transitory bundle branch block
TRANSCRIPT
Acta Xedica Scandinarica. Vol. CLVI, fasc. 111, 1956.
From .the Medical Department, Central Hospital (Head: P. Wising, M. D.), Vaster&, Sweden.
Transitory Bundle Branch Block.
BY NILS BERGQUIST and JAN HA-N.
(Submitted for publication August 20, 1956.)
Extension of the QRS complex of the electrocardiogram to 0 . 1 2 seconds or more has long been considered to indicate organic damage to a branch of the bundle of His. This hypothesis is supported by the fact that the electrocardiograms in histologically demonstrable complete conduction block in a branch invariably have shown a lengthened QRS interval - bundle branch block (9). Further, bundle branch block almost always is associated with diseases which frequently cause pathoanatomic changes in the myocardium. Coronary artery disease is the most common of such conditions, but rheumatic fever, diphtheria, etc. may also be aetiologic factors. Bundle branch block as a rule is irreversible. Sometimes, however, restitution occurs. Occasionally the QRS complex fluctuates between normal and branch block type.
The present report concerns two patients with transient bundle branch block, in whom the altered electrocardiographic pattern was the sole objective evidence of cardiac disorder. Extension of the QRS waves could be repeatedly induced and eliminated by certain manoeuvres.
C a s e I : (1084/1954) N. k, a greaser, born in 1910, had previously been in good health. There was thus no history of rheumatic fever. diphtheria of other disease of significance for the heart. For about a year he had complained of a pricking)) sensation in the precordium unrelated to effort, meals or temperature.
Between these attacks, which generally lasted for about two hours, he had had stabbing precordial pain radiating to the left arm and persisting for some minutes. These symptoms were combined with a sensation of anxiety. Some weeks before admission to hospital he had complained of spells of dizziness with palpitation. The electrocardiogram taken in the office of the patient’s physician showed extended QRS complex as in bundle branch block.
232 NILS BERGQUIST AND JAN H ~ L L B N .
The patient was hospitalized on September 29, 1954. Examination revealed a Eomewhat adipose man with no signs of cardiac decompensation. Physical exam- ination of the heart showed nothing abnormal. The blood pressure was 150/95 mm Hg, the ESR was 15 mm in one hour and the antistreptolysin titre 125 I. U. The roentgenographic outline of the heart was normal - volume 330 ml per m* of body surface. Tests with a cycle ergometer and a work load of 600 kgm per minute produced a pulse rate of 165 beats per minute after four minutes. Repeated electrocardiographic examinations showed sometimes normal QRS waves sometimes slower excursions of bundle branch block type (see below). Because of his anxiety and nervousness the patient was examined by a psychiatrist, who classified him as a hypothymic hypochondriac. After two weeks in hospital he was discharged for rest a t home.
On out-patient examination one month later the electrocardiogram was complete- ly normal. The patient felt better and resumed his moderately strenuous occupa- tion.
He was rehospitalized after a further year. For a month previously he had been nervous had had brief attacks of acute anxiety with pain in the left sub- mamillary region and mild gastric discomfort of fermentative dyspeptic type. An electrocardiogram taken during an attack of dizziness and chest pain showed bundle branch block. The general condition was unchanged since the first hospital- ization - blood pressure 135/80 mm Hg, ESR 12 mm and cardiac roentgenogram normal. As before, the QRS complex vacillated between normal and bundle branch block. The patient’s symptoms gradually improved and he was discharged as f i t for work.
Electrocardiographic observations.
Normal sinus rhythm, upright P waves and a P-Q interval of 0.15 to 0.16 sec. were registered in all of the many electrocardiograms taken. The QRS complex, S-T segments and T waves varied. Long sections of the electrocardiogram could show a QRS wave of 0.09 sec., isoelectric S-T and upright T waves in all leads, while throughout other sections the QRS excursion lasted 0.14 sec., the S-T intervals were depressed in leads I and I1 and slightly elevated in lead 111, and TI and T, were directed downwards.
To elucidate the cause of this remarkable alternation between QRS of normal and branch block type, various manoeuvres were performed. The change back and forth wae thereby frequently demonstrated.
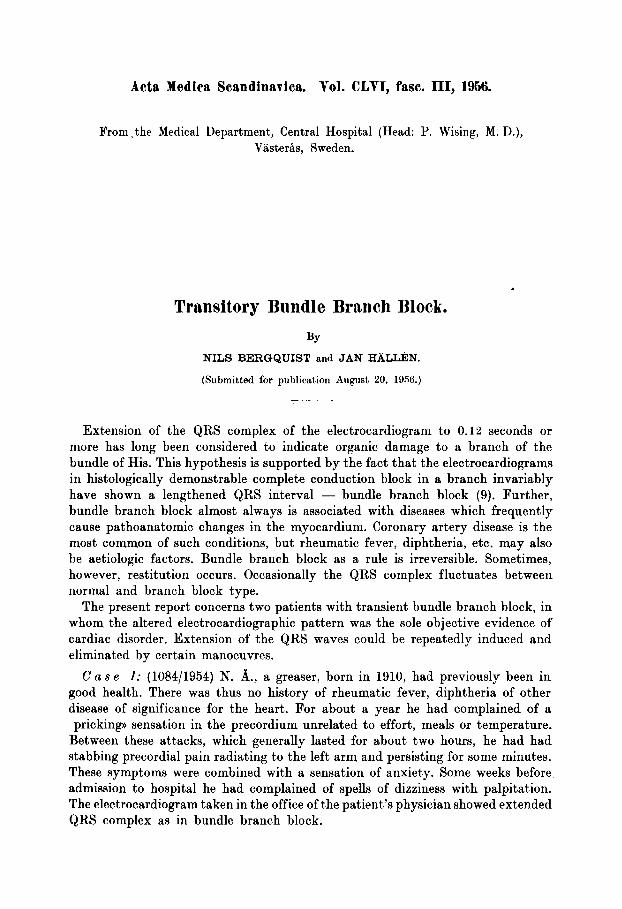
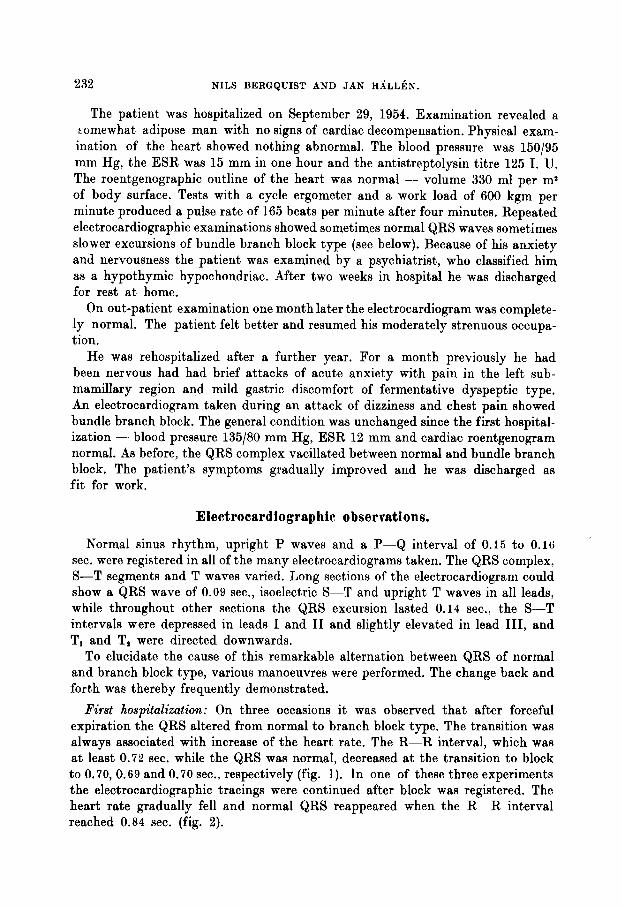
First hospitalization: On three occasions it was observed that after forceful expiration the QRS altered from normal to branch block type. The transition was always associated with increase of the heart rate. The R-R interval, which was a t least 0 .72 sec. while the QRS was normal, decreased a t the transition to block to 0.70, 0.69 and 0.70 sec., respectively (fig. 1). In one of these three experiments the electrocardiographic tracings were continued after block was registered. The heart rate gradually fell and normal QRS reappeared when the R-R interval reached 0.84 sec. (fig. 2).
I
00
01
Q,
Ls
9
00 i P
E F k 2
1 %
R C
z 1 0 FJ
+4 m
C z
g ff:
T
7 n p
* 2 fr
om n
orm
al Q
RS
to b
undl
e br
anch
blo
ck a
t an
R-R
in
terv
al o
f 0.
69 s
ec.
Fig.
2 C
ase
1: F
ollo
win
g in
duct
ion
of b
ranc
h bl
ock
by h
oldi
ng t
he b
reat
h th
e pa
tien
t w
aa a
llow
ed t
o br
eath
e na
tura
lly.
The
tra
cing
s no
rmal
ized
at
R-R
0.84
see
.
234 XILS BERGQUIST AND JAN H A L L ~ N .
Change from the recumbent to the upright position also induced transition from normal QRS to block. Here, too, the phenomenon was associated with increased heart rate and appeared when the R-R interval had fallen to 0.70-0.71 sec. This experiment was performed twice with the same results.
Out-patient examination: One and four months after discharge from hospital, when the QRS complex was normal, attempts were made to induce branch block by changing the patient’s position from recumbent to standing. Despite considerable elevation of the heart rate and decrease of the R-R interval to 0.55-0.56 sec., the experiment was unsuccessful.
Second hospitalization: On two occasions the patient was instructed to hold his breath while recumbent. This resulted in transition from normal QRS t o branch block, also now associated with accelerated heart rate, when the R-R interval had decreased to 0.71 sec. As registration continued, the heart rate gradually diminished and a t R-R intervals of 0.87 and 0.88, respectively, the QRS returned to normal.
As in the first hospitalization, branch block also appeared when the patient assumed the upright position. By carotid sinus pressure it was possible on three occasions to eliminate the block while the patient was still standing. As soon as the pressure was released the tracings again showed block. The R-R interval was 0 . 6 8 4 . 7 1 a t the transition to block and 0 . 8 0 4 . 8 2 a t its reversal.
Thus bundle branch block invariably was associated with acceleration of the heart rate and normalization of the QRS with falling heart rate.
Summary: A 46-year-old man with uncharacteristic spells of dizziness and pre- cordial pain which was not related to effort, had no clinical or roentgenographic signs of cardiovascular disease. The electrocardiogram showed transient bundle branch block which could be induced by raising the pulse rate. The phenomenon was observed during two periods of hospitalization approximately one year apart. In the interval the patient was symptom-free and branch block could not be induced by the methods which were effective during hospitalization, although the heart rate was considerably more accelerated than on the occasions when branch block was registered.
C a s e 2: (1915/1954) S. S., born in 1914, was a cement worker. Apart from the symptoms reported below the anamnesis was unremarkable, with none of the usual causes of permanent cardiac damage such as rheumatic fever or diphtheria. For the past 12 or 13 years he had felt occasional pairing of the heart beat, especially in association with nervousness. For 7 years he had had attacks of anxiety accom- panied by pain in the left side of the chest without relation to effort. At times he had palpitation, even a t rest. As the pain was becoming increasingly frequent he was referred for hospital treatment. The electrocardiogram prior to admission showed extended QRS complex of bundle branch block type.
Examination on October 10, 1954 revealed a man of slender build without signs of cardiac decompensation. Physical examination of the heart disclosed nothing of note. The blood pressure ranged from 160/100 to 145/80 mm Hg and the ESR
TRANSITORY BUNDLE BRANCH BLOCK. 235
from 3 to 7 mm in one hour. The antistreptolysin titre was 200 I. U. The roentgeno- graphic configuration of the heart was normal - volume 280 ml per ma of body surface. Repeated electrocardiograms showed fluctuation between normal QRS complex and stretching of the type in left branch block (see below). In an exercise tolerance test the patient felt unable to continue longer than one minute with a load of 900 kgm per minute although the respiration rate had not reached 30 per minute and the pulse was less than 160 beats per minute. He was discharged and attended the out-patient department for a short time before resuming full employ- ment.
One year later he was hospitalized for a month under the diagnosis of psychogenic depression. He was worried and uneasy on account of his heart. After electroshock and insulin therapy his mental condition improved.
On out-patient examination after a further year the patient was subjectively better. His heavy work with cement did not give rise to cardiac distress. He thought that the cardiac symptoms were influenced by his nervous condition. Bundle branch block was present also on this occasion, and was reversible by the measures described below.
Electrocardiographic observations.
The many electrocardiograms all showed regular sinus rhythm, upright P waves and P-Q interval ranging from 0.12 to 0.15 sec. In some sections of the tracings the cardiac axis was normally placed, with QRS complex measuring 0.07 sec., isoelectric S-T segment and upright T waves in all leads. In other sections the QRS complex was 0.12 sec., there was left cardiac deviation and the S-T segment was slightly depressed in lead I and slightly elevated in lead 111. Here, too, all the T waves were upright.
By various manoeuvres it was possible to produce and register transition between the two above described variations.
First hospitalization: On one occasion QRS of branch block type was registered with the patient standing. The heart rate was high and the R-R interval did not exceed 0.50 sec. After ten minutes’ rest in the recumbent position the QRS complex returned to normal and the smallest R-R interval was now 0 . 6 4 sec. Attempts to produce branch block in normal tracings by means of adrenalin and atropine were unsuccessful; the smallest R-R intervals registered were 0.6 2 and 0.76 sec., respectively. Further studies under various conditions showed that the R-R interval in branch block ranged from 0.50 to 0.64 sec., and in normal QRS complex from 0.76 to 0.58 sec.
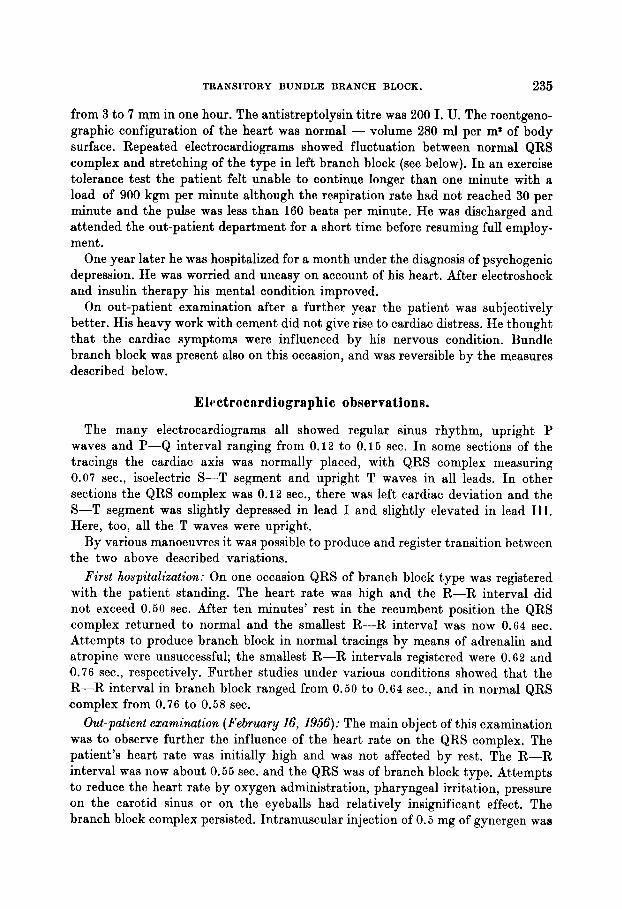
Out-patient examination (February 16, 1956): The main object of this examination was to observe further the influence of the heart rate on the QRS complex. The patient’s heart rate was initially high and was not affected by rest. The R-R interval was now about 0.55 sec. and the QRS was of branch block type. Attempts to reduce the heart rate by oxygen administration, pharyngeal irritation, pressure on the carotid sinus or on the eyeballs had relatively insignificant effect. The branch block complex persisted. Intramuscular injection of 0.5 mg of gynergen waa
236 NILS BERGQUIST AND JAN HALLBN.
TRANSITORY BUNDLE BRANCH BLOCK. 237
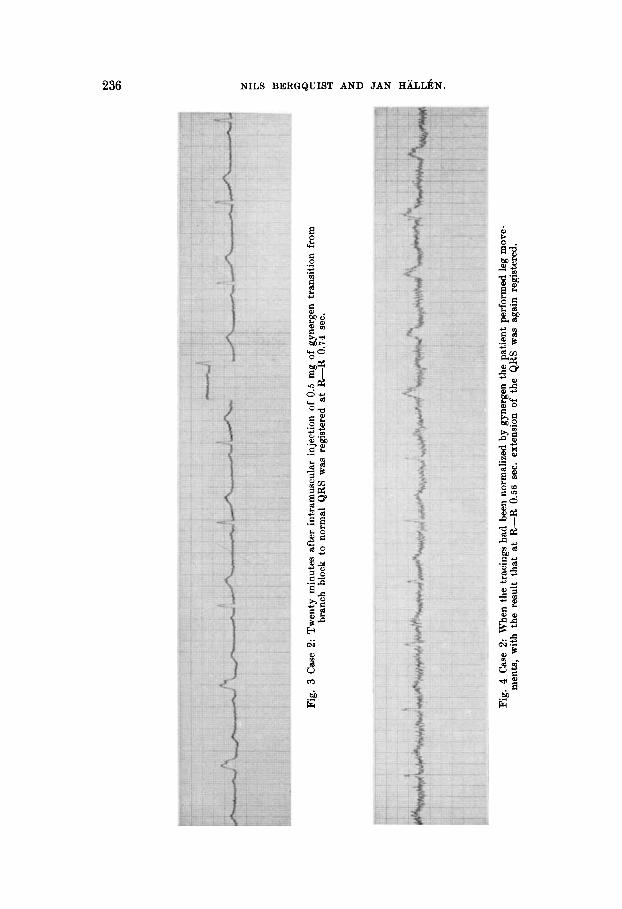
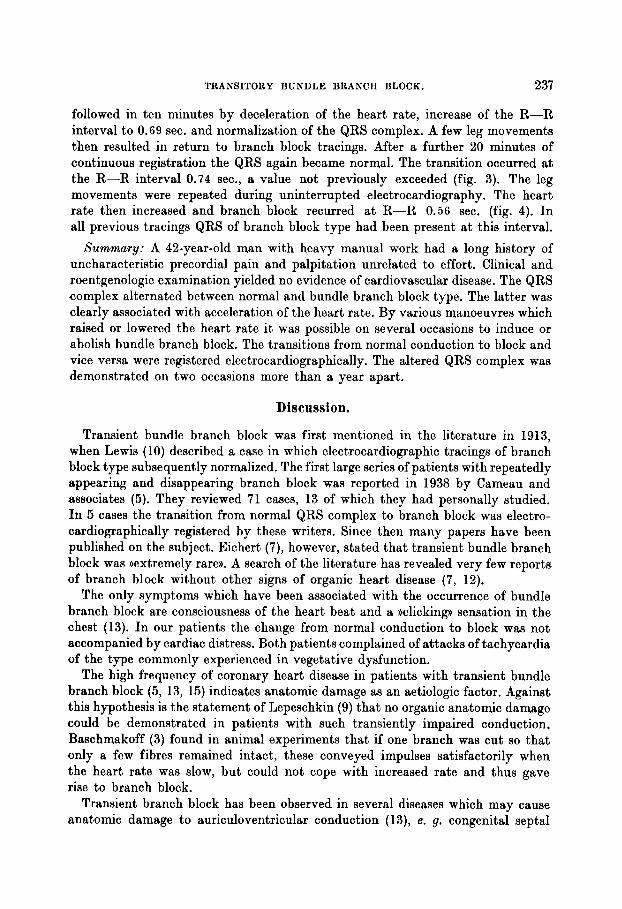
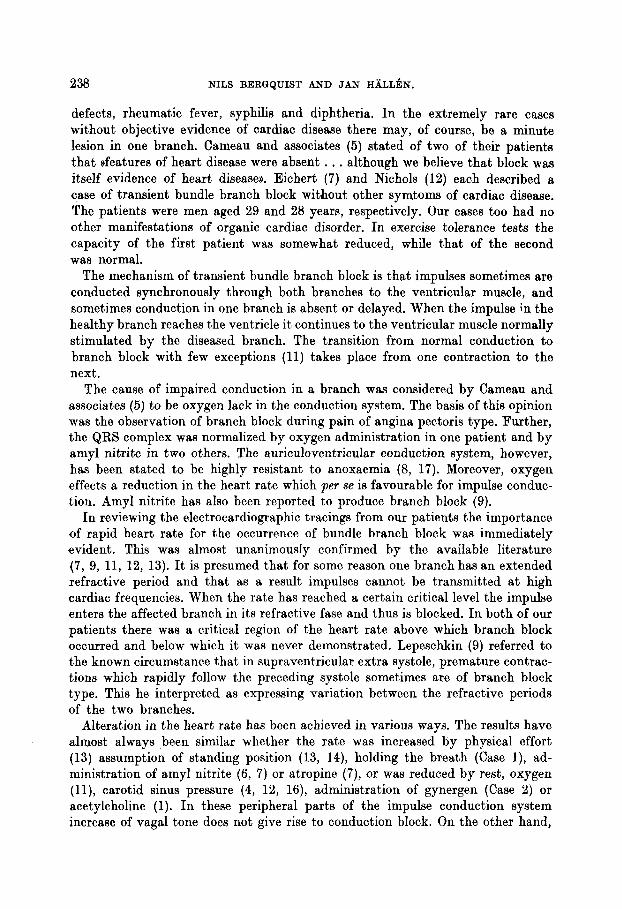
followed in ten minutes by deceleration of the heart rate, increase of the R-R interval to 0.69 sec. and normalization of the QRS complex. A few leg movements then resulted in return to branch block tracings. After a further 20 minutes of continuous registration the QRS again became normal. The transition occurred a t the R-R interval 0.74 sec., a value not previously exceeded (fig. 3). The leg movements were repeated during uninterrupted electrocardiography. The heart rate then increased and branch block recurred a t R-R 0.56 sec. (fig. 4). In all previous tracings QRS of branch block type had been present a t this interval.
Summary: A 42-year-old man with heavy manual work had a long history of uncharacteristic precordial pain and palpitation unrelated to effort. Clinical and roentgenologic examination yielded no evidence of cardiovascular disease. The QRS complex alternated between normal and bundle branch block type. The latter was clearly associated with acceleration of the heart rate. By various manoeuvres which raised or lowered the heart rate i t was possible on several occasions to induce or abolish bundle branch block. The transitions from normal conduction to block and vice versa were registered electrocardiographically. The altered QRS complex was demonstrated on two occasions more than a year apart.
Discussion.
Transient bundle branch block was first mentioned in the literature in 1913, when Lewis (10) described a case in which electrocardiographic tracings of branch block type subsequently normalized. The first large series of patients with repeatedly appearing and disappearing branch block was reported in 1938 by Cameau and associates (5). They reviewed 71 cases, 13 of which they had personally studied. I n 5 cases the transition from normal QRS complex to branch block was electro- cardiographically registered by these writers. Since then many papers have been published on the subject. Eichert (7), however, stated that transient bundle branch block was ))extremely rare)). A search of the literature has revealed very few reports of branch block without other signs of organic heart disease (7, 12).
The only symptoms which have been associated with the occurrence of bundle branch block are consciousness of the heart beat and a ))clicking)) sensation in the chest (13). In our patients the change from normal conduction to block was not accompanied by cardiac distress. Both patients complained of attacks of tachycardia of the type commonly experienced in vegetative dysfunction.
The high frequency of coronary heart disease in patients with transient bundle branch block (5, 13, 15) indicates anatomic damage as an aetiologic factor. Against this hypothesis is the statement of Lepeschkin (9) that no organic anatomic damage could be demonstrated in patients with such transiently impaired conduction. Baschmakoff (3) found in animal experiments that if one branch was cut so that only a few fibres remained intact, these conveyed impulses satisfactorily when the heart rate was slow, but could not cope with increased rate and thus gave rise to branch block.
Transient branch block has been observed in several diseases which may cause anatomic damage to auriculoventricular conduction (13)) e. g. congenital septa1
238 NILS BERGQUIST AND JAN H A L L ~ N .
defects, rheumatic fever, syphilis and diphtheria. In the extremely rare cases without objective evidence of cardiac disease there may, of course, be a minute lesion in one branch. Cameau and associates ( 5 ) stated of two of their patients that ,features of heart disease were absent . . . although we believe that block was itself evidence of heart disease)). Eichert (7) and Nichols (12) each described a case of transient bundle branch block without other symtoms of cardiac disease. The patients were men aged 29 and 28 years, respectively. Our cases too had no other manifestations of organic cardiac disorder. In exercise tolerance tests the capacity of the first patient was somewhat reduced, while that of the second was normal.
The mechanism of transient bundle branch block is that impulses sometimes are conducted synchronously through both branches to the ventricular muscle, and sometimes conduction in one branch is absent or delayed. When the impulse in the healthy branch reaches the ventricle i t continues to the ventricular muscle normally stimulated by the diseased branch. The transition from normal conduction to branch block with few exceptions (11) takes place from one contraction to the next.
The cause of impaired conduction in a branch was considered by Cameau and associatea (5) to be oxygen lack in the conduction system. The basis of this opinion was the observation of branch block during pain of angina pectoris type. Further, the QRS complex was normalized by oxygen administration in one patient and by amyl nitrite in two others. The auriculoventricular conduction system, however, has been stated to be highly resistant to anoxaemia (8, 17). Moreover, oxygen effects a reduction in the heart rate which per se is favourable for impulse conduc- tion. Amy1 nitrite has also been reported to produce branch block (9).
In reviewing the electrocardiographic tracings from our patients the importance of rapid heart rate for the occurrence of bundle branch block was immediately evident. This was almost unanimously confirmed by the available literature (7, 9, 11, 12, 13). It is presumed that for some reason one branch has an extended refractive period and that as a result impulses cannot be transmitted a t high cardiac frequencies. When the rate has reached a certain critical level the impulse enters the affected branch in its refractive fase and thus is blocked. In both of our patients there was a critical region of the heart rate above which branch block occurred and below which i t was never demonstrated. Lepeschkin (9) referred to the known circumstance that in supraventricular extra systole, premature contrac- tions which rapidly follow the preceding systole sometimes are of branch block type. This he interpreted as expressing variation between the refractive periods of the two branches.
Alteration in the heart rate has been achieved in various ways. The results have almost always been similar whether the rate was increased by physical effort (13) assumption of standing position (13, 14), holding the breath (Case l), ad- ministration of amyl nitrite (6, 7) or atropine (7), or was reduced by rest, oxygen (l l) , carotid sinus pressure (4, 12, 16), administration of gynergen (Case 2) or acetylcholine (1). In these peripheral parts of the impulse conduction system increase of vagal tone does not give rise to conduction block. On the other hand,
TRANSITORY BUNDLE BRANCH BLOCK. 239
the fall in the heart rate caused by vagal stimulation provides an acceptable explanation of the restoration of normal conduction.
Case 1 presented some aspects of aetiologic interest for transient bundle branch block. During two separate periods transient block could readily be induced by increasing the heart rate. At these times the patient had certain indefinite symp- toms. I n the interval, when the symptoms were absent, branch block could not be elicited. It is scarcely conceivable that this patient on two different occasions should have sustained similar organic damage to one branch, and that the damage should have disappeared during the intervening time. It would instead seem probable that a difference existed in the refractive periods of the two branches, a difference which periodically - due e. g. to altered biochemical circumstances in the bundle musculature - was adequate to provide conditions for transient bundle branch block.
S u mmnry.
Two cases of transient bundle branch block are described. The patients were middle-aged males without other objective evidence of cardiac disorder, but with symptoms of cardioneurotic type. In both patients bundle branch block could be induced and abolished by various manoeuvres which respectively accelerated and decelerated the heart rate. The transition to and from block was registered electrocardiographically. In one patient transient block was registered during two periods more than a year apart. In the interval block could not be induced, despite a heart rate considerably higher than that otherwise required for the appearance of block. The second patient was also studied twice, with an interval of 16 months. Fluctuations between normal conduction and block were readily induced on both occasions.
References.
1. Bognaresi, G.: Cuore e Circolog. 18: 65, 1934. - 2. Baker, B. M.: Arch. Int. Med. 45: 814, 1930. - 3. Baschmakoff, W. I.: Arch f. d. ges. Physiol. 224: 167, 1930. - 4. Bohnengel, C.: Am. Heart J. 16: 587, 1938. - 5. Cameau, W. I., Hamilton, J., White, P.: Am. Heart J. 15: 216, 1938. - 6. Cohn, A., Macleod, A.: Am. Heart J. 17: 305, 1939. - 7. Eichert, H.: Am. Heart J. 28: 551, 1944. - 8. Hill, G. W.: J. Physiol. 81: 70, 1934. - 9. Lepeschkin, E.: Modern Electrocardiografi. 1951. - 10. Lewis, T.: Brit. Med. J. 1: 484, 1913. - 11. Miller, H., Fulton, F. T.: New England J. Med. 221: 292, 1939. - 12. Nichols, E.: Am. int. med. 30: 196, 1949. - 13. Vesell, H.: Am. J. M. Sc. 202: 198, 1941. - 14. Wendkos, M. H.: Progr. sc. sess. Am. Heart Assoc. 22: 55, 1949. - 15. White, P. D.: Heart Diseases, New York, 1940, The Macmillan Company p. 940. - 16. Wilburne, M., Langedorf, R.: J. Lab. & Clin. Med. 28: 303, 1943. - 17. Yater, W., Cornell, V. H., Clayton, T.: Arch. Int. Med. 57: 132, 1936.