the spinal cord
DESCRIPTION
The spinal cord, its tracts and contentsTRANSCRIPT

THE SPINAL CORD
12-2
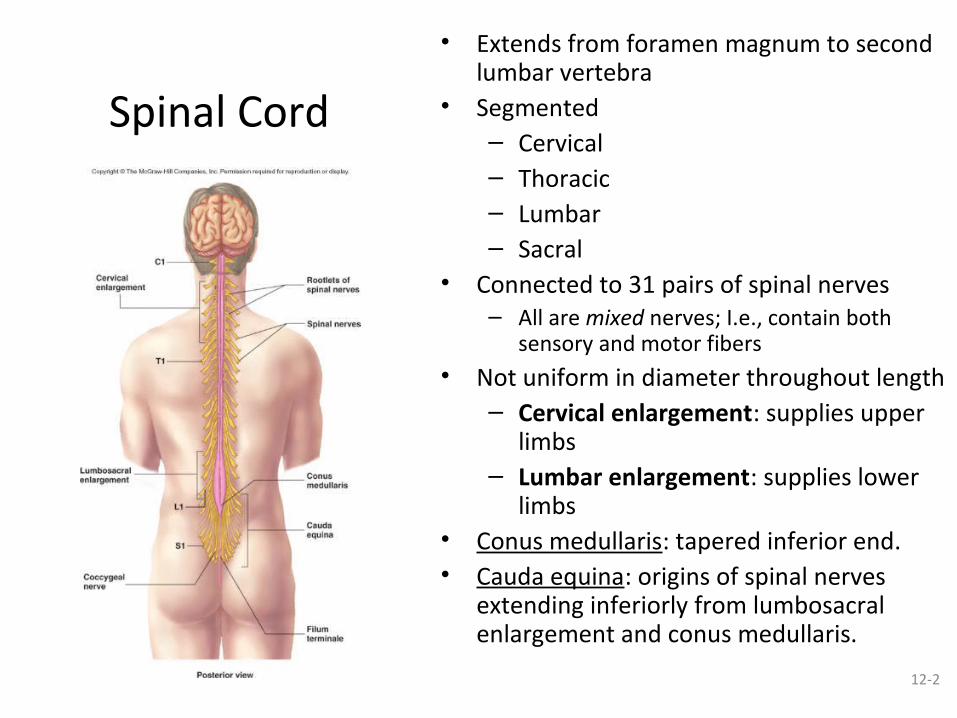
Spinal Cord
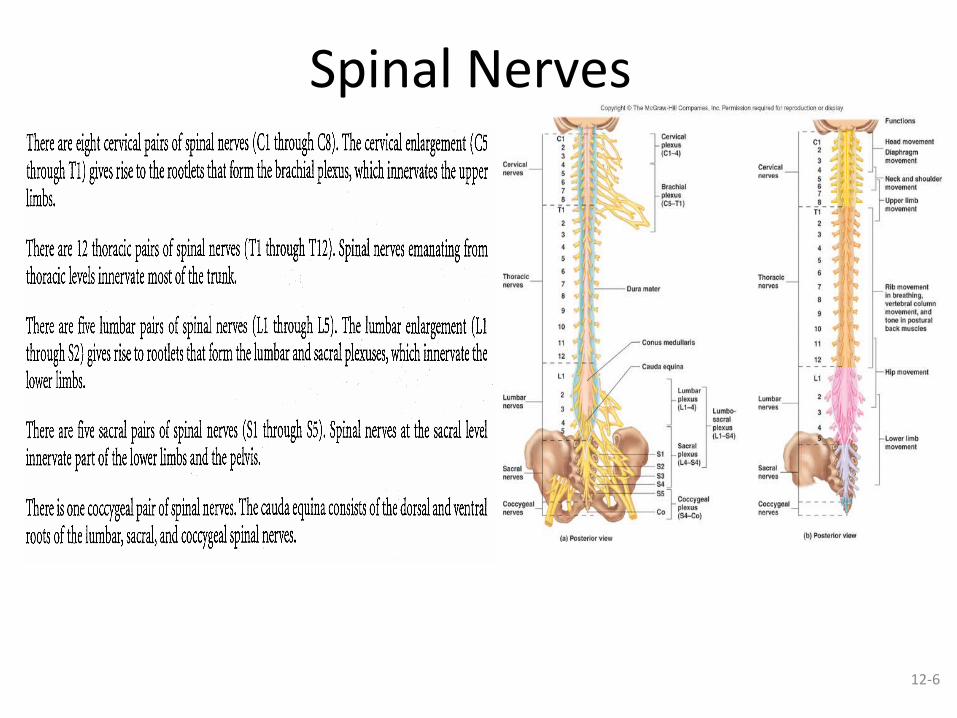
• Extends from foramen magnum to second lumbar vertebra
• Segmented– Cervical – Thoracic– Lumbar– Sacral
• Connected to 31 pairs of spinal nerves– All are mixed nerves; I.e., contain both
sensory and motor fibers• Not uniform in diameter throughout length
– Cervical enlargement: supplies upper limbs
– Lumbar enlargement: supplies lower limbs
• Conus medullaris: tapered inferior end. • Cauda equina: origins of spinal nerves
extending inferiorly from lumbosacral enlargement and conus medullaris.

12-3
Spinal Meninges – Dura mater: outermost layer; continuous
with epineurium of the spinal nerves• No firm connections to vertebrae• Epidural space: external to the dura;
anesthesia injected here in sc. Contains blood vessels, areolar connective tissue and fat.
– Arachnoid mater: delicate net-work of collagen and elastic fibers• Subarachnoid space: between pia and
arachnoid• CSF and blood vessels within web-like
strands of arachnoid tissue• Fluid functions as a shock absorber
– Pia mater: thin layer of elastic and collagen fibers bound tightly to surface of brain and spinal cord• Denticulate ligaments extend from pia
through arachnoid to dura; prevent lateral movement
• Forms the filum terminale, which anchors spinal cord to coccyx and the denticulate ligaments that attach the spinal cord to the dura mater
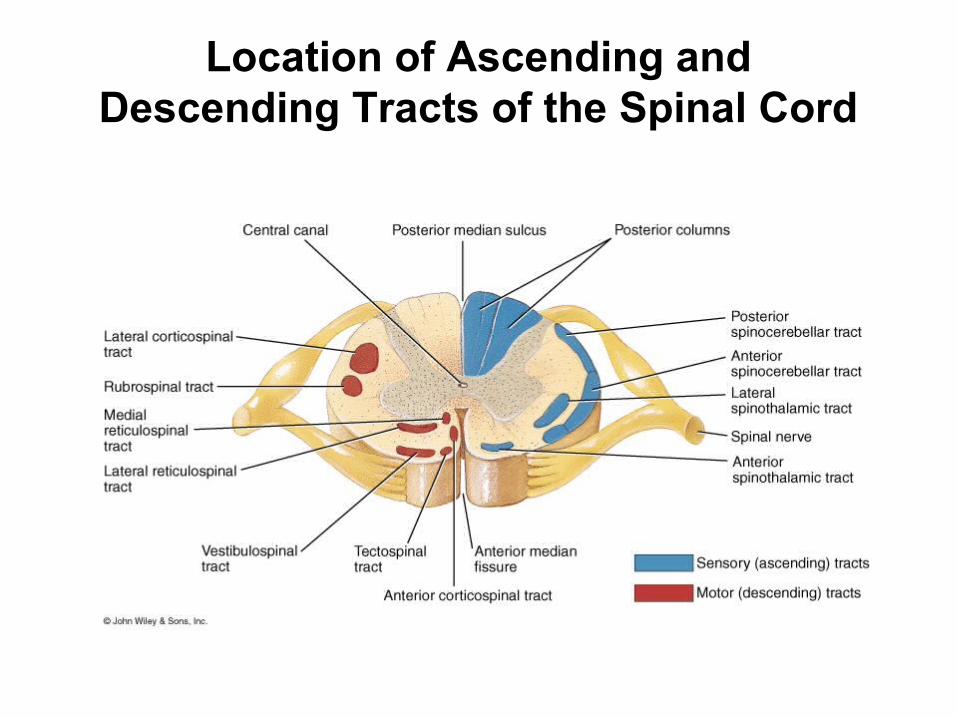
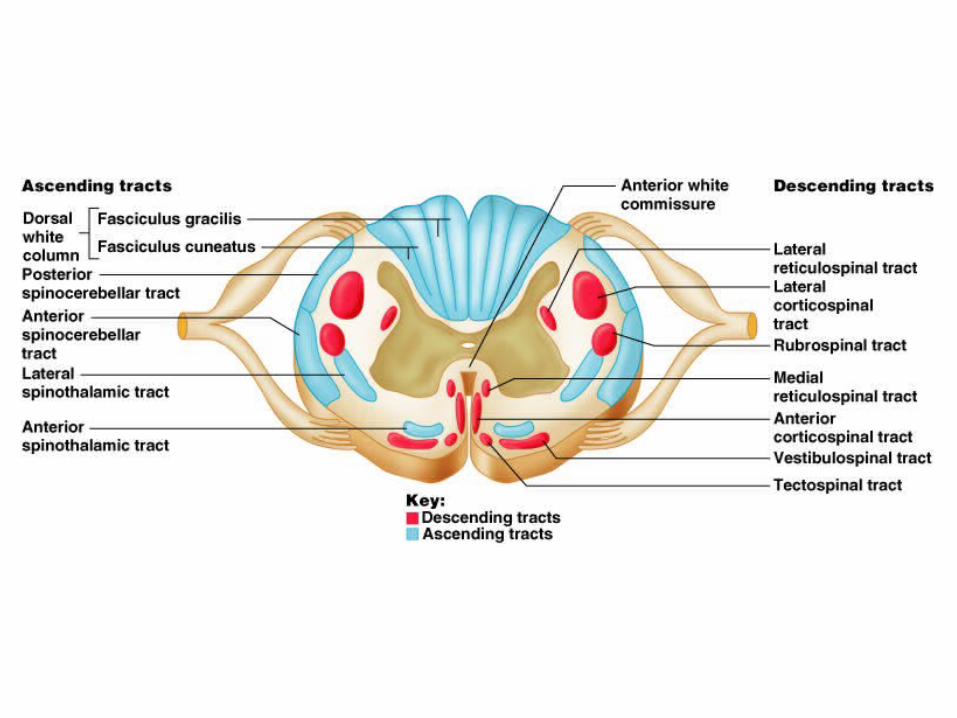
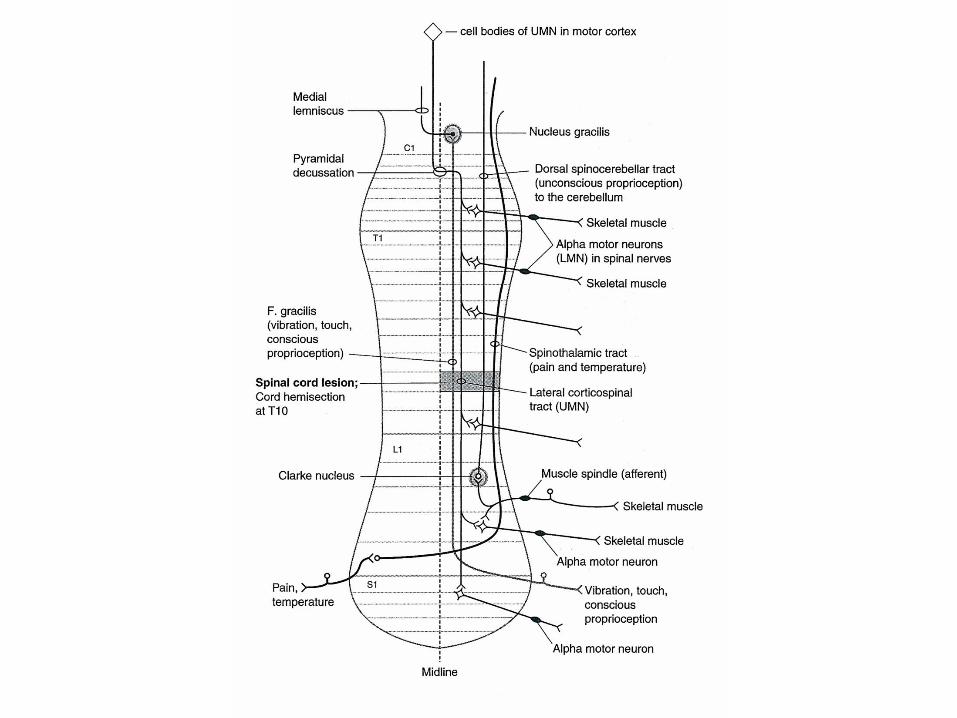
Location of Ascending and Descending Tracts of the Spinal Cord
12-6
Spinal Nerves

12-7
Ascending Tracts
• Carry sensory signals up to the spinal cord
• Typically uses 3 neurons– 1st order neuron - detects
stimulus and carries it to spinal cord
– 2nd order neuron - within s.c.; continues to the thalamus (the sensory relay station)
– 3rd order neuron - carries signal from thalamus to sensory region of cerebral cortex
• Most have names with prefix spino-

Major Sensory or Ascending Tracts Name Location Function
Fasciculus gracilis
Posterior Column
Discriminative touch, proprioceptionWeight discrimination
Fasciculus Cuneatus
PosteriorColumn
Same as FG
Lateral Spinothalamic
LateralColumn
Pain and Thermal sensations
Anterior Spinothalamic
AnteriorColumn
Itch, Tickle, Pressure, Crude touch sensations
Posterior and Anterior Spinocerebellar
LateralColumn
Proprioceptors
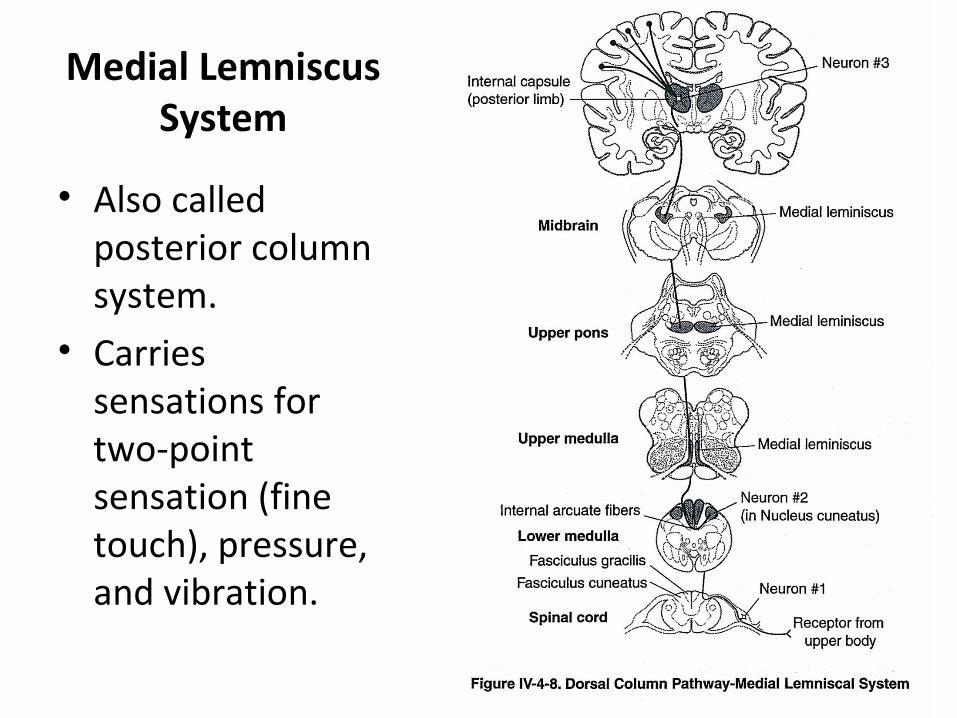
Medial Lemniscus System
• Also called posterior column system.
• Carries sensations for two-point sensation (fine touch), pressure, and vibration.
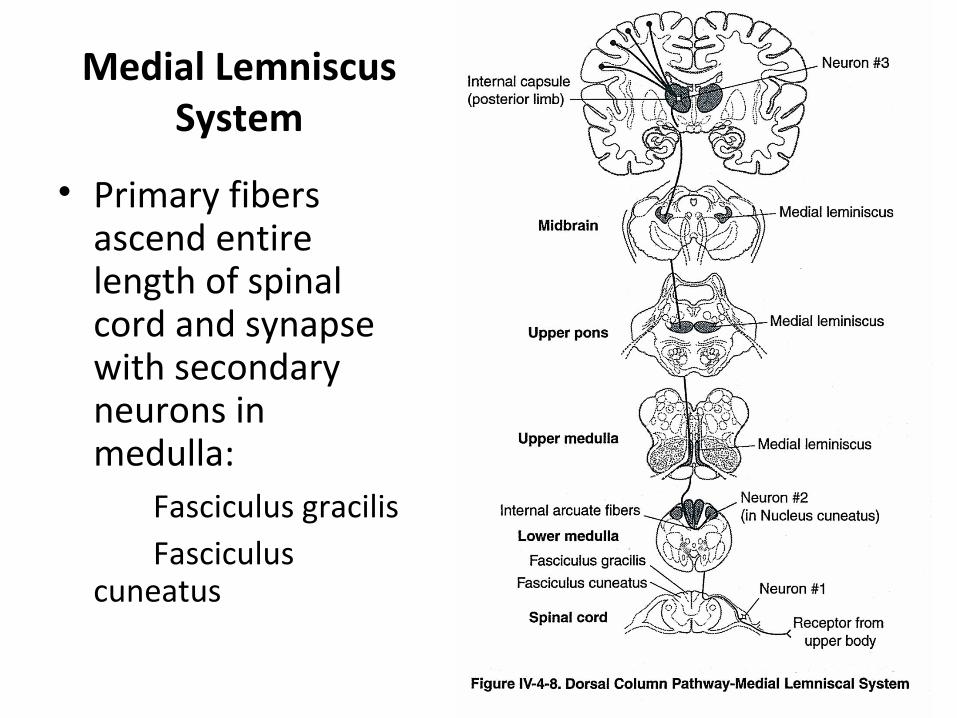
Medial Lemniscus System
• Primary fibers ascend entire length of spinal cord and synapse with secondary neurons in medulla:
Fasciculus gracilisFasciculus
cuneatus
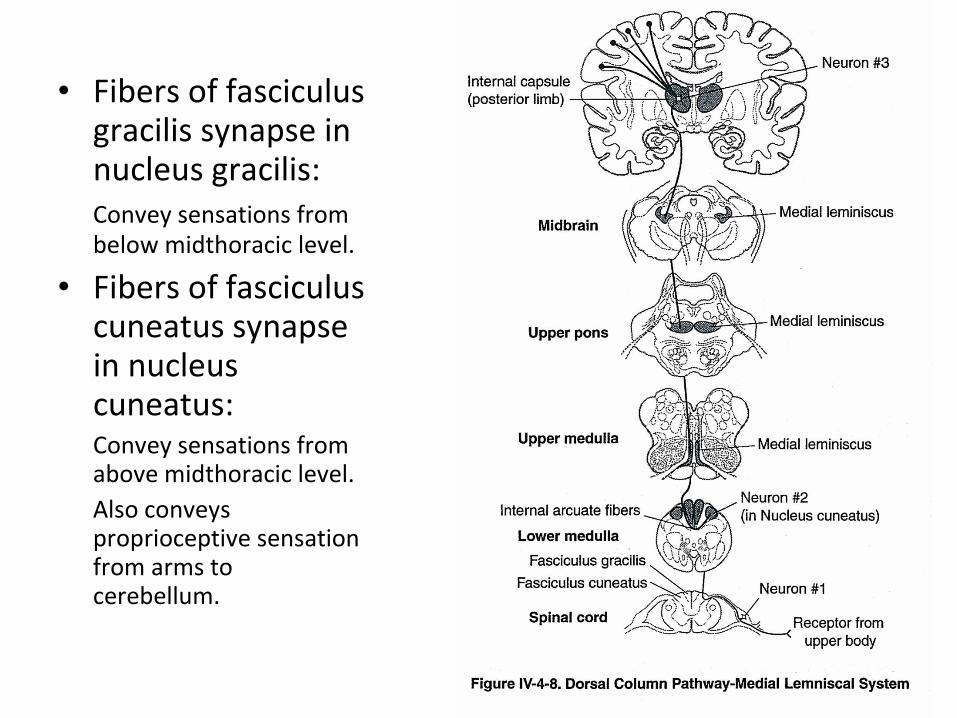
• Fibers of fasciculus gracilis synapse in nucleus gracilis:Convey sensations from below midthoracic level.
• Fibers of fasciculus cuneatus synapse in nucleus cuneatus:Convey sensations from above midthoracic level.Also conveys proprioceptive sensation from arms to cerebellum.

Medial Lemniscus System
• Secondary fibers decussate.
• Secondary fibers ascend to synapse in VPL of thalamus.
• Tertiary fibers ascend through internal capsule to primary sensory cortex.

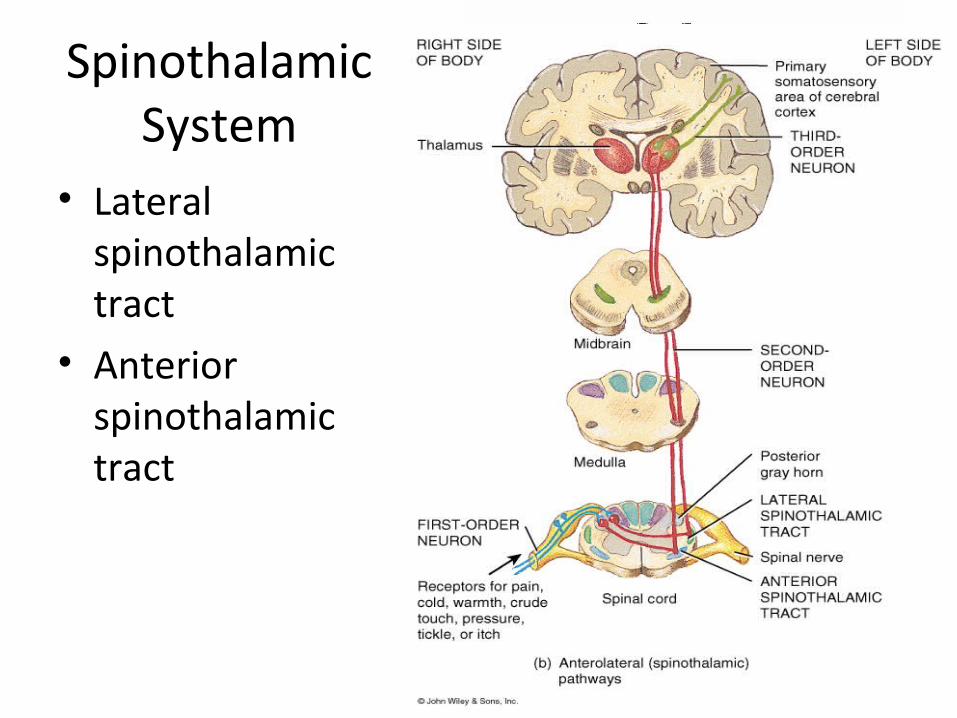
Spinothalamic System
• Lateral spinothalamic tract
• Anterior spinothalamic tract
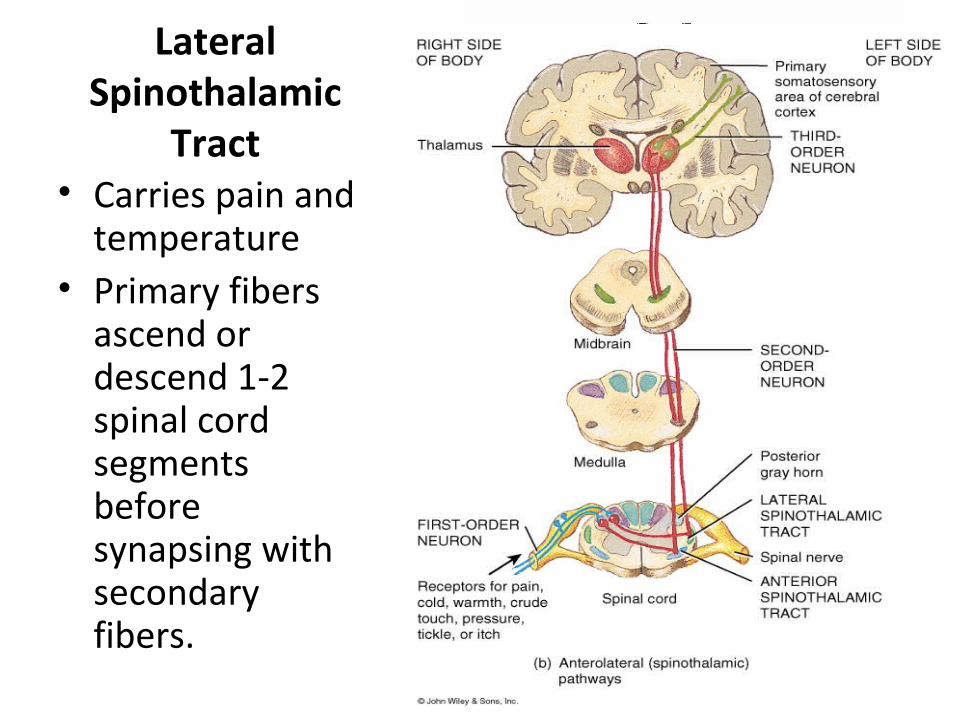
Lateral Spinothalamic
Tract• Carries pain and
temperature• Primary fibers
ascend or descend 1-2 spinal cord segments before synapsing with secondary fibers.

Lateral Spinothalamic
Tract• Secondary axons
decussate through anterior gray and white commissures.
• Secondary axons make up the lateral spinothalamic tract traveling in the lateral column of the spinal cord.

Lateral Spinothalamic
Tract• Secondary fibers
are joined in brainstem by fibers of the trigeminothalamic tract:
(Pain and temperature from face and teeth.)

Lateral Spinothalamic Tract
• Secondary fiber collaterals project to reticular formation:
Stimulate wakefulness and consciousness.
• Secondary fibers project to ventral posterolateral (VPL) nucleus of thalamus.

Lateral Spinothalamic Tract
• Secondary fibers synapse with tertiary fibers in VPL.
• Tertiary fibers (corticopetal fibers) synapse in postcentral gyrus:
Somatic sensory areas 3, 1, 2
• Tertiary fibers form part of internal capsule.
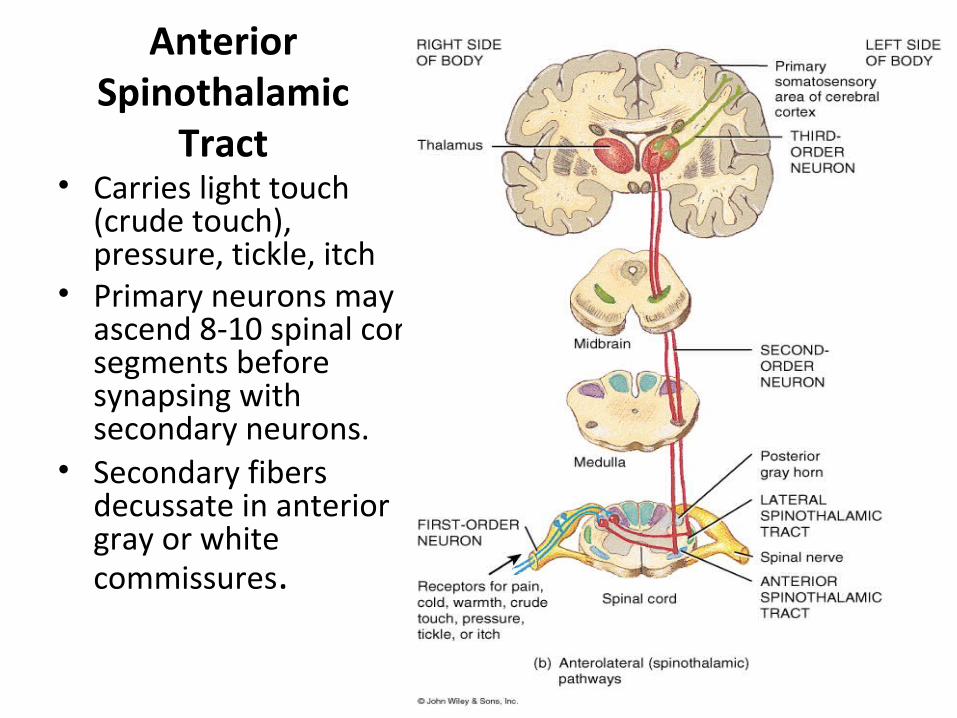
Anterior Spinothalamic
Tract• Carries light touch
(crude touch), pressure, tickle, itch
• Primary neurons may ascend 8-10 spinal cord segments before synapsing with secondary neurons.
• Secondary fibers decussate in anterior gray or white commissures.

Anterior Spinothalamic
Tract• Secondary fibers
ascend to synapse with tertiary fibers in VPL nucleus of thalamus.
• Tertiary fibers ascend through internal capsule to primary sensory cortex.

Posterior Spinocerebellar Tract
• Originates in thoracic and upper lumbar regions.
• Consists of uncrossed fibers that enter cerebellum through inferior cerebellar peduncles.
• Transmits ipsilateral proprioceptive information to cerebellum.
Anterior Spinocerebellar Tract
• Originates in lower trunk and lower limbs.• Consists of crossed fibers that recross in pons
and enter cerebellum through superior cerebellar peduncles.
• Transmits ipsilateral proprioceptive information to cerebellum.
Spino-Olivary Tracts
• Project to accessory olivary nuclei and cerebellum.
• Contribute to movement coordination associated primarily with balance.

Spinotectal Tracts
• Project to superior colliculi of midbrain.• Involved in reflexive turning of the head and
eyes toward a point of cutaneous stimulation.
Spinoreticular Tracts
• Involved in arousing consciousness in the reticular activating system through cutaneous stimulation.
12-27
Spinoreticular Tract
• Pain signals from tissue injury• Decussate in spinal cord and ascend with
spinothalamic fibers• End in reticular formation (medulla and pons)• 3rd and 4th order neurons continue to thalamus
and cerebral cortex

12-28
Descending (Motor) Pathways• Descending tracts deliver efferent impulses from
the brain to the spinal cord, and are divided into two groups– Direct pathways equivalent to the pyramidal tracts– Indirect pathways, essentially all others
• Motor pathways involve two neurons– Upper motor neuron (UMN)
• Begins with soma in cerebral cortex or brainstem• Its axon terminates ON the LMN in anterior horn
– Lower motor neuron (LMN)• Soma in anterior horn; axon leads to muscle• aka ‘anterior horn motor neuron” (also, final common
pathway)
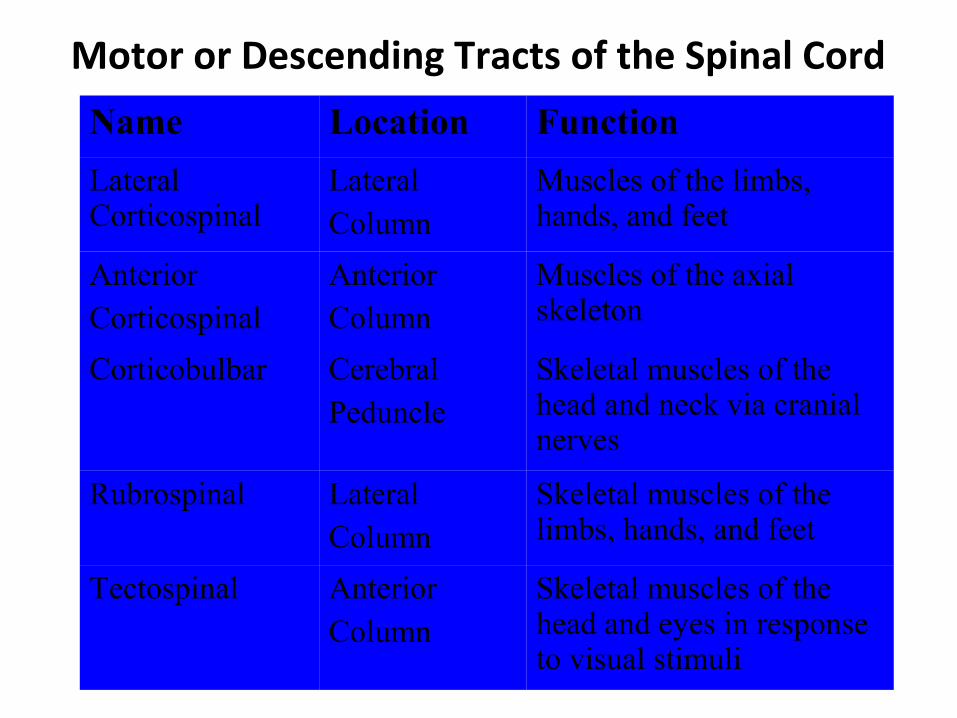
Motor or Descending Tracts of the Spinal Cord
Name Location Function
Lateral Corticospinal
LateralColumn
Muscles of the limbs, hands, and feet
AnteriorCorticospinal
AnteriorColumn
Muscles of the axial skeleton
Corticobulbar CerebralPeduncle
Skeletal muscles of the head and neck via cranial nerves
Rubrospinal LateralColumn
Skeletal muscles of the limbs, hands, and feet
Tectospinal AnteriorColumn
Skeletal muscles of the head and eyes in response to visual stimuli
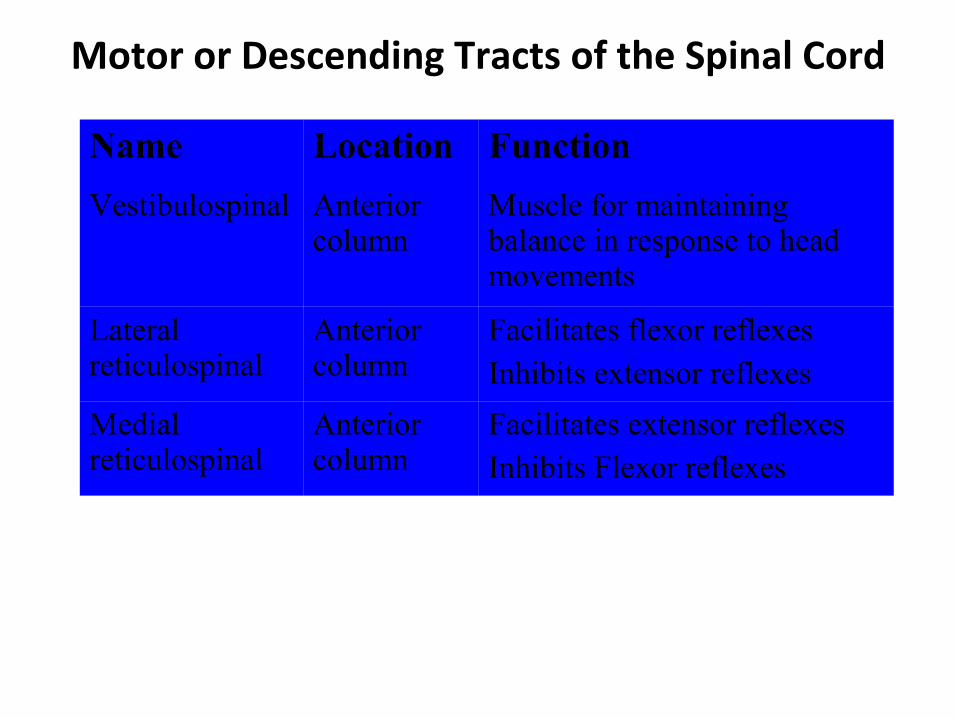
Motor or Descending Tracts of the Spinal Cord
Name Location Function
Vestibulospinal Anterior column
Muscle for maintaining balance in response to head movements
Lateral reticulospinal
Anterior column
Facilitates flexor reflexesInhibits extensor reflexes
Medial reticulospinal
Anterior column
Facilitates extensor reflexesInhibits Flexor reflexes
12-31
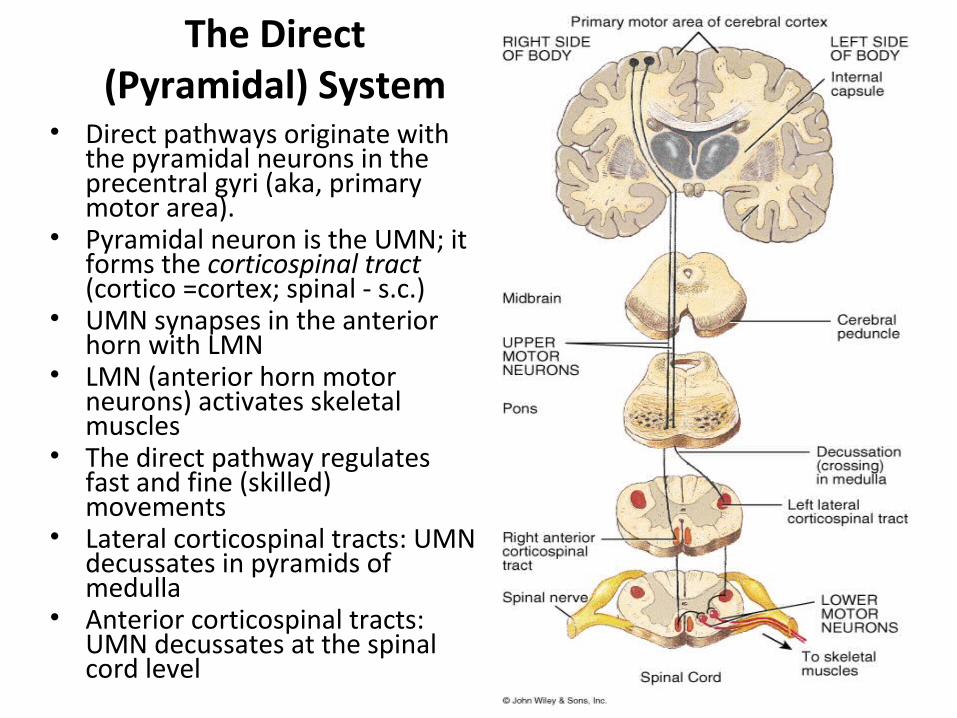
The Direct (Pyramidal) System
• Direct pathways originate with the pyramidal neurons in the precentral gyri (aka, primary motor area).
• Pyramidal neuron is the UMN; it forms the corticospinal tract (cortico =cortex; spinal - s.c.)
• UMN synapses in the anterior horn with LMN
• LMN (anterior horn motor neurons) activates skeletal muscles
• The direct pathway regulates fast and fine (skilled) movements
• Lateral corticospinal tracts: UMN decussates in pyramids of medulla
• Anterior corticospinal tracts: UMN decussates at the spinal cord level
12-32
Indirect (Extrapyramidal) System
• Upper motor neuron (UMN) originates in nuclei deep in cerebrum (not in cerebral cortex); .e., in brain stem,
• UMN does not pass through the pyramids• LMN is an anterior horn motor neuron • This system includes the rubrospinal, vestibulospinal,
reticulospinal, and tectospinal tracts• These motor pathways are complex and multisynaptic

C1-C4 May need breathing assistance
C5- No wrist or hand control, some shoulder and bicep control
C6- Includes some wrist control, no hand control
C7 and T1- Can straighten arms, lacking in hand and finger control
T1-T8- Most often include hand control, lack of trunk control
T9-T12- Have most trunk control, can balance sitting up
Lumbar and Sacral- Loss includes hip flexor and leg control

Diseases of the Spinal Cord


Basic Features of Spinal Cord Disease
• UMN findings below the lesion– Hyperreflexia and Babinski’s
• Sensory and motor involvement that localizes to a spinal cord level
• Bowel and Bladder dysfunction common• Remember that the spinal cord ends at about
T12-L1
History
• Onset– Acute, subacute, chronic
• Symptoms– Pain– Weakness– Sensory– Autonomic
• Past history• Family history

Tempo of Spinal Cord Disease
Acute Subacute Chronic
Trauma Mass lesion
X X
X
Infectious Inherited
X X X X
Vascular Autoimmune
X X
X X
X
Nutritional X
Motor Exam• Strength - helps to localize the lesion– Upper cervical
• Quadriplegia with impaired respiration
– Lower cervical• Proximal arm strength preserved• Hand weakness and leg weakness
– Thoracic• Paraplegia
– Can also see paraplegia with a midline lesion in the brain
• Tone– Increased distal to the lesion

Sensory Exam
• Establish a sensory level– Dermatomes
• Nipples: T4-5• Umbilicus: T8-9
• Posterior columns– Vibration– Joint position sense (proprioception)
• Spinothalamic tracts– Pain– Temperature

Autonomic disturbances
• Neurogenic bladder– Urgency, incontinence, retention
• Bowel dysfunction– Constipation more frequent than incontinence
• With a high cord lesion, loss of blood pressure control
• Alteration in sweating
Investigation of Spinal Cord Disease
• Radiographic exams– Plain films– Myelography– CT scan with myelography– MRI
• Spinal tap– If you suspect: inflammation, MS, rupture of a
vascular malformation

Etiology of Spinal Cord Disease

Traumatic Spinal Cord Disease
• 10,000 new spinal cord injuries per year• MVA, sports injuries the most common • Victims under 30 yrs old, male>>females• Fx/dislocation of vertabrae most likely to
occur at:– C5,6– T12, L1– C1,2

Tumors
• Metastatic or primary• Extramedullary– Extradural - most common• Bony - breast, prostate
– Intradural - very rare• Meninges - meningioma• Nerve root - schwannoma
– Intramedullary - very rare• Metastatic• Primary - astrocytoma or ependymoma

B12 Deficiency
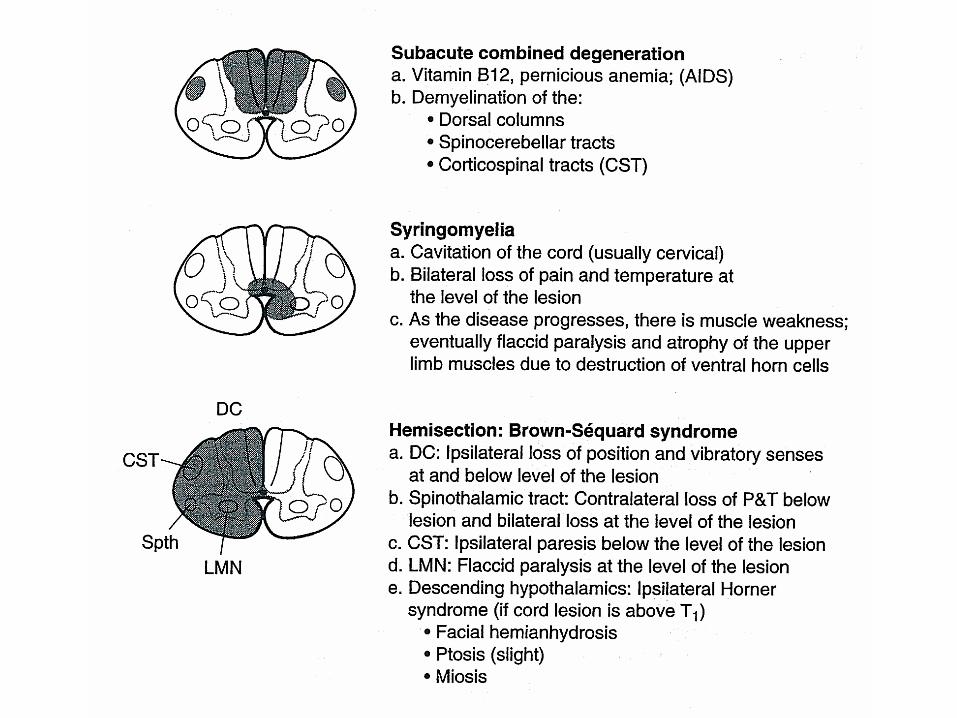
• Subacute combined degeneration of the cord• B12 deficiency– malabsorption of B12 secondary to pernicious
anemia or surgery– insufficient dietary intake - vegan
• Posterior columns and CST involvement with a superimposed peripheral neuropathy

Transverse myelitis
• Inflammation of the spinal cord – Post-infectious– Post-vaccinial– Multiple sclerosis
• Pain at level of lesion may preceed onset of weakness/sensory change/b&b disturbance
• Spinal tap may help with diagnosis

Infections Involving the Spinal Cord
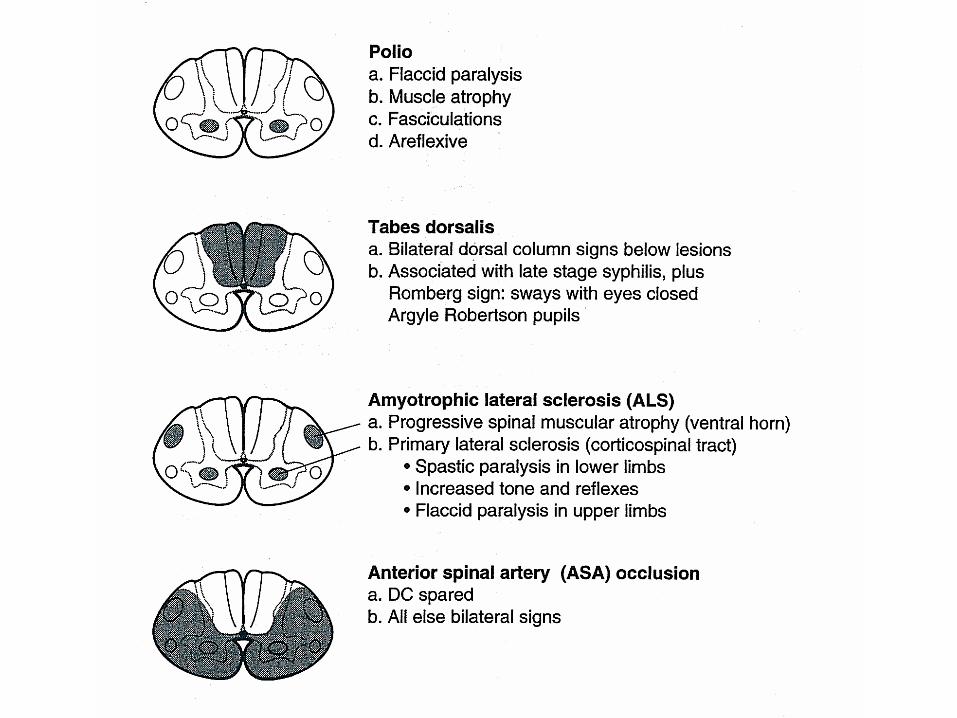
• Polio– only the anterior horn cells are infected
• Tabes dorsalis– dorsal root ganglia and dorsal columns are involved– tertiary syphillis– sensory ataxia, “lightening pains”
• HIV myelopathy– mimics B12 deficiency
• HTLV-1 myelopathy - – tropical spastic paraparesis

Multiple Sclerosis
• Demyelination is the underlying pathology• Cord disease can be presenting feature of MS
or occur at any time during the course of the disease
• Lesion can be at any level of the cord– Patchy– Transverse
• Devic’s syndrome or myelitis optica– Transverse myelitis with optic neuritis

Vascular Diseases of the Spinal Cord
• Infarcts– Anterior spinal artery infarct• from atherosclerosis, during surgery in which the
aorta is clamped, dissecting aortic aneurysm– less often, chronic meningitis or following trauma
• posterior columns preserved (JPS, vib)• weakness (CST) and pain/temperature loss
(spinothalamic tracts)
– Artery of Adamkiewicz at T10-11– Watershed area• upper thoracic

Vascular Diseases of the Spinal Cord, cont
• Arteriovenous malformation (AVM) and venous angiomas– Both occur in primarily the thoracic cord– May present either acutely, subacutely or chronically
(act as a compressive lesion)– Can cause recurrent symptoms– If they bleed
• Associated with pain and bloody CSF
– Notoriously difficult to diagnose
• Hematoma - trauma, occasionally tumor
Other Disease of the Spinal Cord
• Hereditary spastic paraparesis– Usually autosomal dominant
• Infectious process of the vertabrae– TB, bacterial
• Herniated disc with cord compression– Most herniated discs are lateral and only compress a
nerve root• Degenerative disease of the vertabrae– Cervical spondylosis with a myelopathy– Spinal stenosis

Classical spinal cord syndromes
• Anterior spinal artery infarct• Brown Sequard syndrome• Syringomyelia• Conus medullaris/caude equina lesions

Brown Sequard Syndrome
• Cord hemisection• Trauma or tumor• Dissociated sensory loss– loss of pain and temperature contralateral to lesion, one
or 2 levels below• crossing of spinothalamic tracts 1-2 segments above where they
enter
– loss of vibration/proprioception ipsilateral to the lesion • these pathways cross at the level of the brainstem
• Weakness and UMN findings ipsilateral to lesion
Syringomyelia• Fluid filled cavitation in the center of the cord• Cervical cord most common site– Loss of pain and temperature related to the
crossing fibers occurs early• cape like sensory loss
– Weakness of muscles in arms with atrophy and hyporeflexia (AHC)
– Later - CST involvement with brisk reflexes in the legs, spasticity, and weakness
• May occur as a late sequelae to trauma• Can see in association with Arnold Chiari
malformation
Conus Medullaris vs. Cauda Equina Lesion
Finding Conus CE
Motor Symmetric Asymmetric
Sensory loss Saddle Saddle
Pain Uncommon Common
Reflexes Increased Decreased
Bowel/bladder Common Uncommon