the success of neurohormonal blockade: looking back – looking forward: beta-blockers
TRANSCRIPT

The success of neurohormonal blockade: looking back – looking forward:
Beta-blockers
Karl SwedbergSenior professor of Medicine
University of GothenburgProfessor of Cardiology
Imperial College, London
Disclosures:Honoraria/Consultancy: Amgen, Astrazeneca, Novartis,
Pfizer, Servier, ViforResearch grants: Amgen, Servier

Treatment of heart failureTreatment of heart failureFrom two textbooks 1929 and 1974From two textbooks 1929 and 1974
”…and for all this there is only digitalis and rest…”
Paul Dudley White: Textbook in Cardiology, 1929
Moderately severe heart failure Decrease physical activity Institute digitalis Give thiazide every day plus potassium If not enough use furosemide and
if insufficient, combine them
J W Hurst: The Heart 3rd edition, 1974
J Willis Hurst1920-2011

Importance of adrenergic supportImportance of adrenergic support
Am J Medicine 1963; 39:442Am J Medicine 1963; 39:442
”These data suggest that the adrenergic nervous system plays an important compensatory role in the circulatory adjustments of patients to congestive heart failure, and emphasize the need for caution in the use of highly effective antiadrenergic drugs in the treatment of patients with limited cardiac reserve”

Myocardial norepinephrine depletionMyocardial norepinephrine depletion
Thus, norepinephrine depletion interferes with the ability Thus, norepinephrine depletion interferes with the ability of the adrenergic nervous system to support the failing of the adrenergic nervous system to support the failing myocardium and in this manner it may intensify the myocardium and in this manner it may intensify the congestive heart failure state.congestive heart failure state.
Circ Research 1966; 21:51 Circ Research 1966; 21:51

Beta-blockers in heart failure 1973Beta-blockers in heart failure 1973
Hjalmarson and Waagstein had postulated:Hjalmarson and Waagstein had postulated:●● A simple working hypothesis - energy starvationA simple working hypothesis - energy starvation●● High heart rate and sympathetic stimulation may High heart rate and sympathetic stimulation may
facilitate development of heart failurefacilitate development of heart failure●● Heart failure is a potential reversible conditionHeart failure is a potential reversible condition●● Bedside observations: beta-blockers were Bedside observations: beta-blockers were
antiischemic and well toleratedantiischemic and well tolerated

Waagstein et al. Br Heart J 1975; 37:1022Waagstein et al. Br Heart J 1975; 37:1022
First report of First report of blockers in HFblockers in HF

Effect of beta-blockade on ejection fractionby echocardiography
0 6 12 24 >24Months
0:4
0:5
0:1
0:2
0:3
0:4
0:5
0:6
Swedberg et al Br Heart J 1980

Effect of beta-blocker withdrawal
During -Blocker
B A
p<0.1
(Circ/s)
0.2
0.4
0.6
0.8
1.0
Mean VCF
Withdrawal
B A
p<0.01
0.1
0.2
0.3
0.4
0.5
0.6
0.7
(Ratio) EF
During -Blocker Withdrawal
Swedberg et al Br Heart J 1980

Effect of beta-blockade on survival in dilated cardiomyopathy
1 2 3 4 5
102030405060708090
10024 23 21 19 15 14 13 11 7 5
12111098
76
54
32
1
Years
Digitalis, diureticsAND a beta-blocker
Digitalis and diuretics ONLY
Surv
ival
(%)
Swedberg et al Lancet 1979

NorepinephrineNorepinephrine12001200
800800
400400
00ArterialArterialpp<0.001<0.001
Coronary SinusCoronary Sinuspp<0.001<0.001
CHF n = 30CHF n = 30
No HF n = 25No HF n = 25
Swedberg et al. Am J Cardiol 1984Swedberg et al. Am J Cardiol 1984
Myocardial Catecholamine Balance in Heart FailureMyocardial Catecholamine Balance in Heart Failure
Myocardial norepinephrine releaseMyocardial norepinephrine release

MDC Trial (Metoprolol in Dilated MDC Trial (Metoprolol in Dilated Cardiomyopathy)Cardiomyopathy)
ll Multicenter trial in 33 centers in Europe Multicenter trial in 33 centers in Europe and North America. Coordinated from and North America. Coordinated from Göteborg (Coordinator: Finn Waagstein)Göteborg (Coordinator: Finn Waagstein)
ll Primary objective: Death or need for heart Primary objective: Death or need for heart transplanttransplant
ll Randomized, double-blind, Randomized, double-blind, placebo/metoprolol 50 mg 2-3 times dailyplacebo/metoprolol 50 mg 2-3 times daily
ll 383 patients with idiopathic dilated 383 patients with idiopathic dilated cardiomyopathy, EF <40%, followed for 12-cardiomyopathy, EF <40%, followed for 12-18 months.18 months.
Waagstein et al Lancet 1993; 342: 1491Waagstein et al Lancet 1993; 342: 1491

placebo
metoprololRisk reduction 34% (95% CI 62 to -6)
Risk reduction 34% (95% CI 56 to 0)
MDC-trialMDC-trialDeaths or heart transplantations Deaths or heart transplantations
(primary outcome)(primary outcome)
Waagstein F et al Lancet 1993, Andersson B et al Lancet 1998;351:1180

placebo (189)
metoprolol (194)
Risk reduction 0.4 (95% CI 0.16-0.97)
Prevention of cardiac transplantation Prevention of cardiac transplantation in the MDC trialin the MDC trial
Waagstein F. Lancet 1993; Andersson B. Lancet 1998;351:1180

ACC/AHA Guidelines for the ACC/AHA Guidelines for the management of CHF 1995management of CHF 1995

ACC/AHA Guidelines 1995
• ” use of beta-blockers for the treatment of chronic heart failure remains investigational, but the official status of beta-blockers may change as recent data are reviewed. Hence, physicians might consider the use of a beta-blocker in selected patients with chronic heart failure.”

Carvedilol(n=696)
Placebo(n=398)
Survival
Days0 50 100 150 200 250 300 350 400
1.0
0.9
0.8
0.7
0.6
0.5
Risk reduction = 65%p<0.001
Packer et al (1996)Packer et al (1996)
CIBIS-II Investigators (1999)CIBIS-II Investigators (1999)
0 200 400 600 800
Bisoprolol
Placebo
Time after inclusion (days)
p<0.0001
Survival
Risk reduction = 34%
The MERIT-HF Study Group (1999)The MERIT-HF Study Group (1999)
US Carvedilol Programme
CIBIS-II
0.8
1.0
0.6
0
Months of follow-up
Mortality (%)
0 3 6 9 12 15 18 21
20
15
10
5
0
Placebo
Metoprolol CR/XL
p=0.0062Risk reduction = 34%
MERIT-HF
COPERNICUS:COPERNICUS:
MonthsMonths
0000
33 66 99 1212 1515 1818 2121
100100
9090
8080
6060
7070
CarvedilolCarvedilol
PlaceboPlacebo
Risk reduction = 35%
p = 0.00013p = 0.00013
Survival
Packer et al (2001)
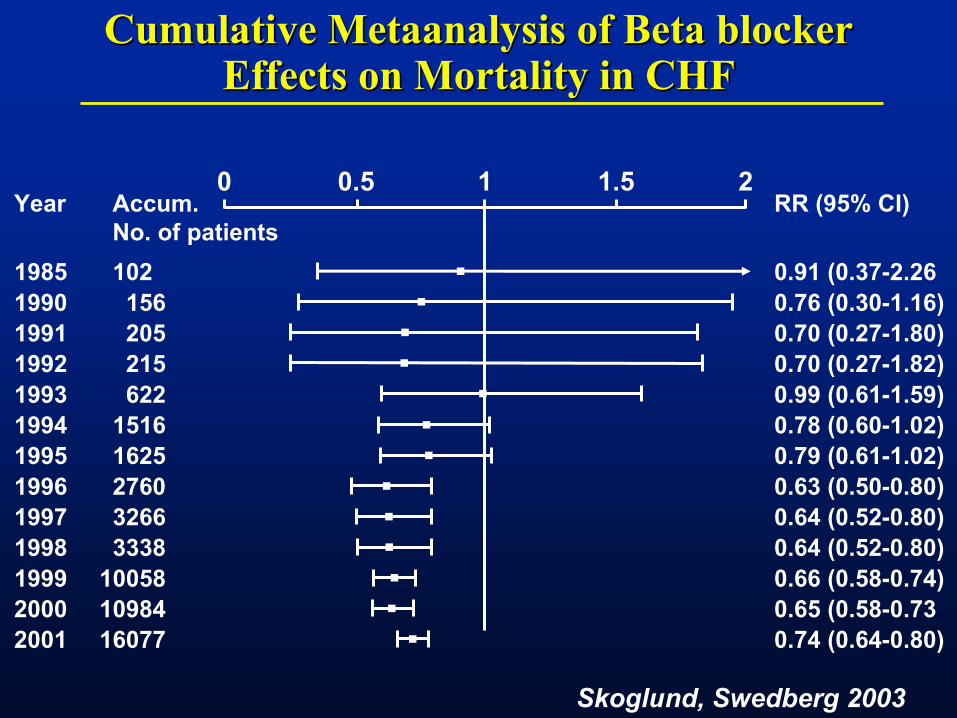
Cumulative Metaanalysis of Beta blocker Cumulative Metaanalysis of Beta blocker Effects on Mortality in CHFEffects on Mortality in CHF
RR (95% CI)
0.91 (0.37-2.260.76 (0.30-1.16)0.70 (0.27-1.80)0.70 (0.27-1.82)0.99 (0.61-1.59)0.78 (0.60-1.02)0.79 (0.61-1.02)0.63 (0.50-0.80)0.64 (0.52-0.80)0.64 (0.52-0.80)0.66 (0.58-0.74)0.65 (0.58-0.730.74 (0.64-0.80)
0 0.5 1 1.5 2Year
1985199019911992199319941995199619971998199920002001
Accum.No. of patients102
156205215622
15161625276032663338
100581098416077
Skoglund, Swedberg 2003

Beta-blocker Trials in Heart FailureBeta-blocker Trials in Heart FailureEffects on MortalityEffects on Mortality
Beta-blockerBeta-blocker
WorseWorseBetterBetter
1.01.00.50.5 0.250.25
TotalTotal
0.910.91
CIBIS IICIBIS II
MERITMERIT
BESTBEST
0.670.67
0.680.68
0.640.64
0.740.74
PreviousPrevious
COPERNICUSCOPERNICUS0.650.65
ResolvdResolvdMetaanalysis incl. Metaanalysis incl. 15202 patients 15202 patients 2243 deaths 2243 deaths

Meta-analysis of 22 beta-blocker studies in Meta-analysis of 22 beta-blocker studies in CHFCHF
Brophy et al Ann Int Med 2001

Mechanism?Mechanism?
ll Why and how do treatment with a beta-Why and how do treatment with a beta-blocker work?blocker work?

23 trials in 19 209 HF patients with beta23 trials in 19 209 HF patients with beta--blocker (mean EF=17%-36%)blocker (mean EF=17%-36%)
McAlister et al. Ann Intern Med. 2009;150:784-794.
BetaBeta-blocker dose and heart rate reduction -blocker dose and heart rate reduction in chronic HF patientsin chronic HF patients
Results of 13 univariable meta-regressions evaluating the effect of individual covariates on mortality benefits of beta-blockers in heart failure

ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
Which beta-blocker dose?Beta-blocker
First dose (mg) Increments
(mg/day)
Target dose (mg/day)
Titration period
Bisoprolol 1.25 2.5, 3.75, 5, 7.5, 10
10 Weeks-month
Metoprolol succinate/CR
12.5/25 25, 50, 100, 200
200 Weeks-month
Carvedilol 3.125 6.25, 12.5, 25, 50
50 Weeks-month
Nebivolol 1.25 2.5, 5, 10 10 Weeks-month

Randomised3029
Carvedilol1511
Metoprolol1518
Assigned to drug and received at least one tablet
Withdrew consent 10Lost to follow-up 3
Withdrew consent 18Lost to follow-up 2
Flow chart of patients
Poole-Wilson et al Lancet 2003

Time (years)
Mortality (%)
0
10
20
30
40
0 1 2 3 4 5
Metoprolol
Carvedilol
hazard ratio 0.83, 95% CI 0.74-0.93, p=0.0017
Primary endpoint of mortality
Number at riskCarvedilol 1511 1367 1259 1155 1002 383Metoprolol 1518 1359 1234 1105 933 352
Poole-Wilson et al Lancet 2003
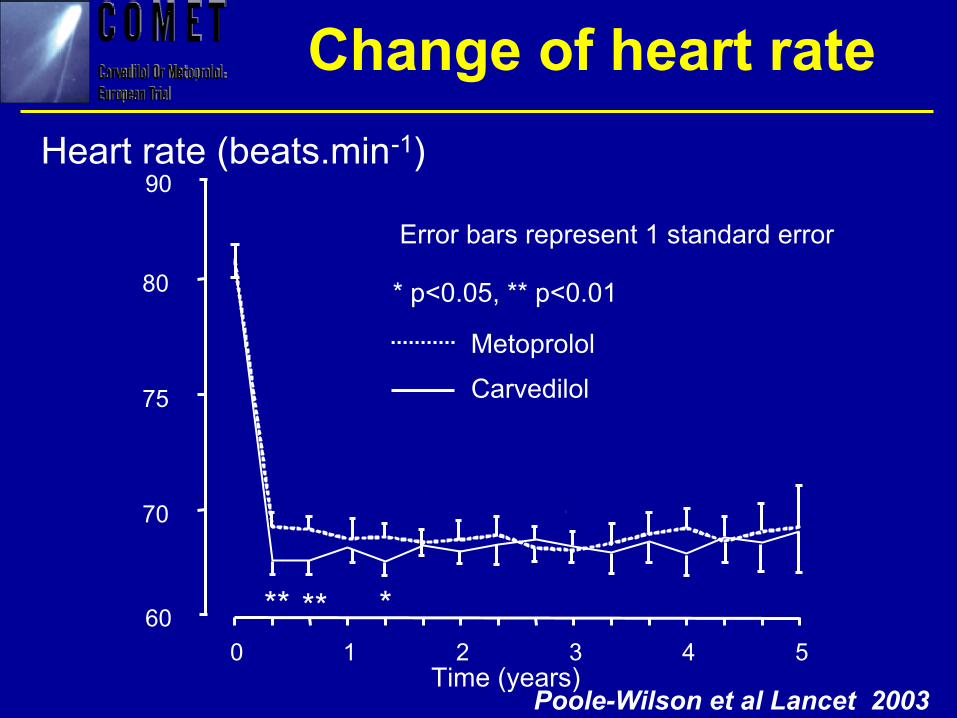
Heart rate (beats.min-1)
Metoprolol
Carvedilol
Time (years)
70
75
80
0 1 2 3 4 560
90
** ** *
Change of heart rate
* p<0.05, ** p<0.01
Error bars represent 1 standard error
Poole-Wilson et al Lancet 2003

ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
Which beta-blocker dose?Beta-blocker
First dose (mg) Increments
(mg/day)
Target dose (mg/day)
Titration period
Bisoprolol 1.25 2.5, 3.75, 5, 7.5, 10
10 Weeks-month
Metoprolol succinate/CR
12.5/25 25, 50, 100, 200
200 Weeks-month
Carvedilol 3.125 6.25, 12.5, 25, 50
50 Weeks-month
Nebivolol 1.25 2.5, 5, 10 10 Weeks-month

•883 patients with CHF at 41 centres, naive to BB or on a low dose.
•Randomised to carvedilol or bisoprolol
•Forced titrated to target doses according to ESC Guidelines

CIBIS-ELD CIBIS-ELD Achieved dose levelsAchieved dose levels
Dose level Bisoprolol n=431 %
Carvedilol n=445 %
12.5% 11 1025% 25 2250% 23 25100% 31 32> 50% 54 54
Dungen et al EJHF 2011
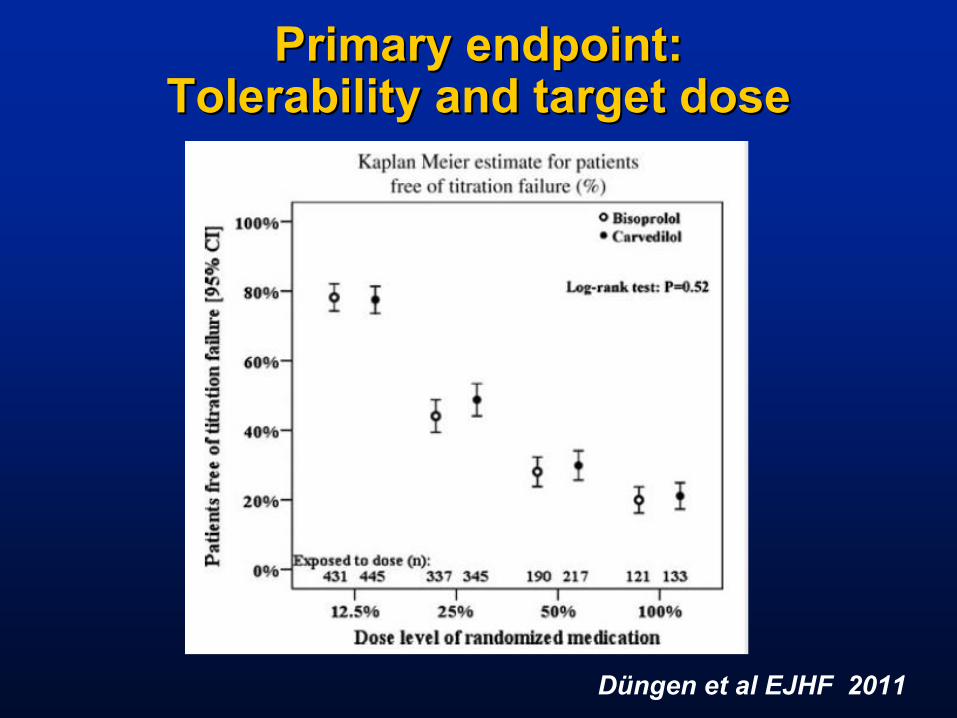
Primary endpoint: Primary endpoint: Tolerability and target doseTolerability and target dose
Düngen et al EJHF 2011

International Journal of Cardiology 155 (2012) 160–166

Heart Rate by Dose LevelHeart Rate by Dose Level
Gelbricht et al. IJC 2012.

SummarySummary
·· Treatment of chronic systolic heart failure Treatment of chronic systolic heart failure with a beta-blocker is the most effective with a beta-blocker is the most effective pharmacological therapy.pharmacological therapy.
·· From the first report of beneficial effects, it From the first report of beneficial effects, it took around 25 years for general acceptance.took around 25 years for general acceptance.
·· There is still a major under-treatment in There is still a major under-treatment in clinical practiseclinical practise