toxic goiter pearls
DESCRIPTION
A word document for toxic goiter questions and answer.TRANSCRIPT

Case Capsule A 30-year-old female patient with a thin build has presented with diffuse enlargement of the thyroid and palpitation of 6 months duration. She complains of increased appetite and loss of weight. She is apparently irritable and says, she is intolerant to hot weather with excessive sweating. She has a preference for cold weather. She also complains of insomnia and loss of concentration ability. She has diarrhea in addition. She is married and has a baby of 6 months old. She complains of amenorrhea for the last 3 months. On examination, patient is agitated and nervous. Examination of the palms revealed that they are moist and sweaty. She has tachycardia, fine and fast tremor and protruded eyeballs. There is visible diffuse enlargement of the thyroid. On auscultation, there is a systolic bruit heard in the upper pole of the thyroid. The carotids are felt in the normal position. The trachea is central. There is no evidence of retrosternal extension. The cervical lymph nodes are not enlarged.
In all goiters or swelling in the neck assess the following: 1. What is the anatomical diagnosis—by assessing the plane—deep to the deep fascia and deep to the
sternomastoid? 2. What is the pathological diagnosis, e.g. nodular goiter, solitary thyroid nodule, carcinoma, etc. 3. What is the functional diagnosis—whether the patient is euthyroid, hyperthyroid, hypothyroid?
Toxic Goiter
Checklist for history1. Onset related to puberty, pregnancy 2. Residence: Endemic area or not 3. Ingestion of goitrogens 4. Intolerance to hot/cold temperature 5. Increased appetite with loss of weight (Hyperthyroidism) 6. Gain in weight (Hypothyroidism) 7. Change in menstrual cycle 8. Bowel habit—diarrhea (hyper), constipation (hypo) 9. Difficulty in swallowing 10. Difficulty in breathing 11. Hoarseness of voice 12. Postural cough during sleeping (retrosternal extension) 13. History of palpitation/shortness of breath on exertion 14. Insomnia, loss of concentration (hyper) 15. Irritability/nervousness (hyper).
Goitrogens are substances that suppress the function of the thyroid gland by interfering with iodine uptake, which can, as a result, cause goiter.
Toxic Goiter

Checklist for examination of thyroid1. Always check the pulse for tachycardia before examining the thyroid 2. Look for tremor of hands and tongue before examining the thyroid 3. Ask the patient to take a sip of water and to hold it in his/her mouth. Then ask the patient to swallow (goiter moves on swallowing) 4. Ask the patient to put out the tongue (thyroglossal cyst moves up) 5. Stand behind the patient and palpate the thyroid (ask the patient to take another sip of water) 6. Decide whether it is diffuse enlargement, single nodule, multiple nodules and the nature of the surface 7. Decide the consistency 8. Look over the top of the head for exophthalmos (look for lid lag, lid retraction and other eye signs) 9. Check the eye movements, double vision 10. Now stand in front of the patient for palpation of the trachea for deviation, for assessing the lower limit by ‘getting below’ 11. Assess the plane of the swelling (stretch the deep fascia by extending the neck and see whether it becomes less prominent, contract
the sternomastoid muscle against resistance and see whether it becomes less prominent 12. Do Pemberton’s test for retrosternal extension 13. Percuss the manubrium sterni for dullness (seen in retrosternal extension) 14. Palpate the carotids on both sides15. Examine the regional lymph nodes 16. Feel the skin (dry in hypothyroidism, shiny skin in hyperthyroidism) 17. Look for pretibial myxedema (hyperthyroidism) 18. Assess the build of the patient (Thin—hyperthyroidism, obese—hypothyroidism) 19. Examine the palms—warm, moist and changes of acropachy in hyperthyroidism20. Assess the behavior of the patient (agitated in toxic, lethargic in hypothyroidism) 21. Ask the patient to rise from squatting position without using hands for support (proximal myopathy in hyperthyroidism) 22. Test the biceps reflex and look for slow relaxing reflex suggestive of hypothyroidism.
Toxic Goiter

Final checklist for clinical examination of thyroid1. Look for signs of toxicity2. Look for signs of malignancy 3. Look for signs of retrosternal extension4. Look for position of carotid artery 5. Look for position of trachea 6. Look for cervical lymph nodes 7. Look for bony swellings especially in the scalp.
Q 1. Why is the swelling a goiter? The points in favor of goiter are:
1. The plane of the swelling is deep to deep fascia and deep to sternocleidomastoid (the deep fascia of the neck is stretched by extending the neck and sees whether the swelling is becoming less prominent or not, similarly contracts the sternomastoid muscles.
2. The swelling moves up and down with deglutition. 3. It occupies the normal position of thyroid. 4. It is having the shape of thyroid.
Q 2. Why does the thyroid gland move up and down with deglutition?
Toxic Goiter

The inferior constrictor muscle has two parts namely, thyropharyngeus and cricopharyngeus and they are attached respectively to thyroid cartilage and cricoid cartilage.
Therefore, when the patient swallows this muscle will contract and the thyroid and cricoid cartilage will move up.
The thyroid gland is attached to the cricoid by means of the suspensory ligament of Berry that is nothing but a condensation of pretracheal fascia.
Therefore, the thyroid gland will move up and down with deglutition.
Q 3. What is goiter? Any enlargement of thyroid gland is called goiter. Even though for neoplasms we call it malignancy and for
inflammation we call it thyroiditis.
Q 4. Can the normal thyroid be felt on palpation? In a reasonably slender person it can be felt as a smooth firm structure that moves upwards during deglutition.
Q 5. How do you grade a goiter?WHO grading (1994) of goiter
Grade 0:
No palpable/visible goiter
Grade 1:
A thyroid that is palpable but not visible when the neck is in normal position
Grade 2 An enlarged thyroid that is visible with the neck in normal position.
Toxic Goiter
:Q 6. What are the signs of retrosternal extension?
1. Cannot ‘get below’ the swelling. 2. Pemberton’s test positive (arm raising test)— when both arms are elevated so as to touch the sides of the
face, after a few moments there will be congestion of face, some cyanosis and distress. This is due to the narrowing of the thoracic inlet and when the arms are elevated this results in obstruction of great veins of the neck.
3. On percussion over the manubrium sterni there will be dullness (normally this is resonant). 4. Radiological assessment.
Q 7. How will you assess the position of trachea? The position of trachea can be assessed by:
1. Palpation of trachea by three finger test (this will be difficult in case of large goiter). 2. Auscultation to detect the position of trachea. 3. Radiological.
Q 8. In which position you normally palpate a patient with thyroid? The examiner stands behind the patient and will do the palpation.
Q 9. What is Kocher’s test? Slight compression on the lateral lobes of thyroid produces stridor.
Toxic Goiter

If this test is positive it signifies that the patient has an obstructed trachea.Q 10. What are the conditions in which you get narrowing of the trachea?
Narrowing of trachea is found in: 1. Carcinoma of the thyroid 2. Retrosternal goiters3. “Scabbard” trachea of long standing multinodular goiter 4. Riedel’s thyroiditis.
Q 11. What is plunging goiter? In this condition, the whole of the enlarged thyroid lies in the superior mediastinum and there is no
palpable thyroid gland in the neck. When the intrathoracic pressure rises as in coughing, the goiter will be seen in the neck, this is called plunging goiter.
Q 12. What is Berry’s sign? In goiter, the carotid artery may be pushed posteriorly by the enlarging thyroid and this is called
displacement. When there is infiltration of the carotid by tumor the carotid pulse on that side will be absent. This absent
carotid pulse is called Berry’s sign.
Toxic Goiter

Q 13. What are the signs of malignancy in a goiter?Signs of malignancy in a goiter
1. Rapidly enlarging thyroid2. Hard consistency (unripe apple) 3. Fixity of the thyroid (the lateral mobility becomes restricted before there is noticeable movement on
deglutition)4. Regional lymph nodes (the first lymph node to be involved in carcinoma is called Delphic lymph node
which is nothing but prelaryngeal lymph node). This is also called the Delphian lymph node 5. Berry’s sign (absent carotid pulse) 6. Horner’s syndrome 7. Hoarseness of voice 8. Stridor due to tracheal obstruction 9. Distant metastases (pulsatile, bony swelling from the scalp).
Q 14. Where will you auscultate for thyroid bruit? The usual position to look for thyroid bruit is at the upper pole where the superior thyroid artery enters the
thyroid gland.
Toxic Goiter

Q 15. What are your points in favor of toxicity in this patient? Symptoms of toxic ity
System SymptomsNervous system Nervousness agitation, irritability, insomnia, nervous instability, tremor of the hands and tongueCardiovascular system Palpitation, dyspnea on system exertion, chest pain, etc…Metabolic and alimentary system Increase in appetite and loss of weight,
change in bowel habit, usually diarrhea; preference for cold weather; excessive sweating; intolerance to hot weather
Menstrual changes Usually amenorrhea or oligo- menorrheaMusculoskeletal Generalized weight loss;
wasting and weakness of small muscles of the hand, shoulder and face.Skin Pretibial myxedemaNail Onycholysis—Plummer’s nail.
Signs of toxic ity1. Uniform, smooth, soft or firm enlargement of thyroid in Graves’ disease (primary) bosselated swelling or solitary nodule in case of secondary 2. The gland is vascular as evidenced by bruit 3. Tremor of the outstretched hands (fine, fast) and tongue 4. Warm and moist hands 5. Tachycardia 6. Extra systoles, atrial fibrillation, and cardiac failure 7. Eye signs 8. Myopathy — weakness of the proximal limb muscle is commonly found. Severe muscular weakness resembling myasthenia gravis occurs
occasionally. Inability to get up from chair is called Plummer’s sign.
Toxic Goiter

Q 16. What are the eye signs of thyrotoxicosis?Eye signs
1. Lid retraction This sign is caused by over activity of involuntary smooth muscle part of the levator palpebrae superior is muscle. If the upper eye lid is higher than normal and the lower lid is in correct position, the patient has lid retraction (this is not exophthalmos)
2. Lid lag (Von Graefe’s sign)
when the upper lid does not keep pace with the eyeball as it follows a finger moving from above downwards, it is lid lag
3. Exophthalmos Here both the eyelids are moved away from center with sclera visible below or all around. Here the eyeball is pushed forwards by increase in retro-orbital fat, edema, and cellular infiltration (sclera should be always visible below the lower edge of eyes in exophthalmos)
4. The other eye signs are:
a. Stellwag’s sign : widening of the palpebral fissure this is due to lid retractionb. Joffroy’s sign —absence of wrinkling of the forehead when the head is bent downc. Möbius’s sign —difficulty in convergence when the patient is asked to look at near
objects5. Severe exophthalmos
Intraorbital edema is super added to the increased deposition of intraorbital fat. It comprises of: a. Intraorbital congestion—watering of eyes, dilated blood vessels in lateral conjunctivab. Increased intraocular tension c. Muscle paralysis (Ophthalmoplegia)—evidenced by double vision, especially when eye is
moved upward end and outwards (muscles of elevation and abduction namely, superior rectus and inferior oblique muscles are affected)
d. Chemosis.
Toxic Goiter

Q 17. What is pretibial myxedema? This is a misnomer and it is seen in primary toxicosis (In Graves’ disease with exophthalmos only). It is usually symmetrical. The earliest stage is a shiny red plaque of thickened skin with coarse hair, which may be cyanotic
when cold. In severe cases the skin of the whole leg below knee is involved, together with that of foot and the
ankle and there may be clubbing of the fingers and toes (Thyroid acropachy).
Q 18. What are the three most important clinical types of toxicity?
Clinical types of thyrotoxicosis1. Primary thyrotoxicosis/Graves/diffuse toxic goiter 2. Secondary thyrotoxicosis/Plummer’s disease/toxic nodular goiter 3. Toxic nodule/adenoma/autonomous nodule.
Q 19. What is the difference between thyro- toxicosis and hyperthyroidism?
Toxic Goiter

Thyrotoxicosis refers to the biochemical and physiological manifestations of excessive thyroid hormone. Hyperthyroidism is a term reserved for disorders that result in the over production of hormone by the
thyroid gland. Thyrotoxicosis need not be due to hyperthyroidism. In short in hyperthyroidism the pathology is in the thyroid gland itself. The causes for hyperthyroidism and toxicosis without hyperthyroidism are shown below:
Causes for hyperthyroidism and toxicosis without hyperthyroidismHyperthyroidism Toxicosis without hyperthyroidism
1. Graves’s disease 1. Subacute thyroiditis*2. Toxic nodular 2. Ectopic functioning thyroid goiter tissue3. Toxic adenoma 3. Silent thyroiditis4. Jod-Basedow’s 4. Struma ovarii disease
5. Metastatic follicular carcinoma (functioning) 6. Trophoblastic tumors7. Postpartum thyroiditis 8. Thyrotoxicosis factitia
*Note: In thyroiditis, inflammation of thyroid causes release of already formed thyroid hormones into the circulation, resulting in toxicosis. In other conditions such as struma ovarii, trophoblastic tumors, etc., there is extrathyroid production of thyroxin from these tissues.
Toxic Goiter

Q 20. What is Graves’ disease? The essential components of Graves’ disease are:
1. Diffuse goiter2. Thyrotoxicosis 3. Autoimmune manifestations like:
a. Infiltrative ophthalmopathyb. Dermatopathy c. Myopathy.
Q 21. What is the essential etiology of Graves’ disease? Graves’ disease is an autoimmune disorder caused by thyroid stimulating immunoglobulins (TSIs) that have been
produced against an antigen in the thyroid. This is directed to the thyroid stimulating hormone receptors (TSHR - Ab). This acts like TSH agonist. TSH-Ab is found only in Graves’ disease.Q 22. What are the precipitating factors for primary thyrotoxicosis? Remember 3 - S
1. Sex (puberty, pregnancy) 2. Sepsis3. Psyche (sudden emotional upset).
Toxic Goiter

Q 23. What are the differences between primary thyrotoxicosis and secondary thyrotoxicosis?
Differences between primary thyrotoxicosis and secondary thyrotoxicosisPrimary Secondary
Etiology Autoimmune Not autoimmune
Onset Abrupt Insidious
Age Usually younger women Usually middle aged or elderly
Due to It is due to abnormal thyroid stimulating antibodies (TSAb)
No such antibodies (it is due to over activity of nodules)
Pathology No pre-existing goiter Pre-existing nodular goiter for a long durationEnlargement of goiter is diffuse, firm or soft Bosselated or nodular not uniformThe entire gland is overactive Internodular thyroid tissue is overactive, rarely one or more nodules
also may be overactiveHyperthyroidism is usually severe Hyperthyroidism usually mild
Manifestations Manifestations not due to hyperthyroidism; pretibial myxedema may occur
Not seen
Presence of bruit Bruit need not be presentCardiac failure is rare Cardiac failure or multiple extrasystole, paroxysmal atrial tachycardia,
paroxysmal atrial fibrillation, or persistent atrial fibrillationEye signs common Except lid lag and retraction other eye signs are not seen
Treatment Can be managed by, drugs, radioiodine, and surgery
Surgery is the treatment of choice after control of the toxicity
Toxic Goiter

Q 24. How will you confirm your diagnosis of toxicity? Confirmation by:
A. Thyroid Function Test – T3, T4 and TSH (Immunochemiluminometric assay is the current method). Free T3, T4 are more significant and meaningful. The T3 and T4 are raised and TSH is lowered in hyperthyroidism. Normal values are total:
Free T3 3.5 – 7.5 mol/L Free T4 10 – 30 nmol/L TSH 0.3 – 3.3 mU/L
Note: The total T3 and T4 hormone level will vary depending upon the amount of thyroid binding globulin (TBG).
Q 25. What are the other investigations required? A. Antithyroglobulin antibody: More than 1:100. B. Thyroid peroxidase (TPO): > 25 units (TPO and TSH antibodies are increased in autoimmune thyroiditis). C. TSH receptor antibodies are difficult to estimate. D. Radioisotope scintigraphy (radionuclide scan).
Q 26. What is the role of isotope scanning in thyroid?
Toxic Goiter

The only absolute indication in thyrotoxicosis for isotope scanning is for the diagnosis of Autonomous Toxic Nodules.
Toxicity with nodularity is an indication. It can identify hypofunctioning nodule (cold). Cold nodule in Graves’ is likely to be malignant.
It is the only method by which one can definitely differentiate primary, secondary and toxic nodules. Isotope scan can also differentiate hyper- thyroidism from toxicosis due to other causes. (To
differentiate hyperthyroid thyrotoxicosis from non-hyperthyroid thyrotoxicosis). The radioactive iodine uptake (RAIU) is increased in hyperthyroidism whereas toxicosis because of extrathyroidal causes the RAIU is decreased (e.g. thyroiditis).
Other indications for isotope scan are: To identify ectopic thyroid tissue. To identify recurrence and metastases in thyroid carcinoma.
Q 27. What is the isotope of choice for diagnostic scanning of the thyroid? 99mTc is the isotope of choice for diagnostic purposes. It is cheap and the radiation is less than
radioiodine. Twenty minutes after intravenous injection of 99mTc, scanning is done over the thyroid. If radioactive iodine is used, 123I is the isotope of choice for diagnostic purposes.
Q 28. What is the half-life of the various radioisotopes used in thyroid?HALF-LIFE OF THE VARIOUS RADIOISOTOPES
Toxic Goiter

ISOTOPE
Half life Route
Rays Comment
123I 13 hours Oral Gamma rays Will not detect nodules < 1 cm size131I 8 days Oral Gamma and beta rays Too much irradiation if used for diagnostic scanning132I 2.3 hours Oral Gamma and beta rays Not used for clinical purposes99TC 6 hours IV Gamma rays Commonly used for diagnostic scanning of thyroid
Q 29. What is the problem with technetium scanning? Carcinoma concentrates technetium and therefore a hot nodule need not necessarily be benign.
Q 30. What is discordant scan? (اِق ض# #َن (ُم&َت A nodule which is warm on technetium scanning and cold on radioiodine scanning is called discordant scan. This is
suggestive of malignancy.
Q 31. Why technetium is preferred over radio- iodine for diagnostic scanning? It gives small amount of radiation and you get the image within minutes.
Q 32. What will be the appearance in scintigraphy in primary, secondary and toxic nodule? Primary : Uniform diffuse increased uptake.
Toxic Goiter
Secondary : Heterogeneous pattern with some focal areas of enhanced uptake. Toxic nodule: Increaseduptake only in the nodule, with no uptake in the surrounding thyroid tissue.
Q 33. What are the toxic situations where there is decreased uptake of isotope in thyroid gland? Low uptake is seen in:
1. Thyroiditis 2. Postpartum thyrotoxicosis3. Struma ovarii 4. Factitious thyrotoxicosis 5. Jod-Basedow thyrotoxicosis.
Q 34. What are the features of toxic adenoma? Toxic Adenoma
Toxic Goiter

1. These are: Benign, monoclonal thyroid tumors of more than 3 cm size 2. Are autonomous rather than responding to TSH stimulation 3. Eye signs and other stigmata of Graves’ are absent 4. Somatic mutation of TSH receptor gene or G protein gene is present 5. T4 may be normal (hence check T3 levels).
Q 35. What are the conditions in which Thyroid Binding Globulins (TBG) are increased? The concentrations of TBG are increased in pregnancy, liver diseases and where there is hyperestrogenism. The
levels of free T3 and T4 in these conditions are normal despite high TBG.
Q 36. What are the conditions in which the TBG levels are decreased? High androgens, severe hypoproteinemia, chronic liver disease and acromegaly.
Q 37. What is the problem with the measurement of free T3 and T4? The method usually used is radioimmunoassay and it is costly.
Q 38. What is the normal free T3 and T4 value? Free T3—3.5 to 7.5 pmol/L Free T4—10 – 30 nmol/L It is to be noted that 0.3% of the total T3 and 0.03% of the
total T4 are free and physiologically active.
Toxic Goiter

Q 39. What is T3 Thyrotoxicosis? T3 alone is raised and TSH is decreased in this condition.
Q 40. What is subclinical hyperthyroidism? Seen in 1% of hyperthyroids Serum TSH is low but the free T4 is normal Symptoms are absent and hence called ‘sub-clinical’.
Q 41. What is apathetic hyperthyroidism (masked)?Apathetic hyperthyroidism
1. Lack almost all of the clinical manifestations 2. Presents as behavior problems 3. May end up at the psychiatrist’s 4. Thyroid gland is not usually enlarged5. Commonly seen in elderly patients6. Decreased appetite and lethargy7. New onset of atrial fibrillation and increased angina.
Q 42. Is there any role for FNAC in thyrotoxicosis? Yes. Sometimes the thyrotoxicosis may be associated with a papillary carcinoma of the thyroid. It is better to do
after controlling toxicosis because of the increased vascularity of the gland.
Toxic Goiter
Q 43. How you will manage thyrotoxicosis? In primary thyrotoxicosis we have 3 options.
1. Antithyroid drugs 2. Radioiodine therapy 3. Surgery.
Q 44. What will be the choice of therapeutic agent in thyrotoxicosis? We have some broad guidelines. This must be modified according to the facilities available and wishes of the
patient. Age over 25 years :
Radioiodine therapy (when development is complete) Under 25 years :
Surgery for large goiter Antithyroid drugs for the small goiter
Toxic nodular goiter usually will not respond very well to radioiodine and antithyroid drugs. Therefore, surgery is the treatment of choice.
Q 45. What are the drugs available for the treatment?
Drugs available for the treatment of thyrotoxicosis1. Thionamides
Toxic Goiter

a. Carbimazole (Neomercazole) Dose 40 – 60 mg daily for first 3 weeks, 20 – 40 mg daily for 4 – 8 weeks, Maintenance of 5 – 20 mg/daily for 18 – 24 months (each tablet is 5 mg)
b. Propylthiouracil (PTU)c. Methimazole 20 – 30 mg daily (single dose)
2. Beta blockers 3. Potassium per chlorate inhibits iodide transport 4. Lugol’s iodine 5. Iopanoic acid—500 mg bid
Severe cases unresponsive to conventional therapy6. Lithium carbonate – 300 mg 6th hourly 7. Guanethidine 30 – 40 mg oral 6th hourly 8. Reserpine 2.5 – 5 mg IM 4th hourly9. Glucocorticoids: dexamethasone 2 mg oral 6th hourly.
Q 46. What is the dose of Propylthiouracil? About 100 to 300 mg 3 times daily orally initially for 4 to 6 weeks followed by 100 mg 3 times daily.
Q 47. What is the action of Propylthiouracil?
Toxic Goiter

1. PTU blocks conversion of T4 to T3 in periphery (liver) 2. Inhibits iodine organification and coupling of iodotyrosines 3. Immunomodulatory effects that reduces thyroid stimulating antibodies.
Q 48. What are the advantages of PTU? 1. PTU may be given during pregnancy at reduced doses. 2. If thyroidectomy is required in second trimester, the patient can be prepared with PTU.3. Useful for the treatment of thyroid storm (multiple doses needed).
Q 49. What are the adverse effects of PTU?Adverse effects of PTU
1. Hepatotoxicity which is not dose related 2. Mild transaminase elevation in 30% 3. Agranulocytosis4. Minor side effects as seen in carbimazole therapy 5. Antineutrophilic cytoplasmic antibody (ANCA) in 20% especially with long-term treatment.
Q 50. What is the action of carbimazole? Carbimazole acts by the following methods:
1. Blockage of organic binding and oxidation of iodine 2. Immunosuppression (decreases thyroid antigen, prostaglandin and cytokine release)
Toxic Goiter
3. Reduction of thyroid autoantibody titers.
Q 51. What are the side effects of carbimazole?Side effects of Carbimazole
1. Fever, rash, urticarial and arthralgia (minor side effects) 2. Liver dysfunction3. Neuritis4. Myalgia 5. Lymphadenopathy6. Psychosis7. Occasional agranulocytosis (< 1 in 200 cases).
Q 52. What is the clinical manifestation of agranulocytosis? Agranulocytosis presents as sore throat, which warrants immediate cessation of the drug.
Q 53. Can the thyroid be enlarged during medical treatment? Yes. During treatment in 1/3rd to half of the patients, the thyroid will shrink. Enlargement usually occurs because of commencement of hypothyroidism, which should be avoided.
Toxic Goiter

Q 54. What is “block and replacement” regime? The thyroid enlargement because of the development of hypothyroidism during medical treatment is prevented by
supplementing low dose of levothyroxine (0.1 mg) along with the antithyroid drugs.
Q 55. In what percentage of patients is medical treatment effective? Permanent remission is possible only in a small minority of adults and 20% of children.
Q 56. What is the dose of beta blocker? Propranolol is the drug of choice for initial control of adrenergic symptoms.
The dose is 20 – 80mg every 6 – 8 hours orally. 1 – 2mg IV propranolol for thyroid storm.
Q 57. What is the action of propranolol? 1. Peripheral conversion of T4 – T3 is blocked 2. Adrenergic antagonistic action helps to alleviate cardiac symptoms, tremor,
etc.Q 58. Is propranolol indicated in all patients with toxicity?
No; 1. It is given for emergency surgical management of toxicity 2. It is also used for control of the adrenergic symptoms.
Contraindications for propranolol1. Bronchial asthma2. COPD3. Heart block4. CCF.
Toxic Goiter
Q 59. If the patient was prepared using propranolol before thyroid surgery, how long should it be continued postoperatively?
Propranolol should be given over a period of 1 week and preferably tapered over a period of 2 weeks after surgery.
Q 60. What are the drugs inhibiting peripheral conversion of T4-T3?Drugs inhibiting peripheral conversion of T4-T31. Beta blockers 2. PTU 3. Glucocorticoids4. Iopanoic acid.
Q 61. What is the minimum duration of medical treatment required before surgery? Thyroidectomy performed immediately after control of thyrotoxicosis is associated with risk of thyroid crisis and it
is preferable to wait approximately two months until after a patient is euthyroid.Q 62. Is there any role for Dexamethasone in the management of thyrotoxicosis?
It is used for the management of thyrotoxic crisis Dose is 2 mg every 6th hourly (injection) The actions are :
a. Inhibits glandular secretion of hormone
Toxic Goiter

b. Inhibits peripheral conversion of T4 to T3c. Immunosuppression.
Q 63. What is Lugol’s iodine and what is its dose? 5% iodine in 10% potassium iodide is called Lugol’s iodine. The dose is 10 drops in a glass of water 3 times daily for 10 days.
Q 64. What are the actions of Lugol’s iodine? 1. Decreases the vascularity of the gland 2. Makes the thyroid firm and less friable (helps in surgical removal) 3. Prevents the release of hormone from the gland (thyroid constipation).
Q 65. What will happen if Lugol’s iodine is given for more than 10 days? After 2 weeks the effect of Lugol’s iodine therapy is lost due to the so called thyroid escape from iodine control.
Q 66. What are the indications for radioiodine therapy? Radioiodine (131I) is usually given to patients above 45 years for primary thyrotoxicosis. Isotope facility must be available.
Q 67. What are the problems of radioiodine therapy? Problems of radioiodine therapy
Toxic Goiter

1. Indefinite follow-up is essential as the patient may develop hypothyroidism (75%)2. Chance of permanent thyroid failure – 90% (hypo is more because of failure of cellular reproduction)3. Theoretical possibility of genetic damage, leukemia, damage to fetus and carcinoma (no convincing
evidence)4. Takes 2 – 3 months for control of symptoms5. Worsening of ophthalmopathy (especially in smokers) and dermatopathy6. Mild anterior neck pain7. Increased risk of benign tumors8. Malignant transformation in young patients 9. May induced hyperparathyroidism.
Q 68. What are the contraindications of radioiodine therapy?CONTRAINDICATIONS OF RADIOIODINE THERAPY1. PREGNANCY 2. LACTATING MOTHERS3. WOMEN DESIRING PREGNANCY WITHIN 1 YEAR4. CHILDREN/ADOLESCENTS (RELATIVE).
Q 69. What is the dose of radioiodine? 300 to 600 MBq, if there is no clinical improvement after 12 weeks further dose is given. Two or more doses are necessary in 20 to 30% of cases.
Q 70. What is the method of radioiodine treatment for toxicity?
Toxic Goiter

1. Make the patient euthyroid with drugs2. Discontinue drugs for 5 days 3. Administer 131I 300–600 MBq (5–10 mCi) 4. Start antithyroid drugs after 1 week and continue for 6 to 8 weeks 5. After 12 weeks, if there is no improvement, give another dose of radioiodine 6. Two or more doses of radioiodine may be required.
Q 71. What are the indications for surgery in thyrotoxicosis?
Indications for surgery in thyrotoxicosis1. Intolerance or non-compliance with antithyroid drugs 2. Contraindications to radioiodine therapy
Toxic Goiter

3. Graves’ disease in children, adolescentsand those who are under the age of 25 years 4. In women who are potential mothers 5. Large goiter 6. Persistent thyromegaly7. If antithyroid medication is required for more than 2 years 8. Graves’ with nodules 9. Ophthalmopathy 10. Pressure symptoms 11. Toxic MNG 12. Substernal goiter 13. Amiodarone induced thyrotoxicosis.
Q 72. What are the drugs used for preparation of a patient for “urgent thyroidectomy”? Combination of oral iopanoic acid 500 mg bid and dexamethasone 1 mg bid and PTU or MMI and beta blockers
for 5 to 7 days.Q 73. What are the advantages of surgery?
Advantages of surgery1. Surgery is effective in achieving euthyroid status in 95–97% of patients2. Controls hyperthyroidism immediately3. Hazards associated with radioiodine therapy are avoided4. Surgery will provide tissue for histology
Toxic Goiter

5. Surgery will remove occult foci of malignancy 6. Childbearing is immediately possible 7. Coexisting parathyroid carcinoma can be removed 8. Is a better treatment for toxicity with ophthalmopathy 9. No need for follow up because nodules are not left behind.
Q 74. What is the surgical treatment of primary thyrotoxicosis? Near total thyroidectomy is now recommended as the treatment of choice.
Q 75. What is the recommended treatment for secondary thyrotoxicosis? Surgery is preferred over radioiodine for secondary thyrotoxicosis because:
1. It will not respond to radioiodine as most of the nodules may not take up radioiodine.2. Large and repeated doses of radioiodine may be required.
Q 76. What is the recommended treatment of toxic nodule? Once the patient is made euthyroid, surgery in the form of Hemithyroidectomy will give permanent relief.
Q 77. & Q 78. What are the types of thyroid surgeries?Types of Thyroid Surgeries
Operation Part of thyroid removed IndicationsI. Lobectomy Removal of one lobe of thyroid Solitary thyroid nodule
II. Hemithyroidectomy Removal of one lobe and isthmus STN Toxic nodule
Toxic Goiter

Follicular neoplasmIII. Bilateral subtotal
thyroidectomy2 g of thyroid remnant is kept on both sides and the rest of the thyroid gland is removed
Toxic goiter Toxic nodular goiter Multi nodular goiter (Near total is the preferred treatment for these conditions now)
IV. Hartley-Dunhill procedure Total lobectomy and isthmectomy on the affected side and 4 g remnant left on the contralateral side
Toxic goiter
V. Near total thyroidectomy 1 to 2 g remnant is left on the contralateral side of the lesion and the rest of the thyroid is removed
Toxic goiter MNG Papillary carcinoma Follicular carcinoma Medullary carcinoma, etc.
VI. Total thyroidectomy isthmusectomy/ isthmectomy
Entire gland is removed Removal of isthmus alone
Thyroid malignancy Emergency decompression of
trachea for anaplastic carcinoma Biopsy for anaplastic carcinoma
Q 79. What is the management of intrathoracic goiter with toxicity? Antithyroid drugs will increase the size of the retrosternal and intrathoracic goiter and therefore dosage should be
carefully adjusted. Surgery is the treatment of choice for intrathoracic goiter with toxicity.
Q 80. What is the management of intrathoracic toxic goiter in pregnancy?
Toxic Goiter

Antithyroid drugs are given in small doses in first trimester to prevent fetal goiter and airway obstruction Antithyroid drugs may be combined with propranolol and surgery is done in the second trimester.
Q 81. What is the treatment for recurrent toxicity? Radioiodine/medical treatment.
Q 82. What are the preoperative preparations for thyroid surgery?
Preoperative preparations for thyroid surgery1. Thyroidectomy is done only after making the patient euthyroid2. Lugol’s iodine is given for a period of 10 days for reducing the vascularity and making the gland firm (for
toxic cases only)
Toxic Goiter

3. Always send the patient for preoperative indirect laryngoscopy (or video laryngoscopy) to rule out occult vocal cord palsy and document for medicolegal purposes
4. Arrange cross matched blood for vascular thyroids 5. Assessment of the cardiac status by ECG6. Assessment of the chest by an X-ray chest and X-ray neck AP view (for detecting tracheal displacement)
and lateral view (for detecting luminal narrowing).o X-ray neck will also reveal soft tissue shadows and calcifications. o X-ray chest may reveal the presence of retrosternal extension
7. Rule out hypertension and diabetes mellitus
Q 83. What are the preliminary steps of thyroid surgery? Surgery is done under general anesthesia using endotracheal intubation (preoperative X-ray neck to rule
out displacement of the trachea and luminal narrowing). Position of the patient: Supine with sand bag behind the shoulders and head ring for adequate neck
extension. Skin is painted with antiseptics and proper draping with sterile towels and head cover.
Toxic Goiter

Kocher’s collar incision is used for incising the skin (1 to 2 cm above the manubrium sternum). Incision is deepened up to the deep fascia by incising the platysma.
Anterior jugular veins seen on the surface of the investing layer, may be ligated (communicating vein seen connecting the two anterior jugulars requires ligation).
Investing layer is opened vertically in the midline. The strap muscles are retracted laterally (in big thyroids, they may be divided either on one side or
bilaterally in the upper part to save the Ansa hypoglossi nerves entering the strap muscles in the lower part)
The Pretracheal fascia is incised vertically and the thyroid gland is mobilized by ligating the middle thyroid vein (this is the first vessel to be ligated).
E s s e n t i a l s t e p s o f t h y r o i d e c t o m y
Identification of parathyroid glands Identification of the recurrent laryngeal nerve Ligation of vessels Removal of the glandIdentify the parathyroids before ligating the vessels.
It is preferable to identify the entire course of the nerve in thyroid surgery
The branches of the superior thyroid vessels are individually skeletonized and ligated as close to the superior pole as possible after identifying the external branch of the superior laryngeal nerve
The gland is now free for removal.Depending on the type of surgery, the extent of removal and the amount of remainder may be decided
Parathyroids have the color of peanut butter, each of 6 × 3 × 3 mm size and less than 40 mg weight.
There is no role for the old axiom “nerve seen is nerve injured”, which is called the ‘ostrich philosophy’
A medial approach to the superior pole via the avascular space between the cricothyroid muscle and the upper pole of the gland is ideal
Beware of the suspensory ligament of Berry, which is the last attachment of the gland to the cricoid cartilage
The recurrent laryngeal nerve (RLN)— Inferior thyroid The first identification is at the so-called Riddle’s “Mass Ligation” of the superior pole is to be avoided The RLN may pass through the
Toxic Goiter

artery junction is critical in identifying the parathyroids (this is a critical area of RLN injury as well).
triangle, which is bound by inferior thyroid artery above, the carotid artery laterally and the trachea medially
substance, superficial or deep to the Berry’s ligament
The superior parathyroid glands are above and behind this junction.
From there, the nerve is traced upwards to the point of its entry into the larynx at the greater cornu of the thyroid cartilage.
Capsular ligation of the inferior thyroid artery:a. Inferior thyroid artery is an end artery to the
parathyroids and hence ligation of the trunk of the inferior thyroid artery is not recommended.
b. The small branches entering the capsule of the gland alone are ligated, thereby preserving the blood supply to the parathyroids.
c. These small branches are therefore situated between the parathyroid and the thyroid gland
Take care of the nerve before the final removal of the gland
The inferior parathyroid glands are below and anterior to this junction having variable positions. The inferior glands may be situated on the inferior pole of the thyroid, thyrothymic ligament, in the thymus or in the perithymic fat
Before entry, the nerve may divide into two or more extralaryngeal branches
Finally, the lower pole veins are ligated. Blind “mass ligation” of the lower pole may injure the RLN in this situation
When there is difficulty in identifying the RLN, the entry point of the nerve can be located by identifying Zuckerkandl’s tubercleThe nerve may cross the inferior
thyroid artery usually deep to the artery, sometimes superficial or may even pass through the fork of the branches of the artery
Q 85. What are the critical areas of recurrent laryngeal nerve injury?
There are 3 critical areas of RLN injury: 1. At the site of where the inferior thyroid artery crosses
the RLN.2. At the region of the suspensory ligament of Berry. 3. At the lower pole of the gland during ‘mass ligation’ of
the vessels of the inferior pole, especially on the right side (Fig. 1.6).
Toxic Goiter

Q 86. What is Zuckerkandl’s tubercle? It is the posterior extension of the lateral lobes of the thyroid gland near the ligament of Berry. It is found in 14–55% of cases. The RLN runs cranially in a fissure between the Zuckerkandl’s tubercle and the main body of the gland or the
tracheal surface. The RLN may have a sharp angle beneath the tubercle. The nerve is so constantly related to this tubercle, that it is often called “an arrow pointing to the RLN.”
Q 87. What is non-recurrent laryngeal nerve? This is seen on the right side as a result of failure of development of the 4th aortic arch. The RLN here may arise as a branch from the vagus at the level of the inferior horn of the thyroid cartilage (instead of going
down, curving around the subclavian artery and coming up). The incidence is 0.2 – 0.5%.
Q 88. What is suspensory ligament of Berry? It is nothing but a condensation of the pretracheal fascia attaching the thyroid gland to the cricoid. The two ligaments on either side form a sling anchoring the gland to the larynx. It must be severed before the gland can be removed. The RLN is in immediate contact with the back of the ligament.
Toxic Goiter

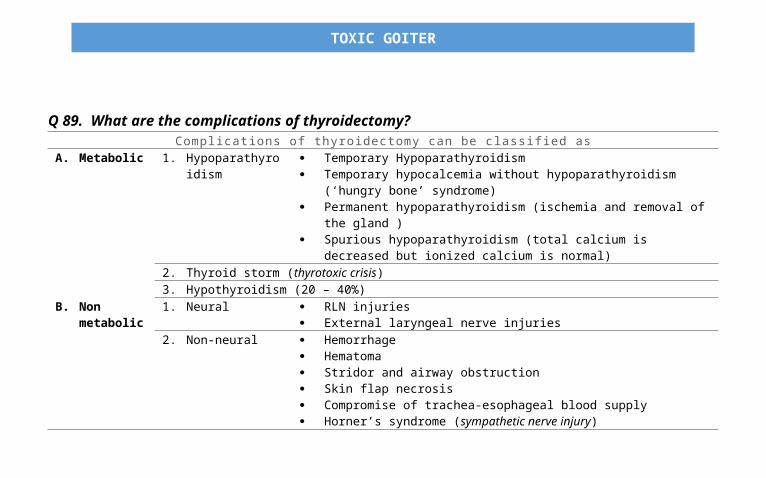
Q 89. What are the complications of thyroidectomy?Complications of thyroidectomy can be classif ied as
A. Metabolic 1. Hypoparathyroidism Temporary Hypoparathyroidism Temporary hypocalcemia without hypoparathyroidism (‘hungry bone’
syndrome) Permanent hypoparathyroidism (ischemia and removal of the gland ) Spurious hypoparathyroidism (total calcium is decreased but ionized calcium is
normal)2. Thyroid storm (thyrotoxic crisis) 3. Hypothyroidism (20 – 40%)
B. Non metabolic
1. Neural RLN injuries External laryngeal nerve injuries
2. Non-neural Hemorrhage
Toxic Goiter

Hematoma Stridor and airway obstruction Skin flap necrosis Compromise of trachea-esophageal blood supply Horner’s syndrome (sympathetic nerve injury) Chylous fistula (extremely rare).
Q 90. What are the two most important complications of thyroidectomy? 1. Hypoparathyroidism 2. Recurrent laryngeal nerve injury. Note : The incidence of both should be less than 1% for an experienced thyroid surgeon.
Q 91. What are the clinical manifestations of hypoparathyroidism?Clinical manifestations of hypoparathyroidism
1. Acral paresthesia2. Circumoral tingling numbness and paresthesia3. Anxiety4. Carpopedal spasm5. Laryngeal stridor6. Spasm of respiratory muscles: dread of suffocation7. Convulsions in later stages
Toxic Goiter

8. Blurring of vision due to spasm of intraocular muscles9. Prolonged unrectified tetany can give rise to cataracts
Note: These clinical manifestations can occur on the same day of surgery or may be noticed later on.
Q 92. What will be the biochemical finding in hypoparathyroidism? Decrease in calcium and increase in phosphorus is the feature of hypoparathyroidism. Decrease in calcium with a decrease in phosphorus is suggestive of “hungry bone” syndrome.
Q 93. What is Chvostek sign? With a knee hammer, gently tap the facial nerve as it courses in front of the external auditory meatus. When
tetany (as a result of hyperparathyroidism) exists, the tapping of the hyperexcitable nerve provokes a brisk muscular twitch on the same side of the face.
Q 94. What is Trousseau’s sign? A sphygmomanometer cuff is placed around the arm and the pressure is raised to 200 mmHg. If tetany is present, in 5 minutes, typical contractions of the hand are seen: the fingers are extended except at the
metacarpophalangeal joints and the thumb is strongly adducted, the combined effect of which is to produce the so-called obstetrician’s hand (accoucheur’s hand).
Note : The migratory superficial thrombophlebitis is also called Trousseau’s sign (seen in visceral malignancies and TAO).
Toxic Goiter

Q 95. What is carpopedal spasm? Strong adduction of the thumb is always present in tetany and this when coupled with extension of the feet is
called “Carpopedal spasm”.
Q 96. What is spurious hypocalcemia? (زاِئ ف) Decrease in total calcium, albumin and hematocrit are seen in first two postoperative days following any surgery
including nonthyroid. This is as a result of antidiuretic hormone release from general stress of the surgery and the consequent water
retention by kidneys and hemodilution. The albumin-bound total calcium is decreased as a result of this. The nonprotein bound free (ionized) calcium will be normal in this situation and therefore estimation of the free
calcium is important to distinguish spurious hypocalcemia from true hypocalcemia.
Q 97. How can you prevent hypoparathyroidism? It is prevented by taking the following precautions during surgery:
1. Identification of parathyroids preoperatively 2. Protection of blood supply to parathyroid glands 3. Capsular ligation of inferior thyroid vessels
Toxic Goiter

4. Autotransplantation of parathyroids in an event of inadvertent removal.
Q 98. What is the treatment of hypoparathyroidism? A. Emergency: 20 mL of 10% calcium gluconate IV in 100 mL of D5W over 10 – 15 minutes B. Chronic Patient:
Calcium alone is not enough for the manage ment of hypoparathyroidism. Calcium carbonate 500 mg oral tablets (1.5 to 2.5 g per day). Vitamin D (ergocalciferol) 50 – 100,000 units per day or dihydrotachysterol (DHT) 250 – 1000 micrograms daily. Magnesium parenteral IV/IM 0.5g (4 mEq) and 2 to 4 mEq per Kg body weight over 3–5 days. Magnesium gluconate oral
500 mg tablets. Note: If true hypocalcemia is identified, it is better to treat it pre-emptively rather than to wait for the symptoms.
Q 99. Can the patient get recurrent thyrotoxicosis after surgery? Yes, in 5% of cases. Cure is possible if the thyroid tissue can be reduced below a critical mass. This will result in reduction of
TSAb. When the mass of thyroid tissue is small it can produce only limited hypertrophy and hyperplasia even if the circulating TSAb is high.
Q 100. What are the causes for stridor postoperatively?
Toxic Goiter

Causes of post - thyro idectomy st r idorA. Hematoma (rule out hematoma first by change of dressing)B. Laryngeal edema; three causes:
1. Edema because of intubation 2. Edema because of hematoma 3. Edema because of hypothyroidism as a result of aggressive antithyroid drug therapy
C. Recurrent laryngeal nerve injury.
Q 101. What are the clinical manifestations of RLN injury? The most common manifestation is hoarseness. The other
manifestations are: Dysphonia Paralytic aphonia Periodic aspiration Ineffective cough.
Note: Unilateral RLN palsy is well-compensated normally Normal voice does not mean that the nerve is intact All hoarseness are not because of nerve injury either.
Q 102. What is the indirect laryngoscopy finding in unilateral RLN palsy? Paramedian position of the paralyzed cord Hyperadduction of the normal cord during phonation as compensation.
Toxic Goiter

Q 103. Is there any role for routine post-operative indirect laryngoscopy? Early routine indirect laryngoscopy is done on fourth or fifth day. Cord paralysis is more common than supposed. Asymptomatic bilateral vocal cord paralysis is possible.
Q 104. What is the treatment of unilateral RLN palsy? Symptomatic improvement is seen within 6 weeks. Perioperative steroids are given to reduce the incidence of temporary RLN palsy resulting from edema or contusion. Steroids should be started within 7 days of surgery. Prednisolone 15 mg tid for 10 days is given. Gradually taper the dose to zero over the next 10 days. If there is not any recovery within 6 months, degeneration is to be suspected (recovery may be delayed for 6 – 12
months; no regeneration after 18 months). Speech therapy is instituted if there is no recovery. Medialization of the cord by Teflon injection or some other technique.
Q 105. What are the clinical presentations and treatment of bilateral RLN palsy? This will cause paralysis in adduction Clinically this may go undetected for long periods. Patient may tolerate minimal airway for many years. May present as inspiratory stridor, dyspnea, or minimal dysphonia.
Toxic Goiter

Emergency endotracheal intubation may be required. It is better to do tracheostomy and wait for 1 year (valved tracheostomy tubes are available). Arytenoidopexy, cordectomy or endoscopic laser treatment is done after 18 months.
Q 106. What is the innervation of external laryngeal nerve (a branch of superior laryngeal nerve)? The nerve supplies the cricothyroid muscle, which is a tensor of the vocal cord.
Q 107. What is the clinical presentation of unilateral external laryngeal nerve injury? Clinical presentation:
1. Loss of high pitch for the voice 2. Voice fatigue 3. Breathy voice 4. Frequent throat clearing.
Indirect laryngoscopy will reveal: 1. Shorter and hyperemic vocal cord2. The affected vocal cord will be at a lower level 3. The glottis chink is oblique (rotation of the posterior commissure to the paralyzed side).
Toxic Goiter

Q 108. What is thyrotoxic crisis (thyroid storm)? It is a sudden life-threatening exacerbation of thyrotoxicosis seen in 1 to 2% of patients. This is a syndrome manifested by high grade fever, sweating, tachypnea, hyperventilation, tachycardia, palpitation,
restlessness, tremor, psychosis, delirium, diarrhea, dehydration, nausea, vomiting, hypotension and end-stage coma.
The causes for crisis are : 1. Inadequate preparation prior to surgery 2. Infection in thyrotoxicosis3. Trauma in thyrotoxicosis 4. Pre-eclampsia5. Diabetic ketoacidosis6. Surgical emergency 7. Emotional stress 8. Vigorous palpation of the gland.
Toxic Goiter

Q 109. What is Bayley’s symptom complex?
Bayley’s symptom complex of thyroid storm1. Insomnia2. Anorexia 3. Vomiting4. Diarrhea 5. Diaphoresis 6. Emotional instability 7. Temperature > 38°C 8. Tachycardia 9. Accentuated symptoms and signs of toxicosis10. System dysfunction.
Toxic Goiter
Q 110. What is the treatment of thyroid storm?Treatment of thyroid storm
A. To control fever 1. Acetaminophen is used2. Aspirin is never used as it can elevate the free thyroid hormones3. Tepid sponging4. Cooling blankets
B. To correct dehydration and electrolyte imbalance
1. IV fluids
C. To control the heart rate 1. Propranalol 1–2 mg IV 6th hourly (40–80 mg QID) orally)2. Esmolol 250 – 500 microgram per Kg body weight loading and 50
microgram/Kg/minute maintenanceD. To inhibit hormone release 1. Logols’ iodine 10 drops 3 times
2. Sodium iodide 1gm IV over 24 hours3. Super saturated potassium iodide (SSKI) 10 drops twice daily
E. To inhibit new hormone synthesis 1. Propylthiouracil (50 – 200 mg)2. Carbimazole (20 mg every 4 hours)
In case of adverse reaction to PTU or carbimazole, use lithium carbonate 300 mg every 6th hoursF. To reduce systemic symptoms 1. Hydrocortisone 100mg IV 6th hourly
2. Dexamethasone injection 6–8 mg IV or 2 mg orally 6th hourlyG. Treatment of CCF
Toxic Goiter

H. Antibiotic coverage for infection I. Sedation J. Dialysis if required
Q 111. What are the methods available to remove T3 and T4 from serum? 1. Oral cholestyramine 2. Peritoneal dialysis3. Hemoperfusion.
Q 112. What is the treatment of thyrotoxicosis in pregnancy? Radioiodine is absolutely contraindicated because of the risk to the fetus. The antithyroid drugs and TSH cross the placenta and therefore the baby is born goitrous and hypothyroid. Low dose antithyroid drugs, preferably PTU is the ideal treatment (to keep the free T4 of pregnant women in the
high normal. Avoid methimazole: Associated with cutis aplasia, and esophageal and choanal atresia. The danger of surgery is miscarriage. Surgery can be carried out in the second trimester.
Q 113. What is the treatment of hyperthyroidism during lactation? Thionamides are secreted in breast milk and this was once considered a contraindication. PTU at a dose of 750 mg is safe.
Toxic Goiter

Q 114. What is postpartum hyperthyroidism? Pregnancy will lead onto exacerbation of auto-immune diseases. This may occur with previously diagnosed or
undiagnosed hyperthyroidism. There is a strong association with HLA-DR3 and HLA-DR5 haplotypes.
Q 115. What is thyrotoxicosis factitia? This is usually seen in health cranks as a result of oral intake of thyroxine (usually taken to reduce weight).
Q 116. What is Jod-Basedow thyrotoxicosis? Large doses of iodide given to hyperplastic endemic goiter which is iodine avid may produce temporary
hyperthyroidism. This is Jod-Basedow thyrotoxicosis.
Q 117. What is neonatal thyrotoxicosis? This is seen in babies born to hyperthyroid mothers. TSAb can cross the placental barrier. The hyperthyroidism
gradually subsides after 3 to 4 weeks.
Q 118. What is thyrocardiac? Severe cardiac damage wholly or partly due to hyperthyroidism. This is usually because of secondary thyrotoxicosis
and is mild. This must be rapidly controlled with propranolol to prevent further cardiac damage.
Toxic Goiter
Q 119. What is struma ovarii? Teratoma of the ovaries may differentiate into thyroid tissue. This thyroid tissue becomes hyperactive resulting in
mild thyrotoxicosis. T3 and T4 are raised with suppressed TSH. Radioactive iodine uptake (RAIU) in neck is suppressed and higher intake is seen in the pelvis.
Q 120. What is Hashitoxicosis? This is because of painless thyroiditis. This is an early stage of autoimmune thyroiditis. FNAC picture is that of Hashimoto’s thyroiditis. Thyrotoxicosis in this situation is mild. Glandular enlargement is seen only in 60% of cases. The inflamed gland releases the already formed thyroid hormones into the bloodstream resulting in toxicosis.
Q 121. What is trophoblastic thyrotoxicosis? The hCG from hydatidiform mole, choriocarcinoma and metastatic embryonal carcinoma exhibit cross specificity to thyroid stimulating hormone receptor (TSHR). This results in thyroid overactivity.
Toxic Goiter

Q 122. What is the histopathological appearance of hyperthyroidism? 1. There is hyperplasia of the acini lined by high columnar epithelium. 2. The acini are empty and some of them contain vacuolated colloid (Scalloping). 3. Pseudopapillary formation is seen.
Q 123. What will happen to exophthalmos after surgery or radioiodine therapy? Both will worsen ophthalmopathy. Thionamides will alleviate the eye problem through
immunosuppression.
Q 124. What is the management of exophthalmos (Thyroid Associated Ophthalmopathy)? Symptom control:
1. Sleeping with head end elevation. 2. 1% methylcellulose eye drops to prevent corneal ulceration. 3. High dose prednisolone orally or hydrocortisone IV. 4. Collimated super voltage radiation to retro orbital space (needs expertise).
Note : Radioiodine is avoided in ophthalmopathy.
Q 125. Is there any role for surgery in exophthalmos? Surgical removal of lateral wall or roof of orbit is done for decompression when optic nerve is in danger.
Toxic Goiter