the society for clinical child and adolescent psychology
TRANSCRIPT
The Society for Clinical Child and Adolescent Psychology (SCCAP):
Initiative for Dissemination of Evidence-based Treatments for Childhood and Adolescent
Mental Health Problems
With additional support from Florida International University and The Children’s Trust.

Keynote Evidence Based Interventions for Pediatric Medical Treatment Adherence
Michael A. Rapoff, Ph.D. Ralph L. Smith Professor of Pediatrics University of Kansas Medical Center

Disclosures
Dr. Rapoff is on the scientific advisory board of Adheris,
a company that works with pharmacy chains to promote
adherence to medications.

“Physicians like to succeed in their
treatment, and an essential ingredient for
that success is a patient’s cooperation”
Groopman, J. (2007). How doctors think (p. 45). Boston: Houghton Mifflin

Learning Objectives
1. Define adherence and types of nonadherence
2. Describe methods for assessing adherence
3. Document the incidence and consequences of
nonadherence to pediatric medical regimens
4. Describe measures of barriers to adherence and their
use in interventions
5. Describe adherence enhancement strategies
6. Review meta-analyses of interventions to improve
adherence to pediatric medical regimens
Adherence Definitions
“The extent to which a person’s behavior (in terms of taking medications, following diets, or executing lifestyle changes) coincides with medical or health advice.”
Haynes et al. (1979). Compliance in health care. Baltimore: The Johns Hopkins University Press.
“The extent to which a person’s behaviour – taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health care provider.”
World Health Organization (2003). Adherence to long-term therapies: Evidence for action. Geneva, Switzerland.

Types of Medication Nonadherence

Types of Medication Nonadherence
• Not filling prescription
• Not (or delays in) refilling prescription
• Omitting doses
• Drug holidays (no doses for several concurrent days)
• “Toothbrush Effect” or “White-coat” Adherence (increased adherence around clinic visits)
• Overdosing or taking extra “make-up” doses

Adherence Measures
• Assays
• Observation
• Automated Devices
• Pill Counts
• Treatment Outcome
• Provider Estimates
• Patient Report
• Rapoff, 2010

Assays
• Assets
– Adjust Drug Levels
– Objective and
Quantifiable
• Liabilities
– Pharmacokinetics may
affect absorption and
excretion rates
– Short-term & Invasive
Observation
• Assets
– Direct measure of non-
medication regimen
adherence
– Can measure
adherence on
repeated occasions
• Liabilities
– Obtrusive and reactive
– Difficult to obtain
representative
samples
Automated Measures
• Assets
– Precise dosing and
dosing interval data
obtained
– Continuous and long-
term measurement
possible
• Liabilities
– Does not measure
consumption
– Mechanical failures

Medication Event Monitoring System
(MEMS)

MEMS
• Records date and time cap removed
• 18-month battery life
• Stores up to 3800 events
• Software to download data
• Cost is ~ $185 per device
• http://www.aardexgroup.com


SmartTrack Compatible Medications:
GSK Advair/Seretide Dose Counter
GSK Flovent Dose Counter
GSK Flixotide No Dose Counter
GSK Serevent
Sepracor Xopenex HFA
Smartinhalers
• Record inhaler installed and removed and canister
actuation, date and time stamped
• 2-3 month between charges
• Reusable
• Have devices for disk and turbo inhalers
• Cost is $195 per device
• Software available to download data
• Nexus6: http://www.smartinhaler.com/
Pill Counts/Canister Weights
• Assets
– Inexpensive &
Feasible
– Superior to patient or
physician estimates
• Liabilities
– Overestimates
adherence
– Does not guarantee
medication taken

Treatment Outcome
• Assets
– Evaluate regimen
efficacy
– Clinically feasible
• Liabilities
– Inexact or unknown
relationship to
adherence
– Factors other than
patient adherence can
affect outcome

Physician Estimates
• Assets
– Clinically feasible
– Generally more
accurate than global
patient estimates
• Liabilities
– Overestimates
adherence
– Physician experience
or familiarity with
patient unrelated to
accuracy
Patient Report
• Assets
– Clinically feasible
– Generally accurate for
nonadherence
• Liabilities
– Overestimates
adherence
– Subject to reporting
bias – “faking good”

Improving Self-Reported Adherence
• Directly evaluate adherence behaviors in an information-
intensive approach (“Which medications are you taking?
What dose? How often? Have you had any side-
effects?”).
• Probe for nonadherence in a non-judgmental and non-
threatening manner (“Many people have trouble
remembering to take their medication. Do you ever
forget to take yours? Do you ever stop taking your
medication on purpose?”)

Improving Self-Reported Adherence
• Time frame for questioning about adherence
should be limited to the previous 7 to 10 days.
• Ask families about barriers to adherence
(personal, financial, social & cultural).
Rand (2000)
RX-Adherence Assessment
“AA” Rating = Automated plus Assay measure
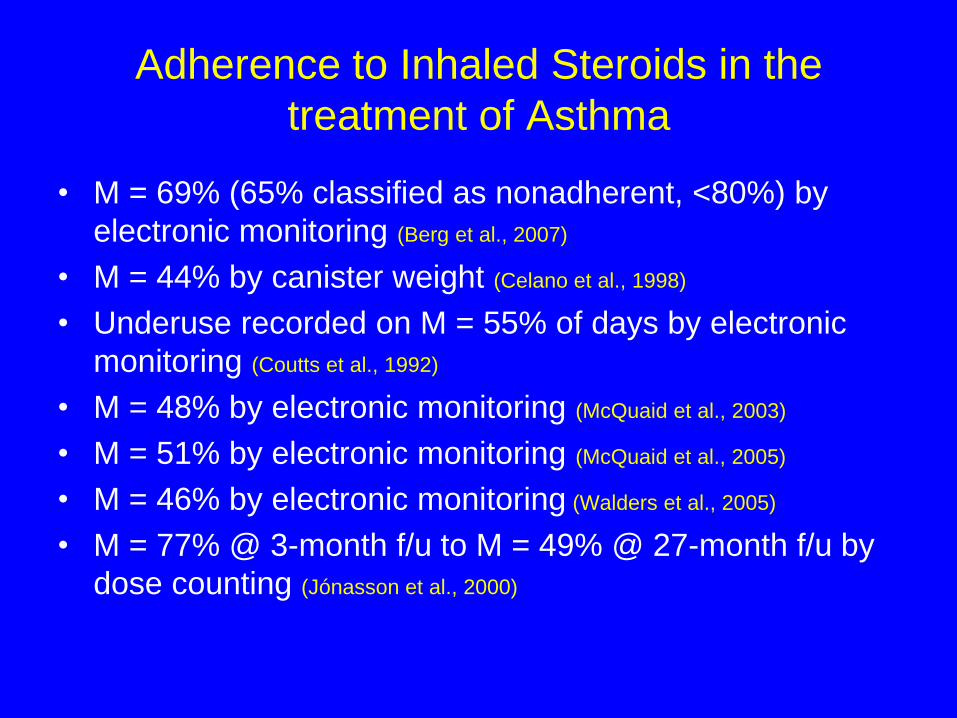
Adherence to Inhaled Steroids in the
treatment of Asthma
• M = 69% (65% classified as nonadherent, <80%) by
electronic monitoring (Berg et al., 2007)
• M = 44% by canister weight (Celano et al., 1998)
• Underuse recorded on M = 55% of days by electronic
monitoring (Coutts et al., 1992)
• M = 48% by electronic monitoring (McQuaid et al., 2003)
• M = 51% by electronic monitoring (McQuaid et al., 2005)
• M = 46% by electronic monitoring (Walders et al., 2005)
• M = 77% @ 3-month f/u to M = 49% @ 27-month f/u by
dose counting (Jónasson et al., 2000)

Adherence to Prednisone in the treatment of
Cancer
• 52% had subtherapeutic levels by serum assay (Festa et
al., 1992)
• 42% had subtherapeutic levels by urine assay (Lansky et
al., 1983)
• 33% had subtherapeutic levels by urine assay (Smith et al.,
1979)
• 19% nonadherent (any missed dose in preceding month)
@ 2-weeks, 40% @ 20-weeks, & 35% @ 50-weeks by
patient and parent report (corroborated by serum assay) (Tebbi et al., 1986)
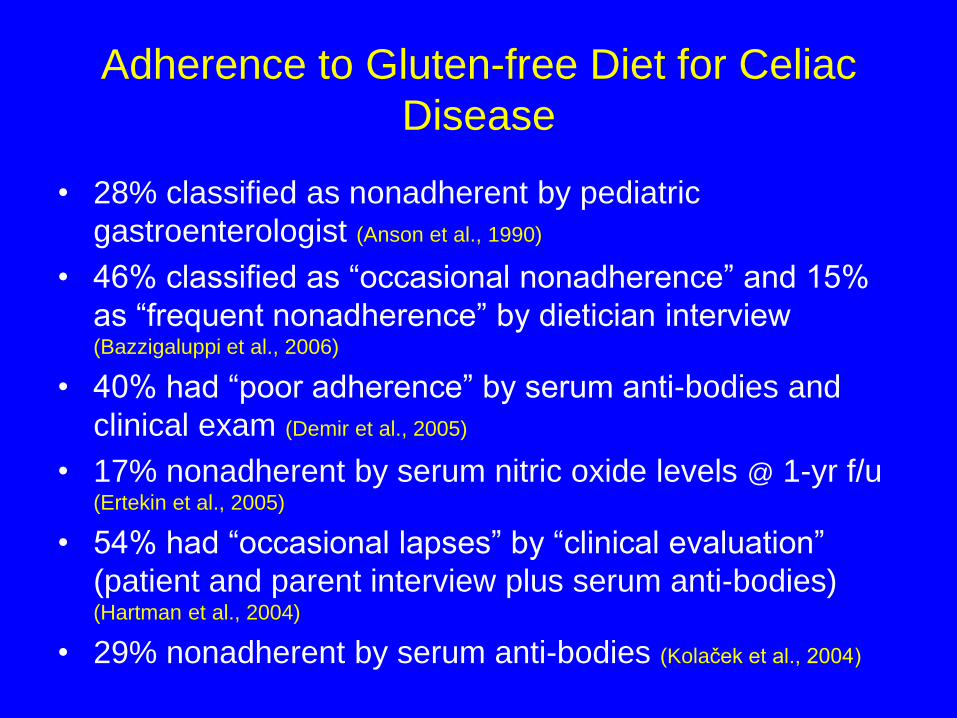
Adherence to Gluten-free Diet for Celiac
Disease
• 28% classified as nonadherent by pediatric
gastroenterologist (Anson et al., 1990)
• 46% classified as “occasional nonadherence” and 15%
as “frequent nonadherence” by dietician interview (Bazzigaluppi et al., 2006)
• 40% had “poor adherence” by serum anti-bodies and
clinical exam (Demir et al., 2005)
• 17% nonadherent by serum nitric oxide levels @ 1-yr f/u (Ertekin et al., 2005)
• 54% had “occasional lapses” by “clinical evaluation”
(patient and parent interview plus serum anti-bodies)
(Hartman et al., 2004)
• 29% nonadherent by serum anti-bodies (Kolaček et al., 2004)

Adherence to Antiretroviral Medications in
the treatment of HIV/AIDS
• 44% of caregiver-youth dyads reported missing doses in
the past week (Dolezal et al., 2003)
• M = 80.9% adherence rate during 1st 3 months & M =
78.5% during last 3 months by electronic monitoring (Martin et al., 2007)
• 40% of caregivers & 56% of patients reported missed
doses in the past month (Mellins et al., 2004)
• 43% of caregivers reported a missed dose in the
previous week (Reddington et al., 2000)
• 30% of caregivers or patients reported missing some or
all doses in the past 3 days (Van Dyke et al., 2002)
• 16% of caregivers or patients reported missing some
doses in the past 3 days (Williams et al., 2006)

Adherence to NSAIDS in the treatment of
JRA
• Baseline M = 86%; 3-mos f/u M = 92%; 6-mos f/u M =
90%; 9-mos f/u M = 92%; 12-mos f/u M = 89% by parent
report over past 3 months (Feldman et al., 2007)
• 3% nonadherent (<60% of doses) by pill counts (Giannini et
al., 1990)
• M = 95% by pill counts (Kvien & Reimers, 1983)
• 45% nonadherent by serum salicylate assay (Litt & Cuskey,
1981)
• 45% nonadherent by serum salicylate assay (Litt et al., 1982)
• Median levels showed partial or no adherence on 21% of
28 days; 48% nonadherent(<80% of doses) by electronic
monitoring (Rapoff et al., 2005)

Adherence to Immunosuppresive
Medications Post-renal Transplantation
• 43% nonadherent by pill counts (Beck et al., 1980)
• 21% nonadherent (<80% doses) by electronic monitoring (Blowey et al., 1997)
• 50% nonadherent by patient report plus serum assay (Ettenger et al., 1991)
• 16% nonadherent by patient report plus serum assay (Feinstein et al., 2005)
• M = 80% by electronic monitoring (Gerson et al., 2004)
• 14% nonadherent (missing medication ≥ 3 times a
month) by patient report (Penkower et al., 2003)
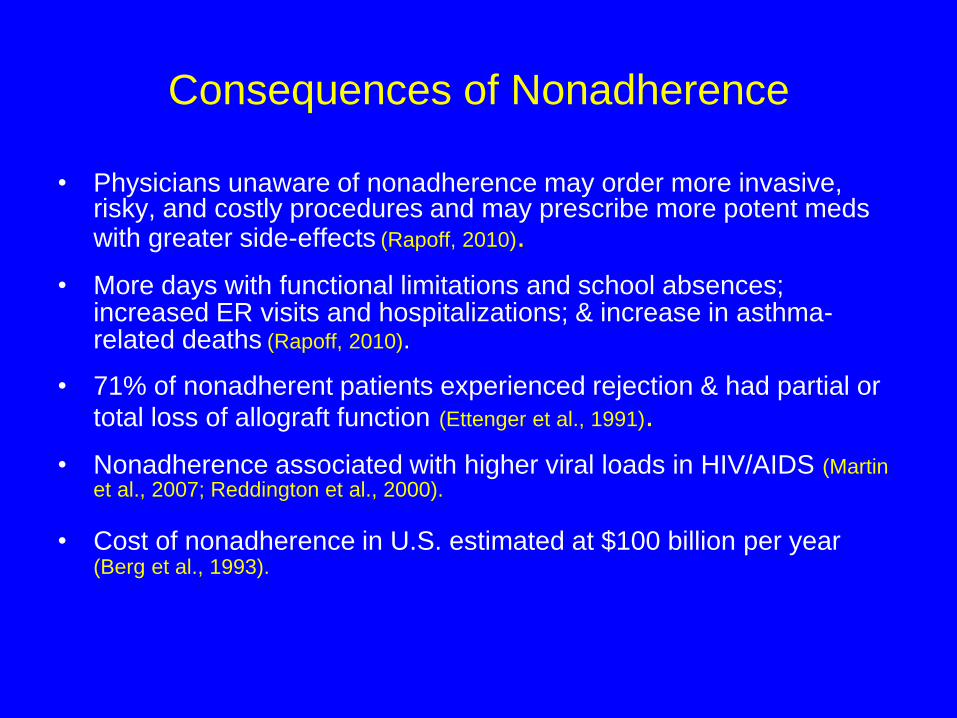
Consequences of Nonadherence
• Physicians unaware of nonadherence may order more invasive, risky, and costly procedures and may prescribe more potent meds with greater side-effects (Rapoff, 2010).
• More days with functional limitations and school absences; increased ER visits and hospitalizations; & increase in asthma-related deaths (Rapoff, 2010).
• 71% of nonadherent patients experienced rejection & had partial or
total loss of allograft function (Ettenger et al., 1991).
• Nonadherence associated with higher viral loads in HIV/AIDS (Martin et al., 2007; Reddington et al., 2000).
• Cost of nonadherence in U.S. estimated at $100 billion per year (Berg et al., 1993).

Barriers to Adherence
• Barriers defined: “the person’s perception of
impediments to adhere to treatments, including a cost-
benefit analysis where the person weighs the pros and
cons of taking action” (Rapoff, 2010).
• Most predictive variable from the Health Belief Model.
• Match unique barriers identified by patients and families
to specific protocols to address each barrier.

Measures of Barriers to Adherence
• Parents Barriers Questionnaire-Juvenile Arthritis
(JA) (Tsai, Matson, Rapoff, & Lindsley)
• Define barriers as “obstacles or things that get in
the way of you helping your child be consistent
in following medical treatments for arthritis.”
• Parents check “yes” for each barrier
experienced in the past week or “no” if it not
experienced.

Parents Barriers Questionnaire –
Juvenile Arthritis (sample items)
• “I just forget when to give my child medications.”
• “It is too hard to give my child medications when
we are not at home.”
• “The pills are too hard for my child to swallow.”
• “My child simply refuses to take the
medications.”
• “I am not sure that my child needs medication.”
• “I did not fill or refill my child’s prescription
because I could not afford them.”

Top Five Barriers identified by parents of
children with JA
• “My child says that the medication tastes bad.”
• “I just forget to give my child the medications.”
• “The pills are too hard for my child to swallow.”
• “I am not always there to remind my child to take
medications.”
• “My child feels physically worse when he/she
takes the pills."

Top Five Barriers identified by parents of
children with a chronic disease (Michele Tsai, in progress)
• Patient or parent forgets
• Patient dislikes medication taste
• Oppositional behavior
• Treatment interferes with daily activities
• Difficulty incorporating treatment regimen into
daily life
Burgess et al., (2008); De Civita et al., (2005); Greenley et al., (2010); Hommel &
Baldassano (2010); Ingerski et al., (2010); Modi & Quittner (2006); Modi et al., (2009);
Modi et al., (2010); Simons & Blount (2007)
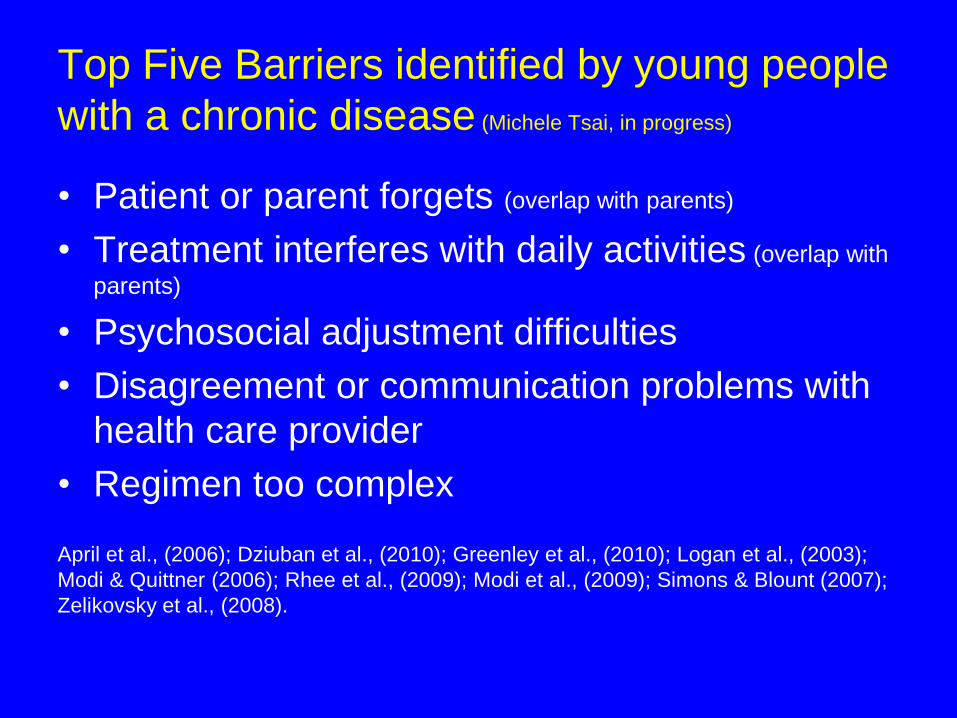
Top Five Barriers identified by young people
with a chronic disease (Michele Tsai, in progress)
• Patient or parent forgets (overlap with parents)
• Treatment interferes with daily activities (overlap with
parents)
• Psychosocial adjustment difficulties
• Disagreement or communication problems with
health care provider
• Regimen too complex
April et al., (2006); Dziuban et al., (2010); Greenley et al., (2010); Logan et al., (2003);
Modi & Quittner (2006); Rhee et al., (2009); Modi et al., (2009); Simons & Blount (2007);
Zelikovsky et al., (2008).

Adherence Enhancement Strategies
• Educational (about disease, treatments, and importance
of adherence)
• Organizational (delivering health care in a way that
facilitates adherence)
• Behavioral (cognitive and behavior change strategies to
enhance adherence)
The What of Education (Content)
• The Disease (causes, course & prognosis)
• Treatments (what to do and why)
• Negative Side Effects (how to minimize)
• Adherence (importance and improvement strategies)
The How of Education (Strategies)
• As an ongoing process
• Effective verbal communication (avoid jargon, stress
instructions, repeat info., encourage questions)
• Written & other media
• Modeling and behavioral rehearsal

Organizational Strategies
• Increase access to health care
• Consumer-friendly clinical settings
• Increase provider supervision
• Simplify regimens
• Minimize negative side effects
Behavioral Strategies
• Increased parental monitoring & supervision
• Prompting adherence
• Adherence incentives
• Discipline strategies
• Contracting
• Self-management strategies (goal setting, self-
monitoring, self-administered consequences, problem-
solving, & cognitive reframing)
• More complex family behavior therapy interventions

Meta-Analyses of Adherence Interventions
• Quantitative syntheses of studies reporting on
interventions to improve adherence to regimens
for chronic pediatric diseases.
• Report effect sizes (ES), the magnitude of
treatment effects as measured by:
d, the difference between the means (M1 – M2) divided by the pooled
standard deviation. Let M1 = experimental group mean and M2 = the
control group mean, so that the difference is positive if it is in the
direction of improved adherence (predicted direction). (Cohen, 1988)
d, for single subject designs uses baseline and treatment mean scores and they are subtracted and divided by the pooled within-phase standard deviations

Effect Size Interpretations
If d = 0.0, the distribution of scores for the experimental
group overlaps completely with the distribution of scores
for the control group. Cohen (1988) classified d as:
“Small”, d = 0.2 (14.7% nonoverlap)
“Medium”, d = 0.5 (33% nonoverlap)
“Large”, d = 0.8 (47.4% nonoverlap)
http://web.uccs.edu/lbecker/Psy590/es.htm (information about effect size and effect-size
calculators-University of Colorado at Colorado Springs)

Effects Size Examples: r = .10 [small]; .30
[medium]; .50 [large]
• Low dose aspirin & ↓ risk of heart attack
= .02 (N = 22,071; 44% reduction in risk)
• Antihypertensives & ↓ risk of stroke
= .03
• Calcium intake & bone mass in premenopausal women
= .08
• Ever smoking and subsequent incidence of lung cancer within 25 yrs.
= .08
• Prominent movie critic reviews & box office success
= .17
• Psychotherapy & well being
= .32
• Viagra & improved male sexual functioning
= .38 Meyer et al., 2001

Meta-Analysis I (Kahana, Drotar, & Frazier,
2008)
• N = 70 adherence-promotion studies identified by literature
search (using multiple search terms, such as intervention,
treatment, adherence, compliance and various chronic
conditions)
• # studies by condition: 32 (45.7%)-asthma; 16 (22.9%)-diabetes;
10 (14.3%)-CF; 2 each with JRA & obesity (2.9%, respectively);
& one each for hemodialysis, hemophilia, HIV, IBD, PKU, seizure
disorders, sickle cell disease, and TB (1.4% each)
• Of the 70 studies, 29 (41.4%) were identified as RCT; 42 (60%)
reported effect size based on an experimental vs. control group
design, while 19 (27.1%) reported effect size based on pre-post
differences and another 9 (12.9%) reported both.

Meta-Analysis I: Demographics
• Mean age ranged from 2 to 15 yrs. (M = 10.2, SD = 3.2)
• Gender prevalence (based on 53 studies): 53.3% males
vs. 47.4% females
• Ethnicity prevalence (based on 26 studies): 82%
Caucasians
• Only 15 studies reported on SES; data could not be
aggregated because they were based on very different
indices of SES
Meta-Analysis I: Intervention Type and
Format
• 34 (48.6%) - multicomponent
• 18 (25.7%) - educational
• 7 (10%) - behavioral
• 7 (10%) - technology based
• 4 (5.7%) - psychosocial
• 63 studies reported format
– 52.4% were groups
– 39.7% were individual based
– the remainder included both group & individual components

Meta-Analysis I: Adherence Measures
• 67 studies reported information on ratings of adherence: – Parents (n = 26; 38.8%)
– Children/Adolescents (n = 17; 25.4%)
– Both parents and youth (n = 11; 16.4%)
– Ratings by psychologists or medical personnel (n = 4; 6%)
– Electronic monitor (n = 2; 3%)
– Blood or urine assay (n = 3; 4.5%)
– Teacher or “outsider” ratings (n = 2; 3%)
– Pharmacy records and parent (n = 1; 1.5%)
– Electronic monitor and child report (n = 1; 1.5%)
Parent or patient reports or combination of the two (n = 54; 81%)
Meta-Analysis I: Results
Weighted (by sample size) mean d across all adherence
outcomes was in the “small” range:
d = .34 (95% confidence interval (CI) = 0.30 – 0.38)
However, there was significant heterogeneity across
adherence outcomes. Therefore, the authors examined
potential moderators of d.
Meta-Analysis I: Moderators of Adherence
Outcome d
Types of Interventions – Behavioral: d = .54 (medium), 95% CI = 0.34-0.73
– Multicomponent: d = .51 (medium), 95% CI = 0.45-0.57
– Psychosocial: d = .44 (small to medium), 95% CI = 0.23-0.65
– Educational: d = .16 (small), 95% CI = 0.10-0.22
– Technology based: d = .08 (NS), 95% CI = 0.09-0.25

Meta-Analysis I: Moderators of Adherence
Outcome d
• Type of Adherence Outcome: self-management, self-care behaviors,
dietary change, and exercise-environmental changes yielded
medium ds, while medication adherence yielded small ds
• Type of Disorder: CF (medium to large), miscellaneous disorders
(medium), diabetes (small to medium), & asthma (small)
• Type of Design: combined pre-post & experimental vs. control group
(medium to large), pre-post only (small to medium), & experimental
vs. control only (small)
• Follow-up: d diminished over time (0-6 mos. f/u, d = .63, 95% CI =
0.46-0.80; 7-12 mos. f/u, d = .24, 95% CI = 0.06-0.42; >12 mos. f/u,
d = .50, 95% CI = -1.15-0.15)

Meta-Analysis II (Graves et al., 2010)
• N = 71 studies identified from literature search with terms
adherence or compliance and paired with treatment,
strategies, improve, interventions, education, medication,
child, adolescent, and pediatric.
• Did not include obesity or lifestyle changes, just chronic
illnesses.
• 34 (48.6%) used a comparison group design
(experimental vs. control), 17 (24.3%) used a within
subject design (pre-post), and 19 (28.2%) used a single-
subject design.

Meta-Analysis II: Chronic Diseases
• Of group designs (N 51) with N =3027 patients (M=35.6):
• 16 (31.4%) asthma
• 15 (29.4%) type 1 diabetes
• 5 (9.8%) CF
• 3 each (5.9%) with HIV/AIDS or post-transplant
• 2 each (3.9%) with hyperlipidemia, JIA, & sickle cell
• 1 each (2%) with epilepsy, hemophilia, & PKU

Meta-Analysis II: Chronic Diseases
• Single subject design studies (N=20), with N=50
patients (M=2.6)
• 7 (36.8%) type 1 diabetes
• 3 (15.8%) each JIA & CF
• 2 (10.5%) asthma
• 1 (5.3%) each epilepsy, lung disease, rheumatic
diseases, & sickle cell
Meta-Analysis II: Adherence Measures
• Group design studies: – Child report (N=14)
– Parent report (N=9
– Diary (N=9)
– 24-h recall (N=8)
– Electronic monitoring (N=10)
– Pill count (N=7)
– Blood or urine assay (N=6)
• Single subject design studies:
– Diary (N=23, 71.9%)
– Electronic monitoring (N=4, 12.5%)
– Pill Count (N=3, 9.4%)
– 24-hr recall (N=2, 6.3%)

Meta-Analysis II: Demographics
• Group design studies:
– Age 2 to 15 yrs. (M = 9.9)
– % males = 24% to 91% (M = 51.7%)
– Minorities = 0% to 100% (M = 39.1%)
• Single subject design studies:
– Age 2 to 17 yrs. (M = 11)
– % males = 0% to 100% (M = 47.1%)
– Minorities = 0% in 2 studies & 100% in 2 studies

Meta-Analysis II: Intervention Types
• For Group Design Studies:
– Combined educational and behavioral (n=24, 47%)
– Organizational (n=6, 11.8%)
– Behavioral (n=5, 9.8%)
– Educational (n=2, 3.9%)
– Variety of combinations (n=13, 25.4%)
• For Single Subject Design Studies:
– Educational and behavioral (n=9, 47.4%)
– Behavioral (n=9, 47.4%)
– Behavioral and organizational (n=1, 5.3%)

Meta-Analysis II: Adherence Outcomes
• Mean effect size (weighted by sample size) for group
designs: d = 0.58 (“medium” range), 95% CI = 0.51-0.65
• Moderators of effect size: Higher effect size for studies
using a wait-list control design (mean d = 1.09) vs. an
alternative treatment design (mean d = 0.43)
• Mean effect size (weighted by sample size) for single-
subject designs: d = 1.53 (“large” range), 95% CI – 1.07-
1.98). No moderators of effect size as homogeneous.
Meta-Analysis II: Health Outcomes
• 31 studies reported health outcomes: direct (e.g., A1C)
indirect (disease activity), healthcare utilization, or
subjective (quality of life = QOL).
• Mean d = .40 (small to medium),
95% CI = 0.31 – 0.50
• d higher for A1C, PFT, disease activity, & healthcare
utilization vs. BMI & QOL

Research Implications from Meta-Analyses
1. Less reliance on indirect measures of adherence
(parent & patient reports)
2. Need for larger, RCTs with attention-placebo and long-
term follow-up
3. Include health outcomes (direct, indirect, health care
utilization & costs, and QOL)
4. Explore moderators of effect sizes
5. Dismantling studies of multicomponent interventions
6. Recruit more ethnically diverse samples
7. Assess treatment fidelity and integrity (i.e., did
patients/families receive intervention as intended &
use the skills/knowledge imparted?)
8. Develop & test technology-based interventions
Clinical Implications for Enhancing
Adherence
1. Educate and re-educate about disease, purpose of
regimen, and need for consistent adherence
2. Secure patient/family agreement to follow regimen
3. Parent involvement key component (monitoring,
supervising, & positive reinforcement)
4. Provide incentives to patients
5. Self-management skills for adolescents
6. One-shot bolus of an adherence intervention will not
have lasting effects: interventions need to be part of
ongoing clinical management of pediatric chronic
diseases

When Is Nonadherence Medical Neglect?
• N = 6 patients perinatally HIV-infected children whose
therapy was failing based on HIV RNA levels
• 3-Step approach taken:
1. Home health care nurse visits 2 times per week for at least 2 wks
2. Directly observed therapy (DOT) while patient was hospitalized
for 4 days
3. Physician-initiated medical neglect report to the Arkansas
Department of Human Services
• Results: for 2 of 6 patients, a medical neglect report was
necessary and resulted in foster care placement with
improvements in viral load
Roberts et al. (2004)

For more information, please go to the main website and browse for workshops
on this topic or check out our additional resources.
Additional Resources
Online resources: 1. Society of Clinical Child & Adolescent Psychology: https://clinicalchildpsychology.org 2. Society of Pediatric Psychology Adherence to Pediatric Medical Regimens Fact Sheet: http://www.apadivisions.org/division-54/evidence-based/medical-regimens.aspx
Books: 1. Rapoff, M.A. (2010). Adherence to pediatric medical regimens, (2nd ed.). New York: Springer.
Peer-reviewed Journal Articles: 1. Berg, J. S., Dischler, J., Wagner, D. J., Raia, J., & Palmer-Shevlin, N. (1993). Medication compliance: A health care problem. The Annals of Pharmacotherapy, 27 (suppl.), 2-21. 2. Berg, C.J., Rapoff, M.A., Snyder, C.R., & Belmont, J.M. (2007). The relationship of children’s hope to pediatric asthma treatment adherence. The Journal of Positive Psychology, 2, 176-184. 3. Burgess, S. W., Sly, P. D., Morawska, A., & Devadason, S. G. (2008). Assessing adherence and factors associated with adherence in young children with asthma. Respirology, 13, 559-563. 4. McQuaid, E.L., Walders, N., Kopel, S.J., Fritz, G.K., & Klinnert, M.D. (2005). Pediatric asthma management in the family context: The family asthma management system scale. Journal of Pediatric Psychology, 30, 492-502. 5. Modi, A. C., & Quittner, A. L. (2006). Barriers to treatment adherence for children with cystic fibrosis and asthma: What gets in the way? Journal of Pediatric Psychology, 31(8), 846-858 6. Rapoff, M.A., Belmont, J.M., Lindsley, C.B., & Olson, N.Y. (2005). Electronically monitored adherence to medications by newly diagnosed patients with juvenile rheumatoid arthritis. Arthritis Care & Research, 53, 905-910. 7. World Health Organization (2003). Adherence to long-term therapies: Evidence for action. Geneva, Switzerland.

Full Reference List
Keynote: Evidence Based Interventions for Pediatric Medical Treatment Adherence by Michael Rapoff, Ph.D.
Websites: 1. Society of Clinical Child and Adolescent Psychology website: http://effectivechildtherapy.com 2. Society of Pediatric Psychology Adherence to Pediatric Medical Regimens Fact Sheet: http://www.apadivisions.org/division-54/evidence-based/medical-regimens.aspx Books: Groopman, J. (2007). How doctors think. New York: Houghton Mifflin. Haynes, R. B. (1979). Introduction. In D. W. Taylor & D. C. Sackett (Eds.), Compliance in health care (pp.
1-7). Baltimore: The Johns Hopkins University Press. Rand, C.S. (2000). “I took the medicine like you told me, doctor”: Self-report of adherence with medical
regimens. In A.A. Stone, J.S. Turkkan, C.A. Bachrach, J.B. Jobe, H.S. Kurtzman & Cain, V.S. (Eds.), The science of self-report: Implications for research and practice (pp. 257-276). Mahwah, NJ: Lawrence Erlbaum.
Rapoff, M.A. (2010). Adherence to pediatric medical regimens, (2nd ed.). New York: Springer. Peer Reviewed Journal Articles: Anson, O., Weizman, Z., & Zeevi, N. (1990). Celiac disease: Parental knowledge and attitudes of dietary
compliance. Pediatrics, 85, 98-103. April, K. T., Feldman, D. E., Platt, R. W., & Duffy, C. M. (2006). Comparison between children with
juvenile idiopathic arthritis and their parents concerning perceived treatment adherence. Arthritis and Rheumatism, 55(4), 558-563. doi: 10.1002/art.22104
Bazzigaluppi, E., Roggero, P., Parma, B., Brambillasca, M.F., Meroni, F., Mora, S., Bosi, E. & Barera, G. (2006). Antibodies to recombinant human tissue-transglutaminase in celiac disease: Diagnostic effectiveness and decline pattern after gluten-free diet. Digestive and Liver Disease, 38, 98-102.
Beck, D. E., Fennell, R. S., Yost, R. L., Robinson, J. D., Geary, D., & Richards, G. A. (1980). Evaluation of an educational program on compliance with medication regimens in pediatric patients with renal transplants. The Journal of Pediatrics, 96, 1094-1097.
Berg, J. S., Dischler, J., Wagner, D. J., Raia, J., & Palmer-Shevlin, N. (1993). Medication compliance: A health care problem. The Annals of Pharmacotherapy, 27 (suppl.), 2-21.
Berg, C.J., Rapoff, M.A., Snyder, C.R., & Belmont, J.M. (2007). The relationship of children’s hope to pediatric asthma treatment adherence. The Journal of Positive Psychology, 2, 176-184.
Blowey, D. L., Hebert, D., Arbus, G. S., Pool, R., Korus, M., & Koren, G. (1997). Compliance with cyclosporine in adolescent renal transplant receipients. Pediatric Nephrology, 11, 547-551.
Burgess, S. W., Sly, P. D., Morawska, A., & Devadason, S. G. (2008). Assessing adherence and factors associated with adherence in young children with asthma. Respirology, 13, 559-563.
Celano, M., Geller, R.J., Phillips, K.M., & Ziman, R. (1998). Treatment adherence among low-income children with asthma. Journal of Pediatric Psychology, 23, 345-349.
Coutts, J. A. P., Gibson, N. A., & Paton, J. Y. (1992). Measuring compliance with inhaled medication in asthma. Archives of Diseases of Children, 67, 332-333.
De Civita, M., Dobkin, P. L., Ehrmann-Feldman, D., Karp, I. & Duffy, C. M. (2005). Development and preliminary reproducibility and validity of the parent adherence report questionnaire: A measure of adherence in juvenile idiopathic arthritis. Journal of Clinical Psychology in Medical Settings, 12(1), 1-12.
Full Reference List
Demir, H., Yüce, A., Caglar, M., Kale, G., Kocak, N., Özen, H., Gürakan, F., & Saltik-Temizel, I.N. (2005).
Cirrhosis in children with celiac disease. Journal of Clinical Gastroenterology, 39, 630-633. Dolezal, C., Mellins, C., Brackis-Cott, E., & Abrams, E.J. (2003). The reliability of reports of medical
adherence from children with HIV and their adult caregivers. Journal of Pediatric Psychology, 28, 355-361.
Dziuban, E. J., Saab-Abazeed, L., Chaudhry, S. R., Streetman, D. S., & Nasr, S. Z. (2010). Identifying barriers to treatment adherence and related attitudinal patterns in adolescents with cystic fibrosis. Pediatric Pulmonology, 45, 450-458.
Ertekin, V., Selimoğlu, A., Türkan, Y., & Akçay, F. (2005). Serum nitric oxide levels in children with celiac disease. Journal of Clinical Gastroenterology, 39, 782-785.
Ettenger, R. B., Rosenthal, J. T., Marik, J. L., Malekzadeh, M., Forsythe, S. B., Kamil, E. S., Salusky, I. B., & Fine, R. N. (1991). Improved cadaveric renal transplant outcome in children. Pediatric Nephrology, 5, 137-142.
Feinstein, S., Keich, R., Becker-Cohen, R., Rinat, C., Schwartz, S.B., & Frishberg, Y. (2005). Is noncompliance among adolescent renal transplant recipients inevitable? Pediatrics, 115, 969-973.
Feldman, D.E., De Civita, M., Dobkin, P.L., Malleson, P., Meshefedjian, G., & Duffy, C. (2007). Perceived adherence to prescribed treatment in juvenile idiopathic arthritis over a one-year period. Arthritis Care & Research, 57, 226-233.
Festa, R. S., Tamaroff, M. H., Chasalow, F., & Lanzkowsky, P. (1992). Therapeutic adherence to oral medication regimens by adolescents with cancer. I. Laboratory assessment. Journal of Pediatrics, 120, 807-811.
Gerson, A.C., Furth, S.L., Neu, A.M., & Fivush, B.A. (2004). Assessing associations between medication adherence and potentially modifiable psychosocial variables in pediatric kidney transplant recipients and their families. Pediatric Transplantation, 8, 543-550.
Giannini, E.H. Brewer, E.J., Miller, M.L., Gibbas, D., Passo, M.H., Hoyeraal, H.M., Bernstein, B., Person, D.A., Fink, C.W., Sawyer, L.A. & Scheinbaum, M.L. (1990). Ibuprofen suspension in the treatment of juvenile rheumatoid arthritis. Journal of Pediatrics, 117, 645-652.
Graves, M.M., Roberts, M.C., Rapoff, M.A., & Boyer, A. (2010). The efficacy of adherence interventions for chronically ill children: A meta-analytic review. Journal of Pediatric Psychology, 35, 368-382.
Greenley, R. N., Stephens, M., Doughty, A., Raboin, T., & Kugathasan, S. (2010). Barriers to adherence among adolescents with inflammatory bowel disease. Inflammatory Bowel Diseases, 16(1), 36-41.
Hartman, C., Hino, B., Lerner, A., Eshach-Adiv, O., Berkowitz, D., Shaoul, R., Pacht, A., Rozenthal, E., Tamir, A., Shamaly, H., & Shamir, R. (2004). Bone quantitative ultrasound and bone mineral density in children with celiac disease. Journal of Pediatric Gastroenterology and Nutrition, 39, 504-510.
Hommel, K. A., & Baldassano, R. N. (2010). Brief report: Barriers to treatment adherence in pediatric inflammatory bowel disease. Journal of Pediatric Psychology, 35(9), 1005-1010.
Ingerski, L. M., Baldassano, R. N., Denson, L. A., & Hommel, K. A. (2010). Barriers to oral medication adherence for adolescents with inflammatory bowel disease. Journal of Pediatric Psychology, 35(6), 683-691.
Jónasson, G., Carlsen, K-H, & Mowinckel, P. (2000). Asthma drug adherence in a long term clinical trial. Archives of Disease in Childhood, 83, 330-333.
Kahana, S., Drotar, D., & Frazier, T. (2008). Meta-analysis of psychological interventions to promote adherence to treatment in pediatric chronic health conditions. Journal of Pediatric Psychology, 33, 590-611.
Full Reference List
Kolaček, S., Jadrešin, O., Petković, I., Mišak, Z., Sonicki, Z., & Booth, I.W. (2004). Gluten-free diet has a
beneficial effect on chromosome instability in lymphocytes of children with celiac disease. Journal of Pediatric Gastroenterology and Nutrition, 38, 177-180.
Kvien, T.K. & Reimers, S. (1983). Drug handling and patient compliance in an outpatient paediatric trial. Journal of Clinical & Hospital Pharmacy, 8, 251-257.
Lansky, S. B., Smith, S. D., Cairns, N. U., & Cairns, G. F. (1983). Psychological correlates of compliance. The American Journal of Pediatric Hematology/Oncology, 5, 87-92.
Litt, I. F., & Cuskey, W. R. (1981). Compliance with salicylate therapy in adolescents with juvenile rheumatoid arthritis. American Journal of Diseases of Children, 135, 434-436.
Litt, I. F., Cuskey, W. R., & Rosenberg, A. (1982). Role of self-esteem and autonomy in determining medication compliance among adolescents with juvenile rheumatoid arthritis. Pediatrics, 69, 15-17.
Logan, D., Zelikovsky, N., Labay, L., & Spergel, J. (2003). The illness management survey: Identifying adolescents’ perceptions of barriers to adherence. Journal of Pediatric Psychology, 28(6), 383-392.
Martin, S., Elliot-DeSorbo, D.K., Wolters, P.L., Toledo-Tamula, M.A., Roby, G., Zeichner, S., & Wood, L.V. (2007). Patient, caregiver and regimen characteristics associated with adherence to highly active antiretroviral therapy among HIV-infected children and adolescents. Pediatric Infectious Disease Journal, 26, 61-67.
McQuaid, E.L., Kopel, S.J., Klein, R.B. & Fritz, G.K. (2003). Medication adherence in pediatric asthma: Reasoning, responsibility, and behavior. Journal of Pediatric Psychology, 28, 323-333.
McQuaid, E.L., Walders, N., Kopel, S.J., Fritz, G.K., & Klinnert, M.D. (2005). Pediatric asthma management in the family context: The family asthma management system scale. Journal of Pediatric Psychology, 30, 492-502.
Mellins, C.A., Brackis-Cott, E., Dolezal, C., & Abrams, E.J. (2004). The role of psychosocial and family factors in adherence to antiretroviral treatment in human immunodeficiency virus-infected children. Pediatric Infectious Disease Journal, 23, 1035-1041.
Meyer, G.J., Finn, S.E., Eyde, L.D., Kay, G.G., Moreland, K.L., Dies, R.R., Eisman, E.J., Kubiszyn, T.W., & Reed, G.M. (2001). Psychological testing and psychological assessment. American Psychologist, 56, 128-165.
Modi, A. C., Crosby, L. E., Guilfoyle, S. M., Lemanek, K. L., Witherspoon, D., & Mitchell, M. J. (2009). Barriers to treatment adherence for pediatric patients with sickle cell disease and their families. Children’s Health Care, 38, 107-122.
Modi, A. C., Monahan, S., Daniels, D., & Glauser, T. A. (2010). Development and validation of the Pediatric Epilepsy Medication Self-Management Questionnaire. Epilepsy and Behavior, 18, 94-99.
Modi, A. C., & Quittner, A. L. (2006). Barriers to treatment adherence for children with cystic fibrosis and asthma: What gets in the way? Journal of Pediatric Psychology, 31(8), 846-858.
Penkower, L., Dew, M.A., Ellis, D., Sereika, S.M., Kitutu, J.M.M., & Shapiro, R. (2003). Psychological distress and adherence to the medical regimen among adolescent renal transplant recipients. American Journal of Transplantation, 3, 1418-1425.
Rapoff, M.A., Belmont, J.M., Lindsley, C.B., & Olson, N.Y. (2005). Electronically monitored adherence to medications by newly diagnosed patients with juvenile rheumatoid arthritis. Arthritis Care & Research, 53, 905-910.
Reddington, C. Cohen, J., Baldillo, A., Toye, M., Smith, D., Kneut, C. Demaria, A., Bertolli, J., & Hsu, H. (2000). Adherence to medication regimens among children with human immunodeficiency virus infection. Pediatric Infectious Disease Journal, 19, 1148-1153.

Full Reference List
Rhee, H., Belyea, M. J., Ciurzynski, S., & Brasch, J. (2009). Barriers to asthma self-management in
adolescents: Relationships to psychosocial factors. Pediatric Pulmonology, 44, 183-191. Roberts, G.M., Wheeler, J.G., Tucker, N.C., Hackler, C., Young, K., Maples, H.D., & Darville, T. (2004).
Nonadherence with pediatric human immunodeficiency virus therapy as medical neglect. Pediatrics, 114, 346-353.
Simons, L. E., & Blount, R. L. (2007). Identifying barriers to medication adherence in adolescent transplant recipients. Journal of Pediatric Psychology, 32(7), 831-844.
Smith, S. D., Rosen, D., Trueworthy, R. C., & Lowman, J. T. (1979). A reliable method for evaluating drug compliance in children with cancer. Cancer, 43, 169-173.
Tebbi, C. K., Cumings, K. M., Kevon, M. A., Smith, L., Richards, M., & Mallon, J. (1986). Compliance of pediatric and adolescent cancer patients. Cancer, 58, 1179-1184.
Van Dyke, R.B., Lee, S., Johnson, G.M., Wiznia, A., Mohan, K., Stanley, K., Morse, E.V., Krogstad, P.A., & Nachman, S. (2002). Reported adherence as a determinant of response to highly active antiretroviral therapy in children who have human immunodeficiency virus infection. Pediatrics, 109, 1-7.
Walders, N., Kopel, S.J., Koins-Mitchell, D., & McQuaid, E.L. (2005). Patterns of quick-relief and long-term controller medication use in pediatric asthma. Journal of Pediatrics, 146, 177-182.
Williams, P.L., Storm, D., Montepiedra, G., Nichols, S., Kammerer, B., Sirois, P.A., Farley, J., & Malee, K. (2006). Predictors of adherence to antiretroviral medications in children and adolescents with HIV infection. Pediatrics, 118, 1745-1757.
Zelikovsky, N., Schast, A. P., Palmer, J. A., & Meyers, K. E. C. (2008). Perceived barriers to adherence among adolescent renal transplant candidates. Pediatric Transplantation, 12, 300-308.
Other Resources World Health Organization (2003). Adherence to long-term therapies: Evidence for action. Geneva,
Switzerland. Retrieved from http://www.EffectiveChildTherapy.fiu.edu