the use of fiberoptic bronchoscopy during percutaneous...
TRANSCRIPT
Diagnostic and Therapeutic Endoscopy, Vol. 4, pp. 13-18Reprints available directly from the publisherPhotocopying permitted by license only
(C) 1997 OPA (Overseas Publishers Association)Amsterdam B.V. Published in The Netherlands
by Harwood Academic PublishersPrinted in Singapore
The Use of Fiberoptic Bronchoscopy During PercutaneousDilatational Tracheostomy with Laryngeal Mask
MAURIZIO ROSSI a, MARCO DE MONTIb’*, DAVIDE SONNINO and BRUNO GIACOMETTI
alntensive Care Unit, General Hospital of Menaggio, 22017 (Como), Italy; bS.S.U.E.m.ll8 (Italian Emergency Medical Service)of Menaggio, 22017 (Como), Italy; CDepartment of General Surgery, General Hospital of Menaggio, 22017 (Como), Italy
(Received 18 September 1996; Revised 12 February 1997; In finalform 27 February 1997)
The aim of our research is to evaluate the advantage by the combined use of fiberopticbronchoscopy and laryngeal mask during the performance of percutaneous dilatationaltracheostomy in an intensive care unit.
Patients: 16 adult patients who were candidates to middle-long term mechanicalventilation.
Environment: Intensive Care Unit of a Community General Hospital.Results: We experienced 3 minor complications (2 minor bleedings and 1 neck emphy-
sema). Difficulties were found in 3 patients with particular anatomical conformation(obese patients with short neck and limited mobility of the cervical spine).
Conclusion: The combined use of fiberoptic tracheo-bronchoscopy with the laryngealmask permits a better endoscopic visualisation of the operatory field, providing a moresecure and precise procedure.
Keywords: Percutaneous dilatational tracheostomy, Fiberoptic tracheo-bronchoscopy, Laryngealmask
INTRODUCTION
Methods of percutaneous dilatational tracheo-stomy, originally described by Ciaglia in 1985 [1],and similar techniques, are having a wideemployment in intensive care in comparison withthe classic surgical tracheostomy. The global inci-dence of complications in the scientific literaturefor the classic technique is about 22% [2-8].Complications mainly include: stomal infections,
stomal granulomas, major bleedings, and sub-cutaneous emphysema.However, employing the percutaneous techni-
que, these same complications only reach a 12%global incidence, with a greatly reduced rate of sto-mal infections. Additionally, the percutaneous tra-
cheotomy has some significant advantages such as:
(a) feasibility of the operation at the patient’sbedside in the Intensive Care Unit;
*Corresponding author. Via Derna 5, 1-20132 Milano, ITALY. Tel.: + 39 2 26 11 13 44, + 39 330 23 05 55.Fax: / 39 344 30596.
13

14 M. ROSSI et al.
(b) low learning curve due to ease of procedure; years old. The SAPS II average value was 49.9,(c) operatory room cost savings; ranging between 21 and 75.(d) short length of procedure. The global mortality rate during the hospital
stay was 56%, out of which 37.5% (6 patients)The introduction of endoscopic guides, first in the Intensive Care Unit. However, no death
suggested by Marelli and associated in 1990 was related to complications due to percutaneous[9,10] and followed by other Authors [11], repre- dilatational tracheostomy.sented an improvement of the original technique The following pathologies were observed: 10and caused a further reduction of complications patients were affected by reacute chronic obstruc-related to tracheostomy, tive bronchopneumonopathy, with pneumonia in
In fact, endoscopic vision permits a precise 5 of these patients; 2 patients were affected byvisualisation of the dilators and tracheostomy intraparenchymatous brain haemorrhage; 3 pa-tube, and allows an immediate correction of tients were affected by a septic state caused byimproper accesses or procedures such as para- surgical pathologies (perforated gastric ulcer; livermedian needle insertion, carcinoma; perforated empyema of the gallblad-
In our experience with the fiberoptic broncho- der). The last patient had an acute respiratoryscope we also employed the laryngeal mask, as failure due to a cardiogenic shock following anpreviously described by Dexter [12] and Tarpey infarction. In average, we performed percutaneous[13], in order to reduce several disadvantages dilatational tracheostomy on the 10th day of ad-associated with the classic procedure, which mittance, ranging between one and twenty days.included difficulty in maintaining the endotra- The average time of the operation was aboutcheal tube in the correct position, and problems 17 min, ranging from a minimum of 10 min forrelated to the relative pressure of the endotra- patients with favourable anatomical conditionscheal tube cuff, positioned immediately proximal to a maximum of about 25 min for obeseto the vocal cords, on the larynx and on the patients with short and less mobile necks.same vocal cords, sometimes damaging these The percutaneous dilatational tracheostomystructures. The laryngeal mask permits, indeed, a was performed at the bedside of the patient bymore clear endoscopic vision of the operatory two doctors of the Intensive Care Unit: onefield in comparison to introducing the scope doctor performed the operation and the otherthrough the endotracheal tube. managed the anaesthesia and particularly drugs,
ventilation, and the correct positioning of thelaryngeal mask. The procedure was also followedby two graduate nurses. The use of fiberoptic
PATIENTS AND METHODS bronchoscope allowed everybody to follow theentire operation on the monitor, permitting a
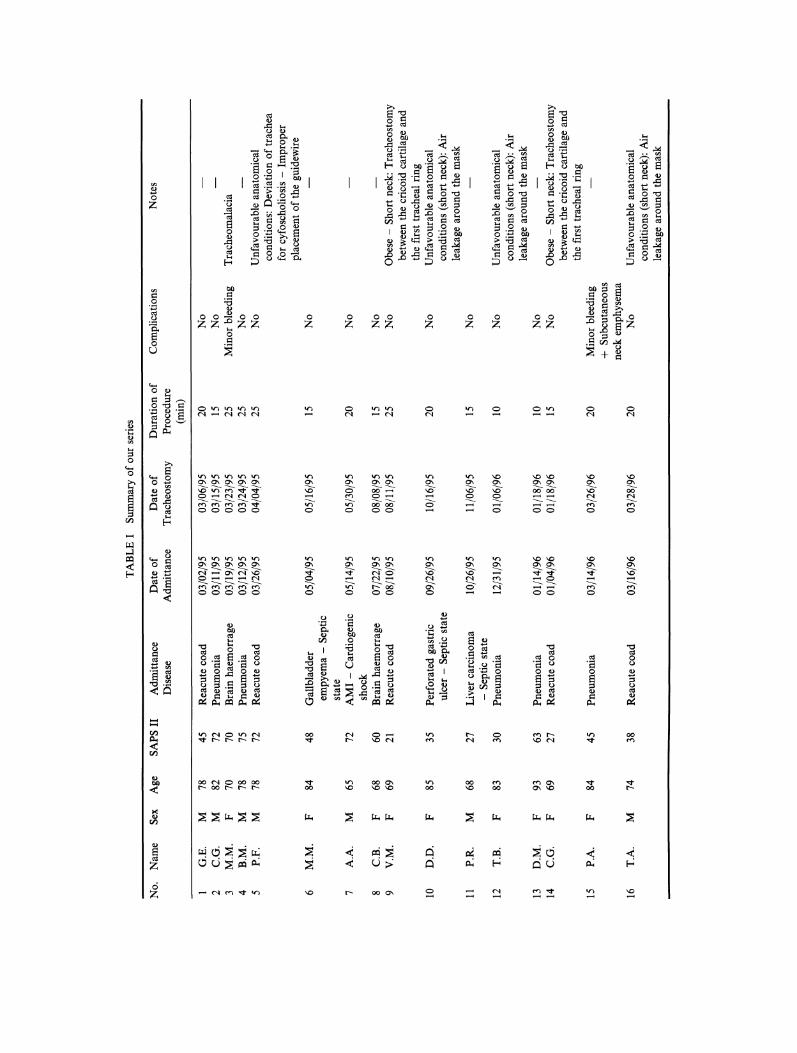
From March 1995 to March 1996 in the Inten- wide participation.sive Care Unit of the Community General Hos- The operation was performed in intravenouspital of Menaggio (Como) 16 percutaneous general anaesthesia. Primary anaesthesia wasdilatational tracheostomy were performed in obtained with propofol 2mg/kg and fentanylpatients candidate to middle-long term mechani- 0.05-0.1 mg; maintenance with propofol 1-3 mg/cal ventilation. Data regarding our series are kg/h, pancuronium 0.8mg/kg. Patients wereshown in Table I. ventilated via a Siemens 900 C until the laryngealOf the 16 patients included in our series, 9 mask was positioned.
were females (56%) and 7 were males (44%), the The ventilation was led in the following way:average age was 77, ranging between 65 and 93 CPPV, TV of 7 ml/kg, FiO2: 1.0.
o oo
o o o 0Z Z ZZ
o o 0 o
0
16 M. ROSSI et al.
We monitored blood’s saturation by a pulse tional tracheostomy was performed following theoximetry (DATEX SATLITE trans), non- schema described by Ciaglia [7]. The neck, par-invasive arterial pressure (COLIN PRESS- tially hyperextended, is prepared with a disinfec-MATE BP 8800), and the electric cardiac activity tant solution and the operatory field surrounded(SOXIL SENTINEL 2A). with sterile linen.We used Ciaglia’s kit for percutaneous tra- Cutis is infiltrated with lidocaine idrocloridate
cheostomy (COOK CRITICAL CARE), a flex- 1% with adrenaline (1:200.000)from the cricoidible fiberoptic bronchoscopy (Olympus BF type margin to the third tracheal ring, in order to3C30 OES Bronchofiberscope) and the laryngeal avoid bleeding from cutaneous and subcutaneousmask n.4 (INTAVENT). layers. A 0.5-1 cm vertical incision of cutis andUnder the direct vision of the laryngoscopy, subcutis is performed, avoiding damage to blood
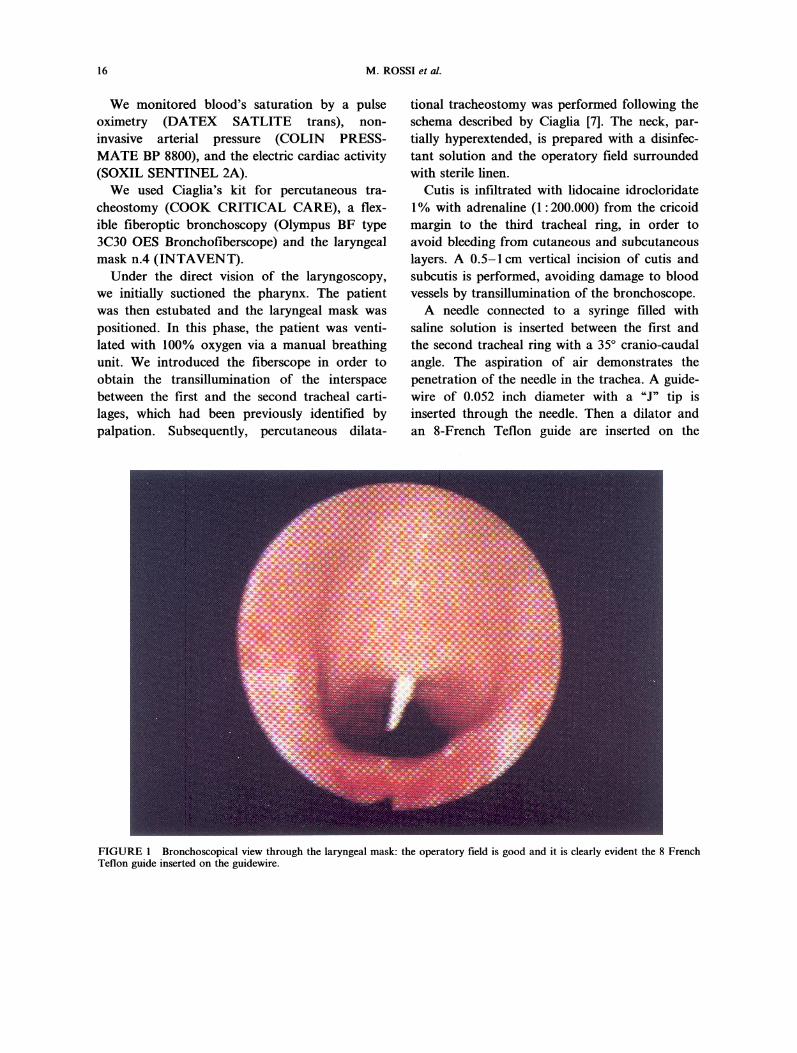
we initially suctioned the pharynx. The patient vessels by transillumination of the bronchoscope.was then estubated and the laryngeal mask was A needle connected to a syringe filled withpositioned. In this phase, the patient was venti- saline solution is inserted between the first andlated with 100% oxygen via a manual breathing the second tracheal ring with a 35 cranio-caudalunit. We introduced the fiberscope in order to angle. The aspiration of air demonstrates theobtain the transillumination of the interspace penetration of the needle in the trachea. A guide-between the first and the second tracheal carti- wire of 0.052 inch diameter with a "J" tip islages, which had been previously identified by inserted through the needle. Then a dilator andpalpation. Subsequently, percutaneous dilata- an 8-French Teflon guide are inserted on the
FIGURE Bronchoscopical view through the laryngeal mask: the operatory field is good and it is clearly evident the 8 FrenchTeflon guide inserted on the guidewire.
THE USE OF FIBEROPTIC BRONCHOSCOPY 17
guidewire in order to make the system rigid(Fig. 1). The guide has a small ring on the distalend in order to avoid damages by the dilators,especially to the posterior wall of the trachea.
Next, dilators from 12 to 36 French are
inserted on the guide.When the required dilatation is obtained, a 7,
8, or 9mm diameter tracheostomy tube is insert-ed, using a smaller dilator as a guide. Subse-quently, the double guide is removed and thetube can be cuffed.
RESULTS AND CONCLUSIONS
Data reported in literature, as previouslydescribed, demonstrates that most common com-plications following percutaneous tracheotomyinclude: subcutaneous emphysema, bleedings,stomal infections, difficulties in tracheostomytube insertion and paramedian insertions. Globalincidence of complications is about 12%. Ourexperience does not significantly differ from theseresults, and particularly, the complications whichoccurred in our patients are described in Table II.
We globally had 3 minor complications, andparticularly two cases of minor bleeding stoppedonly by the compression obtained with the tra-cheostomy tube, and one case of subcutaneousemphysema of the neck which spontaneouslyhealed in a few days.By employing the fiberoptic bronchoscopy and
the laryngeal mask we avoided incorrect intro-duction of the dilators, as we were able to correctany improper placement of the guidewire.The difficulties we encountered always
occurred in patients with unfavourable anatomi-cal conditions (obese patients with short neckand limited mobility of the cervical spine), whichdo not appear ideally suited for this procedure.
In two of these patients, it was necessary toperform the tracheostomy between the cricoidcartilage and the first tracheal ring. In these twoas well as one other patient, we found severaldifficulties in maintaining the laryngeal mask inthe correct position, but were always able tocomplete the procedure.
Notwithstanding several other reports [12], inour series all patients had a nasogastric tube butwe didn’t have any noticeable leakage around the
TABLE II Complications and difficulties occurred during the procedure
Complications No.
Minor bleedingMajor bleeding (Blood transfusions)Inflammatory infiltrateDamage of posterior tracheal wallParamedian placement of the guidewire (Corrected underendoscopic vision)PneumotoraxSubcutaneous neck emphysemaDeaths related to the procedure
TOTAL
2NoNoNo(2)
No
No
3/16 (18%)
Difficulties No.
Tracheostomy performed between the cricoid cartilage 2and the first tracheal ring
Air leakage around the mask
TOTAL
Obese patients with short neck and limited mobility of the cervical spine.
3
5/16(31%)

18 M. ROSSI et al.
laryngeal mask attributable to it; in three cases themask leakage has been ascribed to unfavourableanatomical conditions (obesity and short neck).
Other Authors [14] evidenced that laryngealmask could be dangerous due to the possibilityof aspiration pneumonia: in our experience-thisevidence is not justified since we perform percu-taneous dilatational tracheostomy only in electivepatients and never in emergency, which is adifferent approach compared to other publishedliterature [1 5].We can conclude that the use of fiberoptic
bronchoscopy with the laryngeal mask facilitatesthe performance of the Ciaglia’s percutaneousdilatational tracheostomy. Particularly, endo-scopic vision of the operatory field offered bylaryngeal mask is greatly improved compared toinsertion the instrument through the endotra-cheal tube.
Furthermore, the connection of the scope to amonitor allows the operator and his team to fol-low every step of the operation and perform theprocedure with a greater safe and coordination.
References
[1] Ciaglia, P., Firsching, R. and Syniec, C. Elective percuta-neous dilational tracheostomy: a new simple bedside pro-cedure; preliminary report. Chest 1985; 87: 715-9.
[2] Rosi, R., De Gaudio, A.R. and Frova, G. Complicanzeimmediate delle tecniche di tracheostomia percutanea.Anestes Rianim Intens 1994; 15: 316-22.
[3] Ciaglia, P. and Graniero, K.D. Percutaneous dilationaltracheostomy: Results and long term follow up. Chest1992; 101: 464-7.
[4]
[5]
[61
[7]
[81
[9]
[10]
[11]
[12]
[131
[]
[15]
Grigs, W.M., Myburgh, J.A. and Worthley, L.I. A pro-spective comparison of a percutaneous tracheostomytechnique with standard surgical tracheostomy. IntensiveCare Med. 1991; 17: 261-3.Bodenham, A., Diament, R., Cohen, A. and Webster, N.Percutaneous dilational tracheostomy. A bedside proce-dure on the intensive care unit. Anaesthesia 1991; 46:570-2.Hazard, P., Jones, C. and Benitone, J. Comparative clinicaltrial of standard operative tracheostomy with percuta-neous tracheostomy. Crit. Care. Med. 1991; 19: 1018-24.Heffner, J.E., Miller, K.S. and Sahn, S.A. Tracheostomyin the intensive care unit. Part 2: Complications. Chest1986; 90: 430-6.Meade, J.W. Tracheostomy its complications and theirmanagement a study of 212 cases. N. Eng. J. Med.1961; 265: 519-523.Marelli, D., Paul, A., Manolidis, S., Walsh, G., Odim,J.N.K., Burdon, T.A., Shennib, H., Vestweber, K.H.,Fleiszer, D.M. and Mulder, D.S. Endoscopic guided per-cutaneous tracheostomy: early results of a consecutivetrial. J. Trauma 1990; 311: 433-5.Paul, A., Marelli, D., Chiu, C.J., Vestweber, K.H. andMulder, D.S. Percutaneous endoscopic tracheostomy.Ann. Thoracic Surg. 1989; 47: 314-315.Winkler, W.B., Karnik, R., Seelmann, O., Havlicek, J.and Slany, J. Bedside percutaneous dilatational tra-cheostomy with endoscopic guidance: experience with 71ICU patients. Intensive Care Med. 1994; 211: 476-479.Dexter, T.J. The laryngeal mask airway: a method toimprove visualisation of the trachea and larynx duringfibreoptic assisted percutaneous tracheostomy. Anaesth.Int. Care. 1994; 22: 35-39.Tarpey, J.J., Lynch, L. and Hart, S. The use of the lar-yngeal mask airway to facilitate the insertion of a percu-taneous tracheostomy. Intensive Care Med. 1994; 211:448-449.Barker, P., Langton, J., Murphy, P. and Rowbotham, D.Regurgitation of gastric contents during general anaes-thesia using the laryngeal mask airway. Br. J. Anaesth.1992; 69: 314-315.Lyons, B.J. and Flynn, C.G.M. The laryngeal mask sim-plifies airway management during percutaneous dila-tional tracheostomy. Acta Anaesthesiol. Scand. 1995; 39:414-415.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com