«the unit for breast care» - the tqm project that ... · when invited for total quality...
TRANSCRIPT

APPLICATION FOR TQM APPLIED LEARNING AWARDS Submitted by Danijela Lazarić-Zec (TQM 2004)
January, 2006
Danijela Lazarić-Zec, MD, MPH Public Health Institute of County Istria Pula Department of social medicine Vladimira Nazora 23 52100 Pula Croatia Tel: 385 52 529 018 Fax: 385 52 222 151 e-mail: [email protected]
«The Unit for Breast Care» - the TQM project that shortened duration of diagnostic procedures in women with breast cancer in Istria”
MIPH Alumni Sponsoring the Submission Dr. Selma Sogoric, MD, MPH, Ph.D. (MIPH 2001) Andrija Stampar School of Public Health Department of the Social Medicine and Organization of Health Care Services Medical School, University of Zagreb Rockefellerova 4 10 000 Zagreb, Croatia tel: 385 1 45 66 996 fax: 385 1 45 90 275 e-mail: [email protected] and Sonja Grozic-Zivolic (MIPH 2002) Department of Health and Social welfare of the County of Istria Flanaticka 29 52 100 Pula, Croatia tel: 385 52 37 21 53 fax: 385 52 37 21 54 e-mail: [email protected] Project leader: Marija Tatković, MD, MS; oncologist, General hospital in Pula Project team members: Zoran Cukon, MD, radiologist, General hospital in Pula, Jolanda Šumberac, nurse at oncology department, General hospital in Pula; Romanita Rojnić, MD, chief, Department for health and social welfare, Istrian County Ornela Grujić – Cukon, MS, Croatian health insurance institute, Istrian Department

I. BACKGROUND
Early detection of breast cancer is one of five Istrian public health priorities, selected in the process of strategic planning for health on county level. The process was guided by a group of MIPH alumni, who, after attending the courses in CDC, Atlanta, developed a Counties Public Health Capacity Building Program "Health - Plan for it". Results of the Program are described in three strategic documents: Istria Health Profile, Strategic framework of the Plan for Health and Istrian Plan for Health, all approved by entitled County authorities. Following the principle and the practices derived from "Health - Plan for it", different aspects of public health problem were analysed, and consultations with all relevant "stakeholders" and local experts were conducted. When speaking about the breast cancer we found that breast cancer is first cause of death in women age 35-59. Over the past 15 years age-specific incidence rates of female breast cancer are increasing, especially among women aged 45-64. In the same time, age-specific death rates of breast cancer are decreasing (Picture 1.). Breast cancer is diagnosed in an early stage (≤ 10 mm) in only 19% of women. Picture 1. Age-specific incidence and death rates of female breast cancer per 100.000 women aged above 45 in Istrian County
One of the most important "stakeholders" in the breast cancer detection (as well as treatment) is General hospital in Pula. It is the only general hospital in the County and it is caring for about 200 000 people. When invited for Total Quality Management (TQM) workshop, Istrian Healthy County team counselled the director of the hospital and asked him to select 3-5 professionals for training. We suggested the specialists who already work with breast cancer patients and who will be able to improve health care of women with breast cancer. After some mutual consultations and agreements an intersectorial team composed of oncologist, radiologist and nurse at oncology department was appointed. “Facilitators” from Institute of public health, local government (Department for health and social welfare, Istrian County) and Croatian health insurance institute, Istrian Department joined them in training. Training was organised in Kraljevica, Uvala Scott, Croatia in May 2004 by MIPH alumni from the Andrija Stampar School of Public Health, Zagreb, Croatia with assistance of SMDP, CDC, Atlanta.
0
50
100
150
200
250
average 1991.-1995. average 2000. - 2004.
incidence rate - aged 45-64incidence rate - ages above 65death rate - aged 45-64death rate - aged above 65

II. THEME SELECTION MATRIX
During the education, intersectorial team together with facilitators discussed several problems in detection and treatment of breast cancer. In process of negotiation we tried to reach consensus about the problem. It was not an easy task, but a Theme Selection Matrix helps us a lot. When we put in our team scores for problems, we noticed that "long diagnostic procedure in women with breast cancer" gets the highest team score - so it was seen as a most important. Table 1. Theme Selection Matrix
Themes Customer(s) Impact on Customer(s)
Need to Improve
Overall
Insufficient communication beetwen units in General Hospital Pula caring for patients with breast cancer
doctors, patients
3,5
4
14
long diagnostic procedure in women with breast cancer
outer patients 5
4
20
long waiting lists for patients with health insurance with no possibilities for payed mamography
patients
3,25
3,8
12,35
We want to stress the fact that during this workshop we had not quantitative data on our disposal. All decisions were made on previous experience and personal impressions of TQM team members.
III. PROCESS FLOW CHART Description of the diagnostic procedure in women with breast cancer is completed through the Process Flow Chart (Picture 2.). Some steps of the process are performed in Hospital (coloured in red). Those are also the parts of the process on which we can have influence, we can change it. Mammography and ultrasound of breast can be done in Hospital but also outside - in private radiology units all over the Istrian County. Therefore we coloured this step of process flow chart in blue colour. There were two pathways in diagnostic procedures (after patient’s first contact with health care i.e. general practitioner’s examination): A started with mammography: mammography, ultrasound – cytology - back to GP –
oncologist - back to GP - surgeon B started with oncologist: oncologist - back to GP - mammography, ultrasound –
cytology - back to GP – oncologist - back to GP - surgeon.


Picture 2. Process flow chart
Start of diagnostic procedure
Examination by GP
Further diagnostic procedure is needed?
No End
Yes
Starting with oncologist?
No
Yes
Examination by oncologist
GP
Oncologist recommanded further procedures?
Mamography and ultra-sound
Yes
No End or control for 6 months
GP To oncologist?
Examination by oncologist
Yes
End or control for 6 months
GP
Operation is needed?
No
YesGP
Operation can be done?
No
Chemotherapy
YesOperation
No
End??
End?? citology
Examination by surgeon Preoperative procedures (lab tests, radiology of chest,
examination by cardiologist and anesthesiologist

IV. PROBLEM STATEMENT
Retrospective data about pathways in diagnostic procedure and time needed for every step in this process were analysed. Between December 2003 and May 2004 at Pula's General Hospital 34 women with breast cancer were operated at surgery department. 18 operated women started the diagnostic procedure with mammography (pathway A), while 16 of them performed pathway B (oncologist's examination without previous mammography). The average time needed for diagnostic procedure in all 34 women was 49 days. We found differences in duration of diagnostic procedure for these two pathways: in women started with oncologist in average 44 days, and in women started with mammography 54 days. Another difference was noticed: in pathway A (started with mammography) a step "from mammography to oncologist" was the longest (34 days). In the same time, women in pathway B spend only 17 days for step "from oncologist to mammography" (Picture 3.).
Picture 3. The average time of diagnostic procedure in women with breast cancer
Problem statement: The requested time for the procedure from the first diagnostic step till the operation of the women with breast cancer during the period from December 2003 to May 2004 in Pula's General Hospital was too long (takes 49 days).
V. TARGET FOR IMPROVEMENT
Target for improvement: To decrease the time needed for diagnostic procedure in women with breast cancer from 49 to 24 days (50%) in one-year period. (Picture 4.)
0
10
20
30
40
50
60oncologist - mammography -operationoncologist - mammography andultrasoundmammography - cytology
cytology - operation
mammography - oncologist -operationmammography - ultrasound -oncologistoncologist - cytology
cytology - operation

Picture 4. Duration of diagnostic procedure: starting points, aims and ideals
VI. FISHBONE ANALYSIS AND VERIFICATION OF THE ACTIONABLE ROOT CAUSES
We realized four main cathegories of causes: 1. Insufficient communication (in hospital, with GPs and with patients) 2. Women delaying diagnostic procedure 3. No special Unit for breast care 4. Waiting lists for urgent mammography at Radiology
During process of fishbone analysis we identified five actionable root causes: 1. Possibility of using new special documentation in urgent situations was not
implemented – this was very useful information we get from our team member working in national health insurance
2. Bad organization of urgent mammography at radiology – this was oncologist feedback to radiologist
3. Plan how to organize Unit for breast care was never completed, there were some ideas five years ago but all remained in “heads”
4. Virtual networking of all units included in diagnostic procedure was not established for out-patient’s data, while networking exists for in-patients data
5. No psychological support for women delaying diagnostic procedure was organized, while psychological support for oncology patients (after cancer is detected and operated) exists
0102030405060
Started w ith oncology Started w ithmammography
All w omen
starting pointsaimsideals

Picture 5. Fishbone analysis
Too long diagnostic procedure in women with breast cancer
Insufficient communication
Women delaying diagnostic procedure
No special unit for breast care
Waiting lists for urgent mammography
All cancer patients visiting the some
No criteria
Non adequate personal communication between hospital's units
Hospital on two locations
Diagnostic procedure's process is to complex
Non defined location and
Non defined time-table
No defined organization plan of unit for breast care
Not implemented possibility of using new special documentation in urgent situations
Urgent is not treated as priority
Inadequate organization at Radiology
Low level of care for breast health
Fear from cancer
Miths on incurable cancer
No psychological support for women
Non adequate communication with GPs (no signals that urgent is not treated as urgent)
Non adequate communication with patients (quality of care)
No virtual communication between hospital's units

VII. OBJECTIVES
• To organize Unit for breast care • To eliminate waiting lists for urgent mammography • To improve communication between hospital’s units • To provide better support for preventing women delaying diagnostic procedures
VIII. COUNTERMEASURES
Picture 6. Causes, countermeasures and practical methods
Cause Countermeasure Practical method Not implemented possibility of using new special documentation in urgent situations
implementation of new special documentation in urgent situations
Meeting at Oncology unit, new guidelines for urgent procedures
Bad organization at radiology in cases of urgent mammography
organizational improvements at radiology
Meeting with chief of Radiology
No organization plan of Unit for breast care
organization plan of Unit for breast care
Meetings for hospital's staff and management, Plan paper
Inadequate virtual networking of all units included in diagnostic procedure
improve virtual networking Software modifications, more hardware units
No psychological support for women delaying diagnostic procedure
Organize psychological support
Meetings with coordinator of psychological counseling for patients with cancer
After TQM training, our team presented new project proposal to director and department's chiefs at joint meeting. As our project implementation depends on these "stakeholders", it was very important to gain their commitment.
IX. RESULTS
1. Unit for breast care is organized as a part of oncology department inside existing location, space, staff and equipment, working part time tree days a week.
2. Software modifications and more hardware units improved virtual networking among unit for breast care, surgery and radiology department (Picture 7.).

Picture 7. Virtual network organisation of Unit for breast care with future plans 3. Oncologists from Unit for breast care sent 54 women for urgent mammography,
ultrasound and cytology, average time needed for all steps in urgent procedure was 6 days and breast cancer was detected in 13 women (13/54)
4. There are no more waiting lists for urgent mammography at Radiology 5. Psychological counselling is established for all cancer patients with a possibility of
reaching women who delay diagnostic procedures. Although the psychological support was offered, engaged staff and women didn't use it in observed period. We think that this is an issue that we have to work on.
One-year results indicated that 56 women were operated for breast cancer in General hospital Pula with 25,71 days long diagnostic procedure (women started with oncology - 22,79 days, women started with mammography - 27,91 days) (Picture 8.).
General Hospitalin Pula
Breast Care Unit(part of Oncology Department)
Department ofRadiology
Department ofCitology
Department ofSuregery
Department ofPatology
Radiology UnitUMAG
Radiology UnitPOREČ
Radiology UnitROVINJ
Radiology UnitBUZET
Radiology UnitLABIN
Established communication
Planned in future
PULA

Picture 8. Duration of diagnostic procedure - starting points, aims and results
The time needed for critical steps in diagnostic procedure also decreased: - from mammography to oncologist at 16,11 days (before 34,13 days), - from oncologist to mammography at 4,43 days ( before 17,09 days).
In general, two pathways in diagnostic procedures remains, but in pathway B some modifications are implemented - new Unit for breast care is organzsed. With this new structure pathway B is faster (in urgent situations - 6 days). Organizational improvement at Radiology in urgent mammography procedures contributed in reaching aims in both pathways. As mammography can be done in radiology units outside Hospital, aim in pathway A (starting with mammography) is not reached in total, but the time needed for diagnostic procedures decreased substantially.
All GP's in Istrian County get an information letter about Unit for breast care signed by the director of Hospital.
Unit for breast care in co-operation with League for fight against cancer (NGO) organized 2 educational events for doctors in general practice. During these events Unit for breast cancer was described and discussed.
One-year results were presented on special press conference held in Hospital (Picture 9.) in the presence of the President of the County, director of the Hospital, all hospital departments' chiefs and Healthy county team.
0102030405060
All women Started withoncology/Unitfor breast care
Started withmammography
starting pointsaimsresultsideals

Picture 9. Press conference in General hospital in Pula on results of TQM project
Abstract "Lazaric - Zec D, Tatkovic M, Cukon Z, Sumberac J, Rojnic R, Grujic- Cukon O. Total Quality Management in Istrian County Hospital" was accepted from 13th EUPHA (European Conference on Public Health) Scientific Committee, presented in November 2005 on conference held in Graz, Austria and published in a supplement of European Journal of Public Health (Eur J Public Health. 2005;15 (1 Supp):146). (Picture 10.)
Added values
Some added values are recognized: improved communication between units (personal and virtual), patient's and GP's higher satisfaction with better organized health care and decreased time needed for diagnostic procedure.
X. EFFORTS TO STANDARDIZE RESULTS
TQM was useful method in efforts to decrease time needed for diagnostic procedure in women suspected to have breast cancer. This practice intends to be a challenge for improving quality in other health care problems and settings.
Guidelines for the procedure in Unit for breast care were set: - nurse receive patients in Unit for breast care on behalf of documentation from GP - oncologist examines woman - oncologist decides if there is a need for further urgent procedures (example – there is a
node in patient's breast but there is no mammography done) - oncologist writes special new documentation allowing patient's further urgent diagnostic
procedure (without new GP' documentation for this procedures) - oncologist waits on results of diagnostic procedures (can be reached virtual) - oncologist writes recommendations to GP - nurse is caring for women in urgent diagnostic procedure, - if women didn't come back in 7 days to get results, nurse makes report to oncologist

- oncologist contacts patient's GP, trying to understand why patient didn't come back to oncologist
- oncologist and GP discuss the need for psychological support for patient if necessary - psychologist, specialized in care for oncology patients, contacts patient if psychological
support is needed
All staff in Unit for breast care was informed about new guidelines.
TQM team have monthly meetings discussing improvements and new challenges, setting new tasks, responsible people and deadlines and every three-months discussing monitored results.
New Process flow chart was drawn (Picture 11.). Steps of process are coloured: in green colour newly implemented steps in pathway B including Unit for breast care, in blue colour mammography and ultrasound that can be performed outside Hospital and in red colour routine steps in Hospital.
XI. FUTURE PLANS
1. Pathology and cytology department will be included in second stage of virtual networking inside General hospital Pula.
2. As we recognized our weakness in this TQM project (radiology units outside Hospital were out of our influence), virtual networking with other radiology units in Istria County is also planned (Picture 7.).
3. Further software modifications are also planned: alert in cases women delaying diagnostic procedure, monitoring for duration of diagnostic procedure (monthly, three monthly, six monthly and yearly reports).
All this activities have the common goal: better co-ordination of breast care and forward decrease in duration of diagnostic procedure in women with breast cancer.
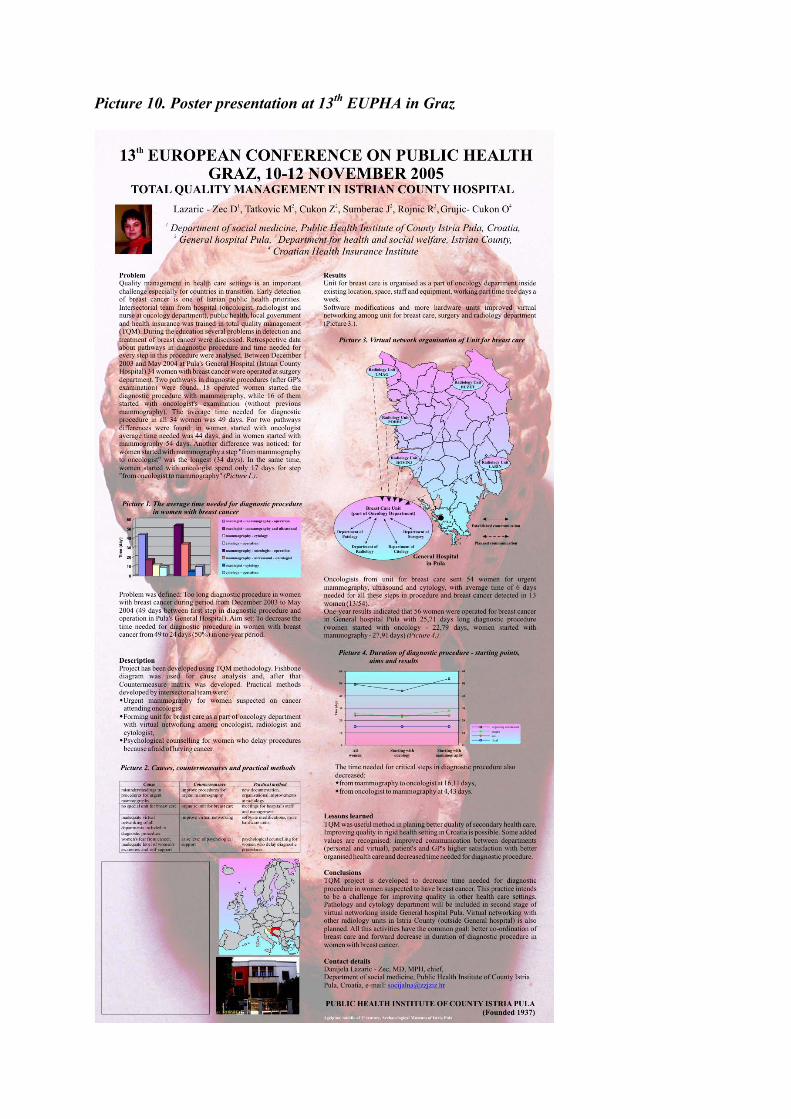
Picture 10. Poster presentation at 13th EUPHA in Graz

Picture 11. New Process Flow Chart - diagnostic procedures in women suspected for breast cancer
Start of diagnostic procedure
Examination by GP
Further diagnostic procedure is needed?
No End
Yes
To Unit for breast care?
No
Yes
Examination in Unit for breast care
Urgent procedures are needeed?
Mamography and ultra-sound
Yes
No End or control for 6 months
GP To oncologist?
Examination by oncologist
Yes
End or control for 6 months
GP
Operation is needed?
No
Yes
GP
Operation can be done?
No
Chemotherapy
YesOperation
No
End??
End?? citology
Examination by surgeon Preoperative procedures (lab tests, radiology of chest,
examination by cardiologist and anesthesiologist
Urgent mamography and ultrasound
Oncologist get results