tracheostomy care joy norton tracheostomy clinical …...reasons for tracheostomy. main reasons for...
TRANSCRIPT
TRACHEOSTOMY CARE Joy Norton Tracheostomy Clinical nurse specialist # 538 [email protected]
Reasons for Tracheostomy.
main reasons for tracheostomy tube insertion are:
(1)Most common indication within the critical care setting is the need for prolonged mechanical ventilation. Usually short term tracheostomy.
(2)Airway management: eg Bypass upper airway obstruction such tumours, trauma, infections, post operative swelling. Again usually short term tube removed once swelling subsided 5-10 days post op.
Can be long term (palliative) if tumour not resectable. (3) Poor cough : Neurological /Motor-neuron disease / Chest trauma
Usually long term trachy. (4) Vocal cord paralysis/chronic aspiration. Usually long term trachy
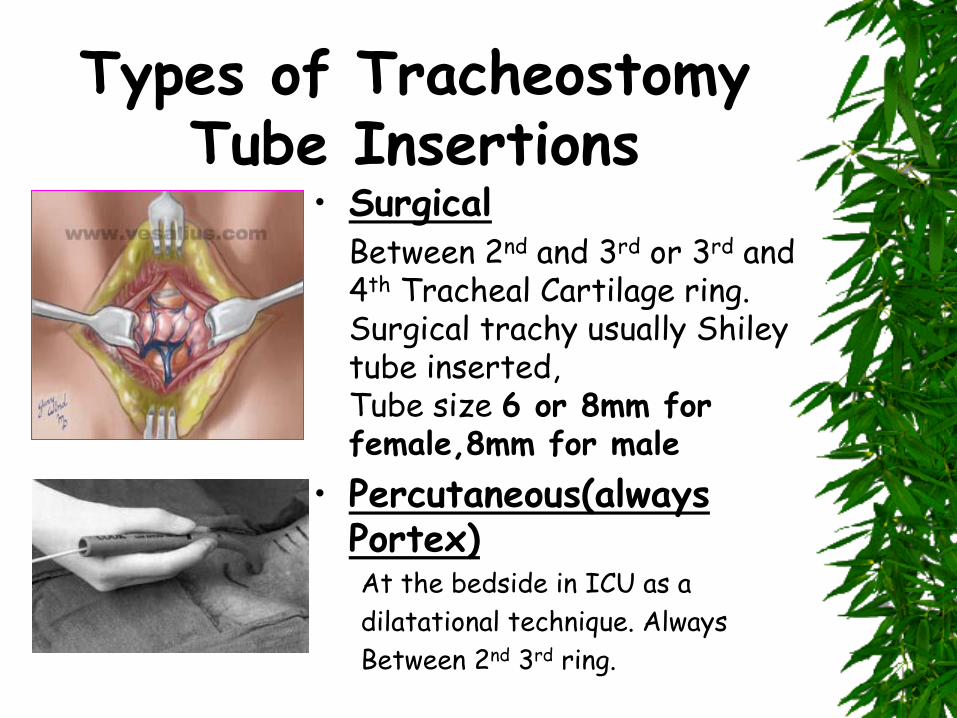
Types of Tracheostomy Tube Insertions
• Surgical Between 2nd and 3rd or 3rd and
4th Tracheal Cartilage ring. Surgical trachy usually Shiley tube inserted, Tube size 6 or 8mm for female,8mm for male
• Percutaneous(always Portex) At the bedside in ICU as a
dilatational technique. Always
Between 2nd 3rd ring.
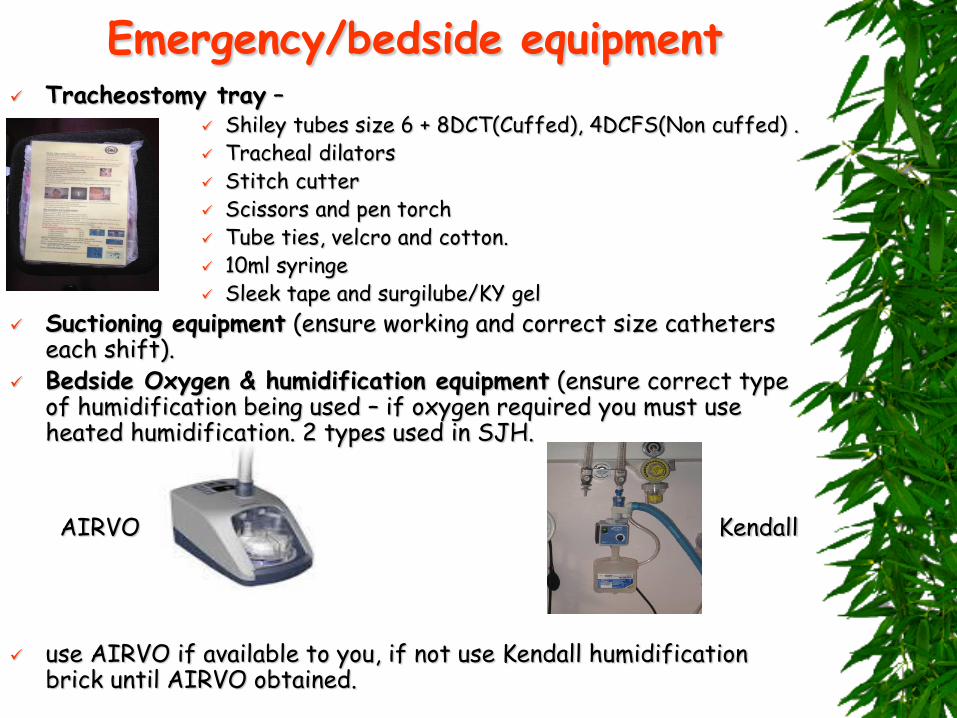
Emergency/bedside equipment Tracheostomy tray –
Shiley tubes size 6 + 8DCT(Cuffed), 4DCFS(Non cuffed) . Tracheal dilators Stitch cutter Scissors and pen torch Tube ties, velcro and cotton. 10ml syringe Sleek tape and surgilube/KY gel
Suctioning equipment (ensure working and correct size catheters each shift).
Bedside Oxygen & humidification equipment (ensure correct type of humidification being used – if oxygen required you must use heated humidification. 2 types used in SJH.
AIRVO Kendall
use AIRVO if available to you, if not use Kendall humidification
brick until AIRVO obtained.
Disposable sterile Portex/Shiley inner cannula.
Gloves – both sterile and non sterile. Infectious waste bag. If old Shiley tube admitted from A&E,Cleaning tool i.e.
mouth swabs/universal sterile swabs (as inner cannula requires cleaning).
Sterile H2O/saline – discard every 24hrs. Communication aids – advice from SLT. Ambu-bag/’C’ circuit within easy reach.
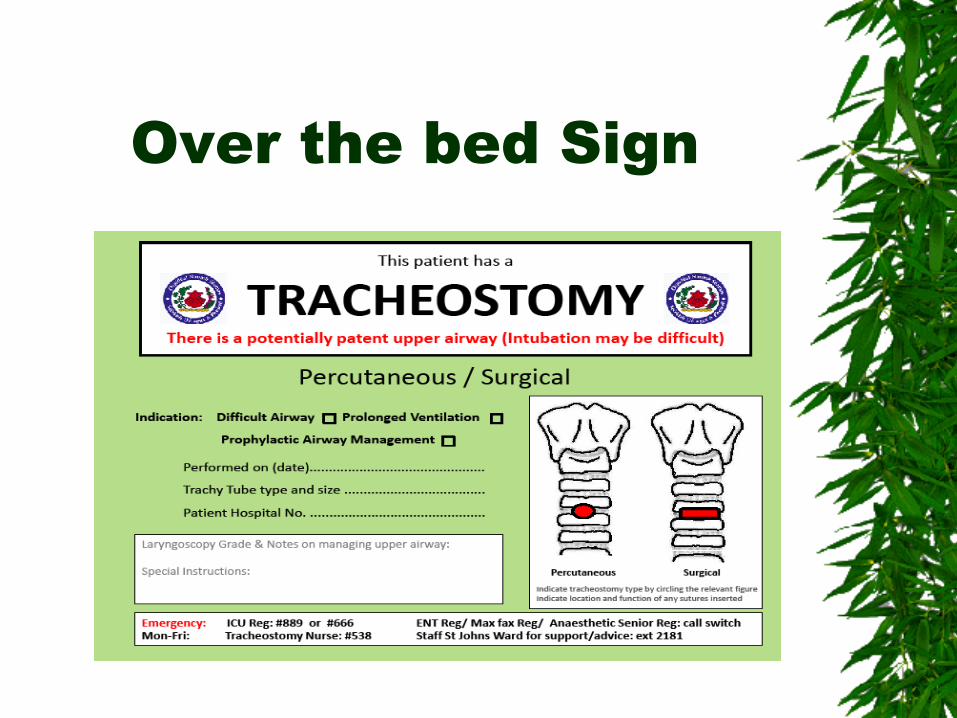
Over the bed Sign
Types of tracheostomy tubes:
Disposable Shileys (4mm, 6mm, 8mm, 10mm): Cuffed non fenestrated ~ DCT Cuffless non fenestrated ~ DCFS Cuffed fenestrated ~ DFEN Cuffless fenestrated ~ DCFN Shileys Tracheosoft XLT Extended Length (6mm, 7mm,
8mm): Proximal ~ extra length required for increased skin to tracheal wall distance Distal ~ longer distal shaft for patients with tracheal malacial or tracheal stenosis Portex (7mm, 8mm, 8.5mm, 9mm): Blue Line Ultra ~ cuffed non fenestrated
Portex adjustable Flange size 7mm,8mm and 9mm
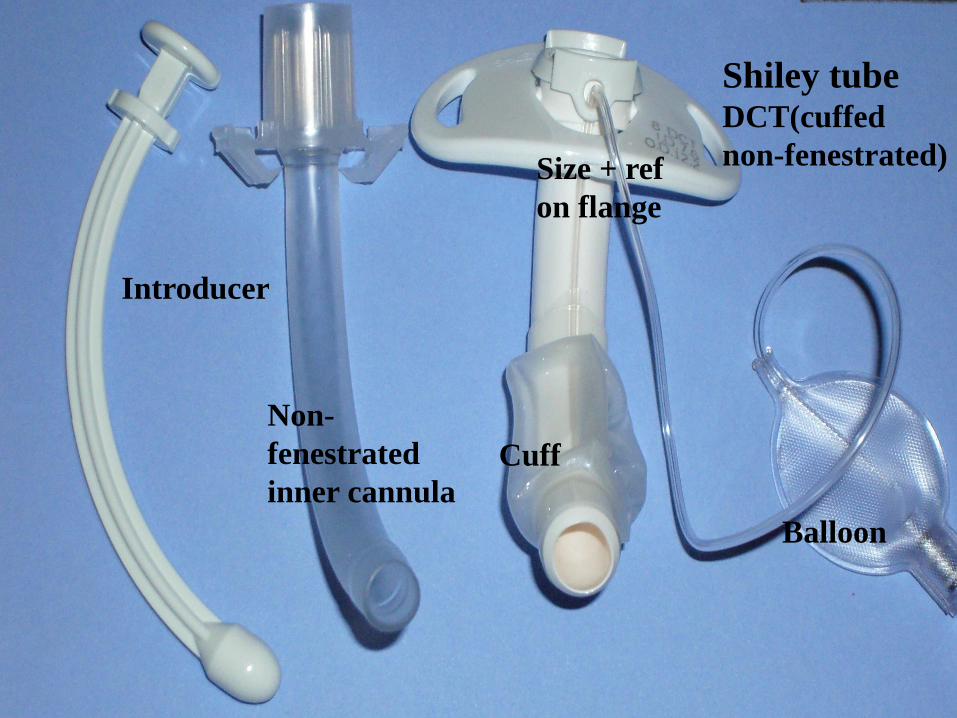
Introducer
Shiley tube
DCT(cuffed
non-fenestrated)
Balloon
Cuff
Non-
fenestrated
inner cannula
Size + ref
on flange
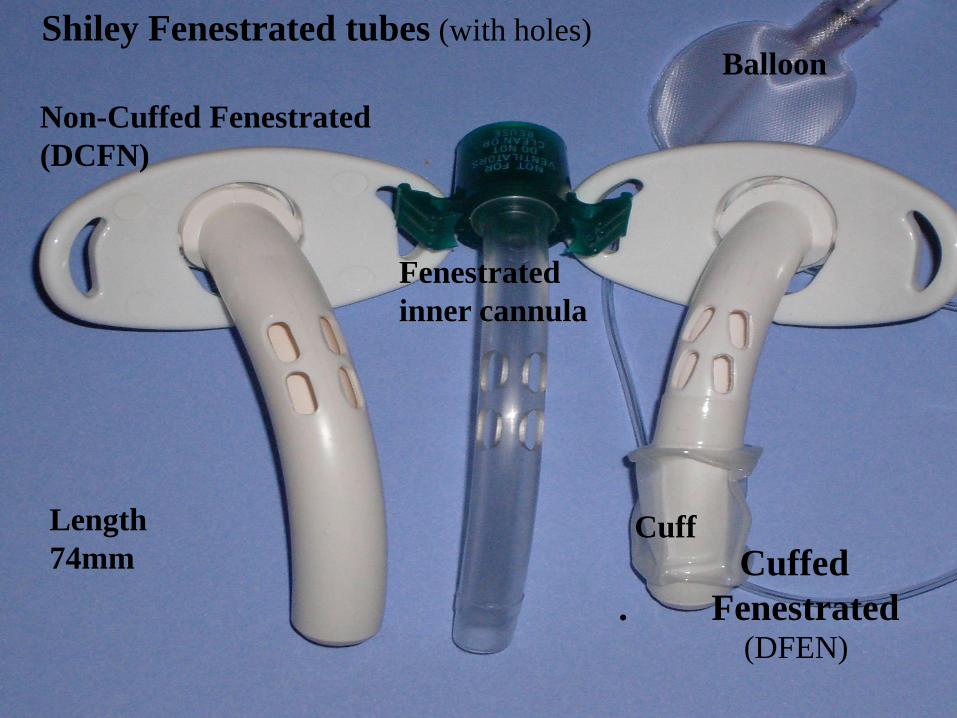
Shiley Fenestrated tubes (with holes)
Non-Cuffed Fenestrated
(DCFN)
Balloon
Cuff
Cuffed
. Fenestrated
(DFEN)
Fenestrated
inner cannula
Length
74mm
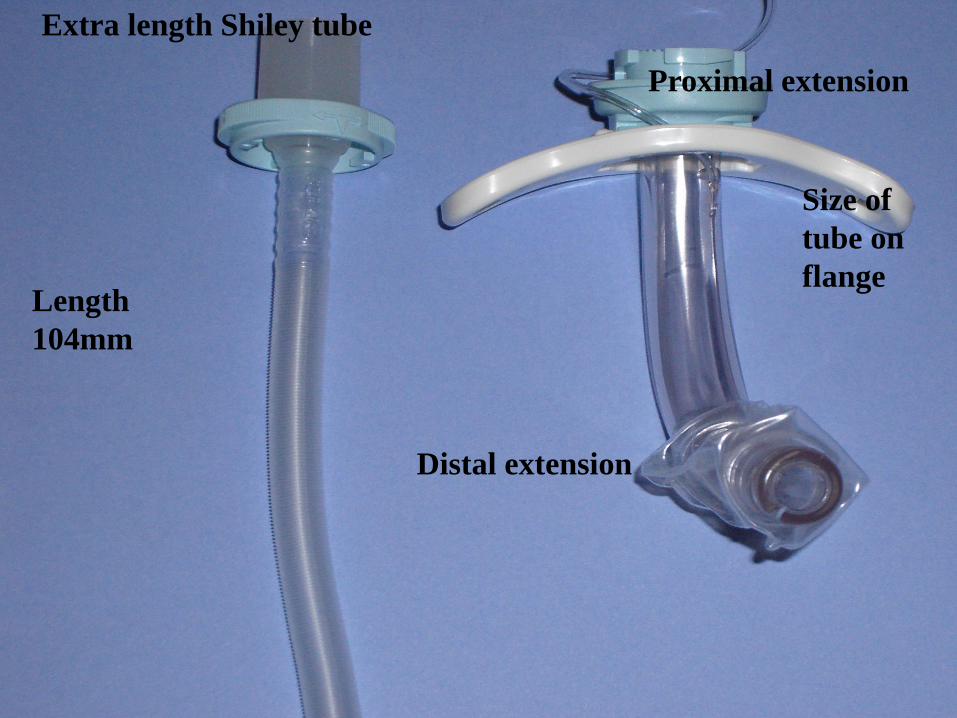
Extra length Shiley tube
Length
104mm
Proximal extension
Distal extension
Size of
tube on
flange
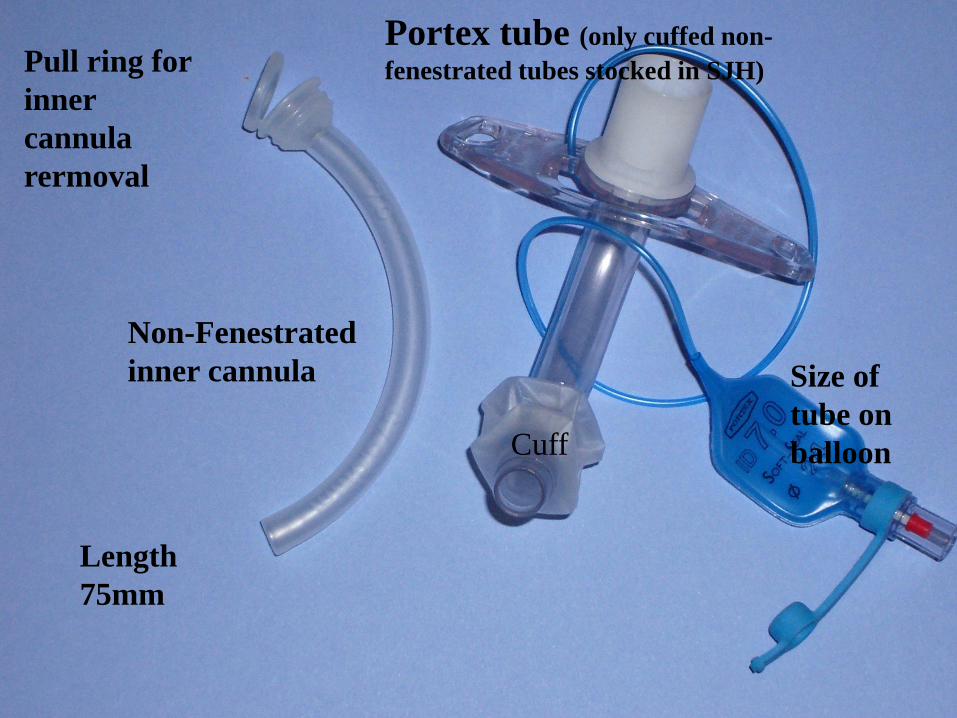
Portex tube (only cuffed non-
fenestrated tubes stocked in SJH)
Size of
tube on
balloon Cuff
Pull ring for
inner
cannula
rermoval
Non-Fenestrated
inner cannula
Length
75mm
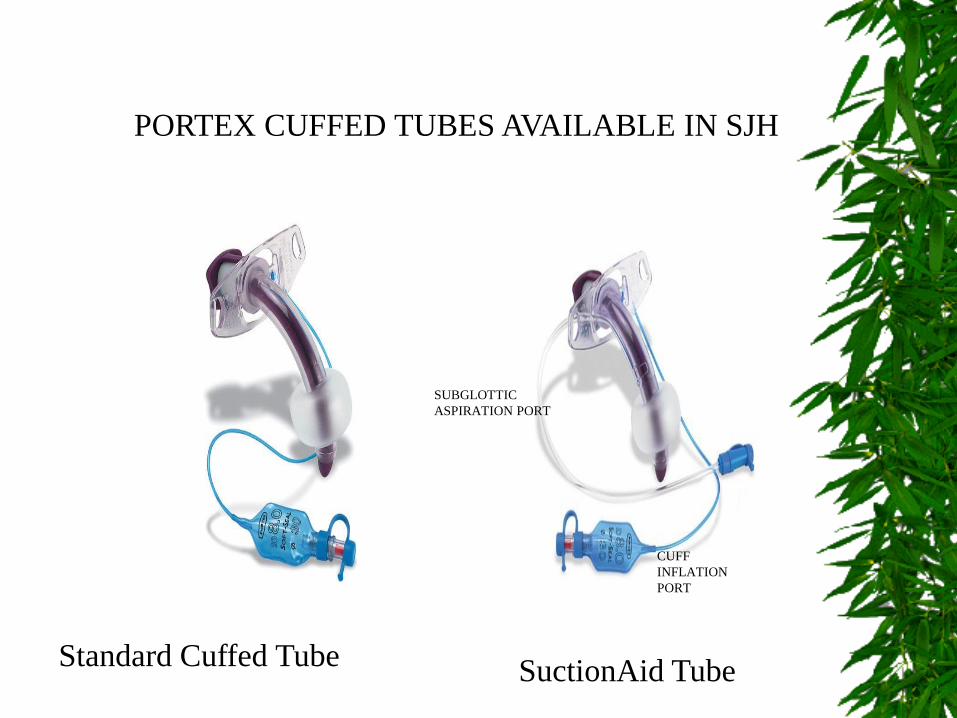
PORTEX CUFFED TUBES AVAILABLE IN SJH
Standard Cuffed Tube SuctionAid Tube
SUBGLOTTIC
ASPIRATION PORT
CUFF
INFLATION
PORT
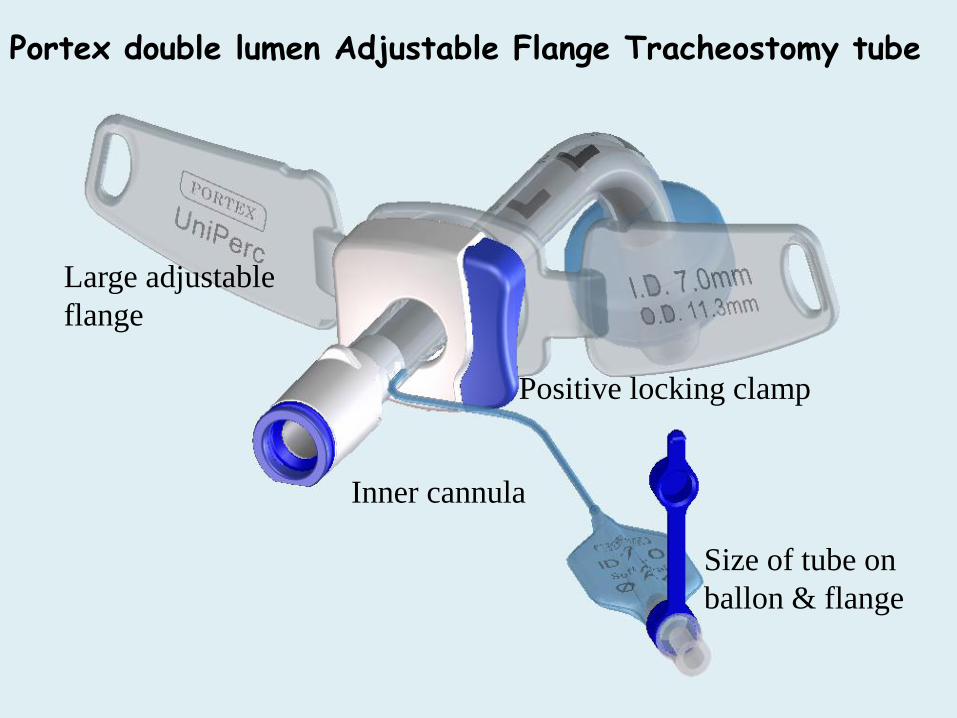
Portex double lumen Adjustable Flange Tracheostomy tube
Inner cannula
Positive locking clamp
Large adjustable
flange
Size of tube on
ballon & flange
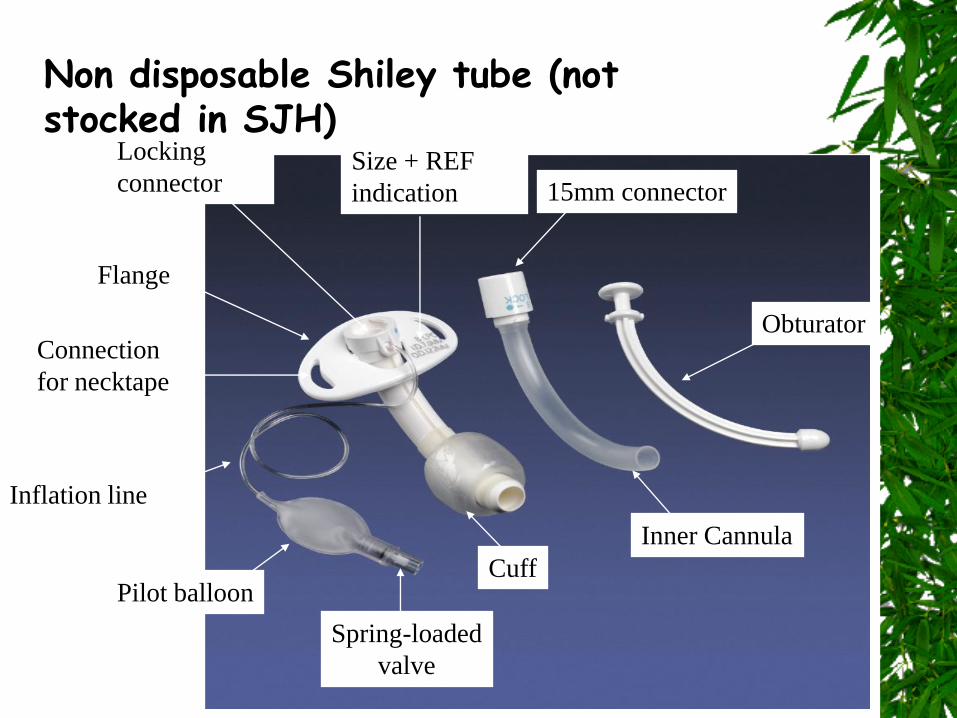
Flange
Connection
for necktape
Inflation line
Pilot balloon
Spring-loaded
valve
Cuff
Inner Cannula
Size + REF
indication 15mm connector
Obturator
Locking
connector
Non disposable Shiley tube (not stocked in SJH)

SHILEY FLEXIBLE TRACHEOSTOMY TUBE
NEW
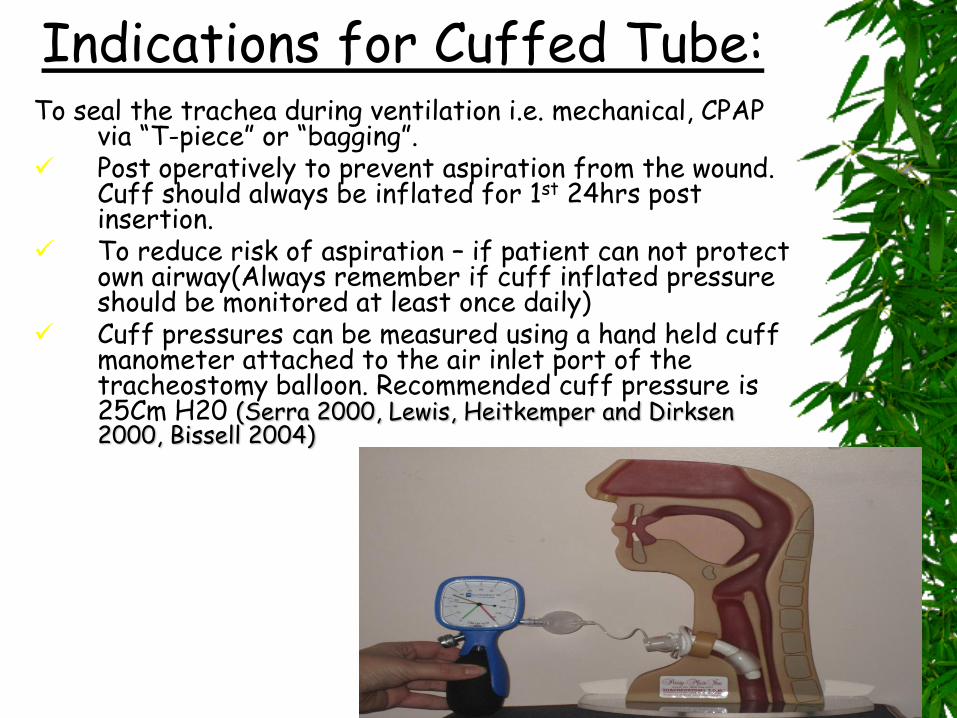
Indications for Cuffed Tube: To seal the trachea during ventilation i.e. mechanical, CPAP
via “T-piece” or “bagging”. Post operatively to prevent aspiration from the wound.
Cuff should always be inflated for 1st 24hrs post insertion.
To reduce risk of aspiration – if patient can not protect own airway(Always remember if cuff inflated pressure should be monitored at least once daily)
Cuff pressures can be measured using a hand held cuff manometer attached to the air inlet port of the tracheostomy balloon. Recommended cuff pressure is 25Cm H20 (Serra 2000, Lewis, Heitkemper and Dirksen 2000, Bissell 2004)
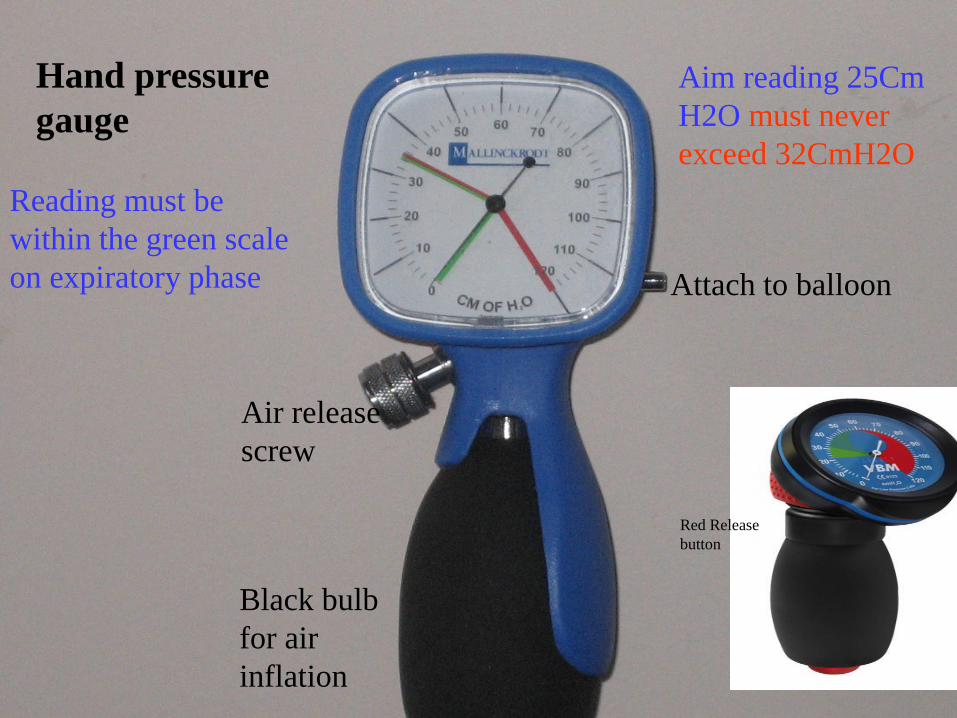
Hand pressure
gauge
Air release
screw
Attach to balloon
Black bulb
for air
inflation
Reading must be
within the green scale
on expiratory phase
Aim reading 25Cm
H2O must never
exceed 32CmH2O
Red Release
button
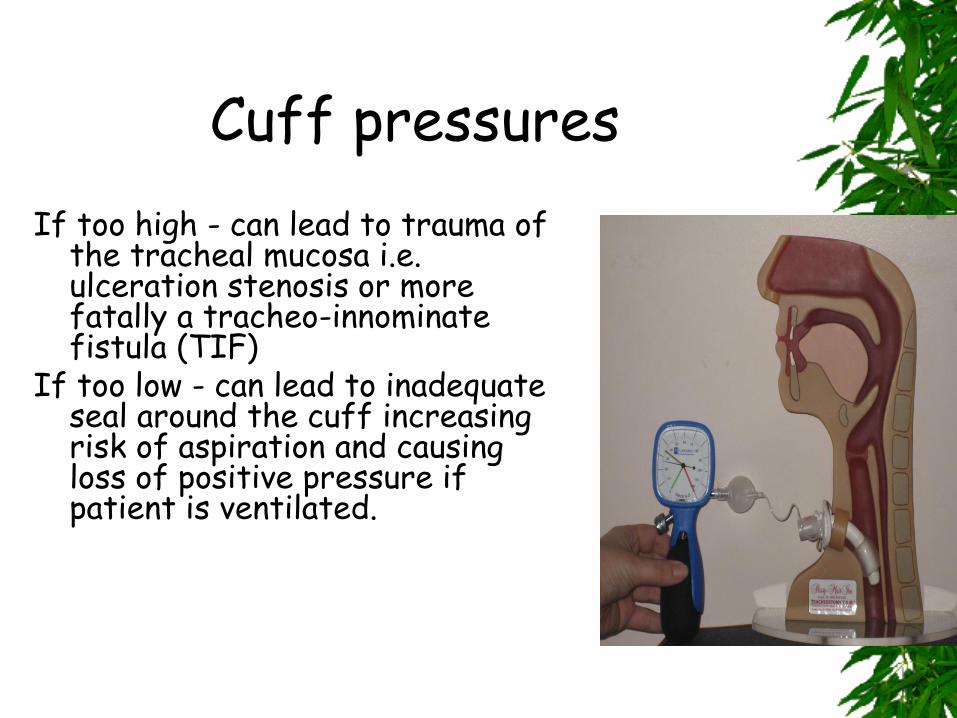
Cuff pressures
If too high - can lead to trauma of the tracheal mucosa i.e. ulceration stenosis or more fatally a tracheo-innominate fistula (TIF)
If too low - can lead to inadequate seal around the cuff increasing risk of aspiration and causing loss of positive pressure if patient is ventilated.
How to deflate cuff ~ 2 person technique:
1. Suction oropharynx. 2. 1st person suction via tracheostomy as 2nd person slowly
aspirates air from inlet valve. 3. Ideally a patients cuff should be deflated before going to the
ward unless high risk of aspiration or newly inserted tube. Indications for cuff re-inflation 1. Desaturation(must check inner cannula patent first) 2. Respiratory or cardiovascular distress 3. ?? Constant oral drooling 4. ?? No swallows observed (National Hospital for
Neurology and Neurosurgery 2003)
5. Haemorrhage –Overinflate cuff and for urgent surgical expoloration
( The board management and trustees of the british journal of Anaesthesia 2005)
Care of Inner cannula, stoma site & ties Inner cannula should be checked at beginning of every shift and then 4hourly but more frequently if sputum is thick and sticky. Shiley tubes To remove shiley inner cannula: Wearing non-sterile gloves press together the 2 clips either side and pull same out.IF clean can reinsert. If soiled dispose in infectious waste bag and Insert a new one.(please record on EPR via iView- lines and devices-
airway management) Inner cannula must be the same size as trachy tube. Ensure box of disposable inner cannulas at patient’s bedside.Shiley inner cannulas come 10 per box. To order inner cannulas Mon-fri before 17.00 call 2660 ward stores, at weekends obtain From other wards. PORTEX tubes To remove Portex inner cannula Pull ring outward towards you with right hand, and with the left hand hold trachy flange to support tube and prevent displacement. If clean re-insert again, inner cannula will click into place. If dirty dispose and replace with a new sterile Portex inner cannula

PORTEX INNER CANNULA SHILEY INNER CANNULA
Cleaning tracheostomy site and ties
• Site
*Inspect and clean the site at least once a day – more frequent if area is moist/dirty from secretions. *Clean as sterile as is possible using normal saline.
• * If there are any signs of excoriation/dryness Vaseline or a barrier cream for example Cavilon can be applied to the surrounding skin (keeping away from the stoma opening).
• Monitor site for signs of bleeding, lyafoam T, Kaltostat dressings used to contain bloody ooze post op. If bleeding from site constant, dressings becoming soaked requiring frequent dressing change (every half hour), inform team who inserted tube eg (ENT/Oral Maxillofacial team), as may need diathermy to bleeding point.
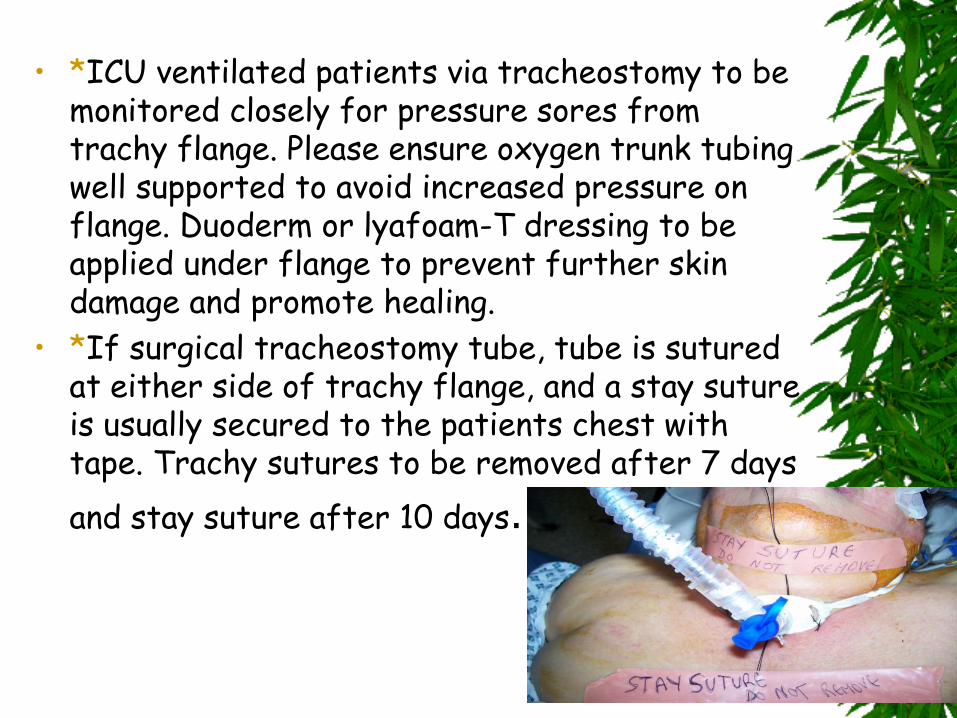
• *ICU ventilated patients via tracheostomy to be monitored closely for pressure sores from trachy flange. Please ensure oxygen trunk tubing well supported to avoid increased pressure on flange. Duoderm or lyafoam-T dressing to be applied under flange to prevent further skin damage and promote healing.
• *If surgical tracheostomy tube, tube is sutured at either side of trachy flange, and a stay suture is usually secured to the patients chest with tape. Trachy sutures to be removed after 7 days
and stay suture after 10 days.
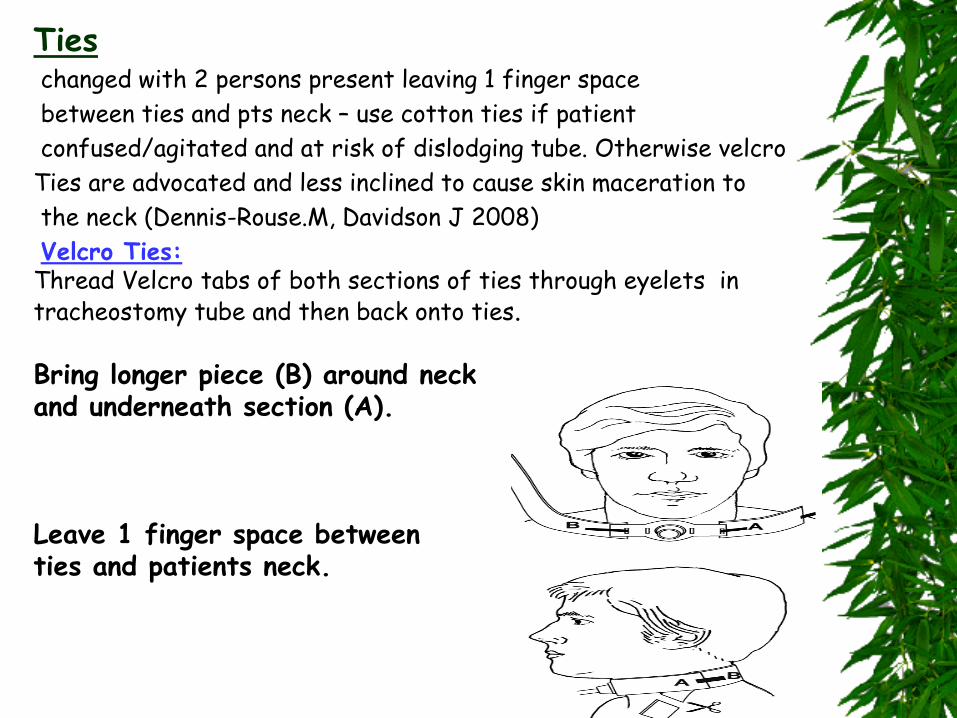
Ties changed with 2 persons present leaving 1 finger space
between ties and pts neck – use cotton ties if patient
confused/agitated and at risk of dislodging tube. Otherwise velcro
Ties are advocated and less inclined to cause skin maceration to
the neck (Dennis-Rouse.M, Davidson J 2008)
Velcro Ties: Thread Velcro tabs of both sections of ties through eyelets in tracheostomy tube and then back onto ties.
Bring longer piece (B) around neck and underneath section (A). Leave 1 finger space between ties and patients neck.
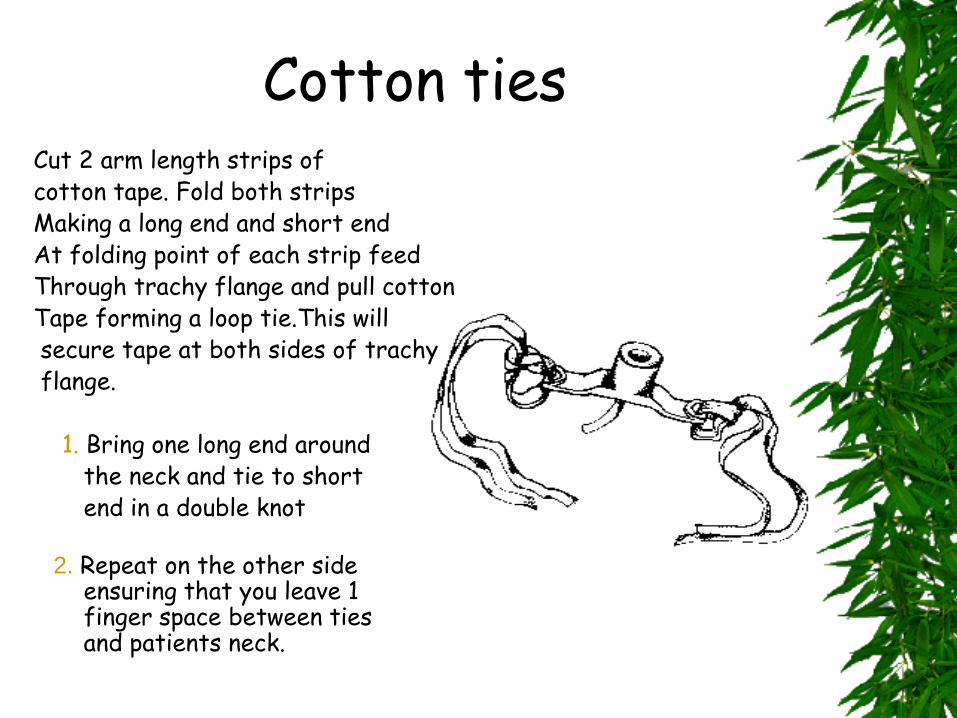
Cotton ties Cut 2 arm length strips of cotton tape. Fold both strips Making a long end and short end At folding point of each strip feed Through trachy flange and pull cotton Tape forming a loop tie.This will secure tape at both sides of trachy flange. 1. Bring one long end around the neck and tie to short end in a double knot 2. Repeat on the other side ensuring that you leave 1 finger space between ties and patients neck.
Indications for tube change
Elective ~ Tracheostomy tubes require to be changed every 28-30days to comply with EU regulations (EEC Directive 1993). ~ For weaning purposes i.e. downsizing, changing to cuffless or fenestrated. Emergency ~ Tube dislodgement or accidental removal. ~ Tube obstruction (decreased risk when
using double lumen tubes).
When / who performs tube change
5 – 7 days post insertion – enables tract to become well established.
1st tube change should be carried out by a competent doctor/Anaesthetist/Tracheostomy safety facilitator/Clinical facilitator ICU.
Scope of Nursing Practice (An Bord Altanais 2003)
A registered nurse who has been assessed and is competent in the procedure can carry out subsequent tube changes .
It should be always carried out with 2 nurses present to ensure patient safety at all times and all changes should be documented in both nursing and medical notes.
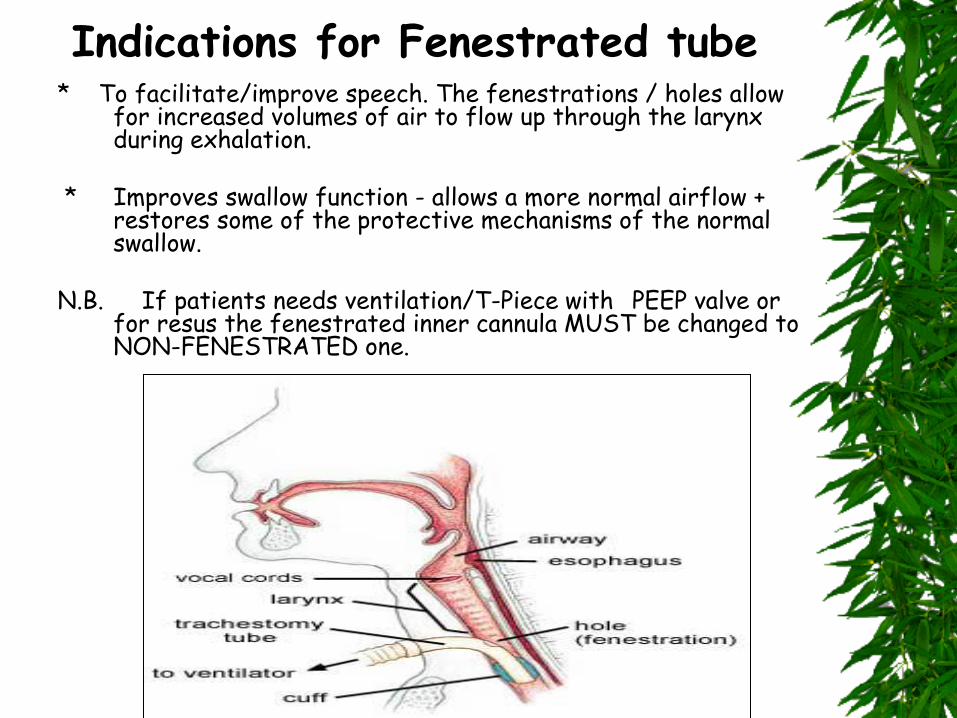
Indications for Fenestrated tube * To facilitate/improve speech. The fenestrations / holes allow
for increased volumes of air to flow up through the larynx during exhalation.
* Improves swallow function - allows a more normal airflow + restores some of the protective mechanisms of the normal swallow.
N.B. If patients needs ventilation/T-Piece with PEEP valve or
for resus the fenestrated inner cannula MUST be changed to NON-FENESTRATED one.
Communication issues • Air no longer directed through the larynx so patient may
not be able to communicate verbally
SLT referal. May require picture chart if unable to read/write, poor vision, deaf.
Passy Muir speaking valve (PMV)
• If cuffed tube, ensure cuff deflated before you apply PMV.
• Please ensure speaking valve removed at night/pt sleeping.
• Do not apply speaking valve if tube insitu less than 48 hours.
• Clean daily with soapy water, rinse and leave to dry.
• Ensure patient has some form of humidification insitu if ventilating on room air as PMV will not
humidify the patients air
• Never apply PMV to
Laryngectomy pt
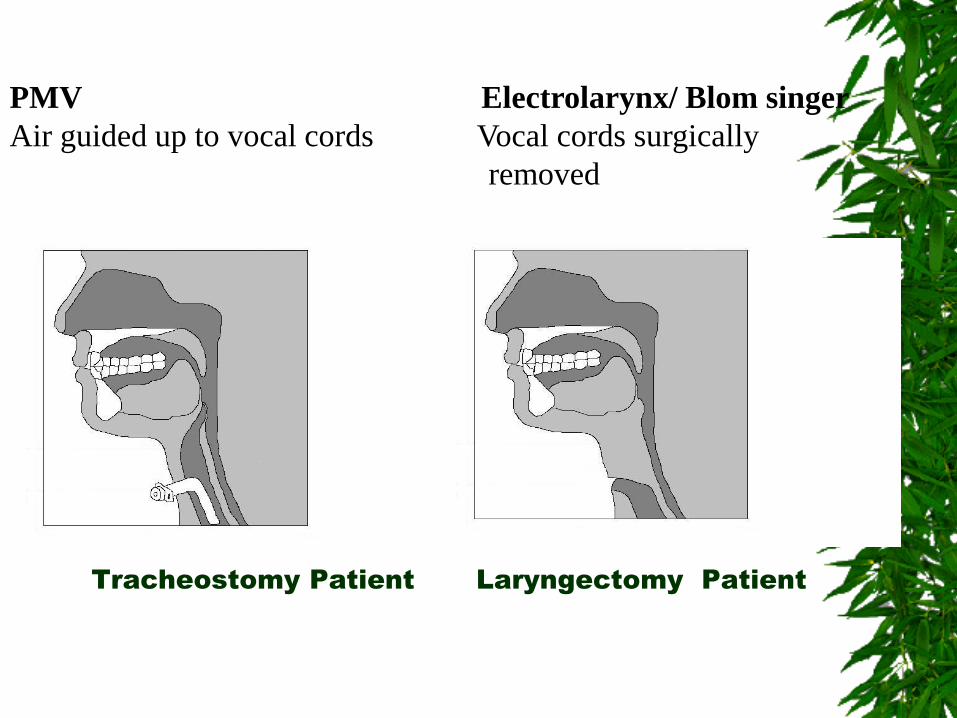
Tracheostomy Patient Laryngectomy Patient
PMV Electrolarynx/ Blom singer
Air guided up to vocal cords Vocal cords surgically
removed

Laryngectomy patient
with Blom singer valve
in situ
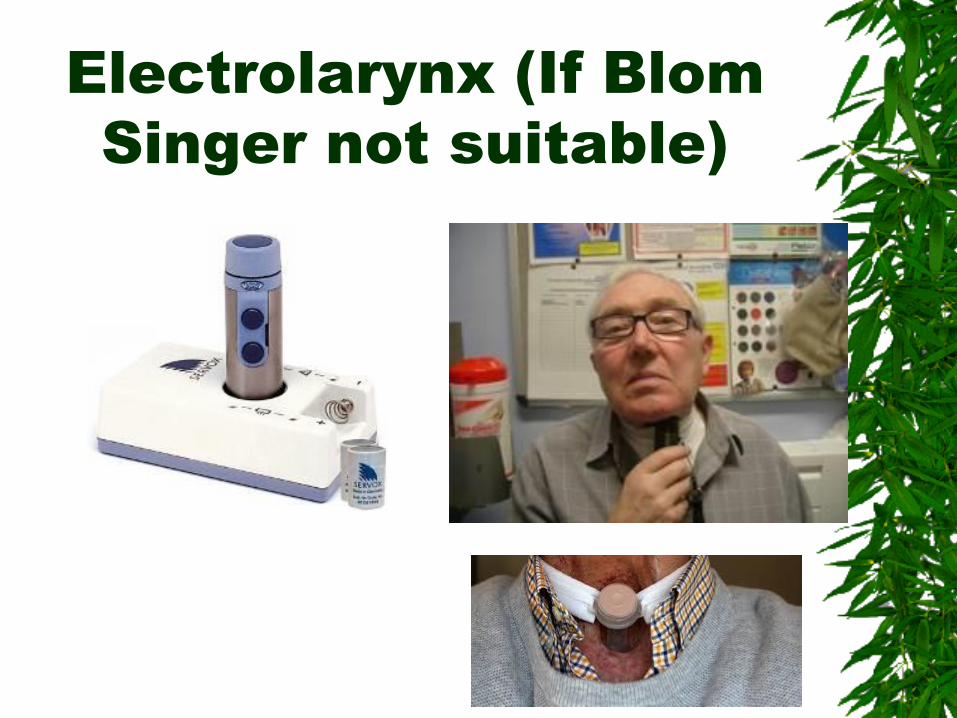
Electrolarynx (If Blom
Singer not suitable)
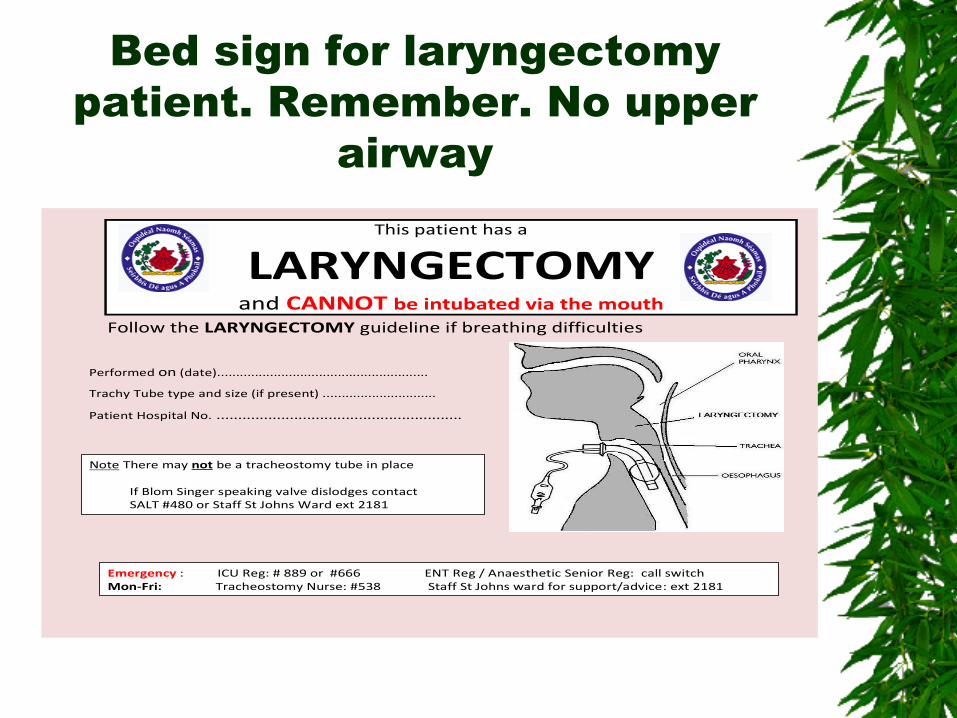
Bed sign for laryngectomy
patient. Remember. No upper
airway
This patient has a
LARYNGECTOMYand CANNOT be intubated via the mouth
Follow the LARYNGECTOMY guideline if breathing difficulties
Performed on (date)........................................................
Trachy Tube type and size (if present) ..............................
Patient Hospital No. .........................................................
Note There may not be a tracheostomy tube in place
If Blom Singer speaking valve dislodges contact SALT #480 or Staff St Johns Ward ext 2181
Emergency : ICU Reg: # 889 or #666 ENT Reg / Anaesthetic Senior Reg: call switch Mon-Fri: Tracheostomy Nurse: #538 Staff St Johns ward for support/advice: ext 2181
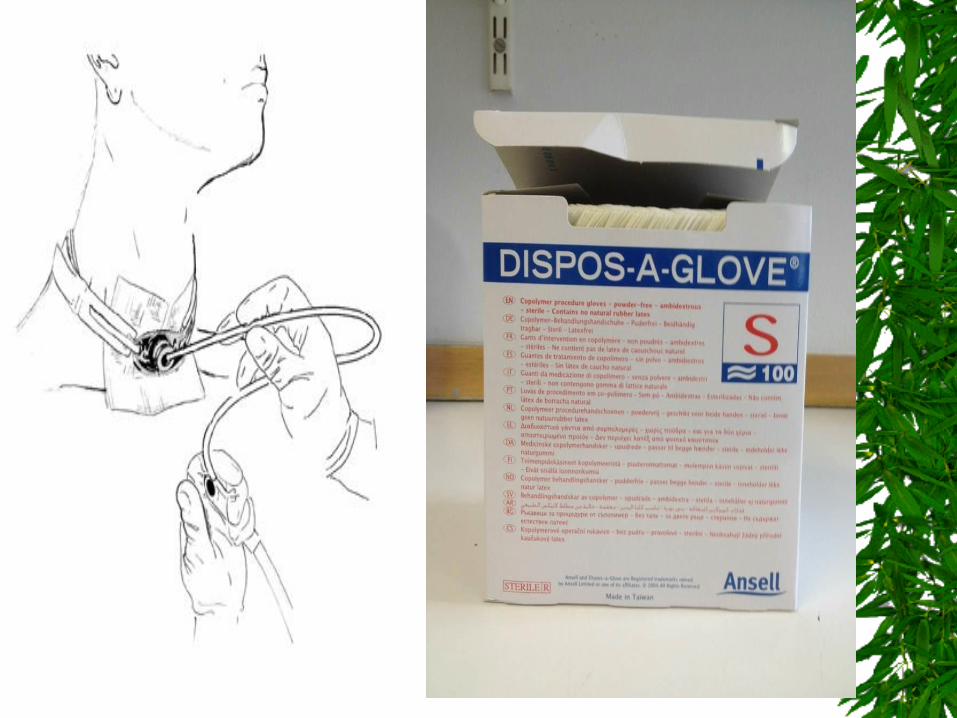
Suctioning: • SUCTION EQUIPMENT must be working and at patients
bedside. • *Suction vacuum pressure <20kpa or 150mmHg • *Sterile catheter tip and technique. • *Only as required (prn) and record on observation sheet • *Suction catheter to be inserted no more than 1cm beyond length
of trachy tube(roughly a pens length)No suction applied on catheter insertion.
• *Suction to be applied only whilst catheter is being withdrawn. • *Recommended time from insertion to removal = 15seconds • *Always use non-fenestrated inner cannula when suctioning. • *Ensure suction container changed when over ¾ full. • *Suction catheters size= size of trachy tubex3 answer divided
x2 • eg size 8 shiley tube x 3 divided by 2=12 so size 12 suction
catheter used. or • SIZE OF TUBE ADD 4 (but only works for tubes sizes 6 & 8) • If you carried out suctioning document it on EPR
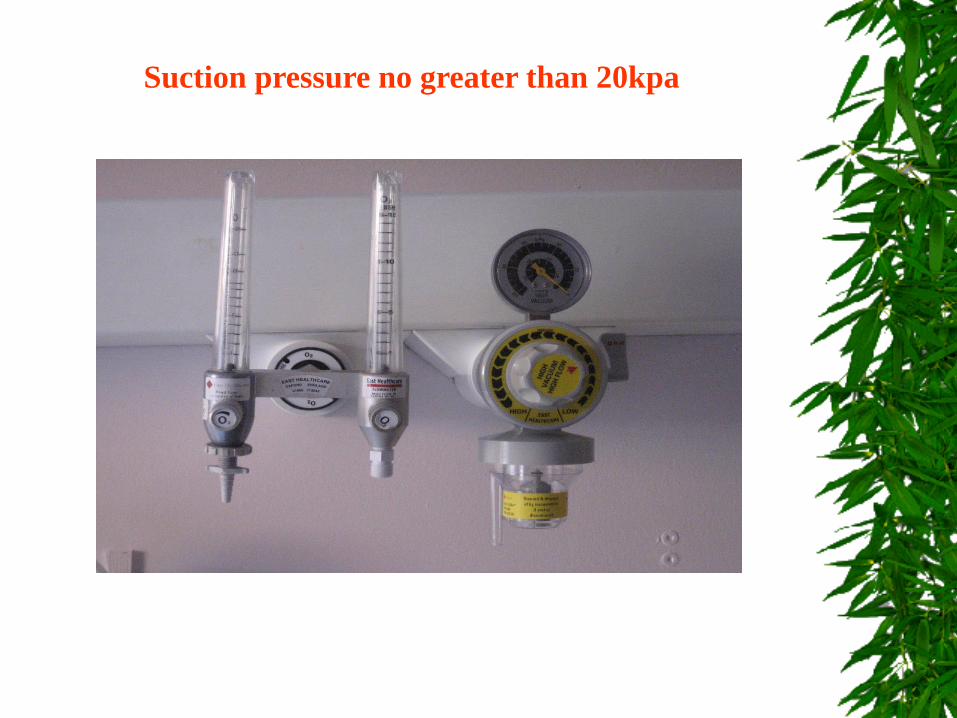
Suction pressure no greater than 20kpa
Decannulation • Patient able to clear own secretions/good strong cough. • No profound myopathy • Maintain SaO2 > 90% (Russell & Matta 2004 ) • ENT patients: downsize tube day 5-7 - smaller, cuffless,
fenestrated tube.cap tube as tolerated • observing for respiratory distress • – proceed to decanulation if patient tolerates capping >24hrs Explain procedure to patient. Remove tracheostomy tube – on expiration (neck muscles etc relaxed). Inspect site for signs of granulation tissue – treat with hydrocortisone 1% cream. Cover with air tight occlusive dressing (i.e. Duoderm + gauze), change dressing PRN, observe for signs of site infection over granulation and excoriation. Usually takes approx 10 days for site to heal – occasionally requires surgical
closure. • Encourage patient to press on stoma on coughing to prevent leakage of
secretions from stoma. • • Max Fax Patients: are NOT usually downsized , can decannulate from day 5 by
Max Fax Reg and exit site sutured closed and sutures removed after 7 days
• Keep tracheostomy tray at patients bedside for 24 hours post
decannulation

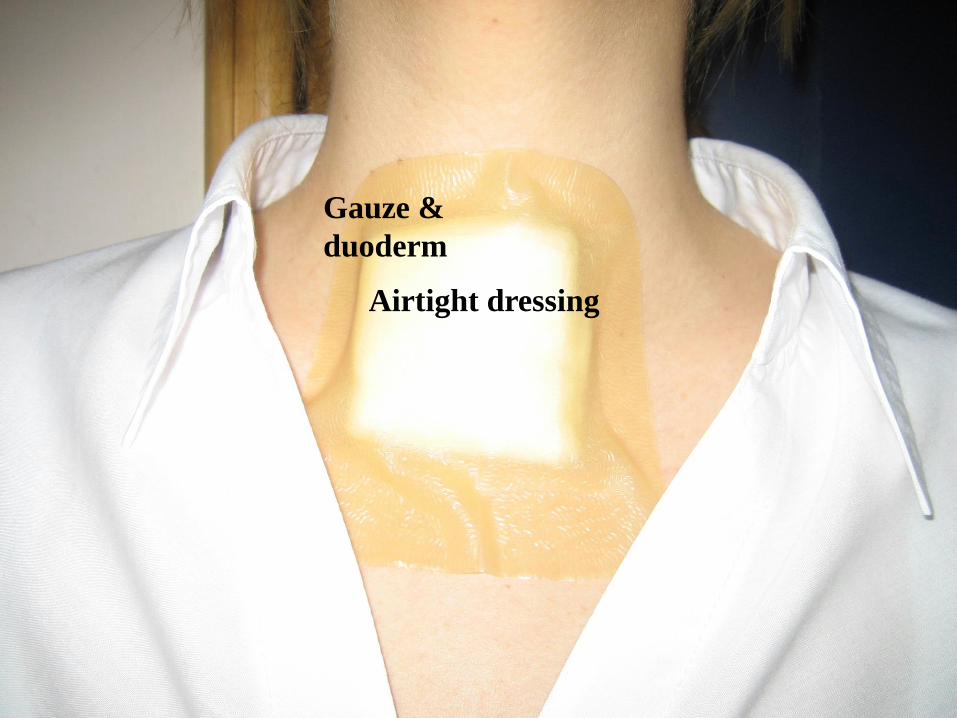
Gauze &
duoderm
Airtight dressing

Gauze duoderm & hypafix for
extra seal

Healing exit site
Tracheostomy
scar
Help and support
Clinical facilitators / senior staff on ICU/HDU, St Johns Ward
Tracheostomy CNS ~ bleep 538
Policy manual on each ward area
Intranet SJH
Laminated prompt card
References National Hospital for Neurology and Neurosurgery, (2003). Multidisciplinary
Tracheostomy Care Policy.
McGrath B (2014) Comprehensive Tracheostomy Care .The National Tracheostomy Safety project manual.John Wiley & sons LTD.
Russell, C. & Matta, B. (2004) Tracheostomy: A Multi Professional Handbook.
Greenwich Medical Media LTD. London An Bord Altranais (2000) Scope of Nursing and Midwifery Practice Framework European Economic Community (1993). “Council directive concerning medical
devices”. Class 11 a - Rule 7. 93 / 42. Bissell, C. (2004) Aaron’s Tracheostomy Page. http://www.tracheostomy.com Serra, A., (2000) Tracheostomy Care. Nursing Standard. 14(42)
Dennis-Rouse, M; Davidson, J (2008) An evidence evaluation of tracheostomy care
practices. Critical Care Nursing Quarterly. 31(2).
Useful website tracheostomy.org.uk