thom skalko and richard williams's presentation from atra
TRANSCRIPT
HR 1906: Access to Rehabilita4on Therapy Act of 2015 and the Role of the Recrea4onal Therapist in
Public Policy
Thomas Skalko, Ph.D., LRT/CTRS, FDRT Richard Williams, Ed.D., LRT/CTRS, FDRT
Session Objec?ves
Upon comple?on of this session, par?cipants will be able to:
1) describe the intent of the Access to Inpa?ent Rehabilita?on Therapy Act of 2015 2) iden?fy at least three ini?a?ves the RT profession has taken to influence public policy 3) Iden?fy their elected officials 4) iden?fy 2 ac?ons to ini?ate efforts in their state 5) demonstrate the ability to draU an advocacy leVer to individual Representa?ves and Senators on the Access to Inpa?ent Rehabilita?on Therapy Act of 2015

Introduc?on
• Public policy is a lot of fuss and bother – Technical – Boring – Expensive
• Why we care, and why you should, too.

Introduc?on
• “You have to be very careful if you don’t know where you’re going because you might not get there.” – Yogi Berra

Introduc?on
• “When you come to a fork in the road, take it.” – Yogi Berra

Introduc?on
• Recrea?onal Therapy is once again at a fork. – Are we a health care profession or not?
– Clinical does not describe a place, it describes a specific process, and it describes specific outcomes.

Some Context • Health care professions
are beholden to an overlapping web of regula?ons and expecta?ons – Clients and their families – Centers for Medicare and Medicaid Services
– Private Insurers – Joint Commission – CARF – Others

Some Context • We have a push and a pull
problem – Health care insurers value
only services that deliver ac?ve treatment and func?onal outcomes
– Recrea?onal Therapy is not always viewed by health care insurers as a profession that delivers ac?ve treatment and func?onal outcomes
– Not all Recrea?onal Therapists in health care sedngs focus on ac?ve treatment and func?onal outcomes

Some Context • Ac?ve Treatment
– Includes preven?on services
– Defined by the Centers for Medicare and Medicaid Services (CMS)
• Provided under an individualized treatment or diagnos?c plan;
• Reasonably expected to improve the pa?ent's condi?on or for the purpose of diagnosis; and
• Supervised and evaluated by a physician
• Func?onal Outcomes – ICF Categories
• Cogni?on • Mobility • Self-‐care • Gedng along with others • Life ac?vi?es • Par?cipa?on in the community
– Ac?vi?es of Daily Living • Mobility • Communica?on • Self-‐care

CMS is very specific what it WILL NOT pay for
• Services meant only for diversion
• Recreation for recreation’s sake

Context

Centers for Medicare and Medicaid Services (CMS)
• CMS is a federal agency that determines how approximately $1 trillion worth of federal health care funds are spent.
$1,000,000,000,000


How much is $1 Trillion?
• It would pay Lebron James’ $20 million annual salary for 50,000 years

How much is $1 Trillion?
• It would pay Lebron James’ $20 million annual salary for 50,000 years

• To put that in perspec?ve, King Tut was walking around less than 4,000 years ago.
Wait, it gets beVer…
• Private insurers largely take their cues from CMS regula?ons
• Private insurers outspend the federal government on health care nearly 2-‐to-‐1.
$1 trillion (feds) + $2 trillion (private) $3 trillion (WOW!)

Who cares?
• Were CMS to consider recrea?onal therapy a covered service across health care – More RT jobs – BeVer paying RT jobs – Greater access to a greater range of clients – Increased ability to help more and more clients

This is why we care, and this is why we invite you to care, too.

Some Historical Context

ATRA Medicare Project
• An attempt to have Centers for Medicare and Medicaid Services (CMS) clarify that Recreational Therapy is a covered service in:
• In-patient rehabilitation facilities (IRFs) • In-patient psychiatric facilities (IPFs) • Skilled-nursing facilities (SNFs)

How CMS Spends Money
– In written communications, CMS repeatedly communicated that RT is a covered service in:
– In-patient rehabilitation facilities – In-patient psychiatric facilities – Skilled-nursing facilities.

ATRA’s First Strategy
• Request in writing from ATRA and from legislators to issue clarification in regulatory language regarding RT’s coverage in – In-patient rehabilitation facilities – In-patient psychiatric facilities – Skilled-nursing facilities.

Letters from Congress to CMS

Letters from Senate to CMS

ATRA’s Next Solution -Introduce Legislation
• ATRA Medicare Project • This clarification would have been budget
neutral • Costs were built into the prospective payment
systems for each setting. • CMS did not respond to this strategy.

ATRA’s Next Solution -Introduce Legislation
HR 4248 was designed to direct CMS to issue guidance through regulations and/or the Medicare Benefits Policy Manual that recreational therapy provided in IRFs, IPFs, and SNFs is a covered service for Medicare beneficiaries when: • Required by the patient’s condition • Prescribed by a physician • Part of a plan of care

ATRA’s Next Solution -Introduce Legislation
• HR 4248 • Approximately 50 Congressional Representatives co-signed on HR 4248 with
• Congresswoman Tauscher
• Congressman English • That is 50 out of 435 Congressional Representatives
ATRA’s Next Solution -Introduce Legislation
• New elections, new Congress
• After the elections, the 110th Congress ended
• HR 4248 died on the books
CMS Review of the Three Hour Rule (2009)
• CMS issued a call for comments about the language of the 3-‐hour rule that applies to inpa?ent rehabilita?on services
• What is the 3-‐Hour Rule? – Known officially as the “intensity of therapy requirement”
– To qualify for in-‐pa?ent rehabilita?on, pa?ents must be able to benefit from 3 hours of intensive therapy 5 of 7 days per week
3-Hour Rule
• “While most patients requiring an inpatient stay for rehabilitation need and receive at least three hours a day of physical and/or occupational therapy, there can be exceptions because an individual patient’s needs vary. In some instances, patients who require inpatient hospital rehabilitation services may need, on a priority basis, other skilled rehabilitative modalities such as speech-language pathology services, or prosthetic-orthotic services and their state of recovery makes the concurrent receipt of intensive physical therapy or occupational therapy services inappropriate.”

ATRA’s Suggested Edits
• “While most pa?ents requiring an inpa?ent stay for rehabilita?on need and receive at least three hours a day of physical and/or occupa?onal therapy, there can be excep?ons because an individual pa?ent’s needs vary. In some instances, pa?ents who require inpa?ent hospital rehabilita?on services may need, on a priority basis, other skilled rehabilita?ve modali?es such as speech-‐language pathology services, or prosthe?c-‐ortho?c services or recrea4onal therapy and their state of recovery makes the concurrent receipt of intensive physical therapy or occupa?onal therapy services inappropriate.”

Support and Opposition Support
• American Academy of Physical Medicine and Rehabilitation
• American Medical Rehabilitation Providers Association
• Fund for Access to Inpatient Rehabilitation
• Harborview Medical Center • Rehabilitation Institute of
Michigan • Pennsylvania Association of
Rehabilitation Facilities • Cleveland VMAC
Opposition • AOTA

Outcome of ATRA’s Effort to Amend 3-Hour Rule
• CMS did not support the inclusion of RT under the 3 hour rule.
• “Further, we do not believe that it is appropriate to mandate that all IRFs provide recreational therapy, music therapy, or respiratory therapy services to all IRF patients, as such services may be beneficial to some, but not all, patients as an adjunct to other, primary types of therapy services provided in an IRF (physical therapy, occupational therapy, speech-language pathology, and prosthetics/orthotics therapy).”

The Current Problem
• CMS rejected the input and removed the professional judgment of the physician and treatment team to determine which therapeu?c services can be used to count toward the 3 Hour Rule
• The ruling also has denied providers and consumers access to qualified modali?es in the IRF sedng.

HR 4755 -‐ ‘‘Access to Inpa?ent Rehabilita?on
Therapy Act of 2014’’
• To amend ?tle XVIII of the Social Security Act to include RT among the therapy modali?es that cons?tute an intensive rehabilita?on therapy program in inpa?ent rehabilita?on
• Introduced in April of 2014, the 112th Congress ended and the bill died on the books with 5 co-‐sponsors.

HR 1906 -‐ ‘‘Access to Inpa?ent Rehabilita?on Therapy Act of 2015’’
• Amends ?tle XVIII of the Social Security Act to include RT among the therapy modali?es that cons?tute an intensive rehabilita?on therapy requirement in an inpa?ent rehabilita?on hospital or unit.

What does HR 1906 do?
• It amends the Social Security Act to include RT among those modali?es that cons?tute intensive rehabilita?on services.
• Out since February 2015. Currently 2 co-‐sponsors: – Thompson, (R-‐PA) – BuVerfield, (D-‐NC)
• Imagine the subsequent extension of this bill across sedngs and funding sources.
Talking Points for HR 1906
Iden?fying Your Elec?ve Representa?ve
1. Get out your phone, tablet, or computer 2. Go to house.gov & enter your 9-‐digit zip code
– Usps.com has a search feature if you need it
3. Go to votesmart.org and search the name of your representa?ve

Iden?fying Your Elected Representa?ve
4. Open a new document (or hand write), and ?tle it “My Elected Representa?ve” 5. On votesmart.org, read your Rep.’s bio and record the following:
– Washington, DC and District office addresses and phone numbers
– Poli?cal party – Birthplace – Schools aVended – Current legisla?ve commiVee assignments and subcommiVees (note any commiVee chairs)
– Anything else interes?ng (something you have in common)

Iden?fying Your Elected Representa?ve
6. Read your Rep.’s Votes, Posi?ons, & Ra?ngs – Get a feel for his or her poli?cal philosophy – Record anything noteworthy

• House – Tim Murphy (18th PA) – Robert Dold 10th (IL) – Frank Guita (1st NH) – Gus Bilirakis (12th FL) – Mimi Walters (45th CA)
• Senate – Richard Burr (NC) – Thom Tillis (NC) – Tammy Baldwin (WI) – Roger Wicker (MS) – Richard Durbin (IL) – Richard Blumenthal (CT) – Christopher Murray (CT) – Johnny Isakson (GA)

2015 Bill
• House Ways and Means subcommiVee/health

“The Ask”
• Ask your Representa?ve to join Congressman Glenn (GT) Thompson and Congressman GK BuVerfield to “co-‐sponsor” the Access to Inpa?ent Rehabilita?on Therapy Act of 2015
• Ask your Senators to sponsor a Senate version of the Access to Inpa?ent Rehabilita?on Therapy Act of 2015 – There is no Senate companion bill as of today.
• Remember, the Access to Inpa?ent Rehabilita?on Therapy Act of 2015 is budget neutral – It will not cost the Federal Government more than is currently spent for pa?ents
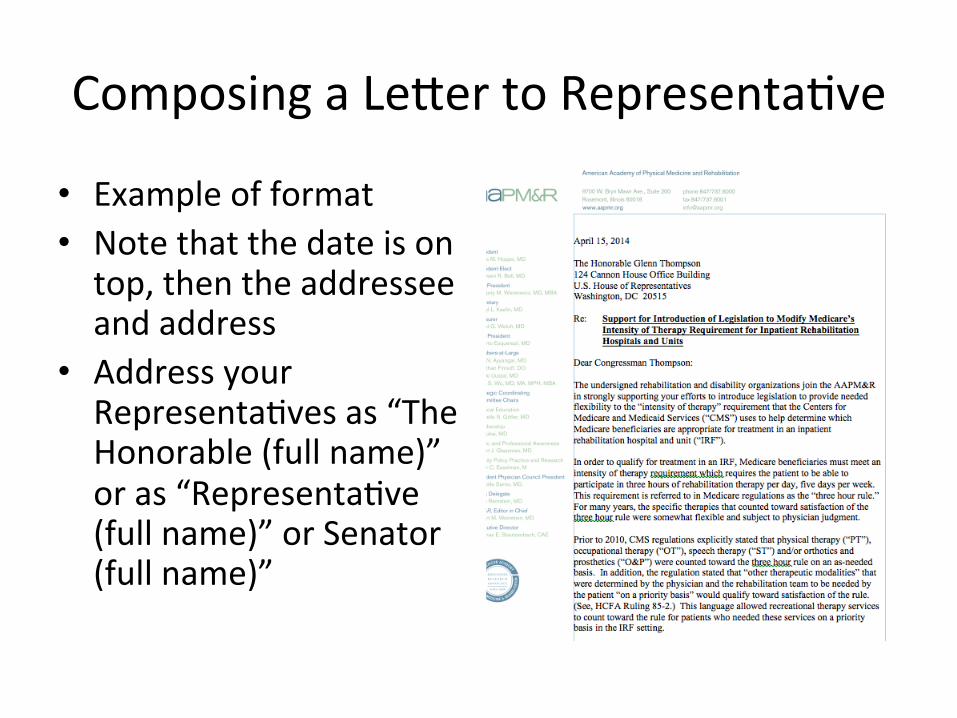
Composing a LeVer to Representa?ve
• Example of format • Note that the date is on top, then the addressee and address
• Address your Representa?ves as “The Honorable (full name)” or as “Representa?ve (full name)” or Senator (full name)”
Composing a LeVer to Representa?ve
(1) Explain briefly why you are wri?ng and who you are. List your creden?als. Request a response, so you must include your name and address, even when using email.)

Composing a LeVer to Representa?ve
(2) Provide more detail. Be factual not emo?onal. Provide specific rather than general informa?on about how the topic affects you and others. If a certain bill is involved, cite the correct ?tle or number whenever possible.

Composing a LeVer to Representa?ve
(3) Close by reques?ng the ac?on you want taken: a vote for or against a bill, change in general policy, or a co-‐sponsorship.
In this case, “I am asking you to join Representa?ves Thompson and BuVerfield in co-‐sponsoring HR 1906”. DO NOT SEND A PHYSICAL LETTER VIA U.S. POSTAL SERVICE Example LeVer: hVps://www.atra-‐online.com/assets/pdf/policy/federal-‐public-‐policy/HR_1906_advocacy_email_Congressperson.pdf

Visi?ng Elected Representa?ves
• Visi?ng Elected Representa?ves (In DC or at home)
• Scheduling – Dos and Don’t when Advoca?ng for Recrea?onal Therapy during a visit with an elected official
– Following up

Do’s and Don’ts • DON’T
– be late – make things up – come with a personal agenda (one visit; one message)
– chew gum – wear a ball cap
• DO – pre-‐visit research on your elected official
– dress professionally – leave your personal poli?cs at the door
– share stories – turn off cell phone – follow up regarding any addi?onal informa?on requested
– send a thank you email

Packet Contents
Copy of the bill Marke?ng Sheets (To be on the ATRA site at soon)
– Mental Health – Physical Medicine and Rehab – Community Based Delivery – Au?sm Spectrum Disorders – Older Persons

Invi?ng an Elected Official to a Recrea?onal Therapy Program
• Plan as far ahead as possible – They’re busy but spend lots of ?me in district – Have several poli?cians in mind, but invite only one at a ?me – Be sure to coordinate with your facility administra?on
• Contact the local office first – You’ll have beVer luck – Establish a contact in the local office – Introduce yourself – Briefly describe your organiza?on and the event (if applicable). – Explain the benefits for the poli?cian
• E.G., the event will give the Congressperson an opportunity to meet with older adults who are his or her cons?tuents. Poli?cians are always keen to meet with cons?tuents.

Ac?vity
• Find a folks in your state. There is a state name plate on seats throughout the audience.
• Hold up the state un?l a person from that state shows up. If nobody shows, give it to us.
• Meet each other. – Exchange contact informa?on – Volunteer to set up a listserv for your state – Find partners close by. – Develop a strategy for your state.

Follow-‐up
• Share your successes. Take a picture with your elected official (BTW. They like photo ops)
• Share with ATRA so we can post in the newsleVer and other ATRA communica?ons.

Challenges:
• Commitment • Engagement

QUESTIONS??????

Professional Commitment and Public Policy
• RT operates in a highly competitive marketplace – Efficiency – Effectiveness – Demonstrable outcomes
• Valued by consumers • In concert with mission of the agency
• We face well-organized and well-funded competitors

Professional Commitment and Public Policy
• AOTA’s Day on the Hill – Annual grass roots lobbying event – 514 OT’s attended the 2012 Day on the
Hill
• Virtual Day on the Hill – 1900 contacts to Congress

Consistent & High Quality RT Practice

Consistent & High Quality RT Practice
– Consistent & High Quality Professional Preparation
– Standards of Practice – Evidence-Based Practice

Consistent & High Quality RT Practice
Consistent & High Quality Professional Prepara?on
– CommiJee on the Accredita4on of Recrea4onal Therapy Educa4on (CARTE)
• Congruent with health care professions – Commission on Accredita?on of Allied Health Educa?on Programs
• Tied into public policy demands on prac??oners – e.g., demonstra?ng KSA of ac?ve treatment
• Addresses the inconsistency among academic prep programs
• Drives quality

Consistent & High Quality RT Prac?ce
Standards of Prac?ce • Based on regulatory language
– CMS
– Joint Commission
– CARF
• Drives quality
• Ensures consistent care
Consistent & High Quality RT Practice
Evidence-‐Based Prac?ce • An absolute demand from policy-‐makers
– CMS discussion
• Professional & ethical obliga?on • 3 tenets
– Best available evidence – Pa?ents’ values – Clinical exper?se

Public Policy and Coverage of RT Services

Public Policy and Coverage of RT Services
• NOT reimbursement – Very few if any RT services are reimbursed – Deliver services à send bill to insurer
• Coverage – RT is a covered service in IRF, IPF, SNF, & when called for in an IEP
– Insurer agrees to cover the costs of certain services before they are delivered
• What do covered services look like?
What Do Covered Services Look Like?
• Active Treatment – Centers for Medicaid and Medicare
Services (CMS) – CMS defines “Active Treatment”
• Provided under an individualized treatment or diagnostic plan
• Reasonably expected to improve the condition patient’s condition
• Supervised and evaluated by a physician – Medicare Benefit Policy Manual (30.2.2.1 - Principles for
Evaluating a Period of Active Treatment)

What Do Covered Services Look Like?
• Medical Necessity – Medical necessity documented in medical
record by physician – Ordered by a physician – “Not primarily recreational or
diversionary”

Public Policy and Coverage of RT Services
• Licenses – Increasingly demanded in regulatory
language – Required of other health care providers
who are considered qualified professionals
– For many health care professions, a state license is required for entry to the profession
• Protects public

What will you do?

Ques?ons?

Informa?on
Thomas Skalko – 252-‐328-‐0018 [email protected]
Richard Williams – 252-‐328-‐0019 [email protected]