thoracic trauma hossam hassan. thoracic trauma anatomy thorax is a hollow cylinder composed of 12...
TRANSCRIPT

Thoracic Trauma
Hossam Hassan
Thoracic Trauma Anatomy Thorax is a hollow cylinder composed of 12 pairs of ribs10articulate posteriorly with
the thoracic spine and anteriorly with the sternum via costal cartilagesthe lower 2 pairs are floating ribs
A nervean artery and a vein are located a long the under side of each rib
Intercostals muscles connect each rib to the one above these muscles with the diaphragm are the primary muscle of ventilation
Anatomy The pleurae are thin membranes
that consist of 2 distinct layers The partial pleurae line the inner
side of the thoracic cavity The visceral pleurae cover the
outer surface of each lung
Anatomy The lungs occupy the right and the left
halves of the thoracic cavity An area called the mediastinum is located
in the middle of the thoracic cavity within the mediastinum lie all the other organs and structures of the chest cavitythe heartgreat vesselstracheamainstem bronchi and esophagus
Any or all of these structures can be injured by thoracic trauma
General Assessment The signs and symptoms of chest truma
related to the chest wall and lungs are sobtachypnea and chest pain
The initial 3 points in general assessment is
1Observation exbruiseslacerationsdistended neck veins
2Palpation extendernessbony crepitus3Auscultation expresence diminished or
absence of breath sounds
Thoracic injuries can be Rib Fractures Flail chest Pulmonary contusion Pneumothorax(open and close) Tension pneumothorx Hemothorax Blunt cardiac injuries Pericardial tamponade Tracheal and bronchial rupture Aortic rupture Diaphragmatic rupture
Chest Trauma History amp PE ATLS protocol ABCDErsquos
Contusions diminished or absent breath sounds SQ emphysema
AMPLE A allergies M Medications (Anticoagulants
insulin and cardiovascular medications especially)
Previous medicalsurgical history L Last meal (Time) E Events Environment surrounding
the injury ie Exactly what happened
CXR-fast easy least expensive for initial evaluation
Ultrasound-may soon replace CXR as initial radiographic study in chest trauma
CT Scan VS Angiography EChO VS Transesophogeal
Echocardiography
FAST
Normal CXR
Pneumothorax
Subcutaneous Emphysema
Hemothorax
Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Thoracic Trauma Anatomy Thorax is a hollow cylinder composed of 12 pairs of ribs10articulate posteriorly with
the thoracic spine and anteriorly with the sternum via costal cartilagesthe lower 2 pairs are floating ribs
A nervean artery and a vein are located a long the under side of each rib
Intercostals muscles connect each rib to the one above these muscles with the diaphragm are the primary muscle of ventilation
Anatomy The pleurae are thin membranes
that consist of 2 distinct layers The partial pleurae line the inner
side of the thoracic cavity The visceral pleurae cover the
outer surface of each lung
Anatomy The lungs occupy the right and the left
halves of the thoracic cavity An area called the mediastinum is located
in the middle of the thoracic cavity within the mediastinum lie all the other organs and structures of the chest cavitythe heartgreat vesselstracheamainstem bronchi and esophagus
Any or all of these structures can be injured by thoracic trauma
General Assessment The signs and symptoms of chest truma
related to the chest wall and lungs are sobtachypnea and chest pain
The initial 3 points in general assessment is
1Observation exbruiseslacerationsdistended neck veins
2Palpation extendernessbony crepitus3Auscultation expresence diminished or
absence of breath sounds
Thoracic injuries can be Rib Fractures Flail chest Pulmonary contusion Pneumothorax(open and close) Tension pneumothorx Hemothorax Blunt cardiac injuries Pericardial tamponade Tracheal and bronchial rupture Aortic rupture Diaphragmatic rupture
Chest Trauma History amp PE ATLS protocol ABCDErsquos
Contusions diminished or absent breath sounds SQ emphysema
AMPLE A allergies M Medications (Anticoagulants
insulin and cardiovascular medications especially)
Previous medicalsurgical history L Last meal (Time) E Events Environment surrounding
the injury ie Exactly what happened
CXR-fast easy least expensive for initial evaluation
Ultrasound-may soon replace CXR as initial radiographic study in chest trauma
CT Scan VS Angiography EChO VS Transesophogeal
Echocardiography
FAST
Normal CXR
Pneumothorax
Subcutaneous Emphysema
Hemothorax
Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Anatomy The pleurae are thin membranes
that consist of 2 distinct layers The partial pleurae line the inner
side of the thoracic cavity The visceral pleurae cover the
outer surface of each lung
Anatomy The lungs occupy the right and the left
halves of the thoracic cavity An area called the mediastinum is located
in the middle of the thoracic cavity within the mediastinum lie all the other organs and structures of the chest cavitythe heartgreat vesselstracheamainstem bronchi and esophagus
Any or all of these structures can be injured by thoracic trauma
General Assessment The signs and symptoms of chest truma
related to the chest wall and lungs are sobtachypnea and chest pain
The initial 3 points in general assessment is
1Observation exbruiseslacerationsdistended neck veins
2Palpation extendernessbony crepitus3Auscultation expresence diminished or
absence of breath sounds
Thoracic injuries can be Rib Fractures Flail chest Pulmonary contusion Pneumothorax(open and close) Tension pneumothorx Hemothorax Blunt cardiac injuries Pericardial tamponade Tracheal and bronchial rupture Aortic rupture Diaphragmatic rupture
Chest Trauma History amp PE ATLS protocol ABCDErsquos
Contusions diminished or absent breath sounds SQ emphysema
AMPLE A allergies M Medications (Anticoagulants
insulin and cardiovascular medications especially)
Previous medicalsurgical history L Last meal (Time) E Events Environment surrounding
the injury ie Exactly what happened
CXR-fast easy least expensive for initial evaluation
Ultrasound-may soon replace CXR as initial radiographic study in chest trauma
CT Scan VS Angiography EChO VS Transesophogeal
Echocardiography
FAST
Normal CXR
Pneumothorax
Subcutaneous Emphysema
Hemothorax
Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Anatomy The lungs occupy the right and the left
halves of the thoracic cavity An area called the mediastinum is located
in the middle of the thoracic cavity within the mediastinum lie all the other organs and structures of the chest cavitythe heartgreat vesselstracheamainstem bronchi and esophagus
Any or all of these structures can be injured by thoracic trauma
General Assessment The signs and symptoms of chest truma
related to the chest wall and lungs are sobtachypnea and chest pain
The initial 3 points in general assessment is
1Observation exbruiseslacerationsdistended neck veins
2Palpation extendernessbony crepitus3Auscultation expresence diminished or
absence of breath sounds
Thoracic injuries can be Rib Fractures Flail chest Pulmonary contusion Pneumothorax(open and close) Tension pneumothorx Hemothorax Blunt cardiac injuries Pericardial tamponade Tracheal and bronchial rupture Aortic rupture Diaphragmatic rupture
Chest Trauma History amp PE ATLS protocol ABCDErsquos
Contusions diminished or absent breath sounds SQ emphysema
AMPLE A allergies M Medications (Anticoagulants
insulin and cardiovascular medications especially)
Previous medicalsurgical history L Last meal (Time) E Events Environment surrounding
the injury ie Exactly what happened
CXR-fast easy least expensive for initial evaluation
Ultrasound-may soon replace CXR as initial radiographic study in chest trauma
CT Scan VS Angiography EChO VS Transesophogeal
Echocardiography
FAST
Normal CXR
Pneumothorax
Subcutaneous Emphysema
Hemothorax
Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing
General Assessment The signs and symptoms of chest truma
related to the chest wall and lungs are sobtachypnea and chest pain
The initial 3 points in general assessment is
1Observation exbruiseslacerationsdistended neck veins
2Palpation extendernessbony crepitus3Auscultation expresence diminished or
absence of breath sounds
Thoracic injuries can be Rib Fractures Flail chest Pulmonary contusion Pneumothorax(open and close) Tension pneumothorx Hemothorax Blunt cardiac injuries Pericardial tamponade Tracheal and bronchial rupture Aortic rupture Diaphragmatic rupture
Chest Trauma History amp PE ATLS protocol ABCDErsquos
Contusions diminished or absent breath sounds SQ emphysema
AMPLE A allergies M Medications (Anticoagulants
insulin and cardiovascular medications especially)
Previous medicalsurgical history L Last meal (Time) E Events Environment surrounding
the injury ie Exactly what happened
CXR-fast easy least expensive for initial evaluation
Ultrasound-may soon replace CXR as initial radiographic study in chest trauma
CT Scan VS Angiography EChO VS Transesophogeal
Echocardiography
FAST
Normal CXR
Pneumothorax
Subcutaneous Emphysema
Hemothorax
Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Thoracic injuries can be Rib Fractures Flail chest Pulmonary contusion Pneumothorax(open and close) Tension pneumothorx Hemothorax Blunt cardiac injuries Pericardial tamponade Tracheal and bronchial rupture Aortic rupture Diaphragmatic rupture
Chest Trauma History amp PE ATLS protocol ABCDErsquos
Contusions diminished or absent breath sounds SQ emphysema
AMPLE A allergies M Medications (Anticoagulants
insulin and cardiovascular medications especially)
Previous medicalsurgical history L Last meal (Time) E Events Environment surrounding
the injury ie Exactly what happened
CXR-fast easy least expensive for initial evaluation
Ultrasound-may soon replace CXR as initial radiographic study in chest trauma
CT Scan VS Angiography EChO VS Transesophogeal
Echocardiography
FAST
Normal CXR
Pneumothorax
Subcutaneous Emphysema
Hemothorax
Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Chest Trauma History amp PE ATLS protocol ABCDErsquos
Contusions diminished or absent breath sounds SQ emphysema
AMPLE A allergies M Medications (Anticoagulants
insulin and cardiovascular medications especially)
Previous medicalsurgical history L Last meal (Time) E Events Environment surrounding
the injury ie Exactly what happened
CXR-fast easy least expensive for initial evaluation
Ultrasound-may soon replace CXR as initial radiographic study in chest trauma
CT Scan VS Angiography EChO VS Transesophogeal
Echocardiography
FAST
Normal CXR
Pneumothorax
Subcutaneous Emphysema
Hemothorax
Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

AMPLE A allergies M Medications (Anticoagulants
insulin and cardiovascular medications especially)
Previous medicalsurgical history L Last meal (Time) E Events Environment surrounding
the injury ie Exactly what happened
CXR-fast easy least expensive for initial evaluation
Ultrasound-may soon replace CXR as initial radiographic study in chest trauma
CT Scan VS Angiography EChO VS Transesophogeal
Echocardiography
FAST
Normal CXR
Pneumothorax
Subcutaneous Emphysema
Hemothorax
Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

CXR-fast easy least expensive for initial evaluation
Ultrasound-may soon replace CXR as initial radiographic study in chest trauma
CT Scan VS Angiography EChO VS Transesophogeal
Echocardiography
FAST
Normal CXR
Pneumothorax
Subcutaneous Emphysema
Hemothorax
Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

FAST
Normal CXR
Pneumothorax
Subcutaneous Emphysema
Hemothorax
Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing
Normal CXR
Pneumothorax
Subcutaneous Emphysema
Hemothorax
Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing
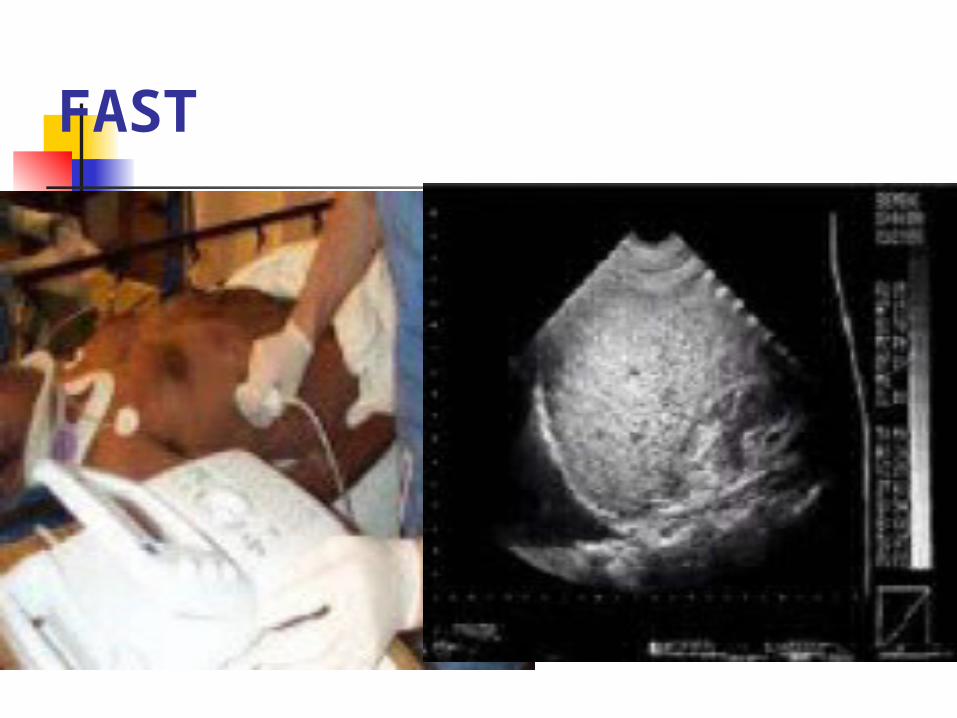
Pneumothorax
Subcutaneous Emphysema
Hemothorax
Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Subcutaneous Emphysema
Hemothorax
Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Hemothorax
Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Management of specific injuries Rib fracture Assessment Simple rib fracture alone are rarely
life threatening in adults Signs and symptoms of fractured
ribs include pain with movementlocal tenderness and perhaps bony crepitus
Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Rib fracture Management The initial management of patient with
simple rib fracture is pain reduction supplemental oxygen in case hypoxia Bed rest Fractured ribs should not be stabilized by
taping or using any other firm bandaging such attempt can limit ventilation and lead to atelactasis (collapse of the alveoli or part of the lung)and pneumonia
Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Flail Chest Flail chest is when 2 or more
adjacent ribs are each fractured in at least 2 places
Assessment Tenderness Bony crepitus Hypoxia might happen then lead to
increase in respiratory rate as well
Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Flail chest Management The key management is BVM (for
positive pressure ventilation) All patient who have an obvious
flail segment should supplied with supplemental O if not respond then will require more aggressive ventilataroy support
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing
Pulmonary contusion A pulmonary contusion is an area of the
lung that has been traumatized to the point where intertitial and leveolar bleeding occur
The amount of intertitial fluids increase in the area between the wall of the cappilaries and alveoli resulting in decreased O transporst across the thickened membranes
Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Pulmonary contusion Managements Patient should closely monitored with
special attention to fluid administration
Ensuring adequate ventilation and enriched O administration
In inadequate ventilations or altered LOC or other major injuries BVM and endotracheal intubation if required
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing
Pneumothorax Simple pneumothorax Open pneumothorax
Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Simple pneumothorax Simple pneumothorax is caused by
the presence of air in the pleural space
Assessment Pleuratic chest pain Difficult and rapid breathing Decreased or absent breath sounds
on the involved side are classic signs Percussion is an excellent indicator
Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Simple pneumothorax Management High concentration of O should
be administrated to patients with pneumothorax
Assisted ventilation might be for those who display signs of hypoxia
Semi sitting position is preferred
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing
Open pneumothorax Penetrating wounds to the chest can
produce open chest wall injuries(open pneumothorax)
Assessment Pain at the injured side SOB The sings might included sucking out
bubbling sound as air moves in and out of the pleural space through the chest wall defected
Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Open pneumothorax Management Close the hole in the chest Closing the hole it could be with a
Vaseline gauze by 3 sides taped Provide supplemental O If signs of increasing respiratory distress
are observed the patient may be developing a tension pneumothorax and the dressing should be removed to assess in decompressing the affected side
Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Tension pneumothorax It is a life threatening situation The amount of air trapped in the pleural
space continues to increase not only is the lung on the affected side collapsed but the mediastinum is also shifted into the opposite side
The intra thoracic pressure increase witch decrease the capillaries blood flow and kinks the vena cava
Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Tension pneumothorax Assessment The presentation of patient with tension
pneumothorax varies according to how much intrathoracic pressure has developed
Signs and symptoms can be minimal or moderate Anxiety Cyanosis Tachypnea Diminished or absent breath sound on the injured
side JVD (jugular vein distension)note in case
hypovolemic this sign might not present
Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Tension pneumothorax Management The management of the patient with a
tension pneumothorax involves reducing the pressure in the pleural space
Needle decompression in the field can be done by the expert people
Chest tube Incase penetrating injury then dressing Refer to the specialist area as soon as
possible
Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Hemothorax Blood in the pleural space
constitutes a hemothorax In adult the pleural space on each
side of the thorax can hold 2500 to 3000 ml of blood
Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Hemothorax Assessment The symptoms are related to the blood loss Sings Sob Tachypnea Decreased breath sound Clinical signs of shock Management transfer to surgical repair
Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Myocardial Contusion Occurs in 76 of patients with
severe blunt chest trauma ndashRight Atrium and Ventricle is
commonly injured ndashInjury may reduce strength of
cardiac contractions Reduced cardiac output
Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Electrical Disturbances due to irritability of damaged myocardial cells
ndashProgressive Problems Hematoma Hemoperitoneum Myocardial necrosis Dysrhythmias CHF amp or Cardiogenic shock
Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Myocardial Contusion Signs amp Symptoms Bruising of chest wall 1048708Tachycardia andor irregular
rhythm 1048708Retrosternal pain similar to MI 1048708Associated injuries Rib Sternal
fractures
Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Chest pain unrelieved by oxygen May be relieved with rest THIS IS TRAUMA-RELATED PAIN
Similar signs and symptoms of medical chest pain
Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Blunt Cardiac Injury EKG (for any blunt chest injury
persistent tachycardia ST-T changes or ectopy)
1048708Cardiac enzymes (CPK CK-MB and Troponin I)
1048708Echocardiography (TEE)
Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Pericardial Tamponade Restriction to cardiac filling caused
by blood or other fluid within the pericardium
ndashOccurs in lt2 of all serious chest trauma However very high mortality
ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

ndashResults from tear in the coronary artery or penetration of myocardium
Blood seeps into pericardium and is unable to escape
200 ml of blood can restrict effectiveness of cardiac contrac
Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Pericardial Tamponade Signs amp Symptoms Dyspnea Possible cyanosis Beckrsquos Triad JVD Distant heart tones Hypotension or narrowing pulse pressure Weak thready pulse Shock
Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Kussmaulrsquos signDecrease or absence of JVD during inspiration
Pulsus ParadoxusDrop in SBP gt10 during inspiration
Electrical AlteransP QRS amp T amplitude changes in every other cardiac cycle
PEA
Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Traumatic Aortic injury
Aorta most commonly injured in severe blunt 85-95 mortality
Injury may be confined to areas of aorta attachment
Signs amp Symptoms Rapid and deterioration of vitals Pulse deficit between right and left upper
or lower extremities
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing
Traumatic Esophageal Rupture Rare complication of blunt thoracic trauma ndash30 mortality ndashContents in esophagusstomach may
move into mediastinum Serious infection occurs Chemical irritation Damage to mediastinal structures Air enters mediastinum
ndash
Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Subcutaneous emphysema and penetrating trauma present
Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Tracheo-bronchial Injury Blunt trauma Penetrating trauma 50 of patients with injury die within
1 hr of injury Disruption can occur anywhere in
tracheobronchial tree
ndash
Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Signs amp SymptomsDyspnea Cyanosis Hemoptysis Massive subcutaneous emphysema Suspect evaluate for other closed
chest trauma
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing
Treatment summary Observe Palpate Auscultation Management always included to
provide supplemental O then aggressive method if required
ATLS protocol ABCDErsquos
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing
Treatment summary Emergency management Needle thoracentesis Tube thoracostomy Subxiphoid pericardotomy Video assisted thoracic surgery
(VATS)
THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

THANK YOU
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing
3 Identification of which of the following is NOT an essential part of the primary survey
A Tension Pneumothorax B Open Pneumothorax C Flail Chest D Cardiac Tamponade E Rib Fractures
4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

4 Upon Identification of a Tension Pneumothorax which is the correct management pathway
A A chest X-ray to confirm the clinical diagnosis B Insertion of a chest drain in the 5th intercostals
interspace in mid-axillary line C Immediate decompression with a 14g 5cm needle in
the 2nd intercostal interspace in mid-calvicular line D An ECG to assess for concurrent cardiac contusion E Completion of a secondary survey to exclude any
concurrent injury
In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

In massive haemothorax which of the following is an indication for emergency thoracotomy
A Production of 500ml of blood on immediate insertion of a
chest drain B Production of 50mlhour of blood for two consecutive
hours in the chest drain C Production 1000ml of blood on immediate insertion of a
chest drain D Production of greater than 1500ml of blood on
immediate insertion of a chest drain E Evidence of greater than 5 rib fractures in conjunction
with radiological evidence of haemothorax
A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

A pulmonary contusion A Can cause immediate respiratory difficulties B Results in increased lung compliance at 24
hours C Does not occur without rib fractures in
children D Can cause ventilationperfusion mismatch
which evolves over 24 hours E Is not associated with Adult Respiratory
Distress Syndrome
When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

When evaluating the chest of a patient with a chest injury you note a fine crackling sensation under the areas that you palpate This is best described as
pulses paradoxus subcutaneous emphysema hemothorax none of the above
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing
In which condition would you observe paradoxical movement of the chest wall
mediastinal shift tension pneumothorax flail chest CheynendashStokes breathing
Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Proper care for a patient with a sucking chest wound includes
pulling the wound open on inhalation to release trapped air sealing the wound with an occlusive dressing covering the wound with sterile gauze decompression of the chest
Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

Which of the following statements correctly differentiates a simple pneumothorax from a tension pneumothorax
A tension pneumothorax requires decompression while a simple pneumothorax does not A simple pneumothorax is caused by air in the pleural space while a tension pneumothorax is caused by blood in the pleural space A simple pneumothorax is caused by damage to the lung from inside while a tension pneumothorax is caused by injury to the outside chest wall There is no difference between a tension pneumothorax and simple pneumothorax
After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing

After placing an occlusive dressing over a sucking chest wound to the right chest you note that the patient has become extremely dyspneic and cyanotic with breath sounds absent on the right side Your next action would be to
perform a needle cricothyroidotomy remove the occlusive dressing and replace it with sterile gauze insert an oropharyngeal airway loosen a corner of the occlusive dressing