the world breastfeeding trends initiative (wbti world breastfeeding trends initiative (wbti ) nepal...
TRANSCRIPT
The World Breastfeeding Trends Initiative (WBTi )
Nepal Report 2012 Core group:
Prof. Dr. Prakash Sundar Shrestha President Nepal Breastfeeding Promotion Forum (NEBPROF) Mr. Raj Kumar Pokharel Chief Nutrition Section, Child Health Division, MOHP Dr. Dhan Raj Aryal Deputy Director Paropakar Maternity Hospital Dr. Jyoti Ratna Dhakhwa President Nepal Paediatric Society (NEPAS) Dr. Laxman Shrestha Associate Professor Department of Child Health, IOM
Dr. Kalpana Tiwari Pant Coordinator South Asia Infant Feeding Research Network (SAIFRN), Nepal
Prepared by:
Prof. Prakash Sundar Shrestha &
Dr. Kalpana Tiwari Pant
Published by:- Supported by:-
i | P a g e
ACKNOWLEDGEMENTS
I am extremely thankful to all the members of Executive Committee of Nepal Breastfeeding
Promotion Forum (NEBPROF) for helping me to form the core group to conduct assessment of
WBTi 2012.
I am very much grateful to the core group members Mr. Raj Kumar Pokharel, Chief Nutrition
Section, Child Health Division, Dr. Jyoti Ratna Dhakhwa, President, Nepal Paediatric Society, Dr.
Dhan Raj Aryal, Deputy Director, Maternity Hospital, Dr. Laxman Shrestha, Associate Professor,
Department of Child Health, Institute of Medicine for their valuable efforts in going through the
details of available documents to identify the gaps and came out with the valuable
recommendations.
My special thank goes to Dr. Kalpana (Tiwari) Pant, Coordinator, SAIFRN Nepal for her tireless
effort as a core group member and also for presenting at workshop as well as in preparing the
report card and detail report of WBTi 2012.
I would be failing in my duty if I don’t acknowledge the hard work done by Mrs. Tulashi Adhikari
Mishra, Lecturer, Maharajgunj Nursing Campus as a master of ceremony during the workshop. I
would like to thank the 3rd year Proficiency Certificate Level (PCL) nursing students (55th Batch) of
Maharajgunj Nursing Campus for designing the cover image of the report.
I would like to thank all the partner organizations and participants in WBTi 2012 Workshop who had
actively participated and given their valuable suggestions without which it won’t have been possible
for us to prepare this report.
I personally thank Dr. Arun Gupta, Regional Coordinator, IBFAN Asia and Dr. J. P. Dadhich,
National Coordinator BPNI for their continued encouragement and guidance for preparing this

ii | P a g e
report. I am also grateful to IBFAN Asia for providing necessary financial support for the workshop
as well as for preparing the report.
Finally I would like to thank Mr. Samir K. C., Computer Manager for taking all trouble for designing,
formatting and setting the WBTi 2012 report to current shape.
Prof. Prakash S. Shrestha, President Nepal Breastfeeding Promotion Forum (NEBPROF)
iii | P a g e

iv | P a g e
v | P a g e
PREFACE
The Global Strategy for Infant and Young Child Feeding was adopted by World Health Assembly
and UNICEF Executive Board in 2002. It was recognized that malnutrition has been responsible
directly or indirectly for 60% of the 10.9 million deaths annually among the children under five. Well
over two thirds of these deaths which are often associated with inappropriate feeding practices,
occur during the first year of life.
The Global Strategy set forth nine operational targets related to both breastfeeding and
complementary feeding. To track the progress of program through the implementation of the Global
Strategy, the World Health Organization developed a tool for assessing national practices, policies
and programs in support of Infant and Young Child Feeding. The International Baby Food Action
Network (IBFAN) Asia developed the WBTi to assess and monitor Infant and Young Child Feeding
practices, policies and programs by developing a guideline for scoring and colour rating
assessment finding. In the beginning network of South Asia decided to use tool in eight countries
including Nepal. Later on this assessment tool was used by different other countries for assessment
of their policies and programs on infant and young child feeding. The use of gaps, they found help
in advocacy which resulted in national action. Finding and result of WBTi was shared with Global
Breastfeeding Partners meeting, IBFAN Coordination Council meeting, IBFAN’s strategic planning
meeting in 2006. In 2008-2009 it became an integral and central part of the Global Breastfeeding
Initiative for Child Survival (gBICS) a joint IBFAN and WABA initiative to enhance and generate new
momentum of Infant Feeding Worldwide. Till middle of 2012 WBTi has been introduced in 82
countries and 51 completed the assessment reports by October 2012.
Nepal Breastfeeding Promotion Forum (NEBPROF) has been conducting WBTi assessment since it
was originally started in Eight South Asia countries, till date we have completed three assessments
(2005, 2008 & 2012). The WBTi report of 2012 has identified the existing gaps in the key factors
associated with breastfeeding and complementary feeding practices. It has also came out with the

vi | P a g e
possible recommendations which will be shared with the UN organizations, Government, Non-
government organizations and relevant stakeholders which will help in developing national strategy
and plan of action on IYCF to improve the nutritional status of children in Nepal.
Prof. Prakash S. Shrestha, President Nepal Breastfeeding Promotion Forum (NEBPROF)

Table of Content Content Page No Acknowledgements i Foreword iii Preface v
Executive Summary 1 Introduction 4 Nepal Context 4 National Commitments 5 About WBTi: How it works? 5 Indicators used in WBTi 6 Methodology 8 Assessment Results 9 Part I: Infant and Young Child Feeding Policies and Programs 9 Indicator :1 Indicator 2: Indicator 3: Indicator 4: Indicator 5: Indicator 6: Indicator 7: Indicator 8: Indicator 9:
Indicator 10: Comparison of finding with previous assessments (Indicators 1 – 10) 24 Part II: Infant & Young Child Feeding Practices 25 Indicator 11: Indicator 12: Indicator 13: Indicator 14: Indicator 15: Comparison of finding with previous assessment (Indicators 11 – 15) 28 Summary of Findings 29 Gaps and Recommendations 30 Conclusion and Way Forward 31
Annexes Annex 1: Presentation 1 33 Annex 2: Presentation 2 35 Annex 3: Schedule of Workshop 39 Annex 4: List of Participants / Partner 40 Annex 5: References 41

1 | P a g e
Executive Summary Nepal 2012 report of the assessment of the state of implementation of the Global Strategy for Infant and Young Child Feeding is accomplished in collaboration of the World Breastfeeding Trends Initiative (WBTi) of IBFAN Asia. The WBTi serves as a lens to show gaps in policy and programs and guide nation to initiate actions to bridge the gaps. More than 51 countries have already completed WBTi assessment around the year 2012. The brain child of International Baby Food Action Network Asia, WBTi is an integrated part of two global projects jointly funded by Norwegian Agency for Development Cooperation (NORAD) and Swedish International Development Cooperation Agency (SIDA). Nepal Breastfeeding Promotion Forum (NEBPROF) had coordinated with IBFAN Asia, Government and partner organization for this 2012 assessment activity. This report is based on the review of relevant documents with intensive analysis of existing policy and programs and its implementation in the country. The core group critically reviewed key documents, websites and published information and interacted with key informants working in the areas. The findings presented in the report is mainly within the scope of the web based toolkit, WBTi guidelines and Nepal scored 91 out of total score 150 and stands in BLUE color based in grid of RED, YELLOW, BLUE and GREEN in ascending order of performance or achievement. Once the report was prepared by the core group, it was shared and discussed with larger group and consensus was achieved in availability of information, identification of gaps and recommendations for bridging the existing gaps. The report has found gaps in both policy and programs. It has shown some improvements as compared to previous two assessments i.e. 2005 and 2008. Particularly in policy, strategies and guidelines of IYCF in emergencies and infant feeding in HIV positive mother. Major finding for indicators 1-15 and gaps including recommendations are summarized. Table 1: Key Findings Indicators 1 – 10
S.N. Indicators Score out of 10 1 National Policy, Programs and Coordination 8 2 Baby Friendly Hospital Initiative 1 3 Implementation of the International Code 7 4 Maternity Protection 2 5 Health and Nutrition Care 4.5 6 Community Outreach 5 7 Information Support 6 8 Infant Feeding and HIV 5.5 9 Infant Feeding during Emergencies 9 10 Monitoring and Evaluation 6
In indicators 1-10 not much improvement has occurred in last five years except some improvement in infant feeding during emergencies and infant feeding and HIV. The gaps and recommendations for indicators 1-10 are listed below
2 | P a g e
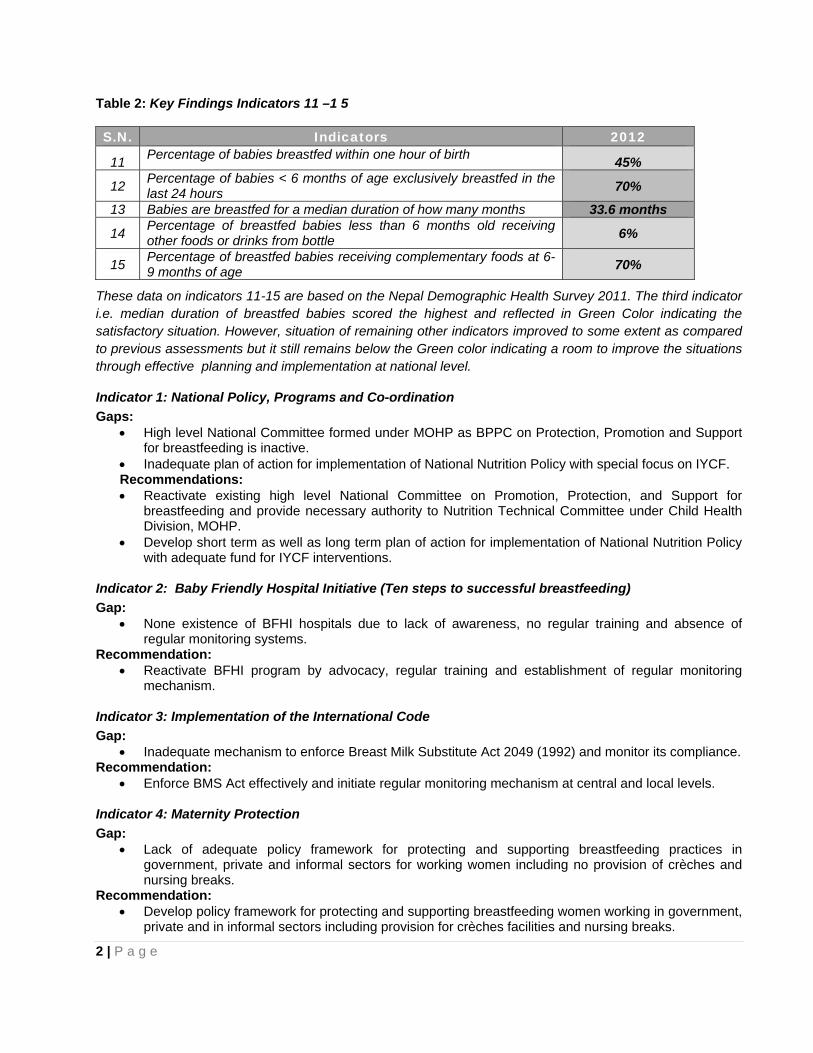
Table 2: Key Findings Indicators 11 –1 5
S.N. Indicators 2012
11 Percentage of babies breastfed within one hour of birth 45%
12 Percentage of babies < 6 months of age exclusively breastfed in the last 24 hours 70%
13 Babies are breastfed for a median duration of how many months 33.6 months
14 Percentage of breastfed babies less than 6 months old receiving other foods or drinks from bottle 6%
15 Percentage of breastfed babies receiving complementary foods at 6-9 months of age 70%
These data on indicators 11-15 are based on the Nepal Demographic Health Survey 2011. The third indicator i.e. median duration of breastfed babies scored the highest and reflected in Green Color indicating the satisfactory situation. However, situation of remaining other indicators improved to some extent as compared to previous assessments but it still remains below the Green color indicating a room to improve the situations through effective planning and implementation at national level.
Indicator 1: National Policy, Programs and Co-ordination Gaps:
• High level National Committee formed under MOHP as BPPC on Protection, Promotion and Support for breastfeeding is inactive.
• Inadequate plan of action for implementation of National Nutrition Policy with special focus on IYCF. Recommendations: • Reactivate existing high level National Committee on Promotion, Protection, and Support for
breastfeeding and provide necessary authority to Nutrition Technical Committee under Child Health Division, MOHP.
• Develop short term as well as long term plan of action for implementation of National Nutrition Policy with adequate fund for IYCF interventions.
Indicator 2: Baby Friendly Hospital Initiative (Ten steps to successful breastfeeding) Gap:
• None existence of BFHI hospitals due to lack of awareness, no regular training and absence of regular monitoring systems.
Recommendation: • Reactivate BFHI program by advocacy, regular training and establishment of regular monitoring
mechanism.
Indicator 3: Implementation of the International Code Gap:
• Inadequate mechanism to enforce Breast Milk Substitute Act 2049 (1992) and monitor its compliance. Recommendation:
• Enforce BMS Act effectively and initiate regular monitoring mechanism at central and local levels. Indicator 4: Maternity Protection Gap:
• Lack of adequate policy framework for protecting and supporting breastfeeding practices in government, private and informal sectors for working women including no provision of crèches and nursing breaks.
Recommendation: • Develop policy framework for protecting and supporting breastfeeding women working in government,
private and in informal sectors including provision for crèches facilities and nursing breaks.

3 | P a g e
Indicator 5: Health and Nutrition Care Systems Gap:
• Inadequate practical training for health professionals regarding infant and young child feeding in pre-service and in-service education system.
Recommendation: • Incorporate adequate practical training in pre-service and in-service training for the health
professionals on infant and young child feeding. Indicator 6: Mother support and community based support for the pregnant and breastfeeding mother Gap:
• Inadequate services and support available on counseling pregnant mothers and breastfeeding mother in outreach clinic.
Recommendation: • Village level health workers should be trained for comprehensive intervention on IYCF to support
pregnant and breastfeeding mothers at community level or outreach clinic. Indicator 7: Information Support Gap:
• Inadequate National Strategy on IEC on Infant and Young Child Feeding in existing program. Recommendation:
• Develop and implement appropriate strategy with adequate fund for IEC on infant and young child feeding.
Indicator 8: Infant Feeding and HIV Gap:
• Inadequate counseling to HIV positive women regarding infant feeding Recommendation:
• Provide adequate counseling on IYCF for HIV positive women at all levels and through all HIV programs.
Indicator 9: Infant Feeding during Emergencies Gap:
• Inadequate experienced human resources on infant feeding in emergencies Recommendation:
• Create adequate expertise for managing IYCF during emergencies. Indicator 10: Mechanisms of Monitoring and Evaluation System Gap:
• Major IYCF activities are not reflected in existing national level monitoring and evaluation components.
Recommendation: • Integration of adequate indicators of infant and young child feeding into national health management
information system.
4 | P a g e
Introduction Under nutrition, particularly in children under two years of age, prevents them from reaching their full development potential. It is well documented that the role of breastfeeding and complementary feeding as key interventions to enhance nutrition, development and survival of infants and young children. On average, more than 24,000 children under five years of age still die every day from preventable causes and according to UNICEF’s State of the World Children 2010, under nutrition contribute to more than one-third of these deaths. Optimal breast feeding not only saves the lives of more than one million children under five; it also improves children's quality of life. The World Health Statistics Report 2009 recognized that poor infant feeding i.e. not being exclusively breastfed for the first months of life-is a risk factor for survival of the child. The evidence presented in the Lancet series on child survival 2003 and Lancet series on neonatal survival 2005, and the Lancet series on maternal and child under nutrition 2008, clearly pointed out the importance of exclusive breastfeeding for the first six months of life which could save more lives than any other intervention studied while enhancing nutritional status. The world today is striving hard to improve child survival in order to achieve the Millennium Development Goals 1, 4, and 5. Over the last few years, breastfeeding has emerged as a single and very viable public health intervention. In order to increase the rates of optimal feeding practices, the WHO and UNICEF developed the Global Strategy for Infant and Young Child Feeding, which provides a framework for action to scale up breastfeeding, and infant and young child feeding interventions. They also developed a tool to monitor these inputs. Breastfeeding Promotion Network of India (BPNI)/International Baby Food Action Network (IBFAN), Asia, developed the World Breastfeeding Trends Initiative (WBTi), which measures inputs and generates national action. WBTi analyses the situation, documents gaps, and builds consensus and recommendations. And stimulates governments to take some action to bridge the gaps in respective countries. The World Breastfeeding Trends Initiative (WBTi) report presents detailed findings on the 15 indicators of the tool, 10 of which relate to policy and programs on infant and young child feeding and 5 on the resultant practices. The national team used the WBTi tool and questionnaire to assess their country's status on the implementation of the Global Strategy for Infant and Young Child Feeding 2002. It helps to find the gaps in the implementation, and used these for advocacy and to initiate new action for scaling up IYCF.
Nepal Context Nepal is in track to achieve the Millennium Development Goals for maternal and child morbidity. Significant improvements have also been made in child nutrition and breastfeeding practices in the last five years. However its sustainablility in urban and rural is a challenge. The Nepal Demographic Health Survey NDHS 2011 indicates that exclusive breastfeeding in children has increased to 70% from 53% in 2006, and almost all children are still breastfed at 2 years of age. Prelacteal feeding has fallen such that only 28% of children receive a pre-lacteal and 85% of children have initiated breastfeeding within 24 hours of birth. Although breastfeeding practices have improved, there is still need to improvement, initiation of breastfeeding within one hour of birth which is currently only 45% and only 70% of children are exclusively breastfed. In order to sustain the achievement made, initiation of breastfeeding within an hour of birth needs activities addressing prelacteal feeding practices due to cultural beliefs and provision of support for initiation of breastfeeding at hospitals to community levels. Children under six months who are not exclusively breastfeeding are consuming water, other milks and complementary foods, in roughly equal proportions, in addition to breast milk. It is interesting to note that about 20% of infants 2-3 months old are given water or other milks in addition to breast milk or predominantly breastfed (NDHS 2011).

5 | P a g e
National Commitments Nepal has made several commitments in line with global commitments related to the survival, adequate nutrition, growth and development of infants and children as fundamental rights. A national consensus for a multi-sectoral action plan addresses for reduction of chronic malnutrition in Nepal and it focuses on actions needed to improve maternal and child nutrition, accessible to everyone, especially during the first 1,000 days of life, ensuring equity, and facilitating access to information, promoting behavior change, with a focus to reach the most marginalized, poorest segments of the population, and taking into account gender related factors. Government prioritizes and that there is a strong link between poverty reduction, food insecurity and nutrition and chronic malnutrition. The Nepal Strategy for Infant and Young Children Feeding has been developed in line with the Nepal multi-sector nutrition plan (2013-2017) and is in final stage. The strategy has identified comprehensive actions that are crucial for improving infant feeding in the country. It has focused on the need to act upon the implementation of advocacy, policy, partnership and coordination to enhance political commitments in support of improving all components of IYCF including legislation and standards to protect promote and support IYCF including breastfeeding and BFHI/CBFI in country (Draft IYCF strategy 2012).
Strategic communication approach is taking and integrated approach to health for women and children, focusing on the critical time from pregnancy through the first 1000 days of a baby's life. Health Priority linked to Maternal Nutrition and Child Health (MNCH) includes newborn care, early initiation and exclusive breastfeeding (Communication Strategy 2011-2016). Promotion of breastfeeding and behavior change communication for improved complementary feeding is also addressed in National Communication Strategy and National HIV/AIDs strategies. Improving infant and young child feeding is one of the most important nutrition strategies for Nepal however; efforts in this area are fragmented and not intensive. Although exclusive breastfeeding has improved substantially since 2006, there is no data on what has caused this improvement as effective monitoring and evaluation system is weak, and none of the recent efforts to improve IYCF practices have been evaluated at national level. Therefore, this assessment finds that IYCF interventions helps to prioritize intervention be refined interventions and intensified implementations at all level. The national IYCF strategy needs to be strengthened to be more comprehensive and detailed and efforts need to be made for its implementation at local levels. The assessment felt the gaps in national commitment, mainly for an oversight and coordinating structure of high level BPCC. National Technical Committee on Nutrition initiated within Child Health Division should be functioning with full authority. Emphasis needs to be placed on building up the capacity of the health system to provide quality skilled counseling and support to caregivers and their families for improved IYCF behaviors. World Bank Review 2012 on IYCF also recommends in line with this gap. The existing National Committee on Promotion, Protection and Support for breastfeeding should be reactivated and coordinated with Nutrition Technical Committee currently existed under Child Health Division, Ministry of Health and Population.
About WBTi: How it works? In 2004-2005, the International Baby Food Action Network (IBFAN) adapted the World Health Organization (WHO) tool for assessment and action. It was first initiated in Asian countries and then lunched in other regions in 2008/9 and has now been introduced to 82 countries. Fifty one countries completed the work of
6 | P a g e
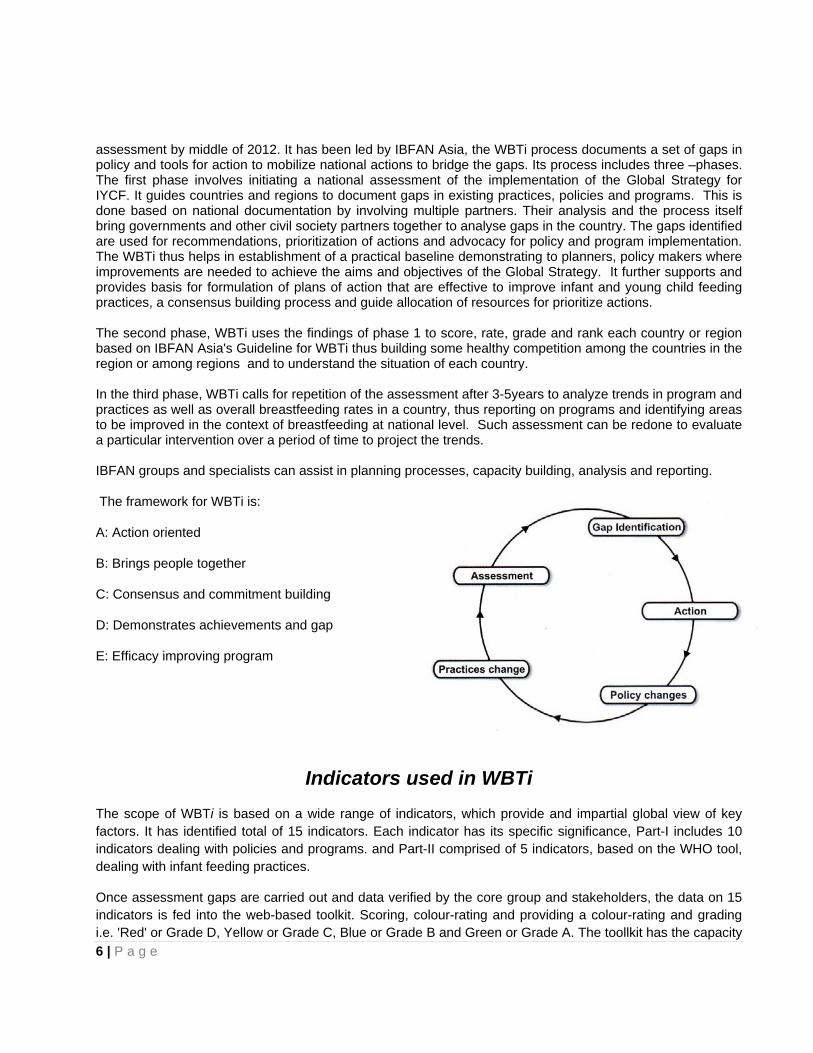
assessment by middle of 2012. It has been led by IBFAN Asia, the WBTi process documents a set of gaps in policy and tools for action to mobilize national actions to bridge the gaps. Its process includes three –phases. The first phase involves initiating a national assessment of the implementation of the Global Strategy for IYCF. It guides countries and regions to document gaps in existing practices, policies and programs. This is done based on national documentation by involving multiple partners. Their analysis and the process itself bring governments and other civil society partners together to analyse gaps in the country. The gaps identified are used for recommendations, prioritization of actions and advocacy for policy and program implementation. The WBTi thus helps in establishment of a practical baseline demonstrating to planners, policy makers where improvements are needed to achieve the aims and objectives of the Global Strategy. It further supports and provides basis for formulation of plans of action that are effective to improve infant and young child feeding practices, a consensus building process and guide allocation of resources for prioritize actions. The second phase, WBTi uses the findings of phase 1 to score, rate, grade and rank each country or region based on IBFAN Asia's Guideline for WBTi thus building some healthy competition among the countries in the region or among regions and to understand the situation of each country. In the third phase, WBTi calls for repetition of the assessment after 3-5years to analyze trends in program and practices as well as overall breastfeeding rates in a country, thus reporting on programs and identifying areas to be improved in the context of breastfeeding at national level. Such assessment can be redone to evaluate a particular intervention over a period of time to project the trends. IBFAN groups and specialists can assist in planning processes, capacity building, analysis and reporting.
The framework for WBTi is:
A: Action oriented
B: Brings people together
C: Consensus and commitment building
D: Demonstrates achievements and gap
E: Efficacy improving program
Indicators used in WBTi The scope of WBTi is based on a wide range of indicators, which provide and impartial global view of key factors. It has identified total of 15 indicators. Each indicator has its specific significance, Part-I includes 10 indicators dealing with policies and programs. and Part-II comprised of 5 indicators, based on the WHO tool, dealing with infant feeding practices.
Once assessment gaps are carried out and data verified by the core group and stakeholders, the data on 15 indicators is fed into the web-based toolkit. Scoring, colour-rating and providing a colour-rating and grading i.e. 'Red' or Grade D, Yellow or Grade C, Blue or Grade B and Green or Grade A. The toollkit has the capacity
7 | P a g e
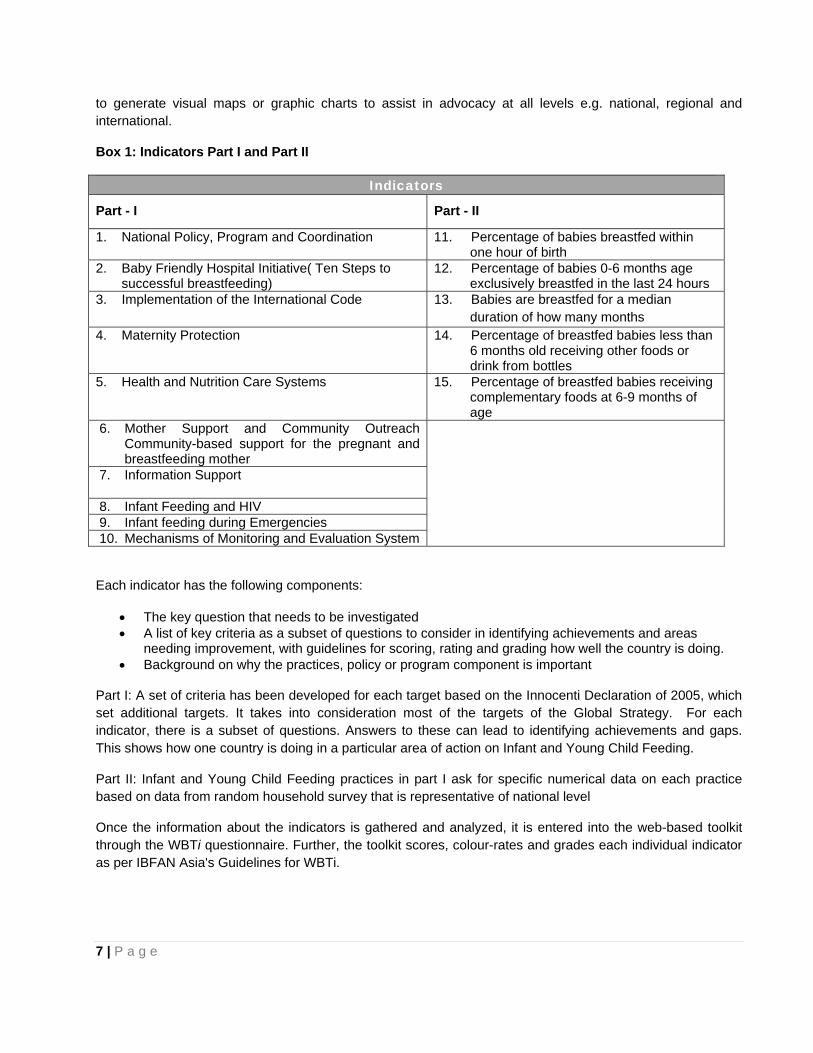
to generate visual maps or graphic charts to assist in advocacy at all levels e.g. national, regional and international.
Box 1: Indicators Part I and Part II
Indicators
Part - I Part - II
1. National Policy, Program and Coordination 11. Percentage of babies breastfed within one hour of birth
2. Baby Friendly Hospital Initiative( Ten Steps to successful breastfeeding)
12. Percentage of babies 0-6 months age exclusively breastfed in the last 24 hours
3. Implementation of the International Code 13. Babies are breastfed for a median duration of how many months
4. Maternity Protection 14. Percentage of breastfed babies less than 6 months old receiving other foods or drink from bottles
5. Health and Nutrition Care Systems 15. Percentage of breastfed babies receiving complementary foods at 6-9 months of age
6. Mother Support and Community Outreach Community-based support for the pregnant and breastfeeding mother
7. Information Support
8. Infant Feeding and HIV 9. Infant feeding during Emergencies 10. Mechanisms of Monitoring and Evaluation System
Each indicator has the following components:
• The key question that needs to be investigated • A list of key criteria as a subset of questions to consider in identifying achievements and areas
needing improvement, with guidelines for scoring, rating and grading how well the country is doing. • Background on why the practices, policy or program component is important
Part I: A set of criteria has been developed for each target based on the Innocenti Declaration of 2005, which set additional targets. It takes into consideration most of the targets of the Global Strategy. For each indicator, there is a subset of questions. Answers to these can lead to identifying achievements and gaps. This shows how one country is doing in a particular area of action on Infant and Young Child Feeding.
Part II: Infant and Young Child Feeding practices in part I ask for specific numerical data on each practice based on data from random household survey that is representative of national level
Once the information about the indicators is gathered and analyzed, it is entered into the web-based toolkit through the WBTi questionnaire. Further, the toolkit scores, colour-rates and grades each individual indicator as per IBFAN Asia's Guidelines for WBTi.

8 | P a g e
Methodology First a core group of 6 persons was formed, by bringing together stakeholders including government, professional bodies, civil society organizations including WHO and UNICEF. A coordinator was identified to lead the process. The core group well understood the indicators of the assessment and questionnaires available at WBTi website. Coordination at National level was the major part of the assessment which was very well undertaken by Nepal Breastfeeding Promotion Forum (NEBPROF). The core group was comprised of 6 persons:
1. Prof. Prakash S. Shrestha 4. Dr. Jyoti Ratna Dhakhwa 2. Mr. Raj Kumar Pokharel 5. Dr. Laxman Shrestha 3. Dr. Dhan Raj Aryal 6. Dr. Kalpana Tiwari Pant
The core group met several times to discuss each issues in details. Then the core group studied and assessed with each indicator, listed findings and took note of the gaps. In order to share the findings in the larger group and to achieve consensus, the National Workshop was organized on 29th November 2012.
Dr. Prakash Sunder Shrestha highlighted on the background of WBTi, global situation and its initiation in Nepal (Annex 1). Dr. Kalpana Tiwari shared on the situation and scores under the each indicator (Annex 2). Workshop Schedules is attached (Annex 3). Based on the presentations and working experiences of the stakeholders, the discussion was initiated and facilitated by Dr. Prakash Shrestha. All the members present in the workshop, actively participated in the discussion and all the inputs given in workshop by participants and members are incorporated in the report.
9 | P a g e
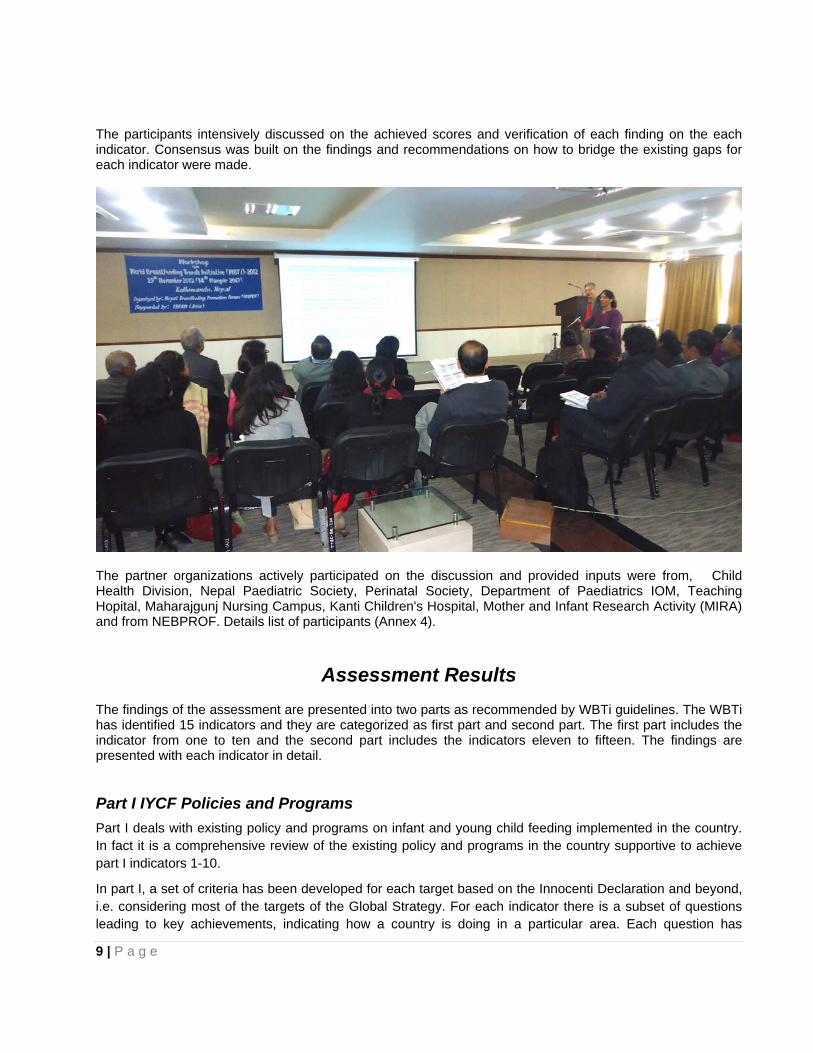
The participants intensively discussed on the achieved scores and verification of each finding on the each indicator. Consensus was built on the findings and recommendations on how to bridge the existing gaps for each indicator were made.
The partner organizations actively participated on the discussion and provided inputs were from, Child Health Division, Nepal Paediatric Society, Perinatal Society, Department of Paediatrics IOM, Teaching Hopital, Maharajgunj Nursing Campus, Kanti Children's Hospital, Mother and Infant Research Activity (MIRA) and from NEBPROF. Details list of participants (Annex 4).
Assessment Results The findings of the assessment are presented into two parts as recommended by WBTi guidelines. The WBTi has identified 15 indicators and they are categorized as first part and second part. The first part includes the indicator from one to ten and the second part includes the indicators eleven to fifteen. The findings are presented with each indicator in detail.
Part I IYCF Policies and Programs Part I deals with existing policy and programs on infant and young child feeding implemented in the country. In fact it is a comprehensive review of the existing policy and programs in the country supportive to achieve part I indicators 1-10.
In part I, a set of criteria has been developed for each target based on the Innocenti Declaration and beyond, i.e. considering most of the targets of the Global Strategy. For each indicator there is a subset of questions leading to key achievements, indicating how a country is doing in a particular area. Each question has
10 | P a g e
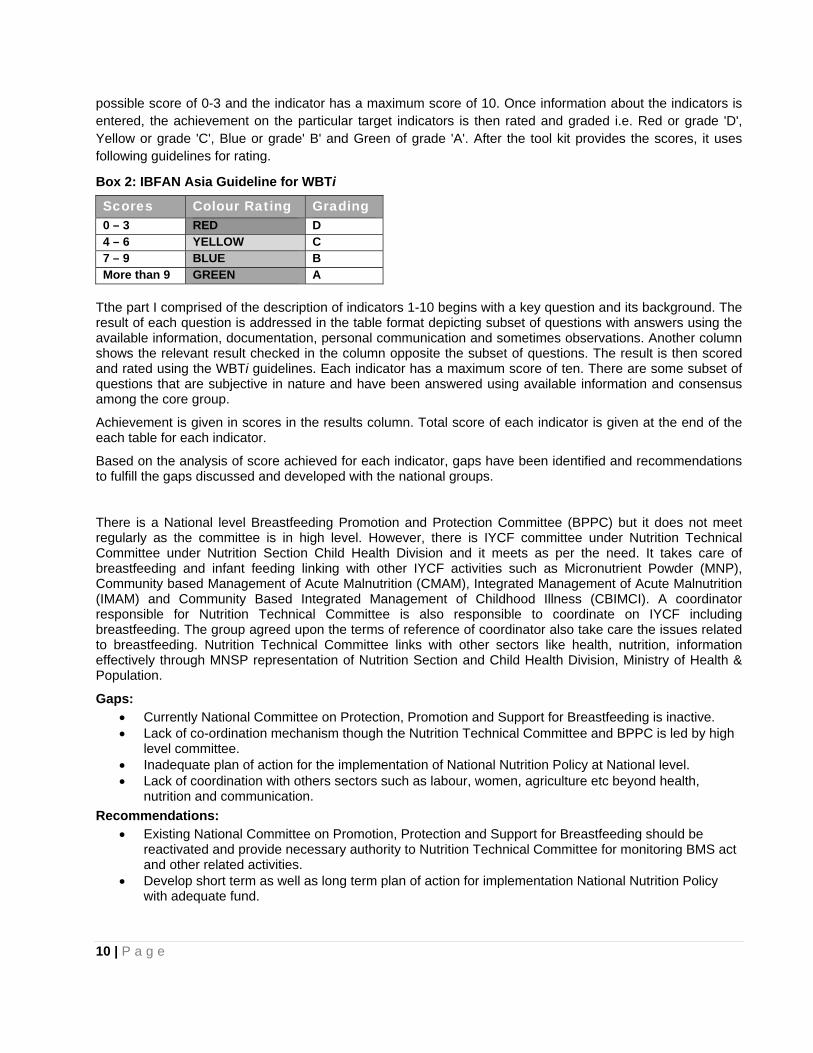
possible score of 0-3 and the indicator has a maximum score of 10. Once information about the indicators is entered, the achievement on the particular target indicators is then rated and graded i.e. Red or grade 'D', Yellow or grade 'C', Blue or grade' B' and Green of grade 'A'. After the tool kit provides the scores, it uses following guidelines for rating.
Box 2: IBFAN Asia Guideline for WBTi
Scores Colour Rating Grading 0 – 3 RED D 4 – 6 YELLOW C 7 – 9 BLUE B More than 9 GREEN A
Tthe part I comprised of the description of indicators 1-10 begins with a key question and its background. The result of each question is addressed in the table format depicting subset of questions with answers using the available information, documentation, personal communication and sometimes observations. Another column shows the relevant result checked in the column opposite the subset of questions. The result is then scored and rated using the WBTi guidelines. Each indicator has a maximum score of ten. There are some subset of questions that are subjective in nature and have been answered using available information and consensus among the core group.
Achievement is given in scores in the results column. Total score of each indicator is given at the end of the each table for each indicator.
Based on the analysis of score achieved for each indicator, gaps have been identified and recommendations to fulfill the gaps discussed and developed with the national groups.
There is a National level Breastfeeding Promotion and Protection Committee (BPPC) but it does not meet regularly as the committee is in high level. However, there is IYCF committee under Nutrition Technical Committee under Nutrition Section Child Health Division and it meets as per the need. It takes care of breastfeeding and infant feeding linking with other IYCF activities such as Micronutrient Powder (MNP), Community based Management of Acute Malnutrition (CMAM), Integrated Management of Acute Malnutrition (IMAM) and Community Based Integrated Management of Childhood Illness (CBIMCI). A coordinator responsible for Nutrition Technical Committee is also responsible to coordinate on IYCF including breastfeeding. The group agreed upon the terms of reference of coordinator also take care the issues related to breastfeeding. Nutrition Technical Committee links with other sectors like health, nutrition, information effectively through MNSP representation of Nutrition Section and Child Health Division, Ministry of Health & Population.
Gaps: • Currently National Committee on Protection, Promotion and Support for Breastfeeding is inactive. • Lack of co-ordination mechanism though the Nutrition Technical Committee and BPPC is led by high
level committee. • Inadequate plan of action for the implementation of National Nutrition Policy at National level. • Lack of coordination with others sectors such as labour, women, agriculture etc beyond health,
nutrition and communication. Recommendations:
• Existing National Committee on Promotion, Protection and Support for Breastfeeding should be reactivated and provide necessary authority to Nutrition Technical Committee for monitoring BMS act and other related activities.
• Develop short term as well as long term plan of action for implementation National Nutrition Policy with adequate fund.

11 | P a g e
Indicator 1: National Policy, Program and Coordination
Key Question: Is there a national infant and young children feeding / breastfeeding policy that protects, promotes and supports optimal infant and young child feeding and the policy is supported by a government program? Is there a mechanism to coordinate like National Infant and Young Child Feeding Committee and Coordinator
In 1990, The Innocenti Declaration recommended that all governments have national breastfeeding committee and coordinators as established mechanism to protect, promote and support breastfeeding in the country. Similarly, The World Summit for Children recommended all governments to develop national breastfeeding policies in 2000. The Global Strategy for Infant and Young Child Feeding calls for urgent action from all member states to develop, implement, monitor and evaluate a comprehensive policy on IYCF. The table below depicts the existing situation of National Policy, program and Coordination in Nepal. The indicator 6 deals with issues related to national policy and IYCF, national plan of action based on the national policy, national breastfeeding committee and financial allocations for IYCF. A separate comprehensive national IYCF strategy is in the process of development but not endorsed by the government.
The larger group agreed that the country has a national IYCF policy and has been approved by the government. National policy promotes initiation of breastfeeding within one hour of birth, exclusive breastfeeding for the first six months, complementary feeding initiated after completion of six months, and it also promotes to continue breastfeeding to 2 years and beyond. However, concrete national Plan of Action is not included in the policy. In last five years it was observed that a plan of action was developed with a lot of effort and adhoc action depending upon the budget available or fund is not adequate to scale up at national level plan of action. However, currently in IYCF is the national priority.
The table given below depicts the existing situation in Nepal on National Policy, Program and Coordination
Table 3: Subset Questionnaire for Indicator & Scoring for each Criteria No.
Criteria Score Adequate
1.1 A National Infant and Young Child Feeding / Breastfeeding policy has been officially adopted / approved by the government
2 √
1.2 The policy promotes exclusive breastfeeding for the first six months, complementary feeding to be started after six months and continued breastfeeding up to 2 years and beyond
2 √
1.3 A National Plan of Action has been developed with the policy 2 √ 1.4 The plan is adequately funded 1 1.5 There is a National Breastfeeding Committee 1 √ 1.6 The National Breastfeeding (Infant and Young Child Feeding)
Committee meets and reviews on a regular basis 1
1.7 The National Breastfeeding Infant and Young Child Feeding) Committee links with all other sectors like health, nutrition, information etc., effectively
0.5 √
1.8 Breastfeeding committee is headed by a coordinator with clear terms of reference
0.5 √
Total Score 8 / 10 There is a National level Breastfeeding Promotion and Protection Committee (BPPC) but it does not meet regularly as the committee is in high level. However, there is IYCF committee under Nutrition Technical Committee under Nutrition Section Child Health Division and it meets as per the need. It takes care of breastfeeding and infant feeding linking with other IYCF activities such as Micronutrient Powder (MNP), Community based Management of Acute Malnutrition (CMAM), Integrated Management of Acute Malnutrition (IMAM) and Community Based Integrated Management of Childhood Illness (CBIMCI). A coordinator responsible for Nutrition Technical Committee is also responsible to coordinate on IYCF including
12 | P a g e
breastfeeding. The group agreed upon the terms of reference of coordinator also take care the issues related to breastfeeding. Nutrition Technical Committee links with other sectors like health, nutrition, information effectively through MNSP representation of Nutrition Section and Child Health Division, Ministry of Health & Population.
Gaps: • Currently National Committee on Protection, Promotion and Support for Breastfeeding is inactive. • Lack of co-ordination mechanism though the Nutrition Technical Committee and BPPC is led by high
level committee. • Inadequate plan of action for the implementation of National Nutrition Policy at National level. • Lack of coordination with others sectors such as labour, women, agriculture etc beyond health,
nutrition and communication. Recommendations:
• Existing National Committee on Promotion, Protection and Support for Breastfeeding should be reactivated and provide necessary authority to Nutrition Technical Committee for monitoring BMS act and other related activities.
• Develop short term as well as long term plan of action for implementation National Nutrition Policy with adequate fund.
13 | P a g e
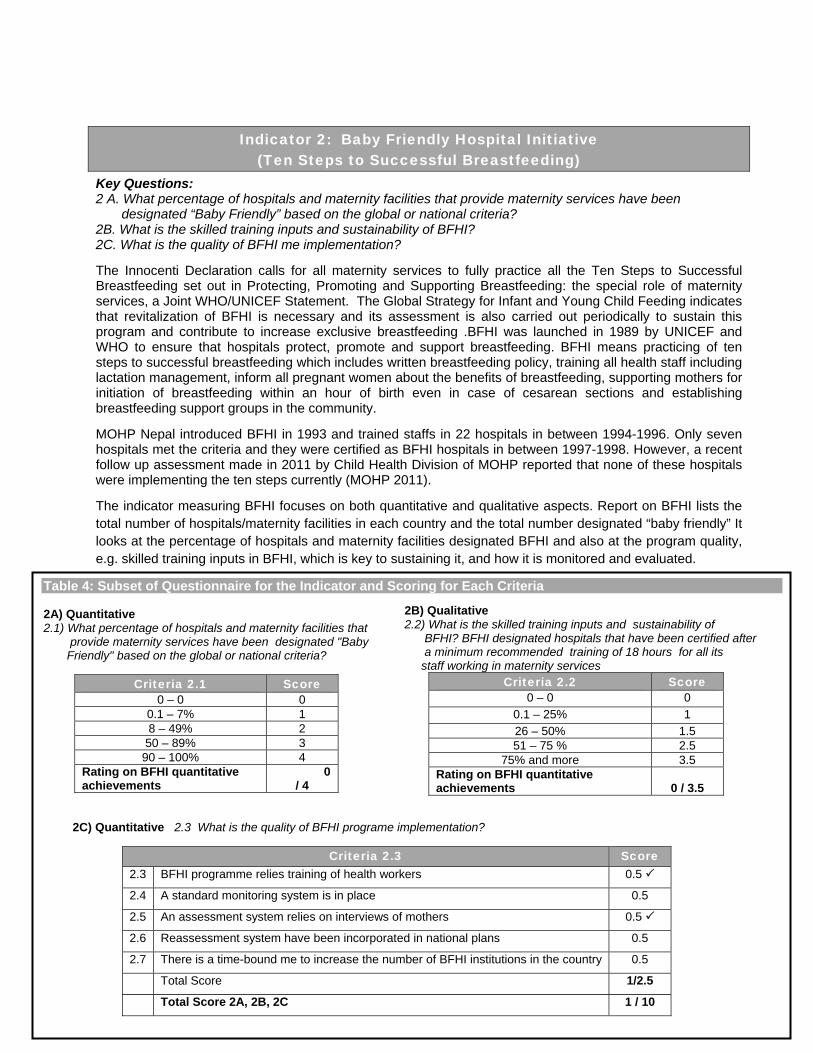
Indicator 2: Baby Friendly Hospital Initiative (Ten Steps to Successful Breastfeeding)
Key Questions: 2 A. What percentage of hospitals and maternity facilities that provide maternity services have been designated “Baby Friendly” based on the global or national criteria? 2B. What is the skilled training inputs and sustainability of BFHI? 2C. What is the quality of BFHI me implementation?
The Innocenti Declaration calls for all maternity services to fully practice all the Ten Steps to Successful Breastfeeding set out in Protecting, Promoting and Supporting Breastfeeding: the special role of maternity services, a Joint WHO/UNICEF Statement. The Global Strategy for Infant and Young Child Feeding indicates that revitalization of BFHI is necessary and its assessment is also carried out periodically to sustain this program and contribute to increase exclusive breastfeeding .BFHI was launched in 1989 by UNICEF and WHO to ensure that hospitals protect, promote and support breastfeeding. BFHI means practicing of ten steps to successful breastfeeding which includes written breastfeeding policy, training all health staff including lactation management, inform all pregnant women about the benefits of breastfeeding, supporting mothers for initiation of breastfeeding within an hour of birth even in case of cesarean sections and establishing breastfeeding support groups in the community.
MOHP Nepal introduced BFHI in 1993 and trained staffs in 22 hospitals in between 1994-1996. Only seven hospitals met the criteria and they were certified as BFHI hospitals in between 1997-1998. However, a recent follow up assessment made in 2011 by Child Health Division of MOHP reported that none of these hospitals were implementing the ten steps currently (MOHP 2011).
The indicator measuring BFHI focuses on both quantitative and qualitative aspects. Report on BFHI lists the total number of hospitals/maternity facilities in each country and the total number designated “baby friendly” It looks at the percentage of hospitals and maternity facilities designated BFHI and also at the program quality, e.g. skilled training inputs in BFHI, which is key to sustaining it, and how it is monitored and evaluated.
Table 4: Subset of Questionnaire for the Indicator and Scoring for Each Criteria 2A) Quantitative 2.1) What percentage of hospitals and maternity facilities that provide maternity services have been designated "Baby Friendly" based on the global or national criteria?
Criteria 2.1 Score 0 – 0 0
0.1 – 7% 1 8 – 49% 2
50 – 89% 3 90 – 100% 4
Rating on BFHI quantitative achievements
0 / 4
2B) Qualitative2.2) What is the skilled training inputs and sustainability of BFHI? BFHI designated hospitals that have been certified after a minimum recommended training of 18 hours for all its staff working in maternity services
Criteria 2.2 Score 0 – 0 0
0.1 – 25% 1 26 – 50% 1.5 51 – 75 % 2.5
75% and more 3.5 Rating on BFHI quantitative achievements
0 / 3.5
2C) Quantitative 2.3 What is the quality of BFHI programe implementation?
Criteria 2.3 Score 2.3 BFHI programme relies training of health workers 0.5
2.4 A standard monitoring system is in place 0.5
2.5 An assessment system relies on interviews of mothers 0.5
2.6 Reassessment system have been incorporated in national plans 0.5
2.7 There is a time-bound me to increase the number of BFHI institutions in the country 0.5
Total Score 1/2.5
Total Score 2A, 2B, 2C 1 / 10
14 | P a g e
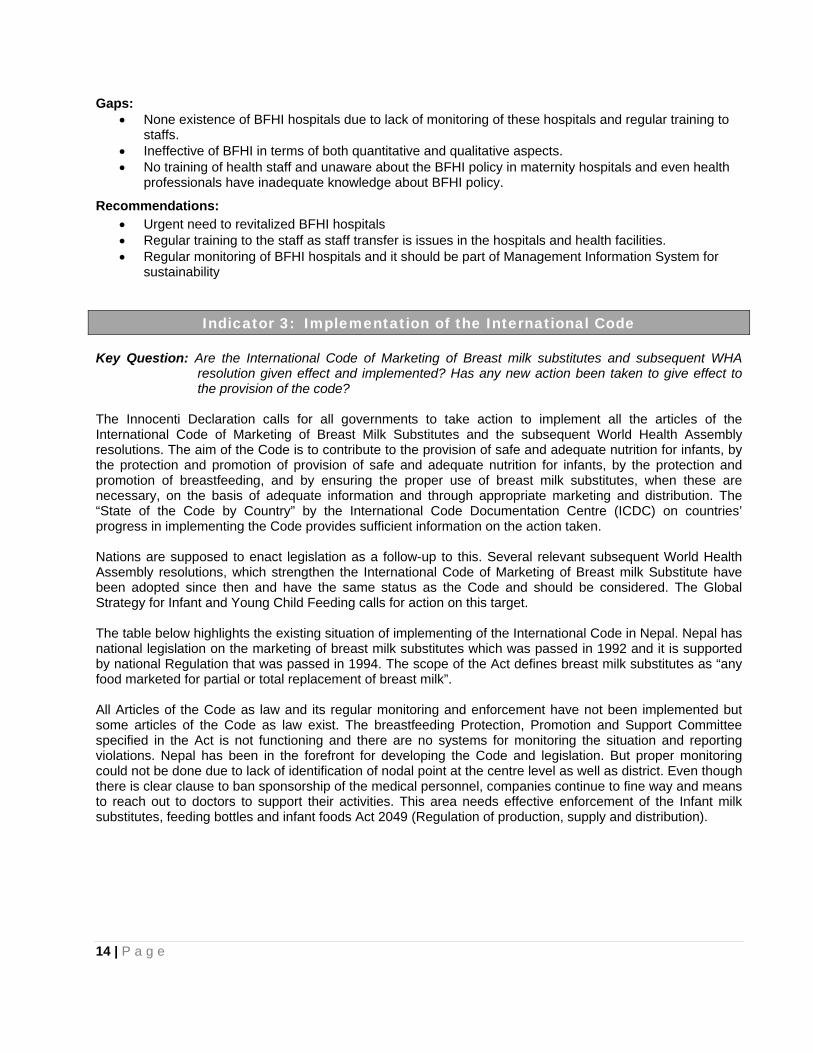
Gaps: • None existence of BFHI hospitals due to lack of monitoring of these hospitals and regular training to
staffs. • Ineffective of BFHI in terms of both quantitative and qualitative aspects. • No training of health staff and unaware about the BFHI policy in maternity hospitals and even health
professionals have inadequate knowledge about BFHI policy.
Recommendations: • Urgent need to revitalized BFHI hospitals • Regular training to the staff as staff transfer is issues in the hospitals and health facilities. • Regular monitoring of BFHI hospitals and it should be part of Management Information System for
sustainability
Indicator 3: Implementation of the International Code Key Question: Are the International Code of Marketing of Breast milk substitutes and subsequent WHA
resolution given effect and implemented? Has any new action been taken to give effect to the provision of the code?
The Innocenti Declaration calls for all governments to take action to implement all the articles of the International Code of Marketing of Breast Milk Substitutes and the subsequent World Health Assembly resolutions. The aim of the Code is to contribute to the provision of safe and adequate nutrition for infants, by the protection and promotion of provision of safe and adequate nutrition for infants, by the protection and promotion of breastfeeding, and by ensuring the proper use of breast milk substitutes, when these are necessary, on the basis of adequate information and through appropriate marketing and distribution. The “State of the Code by Country” by the International Code Documentation Centre (ICDC) on countries’ progress in implementing the Code provides sufficient information on the action taken. Nations are supposed to enact legislation as a follow-up to this. Several relevant subsequent World Health Assembly resolutions, which strengthen the International Code of Marketing of Breast milk Substitute have been adopted since then and have the same status as the Code and should be considered. The Global Strategy for Infant and Young Child Feeding calls for action on this target. The table below highlights the existing situation of implementing of the International Code in Nepal. Nepal has national legislation on the marketing of breast milk substitutes which was passed in 1992 and it is supported by national Regulation that was passed in 1994. The scope of the Act defines breast milk substitutes as “any food marketed for partial or total replacement of breast milk”. All Articles of the Code as law and its regular monitoring and enforcement have not been implemented but some articles of the Code as law exist. The breastfeeding Protection, Promotion and Support Committee specified in the Act is not functioning and there are no systems for monitoring the situation and reporting violations. Nepal has been in the forefront for developing the Code and legislation. But proper monitoring could not be done due to lack of identification of nodal point at the centre level as well as district. Even though there is clear clause to ban sponsorship of the medical personnel, companies continue to fine way and means to reach out to doctors to support their activities. This area needs effective enforcement of the Infant milk substitutes, feeding bottles and infant foods Act 2049 (Regulation of production, supply and distribution).
15 | P a g e
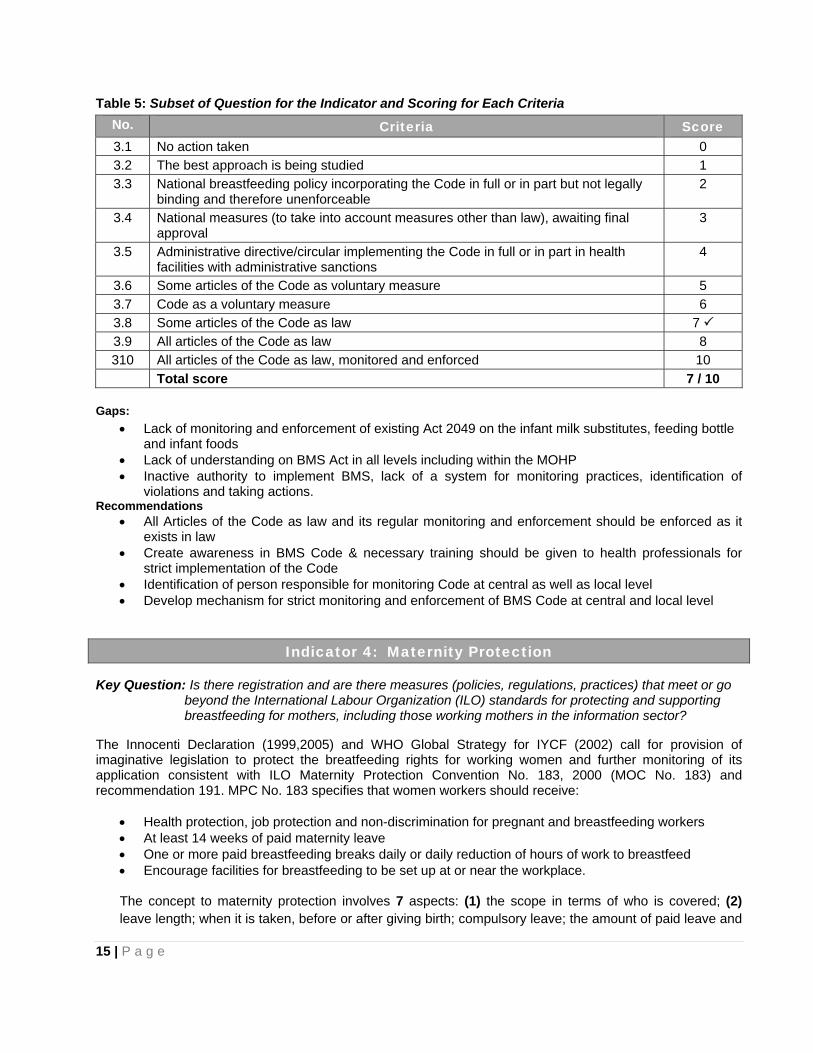
Table 5: Subset of Question for the Indicator and Scoring for Each Criteria
No. Criteria Score 3.1 No action taken 0 3.2 The best approach is being studied 1 3.3 National breastfeeding policy incorporating the Code in full or in part but not legally
binding and therefore unenforceable 2
3.4 National measures (to take into account measures other than law), awaiting final approval
3
3.5 Administrative directive/circular implementing the Code in full or in part in health facilities with administrative sanctions
4
3.6 Some articles of the Code as voluntary measure 5 3.7 Code as a voluntary measure 6 3.8 Some articles of the Code as law 7 3.9 All articles of the Code as law 8 310 All articles of the Code as law, monitored and enforced 10
Total score 7 / 10 Gaps:
• Lack of monitoring and enforcement of existing Act 2049 on the infant milk substitutes, feeding bottle and infant foods
• Lack of understanding on BMS Act in all levels including within the MOHP • Inactive authority to implement BMS, lack of a system for monitoring practices, identification of
violations and taking actions. Recommendations
• All Articles of the Code as law and its regular monitoring and enforcement should be enforced as it exists in law
• Create awareness in BMS Code & necessary training should be given to health professionals for strict implementation of the Code
• Identification of person responsible for monitoring Code at central as well as local level • Develop mechanism for strict monitoring and enforcement of BMS Code at central and local level
Indicator 4: Maternity Protection Key Question: Is there registration and are there measures (policies, regulations, practices) that meet or go beyond the International Labour Organization (ILO) standards for protecting and supporting breastfeeding for mothers, including those working mothers in the information sector? The Innocenti Declaration (1999,2005) and WHO Global Strategy for IYCF (2002) call for provision of imaginative legislation to protect the breatfeeding rights for working women and further monitoring of its application consistent with ILO Maternity Protection Convention No. 183, 2000 (MOC No. 183) and recommendation 191. MPC No. 183 specifies that women workers should receive:
• Health protection, job protection and non-discrimination for pregnant and breastfeeding workers • At least 14 weeks of paid maternity leave • One or more paid breastfeeding breaks daily or daily reduction of hours of work to breastfeed • Encourage facilities for breastfeeding to be set up at or near the workplace.
The concept to maternity protection involves 7 aspects: (1) the scope in terms of who is covered; (2) leave length; when it is taken, before or after giving birth; compulsory leave; the amount of paid leave and
16 | P a g e
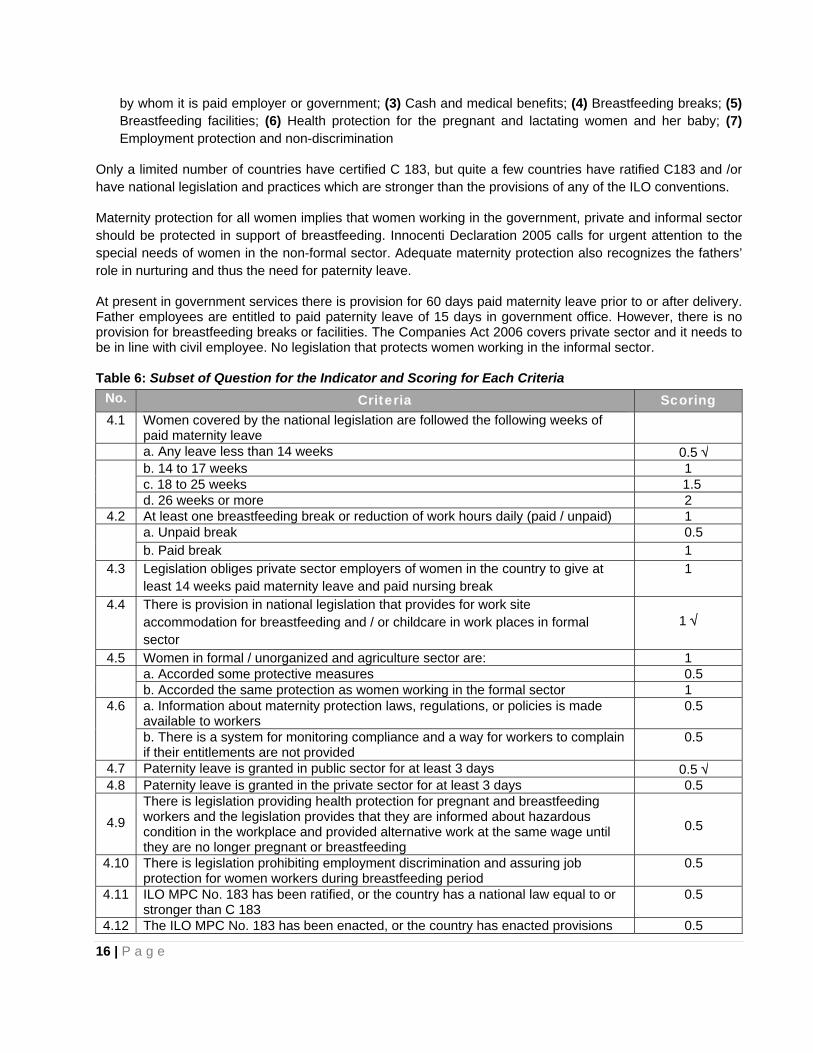
by whom it is paid employer or government; (3) Cash and medical benefits; (4) Breastfeeding breaks; (5) Breastfeeding facilities; (6) Health protection for the pregnant and lactating women and her baby; (7) Employment protection and non-discrimination
Only a limited number of countries have certified C 183, but quite a few countries have ratified C183 and /or have national legislation and practices which are stronger than the provisions of any of the ILO conventions.
Maternity protection for all women implies that women working in the government, private and informal sector should be protected in support of breastfeeding. Innocenti Declaration 2005 calls for urgent attention to the special needs of women in the non-formal sector. Adequate maternity protection also recognizes the fathers’ role in nurturing and thus the need for paternity leave.
At present in government services there is provision for 60 days paid maternity leave prior to or after delivery. Father employees are entitled to paid paternity leave of 15 days in government office. However, there is no provision for breastfeeding breaks or facilities. The Companies Act 2006 covers private sector and it needs to be in line with civil employee. No legislation that protects women working in the informal sector.
Table 6: Subset of Question for the Indicator and Scoring for Each Criteria
No. Criteria Scoring 4.1 Women covered by the national legislation are followed the following weeks of
paid maternity leave
a. Any leave less than 14 weeks 0.5 √ b. 14 to 17 weeks 1
c. 18 to 25 weeks 1.5 d. 26 weeks or more 2
4.2 At least one breastfeeding break or reduction of work hours daily (paid / unpaid) 1 a. Unpaid break 0.5
b. Paid break 1 4.3 Legislation obliges private sector employers of women in the country to give at
least 14 weeks paid maternity leave and paid nursing break 1
4.4 There is provision in national legislation that provides for work site accommodation for breastfeeding and / or childcare in work places in formal sector
1 √
4.5 Women in formal / unorganized and agriculture sector are: 1
a. Accorded some protective measures 0.5 b. Accorded the same protection as women working in the formal sector 1
4.6 a. Information about maternity protection laws, regulations, or policies is made available to workers
0.5
b. There is a system for monitoring compliance and a way for workers to complain if their entitlements are not provided
0.5
4.7 Paternity leave is granted in public sector for at least 3 days 0.5 √ 4.8 Paternity leave is granted in the private sector for at least 3 days 0.5
4.9 There is legislation providing health protection for pregnant and breastfeeding workers and the legislation provides that they are informed about hazardous condition in the workplace and provided alternative work at the same wage until they are no longer pregnant or breastfeeding
0.5
4.10 There is legislation prohibiting employment discrimination and assuring job protection for women workers during breastfeeding period
0.5
4.11 ILO MPC No. 183 has been ratified, or the country has a national law equal to or stronger than C 183
0.5
4.12 The ILO MPC No. 183 has been enacted, or the country has enacted provisions 0.5
17 | P a g e
equal to or stronger than C 183 Total score 2 / 10
Gaps: • Existing policy and legislation covers only government employees but it does not include private and
informal sectors • Inadequate or only 8 weeks of maternity leave and no provision of breastfeeding breaks.
Recommendations: • National policy and legislation on maternity leave should cover government, private and informal
sectors and efforts should be made for effective implementations • The maternity leave needs to be increased at least to 14 weeks as recommended by ILO and
provision for breast feeding breaks or provision of crèches at formal and informal sectors.
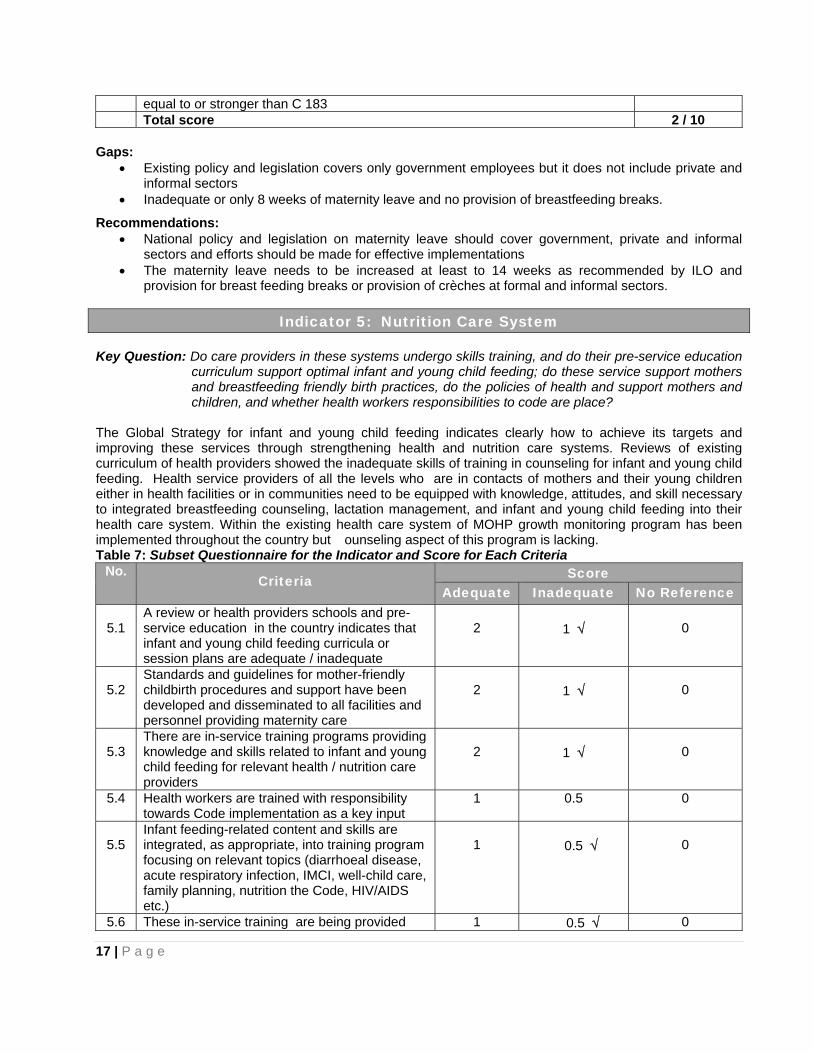
Indicator 5: Nutrition Care System Key Question: Do care providers in these systems undergo skills training, and do their pre-service education
curriculum support optimal infant and young child feeding; do these service support mothers and breastfeeding friendly birth practices, do the policies of health and support mothers and children, and whether health workers responsibilities to code are place?
The Global Strategy for infant and young child feeding indicates clearly how to achieve its targets and improving these services through strengthening health and nutrition care systems. Reviews of existing curriculum of health providers showed the inadequate skills of training in counseling for infant and young child feeding. Health service providers of all the levels who are in contacts of mothers and their young children either in health facilities or in communities need to be equipped with knowledge, attitudes, and skill necessary to integrated breastfeeding counseling, lactation management, and infant and young child feeding into their health care system. Within the existing health care system of MOHP growth monitoring program has been implemented throughout the country but ounseling aspect of this program is lacking. Table 7: Subset Questionnaire for the Indicator and Score for Each Criteria
No. Criteria Score
Adequate Inadequate No Reference
5.1 A review or health providers schools and pre-service education in the country indicates that infant and young child feeding curricula or session plans are adequate / inadequate
2
1 √
0
5.2
Standards and guidelines for mother-friendly childbirth procedures and support have been developed and disseminated to all facilities and personnel providing maternity care
2
1 √
0
5.3
There are in-service training programs providing knowledge and skills related to infant and young child feeding for relevant health / nutrition care providers
2
1 √
0
5.4 Health workers are trained with responsibility towards Code implementation as a key input
1 0.5 0
5.5
Infant feeding-related content and skills are integrated, as appropriate, into training program focusing on relevant topics (diarrhoeal disease, acute respiratory infection, IMCI, well-child care, family planning, nutrition the Code, HIV/AIDS etc.)
1
0.5 √
0
5.6 These in-service training are being provided 1 0.5 √ 0

18 | P a g e
throughout the country 5.7 Child health policies provide for mothers and
babies to stay together when one of them is sick 1 0.5 √ 0
Total score 4.5 / 10
Gaps: • Inadequate practical training in pre-services education and in-service training of health professionals • Inadequate standard and guidelines for mother-friendly childbirth procedures and support in health
facilities where maternity care are provided • Health workers are not adequately trained in practical skills on how to support mothers
Recommendations: • Review curriculum of health professionals, and integration of IYCF practical skills within the
curriculum • Develop standard guidelines on Mothers Friendly Childbirth and implement in all maternity services
through trained health workers. • Training of all health workers in practical skills to support breastfeeding mothers
Indicator 6: Mother Support and Community Outreach – Community – based
support for the pregnant and breastfeeding mother
Key Question: Do care providers in these systems undergo skills training, and do their pre-service education curriculum support optimal infant and young child feeding; do these services support mother and breastfeeding friendly birth practices, do the policies of health care service support mothers and breastfeeding friendly birth practices, do the policies of health care service support mothers and children, and whether health workers responsibilities to Code are in place?
Mother Support is defined by the Global initiative for Mother Support (GIMS) is “any support provided to mothers for the purpose of improving breastfeeding practices for both mother and infant and young child. Women need the support of evidence-based public health policies, health providers, employers, friends, family, the community, and particularly of their women and mothers.
Step 10 of BFHI and the Global Strategy for IYCF recognizes the need of mother support and peer support based in the community for succeeding in optimal breastfeeding practices.
Mother support not only covers mother to mother but it also includes accurate and timely information to help a woman build confidence; sound recommendations based up to date research; compassionate care before, during and after childbirth; empathy and active listening, hands-on assistance practical guidance. It also means support and counseling by health professional and health care workers including community outreach services for optimal feeding.
In Nepal, although mothers group do exist in all wards supported by Female Community Health Volunteers (FCHVs) but all women do ho have access to community-based support system and services on infant and young child feeding. Women get suggestion from FCHVs on importance of breastfeeding and complementary feeding but not practical supports for optimal IYCF. 65% of mothers deliver at home and 35% deliver at health facilities where they are supposed to receive infant and young child feeding after birth. This is not practiced in any hospital including those were certified as BFHI in 1997 – 1998 (BFHI assessment report 2011). Although IYCF services have national coverage and some project districts are focus more and others are not, hence practical skilled support to mothers for optimal IYCF is inadequate at National Level.
Strengthening coordination with BPNI for standardized skilled based trainings and learning form BPNI’s 20 years of intensive work in all aspects of IYCF could be a guiding cost effective and cultural similarities to Nepal (20 years of BPNI 1991-2011).

19 | P a g e
Table 8: Subset Questionnaire for the Indicator and Scoring for Each Criteria No.
Criteria Score Yes To some
degree N0
6.1
All pregnant women have access to community-based support system and services on infant and young child feeding
2
1 √
0
6.2 All women have access to support for infant and young child feeding after birth 2 1 √ 0
6.3 Infant and young child feeding support services have national coverage 2 1 √ 0
6.4
Community-based support services for the pregnant and breastfeeding women are integrated into an overall infant and young child health and development strategy (inter-sectoral and intra-sectoral)
2
1 √
0
6.5
Community-based volunteers and health workers possess correct information and are trained in counseling and listening skills for infant and young child feeding
2
1 √
0
Total score 5 / 10
Gaps: • Services unavailable on counseling pregnant mothers and breastfeeding mother in outreach clinic. • Lack of counseling and listening skills among community level workers. • Lack of crèche facilities at both government and private sectors. • IYCF support services are inadequate at all levels due to inadequate training on skills to support
breastfeeding mothers. Recommendations:
• Village level health workers should be trained for comprehensive intervention on IYCF to support at community level or outreach clinic.
• Supporting mothers for IYCF at community level is intensive workloads and health workers need performance based evaluation system to encourage its implementation for mothers support services.
Indicator 7: Information Support
Key Question: Are comprehensive Information, Education and Communication (IEC) strategies for improving infant and young child feeding (breastfeeding and complementary feeding) being implemented?
Behaviour Change is an important strategy, often used in counseling sessions, home visits, action-oriented group discussions and dramas focused on problem based solution. Information, education and communication (IEC) strategies are crucial to improve IYCF practices. IEC approaches include the use of electronic media, print media, interpersonal communication, dramas and community activities for motivational material to mothers, families and community to communicate important appropriate , action oriented messages or information .
A national Comprehensive IEC strategy includes messages on IYCF in Nepal. World Breastfeeding Week is celebrated nationally with some allocated budget for all 75 districts. Individual counseling and group education services related to IYCF are available within the health/nutrition care system or through community outreach but the implementation is not adequate.

20 | P a g e
Table 9: Subset Questionnaire for the Indicator and Scoring for Each Criteria No.
Criteria Score Yes To some
degree No
7.1 There is comprehensive national IEC strategy for improving infant and young child feeding 2 1 √ 0
7.2 IEC (e.g. World Breastfeeding Week) that include infant and young child feeding are being actively implemented at local levels
2
1 √ 0
7.3
Individual counseling and group education services related to infant and young child feeding are available within the health / nutrition care system or through community outreach
2
1 √
0
7.4
The content of IEC messages is technically correct, sound based on national or international guidelines 2 √ 1 0
7.5 A national IEC campaign or programme using electronic and print media and activities has channeled message on infant and young child feeding to targeted audiences in the last 12 months
2
1 √
0
Total score 6 / 10 Gaps:
• Inadequate national IEC strategy for improving IYCF and lack of sufficient budget to scale up interventions
• Inadequate implementation of individual and group education services in IYCF in health care system although the some activities in place in some projects areas.
• Inadequate national level IEC campaign / on IYCF to targeted audiences Recommendations:
• Advocacy to comprehensive National IYCF policy that include on IEC strategy • Adequate budget allocation to IEC on IYCF at central / district level
Indicator 8: Infant feeding and HIV
Key Question: Are the policies and programs in place to ensure that HIV-positive mothers are informed about the risks and benefits of different infant feeding options and supported in carrying out their infant feeding decisions?
The Global Strategy for IYCF recommended the country to have a comprehensive policy on infant and young child feeding that includes infant and HIV. National guidelines on HIV/AIDS Strategy and guidelines on Prevention of Mother-to-Child Transmission of HIV in Nepal addresses the Breastfeeding in relation to HIV/AIDS in terms of WHO on ART in adults and children, prevention of mother to child transmission (PMTCT). Although implementation of HIV and infant feeding counseling has improved, still inadequate counseling to HIV positive mothers is noted due to lack of adequate training on PMTCT at all levels.

21 | P a g e
Table 10: Subset Questionnaire for the Indicator and Scoring for Each Criteria No.
Criteria Score Adequate Inadequate No
Reference 8.1 The country has a comprehensive policy on infant and
young child feeding that includes infant feeding and HIV 2 √ 1 0
8.2 The infant feeding and HIV policy gives effects to the International Code / National Legislation 1 √ 0.5 0
8.3
Health staff and community workers receive training on HIV and infant feeding policies, the risks associated with various feeding options for infants of HIV-positive mothers and how to provide counseling and support
1
0.5 √
0
8.4
Voluntary and Confidential Counseling and Testing (VCCT) is available and offered routinely to couples who are considering pregnancy and to pregnant women and their parents
1 0.5 √ 0
8.5 Infant feeding counseling in line with current international recommendations and locally appropriate is provided to HIV positive mothers
1
0.5 √
0
8.6
Mothers are supported in making their infant feeding decisions with further counseling and follow-up to make implementation of these decisions as safe as possible
1
0.5 √
0
8.7
Special efforts are made to encounter misinformation on HIV and infant feeding and to promote, protect and support 6 months to exclusive breastfeeding and continued breastfeeding in general population
1 0.5 √ 0
8.8
On-going monitoring is in place to determine the effects of interventions to prevent HIV transmission through breastfeeding on infant feeding practices and over health outcomes for mothers and infants, including those who are HIV negative or of unknown status
1
0.5
0
8.9
The Baby-Friendly Hospital Initiative incorporated provision of guidance to hospital administrators and staff in settings with high HIV prevalence on how to assess the needs and provide support for HIV positive mothers
1
0.5
0
Total score 5.5 / 10
Gaps: • Weak advocacy and implementation of policy and guidelines on HIV and infant feeding at all levels • Lack of adequate trainings to health workers on infant feeding in HIV • No more BFHI hospitals and trained staff to support HIV mothers • Lack of monitoring system to determine the effects of intervention to prevent HIV transmission
through infant feeding practices who are unknown of the HIV status Recommendations:
• Review on existing situation of implementation of infant feeding in HIV • Revitalize BFHI and inclusion of training on PMTCT to health professionals • Strengthen implementation of policy and strategies on HIV and infant feeding with regular monitoring
22 | P a g e
Indicator 9: Infant feeding during Emergencies
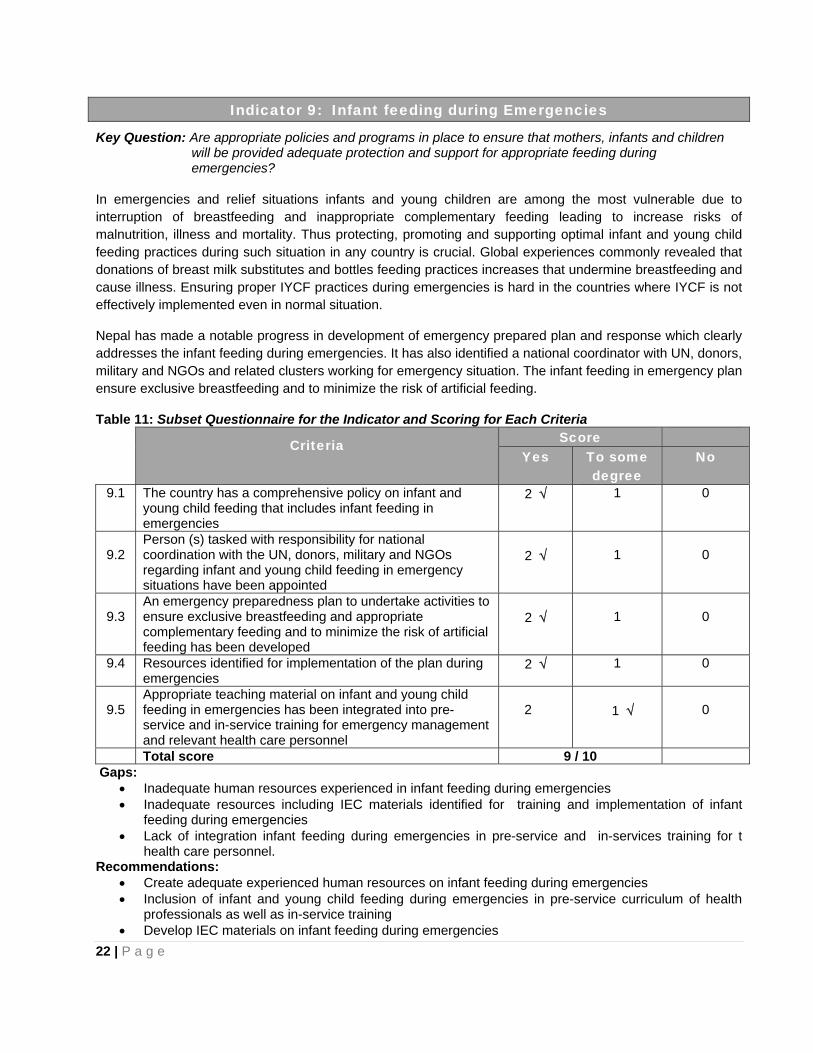
Key Question: Are appropriate policies and programs in place to ensure that mothers, infants and children will be provided adequate protection and support for appropriate feeding during emergencies?
In emergencies and relief situations infants and young children are among the most vulnerable due to interruption of breastfeeding and inappropriate complementary feeding leading to increase risks of malnutrition, illness and mortality. Thus protecting, promoting and supporting optimal infant and young child feeding practices during such situation in any country is crucial. Global experiences commonly revealed that donations of breast milk substitutes and bottles feeding practices increases that undermine breastfeeding and cause illness. Ensuring proper IYCF practices during emergencies is hard in the countries where IYCF is not effectively implemented even in normal situation.
Nepal has made a notable progress in development of emergency prepared plan and response which clearly addresses the infant feeding during emergencies. It has also identified a national coordinator with UN, donors, military and NGOs and related clusters working for emergency situation. The infant feeding in emergency plan ensure exclusive breastfeeding and to minimize the risk of artificial feeding.
Table 11: Subset Questionnaire for the Indicator and Scoring for Each Criteria
Criteria Score Yes To some
degree No
9.1 The country has a comprehensive policy on infant and young child feeding that includes infant feeding in emergencies
2 √ 1 0
9.2
Person (s) tasked with responsibility for national coordination with the UN, donors, military and NGOs regarding infant and young child feeding in emergency situations have been appointed
2 √
1
0
9.3
An emergency preparedness plan to undertake activities to ensure exclusive breastfeeding and appropriate complementary feeding and to minimize the risk of artificial feeding has been developed
2 √
1
0
9.4 Resources identified for implementation of the plan during emergencies
2 √ 1 0
9.5
Appropriate teaching material on infant and young child feeding in emergencies has been integrated into pre-service and in-service training for emergency management and relevant health care personnel
2
1 √
0
Total score 9 / 10 Gaps:
• Inadequate human resources experienced in infant feeding during emergencies • Inadequate resources including IEC materials identified for training and implementation of infant
feeding during emergencies • Lack of integration infant feeding during emergencies in pre-service and in-services training for t
health care personnel. Recommendations:
• Create adequate experienced human resources on infant feeding during emergencies • Inclusion of infant and young child feeding during emergencies in pre-service curriculum of health
professionals as well as in-service training • Develop IEC materials on infant feeding during emergencies

23 | P a g e
Indicator 10: Mechanisms of Monitoring and Evaluation System Key Question: Are monitoring and evaluation data routinely collected and used to improve infant and young child feeding practices? A system of monitoring and evaluation with Health and Nutrition Care System focused on IYCF is necessary in order to achieve national goals and target on IYCF. The table given below depicts the existing situation in Nepal on Monitoring and Evaluation
No. Criteria
Score
Yes To some degree
No
10.1 Monitoring and evaluation components are built into major infant and young child feeding me activities
2 1 √ 0
10.2
Monitoring or Management Information System (MIS) data are considered by programme managers in the integrated management process
2
1 √
0
10.3
Baseline and follow-up data are collected to measure outcomes for major infant and young child feeding programme activities
2
1 √
0
10.4 Evaluation results related to major infant and young child feeding programme activities are reported to key decision-makers
2 √ 1 0
10.5
Monitoring of key infant and young child feeding practices is built into a border nutritional surveillance and / or health monitoring system or periodic national health surveys
2
1 √
0
Total score 6 / 10
Gaps: • A national level monitoring and evaluation components are not built into major IYCF activities • Nutritional surveillance or health monitoring system does not include all key IYCF practices
Recommendation: • Integration of adequate indicators of infant and young child feeding into national health management
information Initiation and establishment of regular monitoring and evaluation system with focus on key IYCF

24 | P a g e
Table 13: Comparison with previous Assessment (Indicators 1-10)
Indicators 6 – 15 Score and Colour 2005 2008 2012
1. National Policy, Program and Coordination 5 5.5 8
2. Baby Friendly Hospital Initiative 3.5 2.5 1
3. Implementation of the International Code 7 7 7
4. Maternity Protection 0 2 2
5. Health and Nutrition Care 3.5 4.5 4.5
6. Community Outreach 3 4 5
7. Information Support 3 5
6
8. Infant Feeding and HIV 3.5 4 5.5
9. Infant Feeding during Emergencies 0 1 9
10. Monitoring and Evaluation 3 5 6
The comparison between data 2005, 2008 and 2012 indicators indicates some improvement in National policy, program & coordination, there is marked improved in infant feeding during emergencies and infant feeding and HIV but not much change in other indicators. As regards BFHI at present none of the hospitals are baby friendly & regarding maternity protection not much change has occurred. Indicators 1-10 need effective action plan specially revitalization of BFHI and maternity protection needs immediate & urgent attention. Infant feeding & HIV also needs attention particularly in implementation aspects.

25 | P a g e
Part II: Infant and Young Child Feeding Practices The part II include numerical data on each infant and young child feeding from a National level household survey. These indicators data is based on existing recent national level survey which is the actual result of how policy and program on IYCF contributed to the communities at large. The five indicators 11-15 are dealt with separately. In the description of each indicator, there is a key question addressing the indicator itself followed by the background. Then the results of these indicators are expressed in numeric value, with a percentage along with table. Then it followed by the rating and grading system as per WBTi guidelines. The indicator result is given in first column, WHO's key to rating and WBTi guidelines in the next column. WBTi toolkit helps to provide this scoring as well as colour rating and grading.
Indicator 11 Early Initiation of Breastfeeding Key question: Percentage of baby's breastfed within one hour of birth. Only 35% of babies delivered in health facility and rest (65%) are delivered at home in Nepal (NDHS, 2011). Breastfeeding is started late in many of home deliveries due to cultural or traditional beliefs and practices. Steps three of the Ten Steps of Successful Breastfeeding of Baby Friendly Hospital Initiative suggest the baby should be placed skin to skin with the mother in the first half an hour of delivery and offered the breast within the first hour in all normal deliveries. In the circumstances of a cesarean section the baby should be offered breastfeeding when mother is able to response and it happens within few hours of the general anesthesia however, mother needs support for timely initiation of breastfeeding and establishment of breastfeeding. The baby should start to breastfeed even before any routine procedure such as weighting, umbilical cord care, is performed. Timely initiation of breastfeeding helps for better temperature maintain of the newborn baby, enhances bonding between the mother and the baby, and also increases chances of establishing exclusive breastfeeding early and its success and thus reduce neonatal mortality. Although the early initiation of breastfeeding rate is improved from 35.4% in 2006 to 45% in 2011, still more than fifty percent (55%) mother do not initiate the breastfeeding within an hour of birth. Increasing this rate is crucial in order to establish exclusive breastfeeding and control pre-lacteal feedings. Early initiation of breastfeeding is very crucial to low birth weight babies as 12-30 percent of children are born with low birth weight in Nepal. Young and prime mothers need intensive breastfeeding support during initiation of breastfeeding. Indicator / Result: Early Initiation of Breastfeeding 45% Table 11: Early Initiation of Breastfeeding
Indicator 11 WHO’s Key to rating %
Existing Status %
IBFAN Asia Guideline for WBTi
Initiation of Breastfeeding (within 1 hour)
Scores Colour-rating Grading 0.1 – 29 3 RED D 30 – 49 45% 6 YELLOW C 50 – 89 9 B LUE B 90 – 100 10 GREEN A
Source: Nepal Demographic Health Survey 2011

26 | P a g e
Indicator 12: Exclusive Breastfeeding for the First Six Months Key Question: Percentage of babies < 6 months of age exclusively breastfed in the last 24 hours Although it has been strongly recommended that exclusive breastfeeding for the first six months is very crucial for survival, growth and development of infants and young children. It lowers the risk of diarrheal diseases. Nepal Demographic Health Survey (NDHS 2011) indicates that exclusive breastfeeding in children 0-6 months has increased to 70% in 2011, from 53% in 2006. Children who are not exclusively breasted are given water, other milks and foods in addition to breast milk. These negative practices are prevailing even among very young children.Indicator / Result: Exclusive Breastfeeding for first six months – 70%
Table 15: Exclusive breastfeeding
Indicator 12 WHO’s Key to rating %
Existing Status %
IBFAN Asia Guideline for WBTi
Exclusive breastfeeding for first six months
Scores Colour-rating Grading 0.1 – 11 3 RED D 12 – 49 6 YELLOW C 50 – 89 70% 9 B LUE B 90 – 100 10 GREEN A
Source: Nepal Demographic Health Survey 2011
Indicator 13: Median Duration of Breastfeeding Key Question: Babies are breastfed for a median duration of how many months? The Innocenti Declaration 1990 and the Global Strategy for Infant and Young Child Feeding 2002 recommend that babies continue to be breastfed for two years of age or beyond along with adequate and appropriate complementary foods starting after six months of age. Breast milk continues to be an important source of nutrition and fluids as well as immunological protection for the infant and the young child. Breastfeeding practice brings mother and child into a bonding and interaction between mother and child leading to an optimal development of the infant and young child.
It is interesting to note that median duration of breastfeeding in Nepal is exceptionally high i.e. 33.6 months and it needs to be maintained in future as well. Such longer duration of breastfeeding is the result of tradition throughout Nepal.
Indicator / Result: Median duration of breastfeeding – 33.6 months Table 16: Median duration of Breastfeeding
Indicator 13 WHO’s Key to rating
Existing Status
IBFAN Asia Guideline for WBTi
Median duration of breastfeeding
Scores Colour-rating Grading 0 .1 – 17 months 3 RED D18 – 20 months 6 YELLOW C21 – 22 months 9 B LUE B23 – 24 months 33.6 months 10 GREEN A
Source: Nepal Demographic Health Survey 2011
27 | P a g e
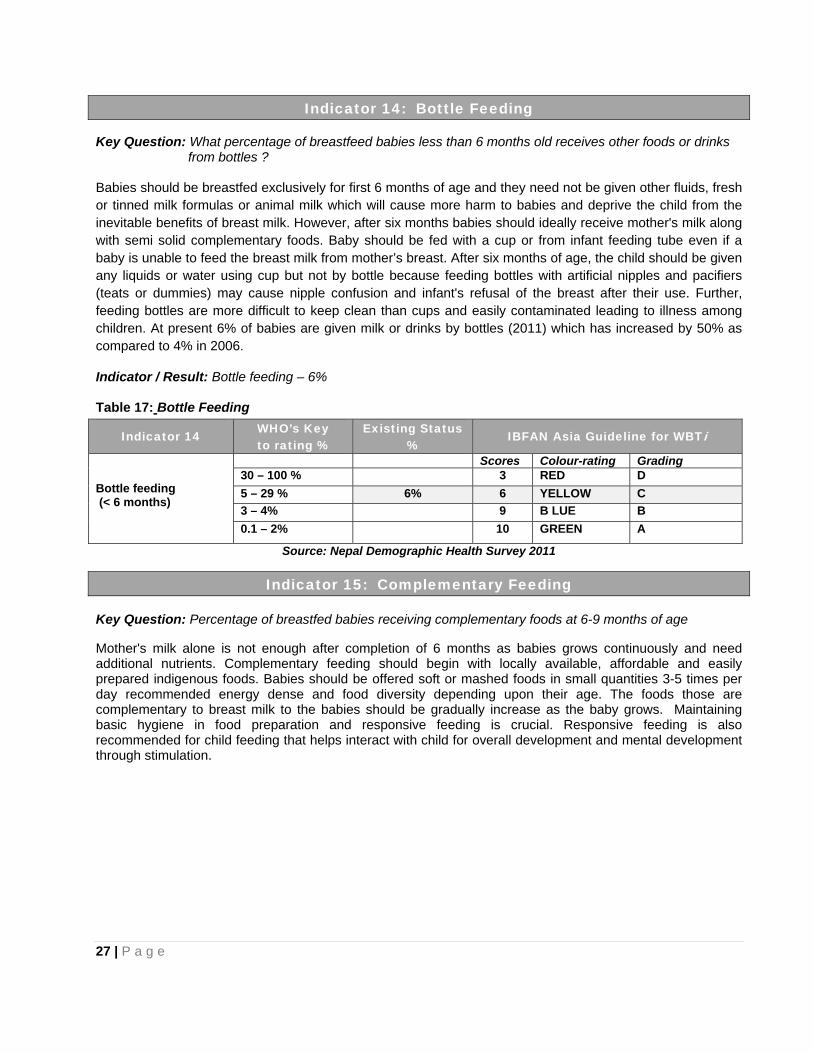
Indicator 14: Bottle Feeding
Key Question: What percentage of breastfeed babies less than 6 months old receives other foods or drinks from bottles ? Babies should be breastfed exclusively for first 6 months of age and they need not be given other fluids, fresh or tinned milk formulas or animal milk which will cause more harm to babies and deprive the child from the inevitable benefits of breast milk. However, after six months babies should ideally receive mother's milk along with semi solid complementary foods. Baby should be fed with a cup or from infant feeding tube even if a baby is unable to feed the breast milk from mother’s breast. After six months of age, the child should be given any liquids or water using cup but not by bottle because feeding bottles with artificial nipples and pacifiers (teats or dummies) may cause nipple confusion and infant's refusal of the breast after their use. Further, feeding bottles are more difficult to keep clean than cups and easily contaminated leading to illness among children. At present 6% of babies are given milk or drinks by bottles (2011) which has increased by 50% as compared to 4% in 2006.
Indicator / Result: Bottle feeding – 6% Table 17: Bottle Feeding
Indicator 14 WHO’s Key to rating %
Existing Status %
IBFAN Asia Guideline for WBTi
Bottle feeding (< 6 months)
Scores Colour-rating Grading 30 – 100 % 3 RED D 5 – 29 % 6% 6 YELLOW C 3 – 4% 9 B LUE B 0.1 – 2% 10 GREEN A
Source: Nepal Demographic Health Survey 2011
Indicator 15: Complementary Feeding Key Question: Percentage of breastfed babies receiving complementary foods at 6-9 months of age Mother's milk alone is not enough after completion of 6 months as babies grows continuously and need additional nutrients. Complementary feeding should begin with locally available, affordable and easily prepared indigenous foods. Babies should be offered soft or mashed foods in small quantities 3-5 times per day recommended energy dense and food diversity depending upon their age. The foods those are complementary to breast milk to the babies should be gradually increase as the baby grows. Maintaining basic hygiene in food preparation and responsive feeding is crucial. Responsive feeding is also recommended for child feeding that helps interact with child for overall development and mental development through stimulation.

28 | P a g e
Indicator / Result: Complementary feeding – 70% Table 18: Complementary Feeding
Indicator 15 WHO’s Key to rating %
Existing Status %
IBFAN Asia Guideline for WBTi
Complementary feeding (6-9 months)
Scores Colour-rating Grading 0.1 – 59 % 3 RED D 60 – 79 % 70% 6 YELLOW C 80 – 94% 9 B LUE B 95 – 100% 10 GREEN A
Source: Nepal Demographic Health Survey 2011
Comparison with previous assessments (Indicator 11 – 15) The comparison between data 2005, 2008 and 2012 indicate some improvements in the initiation of breastfeeding from 31% to 45%, exclusive breastfeeding from 68% to 70% where as slight decreasing trends observed in median duration of breastfeeding and babies receiving in complementary feeding from 68% to 70%. However, the bottle feeding has increased to 6%.
Table 19: Comparison with previous Assessments
Indicators Status in the assessment
in 2005
Status in the assessment
in 2008
Current status 2012
1. Percentage of babies breastfed within one hour of birth 31% 35.4% 45%
2. Percentage of babies < 6 months of age exclusively breastfed in the last 24 hours 68% 53% 70%
3. Babies are breastfed for a median duration of how many months 30 months 34 months 33.6 months
4. Percentage of breastfed babies less than 6 months old receiving other foods or drinks from bottle
3%
4%
6%
5. Percentage of breastfed babies receiving complementary foods at 6-9 months of age 66% 75% 70%
Indicators 11 – 15 needs effective action plan and unlikely to improve with current level of activity, we need to think seriously to have concrete plan of action with a budgetary provision and mechanism of accountability established.

29 | P a g e
Summary of Findings
Box 3: Part I:- IYCF Policies and Programs IYCF Practices Score
Indicator 1 : National Policy, me and Coordination 8 / 10 Indicator 2 : Baby Friendly Hospital Initiatives (Ten steps to successful breastfeeding)
1 / 10
Indicator 3 : Implementation of the International Code 7 / 10 Indicator 4 : Maternity Protection 2 / 10 Indicator 5 : Health and Nutrition Care System 4.5 / 10 Indicator 6 : Mother Support and Community Outreach – Community based Support for the pregnant and breastfeeding mother
5 / 10
Indicator 7 : Information Support 6 / 10 Indicator 8: Infant Feeding and HIV 5.5 / 10 Indicator 9 : Infant Feeding during Emergencies 9 / 10 Indicator 10 : Mechanisms of Monitoring and Evaluation System 6 / 10
Score (Part II) 54 / 100
Guidelines
Scores (Total) Part-II Colour-rating Grading Existing Situation 0 – 30 RED D
31 – 60 YELLOW C √ 61 – 90 BLUE B 91 – 100 GREEN A
Box 4: Part II:- Infant and Young Child Feeding (IYCF) Practices IYCF Practices Result Score
Indicator 11: Early initiation of breastfeeding 45% 6 / 10 Indicator 12: Exclusive breastfeeding for the first six months 70% 9 / 10 Indicator 13: Median duration of breastfeeding 33.3 months 10 / 10 Indicator 14: Bottle feeding 6% 6 / 10 Indicator 15: Complementary feeding 70% 6 / 10
Score (Part I) 37 / 50 Guidelines
Scores (Total) Part-I Colour-rating Grading Existing Situation 0 – 15 RED D 16 – 30 YELLOW C 31 – 45 BLUE B √ 46 – 50 GREEN A

30 | P a g e
Combined of Part I and Part II (Indicator 1 – 15): Policies and Programs and IYCF Practices
Box 5: Total score of Infant and Young Child Feeding Policies and Programs ; Practices (indicators 1 – 15) are calculated out of 150 Guidelines Scores (Total) Part-II Colour-rating Grading Existing Situation
0 – 45 RED D 46 – 90 YELLOW C
91 – 135 BLUE B √ 135 – 150 GREEN A
Part I indicators are in better position as compared to Part I. Situation has improved to some extent in policies & programs. Therefore out of 150 score, Nepal scored 91 just crossed the border of yellow & reached blue. Therefore there is room for more improvement and higher score to be achieved in future through intensive policy revision and plan for actions. Hence there is a need for rigorous implementation of IYCF from central level to local level as national movement & campaign.
Gaps and Recommendations:
• Existing Committee of BPCC at secretarial level in MOPH and inactive therefore reactivate existing National committee on Promotion, Protection and Support for Breastfeeding and provide necessary authority to Nutrition Technical Committee.
• National Nutrition Policy has not been fully implemented at national scale due to inadequate fund and lack of proper training therefore develop short term as well as long term plan of action for implementation of National Nutrition Policy with adequate fund.
• BFHI is non functional due to lack of regulating mechanism hence revitalize BFHI by advocacy, training and establishment of regular monitoring mechanism.
• Ineffective authority and lack of nodal person for enforcement of BMS Act therefore enforce BMS Act effectively; and initiate explicit monitoring mechanism at central and local level.
• Currently provision for maternity protection like leave, nursing breaks and crèches are inadequate so develop policy framework for protecting and supporting breastfeeding women working in government, private and in informal sectors including provision for crèches facility and nursing breaks.
• At present inadequate skill based training to health professionals in IYCF so incorporate adequate practical training in pre-service and in-service training of the health professionals in IYCF.
• Existing IEC strategy is inadequate in IYCF therefore develop and implement appropriate strategy with adequate fund for IEC on infant and young child feeding.
• Existing program on IYCF and HIV is inadequate in counseling practice so provide adequate counseling on IYCF for HIV positive women at all level.
• Inadequate experienced human resources in IYCF during emergencies therefore create adequate expertise for managing IYCF during emergencies.
• Currently National health monitoring system do not fully incorporate indicators in IYCF therefore there is a need of integration on IYCF indicators into national health and nutrition monitoring system.

31 | P a g e
Concluding Remarks and the Way Forward The 2012 Nepal Report reveals glaring gaps in both policy and programs that support infant and young child feeding with specific focus on breastfeeding. It is quite evident that not much has significantly changed over the past four years in the policy environment except that maternity benefits have been increased to some extent for women working in the government; such benefits are not available to women working in the private and the informal sectors. There has also been not much progress in providing crèches and nursing breaks as a support to breastfeeding and the number of crèches to support women working in the informal sector continues to be woefully inadequate. Program focus on breastfeeding and complementary feeding is just a lip service; serious inputs are needed to increase early initiation and exclusive breastfeeding. Increase in early initiation of breastfeeding in very slow with about 3% per year at present it is 45% only (NDHS 2011). According to NDHS data exclusive breastfeeding has increased for 53% (NDHS 2006) to 70% (NDHS 2011) but there is no supportive evidence as to what made it to increase. Rate of the complementary feeding has gone down to 70% from 75%. Babies < 6 months receiving other food or drink by bottle has increased by 50% from 4% (2006) to 6% (2011). These gaps can only be bridge through active implementation of the comprehensive recommendations being made in the report. These include skilled support to women at the time of birth and later to support breastfeeding. Policy on maternity entitlements must be announced for all breastfeeding women of the private sector, informal sector including self-employed women and agricultural labourers. The requisite numbers of quality crèches need to be set up. These require trained human and other adequate resources. Laws regulating the presence of crèches on worksites and nursing breaks need to be strictly implemented. Revitalize of BFHI hospital with adequate mechanism for skilled based training, monitoring, reassessment at regular interval with adequate budget allocation for long term activities. There has been some improvements in infant and young child feeding during emergencies as well as in infant feeding by the HIV mother as government has came out with guidelines for both feeding during emergencies and HIV. Some training has been already initiated in IYCF and HIV programs. Protection of breastfeeding from commercial sector continues to be a serious issue. Though the Nepal government has passed the Breastmilk Substitute Act 2049.The BMS Act is our obligation to protect women and children, stated in its objects and reasons; however implementing the Act does not figure in the business of the government programs either at centre or at district level where the action lies. The health system including health professionals at all levels are ignorant about this Act; there is no system for monitoring violations of BMS Code. Mechanisms to implement the Act need to be put in place immediately with manpower trained in monitoring the code. The real issue that will transform nutrition in Nepal, breastfeeding – early initiation & exclusive for the first six months timely introduction appropriate complementary food and prolonged breastfeeding for two years and beyond. But the problem is – we have no product, no gimmick, and no magic bullet. Decision makers need to understand that changing the paradigm of infant feeding is worth a huge investment. We know that the economic benefits of breastfeeding to a family and a nation are of exceptional value even in the terms of hard currency. We also know what works for enhancing breastfeeding practices; this is one to one or group skilled counseling along with the requisite systematic support. In spite of decades of studies and data showing that breastfeeding is the single most important intervention for survival and nutrition, it is deplorable that not much has been done except for a few posters, a little training, and lip service. Breastfeeding, to succeed, needs investment and a clear policy backed by adequate and clear action plan. At the policy level, breastfeeding interventions must be seen as an integral and central part of preventive care approach in the new Child Health Policy, having its own budget line, just as other interventions that are curative in nature have. Moreover, besides having its own budget line, breastfeeding interventions must be coordinated at a highest level, both at the level of Ministries and at National Policy Level as a centre to multi sectoral plan of action.

32 | P a g e
We hope that next three years would result in bridging these gaps and the next assessment in 2015 would reveal many more positive changes, and also move Nepal to a better colour. Nepal was in the YELLOW band in 2008. It has moved to BLUE band in 2012. The country should aspire to reach the GREEN as defined in the WBTi in order to ensure child born meets its right to survival with health.

33 | P a g e
ANNEX-1
The World Breastfeeding Trends Initiative ( WBTi ) Prof. Prakash S. Shrestha
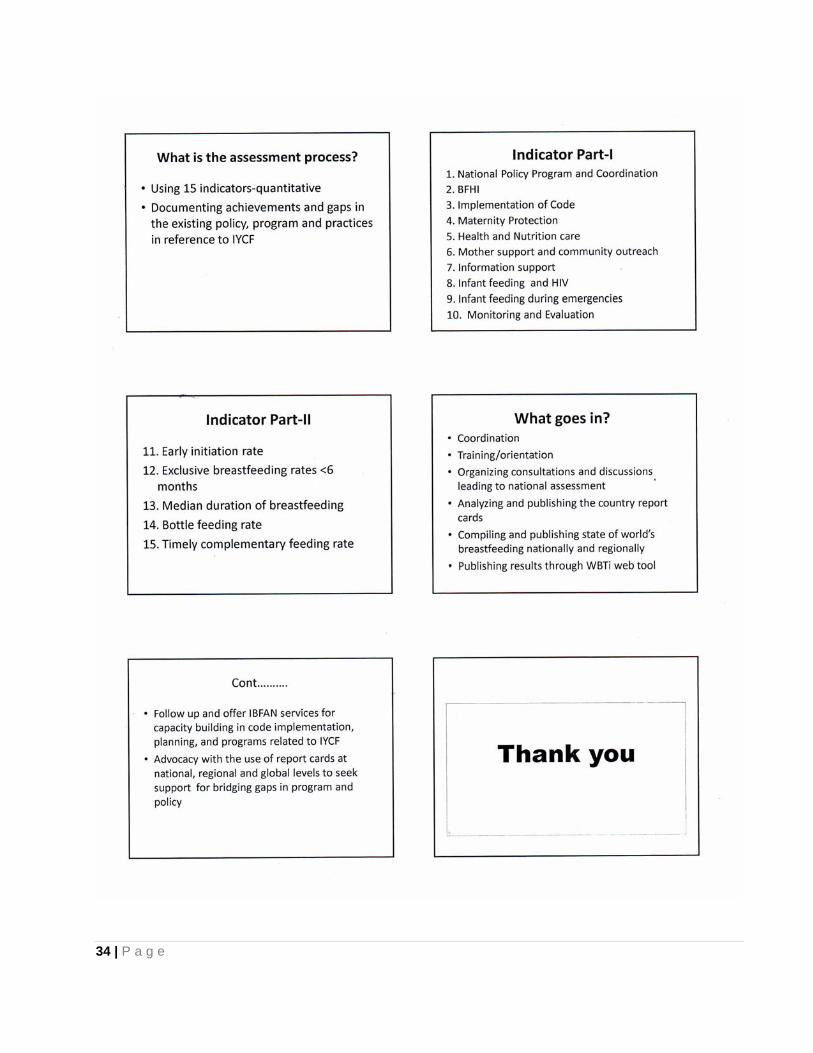
34 | P a g e

35 | P a g e
ANNEX-2 WBTi Assessment 2012
Dr. Kalpana Tiwari
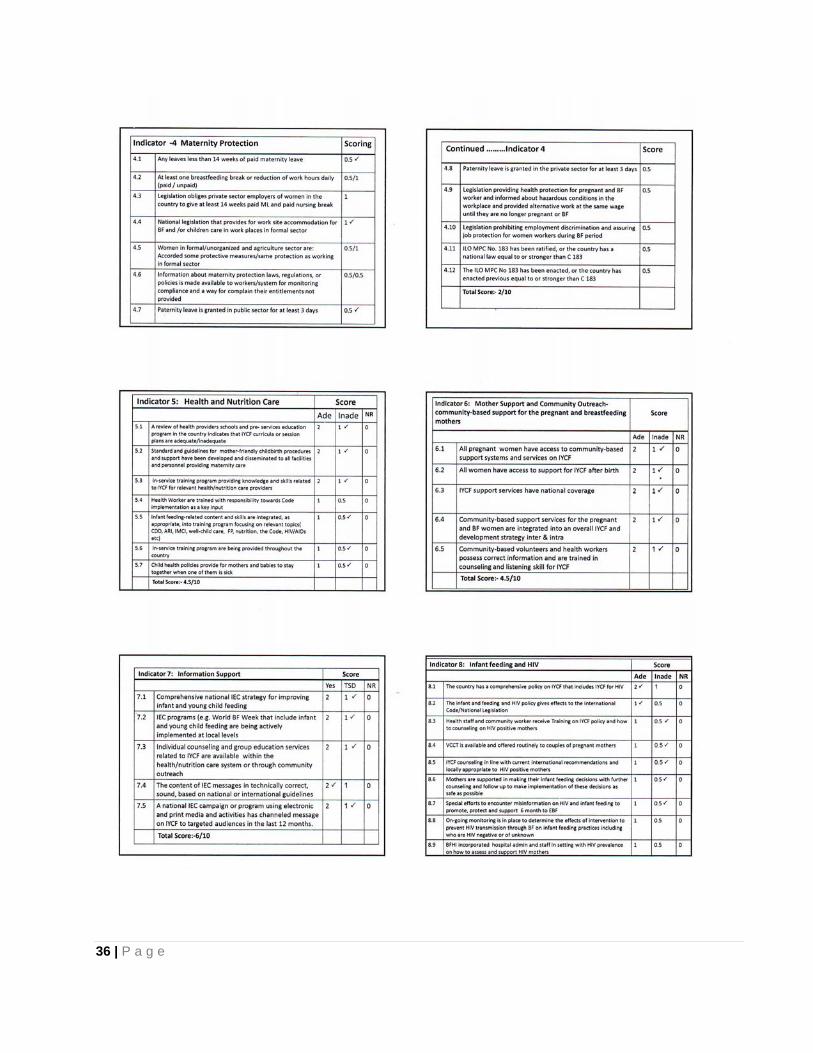
36 | P a g e
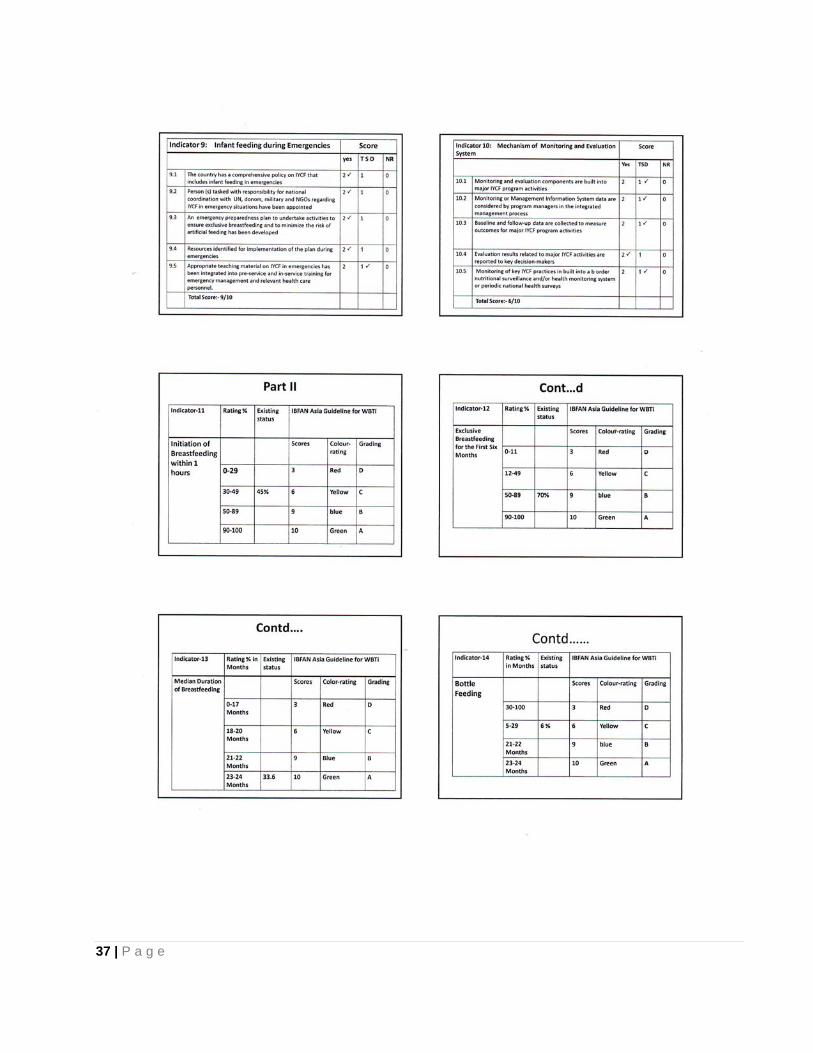
37 | P a g e

38 | P a g e
39 | P a g e
ANNEX – 3 PROGRAM SCHEDULE
Workshop on World Breastfeeding Trends Initiative ( WBTi ) – 2012
Venue:- Trade Tower Nepal (British College Building), Thapathali, Kathmandu Date:- 14th Mangsir 2069 (29th November 2012) Day:- Thursday Time:- 10:00 AM to 4:00 PM 10:00 – 10:15 Introduction of Participants 10:15 – 10:30 Welcome addressed – President, NEBPROF 10:30 – 11:00 Tea break 11:00 – 11:30 Highlights on WBTi – Prof. Prakash S. Shrestha 11:30 – 12:30 Presentation of WBTi – 2012 report – Mrs. Kalpana Tiwari 12:30 – 1:30 Lunch break 1:30 – 3:45 Discussion 1:45 – 4:00 Vote of thanks – Mrs. Tara Pokharel, General Secretary, NEBPROF Organized by:- Nepal Breastfeeding Promotion Forum (NEPROF)
40 | P a g e
ANNEX – 4 WBTi 2012 workshop held on 29th November 2012 at Kathmandu,Nepal Sr.No. Name of the Participant Organization 1. Prof. Fakir Chandra Gami Department of Child Health
2 . Prof. Prakash S Shrestha Nepal Breastfeeding Promotion Forum (NEBPROF)
3. Mrs. Ram Laxmi Doubadel “
4. Mrs. Sunita Bhattarai “
5. Mrs. Sushila Adhikari T. U. Teaching Hospital
6. Mrs. Krishna Shova Shrestha “
7. Dr. Indira Satyal Perinatal Society of Nepal (PESON)
8. Dr. Kalpana Tiwari Nutrition Health Research and Community Services (NHRCS)
9. Mrs. Nira Joshi New Era
10. MS. Sharmila Dhakal NHRCS
11. Dr.Sakura Shrestha Sidhi Memorial Hospital
12. Mrs.Sarita Shrestha NEBPROF
13. Mr.Sumit Karn Nutrition Section, Child Health Division
14 Mrs. Sharmila Parajuli NBPROF
15. Dr. Binod Man Shrestha Kanti Children’s Hospital
16. Dr. Jyoti Ratna Dhakhwa Nepal Paediatric Society (NEPAS)
17. Dr. Dhan Raj Aryal Maternity Hospital
18. Mrs. Tulashi Adhikari Maharajganj Nurshing Campus
19. Dr.Luna Bajaracharjee Department of Child Health, IOM
20. Dr. Daman Raj Poudel Department of Child Health, IOM
21. Dr. Arun Sharma “
22. Dr. Prabina Shrestha T.U.Teaching Hospital, IOM
23. Dr. Surya Bahadur Shrestha “
24. Dr. Kalpana Subedi Kanti Children’s Hospital
25. Mrs. Tara Pokharel Maharajganj Nursing Campus
26. Dr. Sarala Shrestha Dean Office, Institute of Medicine
27. Prof. Ramesh Kant Adhikari Kathmandu Medical College
28. Dr. Laxman Shrestha Department of Child Health
29. Prof. Dharma Saran Manandhar Mother and Infant Research Activity (MIRA)
30. Mr .Bachu Wagle NEBPROF
41 | P a g e
References
1. Arun Gupta, Radha Holla, J P Dadhich, Shoba Suri, Marta Trejos, and Joyce Chanetsa 2012. The status of policy and programs on IYCF in 40 countries. Reprinted in Health Policy and Planning: A Journal on health in development
2. 20 years of BPNI 1991-2011. An overview of BPNI's accomplishments: Analytical Report of Effectiveness Impact created by BPNI on Policies and s of Breastfeeding and Infant and Young Child Feeding Practices in India.
3. BPHI/IBFAN 2012. "The 4 in 1' training me –Capacity building initiative for building health/nutrition worker's skills in IYCF counseling.
4. Nepal Demographic and Health Survey, 2006 5. Nepal Demographic and Health Survey 2011 6. National Nutrition policy and Strategy 2004 7. National Neonatal Policy and Strategy 2004/ 2008 8. National Plan for Action on Nutrition (NPAN-Draft) 2007 9. Nutrition Training Manual for VHW, HA, NAM, CMA 2006 10. School Health and Nutrition Training Manual 2007 11. Newborn Care Training Guide for PCL Nursing 2005 12. Newborn Care Training for MBBS 2005 13. Survey results for Community Based Maternal Neonatal Care2007 14. Curriculum for MBBS, Institute of Medicine 2008 15. National Guidline on Paediatric HIV and AIDS 2006 16. Maternal and Neonatal Care Protocol/ Guidelines for Nurses of TUTH 2006 17. Anti retroviral Drugs for Treating Pregnant Women and Preventing HIV Infection in Infants 2004 18. National Policy on Skilled Birth Attendants 2005 19. Small Area Estimation of Poverty, caloric Intake and Malnutrition in Nepal 2006 20. Curriculum for MD (Paediatrics), Institute of Medicine 1996 21. Nepal Family Health Survey 1996 22. Neonatal and Infant Nutrition Training Manual for Health Workers 2007 23. National Maternity Care Guideline Nepal 2004 24. Tenth National Five Year Plan 1996 25. Neonatal and Infant Nutrition Training Manual for Health Workers 2007 26. National Maternity Care Guidelines Nepal 27. Tenth National Five Year Plan 2005 28. National Essential Maternal and Neonatal health Care Services Package for Nepal 2005 29. A Report of Nepal Maternal and neonatal and Neonatal Forum 2005 30. Nepal Breatmilk Substitute Act 2049(1992) 31. Nepal Breastmik Substitute law 2051 (1994) 32. SAARC Model Code for Protection of Breastfeeding and Young Child Nutrition 1996 33. National Breastfeeding Committee, Documents 1998 34. BFHI Activities, Nepal Pediatric Society 1998 35. International Code Document1994 36. Civil Service Act 2000 37. Maternity Benefit Act 2006 38. C183 Maternity Protection Convention (ILO) 2000 Document 39. CBIMCI me Health Sector Strategy 2004 40. Community Based Maternal Newborn Care Package (CBMNCP) 2007 41. Curriculum of Certificate Level Nursing, Institute of Medicine 2003 42. Curriculum of Certificate Level Nursing, Stupa Nursing College 2006 43. Annual Report Department of Health Services 2064 (2006/2007) 44. Annual Report Department of Health Services,2007/2008 45. Annual Report 2011 / 12 46. Statement published by Nepal Government during flood at Koshi Region 2008 47. Curriculum for Certificate Nursing BPKIHS 2003 48. Curriculum for Certificate Nursing, BPKIHS 2003 49. Three Year Interim Plan Government of Nepal 2064-2067 (2007-2010) 50. Curriculum of ANM, CTEVT 2000 51. Curriculum for CMA, CTEVT 2000 52. Curriculum of B.SC Nursing , Institute of Medicine2005 53. Curriculum for M.Sc Nursing, Women Health and Development, Institute of Medicine 2003

42 | P a g e
54. Preventing Mother to Child Transmission of HIV in Nepal 2004 55. Curriculum for M.Sc.Nursing Paediatrics, Institute of Medicine 2003 56. Curriculum for MD (Paediatrics), BPKIHS 2000 57. National Safe Motherhood and Newborn Health Long Term Plan (2006-2017) 2006 58. National Neonatal Long Term Plan (2005-2017) 2006 59. Health Sector Strategy: An Agenda for Reform 2004 60. National Reproductive Health Strategy 1998 61. Adapted from A Field Guide to designing a health communication strategy: A Resource for Health
Communication Professionals. Johns Hopkins Bloomberg School of Public Health/Center for Communications 62. Accelerating Progress in Reducing Maternal and Child Undernutrition in Nepal 2012:A review of global evidence
of essential nutrition interventions for the Nepal Health Sector Plan II and Multispectral Plan of Action for Nutrition
63. National Strategy on HIV/AIDs Nepal 2011, MOHP 64. Nutrition Assessment and Gap Analysis 2009 65. National Communication Strategy on Maternal, Newborn and Child Health 2011-16 66. Interagency Nutrition Cluster Contingency Prepared and Response Plan 2011 67. Multi-sectoral Nutrition Plan 2012 For Accelerating the Reduction of Maternal and Child Under-nutrition in Nepal
Volume I (NPC-2012) 68. MoHP. Assessemnt and Stregthening the Implementation of the Code on Breast Milk Substitutes and the Baby
Friendly Hospital Initiative.2011 69. Nira Joshi, Kingsley E. Agho, Michael J. Dibley, Upul Senarath and Kalpana Tiwari “Determinants of
inappropriate complementary feeding practices in young children in Nepal: secondary data analysis of demographic and Health Survey 2006” Vol. 8, Maternal & Child Nutrition 2012
70. Pandey S. Tiwari K., Senarath U, Agho K. E. and Dibley M. J. (2010) “Determinants of Infant and Young Child Feeding Practices in Nepal: secondary data analysis of Demographic and Health Survey 2006. Food and Nutrition Bulletin 31, 334-351
