transesophageal echocardiographic features of stenotic bioprosthetic valves in the mitral and...
TRANSCRIPT
Transesophageal Echocardiographic Features of Stenotic Bioprosthetic Valves in the Mitral and Tricuspid Valve Positions Mohsin Alam, MD, Howard S. Rosman, MD, Gerard0 A. Polanco, MD, Mita Sheth, MD, Remigio Garcia, MD, and Jeffrey B. Serwin, MD
A frequent long-term complication of bioprosthet- ic valves is spontaneous degeneration of the cusps with clinical features of valve regurgita-
tion or, less frequently, valve stenosis.’ Transthoracic echocardiography with cardiac Doppler is valuable in diagnosing stenosis of bioprosthetic valves.2 However, a major drawback of this approach is that all 3 bioprosthet- ic cusps are not consistently demonstrated owing to sound attenuation from the intervening chest wall and lungs, and to reverberation from the metal portion of the valve ring and stents. These problems are usually over- come by using a transesophageal ultrasound probe. We recently described our transesophageal echocardiograph- ic investigations in predominantly regurgitant biopros- thetic valves.3 Those patients are not included in this study. To the best of our knowledge, there are no reports on stenotic bioprostheses studied by transesophageal echocardiography.
Transesophageal (single-plane) and transthoracic echocardiography, and color flow Doppler studies were performed in 27 bioprosthetic mitral and tricus- pid valves implanted in 24 patients using standard equipment (Hewlett-Packard Sonar 500 and 1000) and techniques. 4 Nineteen patients with 21 biopros- theses (19 mitral and 2 tricuspid) were clinically nor- mal without cardiac symptoms or regurgitation mur- murs, whereas the remaining S patients with 5 mitral and 1 tricuspid prosthesis presented with symptoms of progressive dyspnea or congestive heart failure, or both. Diagnosis of valve stenosis was subsequently confirmed in these symptomatic patients by cardiac catheterization and angiography performed in 5 pa- tients and by valve replacement surgery in 6. None of the patients at presentation had active infective endo- carditis.
Ultrasound tests were performed on the same day in 20patients and the valve cusps were identifiedfrom the stents by their opening and closing motions. If the cusps had a dense, bright appearance, they were deemed to be thick. The cusps were measured at their maximal thickness site during systole. The valve cusp separation at its narrowest point was measured in early diastole by frame-by-frame analysis on video-
From the Division of Cardiovascular Medicine, K-14, Heart and Vascu- lar Institute, Henry Ford Hospital, 2799 West Grand Boulevard, De- troit, Michigan 48202. Manuscript received March 7, 1991; revised manuscript received and accepted April 29, 199 1.
tape. Transthoracic continuous-wave Doppler was used to obtain peak transmitral and tricuspid flow velocities. Mean valve gradient (Bernoulli equation) and valve area (pressure half-time method) were then calculated using an on-line computer. All valves were interrogated by color flow Doppler for the presence or absence of valve regurgitation and, once identified, it was semiquantitated by previously described tech- niques.’
Transthoracic echocardiography demonstrated limited segments of valve cusps in 15 cases, but failed to demonstrate any cusp in 6 other normal valves. Because all 3 cusps could not be visualized by this approach, the cusp separation could not be measured. Mean Doppler mitral valve gradient was 7 f 4 mm Hg and mean valve area was 2.1 f 0.7 cm2. Mild mitral regurgitation was demonstrated by color flow Doppler in 2 cases.
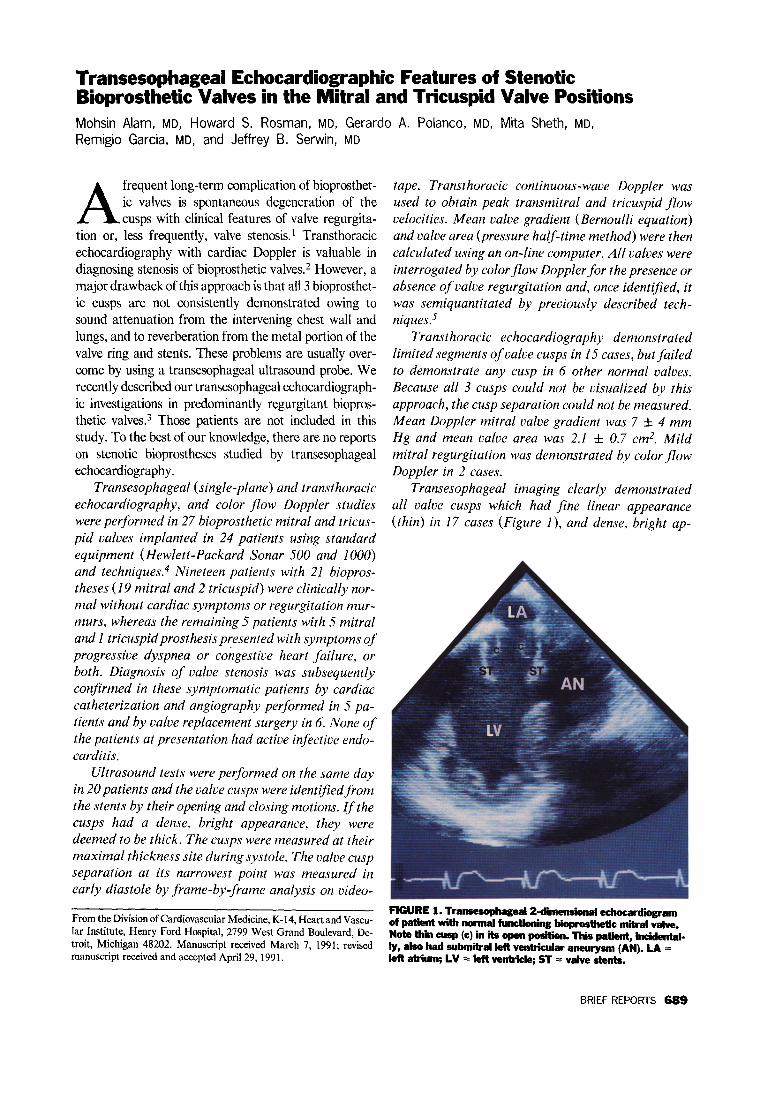
Transesophageal imaging clearly demonstrated all valve cusps which had fine linear appearance (thin) in 17 cases (Figure l), and dense, bright ap-
FIGURE 1. Transesophageal2-dimende11al echocardio of patlent With normal hnctioning bhprosbtic mitral Valve. Note thin cusp (c) in its open posith. This patient, hidental- ly, also had submitral left ventricular aneurysm (AN). LA = ,^y -A.2 _.-_ I .I - I-Y-.--. A-.-- -1 .- - *
BRIEF REPORTS 689

FIGURE 2. TranseqWgeal2L-dimensiod edmxadogram ofpatientwithsbnoticbbpwtheticmitralvalve.Notedense, bright Cusp (c) edmfs with redided opening &ring diastole. l.A=leftatrh~;LV=Wwntride;RA=&htabiun;RV= light-.
pearance (thick) in 4. Thin valves had a maximal cusp thickness ofO.5 to 2 mm and thick nonstenotic valves 2 to 3 mm. Diastolic cusp separation varied in clini- cally normal valves from 1 .O to 1.8 cm (mean I .4). Mild mitral regurgitation was demonstrated in 6 bio- prostheses.
Transthoracic echocardiography failed to demon- strate the valve cusps in 3 of 6 stenotic valves. In 3 other cases, dense and bright cusp echoes were demon- strated, suggesting thick or calcified valves, or both. Mean Doppler mitral/tricuspid valve gradient was 14 f 4 mm Hg and mean valve area 1.01 f 0.3 cm2 compared with 18 f 4 mm Hg and 0.8 f 0.2 cm2, respectively, by cardiac catheterization. Mild mitral/ tricuspid regurgitation was present in 2 patients by transthoracic color flow Doppler.
Transesophageal 2-dimensional echocardiogra- phy of the stenotic valves, however, clearly demon- strated all valve cusps with areas of thickening mea- suring 3 to 6 mm involving I or more cusps in all 6 cases (Figure 2). Furthermore, cusp mobility was se- verely restricted with cusp separation measuring 0.3 to 0.7 cm (mean 0.5). Color jlow Doppler demon- strated concomitant mild mitral/tricuspid valve re- gurgitation in 4 patients (Figure 3) and moderate mitral regurgitation in 1.
Diagnosis of bioprosthetic mitral and tricuspid valve stenoses may be difficult. The cardiac auscultatory find- ings are not very specific because an opening sound and diastolic rumble can be heard in normal functioning mi- tral and tricuspid bioprostheses. Consequently, these pa-
~GURE 3. Tranwwphfgeal &. flow bppk3r of patient in Figve 2 with stenotic v mitral valve (BMV). Note narrow mltml regurgitant jet (MR) occupying <20% of ledt ab+alchamber.LA=leRatriun;LV=leftvedride.
tients are often undiagnosed until they develop decom- pensated congestive heart failure.
Transesophageal 2-dimensional echocardiography was excellent in demonstrating the presence or absence of thii or thick valve cusps with normal or restricted cusp opening. The features of thickened and calcified valve cusps were subsequently confirmed during surgery in all stenotic bioprostheses. In clinically normal functioning valves, the mere presence of a thick cusp by itself does not indicate severe stenosis and the need for valve replace- ment surgery. However, in the absence of endocarditis and thrombus formation, a thick valve may represent subclinical degeneration.2 Patients with severe valve ste- nosis can be distinguished from these patients by cusp thickness >3 mm and cusp opening <0.7 cm with transe- sophageal2-dimensional echocardiography, and by valve area < 1 .O cm2 with cardiac Doppler and catheterization. In conclusion, transesophageal echocardiography com- plements transthoracic imaging in diagnosing biopros- thetic mitral and tricuspid valve stenoses.
1. Magilligan DJ Jr, Lewis JW Jr, Stein PD, Alam M. The porcine bioprosthetic heart valve: experience at 15 years. Ann Thorac Surg 1989;48:324-330. 2. Alam M, Rosman HS, Lakier JB, Kemp S, Khaja F, Hautamaki K, Magilligan DJ Jr, Stein PD. Doppler and echocardiographic features of normal and dysfunc- tioning bioprosthetic valves. J Am CON Cardiol 1987;10:85 l-858. 3. Alam M, Serwin JB, Rosman HS, Polanco GA, Sun I, Silverman NA. Transe- sophageal echocardiographic features of normal and dysfunctioning bioprosthetic valves. Am Heart J 1991;121:1149-1155. 4. Stewart JB, Khandheria BK, Oh JK, Abel MD, Hughes RW Jr, Edwards WD, Nichol BA, Freeman WK, Tajik AJ. Transesophageal echocardiography: tech- nique, anatomic correlations, implementation and clinical applications. Muyo Clin Pmc 1988;63:649-680. 5. Helmcke F, Nanda NC, Hsiung MC, Soto B, Adley CK, Goyal RG, Gatewood RP. Color Doppler assessment of mitral regurgitation with orthogonal planes. Circulation 1987;75:175-183.
690 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 68 SEPTEMBER 1, 1991