title from previous. learning objectives understand the formulary background, concept, structure,...
TRANSCRIPT

Title from previousRole of Formularies
Improved Pharmacotherapy
Gordon Schiff MDDirector Clinical Quality Research & Improvement
Dept of Medicine Cook County Professor of Medicine Rush University
MODULE/LECTURE 2

Learning Objectives
• Understand the formulary background, concept, structure, and ways formularies can facilitate better prescribing decision-making.
• Understand the concept of “drugs of choice” • Critically discuss specific examples of local
formulary decisions, and launch student projects for in-depth study of a formulary drug application case study.
• Analyze controversies and issues surrounding formulary implementation and current practices
Outline - Hour 1
1. Exercise: Formulary culture survey
2. Background & history of formularies
3. How formularies work
4. Examples from Cook County 1. Selective COX2 2. “Specific” criteria ??
5. Global perspectives/examples1. CDC Drugs of Choice 2. WHO Essential Drugs
BREAK
Outline –Hour 2
6. FLIP and formularies; FLIP tools
7. Audience Response Lab:
Culture survey discussion
8. Project development
9. Assessment




Baghdad
Basra
Baghdad
Basra

Ancient Formulary
Sumerian Cuneiform Tablet from
Nippur 3000 BC
Early U.S. Formularies• Lititz Pharmacopoeia published in 1778 for use by
the Continental forces
• Coste’s Compendium Pharmaceuticum of 1780 used by French forces during the American Revolution
• United States Pharmacopeia Convention meets in Old Senate Chamber Jan 1, 1820– Selects drugs for the Pharmacopeia of the United States – Oldest non-profit organization in the U.S.

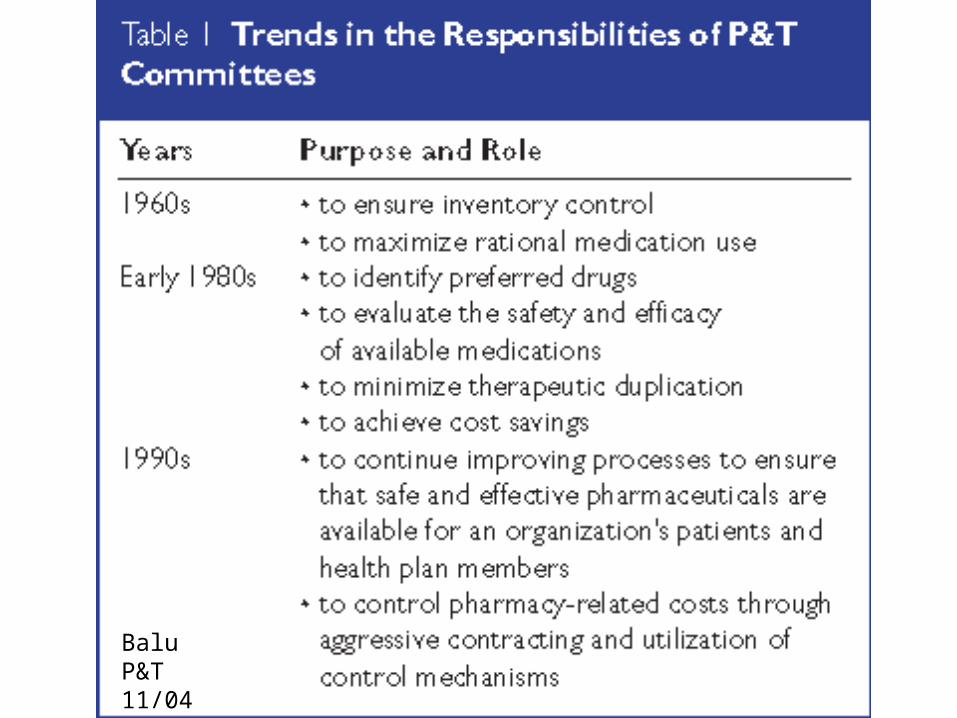
Balu P&T 11/04

Drug Formulary:
“A continually updated list of medications and related information, representing the clinical judgment of physicians, pharmacists and other experts in the diagnosis and/or treatment of disease and promotion of health.”
Drug Formulary System:•Ongoing process
•Collaboration of physicians, pharmacists, and other health care professionals
•Establishes policies on the use of drug products and therapies most medically appropriate and cost-effective to best serve the health interests of a given patient population.
•http://www.amcp.org/amcp.ark?c=stu&sc=glossary

Inpatient
Outpatient
Public Sector Medicaid National VA (+ regional/local)
Privatized-Public SectorMedicare Part D (2801 private plans)
Private Sector PBMsOther HMO/InsurerRetail pharmacy chains
Hospital Formularies
Nursing Homes
Types of Formularies in U.S.
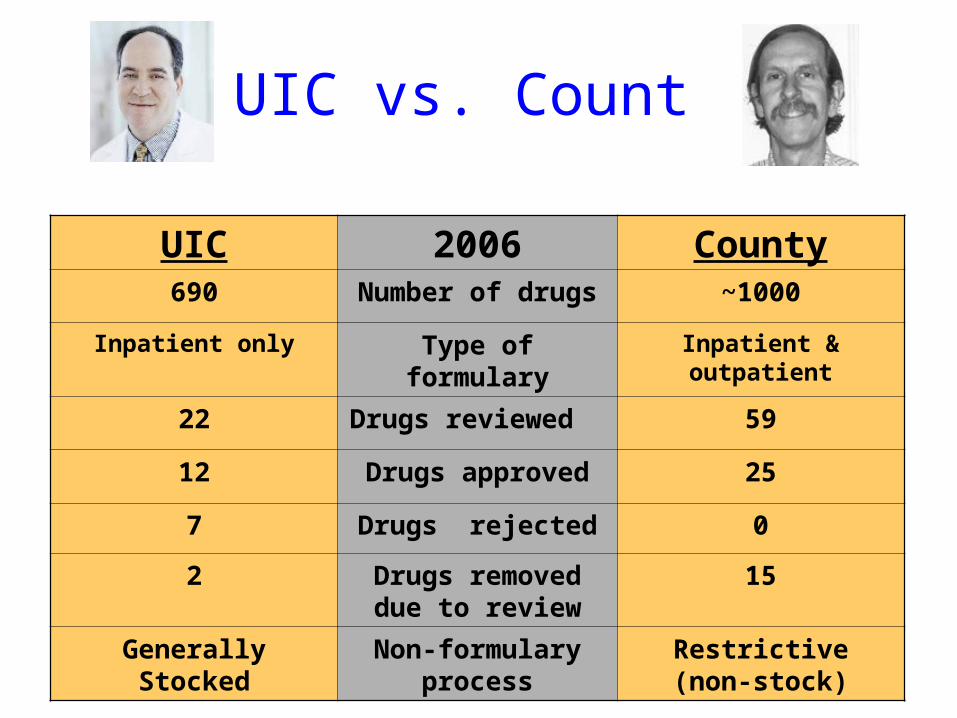
UIC vs. County
UIC 2006 County690 Number of drugs ~1000
Inpatient only Type of formulary Inpatient & outpatient
22 Drugs reviewed 59
12 Drugs approved 25
7 Drugs rejected 0
2 Drugs removed due to review
15
Generally Stocked Non-formulary process
Restrictive (non-stock)

Formulary Management
Drug Usage Monitoring
Drug Use Policy-making
Pharmacy and Therapeutics Committee
Drug Use
Drug Use
Drug Use
Drug UseDrug Use
Drug Use Drug Use

Formulary Management
Drug Usage Monitoring
Drug Use Policy-making
Pharmacy and Therapeutics Committee
Drug Use
Drug Use
Drug Use
Drug UseDrug Use
Drug Use Drug Use

Formulary Management
Drug Usage Monitoring
Drug Use Policy-making
Pharmacy and Therapeutics Committee
Restrictions Guidelines Therapeutic InterchangeLab MonitoringEducation Alerts Drug rep policies
Adverse Reactions Med Error & SafetyOverall UtilizationNon-formulary UsageCriteria-Based Monitoring
AdditionsDeletionsRestrictionsEnsure Availability Periodic ReviewsPublish FormularyCommunicate
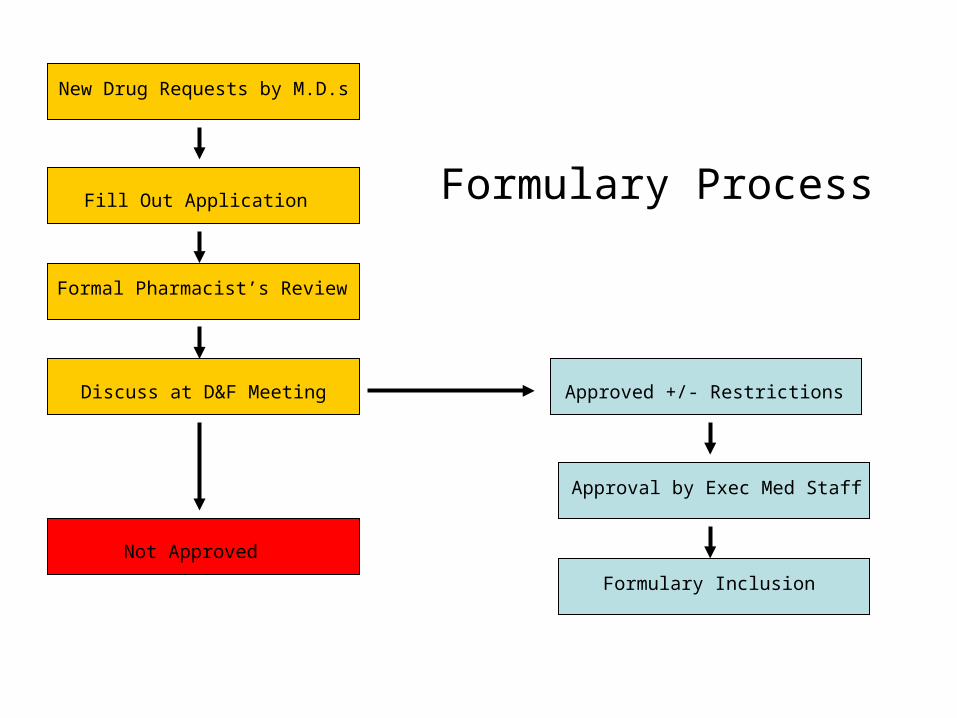
New Drug Requests by M.D.s
Fill Out Application
Formal Pharmacist’s Review
Discuss at D&F Meeting
Not Approved
Approved +/- Restrictions
Approval by Exec Med Staff
Formulary Inclusion
Formulary Process

Cook County COX2 Approval Mechanism (via Pharm HELP Desk)
• GI Assessment Tool Scoring • Age (1-18)• Health Status (0-4) • RA (2)• Prednisone (5) • Ever GI Bleeding (8) • GI Side effects (2)
Score• > 20 Automatic OK 16-20 Trial Salcylate
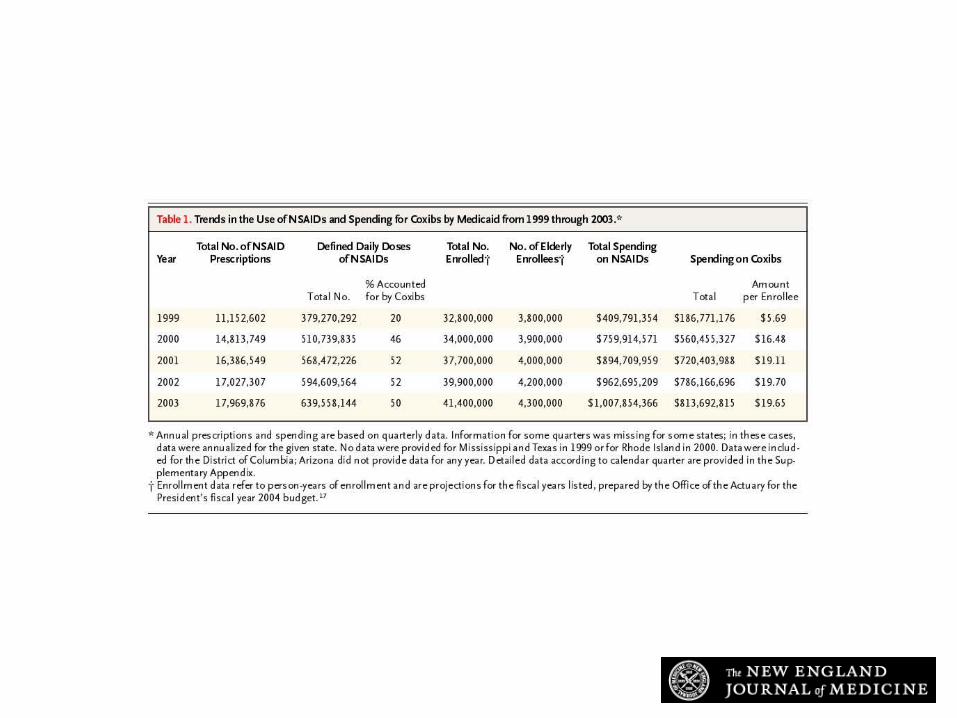
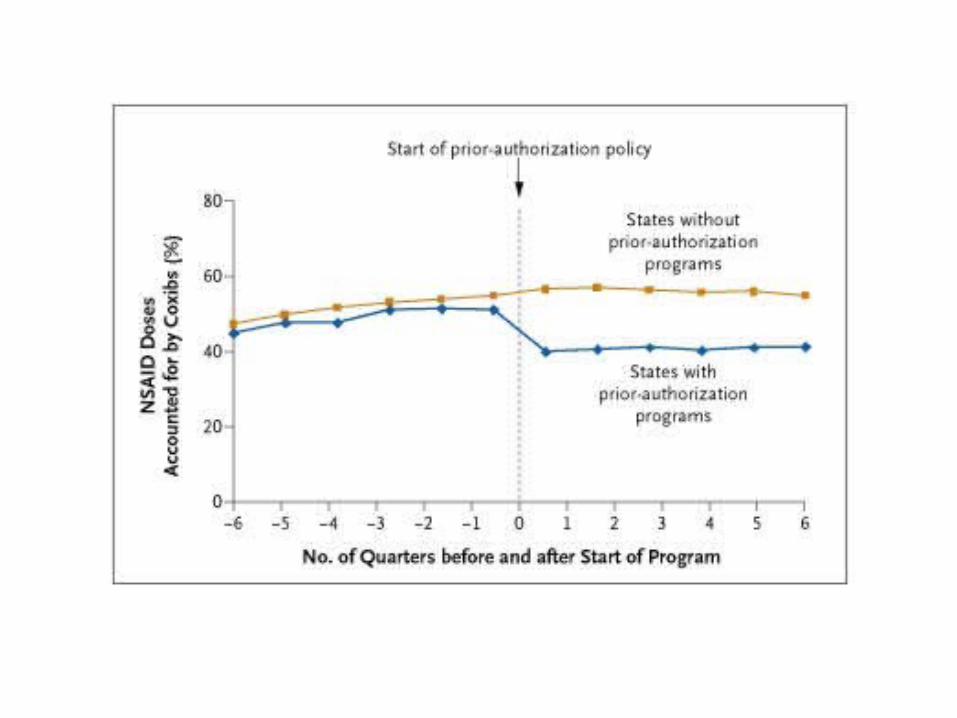
Fischer M et al. N Engl J Med 2004;351:2187-2194
Trends in the Use of NSAIDs and Spending for Coxibs by Medicaid from 1999 through 2003

Medicaid Cook County1999 20% NA2000 46% NA2001 52% 2.50%2002 52% 4.10%2003 50% 3.40%2004 NA 2.80%
COX2:NSAIDs %’s Cook County vs. Medicaid
2001 N=431/17,259
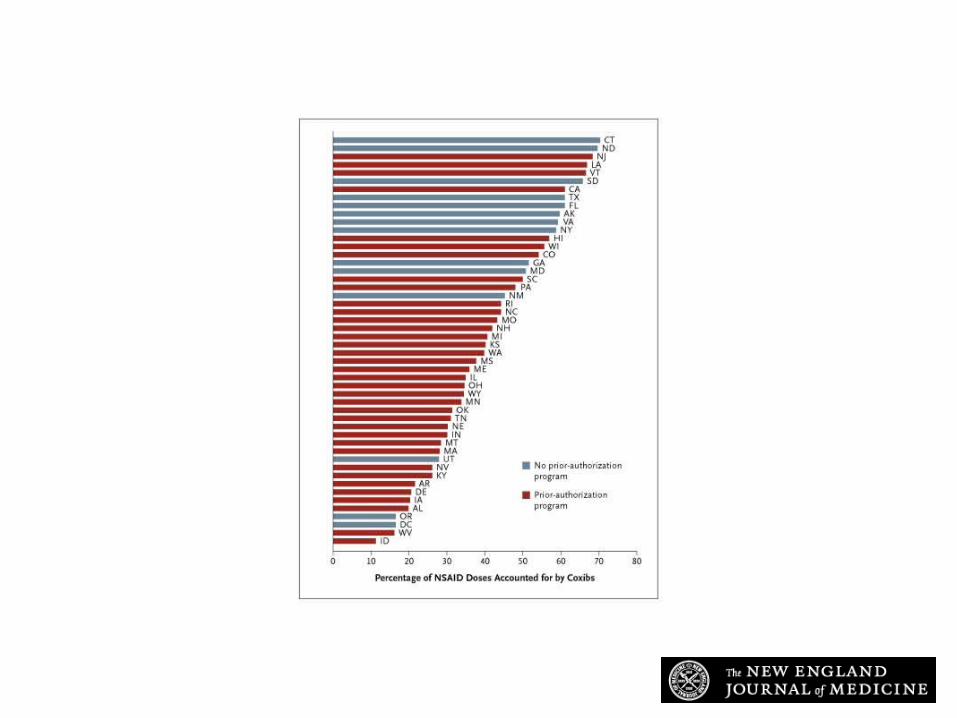
Fischer M et al. N Engl J Med 2004;351:2187-2194
Percentage of Defined Daily Doses of NSAIDs Accounted for by Coxibs in the Fourth Quarter of 2003, According to Whether a Prior-Authorization Program Had Been Implemented
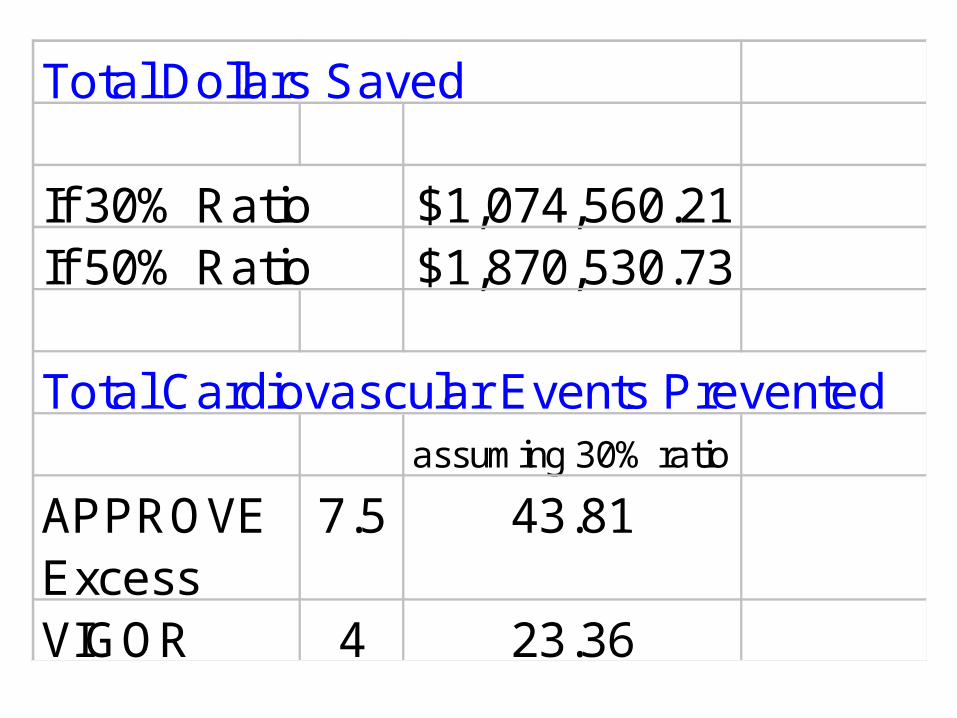
Total Dollars Saved
If 30% Ratio $1,074,560.21If 50% Ratio $1,870,530.73
Total Cardiovascular Events Prevented assuming 30% ratio
APPROVE Excess
7.5 43.81
VIGOR 4 23.36
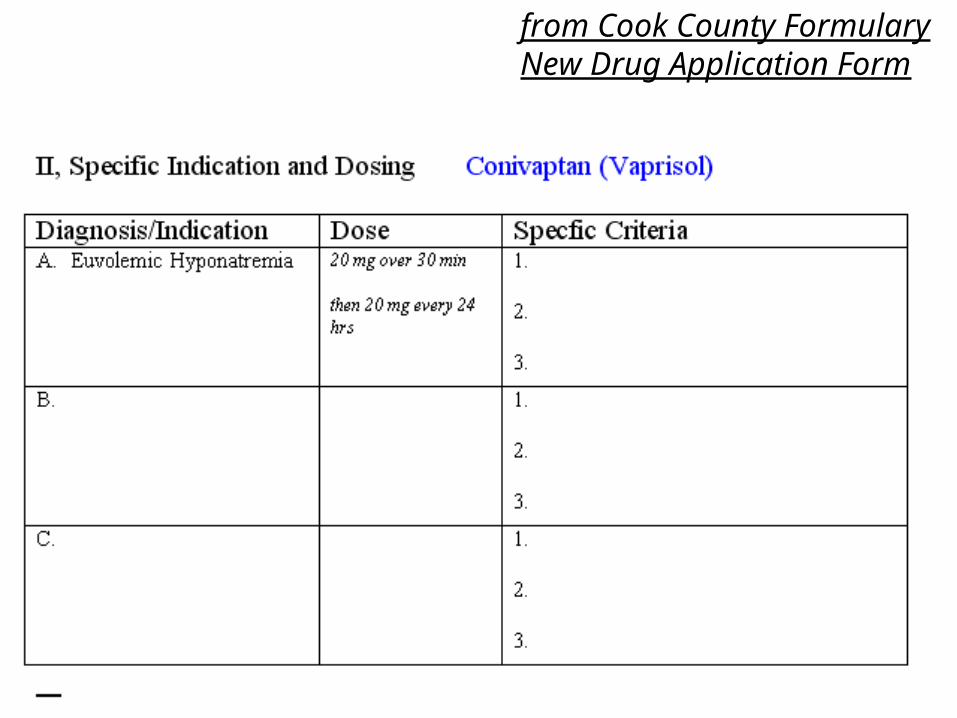
from Cook County Formulary New Drug Application Form


New Drug D & F Application 4 Roles of Specific Criteria
• Organize evidence-based D&F review of value, indications, role for new drug
• Educate, once drug approved
• Guide real-time utilization of drug, ideally computer delivered at time of order
• Retrospective review of appropriateness

Blank 4 23.5%Completely Confused Non Criteria 2 11.8%
Non-specfic Criteria 5 29.4%Somewhat specific/useful 1 5.9%
Clear specific criteria 5 29.4%
TOTAL 17
D&F Drug Indications and CriteriaProperly Filled out on New Form 2/03-4/04
Leading Challenges to CCH/UIC Formulary Committees
• MD’s circumventing formulary and formulary application process for new drugs by using non-formulary ordering route
• Inadequacies of the studies on which to base decisions• Lack of dedicated time of members to fully and critically
digest literature and deliberate at the meetings • Wrestling with extremely costly ($10k/yr) new agents that
appear to be effective, but pose major stain on institutions’ drug budget resources
• Pharmaceutical industry influences and practices (including lobbying members, pricing schemes)
“CDC Drugs of Choice
Methodology
This report was produced through a multistage process. Beginning in 2004, CDC personnel and professionals knowledgeable in the field of STDs systematically reviewed evidence, including published abstracts and peer-reviewed journal articles concerning each of the major STDs, focusing on information that had become available since publication of the Sexually Transmitted Diseases Treatment Guidelines, 2002 (1). Background papers were written and tables of evidence were constructed summarizing the type of study (e.g., randomized controlled trial or case series), study population and setting, treatments or other interventions, outcome measures assessed, reported findings, and weaknesses and biases in study design and analysis. A draft document was developed on the basis of the reviews.
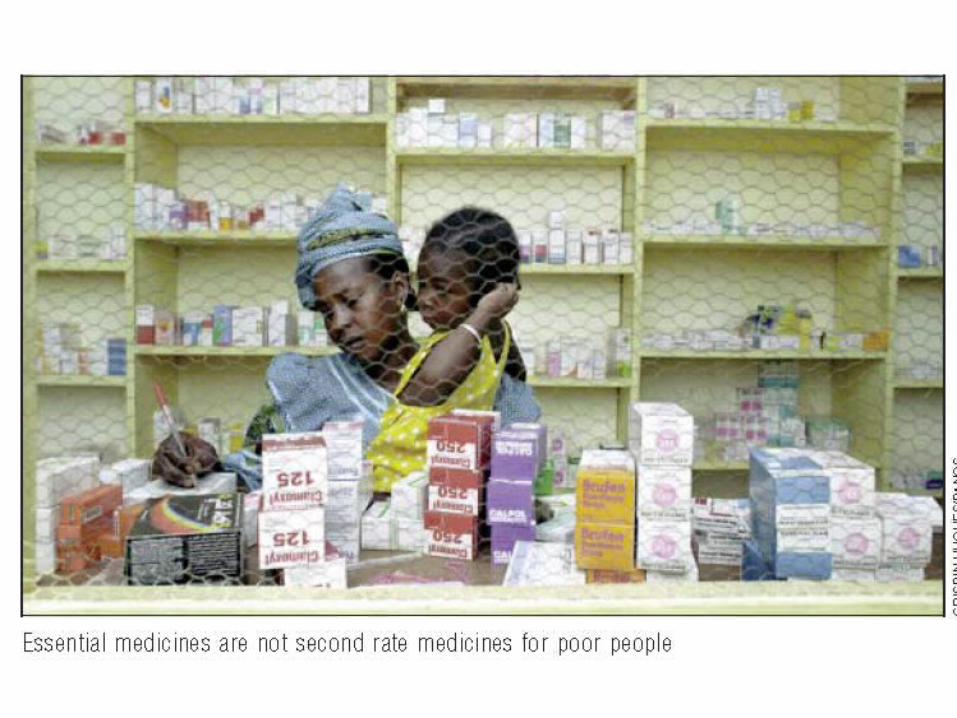
WHO Essential Drugs List
• In 1977, WHO published the first Model List of Essential Medicines containing 208 individual drugs which together could provide safe, effective treatment for the majority of communicable and non-communicable diseases

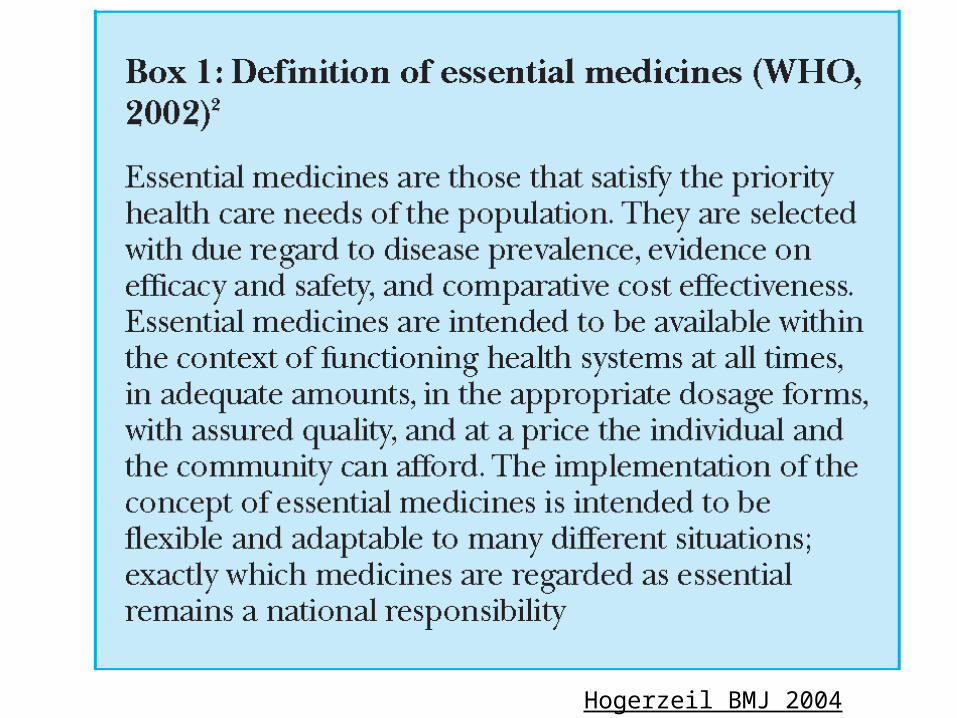
Hogerzeil BMJ 2004
• With these models, and inspired by WHO’s HFA program, in 1982 Bangladesh implemented its National Drug Policy (NDP). An expert committee assembled a list of recommendations based on WHO’s EDC, and the NDP aimed to ensure that procurement, local production, quality control, distribution, and use of pharmaceuticals came under the control of a single government body. This was to be a major part of national health policy.
Bangladesh Essential Drugs Program-1982
• No sooner had a form of the NDP been implemented than foreign-owned drug companies mobilized a campaign of misinformation, threats, and intimidation. For example, on June 1, 1982, the Bangladesh Times publicized the NDP. That same morning, the U.S. ambassador made an unscheduled call on the government to deliver the message that the policy was not acceptable to the U.S. government. Although the U.S. government had no overt interest in the NDP, drug companies, which had made considerable donations to the election campaigns of members of the U.S. government, assuredly did. They mobilized the influence their money had purchased against the NDP, which is why a superpower became involved in the internal health affairs of a small country on the other side of the globe

BreakDownstairs
• Audience Response (30 minutes)
• Formulary Myths
• ISMP Data (“Myths are still true”)
• Projects: Tools and drugs
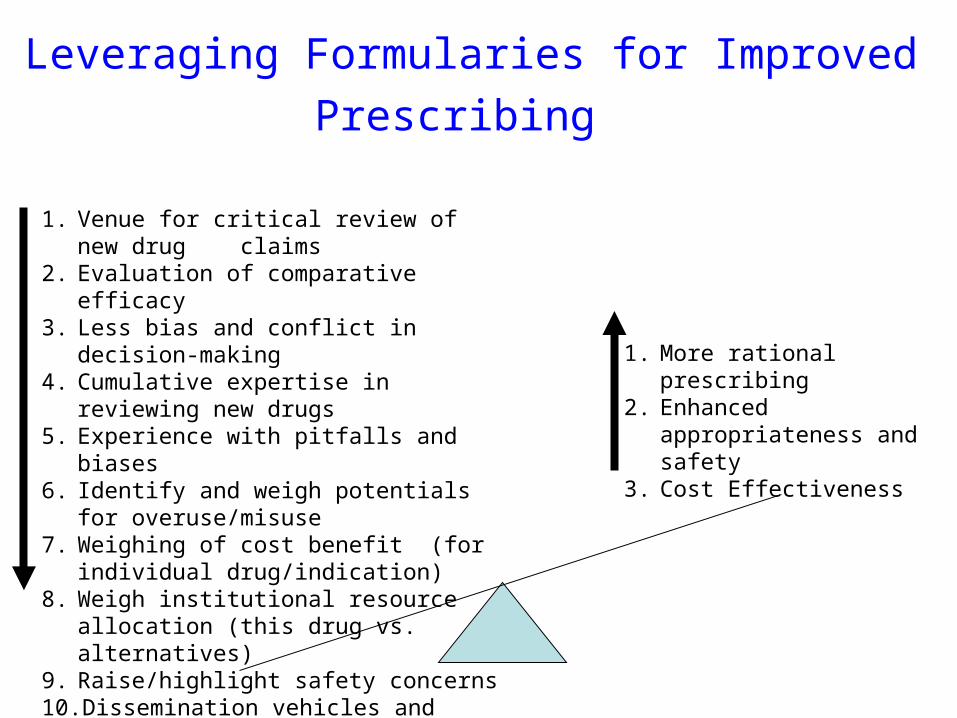
Leveraging Formularies for Improved Prescribing
1. Venue for critical review of new drug claims
2. Evaluation of comparative efficacy3. Less bias and conflict in decision-making4. Cumulative expertise in reviewing new
drugs5. Experience with pitfalls and biases6. Identify and weigh potentials for
overuse/misuse7. Weighing of cost benefit (for individual
drug/indication)8. Weigh institutional resource allocation
(this drug vs. alternatives)9. Raise/highlight safety concerns10. Dissemination vehicles and tools
(guidance and warnings)
1. More rational prescribing2. Enhanced appropriateness
and safety3. Cost Effectiveness
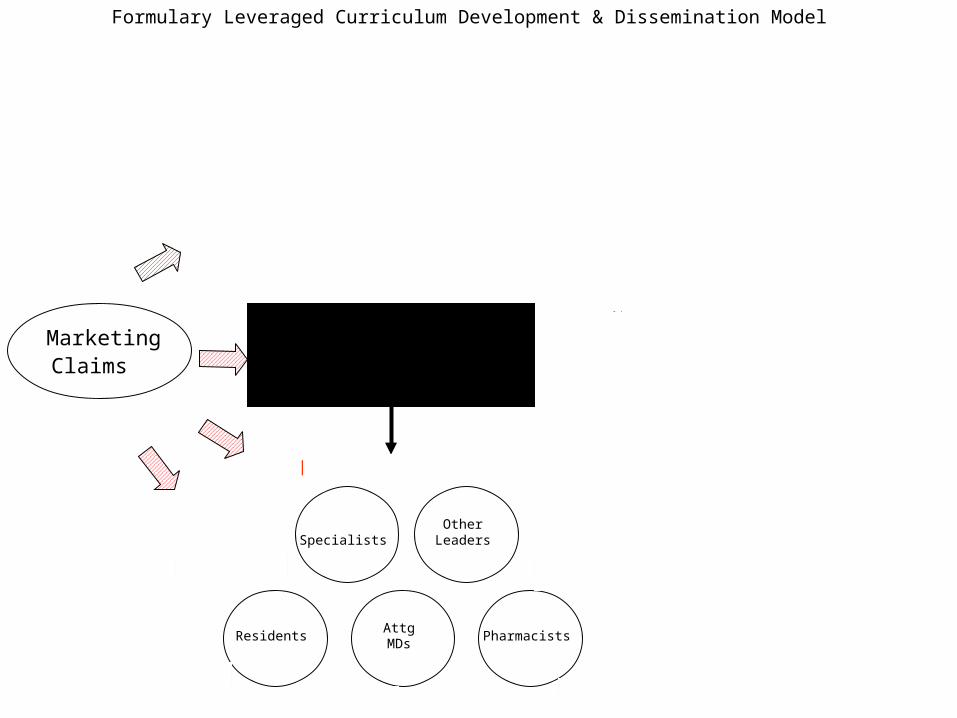
Marketing Claims
Enhanced Input
Critical Knowledge
Recommendations Drugs of Choice & Why
Restrictions/Guidelines for Appropriate Use
Distillation of Drug Specific & Generic Issues
Enhanced Output
OtherLeaders
AttgMDs
Residents Pharmacists
12 Modules
Principles Advanced Seminar
Drug Info Specialists
Formulary Leveraged Curriculum Development & Dissemination Model
Own Drug
Use Criteria
Credibility
Delivery
Buy-in
Formulary Decisionmaking
Specialists

Formulary Decisionmaking
Marketing Claims
Enhanced Input
Critical Knowledge
Recommendations Drugs of Choice & Why
Restrictions/Guidelines for Appropriate Use
Distillation of Drug Specific & Generic Issues
Enhanced Output
SpecialistsOther
Leaders
AttgMDs
Residents Pharmcsts
14 Modules
Principles Advanced Seminar
Drug Info Specialists
Formulary Leveraged Curriculum Development & Dissemination Model
Own Drug
Use Criteria
Credibility
Delivery
Buy-in

Formulary Myths
1. Causal empiricism
2. FDA approval implies everyday use for all
3. Interferes with clinical freedom
4. Every patient is unique
5. Specialist knows best
6. Education requires experience with multiple drugs
7. Widespread use = drug of choice
8. Newer is better/safer
9. Sicker patients need more drugs
10.Formulary sacrifices patient care to cost
11.Redundant with drug utilization review
Schiff, Rucker Med Care 1991
ISMP 2004 Survey Results Formulary Myths Still True !!
• 70% reported causal empiricism comments impacting formulary decisions
• 73% reported specialist knows best comments impacting formulary decisions
• 49% reported never hearing FDA use implies everyday use for all comments in formulary deliberations
http://www.ismp.org/Survey/surveyresults/Survey200411R.asp


MediMedia owns P&T

MediMedia owns Triple Ihttp://www.tripleimedimedia.com/about_us/

Advanstar owns Formulary
They are a “leading provider of integrated marketing solutions” and they are the “leading communications company serving the pharmaceutical industry”
They also own…

How I’ve FLIPPED –Bill GTry to treat any complaint or disease
non-pharmacologically unless truly. Necessary as drugs are poisons and our role is to first do no harm.
New drugs are inherently more risky and likely dangerous than old drugs And should be used sparingly only when truly necessary.
One paper does not always tell the whole story, a thorough review of the Literature is important if you plan on changing your treatment or begin to use a medication.

How I’ve FLIPPED –Gordy S
Realization that no conflict-of-interest voting policy, even on my own Committee
Different conceptualizations and processes on different formulary committees related to “P&T” vs. “formulary” functions
-Medicaid- completely separate
Outpatient dominates CCH, inpatient rules at UIC w/ resulting entirely different framework for discussion
Selected Quotes from Formulary Focus Groups:
What do Clinicians think of their Formulary and the Formulary Process?

Selected quotes UIC• What works on our committee is that we make decisions based
on literature.• [I am] generally satisfied with the Drug Information Center.
Other institutions don’t have as much detail. The DIC does the best they can with the information that is available. For new drugs there isn’t really that much to work with anyway.
• Non-formulary drug requests and discouraging people to avoid non-formulary are continuously a problem. People don’t understand why they shouldn’t use non-formulary. Improvement is needed to understand what the formulary is there for.
• [The committee’s been] almost the same in format for 22 years. It’s tried and true and very standard. It has a survival or Darwinian quality.

Selected quotes Cook County• [One strength of the committee is] participation of clinical
pharmacists to give support and do good drug evaluations.
• Many departments are represented and this is educational.
• The studies available for drugs/new drugs are of poor quality. For example, drugs for senile dementia or diabetic neuropathy.
• Although the committee communicates what is happening in hospital, there are still problems with dissemination. Dissemination is not always successful.
• Making people “jump through hoops” is bad for patients because people should have their medicine.

• We often say we will audit drugs put on the formulary but this does not happen. Doctors feel more comfortable with this kind of evaluation. We put a lot of drugs on which are expensive with marginal benefit. Data does not come back to the committee about usage or patient outcome.
• We are trying to treat everything possible when we cannot afford to. We make some decisions about what to treat and what not to treat, for example we stopped doing bone marrow transplants but we do give anti-rheumatologics
• If you have patient experience you typically give evidence that is more anecdotal, but it does not go unchallenged. Sometimes the committee invites specialists to talk to the group but they are less open now. Some only show up when there is a controversial drug.
• It is not the formulary committee’s role to be a pharmacy budget organization but we still have to make these kinds of decisions. This causes schizophrenic decisions. A lot is lacking in decision-making.
• County has an excellent cardiovascular formulary which has saved millions of dollars. Not running for expensive cures. This restrictiveness is one reason we miss some of the major adverse drug reactions. By the time treatments become cost-effective the ADR’s are discovered.
Selected quotes Cook County