the use of bone stimulators with athletes · treatment of non-unions • 1985 - brighton and...
TRANSCRIPT

The Use of Bone Stimulators With Athletes
James Sullivan DPM, ATCEATA Symposium 2006
Philadelphia, Pennsylvania
Bone
• Anatomical Structure
• Physiological Organ

Bone
• Anatomical Structure
• Provides rigid framework• Serves as a lever system for movement• Provides protection to vulnerable viscera

Physiological Organ
• Contains hemopoetic tissue• Production of Erythrocytes• Production of Leukocytes• Production of Platelets
Physiological Organ of Storage
• Calcium • Phosphorus• Magnesium• Sodium

Bone Cells
• Osteoblasts• Osteoclasts• Osteocytes• Bone Morphogenic Protein

Osteoblasts
• Essential for osteogenesis or ossification, since they produce the matrix in which calcification will occur. Once calcification occurs in the matrix, the tissue is bone.
Osteocytes
• An osteoblast once surrounded by the organic intercelluar substance, (or matrix), that it forms, it is then within the lacuna. It is now an osteocyte. Each osteocyte extends cytoplasmic processes or canuliculi to connect to neighboring osteocytes.

Bone Morphogenic Protien
• Bone Morphogenic Protien, (BMP), is responsible for differentiation of the mesenchymal cells to osteoblasts.


Blood Supply to Bone
• Afferent vascular system involving nutrient and metaphyseal arteries that combine to supply the inner two thirds of the cortex and the periosteal arteries that supply the outer one third.

Blood Supply to Bone
• Efferent vascular system that conveys venous blood

Cortical Bone
• Initial bleeding followed by clotting of vessels at fracture sight and a few millimeters away from the fracture sight.
• Fracture hematoma gives a medium for early stages of healing

Cortical Bone
• Internal and external callus formation occurs
• Stage of Clinical Union• Stage of consolidation or radiographic
union

Cancellous Bone
• Healing primarily occurs through an internal or endosteal callus formation, within the fracture hematoma
• Woven or non-lemellar bone quickly forms within the endosteal callus
• Woven bone is replaced with lemellar bone which creates a clinical union, remodeling and consolidation follows


Fracture Demographics
• >6,000,000 Fractures Annually• 3% - 5% Non-Healing• 200,000 - 300,000 Non - Healing

Stages of Fracture Healing
• Hematoma Formation and Inflammation• Cartilage Formation• Cartilage Calcification and Angiogenesis• Bone Formation• Remodeling of Fracture Callus


Historical BackgroundHistorical Background
Authors Publication Date Topic
Fukada and Yasuda 1954, 1957 Piezoelectric Properties of Dry Bone
Bassett and Becker 1962 Electrical Properties of Hydrated Bone
Friedenberg and Brighton 1966 Electrical Properties of Hydrated Bone
Shamos and Lavine 1967 Piezoelectric Properties of Biological
Tissues
Anderson and Eriksson 1968 Electrical Properties of Hydrated
Collagen
Bassett and Pawluk; Lotke, Black,
Richardson; Grodzinsky, Lipshitz,
Glimcher
1972, 1974,
1978
Electromechanical Properties of
Articular Cartilage

History of Bone Stimulators
• 1979 - FDA approves PEMF technology for treatment of non-unions
• 1985 - Brighton and Pollack report on the treatment of non-unions with direct current
• 1986 - FDA approves the use of capacitive coupling technology for treatment of non-unions

History of Bone Stimulators
• 1994 - FDA approves the use of CMF technology in the treatment of non-unions
• 1994 - FDA approves the use of ultrasound technology in the use of fresh fractures

The Bone Formation CycleThe Bone Formation Cycle
Nutr it ionNutr it ion
3. CellsOsteogenicity
1. Matrix:Osteoconduction
2. BiologicalStimulantsOsteopromotionOsteoinduction

Biophysical Stimulationof Bone Formation
Biophysical Stimulationof Bone Formation
Electrical and Electromagnetic Field– CCEF, CMF, DC, PEMF
Ultrasound– SAFHS, Lithotripter fields
Laser– Invasive, experimental
Mechanical– Dynamic loading of external fixation, vibration

Biochemical MechanismsBiochemical Mechanisms
CCEFCMFPEMF
At the cell/tissue level, considerthese different techniques to besimilar to biophysical stimuliWhat might be the commonmechanism(s) underlying thecell/tissue level response?

Common Biologic StimulantsCommon Biologic Stimulants
Insulin-like growth factor (IGF)Transforming growth factor-beta (TGF-B)Platelet-derived growth factor (PDGF)Fibroblast growth factor (FGF)Bone morphogenic protein 2 (BMP-2)Bone morphogenic protein 7 (BMP-7)

Bone formation:Growth factorsenhance boneECM formation
Bone formation:Growth factorsenhance boneECM formation
Biological Stimulants in Bone FormationBiological Stimulants in Bone Formation
2. BiologicalStimulants
Growth factor effect on bone formation
Osteoprogenitors Pre-osteob last Osteoblast Osteocyte
Pro liferationphase
Differentiationphase
Matrix formationphase
Chemotaxis: Growthfactors attract progenitors
Chemotaxis: Growthfactors attract progenitors
Differentiation:Growth factors
increasediffe rentiation
rates
Differentiation:Growth factors
increasediffe rentiation
rates
Proliferation:Growth factors
enhanceprol ifera tion rates
Proliferation:Growth factors
enhanceprol ifera tion rates

Osteocytes
• REMEMBER - Once and osteoblast surrounds itself with that organic substance called the matrix it becomes and osteocyte. The osteocytes then extend cytoplasmic processes to connect to neighboring osteocytes. BONE FORMATION

IGF-IIIGF-II
Magnetic Field
1) Increased IGF-II Production2) Increased IGF-II Receptor Expression3) Increased Cell Proliferation
Amplification Cascade
IGF-II
IGF-II
IGF-II
IGF-II
IGF-II
IGF-II
IGF-II
IGF-II
IGF-II
IGF-II
IGF-II
IGF-II
Growth Factor StudiesGrowth Factor Studies
CMF Effects on Osteoblasts
• Fitzsimmons, et al, 1995 ^IGF-II• Fitzsimmons, et al, 1995 ^IGF-II• Fitzsimmons, et al, 1994 ^Ca Flux• Ryaby, et al, 1994 ^IGF-II in Fx• Callus

Educational Purposes Only. Do Not Copy or Distribute.
GF Receptors
Growth Factors (i.e. IGFs)
Growth Factor Model


Educational Purposes Only. Do Not Copy or Distribute.
CMF Signal DifferentiationCMF Signal Differentiation
ITS DIFFERENT!!!
1990’s OrthoLogic TechnologyCMF ( ombined agnetic ield)C M F
Mag
netic
Fie
ld
Mag
netic
Fie
ld
0
0
20
20
(Gau
ss)
(Gau
ss)
Mag
netic
Fie
ld
T
Educational Purposes Only. Do Not Copy or Distribute.
Pulsed Magnetic Fields Improve Osteoblast ActivityPulsed Magnetic Fields Improve Osteoblast ActivityDuring the Repair of an Experimental Osseous DefectDuring the Repair of an Experimental Osseous Defect
Cane et al. (1993) Cane et al. (1993) J. Orthop. Res.J. Orthop. Res. 11:664-670 11:664-670
• Transcortical holes in horses
• 75 Hz PEMF continuous for 30 days
• Histomorphometric analysis (BV% andMAR)
• > 2-fold increase in TBV (p<.01) and MAR(p<.001) with PEMF exposure

Educational Purposes Only. Do Not Copy or Distribute.
Pulsed Magnetic Fields Improve Osteoblast ActivityPulsed Magnetic Fields Improve Osteoblast ActivityDuring the Repair of an Experimental Osseous DefectDuring the Repair of an Experimental Osseous Defect
Cane et al. (1993) Cane et al. (1993) J. Orthop. Res.J. Orthop. Res. 11:664-670 11:664-670

Educational Purposes Only. Do Not Copy or Distribute.
PEMF – PMA Study (EBI)PEMF – PMA Study (EBI)
• 146 nonunions
• > 9 months post injury
• 2.3 average number of prior surgeries
• 63.5% efficacy in 115 patients @ long term(4 year) follow-up
• 8 – 10 hours/day


CMF TechnologyCMF Technology
Frequency within theoptimal range for bonestimulation (<150 Hz)– AC (Sine Wave)
• Frequency: 76.6 Hz• .2-.4 gauss
– DC (Static Field)• .2 gauss

XTM Tibial Analysis Site
•Synchrotron-based x-ray tomographic microscopy
CMF Reversal of OVX-osteopeniaCMF Reversal of OVX-osteopenia•Direct calculation oftrabecular bonecompressivemodulus by FEM

CMF Effect on Growth Factor ProductionRat Spine Fusion Model
CMF Effect on Growth Factor ProductionRat Spine Fusion Model
0
10
20
30
40
PCR
Pro
duct
s (n
g)
IGF-1 CONT
IGF-1 CMF BMP-7CONT
BMP-7 CMF BMP-2CONT
BMP-2 CMF

OL1000 Clinical StudyOL1000 Clinical Study
The “Gold Standard” Clinical Study– Strict entrance criteria– Rigorous endpoint– Independent radiographic verification– No forced adjunctive treatment

OL1000 Clinical StudyOL1000 Clinical Study
Entrance Criteria– Nonunion (trauma)– >9 months post-injury– No surgery prior 3 months– No radiographic evidence of healing for prior 3 months
• Independent, blinded panel verification
Study Participants– 112 patients with 116 nonunions– 29.3 months mean time since initial injury
• Range from 8.5 months to 256.0 months– 2.5 mean number of prior surgeries
• Range from 0 to 11

OL1000 Clinical StudyOL1000 Clinical Study
Healed Criteria– Clinically
• No pain or motion at the fracture site– Radiographically
• 3 of 4 cortices bridged• Independent, blinded panel verification

OL1000 Clinical Study ResultsOL1000 Clinical Study Results
Two Reference Points1) Original Study2) Original Long-term Follow-up
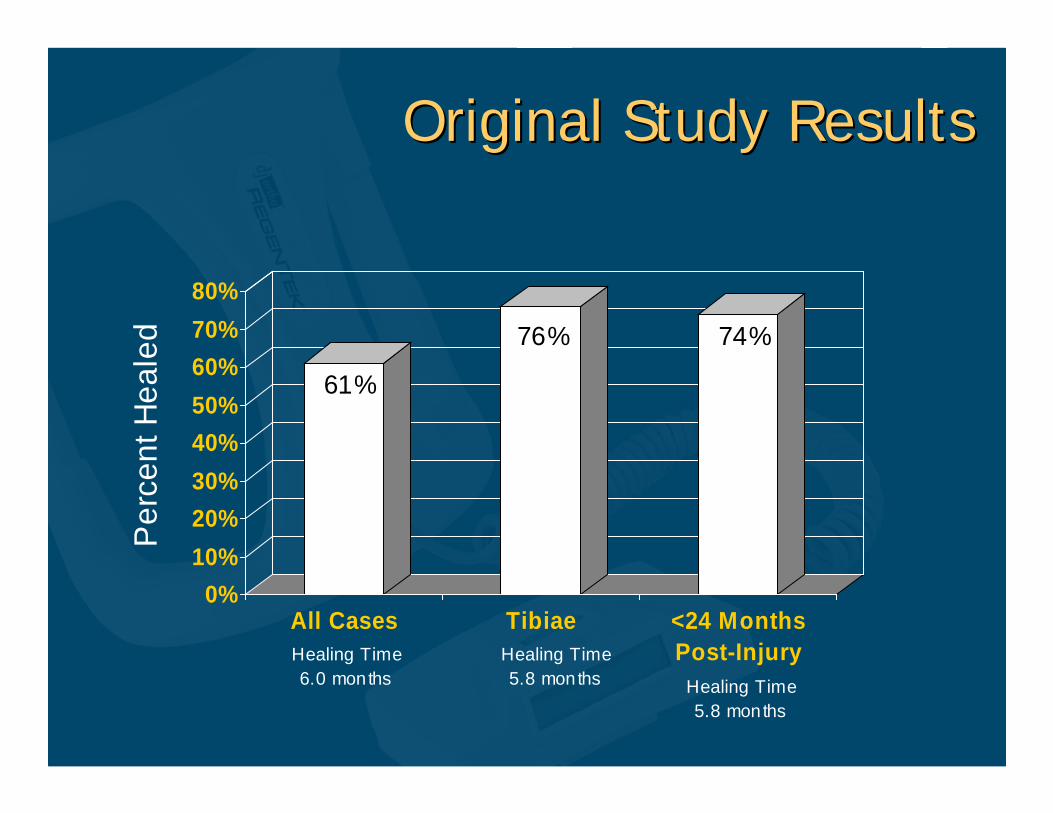
Original Study ResultsOriginal Study Results
0%10%20%30%40%50%60%70%80%
All Cases Tibiae <24 MonthsPost-Injury
Per
cent
Hea
led
61%
76% 74%
Healing Time6.0 months
Healing Time5.8 months Healing Time
5.8 months

Long-Term Follow-upLong-Term Follow-up
All patients (100%) remained healed at aminimum of two years post-treatmentfollow-up– 10% drop-outOL1000 is the only BGS that did not haveefficacy results downgraded at long-termfollow-up

dj Ortho Regentek™ OL1000dj Ortho Regentek™ OL1000
CMF technology– Combined Magnetic Field
30 minutes per dayLightweightNoninvasiveOne-button operation


Bone Stimulators
• When do you use a Bone Stimulator on a fracture with an athlete??????


Stress Fractures
• SIMPLY - Failure of the normal reparative process of bone to keep pace with the microtrauma or stresses of activity.
• Osteoblastic activity can not keep up with ostoclastic activity or the break down of bone due to some sort of trauma.

Stress Fractures
• TIBIA = The most common site of Stress Fractures in athletes accounting for up to 50% in some literature.
• Stress Fractures in the Athlete, Monteleone, G, Orthopedic Clinics of N America, 1995.

Fifth Metatarsal
• Jones Fracture - Fracture involving the metaphysial-diaphysial junction. Intra-articular involving 4th and 5th metatarsals.
• Avulsion Fractures - Lateral band of the Plantar Aponeurosis, Richi, WR, Rosenthal, DJ, 1984.
• Diaphysial Stress Fractures - Involves the proximal 1.5 cm of metatarsal.

Fifth Metatarsal
• The blood supply to the fifth metatarsal is identical to most other tubular bones.
• Nutrient artery to shaft.• Metaphysial and epiphysial arteries to the
base and tuberosity.
• Shereff, MJ., 1991 and Smith, JW., 1992

Fifth Metatarsal
• Periosteal plexus provides blood to the periosteum and the cortical bone.
• Large extraosseous vascular plexus is adjacent to the intermetatarsal articulation.
• Shereff, MJ., et al, Foot and Ankle, 350-353, 1991.

Treatment of Stress Fractures
• 1. Decrease or Stop Activity with or without immobilization
• 2. Treat the inflammatory condition• 3. Correct the biomechanical etiology
• CAN WE DO MORE TO FACILITATE THE RETURN TO PLAY?

Calendar Year
• January to December
• Average 12 Months

College Athletics
• Football Season - August to January• Hockey Season - September to March• Track and Field Season - March to June
• Average - 5.6 Months


Educational Purposes Only. Do Not Copy or Distribute.
SummarySummary
• Physical stimulation affects bone repair in wellcontrolled human clinical trials
• Cell/tissue level mechanism may be due tostimulation of local growth factor biosynthesis
• Many questions remain unanswered at theclinical level, specifically patient outcomes

Educational Purposes Only. Do Not Copy or Distribute.
SummarySummary
• Comparable efficacy for most of the EMF/UStechnologies
Newer technologies (CMF and US) have:
• Improved patient compliance due to reduceddaily treatment time
–Non-contact vs. contact mode–Portability
