to i- '°o.'0. - adc.bmj.com · tions-for example paracetamol elixir bp contains 10% v/v...
TRANSCRIPT

Alco(hOI intoxication, an lunderdiagnosed problem? 763
was 7t) mmol/l. The following morning she admittedto having drunk a cocktail of alcoholic beveratgesbefore the episode.
Case 4. A 12 year old girl was admitted with a threehour history of vomiting followed by loss of con-sciousness. The possibility of alcohol or drug inges-tion was denied. She was drowsy but responded toverbal commands. No alcohol related smell wasdetected on her breath. Her axillary temperaturewas 35-1°C. A toxicology screen was negative. Herserum alcohol concentration was 44-5 mmol/l aindplasma glucose was 5-7 mmol/l. After the laboratoryresults were available she admitted to having drunka 'small gin and tonic' with friends.
Discussion
Our experience shows the importance of consideringalcohol intoxication in childreni with unexplaineddrowsiness, hypoglycaemia. or hypothermia. Themode of presentation may be confused with otherconditions such as head in'ury or post-ictal state. Itwas characteristic that parents were often reluctatntto admit even the possibility of alcohol ingestioni bytheir children, who in turn rarely volunteered theinformation. Detection of an alcohol related smellon the breath was an unreliable sign and emphasisesthe value of blood alcohol measurements. Theimportance of diagnosis arises from the potentiallyserious complication of alcohol induced hypo-glycaemia' and the necessity to monitor bloodglucose concentrations. In adults the blood alcoholconcentration is aLlso a guide to the severity of theintoxication, values over 30) mmol/l being associatedwith increasing confusion while concenitrations
greater than 85 mmol/l may be fatal.4 It is uncertain,however, whether these adult blood concentrationshave the same clinical importance in children, whereage related variations in alcohol susceptibility andmetabolic clearance may occur.?5
In our patients alcoholic beverages were the mostcommonly identified source of ethanol. The Amer-ican Academy of Pediatrics Committee on Drugs,however, has recently emphasised the potentiallytoxic concentrations of ethanol in some paediatricpharmaceutical preparations.6 In the United Kingdomalcohol is used similarly in many paediatric prepara-tions-for example paracetamol elixir BP contains10% v/v and chlorpheniramine elixir BP 6-3% v/v.Although the harmful effect of ethanol in theseconcentrations remains to be established it couldhave an additive effect in fasting related hypo-glycaemia or cause problems in accidental ingestionif its presence went unrecognised.
References
Le Conte M. Saint-Jacques 1. Cagnat R, Vellicux F, Bois-siere 11. Le coma alcoolique par intoxication accidentelle chezl'enfaint. Sewtl Hop Paris 1978X54:315-24.
2 Curry AS. Walker GW, Simpson GS. Determination of ethanolin blood by gas chromatography. Anaiyst 1966;91:742-3.
3 MacLaircn NK, Valman HB, Levin B. Alcohol-induced hypo-glycaemial in childhood. Br Med J 1970;1:278-80.
4 Johnson RA, Noll EC, Rodney WM. Survival after a serumethanol concentration of 1½/2%. Lancet 1982;ii:1394.
5 Ragan FA. Samuels MS, Hite SA. Ethanol ingestion inchildren. A five year review. JAMA 1979;242:2787-8.Pruitt AW. Anyan WR. Hill RM, et al. American Academy ofPediatrics Committee on Drugs. Ethanol in liquid preparationsintended for children. Pediatrics 1984;73:405-7.
Correspondcnce to Dr I A Auchterlonie, Raeden Centre, Mid-stocket Roaid. Aberdeen AB2 4PE.
Received 13 March 1985
Hypertrichosis due to primary hypothyroidism
S R STERN AND C J H KELNAR
Royal Hospital for Sick Children, Edinburgh
SUMMARY A 10 year old girl with hvpertrichosisassociated with primary hypothyroidism that re-solved after 6 months' replacement treatment withthyroxine is reported. It is important to consider thediagnosis of hypothyroidism in children withabnormal hairiness or distribution of body hair.
Hypertrichosis and hirsutism are common reasonsfor seeking medical advice, particularly in youngwomen. Only a small proportion of subjects have adiagnosable condition, and treatment is often un-satisfactory, especially in childhood.' Hypothyroid-ism is usually associated with loss of hair.2 Wereport a 10 year old girl whose hypertrichosis wasassociated with primary hypothyroidism and re-
on 26 March 2019 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.60.8.763 on 1 A
ugust 1985. Dow
nloaded from
764 Archives of Disease in Childhood, 1985, 60
solved after replacement treatment with thyroxinefor six months.
Case report
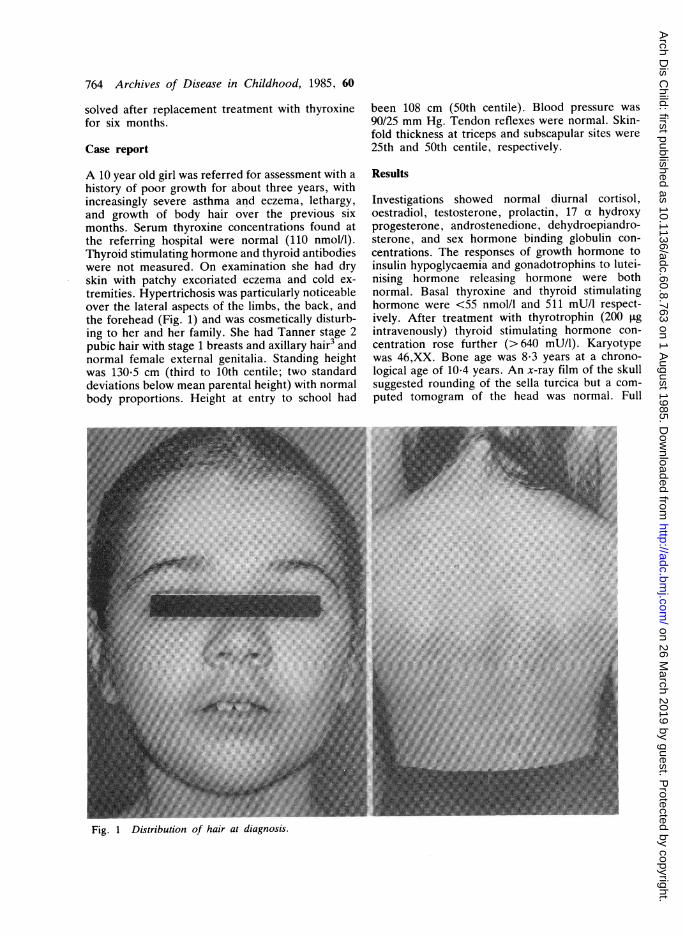
A 10 year old girl was referred for assessment with ahistory of poor growth for about three years, withincreasingly severe asthma and eczema, lethargy,and growth of body hair over the previous sixmonths. Serum thyroxine concentrations found atthe referring hospital were normal (110 nmol/l).Thyroid stimulating hormone and thyroid antibodieswere not measured. On examination she had dryskin with patchy excoriated eczema and cold ex-tremities. Hypertrichosis was particularly noticeableover the lateral aspects of the limbs, the back, andthe forehead (Fig. 1) and was cosmetically disturb-ing to her and her family. She had Tanner stage 2pubic hair with stage 1 breasts and axillary hair3 andnormal female external genitalia. Standing heightwas 130-5 cm (third to 10th centile; two standarddeviations below mean parental height) with normalbody proportions. Height at entry to school had
been 108 cm (50th centile). Blood pressure was90/25 mm Hg. Tendon reflexes were normal. Skin-fold thickness at triceps and subscapular sites were25th and 50th centile, respectively.
Results
Investigations showed normal diurnal cortisol,oestradiol, testosterone, prolactin, 17 a hydroxyprogesterone, androstenedione, dehydroepiandro-sterone, and sex hormone binding globulin con-centrations. The responses of growth hormone toinsulin hypoglycaemia and gonadotrophins to lutei-nising hormone releasing hormone were bothnormal. Basal thyroxine and thyroid stimulatinghormone were <55 nmoUl and 511 mU/l respect-ively. After treatment with thyrotrophin (200 igintravenously) thyroid stimulating hormone con-centration rose further (>640 mU/l). Karyotypewas 46,XX. Bone age was 8-3 years at a chrono-logical age of 10-4 years. An x-ray film of the skullsuggested rounding of the sella turcica but a com-puted tomogram of the head was normal. Full
Fig. 1 Distribution of hair at diagnosis.
on 26 March 2019 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.60.8.763 on 1 A
ugust 1985. Dow
nloaded from

Hypertrichosis due to primary hypothyroidism 765# e ES . agSejzjaogzs; l l X_ l l | | dSP _ l l __ | J *_ _ __ |_ __I fi # | _ 1| _ eB_ lX# | _ 1|_ | | _ _S%fi_ e R il _XMJ _ I | _ _EN§- Fo ...... | s g I | _ S... ...... 0 %,r . ........ . . _ _ ................. # l§Af RRM | B __ _ _ l | _ _|- A4EA ASIA
*tt i.'J_ | 1|1 W 1|_ | __A4|l__ .......... |* :;.: .:. . .' :: : ;: Y_ ! ! g l 0 I | _. . '.''. ' . ._ | | | , N I I-_'°o.'0.
Flg. 2 Dlstrlbutlon ofhalr after six months' treatment with thyroxine.
blood count showed an eosinophilia (806x 10'/I) andradioallergosorbent tests yielded strongly positiveresults for grass pollen. Abdominal ultrasoundshowed no adrenal abnormality but cystic enlarge-ment of the left ovary.
After receiving appropriate replacement withthyroxine (0.1 mg/m2/24 hours) the girl grew at anormal rate with appropriate advance in bone age.Thyroxine and thyroid stimulating hormone con-centrations became normal. She lost 4 kg in weight,skinfold thicknesses reached the 10th centile, andperformance at school and wellbeing improveddramatically. During six months her hypertrichosisresolved progressively (Fig. 2).
Discussion
It is unusual to find a cause for hypertrichosis orhirsutism and treatment is often unsatisfactory. 1 Thecausal association between hypothyroidism andhypertrichosis has not been reported in paediatricstudies, though congenitally hypothyroid infantsoften have a low hairline. Perloff reported four cases
of what he called hirsutism in children, with bodydistribution of hair similar to ours, who respondedto replacement treatment (thyroid extract),4 con-trasting with the case reported by Maekawa et al inwhich an underlying abnormality of keratinisationwas thought to lead to hair retention.5 The patho-physiology of the relation is unknown. The in-creased body hair in our patient was not generally inareas sensitive to androgen (hirsutism) despite somepubic hair growth. Clearly, stimulation of thegrowth of hair by hyperprolactinaemia mediated bythyroid releasing hormone, either directly or viaadrenal androgens, was not the mechanism in ourpatient.
Cystic ovarian enlargement in untreated hypo-thyroidism is well recognised.6 In most cases, as inours, ovarian size returns to normal with treatment.
It is difficult to explain the normal plasmathyroxine concentration obtained at the referringhospital, particularly in the absence of a simulta-neous measurement of thyroid stimulating hor-mone. In view of the length of the history ofimpairment of growth, compensated hypothyroid-
on 26 March 2019 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.60.8.763 on 1 A
ugust 1985. Dow
nloaded from

766 Archives of Disease in Childhood, 1985, 60
ism seems unlikely, and an error in handling or assayis more probable. Measurement of thryroid stimu-lating hormone might have enabled the diagnosisconsiderably earlier.We suggest that full assessment of thyroid func-
tion be carried out in all cases of hypertrichosis orabnormal distribution of body hair. If hypothyroid-ism is noted and treated the loss of body hair may bedramatic and, to the patient, extremely rewarding.
References
Ginsburg J, White MC. Hirsutism and virilization. Br Med J1980;280:369-7 1.
2 Church RE. Br J Dermatol 1965;77:661.3 Tanner JM. Growth at adolescence. 2nd ed. Oxford: BlackwellScience Publications. 1962.
4 Perloff WH. Hirsutism-a manifestation of juvenile hypo-thyroidism. JAMA 1955;157:651-2.
5 Maekawa Y. Rolled hair and hypertrichosis-a manifestation ofjuvenile hypothyroidism. J Dermatology (Tokyo) 1983;10:157-60.
6 Lindsay AN, Voorhess ML, MacGillivray MH. Multicysticovaries in primary hypothyroidism. Obstet Gynecol 1983;61:433-7.
Coirespondence and requests for reprints to Dr C J H Kelnar,Royal Hospital for Sick Children, Edinburgh EH9 ILF.
Received 5 March 1985
Congenital hypothyroidism with hereditary, raised thyroxinebinding globulin
L N J ARCHER, B P O'MALLEY, AND P G F SWIFT
Departments of Child Health and Pharmacology, University of Leicester and Departnment of Paediatrics,Leicester Royal Infirmary
SUMMARY A boy with congenital hypothyroidismand hereditary raised thyroxine binding globulin isdescribed. This hitherto unreported combinationresulted in under treatment of the thyroid deficiencyuntil serum thyroid stimulating hormone measure-ment became routinely available. Inadequate L-thyroxine replacement treatment between 2 and 7years of age caused retarded bone maturation, poorgrowth velocity, and probably added to his educa-tional difficulties.
Abnormalities in serum thyroxine binding globulinmay be inherited or acquired,' and result in raisedor depressed total thyroid hormone concentrationseven in euthyroid subjects. If true thyroid dysfunc-tion occurs in the presence of thyroxine bindingglobulin derangement, diagnosis and managementwill be unsatisfactory unless the existence of bothabnormalities is recognised. We report a patientwith congenital hypothyroidism in association withhereditary, raised thyroxine binding globulin, acombination not previously described.
Case history
A boy (birthweight 3180 g) was born at term in 1970.Perinatal and family medical histories were normal.A clinical diagnosis of hypothyroidism was made at3 months of age when he presented with an
umbilical hernia, and this was confirmed by aprotein bound iodine value of 3 [tg/100 ml (normalrange 4-0 to 8-4 Ftg/100 ml). Treatment with oral L-thyroxine (150 'tg daily) was begun at 14 weeks ofage. He smiled at 3 months, sat unsupported at 8months, and walked at 20 months. At 22 months,the family moved to a new area, at which time hisheight was at the 50th centile, three ossificationcentres had been reported on a wrist radiograph(now unavailable), and the protein bound iodineconcentration was 12 ,tg/100 ml. Apart from hisdelay in walking, development was considerednormal. In view of the high protein bound iodineconcentration, thyroxine treatment was graduallyreduced. At 2½/2 years it was stopped completely forfive weeks, whereupon the protein bound iodine fellto 1-7 [tg/100 ml. L-thyroxine treatment (50 [ig orallydaily) was begun again, after which the proteinbound iodine rose to 15-2 [tg/100 ml. Again histhyroxine treatment was reduced to 25 [tg daily andhe remained on this dose from age 2-8 years until7-25 years. Over this period his height fell from the50th centile to the 3rd centile with a correspondinglyslow rate of increase. Radiological bone age wasreported as 'within normal limits' at chronologicalage 2 years, and was 6 years (Greulich and Pyle) at achronological age of 8 years. He entered a normalprimary school, but required remedial teachingbecause of slow progress. Although poor growthcaused concern, no alteration was made to thethyroxine dose (25 [tg daily) as protein bound iodine
on 26 March 2019 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.60.8.763 on 1 A
ugust 1985. Dow
nloaded from