total hip replacement
DESCRIPTION
Total Hip ReplacementTRANSCRIPT

Bulletin on the effectiveness of health serviceinterventions fordecision makers
Nuffield Institute for Health,University of Leeds,
NHS Centre for Reviewsand Dissemination, University of York
OCTOBER 1996 VOLUME 2 NUMBER 7 ISSN: 0965-0288
Total hip replacement
EffectiveHealth Care
■ The rate of elective totalhip replacement isincreasing. Around 40,000were carried out by theNHS in 1994/95 and asubstantial number by theprivate sector.
■ Total hip replacement is ahighly cost-effectiveprocedure, howeveroutcomes vary across thecountry.
■ Decision aids to identifypatients suitable for referalfor total hip replacementhave been developed.
■ A large number of hipprostheses are used inBritain widely differing inprice. Very few of thesehave had proper long-termevaluation.
■ The cheaper, standardcemented, implants such asthe ‘Charnley’ and the‘Stanmore’ have been the
most thoroughly evaluatedand have been shown tohave the lowest long-termfailure rates over 10–20years follow-up.
■ Purchasers and providersshould promote the use ofthose prostheses whichhave been shown toperform best in long-termfollow-up.
■ New prostheses shouldonly be used after theyhave been thoroughlyevaluated or as part of anational coordinated study.
■ There is some evidencethat patients operated onby trainees and surgeonswith low volume of activityhave poorer outcomes.
■ Purchasing ‘lifetime hipcare’ rather than individualprocedures may provide anincentive to promotequality.

2 EFFECTIVE HEALTH CARE Total hip replacement OCTOBER 1996
A. BackgroundElective total hip replacement(THR) surgery is performedprimarily to relieve pain, stiffnessand deformity caused by disease ofthe hip joint.
There has been an increase in theoverall rate of THRs performedover the last decade (Fig. 1) withover 38,000 elective THRsperformed by the NHS in Englandin 1994/5. Over three-quarters ofthese were performed as a primaryprocedure.1 The demand forprimary THR may increase furtherbecause disease of the hip is age-related and people are livinglonger (Table 1).
Some hip replacements fail after aperiod of time by breaking,loosening, wearing or becominginfected. Hip replacements toreplace a failed one (revisionprocedure) form about 11% of allelective THRs and are likely toincrease as the length of life of
those receiving hip replacementsincreases.
In a study of three English healthdistricts in 1991, 20% of THRs hadbeen performed privately.2 This isconfirmed by a recent estimatethat around 11,000 operations areundertaken in the private sectoreach year. (Houghton, personalcommunication, 1995)
This bulletin considers theresearch evidence on whetherhealth care needs are being met,the effectiveness and cost-effectiveness of different types ofTHR surgery and suggests howthis evidence can be used bypurchasers, providers and policymakers to improve the quality of
care. Relevant literature wasidentified by electronic andmanual searches, as detailed inAppendix 2.
There are important aspects of thissubject that are not dealt with inthis bulletin:
• Rehabilitation after surgery:whilst the quality of surgery isimportant, the degree to which itcan improve physical and socialfunctioning may be affected bythe programme of post-operativerehabilitation. Research onrehabilitation was not reviewedas part of this bulletin.
• Antibiotics to prevent infection:One of the complicationsfollowing THR is loosening ofthe prosthesis due to infection
which may result in the need fora revision. A systematic reviewof the research on antibioticprophylaxis in THR is beingconducted by the NHS Centrefor Reviews and Disseminationon behalf of the Standing Groupon Health Technology and willbe available at the end of 1997.
• Prevention of deep veinthrombosis: Anothercomplication of major surgerylike THR is the development ofdeep vein thrombosis and, morerarely, pulmonary embolus.There is a widely held view thatall patients should be giventhromboprophylaxis (such as thelow molecular weight heparin orwarfarin). There is a concernhowever, that the incidence ofserious complications is now solow, and the costs and risk ofusing the drugs relative topotential benefits too high tojustify routinethromboprophylaxis.
The whole question ismethodologically complex andmany of the studies and reviewsin this area are of doubtfulquality or relevance tocontemporary practice. On thebasis of existing knowledge wefeel that it is not possible toproduce valid evidence-basedrecommendations on this issueas part of this bulletin.
B. Need forsurgeryB.1 Who should receive THRsurgery?: Although severity ofpain and disability are theprincipal indications for surgery,few studies have examined theappropriate indications for surgeryin detail.
According to the US NationalInstitutes for Health ConsensusDevelopment ConferenceStatement,3 ‘Candidates forelective THR should haveradiographic evidence of jointdamage and moderate to severe
Age Male Female
45-54 0.4 0.5
55-64 1.6 1.9
65-74 2.5 3.8
75-84 3.4 4.6
85+ 1.7 1.9
Table 1 Age and sex-specific electiveTHR rates per thousand population,English NHS hospitals 1994/51
Fig. 1 Rate of Elective Total Hip Replacement in England (Age-sex standardisedrate/1,000 population 45+)1
1990/91
0
.5
1
1.5
2
1991/92 1992/93 1993/94 1994/95

Total hip replacement EFFECTIVE HEALTH CARE 3OCTOBER 1996
pain and/or disability that is notrelieved by an extended course ofnon-surgical management.’However, this does not provideclear indications for referal ortreatment. A recent study4
employed a structured approach todevelop consensus indications forthe appropriateness of surgerybased primarily on the Charnleyscore of severity.5
Particularly helpful, especially forgeneral practitioners andpurchasers, is a recent set ofpatient referal appropriatenessratings and urgency rankings.6
Structured as a decision tree, itallows GPs to take into accountimportant clinical and socialfactors which indicate the likelybenefit patients will derive from aTHR. These include factors such asthe patientís age, level offunctioning, degree of pain,problems with work or caregivingand the likely survival of theprosthesis based on patientcharacteristics. This decision aidcan be used by practitioners andmanagers to rapidly assess theneed and urgency for referral, andthe degree of appropriateness ofreferral for hip or kneereplacement in audit.
B.2 Unmet need for THR: Astudy of Oxford districts showedthat there has been a trend
towards greater equity in localNHS THR surgery in the decadefrom 1976–85.7 Recent nationaldata however, show that there arestill significant variations in districtage and sex adjusted rates (Fig. 2and Appendix 1).
Various community surveys havebeen carried out to estimate thedegree of unmet need for THR inthe population. A postalquestionnaire and follow-uptelephone interview of a generalpractice population in Oxford in1993 estimated that 3.3% had hipsymptoms which warrantedsurgery.8 A large postalquestionnaire survey in NorthYorkshire has estimated that about2% of people over 55 may benefitfrom knee replacement9 and thatover 1% had levels of pain anddisability consistent with the needto consider THR.10
These studies are limited by theirsole reliance on a limited set ofsymptoms. A population study of28,000 adults has recently beenundertaken in Avon and Somerset,which screened a randomlyselected sample of the population.Five per cent reported symptomsof hip disease11 and these will befollowed up with detailed history,clinical and radiologicalexamination with the aim ofestimating the population
requirements for THR surgery. Thefull results will be available at theend of 1996 and may give morereliable estimates of levels ofunmet need.
It is not clear the extent to whichidentified unmet need is the resultof a backlog created by insufficientsurgery in the past or whethercurrent rates of surgery are failingto meet the needs of new orincident cases. Estimates of need arealso likely to vary over time ascritiera change in reponse tochanges such as advances inanaesthetic technique which reducethe risk of surgery for older patients.
C. Effectivenessof THRThere is no doubt that total hipreplacement results in a significantand sustained improvement in thequality of life for the majority ofpatients who have the operation.12
Because of the dramatic andimmediate effects on pain andmobility there is no need forplacebo-controlled trials toestablish the effectiveness of theprocedure.
The outcomes of primary THRsurgery however, in terms oftechnical success, morbidity andpatient satisfaction, are highlyvariable.13,14 The success of THRdepends inter alia on the type ofprosthesis used, method of fixation(whether cement is used and whattype), the surgical technique, and arange of measurable andunmeasurable patient andclinician factors.
C.1 Large number ofunevaluated prostheses: It hasbeen estimated that there arearound 62 different replacementhip joints available in Britainmanufactured by 19 differentcompanies, ranging in cost from£250 to £2000; half of these havebeen introduced since 1990.15
Most of these prostheses have notbeen properly evaluated and so noone knows how long they will last.
Fig. 2 Rate of elective total hip replacement in England by region and district(Age-sex standardised rate/1,000 population 45+)1
4 EFFECTIVE HEALTH CARE Total hip replacement OCTOBER 1996
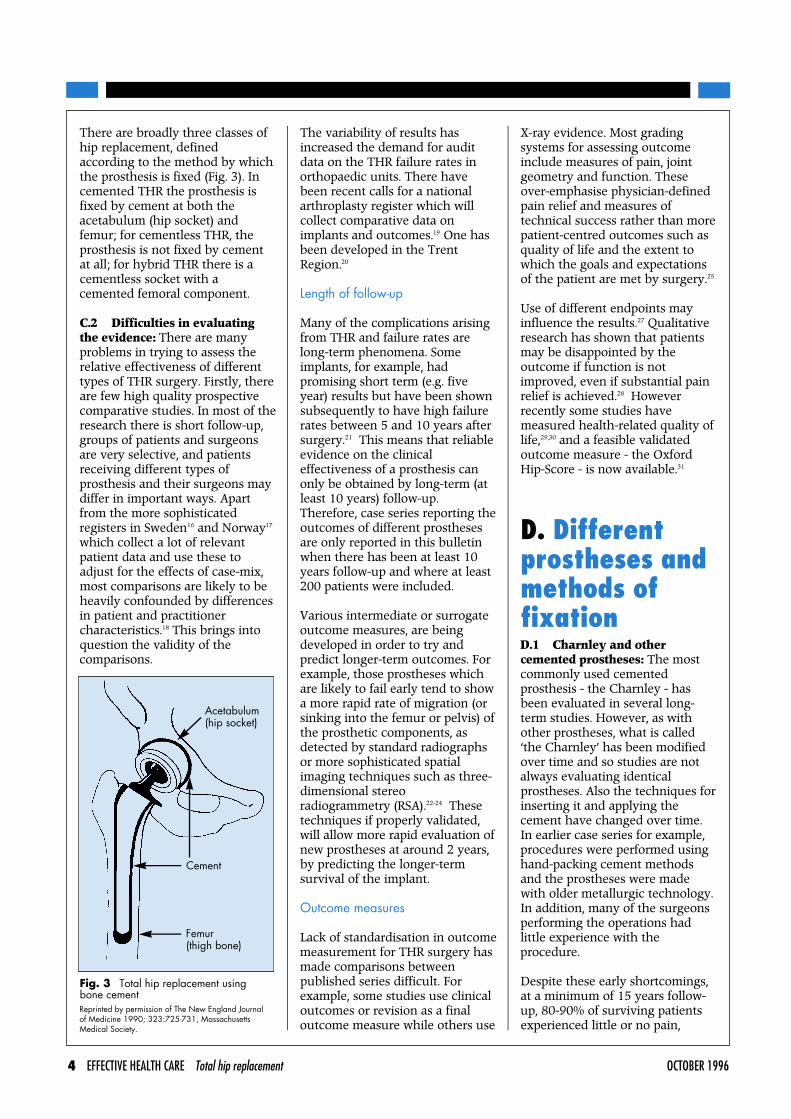
There are broadly three classes ofhip replacement, definedaccording to the method by whichthe prosthesis is fixed (Fig. 3). Incemented THR the prosthesis isfixed by cement at both theacetabulum (hip socket) andfemur; for cementless THR, theprosthesis is not fixed by cementat all; for hybrid THR there is acementless socket with acemented femoral component.
C.2 Difficulties in evaluatingthe evidence: There are manyproblems in trying to assess therelative effectiveness of differenttypes of THR surgery. Firstly, thereare few high quality prospectivecomparative studies. In most of theresearch there is short follow-up,groups of patients and surgeonsare very selective, and patientsreceiving different types ofprosthesis and their surgeons maydiffer in important ways. Apartfrom the more sophisticatedregisters in Sweden16 and Norway17
which collect a lot of relevantpatient data and use these toadjust for the effects of case-mix,most comparisons are likely to beheavily confounded by differencesin patient and practitionercharacteristics.18 This brings intoquestion the validity of thecomparisons.
The variability of results hasincreased the demand for auditdata on the THR failure rates inorthopaedic units. There havebeen recent calls for a nationalarthroplasty register which willcollect comparative data onimplants and outcomes.19 One hasbeen developed in the TrentRegion.20
Length of follow-up
Many of the complications arisingfrom THR and failure rates arelong-term phenomena. Someimplants, for example, hadpromising short term (e.g. fiveyear) results but have been shownsubsequently to have high failurerates between 5 and 10 years aftersurgery.21 This means that reliableevidence on the clinicaleffectiveness of a prosthesis canonly be obtained by long-term (atleast 10 years) follow-up.Therefore, case series reporting theoutcomes of different prosthesesare only reported in this bulletinwhen there has been at least 10years follow-up and where at least200 patients were included.
Various intermediate or surrogateoutcome measures, are beingdeveloped in order to try andpredict longer-term outcomes. Forexample, those prostheses whichare likely to fail early tend to showa more rapid rate of migration (orsinking into the femur or pelvis) ofthe prosthetic components, asdetected by standard radiographsor more sophisticated spatialimaging techniques such as three-dimensional stereoradiogrammetry (RSA).22-24 Thesetechniques if properly validated,will allow more rapid evaluation ofnew prostheses at around 2 years,by predicting the longer-termsurvival of the implant.
Outcome measures
Lack of standardisation in outcomemeasurement for THR surgery hasmade comparisons betweenpublished series difficult. Forexample, some studies use clinicaloutcomes or revision as a finaloutcome measure while others use
X-ray evidence. Most gradingsystems for assessing outcomeinclude measures of pain, jointgeometry and function. Theseover-emphasise physician-definedpain relief and measures oftechnical success rather than morepatient-centred outcomes such asquality of life and the extent towhich the goals and expectationsof the patient are met by surgery.25
Use of different endpoints mayinfluence the results.27 Qualitativeresearch has shown that patientsmay be disappointed by theoutcome if function is notimproved, even if substantial painrelief is achieved.28 Howeverrecently some studies havemeasured health-related quality oflife,29,30 and a feasible validatedoutcome measure - the OxfordHip-Score - is now available.31
D. Differentprostheses andmethods offixationD.1 Charnley and othercemented prostheses: The mostcommonly used cementedprosthesis - the Charnley - hasbeen evaluated in several long-term studies. However, as withother prostheses, what is called‘the Charnley’ has been modifiedover time and so studies are notalways evaluating identicalprostheses. Also the techniques forinserting it and applying thecement have changed over time.In earlier case series for example,procedures were performed usinghand-packing cement methodsand the prostheses were madewith older metallurgic technology.In addition, many of the surgeonsperforming the operations hadlittle experience with theprocedure.
Despite these early shortcomings,at a minimum of 15 years follow-up, 80-90% of surviving patientsexperienced little or no pain,
Cement
Femur(thigh bone)
Acetabulum(hip socket)
Fig. 3 Total hip replacement usingbone cementReprinted by permission of The New England Journalof Medicine 1990; 323:725-731, MassachusettsMedical Society.

Total hip replacement EFFECTIVE HEALTH CARE 5OCTOBER 1996
though X-ray results, showingchanges in the bone, were lessencouraging. More experience,new techniques for insertion(including pressurization ofcement), improved design andnewer metallurgy have led tominimal loosening rates at 5 and10 year follow-up. Altogether, 20series meeting our criteria (C.2)were found for the Charnleyprosthesis (Table 2a).16,21,26,32-49
A further two series examinedoutcomes for acetabularcomponents only (Table 2b).45,50
Most of these studies show that at10-20 years follow-up, around 90%or more of patients followed havereasonably good clinical outcomes.
Implant survivorship at a level of90% or better has been found withsome alternative cementedimplants, notably the Stanmore,and the Lupinus (Table 3).21,26,51-53
The comparability of the Stanmoreand the Charnley was alsosuggested by a recent randomisedcontrolled trial.54 In contrast, the10 year follow-up results of othercemented implants such as theMcKee-Farrar, the Exeter mattsurface, Muller curved and theChristiansen are not so impressive(Table 3).21
D.2 Non-cemented prostheses:Tables 4a and 4b summarize thefour series which assessed theoutcome of primary surgery with acementless femoral component or acementless acetabulum and meetthe criteria.53,55-57 These prosthesesare generally poorer than thecemented prostheses. Non-cemented prostheses are not ahomogeneous group. The earlygeneration of, mainly, porousimplants gave disappointing results.Failure rates were generally higherthan for cemented prostheses,partly because they were not fixingwell into the bone. Newer ones,which have a hydroxyapatitecoating in order to promote boneingrowth, are producing moreencouraging results which remainto be confirmed in trials withlonger follow-up.58
Cemented and uncementedprostheses have also beencompared in randomisedcontrolled trials (Table 5)12,59-63
Results from the trials aremarginally in favour of cementedprostheses, but are inconclusivebecause of small numbers,inadequate adjustment of riskfactors and limited duration offollow-up.
Overall the case series and trialsfavour the routine use ofcemented prostheses, in particularthe Charnley and the Stanmore.This is supported by data collectedfrom all 64 Norwegian hospitalsperforming THR.64 24,408 primaryTHR operations were registeredbetween September 1987 andFebruary 1993. The cumulativefailure after 4.5 years was 2.7% forcemented, compared with 6.5% forcementless.
D.3 Revisions: Generally thereare much poorer outcomesfollowing revision of THR, thanwith primary THR, with looseningrates ranging from 20%65 to 29%66
and with re-revision rates of 6.7%and 19% respectively. Results ofcemented revisions with orwithout bone grafting appearinadequate in the intermediate (5-10 years) and long run (greaterthan 10 years). The overall datarelevant to cementless revisionsurgery are short-term, of poorquality and inconclusive.
E. Volume andspecialisationE.1 Skills: Implant design andthe method of fixation are not theonly aspects of surgery whichaffect the outcomes of care. It islikely that surgical skill andtechnique are also important. Arandomised controlled trialcomparing the Charnley with theStanmore implant, for example,found that the THRs carried outby trainees in England were over11 times more likely to need arevision than those carried out bya consultant (P=0.005).54
E.2 Volume: Ten studies wereidentified which have examinedthe relationship between the shortterm outcome of patientsundergoing hip or kneereplacement and hospital orsurgeon volume of surgicalactivity.16, 67-75 Most were carriedout in the USA and were mainlybased on retrospective analyses ofdischarge abstract data. Only 6 ofthem made any serious attempt toadjust for differences in case mixbetween high and low volumeinstitutions or clinicians.16,67,69,70,72,73
All but two of the better studies12,69
found that higher hospital volumeand/or clinician volume of jointreplacement surgery wasassociated with a lower rate of postoperative death, shorter length ofstay or post-op complications.However the level at which thisoccurs appears to be relatively low.Only the study based on a largeSwedish Registry, examined anyassociation with medium- or long-term outcomes. It foundsignificant variations in the rate ofaseptic loosening betweenconsultants. This could not beexplained however, by differencesin the volume of activity.16
F. EconomicaspectsF.1 Cost-effectiveness of THR:THR results in a considerableimprovement in quality of life in ahigh proportion of patients whichis sustained for several years.29,30
THR has also been estimated to behighly cost-effective.
Williams76 (assuming a failure andrevision rate of 2% per year)estimated the cost utility of THR atabout £750 per Quality AdjustedLife Year (QALY) gained. Thiscompared favourably with acost/QALY gained of £14,000 forone year of hospital haemodialysis,and of £5,000 for hearttransplantation. Broadly similarconclusions have been reached inother studies.12,77,78 A recent UScost-effectiveness analysis from a

6 EFFECTIVE HEALTH CARE Total hip replacement OCTOBER 1996
Authors/study design/age of patients
Britton et al (1996)26
Descriptive (prospective)
Older (1986)32
Descriptive (prospective)including pre-op status
42-55 yrs (median=64)
Johnston & Crowninshield(1983) 33
Descriptive (retrospective)
Age not stated
Neumann et al (1994)34
Descriptive (prospective)including pre-op status
34-79 yrs (median=62)
Older & Butorac (1992)35
42-85 yrs (mean=68)
Wroblewski & Siney(1993)36
Descriptive (prospective)post-op status only
23-68 yrs (mean=47)
Dall et al (1993)37
Descriptive (retrospective)
Mean age = 60 yrs
Schulte et al (1993) 38
Descriptive (prospective)including pre-op status
29-86 yrs (mean=65)
Skeie et al (1991)39
Descriptive (prospective)post-op status only
23-88 yrs (mean=66)
Thomas & McMinn(1991)40
Descriptive (retrospective)
Ages not stated
Charnley (1979)41
Ages not available
Stauffer (1982)42
Descriptive (retrospective)
39-84 yrs (mean=64)
Johnsson et al (1988)43
Descriptive (retrospective)
M 36-87 yrs (median=65)F 47-84 yrs (median=67)
No. of operations/% follow-up/duration offollow-up (yr)
20894% (amongst alive)24% died1-16 yrs
21770.5%10-12 yrs
32655.8%10 yrs
24196% survivors (n=103)15-20 yrs
38834%17-21 yrs
1324 -18-26 yrs (av 10 yrs)
811 66.2%10-12 yrs
32298.5%20+ yrs
629 89.7%10-15 yrs
1069 -10+ yrs
302-12-15 yrs
20790%10 yrs
204100%4-14 yrs
Other risk factors
Diagnosis OA,diagnosis RA
Age at surgery, sex,diagnosis OA,diagnosis RA,surgical approach,patient risks:infection
-
Age at surgery, sex,body mass index,diagnosis OA,diagnosis RA,surgical approach,previous surgery,weight
Age, sex, diagnosisOA, diagnosis RA,patient risks:infection
Age at surgery,diagnosis OA,diagnosis RA,surgical approach
Age at surgery, sex,diagnosis OA,diagnosis RA,bilateral/unilateral
Diagnosis OA,diagnosis RA
Diagnosis OA,diagnosis RA
-
-
Age, sex, diagnosisOA, diagnosis RA,surgical approach
Age, sex, diagnosisOA, surgicalapproach, other
Status ofsurgeon/typeof hospital
Consultant/District generalhospital
Consultant/Specialist centre
-/Teachinghospital
Consultant/Teaching hospital
-/Districtgeneral hospital
-/Specialistcentre
-/Teachinghospital
Consultant/Teaching hospital
-/Districtgeneral hospital
-/Specialistcentre
-
-/Specialistcentre
-/Teachinghospital
Outcomemeasures
Survivorship,pain, observer-defined function,gait, jointgeometry
Survivorship,pain, observer-defined function,gait, jointgeometry, X-raycriteria
X-ray criteria
Survivorship,pain, observer-defined function,joint geometry,X-ray
Survivorship,X-ray
Survivorship,pain, observer-defined function,joint geometry,X-ray definedcriteria
Survivorship,pain, observer-defined function(d’Aubigne), jointgeometry, X-raydefined criteria
Survivorship,pain, observer-defined function,joint geometry,X-ray definedcriteria
Survivorship,pain, observer-defined function,joint geometry,X-ray definedcriteria
Survivorship
-
Survivorship,X-ray
Survivorship
Results
Survivorship at 10yrs 84%(revision); at 10yrs and14yrs 84% and 79%(revision, moderate orsevere pain)
88% satisfactory, 6%revision, 92% satisfied
9% femoral loosening,7.9% acetabular loosening
Probability of revision10.7% at 20 yrs, 7% <3for pain movement(Charnley score), 30%loosening
Revision 6%, loosening17% cups, survivorship89% at 20 yrs (cup & stem)
Dislocation 0.63%, revision0.11%, infection 0.3-1.5%,pain free 85%; normalfunction 60%
Survivorship 87% 10-12yrs, 8% revised
90% survivorship (retainedimplant), 85% pain free,53% no walking aids, 10%revised
92% survivorship at 13years; 86% patients goodresult, 7% revised
92% survivorship at 10 yrs,no improvement followingchanges of cementtechniques
>5.8% revisions
Revisions 10.8%, cuploosening 11.3%, stemloosening 29.9%
Revision 14.7%
Table 2a Charnley primary total hip replacement series with at least 200 THRs and 10 years follow-up (with trochanteric osteotomy) using old cementation

societal perspective, estimated thatfor most people the procedure wasrelatively cost-effective.79 Forwomen under 60 the ratio rangedfrom $16,000 per QALY gained,(cost saving) to $27,000 per QALYgained in the best and worst casescenarios respectively. Even formen over 84 years the costeffectiveness ranged from $4,600to $80, 000 per QALY gained.These estimates vary according toa number of factors such as theseverity of the pre-operative state,
potential for achieving benefit,length of remaining life and co-existing disease.
F.2 Cost containment andpromoting quality: In view of theexpanding costs of THR, costcontainment programmes havebeen established in some UShospitals. Because the cost of theprosthesis is becoming anincreasing proportion of the totalhospital THR costs, theseprogrammes have tended to
concentrate on keeping down thecost of the prosthesis. A 14%reduction in prosthesis costs wasreported in one hospital in theUSA by adopting a structuredapproach to the choice ofprosthesis.80 Standardisation of thehip prosthesis has been estimatedto be able save about 25% of thecost of implants in some UShospitals.81
Because the Charnley andStanmore prostheses are both
Total hip replacement EFFECTIVE HEALTH CARE 7OCTOBER 1996
Authors/study design/age of patients
Malchau et al (1993)21
(incorporates Ahnfelt et al,1990 16)
Descriptive (prespective),Swedish national registry
M median = 66 yrsF median = 64 yrs
Carter et al (1991) 44
Descriptive (retrospective)
Ages not stated
Garcia-Cimbrelo &Munera (1992)45
Descriptive (retrospective)
18-79 yrs (mean=56)
Wejkner & Stenport(1988) 46
Descriptive (retrospective)
>30 <80 yrs (mean=64)
Eftekhar (1987) 47
Descriptive (retropective)
Ages not stated
Kavanagh et al (1989) 48
Descriptive (retrospective)
M 35-85 yrs (mean=65)F 39-84 yrs (mean=64)
Iannoti et al (1986) 49
Descriptive (retrospective)
mean=62.2 (SD=10.8)
No. of operations/% follow-up/duration offollow-up (yr)
92,675100%?10 yrs
1616 31%10-20 yrs
68060% at 10 yrs18 yrs
32550%10-14 yrs
1009 (20% revision/conversions)69%5-15 yrs
33349.8%15 yrs
258 (primary)100%3-10 yrs
Other risk factors
Age, sex, diagnosisOA, diagnosis RA,other
Not stated
Age, sex, diagnosisOA, diagnosis RA,body mass index,surgical approach
Age at surgery, sex,body mass index,diagnosis OA, otherdiagnoses, previoussurgery, surgicalapproach
Surgical approach
Age at surgery, sex,body mass index,diagnosis OA,surgical approach,previous surgery
Age at surgery, sex,body mass index,diagnosis OA, otherdiagnoses
Status ofsurgeon/typeof hospital
All grades ofsurgeon/Alltypes of hospital
-/Districtgeneral hospital
Seniorsurgeons/specialist centre
-/Teachinghospital, 86%hip surgeons
-/Specialistcentre, Singlesurgeon
-/Specialistcentre
-/Teachinghospital
Outcomemeasures
Survivorship
Survivorship
Survivorship,pain, observer-defined function,gait, jointgeometry, X-ray
Pain, observer-defined function,gait, X-raycriteria
Survivorship
Pain, observer-defined function,gait, X-raycriteria
Pain, observer-defined function,gait, X-raycriteria
Results
Revisions around 9%.Similar results for C.A.D.and Lubinus.Worse results for othercemeneted implants: Mullercurved, Exeter, Spectron,PCA and the Christiansen.
Survivorship 91% 10 yrs,Survivorship 82% 20 yrs
Survivorship 81% at 18 yrs,survivorship 91.6% at 10yrs, pain 4.6 at 17 yrs(Aubigne/Postel &Charnley), walking 4.6 at17 yrs, ROM 4.4 at 17 yrs
56% excellent, 28% good,8% fair, 8% failure(Charnley scores)
Mechanical failure andinfectious causes
Probability of failure: 1 yr,0.9%; 5 yrs, 4.1%; 10 yrs,8.9%; 15 yrs, 12.7%
75% satisfactory pain; 95%satisfactory function
Table 2a Continued
Carlsson et al (1986) 50
Descriptive (retrospective)
Garcia-Cimbrelo &Munera (1992) 45
Descriptive (retrospective)
20768.7% (207 OA, 34RA)5-12.5 yrs (OA)3.4-12 yrs (RA)
79186%12.8 yrs (mean)
Age at surgery, sex,diagnosis OA,diagnosis RA, other
Age at surgery, sex,diagnosis OA,diagnosis RA, other
-/Teachinghospital
-/Teachinghospital
OA 26% loosening, RA34% loosening
81% survivorship at 18 yrs
X-ray criteria
Survivorship, X-ray criteria
Table 2b Primary surgery with a Charnley cemented acetabulum (with at least 200 THRs and 10 years follow-up)

8 EFFECTIVE HEALTH CARE Total hip replacement OCTOBER 1996
Authors/study design
August et al (1986) 51
Descriptive(retrospective)
Jantsch et al (1991)52
Descriptive(retrospective)
Britton et al (1996)26
Descriptive (prospective)
Comparison withCharnley (Table 2a)
Bryant et al (1991) 53
Descriptive (prospective)
Prosthesis
McKee-Farrar
McKee-Farrar
Stanmore
Ring
No. ofoperations/% follow-up/duration offollow up (yr)
80828.4%13.9 yrs (mean)
33056%14 yrs (mean)
98294% (amongstalive) 24% died1-16 yrs
25390.5%1-21 yrs
Other riskfactors
Age atsurgery,diagnosis OA,diagnosis RA,surgicalapproach
Age atsurgery, sex,weight,diagnosis OA,diagnosis RA
Diagnosis OA,diagnosis RA
Age atsurgery,diagnosis OA,diagnosis RA
Status ofsurgeon/typeof hospital
-/Districtgeneralhospital, 72%by consultant
-/Specialistcentre
Consultant/District generalhospital
-/Teachinghospital
Outcomemeasures
Pain,observer-definedfunction,gait, jointgeometry,X-ray criteria
Pain,observer-definedfunction,gait, jointgeometry
Survivorship,pain,observer-definedfunction,gait, jointgeometry
Survivorship
Results
Good/excellent (Harris),49%; survivorship 91% 10yrs, 84% 15 yrs, 49% 19yrs
62% excellent/good (Mayoscore); 22% poor.35% of those followed uprevised
Survivorship at 10yrs 93%(revision); at 10yrs and14yrs 88% and 80%(revision, moderate orsevere pain)
70% and 60.4% cumulativesurvivorship (revision) after10 yrs and 20 yrsrespectively
Table 3 Primary surgery with other cemented prostheses (with at least 200 THRs and 10 years follow-up)*
Authors/Study design
Engh et al (1990)55
Descriptive (prospective)
Bryant et al (1991)53
Descriptive(retrospective)
Engh et al (1990)55
Descriptive(retrospective)
Prosthesis
AML
Ring Mark2
PCA
No. ofoperations/% follow-up/duration offollow up (yr)
1048 (primary)91.5%2-11 yrs
25346.7%11-21 yrs
95991.5%2-12 yrs
Status ofsurgeon/typeof hospital
-/Specialistcentre
-/Teachinghospital
-/Specialistcentre
Outcomemeasures
Survivorship,pain,observer-definedfunction,gait, jointgeometry,X-ray criteria(Postel-d’Aubigne)
Survivorship,pain,observer-definedfunction,gait, jointgeometry
Survivorship,pain,observer-definedfunction,gait, X-raycriteria
Results
Survivorship: 96.4%(revision) at 10 yrs; 90.8%(mechanical failure) at 10yrs 19.5% revision
Survivorship 60.4% at 21yrs; 26.5% revisions; 6.4%excellent, 31.9% good,40.4% fair, 21.3% poor
Survivorship at 10 yrs:96.4% (revision); 90.8%(revision and loosening)
Table 4a Primary surgery with cementless femoral prostheses (with at least 200 THRs and 10 years follow-up)
*Also see Malchau et al 199321 Table 2a
Other riskfactors
Age atsurgery, sex,weight,diagnosis OA,diagnosis RA,surgicalapproach,patient co-morbidity,patient risks:Type femoralstemthromboembolism?
Age atsurgery, sex,diagnosis OA,diagnosis RA
Age atsurgery, sex,weight, bodymass index,diagnosis OA,diagnosis RA,other
Hauser et al (1993)56
Descriptive (prospective)including pre-op status
Scmitt et al (1993)57
Descriptive(retrospective)
EndlerBelgrist
Spiked 134Screw rings77
715-5-10 yrs
227-9.5 yrs (mean)
-/Teachinghospital
-/TeachingHospital
X-ray criteria
Revision,X-ray criteria
Probability of survival after5 yrs: Endler 94% Balgrist88-91% after 10 yrs: Endler44%
Screw: 1/3 migration, 13%revisionSpikes: 15% migration, 2%revision
Table 4b Primary surgery with a cementless acetabulum (at least 200 THRs and 10 years follow-up)
-
-

amongst the cheapest and bestperforming prostheses for mostpatients, cost minimisation andthe promotion of quality can beachieved by standardising onthese implants. A survey of 261NHS hospitals showed that 30types of cemented and 35 types ofcementless hip replacements arecurrently used in orthopaedicpractice.82 The Charnley lowfriction implant was only used in
about 75% of the hospitals. Asurvey of Fellows of the BritishOrthopaedic Association alsosuggests that only around aquarter of surgeons use ‘modern’cementing techniques.83
An increasing proportion of thetotal expenditure on hipreplacement surgery is onrevisions due to the failure of hipprostheses. One approach put
forward for increasing quality ofsurgery is for purchasers to buy alifetime care package whichincludes the present cost of thesurgery plus a premium for anyfuture surgery due to failure.84
The lowest price will be offered byproviders who, because they knowthat their surgery is of highquality, are less likely to have tocarry out a revision in the short-term. Thus, rather than the price
Total hip replacement EFFECTIVE HEALTH CARE 9OCTOBER 1996
Authors/Study design
Godsiff et al (1992)59
UK
Wykman et al (1991)60
(incorporates 119patients in Olsson et al,198561)
Sweden
Onsten & Carlsson(1994)62
Sweden
Rorabeck et al (1996)63
(4 year follow up ofRorabeck, 1994 12 andsame results as Mulliken,1996)
Canada
Marston et al (1996)54
England
Prosthesis
Ringfemoralcemented,acetabulumcementlessv femoralandacetabulumcementless
Charnleycemented vHonartPatel-Garches(press fit).
AllpolythenecementedCharnleysocket vsuncemeneted porousHarris-Galantetype 1socket.
Mallorycemented vMalloryuncemented
Charnleycemented vsStanmorecemented
No. ofoperations/% follow-up/duration offollow up (yr)
Cemented 30.Uncemented 284 months (81%),1 year (100%), 2years (81%)
75 v 756 months1 year5 yearsCharnley 91%HP Garches 93%
30 Charnley vs30 H-G100%12 years
125 cemented126 cementlessup to 6 (59% followedup for at least 4years)
200 vs 213 hips(360 patients)5-10 years(mean 6.5)5yrs 80% Ch,70% Stan10yrs 8% Ch,7% Stan
Other riskfactors
Age atsurgery, sex
Age atsurgery, sex,weight,diagnosis OA,diagnosis RA,surgicalapproach,infectionbilaterial andunilateraldisease
Sex, side, age,weight
Age atsurgery, sex,weight,diagnosis OA,diagnosis RA,surgicalapproach,patient risks:infection/thromboembolism
Age atsurgery, sex,weight,diagnosis OA,diagnosis RA,surgicalapproach,seniority ofsurgeon
Status ofsurgeon/typeof hospital
Consultant/District generalhospital
Major hospital
Specialist unit
Consultant/Teachinghospital
Specialisthospital
Outcomemeasures
Pain, use ofwalkingaids, activity
Pain,observer-definedfunction,gait, jointgeometry, X-ray criteria.Harris hipscore,patientsatisfaction,re-operation
Socketmigrationand rotationbyradiostereometry (RSA).
Pain andfunction byHarrisScore)
Pain,observer-definedfunction(Harris hipscore,d’Aubigne).Patientdefinedarthritisscore,SIP,TTO
Clinical andradiologicalassessment,revision
Results
Pain-free at 4 months: 58%cemented, 43%uncemented; pain free at 1yr: 63% cemented, 50%uncemented; pain free at 2yrs: 65% cemented, 63%uncemented. Walkingwithout support at 2 yrs:96% cemented, 62%uncemented (p<0.05).(Difference not significant at4 months or at 1 year
At 2 years, excellent orgood (Harris Hip Score)79% Charnley, 70% HPGarches. Revisions formechanical loosening in6.7% Charnley and 18.7%HP Garches (11% and 19%overall)
No revisions after 2 years.Mean Harris Hip score wasequal at baseline and after2 years.No difference in migrationor rotation
Both showed large andsustained increases inhealth related quality of life. No difference at 4 years indisease specific andpatient-centred measures. Cemented metal-backedacetabular componentshave high rate ofradiographic failure
Mean Harris Score postoperatively = 46 91 in bothgroups.Revision rate the same inboth groups. In all but onerevisions the operatingsurgeon was atrainee.(P<0.005)
Slightly higher radiologicalevidence of subsidence ofthe Stanmore stem than inthe Charnley in the first 6months (P=0.003)
Table 5 Randomised controlled trials comparing prostheses
of a THR being the determinant ofpurchaser choices, total futureexpected expenditure and benefitswould be more important. Noresearch evaluating such a schemehas been identified.
The Safety and Efficacy Register ofNew Interventional Procedures(SERNIP) recently established bythe Medical Royal Colleges mayplay a role in helping to controlthe diffusion of untestedprostheses.85
G. Implicationsfor services andresearch• A wide variety of untested
prostheses are in use in the NHS.Commissioners should be awareof what prostheses are beingused by those with whom theycontract for THR and shouldensure that cheap andthoroughly evaluated standardimplants like the Charnley lowfriction or the Stanmore areroutinely used unless there isadequate justification for anexception.
• Commissioners and providersshould ensure that new implantsand techniques, that have notbeen demonstrated to be morecost-effective than the standard,ones are not introduced withoutproper evaluation.
• In order to promote quality,providers and purchasers shouldrequire information on and ormonitor the outcomes of THR,and require audit of adversecases and high rates of revision.One aspect of potentialimportance is the grade ofsurgeon carrying out theoperation and the level ofsupervision.
• Commissioners might wish toconsider contracting for thelifetime hip care of patientsincluding a premium to cover
the risk of future costs due torevision of surgery.
Research Areas
• The likely impact of populationageing, changes in thresholds forsurgery, and trends in hipdisease to assess future need fororthopaedic services.
• The effect of a range ofenvironmental factorsinfluencing outcomes such asskills, training and supervision ofjunior staff.
• Validation of ‘pro-active’methods of predicting the long-term success of hip surgerywhich can be carried out usingfeasible measures within a fewyears of the operation. This willfacilitate more rigorous testingof new equipment.
• The use of these early indicatorsof failure in order to identifypatients who would benefitfrom earlier revision, thusavoiding more complex surgeryat a later date and improvinglong-term outcomes.
• Evaluation of approaches topromoting quality such aspurchasing ‘lifetime hip care’
Appendix 1: Routine hospital data
Data on the number of procedurescame from the Hospital EpisodeStatistics for the relevant years.Total Hip Replacement proceduresand prosthetic replacement of thehead of femur (OPCS codes W37,W38, W39, W46, W47, and W48and all subsidiary codes).Emergency cases and those wherethe primary diagnosis wasfractured neck of femur (ICDcodes 820 and 821) were excluded.
Appendix 2: Search strategy
The following databases weresearched: Medline (1966-1995);EM-base (1981-1995); ScienceCitation Index (1975-1995).
A manual search was made ofIndex Medicus and of referenceslisted in other publications.
For the general search the keywords used were: hip replacement,hip arthroplasty, hip prosthesis.The searches were limited tohuman subjects and Englishlanguage articles. Foreign articleswere reviewed if there was anabstract in English.
Studies using experimental andobservational data which followedup patients and measured patientoutcomes, including radiographicchanges, were identified.
References1. Department of Health. Hospital Episode
Statistics (HES) and population data provided bythe statistics division, DOH, 1996.
2. Williams MH, Frankel SJ, Nanchahal K, Coast J,Donovan J. DHA Project: Research ProgrammeEpidemiologically Based Needs Assessment.Total Hip Replacement. Health CareEvaluation Unit/NHS Management Executive,Dept Epidemiology & Public Health Medicine,University of Bristol,Bristol 1992;1.
3. National Institutes of Health. NationalInstitutes of Health Consensus DevelopementConference Statement - Total hip replacement.September 12-14, 1994.
4. Imamura K, Gair R, McKee M, Black N.Appropriateness of total of hip replacement inthe United Kingdom. (in press).
5. Charnley J. The long term results of lowfriction arthroplasty the hip performed as aprimary intervention. J Bone Joint Surg1972;54:61-76.
6. Naylor CD, Williams JI, the Ontario Panel onHip and Knee Arthroplasty. Primary hip andknee replacement surgery: Ontario criteria forcase selection and surgical priority. Quality inHealth Care 1996;5:20-30.
7. Seagroatt V, Tan HS, Goldacre M, Bulstrode C,Nugent Gill L. Elective and total hipreplacement:incidence, emergencyreadmission rate, and post operative mortality.BMJ 1991;303:1431-5.
8. Edwards MSD, Newton JN, Murray DW,Bulstrode CJK. What is the need for total hipand knee replacement in the community?British Orthopaedic Research Society, 1994.
9. Tennant A, Fear J, Pickering A, Hillman M,Cutts A, Chamberlain MA. Prevalence of kneeproblems in the population aged 55 years andover: identifying the need for kneearthroplasty. BMJ 1995;310:1291-3.
10. Fear J, Hillman M, Chamberlain MA, TennantA. Prevalence of hip problems in thepopulation aged 55 years and over: access tospecialist care and future demand for hiparthroplasty. Br J Rheumatology (in press).
11. Eachus J, Williams M, Chan P, Davey Smith G,Grainge M, Donovan J, Frankel S. Deprivationand cause specific morbidity: evidence fromthe Somerset and Avon survey of health. BMJ1996;312:287-92.
12. Rorabeck CH, Bourne RB, Laupacis A, et al. Adouble blind study of 250 cases comparingcemented with cementless total hiparthroplasty:cost effectiveness and its impacton health-related quality of life. Clin Orthop1994;298:156-64.
13. Williams MH, Frankel SJ, Nanchahal K, Coast J,Donovan JL. Total Hip Replacement. In:Stevens A, Raftery J, eds. Health Care NeedsAssessment. 1st ed. v. 1. Oxford: RadcliffeMedical Press, 1994:448-523.
10 EFFECTIVE HEALTH CARE Total hip replacement OCTOBER 1996

14. Bulstrode CJK, Murray DW, Carr AJ, et al.Designer hips. BMJ 1993;306:732-3.
15. Murray DW, Carr AJ, Bulstrode CJ. Whichprimary total hip replacement? J Bone JointSurg Br 1995;77:520-7.
16. Ahnfelt L, Herberts P, Malchau H et al.Prognosis of total hip replacement. A Swedishmulticenter study of 4664 revisions. ActaOrthop Scand Suppl 1990;238:1-26.
17. Havelin LI, Espehaug B, Vollset SE, et al. TheNorwegian arthroplasty register: A survey of17,444 hip replacements 1987-1990. ActaOrthop Scand 1993;64:245-51.
18. Morris R. Evidence-based choice of hipprostheses. J Bone Joint Surg Br 1996;78-B:691-3.
19. Sochart DH, Long AJ, Porter ML. Jointresponsibility: the need for a nationalarthroplasty register. BMJ 1996;313:66-7.
20. Harper WM, Gregg PJ. Trent regionalarthroplasty study: interim report and oneyear results. In: Wallace WA, ed. JointReplacement in the 1990s. Clinical Studies,Financial Implications and MarketingApproaches. 1st ed. Bury St EdmUnds:Mechanical Engineering Publications Ltd,1992:49-50.
21. Malchau H, Herberts P, Ahnfelt L, Johnell O.Prognosis of total hip replacement in Sweden.Follow-up of 92,675 operations performed in1978-1990. Acta Orthop Scand 1993;64:497-506.
22. Stocks GW, Freeman MAR, Evans SJW.Acetabular cup migration: prediction ofaseptic loosening. J Bone Joint Surg 1995;77B: 853-861.
23. Walker P, Mai S, Cobb A, Bently G, Hua J.Prediction of clinical outcome of total hipreplacement from migration measurements onstandard radiographs. J Bone Joint Surg Br1995;77:705-14.
24. Freeman MAR & Plante-Bordeneuve P. Earlymigration and late aseptic failure of proximalfemoral prostheses. J Bone Joint Surg, 1994;76B: 432-438.
25. Heaton J, Williams M, Long A, Dixon P, BrettleA. Measuring the health outcomes of total hipreplacement through the commissioningprocess. Outcome Measurement Reviews No.1Leeds:UK Clearing House for HealthOutcomes, May 1995
26. Britton AR, Murray DW, Bulstrode CK,McPherson K, Denham RA. Long termcomparison of Charnley and Stanmore designtotal hip replacements. J Bone Joint Surg Br1996;78-B 802-8.
27. Murray D, Carr A, Bulstrode CJK. Survivorshipanalysis in orthopaedics. In: Wallace WA, ed.Joint Replacement in the 1990s. ClinicalStudies, Financial Implications and MarketingApproaches. 1st ed. Bury St Edmonds:Mechanical Engineering Publications Ltd,1992:61-3.
28. Donovan JL, Blake DR, Fleming WG. Thepatient is not a blank sheet: lay beliefs andtheir relevance to patient education. Br JRheumatol 1989;28:58-61.
29. Rissanen P, Aro S, Sintonen H, Slatis P,Paavolainen P. Quality of life and functionalability in hip and knee replacements: aprospective study. Quality of Life Research1996;5:56-64.
30. Laupacis A, Bourne R, Rorabeck C, et al. Theeffect of elective total hip replacement onhealth-related quality of life. J Bone Joint Surg1993;75:1619-26.
31. Dawson J, Fitzpatrick R, Carr A, Murray, D.Questionnaire on the perceptions of patientsabout total hip replacement. J Bone Joint Surg1996;78-B 185-90.
32. Older J. Low friction arthroplasty of the hip. Aten to twelve year follow-up study. ClinOrthop 1986;211:36.
33. Johnston RC, Crowninshield RD.Roentegenologic results of total hiparthroplasty. A ten year follow-up study. ClinOrthop 1983;181:92-8.
34. Neumann L, Freund KG, Sorenson KH. Long-term results of Charnley total hipreplacement: Review of 92 patients at 15 to 20years. J Bone Joint Surg 1994;76:245-51.
35. Older J, Butorac R. Charnley low frictionarthroplasty (LFA): a 17-21 year follow-upstudy. J Bone Joint Surg 1992;74B suppl 3:251.
36. Wroblewski BM, Siney PD. Charnley lowfriction arthroplasty of the hip: Long termresults. Clin Orthop 1993;292:210-4.
37. Dall DM, Learmonth ID, Solomon M, et al.Charnley hips followed for 3-17 years. ActaOrthop Scand 1993;64:252-6.
38 Schulte KR, Callaghan JJ, Kelley SS, et al. THeoutcome of Charnley hip arthroplasty withcement after a minimum 20 year follow-up.The results of one surgeon. J Bone Joint Surg1993;75:961-75.
39. Skeie S, Lende S, Sjoberg EJ, et al. Survival ofthe Charnley hip in coxarthrosis. A 10-15 yearfollow-up of 629 cases. Acta Orthop Scand1991;62:98-101.
40. Thomas AMC, McMinn DJW. Techniques forthe enhancement of the bone cementinterface in joint replacement. J Jpn OrthopAssoc 1991;65:S381.
41. Charnley J. Low Friction Arthroplasty of theHip: Theory and Practice. Springer-Verlag,Berlin 1979:20-5.
42. Stauffer RN. A ten year follow-up study oftotal hip replacement: with particularreference to roentgenographic loosening ofthe components. J Bone Joint Surg1982;64A:983-90.
43. Johnsson R, Thorngren KG, Persson BM.Revision of total hip replacement for primaryosteoarthritis. J Bone Joint Surg 1988;70B :56-62.
44. Carter SR, Pynsent PB, McMinn DWJ. Greaterthan ten year survivorship of Charnley lowfriction arthroplasty. J Bone Joint Surg1991;73:71.
45. Garcia-Cimbrelo E, Munera L. Early and lateloosening of the acetabular cup after low-friction arthroplasty. J Bone Joint Surg1992;74A:1119-29.
46. Wejkner B, Stenport J. Charnley total hiparthroplasty : a ten to 14-year follow-up study.Clin Orthop 1988;231:113-9.
47. Eftekhar NS. Long term results of cementedtotal hip arthroplasty. Clin Orthop1987;225:207-17.
48. Kavanagh BF, Dewitz MA, Ilstrup DM, et al.Charnley total hip replacement with cement:fifteen year results. J Bone Joint Surg1989;71A:1496-503.
49. Ianotti JP, Balderston RA, Booth RE, et al.Aseptic loosening after total hip arthroplasty.Incidence, clinical significance, and etiology. JArthroplasty 1986;1:99-107.
50. Carlsson AS, Gentz GF, Sanzen L. Socketloosening after hip arthroplasty radiographobservations in 241 cases up to 15 years. ActaOrthop Belg 1986;57:97-100.
51. August AC, Aldam CH, Pynsent PB. TheMcKee-Farrar hip arthroplasty: a long-termstudy. J Bone Joint Surg 1986;68:520-7.
52. Jantsch S, Schwagerl W, Zenz P, et al. Long-term results after implantation of McKee-Farrar total hip prostheses. Arch OrthopTrauma Surg 1991;110:230-7.
53. Bryant MJ, Mollan RAB, Nixon JR. Survivorshipanalysis of the ring hip arthroplasty. JArthroplasty 1991;6(suppl):S5-S10.
54. Marston RA, Cobb AG, Bentley G. Stanmorecompared with Charnley total hipreplacement: a prospective study of 413arthroplasties. J Bone Joint Surg 1996;78-B:178-84.
55. Engh CA, Glassman AH, Suthers KE. The casefor porous-coated hip implants: The femoralside. Clin Orthop 1990;261:63-81.
56. Hauser R, Jacob HAC, Kern S, et al. The“Balgrist” hip socket.A four to ten yearsurvivorship analyis of cementless acetabularcomponents in total hip replacement.Z Orthop Ihre Grenzgeb 1993;131:585-93.
57. Scmitt D, Bigard O, Bresler F, et al. The resultswith two types of uncemented acetabularcups in total hip replacement. Int Orthop1993;17:357-64.
58. Soballe K, Overgaard S. The current status ofhydroxyapatite coating of prostheses. J BoneJoint Surg Br 1996;78-B:689-91.
59. Godsiff SP, Emery RJH, Heywood-WaddingtonMB, et al. Cemented versus uncementedfemoral components in the ring hip prosthesis.J Bone Joint Surg 1992;74:822-4.
60. Wykman A, Olsson E, Axdorph G, et al. Totalhip arthroplasty: A comparison betweencemented and press-fit noncemented fixation.J Arthroplasty 1991;6:19-29.
61. Olsson E, Goldie I, Wykman A. Total hipreplacement. A comparison between cemented(Charnley) and non-cemented (HP Garches)fixation by clinical assessment and objectivegait analysis. Scand J Rehabil Med 1985:107-16.
62. Onsten I, Carlsson AS. Cemeneted versusuncemented socket in hip arthroplasty. ActaOrthop Scand 1994;65:517-521.
63. Rorabeck CH, Bourne RB, Mulliken BD, NayakN, Laupacis A, Tugwell P. The Nicholas AndryAward: comparative results of cemented andcemenetless total hip arthroplasty.ClinOrthopaedics Related Research:1996;325:330-44.
64. Havelin LI, Espehaug B, Vollset SE, EngesaeterLB. Early aseptic loosening of uncementedfemoral componenets in primary total hipreplacemenet, A review based on theNorwegian arthroplasty register. J Bone JointSurg Br 1995;77-B:11-7.
65. Marti RK, Schuller HM, Besselaar PP, VanfrankHaasnoot EL. Results of revision of hiparthroplasty with cement. J Bone Joint Surg1990:346-54.
66. Pellicci PM, Wilson PD, Sledge CB, et al.Revision total hip arthroplasty. Clin Orthop1982;170:8-20.
67. Luft HS, Bunker JP, Enthoven AC. Shouldoperations be regionalised? The empiricalrelationship between surgical volume andmortality. NEJM 1979;301:1364-1369.
68. Burns LR, Wholey DR. The effects of patient,hospital, and physician characteristics onlength of stay and mortality. Medical Care1991;29:251-271.
69. Farley DE, Ozminkowski RJ. Volume-outcomerelationships and inhospital mortality: Theeffect of changes in volume over time. MedicalCare 1992;30:77-94.
70. Hughes RG, Hunt SS, Luf HS. Effect of surgeonvolume and hospital volume on quality ofcare in hospitals. 1987:339-358.
71. Riley G, Lubitz J. Outcomes of surgery amongthe Medicare aged: surgical volume andmortality. Health Care Financing Review1985;7:37-47.
72. Maerki SC, Luft HS, Hunt SS. Selectingcategories of patients for regionalization.Medical Care 1986;24:148-158.
73. Benjamin G. Three essays on volume,complications and hospital resource use: thecase of knee replacement surgery [PhD]:Indiana University, 1995. 114 p.
74. Fowles J, Bunker JP, Schurman DJ. Hip surgerydata yield quality indicators. Business andHealth 1987;June:44-46.
75. Lavernia CJ, Guzman JF. Relationship ofsurgical volume to short-term mortality,morbidity and hospital charges inarthroplasty. J Arthroplasty 1995;10:133-140.
76. Williams A. Economics of coronary arterybypass grafting. BMJ 1985;291:326-9.
77. May PC. Costs per case or costs per Quality-Adjusted-Life-Year? How do we assess valuefor money. In: Wallace WA, ed. JointReplacement in the 1990s. Clinical Studies,Financial Implications and MarketingApproaches. 1st ed. Bury St Edmunds:Mechanical Engineering Publications Ltd,1992:15-9.
78. James M, St Leger S, Rowsell K. Prioritisingelective care: a cost utility analysis oforthopaedics in the north west of England. JEpidem Community Health 1996;50:182-189.
79. Chang RW, Pellissier JM, Hazen GB. A cost-effectiveness analysis of total hip arthroplastyfor osteoarthritis of the hip. JAMA1996;275:858-865.
80. Zuckerman JD, Kummer FJ, Frankel VH. Theeffectiveness of a hospital based strategy toreduce the cost of total joint implants. J BoneJoint Surg 1994;76A:807-11.
81. Healy WL, Kirven FM, Iorio R, Patch DA,Pfeifer BA. Implant standardisation for totalhip arthroplasty. J Arthroplasty 1995;10:177-83.
82. Newman KJH. Total hip and kneereplacements: A survey of 261 hospitals inEngland. J R Soc Med 1993;86:527-9.
83. Hashemi-Nejad A, Goddard N, Birch NC.Current attitudes to cemeneting techniques inBritish hip surgery.Ann R Coll Surg Engl1994;76:396-400
84. Pynsent PB, Carter SR, Bulstrode CJK. Thetotal cost of hip-joint replacement; a model forpurchasers. J Public Health Med 1996;18:157-168.
85. Sheldon TA, Faulkner A. Vetting newtechnologies BMJ 1996;313:508.
Total hip replacement EFFECTIVE HEALTH CARE 11OCTOBER 1996

12 EFFECTIVE HEALTH CARE Total hip replacement OCTOBER 1996
The Research Team:
This bulletin is based on a reviewcommissioned from theDepartment of Social Medicine,University of Bristol.
Writing of the bulletin and additionalresearch by the Effective Health Careresearch team:NHS Centre for Reviews andDissemination, University of York
■ Professor Trevor Sheldon, JointManager of Effective Health Care
■ Alison Eastwood
■ Dr Amanda Sowden
■ Frances Sharp
Members of the Steering Group:■ Dr Peter Bourdillon, Head of Specialist
Clinical Services Division, NHSExecutive
■ Dr Jenny Carpenter, Health CareDirectorate Public Health, NHSExecutive
■ Ian Donnachie, Chief Executive,Bradford Health Authority
■ Professor Mike Drummond, Centre forHealth Economics, University of York
■ Jane Emminson, Chief Executive,Wolverhampton Health Executive
■ Mr Philip Hewitson, Leeds FHSA/NHSExecutive
■ Dr Anthony Hopkins, Director ofResearch Unit, RCP
■ Dr Liz Kernohan, Deputy Director ofPublic Health, Bradford HealthAuthority
■ Andrew Long, Joint Manager ofEffective Health Care, NuffieldInstitute for Health, University ofLeeds
■ Dr Diana McInnes, Principal MedicalOfficer, DoH
■ Dr Tom Mann, Head of Division,Health Care Directorate Public Health,NHS Executive
Acknowledgements:Effective Health Care would like toacknowledge the helpful assistance of thefollowing, who commented on earlierdrafts of the bulletin:
■ Annie Britton, London School ofHygiene and Tropical Medicine,London
■ Mr Christopher Bulstrode, NuffieldOrthopaedic Centre, Oxford
■ Professor Peter Croft, NorthStaffordshire Medical Institute
■ Dr Ray Fitzpatrick, Nuffield College,Oxford
■ Mr Michael Freeman, Harley Street,London
■ Professor P.J. Gregg, Glenfield Hospital,Leicester
■ Dr Rajan Madhok, Gateshead andSouth Tyneside Health Authority
■ Mr David Murray, NuffieldOrthopaedic Centre, Oxford
We gratefully acknowledge thecontribution of staff in the StatisticsDivision (SD2A) of the Department ofHealth who provided data for thisbulletin.
Subscriptions and enquiries:
Effective Health Care bulletins are published in association with Churchill Livingstone. The Department of Health funds alimited number of these bulletins for distribution to decision makers. Subscriptions are available to ensure receipt of a personalcopy. 1996 subscription rates, including postage, for bulletins in Vol. 2 (8 issues) are: £40/$60 for individuals, £65/$97 forinstitutions. Individual copies of bulletins from Vol. 2 are available priced £9.50/$15. Discounts are available for bulk ordersfrom groups within the NHS in the UK and to other groups at the publishers discretion.
In addition, paying subscribers to the new series are entitled to purchase a complete set of the bulletins from the first series,Vol. 1 (Nos. 1-9) for £25, including a binder. Individual back issues from Vol. 1 are available at £5/$8.
Please address all orders and enquiries regarding subscriptions and individual copies to Subscriptions Department, PearsonProfessional, PO Box 77, Fourth Avenue, Harlow CM19 5BQ (Tel: +44 (0) 1279 623924, Fax: +44 (0) 1279 639609). Chequesshould be made payable to Pearson Professional Ltd. Claims for issues not received should be made within three months ofpublication of the issue.
Enquiries concerning the content of this bulletin should be addressed to NHS Centre for Reviews and Dissemination, Universityof York, York YO1 5DD; Fax (01904) 433661 email [email protected]
Copyright NHS Centre for Reviews and Dissemination and Nuffield Institute for Health, 1995. NHS organisations in the UK are encouraged toreproduce sections of the bulletin for their own purposes subject to prior permission from the copyright holder. Apart from fair dealing for the purposes ofresearch or private study, or criticism or review, as permitted under the Copyright, Designs and Patents Act, 1988, this publication may only be produced, storedor transmitted, in any form or by any means, with the prior written permission of the copyright holders (NHS Centre for Reviews and Dissemination, University ofYork, York YO1 5DD).
The NHS Centre for Reviews and Dissemination is funded by the NHS Executive and the Health Departments of Scotland, Wales and Northern Ireland; acontribution to the Centre is also made by the University of York. The views expressed in this publication are those of the authors and not necessarily those ofthe NHS Executive or the Health Departments of Scotland, Wales or Northern Ireland.
Printed and bound in Great Britain by Bell and Bain Ltd, Glasgow. Printed on acid-free paper. ISSN: 0965-0288
Effective Health Care BulletinsVol. 11. Screening for osteoporosis to prevent
fractures2. Stroke rehabilitation3. The management of subfertility4. The treatment of persistent glue ear in
children5. The treatment of depression in primary
care6. Cholesterol: screening and treatment7. Brief interventions and alcohol use
8. Implementing clinical practice guidelines9. The management of menorrhagia
Vol. 21. The prevention and treatment of
pressure sores2. Benign prostatic hyperplasia3. Management of cataract4. Preventing falls and subsequent injury in
older people5. Preventing unintentional injuries in
children and young adolescents6. The management of breast cancer
The Effective Health Care bulletins arebased on a systematic review andsynthesis of research on the clinicaleffectiveness, cost-effectiveness andacceptabi l ity of heal th serviceinterventions. This is carried out by aresearch team us ing establ ishedmethodological guidel ines, withadvice from expert consultants foreach topic. Great care is taken toensure tha t the work, and theconclusions reached, fair ly andaccurately summarise the researchfindings. The University of York andthe University of Leeds accept noresponsibility for any consequentdamage aris ing from the use ofEffective Health Care.