tranexamic acid & post partum haemorrhage - bbts | home · pdf filetranexamic acid &...
TRANSCRIPT

Prof Beverley Hunt, Guy’s & St Thomas’ NHS Foundation Trust
Kings College, London Medical Director of Thrombosis UK
Twitter: @bhwords
Tranexamic acid & post partum haemorrhage

Tranexamic acid a lysine binding analogue

TXA IN TRAUMATIC HAEMORRHAGE
• 20,211 trauma patients with or at risk of significant
haemorhage randomised to TXA or placebo.
• Results show a 15% relative reduction in death from
bleeding, and 9% from all cause mortality in the TXA
treated group.
• No evidence of an increase in adverse effects, including thromboembolic events, in the TXA treated group.
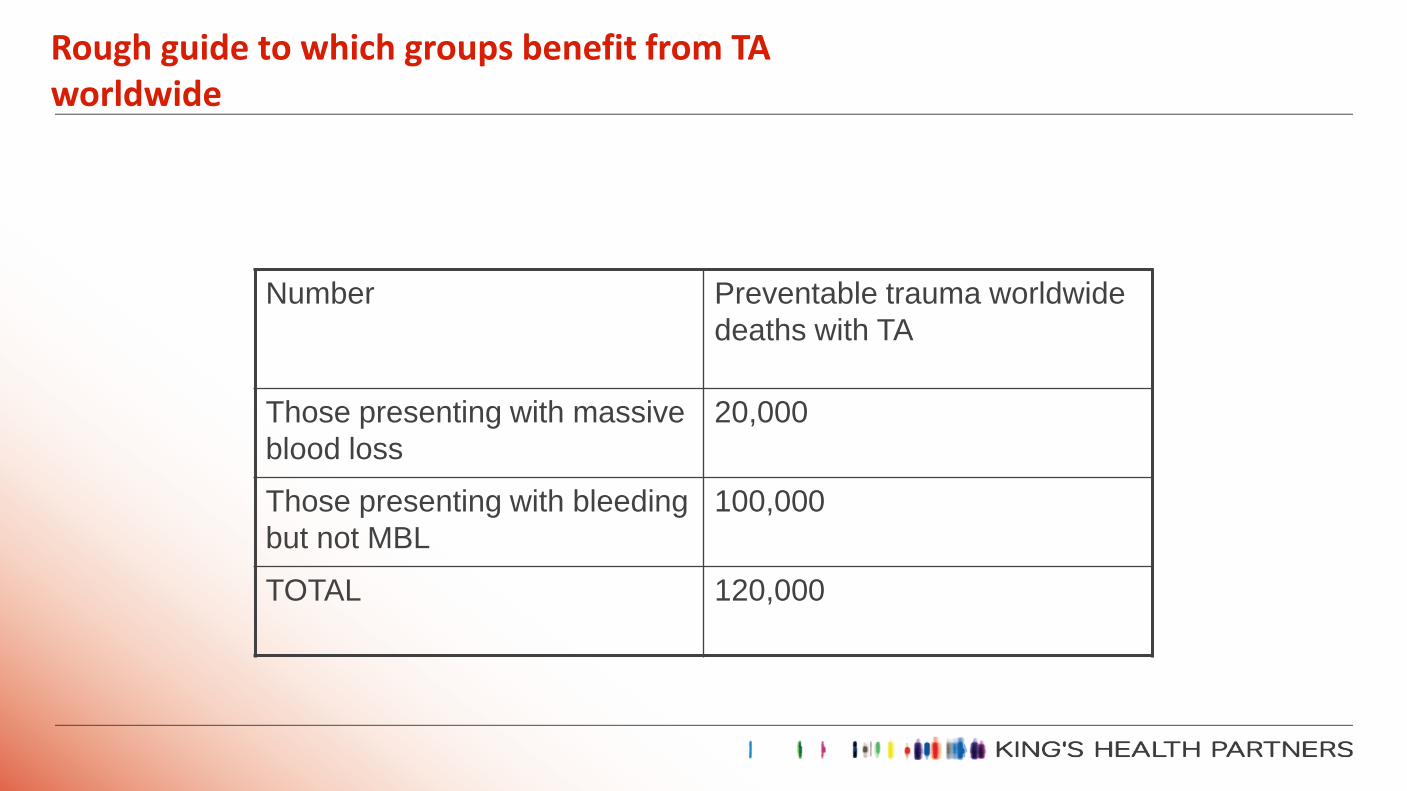
Rough guide to which groups benefit from TA worldwide
Number Preventable trauma worldwide
deaths with TA
Those presenting with massive
blood loss
20,000
Those presenting with bleeding
but not MBL
100,000
TOTAL 120,000

Systematic review identified 129 trials between 1972-2011 including 10 488
patients
Ker et al. BMJ 2012; 344:e3054
TXA
TXA better TXA worse
0.62 (0.58-0.65)
RR (95% CI)
0.4 0.8 1.2 1.6
Transfusion
TXA
RR (95% CI)
TXA better TXA worse
0 0.4 0.8 1.2 1.6
0.61 (0.38-0.98)
Mortality
72
trials 95 trials
TXA use in surgery

Protocol Code: ISRCTN11225767
Tranexamic acid for the treatment of gastrointestinal
bleeding: an international randomised,
double blind placebo controlled trial

Topical use of tranexamic acid S. Alshryda et al, North Tees & Hartlepool Hosp, J Bone Joint Surg Am, 2013 Nov 06;95(21):1961-1968. of of
The TRANX-K (Tranexamic Acid in Total Knee Replacement) trial was a double-blind, placebo-controlled trial of the effect of topical (intra-articular) application of TA on blood loss & transfusion following a unilateral total knee replacement.
1gm TA in 50mls saline sprayed into the wound at the end of TKR
TA reduced
-blood transfusion by 15.4% blood loss by 168 mL the length of stay by 1.2 days
New patent: self-propelled particles that transport cargo through
flowing blood and halt hemorrhage.
R. Baylis et al. Science Advances, 2015; 1 (9): e1500379 DOI:

THE WOMAN TRIAL OVERVIEW AND PROGRESS
Protocol Code: ISRCTN76912190
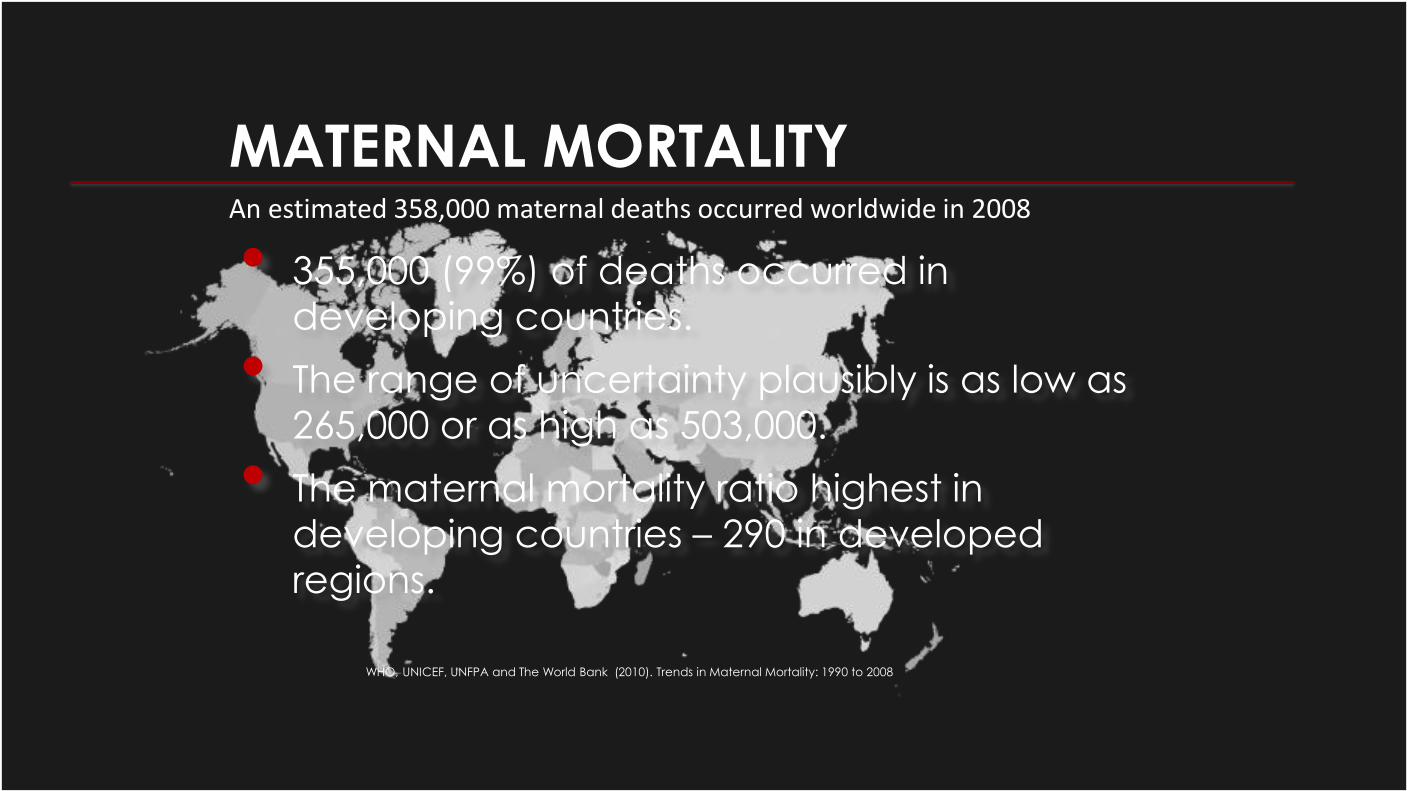
MATERNAL MORTALITY • 355,000 (99%) of deaths occurred in
developing countries.
• The range of uncertainty plausibly is as low as
265,000 or as high as 503,000.
• The maternal mortality ratio highest in developing countries – 290 in developed
regions.
WHO, UNICEF, UNFPA and The World Bank (2010). Trends in Maternal Mortality: 1990 to 2008
An estimated 358,000 maternal deaths occurred worldwide in 2008

• Three randomised trials with 461 participants.
• In two trials, TXA was administered before the incision for a
caesarean section.
• In one trial, TXA was administered immediately after
spontaneous vaginal delivery.
SYSTEMATIC REVIEW OF TXA IN PPH

SYSTEMATIC REVIEW OF TXA IN PPH REDUCED BLOOD LOSS
but trials quality too poor to confirm or refute moderate
effects.
TXA better TXA worse
-200 -100 100 200 0
Study
Gai 2004
Gohel 2007
Yang 2001
Total (95% CI)

RATIONALE FOR THE WOMAN TRIAL • Bleeding is a leading cause of postpartum mortality.
• Blood transfusion can be dangerous.
• Antifibrinolytics reduce blood loss after surgery.
• CRASH-2 trial of 20,211 trauma patients showed TXA safely reduces the risk of death from bleeding by a relative 15%.
• Trials in PPH too small to confirm or refute moderate effects.
• A simple, relatively cheap intervention like TXA could prevent deaths and morbidity associated with PPH.

AIMS • Primary outcomes: To quantify the effect of
tranexamic acid (TXA) on death and hysterectomy in women with clinician diagnosed PPH.
• Secondary outcomes to quantify the effect of TXA on:
• Death
• Surgical Interventions
• Blood transfusion
• Health status measured using the EQ-5D scale
• Thromboembolic events
• Other relevant medical events
• Length of stay at hospital/time spent in an intensive care unit
• Receipt of mechanical ventilation
• Status of breastfed baby/ies

CONTRIBUTIONS
0.1%
0.2%
0.3%
0.4%
0.9%
1.7%
1.9%
2.0%
2.4%
2.7%
3.0%
3.3%
3.6%
4.5%
5.2%
5.2%
10.5%
20.6%
31.6%
0% 5% 10% 15% 20% 25% 30% 35%
Colombia
Egypt
Ghana
Jamaica
Burkina Faso
Ethiopia
Bangladesh
Zambia
Democratic Republic of Congo
Tanzania
Albania
Nepal
United Kingdom
Sudan
Kenya
Cameroon
Uganda
Pakistan
Nigeria
Percentage Contribution
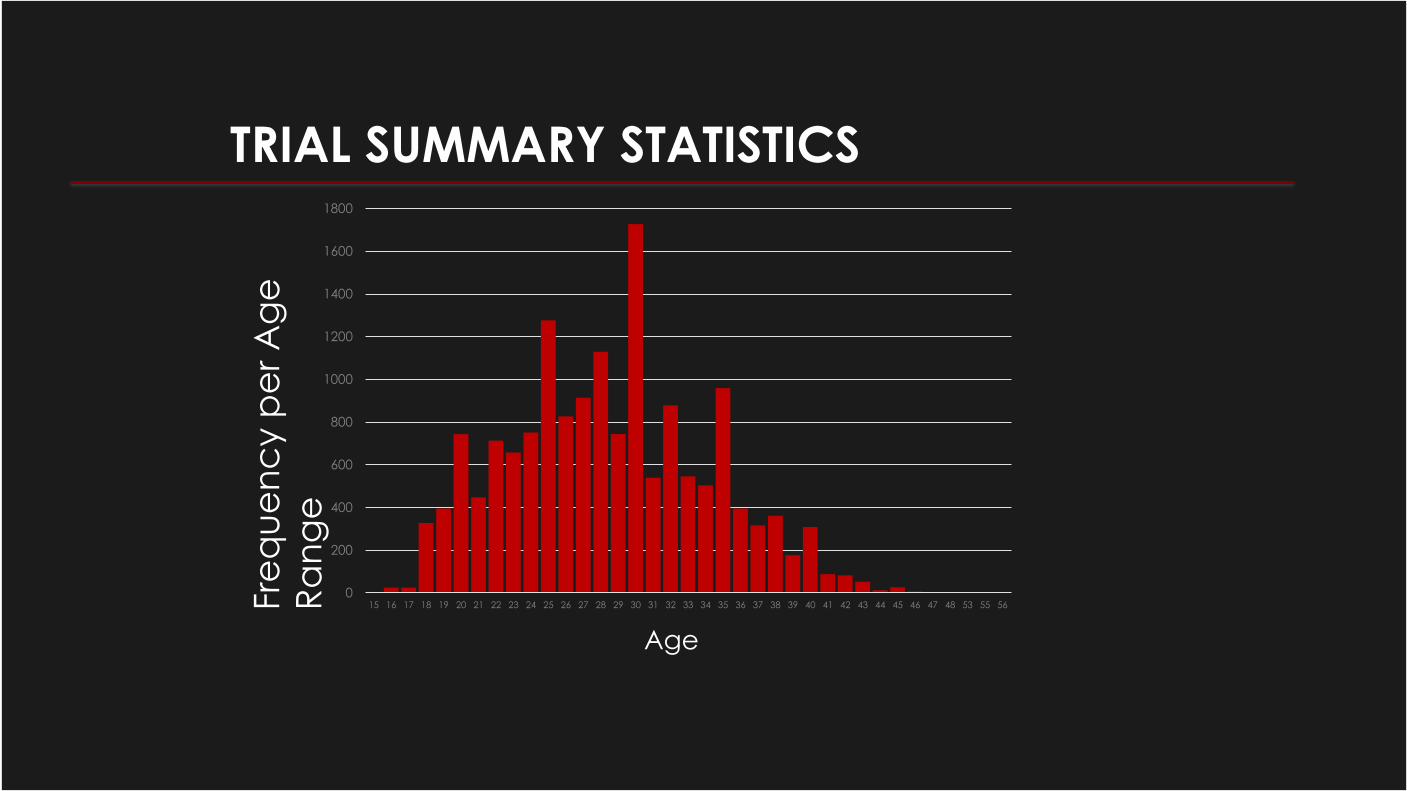
TRIAL SUMMARY STATISTICS
Fre
qu
en
cy p
er
Ag
e
Ra
ng
e
0
200
400
600
800
1000
1200
1400
1600
1800
15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 53 55 56
Age

0
10
20
30
40
50
60
70
80
90
100
Vaginal Caesarean section
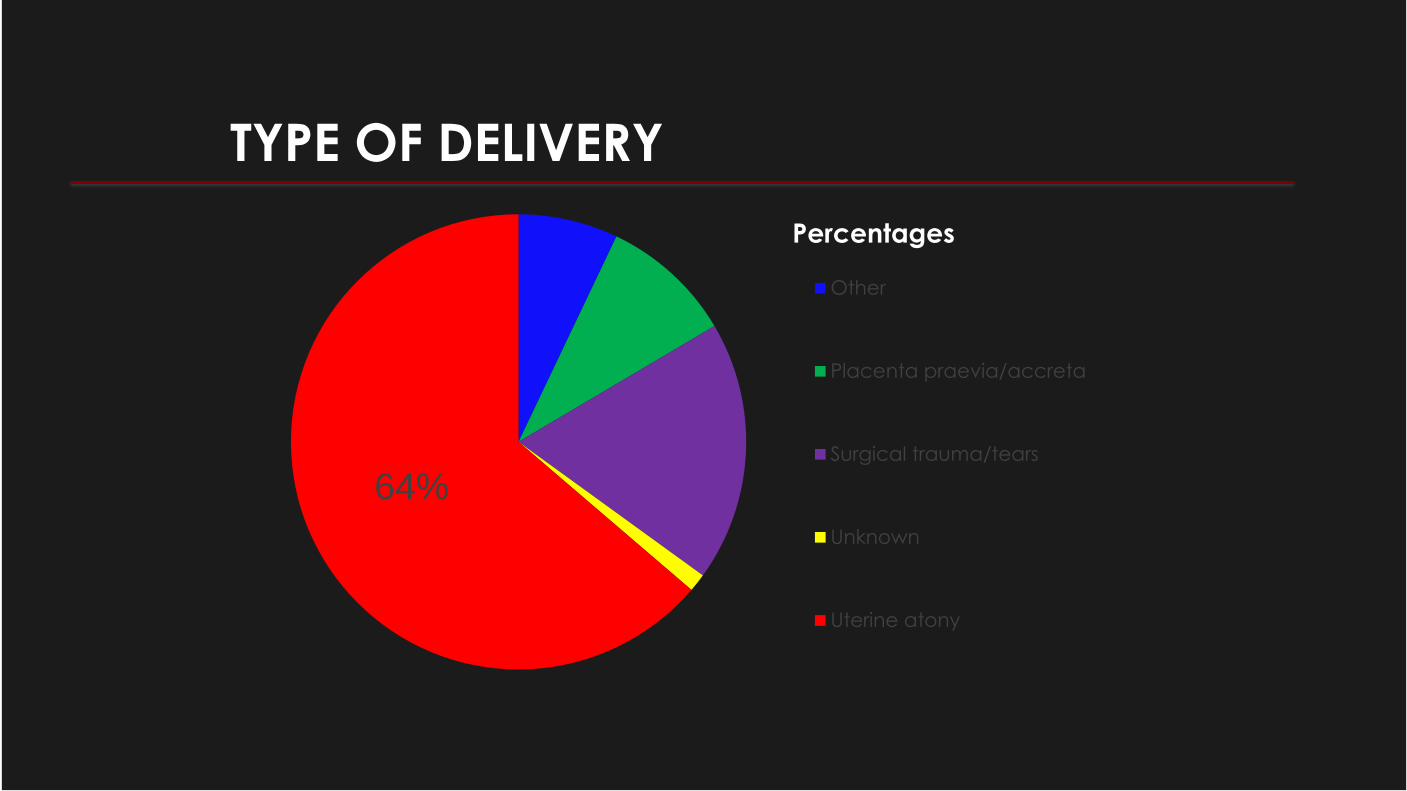
TYPE OF DELIVERY
TYPE OF DELIVERY
64%
Other
Placenta praevia/accreta
Surgical trauma/tears
Unknown
Uterine atony
Percentages

CAUSE OF DEATH
Bleeding 69
Pulmonary embolism 4
Other 27
Percentages
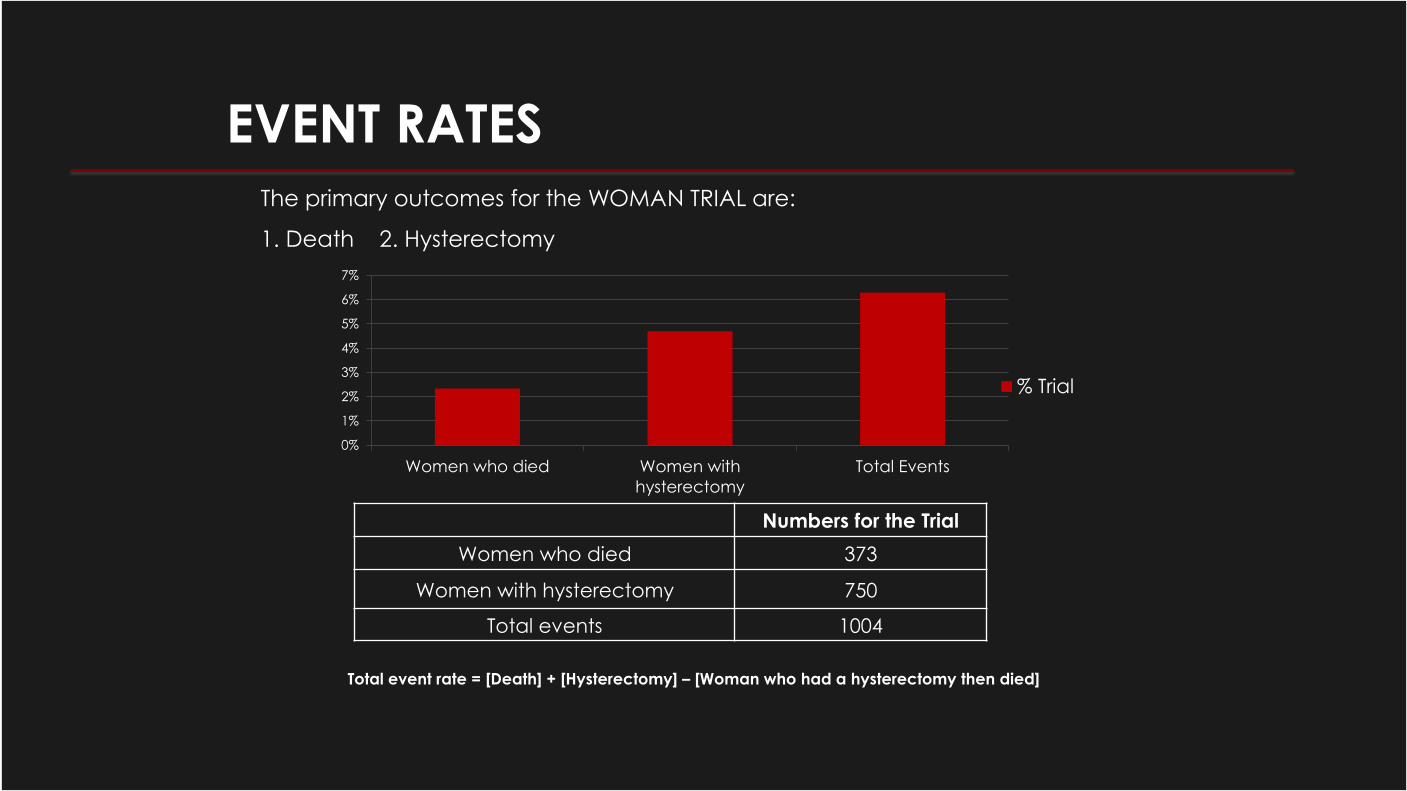
EVENT RATES
The primary outcomes for the WOMAN TRIAL are:
1. Death 2. Hysterectomy
Numbers for the Trial
Women who died 373
Women with hysterectomy 750
Total events 1004
Total event rate = [Death] + [Hysterectomy] – [Woman who had a hysterectomy then died]
0%
1%
2%
3%
4%
5%
6%
7%
Women who died Women with
hysterectomy
Total Events
% Trial

BLOOD LOSS DISTRIBUTION
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
5500
6000
6500
Blood Loss in m/l
Nu
mb
er
of
Pa
tie
nts
PROGRESS SUMMARY • The trial is completed with 20,000 women recruited from 202 sites in 20 countries.
• 88% women gave birth at the recruiting hospital.
• 96% received prophylactic uterotonics.
• Primary causes of PPH were:
• Uterine atony in 65% • Surgical/ trauma/tears in 19% • Placenta previa/accretes in 10% • Other causes 7% • Unknown cause 1%
• 2% died and 5% had a hysterectomy.
• Of those who had a hysterectomy, 0.8% died.
• The majority (71%) who died, delivered in the randomising hospital.

CONCLUSIONS
• Women continue to die from PPH
even when they deliver in hospital.
• More effective treatments are
needed to improve outcomes.
• The WOMAN trial will resolve the uncertainty regarding the
effectiveness and safety of TXA as
a treatment for PPH.

Make sure you know the result by registering
your interest at
www.womantrial.LSHTM.ac.uk
Clinical Trials Unit London School of Hygiene & Tropical Medicine
Keppel Street, London WC1E 7HT
Tel: +44(0)20 7299 4684 Fax: +44(0)20 7299 4663
Email: [email protected]
Follow the trial and join the discussion