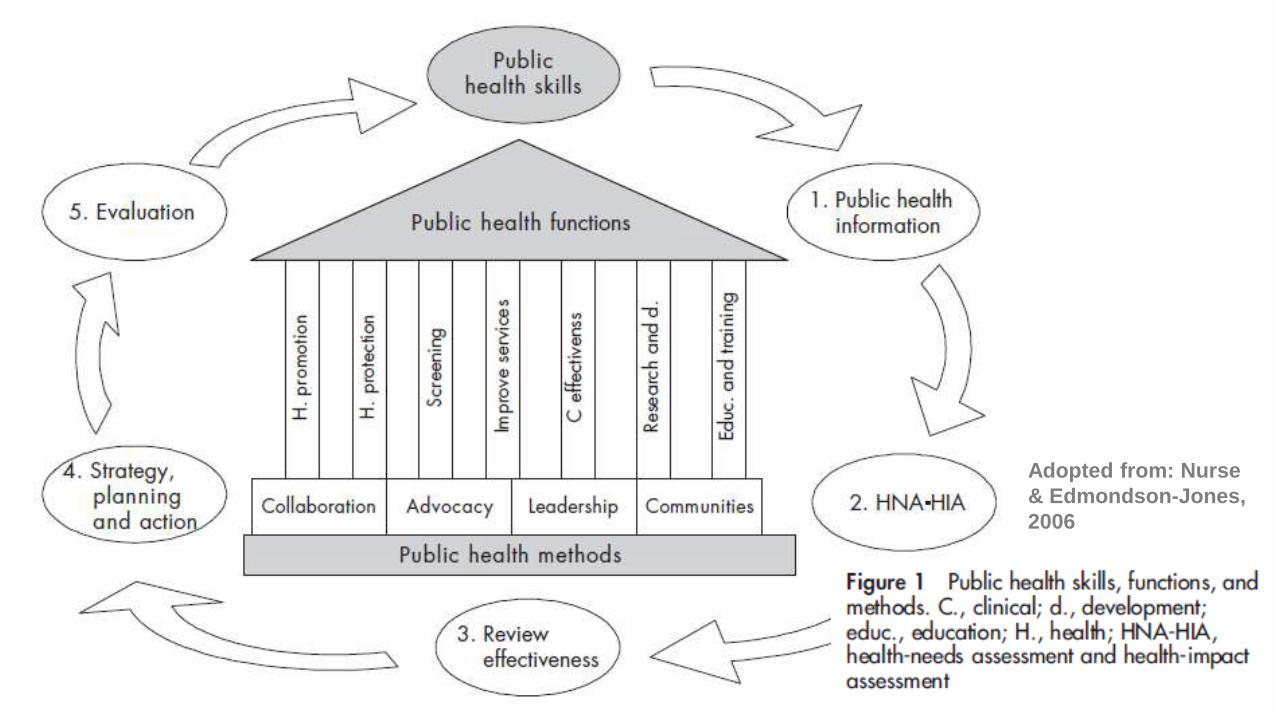
Adopted from: Nurse
& Edmondson-Jones,
2006
Evolution of Public Health
1) Health Protection
Antiquity – 1830
• Enforced regulation of
human behaviour
• Religious practices,
customs and
quarantine
Evolution of Public Health
2) Miasma Control
1840 – 1870
• Addressing unsanitary
environmental
conditions
• Potable water and
sanitation programs
Evolution of Public Health
3) Contagion Control
1880 – 1930
• Germ theory:
infectious origins of
diseases
• Vaccination,
Chemotherapy
Evolution of Public Health
4) Preventive Medicine
1940 – 1960
• Focus on “high-risk”
groups
• Medical dominance
• Treatment of
communicable diseases

Evolution of Public Health
5) Primary Health Care
1970 – 1980
• Health for All
• Preventive approach
• Emphasis on equity
• Social determinants of
health
Evolution of Public Health
6) Health Promotion
1990 – present
• Educational, economic
and political actions
enabling (empowering)
individuals and
communities to increase
control over, or improve,
their health

Health PromotionIt is widely considered that health promotion is the
cornerstone of primary health care and is therefore a core
function of public health.
Factors amenable to HP include:
• Individual lifestyle factors
• Social and community networks
• Living and working conditions
• General socio-economic, cultural, and environmental conditions
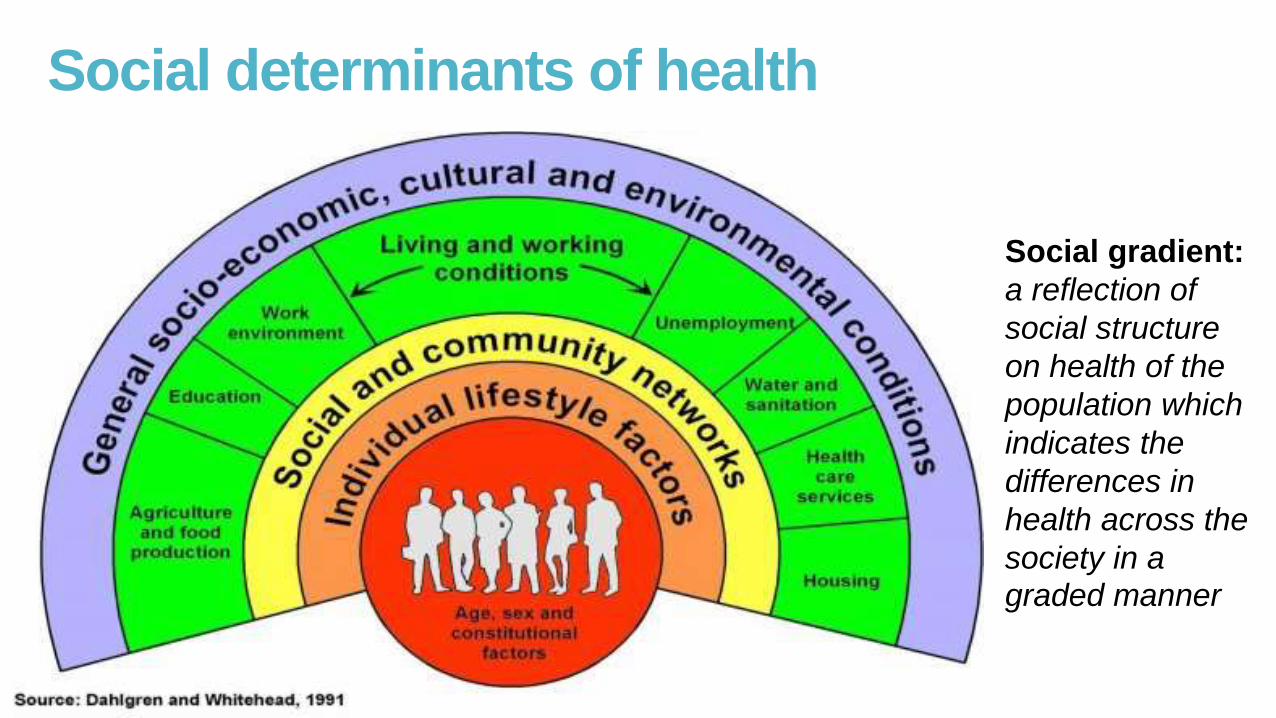
Social determinants of health
Social gradient:
a reflection of
social structure
on health of the
population which
indicates the
differences in
health across the
society in a graded manner

1) The medical approach
Preventive services
Aims to reduce morbidity & mortality
Three levels of prevention
Expert-led, top-down
2) Behavior change
Encourage individuals to
adopt healthy behaviors
One-to-one counselling
Seek to ensure
compliance
Expert-led, top-down
3) Educational approach
Does not set out to
persuade change
Provide knowledge
so that people can
make an informed
choice
Health education
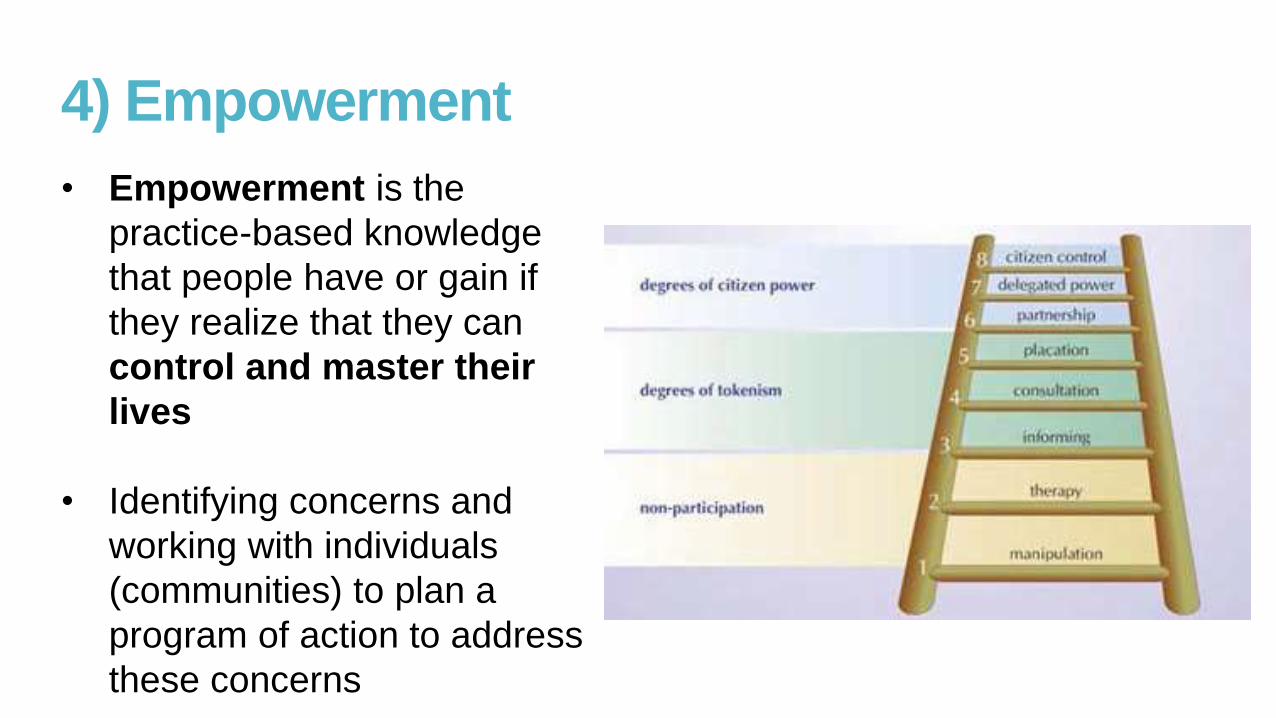
4) Empowerment
• Empowerment is the
practice-based knowledge
that people have or gain if
they realize that they can
control and master their
lives
• Identifying concerns and
working with individuals
(communities) to plan a
program of action to address
these concerns
5) Social change
• Focus at the policy
• Environmental level
• Broader socio-economic
determinants of health
• ‘To make the healthy
choice the easier choice’
• Lobbying, policy
planning, advocacy
Critique of approaches directed towards individual or lifestyle determinants of health
It involves considerable effort for a person to change his or her
habits or routines.
People adopt a certain behaviour or lifestyle for various reasons.
Health is not always a salient issue in people’s lives.
People are sometimes prevented from making lifestyle
changes for reasons outside their personal control. Not
everyone has the same choices.

Health needs assessment
Normative needs
Felt needs
Expressed needs
Comparative needs
Maslow hierarchy
of basic needs
Health needs assessment
What information is needed?
How can I find out this information?
What am I going to do with the information?
What scope is there to act on the information?

What information is needed?
A community profile:
Age profile, social networks
Extent of economic activity and unemployment, housing, transport links, green areas, air pollution
Availability of health service provision
Health improvement programs
Indicators of the state of health:
Self-reported health
Life expectancy
Mortality rates and cause
Morbidity
A community profile:
Age profile, social networks
Extent of economic activity and unemployment, housing, transport links, green areas, air pollution
Availability of health service provision
Health improvement programs
Indicators of the state of health:
Self-reported health
Life expectancy
Mortality rates and cause
Morbidity
Gathering information
Routine information (e.g. census,
local authority data)
Public meetings and forums
Interviews with users
Focus groups
Use local media
Rapid appraisals, ethnographic
studies
Whose needs count?
There will be disadvantaged individuals
who do not have opportunities for
expression: harder to reach groups:
Homeless
Unemployed
Residing in a remote area
Ethnic minorities
Illegal immigrants
Getting cross-section of a community,
comparing information between different
population groups will help to identify
health needs of the disadvantaged
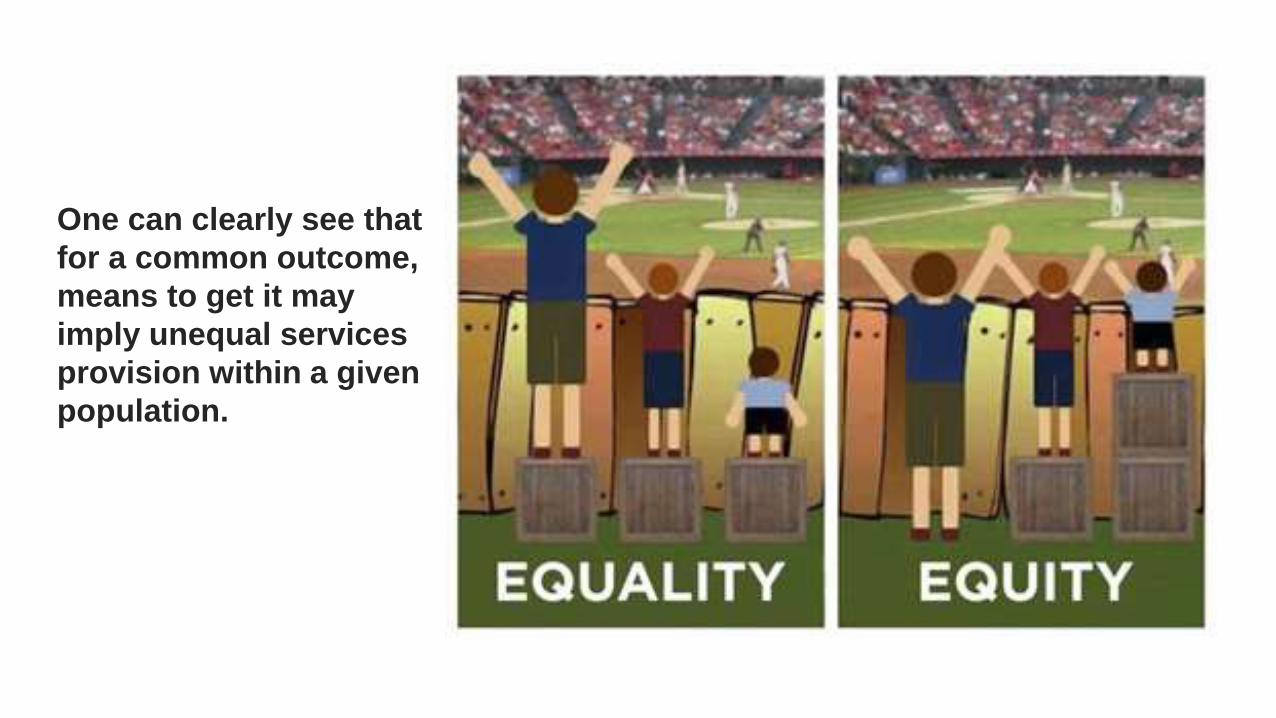
One can clearly see that
for a common outcome,
means to get it may
imply unequal services
provision within a given
population.
Setting priorities
The issue should be a major cause of premature death or
avoidable ill health in the population as a whole or amongst specific
groups
There are marked inequalities in those who suffer ill health or
premature death
Effective intervention should be possible
Locally determined priorities, e.g. diabetes, elderly people’s health

Summary1) We discussed the principles of health promotion: definitions and models
of health, approaches to health promotion, social determinants of health.
2) We discussed how health needs are to be defined and how this should
inform program planning and development.
3) Health Promotion is a concept and a strategy for reducing health
inequalities and closing the health gap between the rich and the poor, and
the socially advantaged and disadvantaged groups.
4) Action at all levels is required: empowering individuals and
communities, building community capacity, advocacy, building healthy
public policy to create environments that support and sustain health and
well-being.

References:Antonovsky, A. (1996) ‘The salutogenic model as a theory to guide health promotion’, Health Promotion
International, 11 (1), pp. 11–18.
Awofeso, N. (2004) ‘What’s new about the “new public health” ?’ American Journal of Public Health, 94 (5),
pp. 705–709.
Dahlgren, G, Whitehead, M. (1991): Policies and Strategies to Promote Social Equity in Health.
Dahlgren, G. & Whitehead, M. (2006) Levelling up (part 2): European strategies for tackling social inequities in
health. Studies on social and economic determinants of population health, no. 3. (pp. 1–34) Copenhagen,
Denmark: World Health Organization, Regional Office for Europe.
Lindström, B. & Eriksson, M. (2005) ‘Salutogenesis’, Journal of Epidemiology and Community Health, 59 (6),
pp. 440–442.
Naidoo, J. & Wills, J. (2009) Foundations for health promotion. 3rd ed. Edinburgh: Baillière Tindall Elsevier.
Nurse, J. & Edmondson-Jones, P. (2007) ‘A framework for the delivery of public health: an ecological
approach’, Journal of Epidemiology and Community Health, 61 (6), pp. 555 -558.