the wide awake approach to ulnar nerve entrapment: … awake hand surgery enables treatment in one...
TRANSCRIPT
Research study
Page 1 of 5
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f Int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t. A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Bismil QMK, Lowe S, Viner L, Bismil MSK. The wide-awake approach to ulnar nerve entrapment: results of an integrated one-stop wide-awake surgical pathway. OA Case Reports 2013 Jun 21;2(5):44.
The wide awake approach to ulnar nerve entrapment: results of an integrated one stop wide awake surgical pathway
QMK Bismil1*, S Lowe2, L Viner3, MSK Bismil4
AbstractIntroductionThe wide awake approach to hand surgery is gaining increasing popu-larity worldwide, but PubMed search does not reveal any publications on wide awake ulnar nerve surgery. In this research study, we describe our surgical experience, techniques and results of the wide awake management of ulnar nerve entrapment at both elbow and wrist. This study is based on a background of having established the world’s first totally one stop wide awake (OSWA) hand surgery service, with published outcomes.Materials and methodsWe performed a retrospective review of our 2011/12 ulnar nerve entrap-ment cases, which comprised 40 patients with ulnar nerve dysfunction.ResultsThe main outcome measures were sensorimotor improvement, including improvement of the Quick-DASH score, patient satisfaction and cost-effectiveness and efficiency. DiscussionNo surgical complications were expe-rienced by the patients and all of them were satisfied with their treat-ment. All patients were followed-up to a good outcome including objective
sensorimotor improvement in ulnar nerve function.ConclusionThe wide awake approach to ulnar nerve decompression is safe, effec-tive and comparable to the historical approach; and is amenable to a one stop patient pathway.
IntroductionWide awake hand surgery enables treatment in one management stop, through a patient-centric pathway, which is broadly more akin to dental treatment than a traditional multi-stop surgical approach. The one stop wide awake (OSWA) hand surgery service is now well-described in the worldwide published literature1,2. Wide awake hand surgery, is hand surgery, without general anaesthesia or regional anaesthesia or sedation or tourniquets. There have been great advances in the technique(s) for hand surgery, over the last decade. It is now over 30 years, since the first peer reviewed publications on wide awake hand surgery3, and despite inherent potential advan-tages (lower risk, a more convenient pathway for the patient and cost-savings for national state-funded healthcare)1,2, the worldwide transi-tion to the technique has been slow, according to the published litera-ture1–22. The published literature on ulnar nerve compression/decom-pression, reflects that there are two encouraging case series, each comprising 20 cases, which were performed using a local anaesthetic technique in 2001 and 198223,24. However, a contemporaneous search on PubMed for the relevant terms is instructive: Ulnar Nerve and Local An(a)esthesia or local an(a)esthetic; or wide awake ulnar nerve; or wide
awake cubital tunnel; or wide awake ulnar tunnel; or ulnar nerve entrap-ment. This demonstrates that there has been little recent progress with wide awake ulnar nerve surgery as would have been expected; despite the recent advances with wide awake hand surgery. There is no previous description of an all-encompassing or totally OSWA surgical pathway for the totality of ulnar nerve entrap-ment, irrespective of site. The aim of this research study was to discuss the wide awake approach to ulnar nerve entrapment, which we have pioneered in the UK.
Materials and methodsAll the patients in this study were managed according to the OSWA ulnar nerve entrapment pathway, with a clinical diagnosis of unilat-eral isolated ulnar nerve dysfunction (Figure 1).
Clinical evaluationThe conduction of clinical evaluation included the following:
History: Sensorimotor ulnar nerve dysfunction distal was observed on the site of entrapment.
Biro Test: Sympathetic dysfunction resulted in reduced sweating in little (ulnar nerve) versus index (median nerve) pulp biro slides more easily on affected digits.
Scratch Collapse Test: The patient was asked to resist bilateral shoulder external rotation, with the elbows fully flexed. The area of suspected ulnar nerve compression was then lightly scratched and then resisted shoulder external rotation was immediately repeated. In ulnar nerve dysfunction, there was momentary loss of shoulder external rotation resistance on the affected side.
Traum
a &
Ort
hopaedic
s
Corresponding authorEmail: [email protected] 1 Consultant Orthopaedic Surgeon, Queen Anne
Street Medical Centre, 18-22 Queen Anne Street, Off Harley Street, London, W1G 8HU
2 General Practitioner, Westside Surgery, Slea-ford Road, Boston, PE21 8EG
3 Director, Turnpike Medical Wide Awake Or-thopaedic Surgery, Horncastle Road, Louth, Lincolnshire, LN11 9QT
4 Consultant Orthopaedic Surgeon, Expert-Orthopaedics.Com Ltd. 2, Allington Garden, Boston, Lincolnshire, PE21 9DP

Research study
Page 2 of 5
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Bismil QMK, Lowe S, Viner L, Bismil MSK. The wide-awake approach to ulnar nerve entrapment: results of an integrated one-stop wide-awake surgical pathway. OA Case Reports 2013 Jun 21;2(5):44.
Tinel’s Test: The ulnar nerve irri-tability was reproduced by percus-sion over the cubital or ulnar tunnel.
Surgery was performed under local anaesthesia using a lignocaine (lidocaine) and low-dose adrenaline mix, with no tourniquet. A tourniquet on the upper arm was painful for the wide awake patient and would encroach upon the surgical field for proximal operations. In our experi-ence of wide awake surgery, metic-ulous dissection enabled surgery without diathermy. The standard for ulnar nerve surgery was 10 ml of 2% lignocaine, with adrenaline 1:200,000, which was drawn up, with a 21-gauge needle and infiltrated with a 25-gauge needle.
Cubital tunnel decompression technique (proximal)The following steps were followed in this technique, also see Table 1: 1. The patient lied down in supine
position.2. Surgical marking positioning
was done as depicted in Figure 2. The following were the findings observed for this surgical mark:
a. Double sandbag was large at base, smaller on top and tucked into axilla.
b. Shoulder abduction was at 60°.
Figure 1: OSWA Ulnar Nerve Pathway.
Figure 2: Cubital Tunnel Release Positioning.
Figure 3: Cubital Tunnel Release Intraoperative.
Table 1. Keys to successful one stop wide awake management (adapted from original OSWA paper1).
No tourniquets Too painful for the pati ent for complex surgery. Unnecessary. A tourniquet for cubital tunnel syndrome interferes with access to the cubital tunnel.
Local anaestheti c technique: 2% lignocaine with adrenaline 1:200,000. Plain lignocaine for digits.Infi ltrate in theatre prior to scrub to allow anaestheti c to work.
Careful surgical dissecti on and meti culous technique Point bleeding managed with pressure from rolled small swab.
Experienced, small team with clear and defi ned roles Simple health questi onnaire fi lled up online by pati ent Pre-consultati on informati on provided at www.oswa.me Focused consultati on with thorough discussion of pros versus cons and risks versus benefi ts of treatment opti ons.
Compact functi onal outpati ents and theatre space enabling easy, safe and eff ecti ve pati ent fl ow.
Effi cient, thorough evidence-based treatment with robust audit and governance faciliti es/mechanisms/processes.
Research study
Page 3 of 5
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f Int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t. A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Bismil QMK, Lowe S, Viner L, Bismil MSK. The wide-awake approach to ulnar nerve entrapment: results of an integrated one-stop wide-awake surgical pathway. OA Case Reports 2013 Jun 21;2(5):44.
c. External rotation was maximal. d. Mark was epicondyle/condyle. e. Curvilinear incision was guided
by palpation of the nerve and in relation to the medial epicondyle.
3. Locate the nerve on proximal forearm.
4. Decompress cubital tunnel full-length nerve hook should pass easily around the nerve (Figure 3).
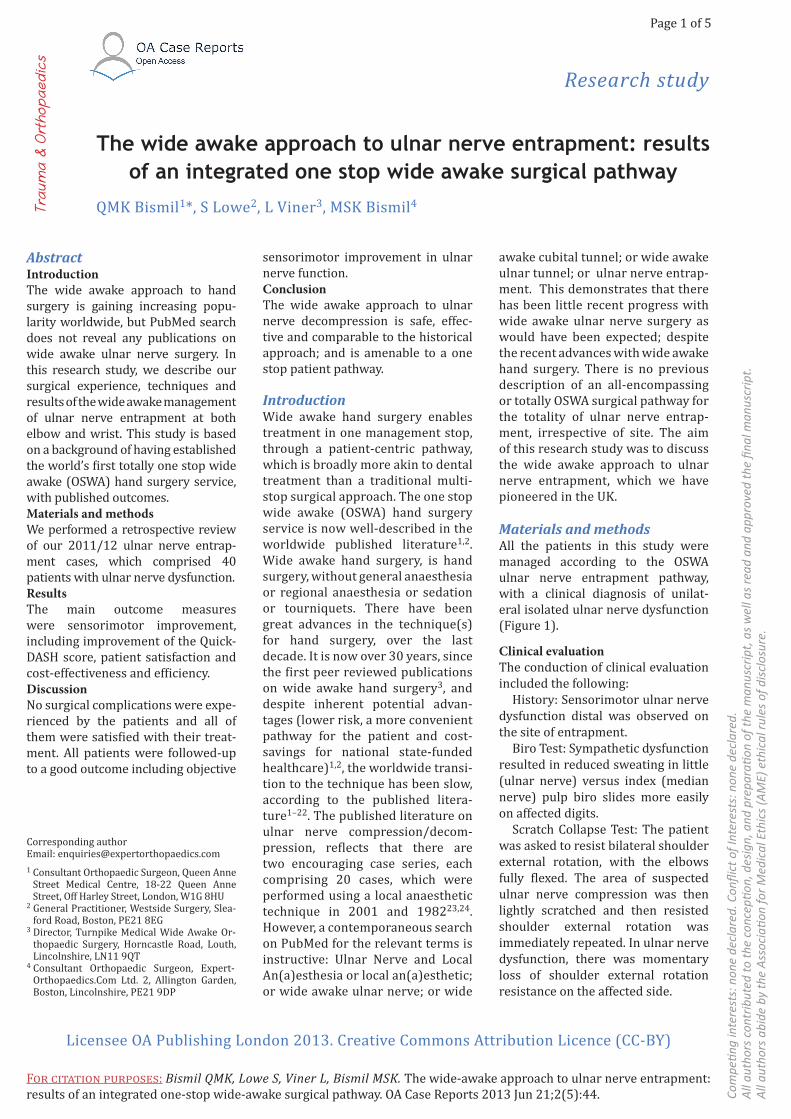
Ulnar tunnel (distal) decompression techniqueThe following steps were adhered to in this technique, also see Table 2:1. The patient was positioned supine.2. Forearm of the patient was supi-
nated on arm table.3. Palpate the pisiform and flexor carpi
ulnaris (FCU) as shown in Figure 4.4. Longitudinal incision was made
over the FCU as shown in Figure 5.5. Locate the ulnar nerve in relation
to the FCU, mobilise the FCU and identify ulnar nerve and protect ulnar artery (Figure 6).
6. Decompress the entirety of the ulnar tunnel.
At the OSWA service we operate continuous audit processes. All patients were requested to contact us immediately in case of any problems. For the purposes of this audit, all patients were seen once by the orthopaedic surgeon in the clinic. Online follow-up was then continued for at least three months post-surgery.
ResultsResults of wide awake ulnar nerve pathwayThe protocol for the one stop wide awake ulnar nerve pathway is
Figure 4: Ulnar Tunnel Release Step 1. Figure 5: Ulnar Tunnel Release Step 2. Figure 6: Ulnar Tunnel Release Step 3.
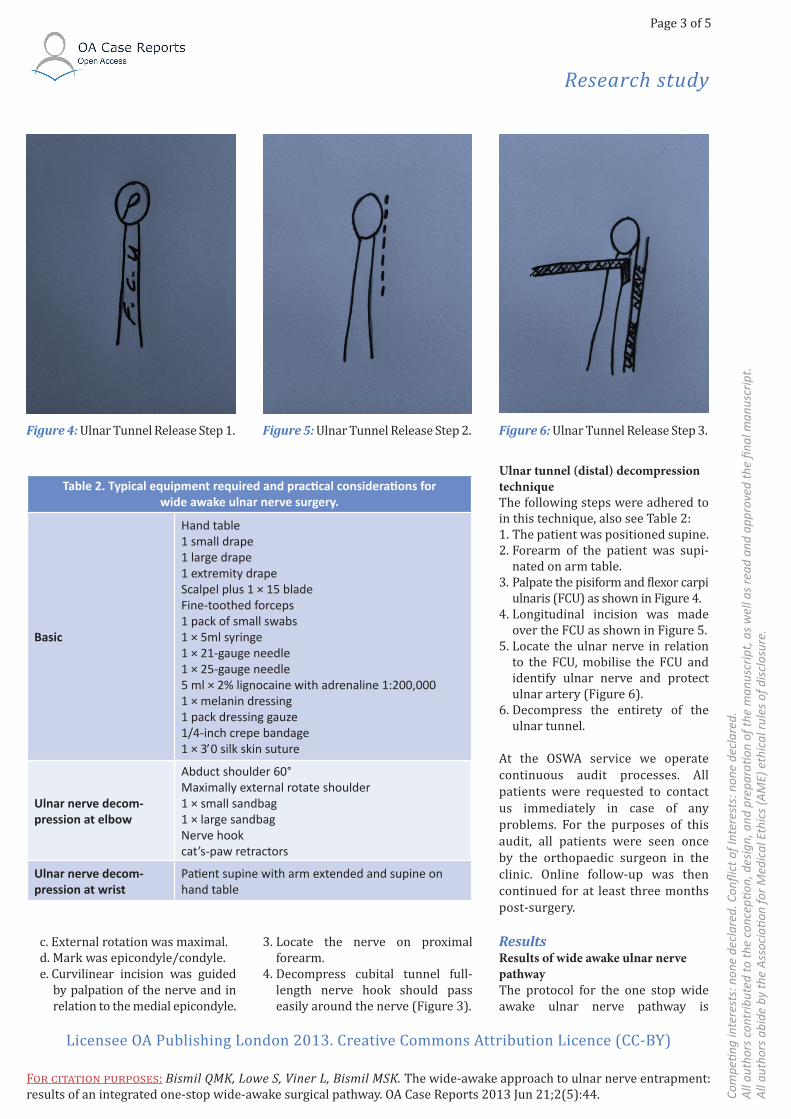
Table 2. Typical equipment required and practi cal considerati ons for wide awake ulnar nerve surgery.
Basic
Hand table1 small drape1 large drape1 extremity drapeScalpel plus 1 × 15 bladeFine-toothed forceps1 pack of small swabs1 × 5ml syringe1 × 21-gauge needle1 × 25-gauge needle5 ml × 2% lignocaine with adrenaline 1:200,000 1 × melanin dressing1 pack dressing gauze1/4-inch crepe bandage1 × 30 silk skin suture
Ulnar nerve decom-pression at elbow
Abduct shoulder 60°Maximally external rotate shoulder1 × small sandbag1 × large sandbagNerve hookcat’s-paw retractors
Ulnar nerve decom-pression at wrist
Pati ent supine with arm extended and supine on hand table

Research study
Page 4 of 5
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t.A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Bismil QMK, Lowe S, Viner L, Bismil MSK. The wide-awake approach to ulnar nerve entrapment: results of an integrated one-stop wide-awake surgical pathway. OA Case Reports 2013 Jun 21;2(5):44.
depicted in Figure 1. There were 40 cases of clinical ulnar nerve compression. Three injections (mild syndrome as per QuickDASH score) were administered. Thirty-seven operations (moderate to severe syndrome as per QuickDASH score) were performed, of these three oper-ations were ulnar tunnel decompres-sions and 34 operations were cubital tunnel decompressions. The cubital tunnel patients’ diagnoses were made clinically and the diagnosis was confirmed with nerve conduc-tion studies as required. The three ulnar tunnel syndrome cases were diagnosed clinically. Two of the ulnar tunnel patients previously had cubital tunnel release, with no improve-ment. There were no intra-operative surgical complications experience by the patients and there were no microbiologically-proven post-oper-ative infections. In all the patients, there were significant subjective and objective improvements in ulnar nerve sensorimotor function post-surgery, including improvements in the validated QuickDASH score.
All the patients were satisfied with the OSWA treatment pathway.
Surgery was provided to the National Health Service at around 50% of tariff.
Diagnostic tests and the OSWA ulnar nerve pathwayThe OSWA ulnar nerve pathway is depicted in Figure 1.
All patients were managed to a successful outcome through the OSWA ulnar nerve pathway, and nerve conduction studies did not affect the management. As part of the informed consent and the discussion of pros and cons and risks and bene-fits, all the patients were offered elec-trodiagnostic studies, but in this case series, these tests did not affect the management pathway in any case. All the patients who had undergone surgical treatment, showed posi-tive Ulnar Biro, Scratch Collapse and Tinel’s tests. In the ulnar tunnel
syndrome, there was irritability of the ulnar nerve in the ulnar tunnel rather than in the cubital tunnel, and sensorimotor dysfunction was distal to the site of compression.
DiscussionIt is now generally accepted that the standard procedure for ulnar nerve entrapment proximally in the cubital tunnel is simple decompression25, but more extensive surgery is also described in the literature. Distal entrapment in the ulnar tunnel is less well described, but in our experience it is not uncommon, and decompres-sion is the standard surgical proce-dure26. As per the recent paper by Hagert on wide awake treatment of (occult) proximal median nerve entrapment27: it is our experience that distal ulnar nerve entrapment may similarly be overlooked and is not usually detected on nerve conduction studies. Moreover, in the present series all the three cases of ulnar tunnel syndrome had a false negative nerve conduction study result for ulnar tunnel entrapment; and this has confounded the diag-nosis of their clinically obvious ulnar tunnel syndromes. This under-lines the general recognition in the literature that electrophysiology is a possible adjunct to thorough clin-ical assessment in peripheral nerve entrapment; but that these syndrome are essentially clinical diagnoses28.
In this research study, we describe a totally wide awake approach to ulnar nerve entrapment, irrespective of the site, and all management was performed in one discrete manage-ment stop. The wide awake hand surgery techniques we utilize enable optimisation of patient pathways. Through the wide awake approach, patients can be safely and effectively treated in one management stop1 and outside the main operating theatre5–7.
A wide awake injection technique using epinephrine is now standard worldwide4. A multitude of recent
studies have conclusively demon-strated that a wide awake injection technique using local anaesthesia with low-dose epinephrine is safe and effective. This refutes decades of surgical dogma1,2,9–13. The injection technique can be optimised to mini-mise the associated pain14.
The wide awake approach enables intra-operative optimisation, and as described by Lavyne and Bell in the original case series of local anaes-thetic surgery for cubital tunnel syndrome: the usual scenario is an immediate sensorimotor improve-ment on the surgical table; once the complete decompression has been performed. Feedback from the wide awake patient can therefore be used to optimise the surgery. Usually, this is the best guide to ensure that a complete decompression has been performed, but moreover, this can be a guide to fine tune the procedure with techniques, such as epineu-rotomy.
ConclusionWide Awake Hand Surgery (WAHS) techniques rebalance surgical risk: by eliminating the risks of general anaesthesia, regional anaesthesia, sedation and tourniquets; there is a rebalancing of risk for patients undergoing totally wide awake ulnar nerve decompression. The present audit demonstrated that a one stop wide awake (OSWA) approach to ulnar nerve entrapment is safe and effective, with high levels of patient satisfaction, and is efficient in terms of processes and cost-savings for state healthcare.
Abbreviations listFCU, flexor carpi ulnaris; OSWA, one stop wide awake.
References1. Bismil M, Bismil Q, Harding D, Harris P, Lamyman E, Sansby L. Transition to total one-stop wide-awake hand surgery service-audit: a retrospective review. JRSM Short Rep. 2012 Apr;3(4):23.

Research study
Page 5 of 5
Com
peti n
g in
tere
sts:
non
e de
clar
ed. C
onfl i
ct o
f Int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
ti on,
des
ign,
and
pre
parati o
n of
the
man
uscr
ipt,
as
wel
l as
read
and
app
rove
d th
e fi n
al m
anus
crip
t. A
ll au
thor
s ab
ide
by th
e A
ssoc
iati o
n fo
r Med
ical
Eth
ics
(AM
E) e
thic
al ru
les
of d
iscl
osur
e.
Licensee OA Publishing London 2013. Creative Commons Attribution Licence (CC-BY)
FOR CITATION PURPOSES: Bismil QMK, Lowe S, Viner L, Bismil MSK. The wide-awake approach to ulnar nerve entrapment: results of an integrated one-stop wide-awake surgical pathway. OA Case Reports 2013 Jun 21;2(5):44.
2. Bismil Q, Bismil M, Bismil A, Neathey J, Gadd J, Roberts S, et al. The development of one-stop wide-awake Dupuytren’s fasciectomy service: a retrospective review. JRSM Short Rep. 2012 Jul;3(7):48.3. Robbins TH. Dupuytren’s contracture: the deferred Z-plasty. Ann R Coll Surg Engl. 1981 Sep;63(5):357–8.4. Worldwide Awake Hand Surgery Group [Advancing Hand Surgery]. London: The OSWA Service London; 2012.5. Leblanc MR, Lalonde DH, Thoma A, Bell M, Wells N, Allen M, et al. Is main operating room sterility really necessary in carpal tunnel surgery? A multicenter prospective study of minor procedure room field sterility surgery. Hand (N Y). 2011 Mar;6(1):60–3.6. Leblanc MR, Lalonde J, Lalonde DH. A detailed cost and efficiency analysis of performing carpal tunnel surgery in the main operating room versus the ambula-tory setting in Canada. Hand (N Y). 2007 Dec;2(4):173–8.7. Lalonde DH. How the evidence has changed my practice. Plast Reconstr Surg. 2011 Dec;128(6):1312–4.8. Mustoe TA, Buck DW 2nd, Lalonde DH. The safe management of anesthesia, sedation, and pain in plastic surgery. Plast Reconstr Surg. 2010 Oct;126(4):165e–76e.9. Denkler KA. Epinephrine in the digits. Plast Reconstr Surg. 2011 Aug;128(2):598–9.10. Denkler K. Myth of not using lidocaine with epinephrine in the digits. Am Fam Physician. 2010 May;81(10):1188.11. Lalonde D, Bell M, Benoit P, Sparkes G, Denkler K, Chang P. A multicenter
prospective study of 3,110 consecutive cases of elective epinephrine use in the fingers and hand: the Dalhousie Project clinical phase. J Hand Surg Am. 2005 Sep;30(5):1061–7.12. Lalonde DH, Lalonde JF. Discussion. Do not use epinephrine in digital blocks: myth or truth? Part II. A retrospective review of 1111 cases. Plast Reconstr Surg. 2010 Dec;126(6):2035–6.13. Fitzcharles-Bowe C, Denkler K, Lalonde D. Finger injection with high-dose (1:1,000) epinephrine: Does it cause finger necrosis and should it be treated? Hand (N Y). 2007 Mar;2(1):5–11.14. Wheelock ME, Leblanc M, Chung B, Williams J, Lalonde DH. Is it true that injecting palmar finger skin hurts more than dorsal skin? New level 1 evidence. Hand (N Y). 2011 Mar;6(1):47–9.15. Strazar R, Lalonde D. Minimizing injection pain in local anesthesia. CMAJ. 2012 Dec;184(18):2016.16. Lalonde DH. “Hole-in-one” local anesthesia for wide-awake carpal tunnel surgery. Plast Reconstr Surg. 2010 Nov;126(5):1642–4.17. Lalonde DH. Reconstruction of the hand with wide awake surgery. Clin Plast Surg. 2011 Oct;38(4):761–9.18. Higgins A, Lalonde DH, Bell M, McKee D, Lalonde JF. Avoiding flexor tendon repair rupture with intraoperative total active movement examination. Plast Reconstr Surg. 2010 Sep;126(3):941–5.19. Lalonde DH. Wide-awake flexor tendon repair. Plast Reconstr Surg. 2009 Feb;123(2):623–5.20. Denkler K. Dupuytren’s fasciectomies in 60 consecutive digits using lidocaine
with epinephrine and no tourniquet. Plast Reconstr Surg. 2005 Mar;115(3):802–10.21. Nelson R, Higgins A, Doumit J, Conrad J, Bell M, Lalonde D. Erratum to: The wide-awake approach to Dupuytren’s disease: fasciectomy under local anes-thetic with epinephrine. Hand (N Y). 2010 Jun;5(2):213.22. Hagert E, Lalonde DH. Wide-awake wrist arthroscopy and open TFCC repair. J Wrist Surg. 2012 Aug;1(1):55–60. 23. Lankester BJ, Giddins GE. Ulnar nerve decompression in the cubital canal using local anaesthesia. J Hand Surg Br. 2001 Feb;26(1):65–6.24. Lavyne MH, Bell WO. Simple decom-pression and occasional microsurgical epineurolysis under local anesthesia as treatment for ulnar neuropathy at the elbow. Neurosurgery. 1982 Jul;11(1 Pt 1):6–11.25. Caliandro P, La Torre G, Padua R, Giannini F, Padua L. Treatment for ulnar neuropathy at the elbow. Cochrane Data-base Syst Rev. 2012 Jul;7:CD006839.26. Bachoura A, Jacoby SM. Ulnar tunnel syndrome. Orthop Clin North Am. 2012 Oct;43(4):467–74.27. Hagert E. Clinical diagnosis and wide-awake surgical treatment of proximal median nerve entrapment at the elbow: a prospective study. Hand. 2012 Oct.28. Graham B. The value added by elec-trodiagnostic testing in the diagnosis of carpal tunnel syndrome. J Bone Joint Surg Am. 2008 Dec;90(12):2587–93.