translating science to policytranslating research into policy and action translating community-based...
TRANSCRIPT
Translating Science to PolicyProtecting Children’s Environmental HealthA Conference Held on March 30, 2009
Hosted by The Columbia Center for Children’s Environmental Health in collaboration with WE ACT for Environmental Justice
COLUMBIA CENTERFOR CHILDREN’SENVIRONMENTALHEALTH
MAILMAN SCHOOL OF PUBLIC HEALTHColumbia University
Columbia Center for Children’s Environmental Health (CCCEH)
The Columbia Center for Children’s Environmental Health—part of the MailmanSchool of Public Health at Columbia University—is a leading research organizationdedicated to understanding and preventing environmentally related disease in chil-dren. Founded in 1998, the Center conducts research in New York City, including astudy of mothers and children in Northern Manhattan and South Bronx, a WorldTrade Center Study, as well as cohort studies in Krakow, Poland, and Chongqing,China. Its mission is to improve the respiratory health and cognitive development ofchildren and to reduce their cancer risk by identifying environmental toxicants andconditions related to poverty that increase their risk of disease. In NYC, the Centercollaborates with residents and partner organizations in Washington Heights, Harlemand the South Bronx to share research findings with the local communities in waysthat are meaningful and usable in daily life. CCCEH is one of several National Centersfunded by the NIEHS and EPA and one of three Disease Investigation throughSpecialized Clinically-Oriented Ventures In Environmental Research (DISCOVER)Centers funded by the NIEHS. www.ccceh.org.
WE ACT for Environmental Justice
Founded in 1988, WE ACT for Environmental Justice (West Harlem EnvironmentalAction, Inc.) was New York’s first environmental justice organization created to buildcommunity power to improve environmental health, policy and protection in com-munities of color. WE ACT is a nationally recognized organization in the field of com-munity-based participatory research in partnership with the Mailman School of PublicHealth at Columbia University. Based in Northern Manhattan, WE ACT advances itsmission through research, public education, advocacy, organizing, governmentaccountability, litigation, legislative affairs, and sustainable economic development.WE ACT works for environmental and social justice on issues of land use, waterfrontdevelopment, brownfields redevelopment, transportation and air pollution, openspace and environmental health. In its first organizing campaign, WE ACT won a $1.1million settlement of its lawsuit against the City regarding the North River sewagetreatment plant in late December 1993, as well as a monitoring role with the NaturalResources Defense Council in the enforcement of the city-state consent agreement ona five-year plan to fix the North River Plant. www.weact.org.
Mailman School of Public Health
The only accredited school of public health in New York City and among the first inthe nation, Columbia University Mailman School of Public Health pursues an agendaof research, education, and service to address the critical and complex public healthissues affecting millions of people locally and globally. The Mailman School is therecipient of some of the largest government and private grants in ColumbiaUniversity’s history. Its more than 1,000 graduate students pursue master’s and doc-toral degrees, and the School’s 300 multi-disciplinary faculty members work in morethan 100 countries around the world, addressing such issues as infectious and chronicdiseases, health promotion and disease prevention, environmental health, maternaland child health, health over the life course, health policy, and public health pre-paredness. www.mailman.columbia.edu.

Translating Science to PolicyProtecting Children’s Environmental HealthA Conference Held on March 30, 2009
Hosted by The Columbia Center for Children’s Environmental Health in collaboration with WE ACT for Environmental Justice
The conference was sponsored by: The John Merck Fund, The New York Community Trust, Passport Foundation, The National Institute of Environmental Health Sciences, and the US Environmental Protection Agency.
The Center’s work has been made possible by joint funding from:
The National Institute of Environmental Health Sciences US Environmental Protection Agency National Cancer InstituteIrving Institute for Clinical and Translational Research
Private Foundations, including:The Atlantic Foundation, The Bauman Foundation, Beldon Fund, Blanchette Hooker Rockefeller Fund, Educational Foundation of America, Energy Foundation, Gladys & Roland Harriman Foundation, Johnson Family Foundation, The John Merck Fund, Alida R. Messinger Charitable Trust, The John & Wendy Neu Family Foundation, The New York Community Trust, The New York Times Company Foundation,Passport Foundation, Rockefeller Brothers Fund, Rockefeller Financial Services, Schmidt Family Foundation, September 11 Children’s Fund, V. Kann Rasmussen Foundation.
And Individual Donors.

Table of Contents
Conference Overview
Executive Summary ....................................................................................................................................................................................4
Children’s Environmental Health: A Decade of Research ..............................................................................................................6Frederica Perera, DrPHProfessor and Director, Columbia Center for Children's Environmental Health and Disease Investigationthrough Specialized Clinically-Oriented Ventures In Environmental Research (DISCOVER) Center, Mailman School of Public Health, Columbia University
Partnership in Public Health Research: A Decade of Activism......................................................................................................7Peggy ShepardExecutive Director, WE ACT for Environmental Justice
Conference Highlights: Keynote Speakers
Protecting Children’s Environmental Health .....................................................................................................................................8Lisa P. Jackson, Administrator, US Environmental Protection Agency
The Promise: Children’s Environmental Health ...............................................................................................................................11Linda S. Birnbaum, PhD, DABT, ATSDirector, National Institute of Environmental Health Sciences
Conference Highlights: Presentations*
Case Study 1: Air Pollution and Climate Change
Impact of Prenatal Exposure to Air Pollution from Traffic and Other Fossil Fuel Combustion Sources on Children’s Health and Development ..........................................................................15Frederica Perera, DrPHProfessor and Director, Columbia Center for Children's Environmental Health and Disease Investigation through Specialized Clinically-Oriented Ventures In Environmental Research (DISCOVER) Center, Mailman School of Public Health, Columbia University
Fossil Fuels, Climate Change and Children’s Health: Impacts and Opportunities..........................................................17Patrick Kinney, ScDAssociate Professor and Director, Program in Climate and Health, Mailman School of Public Health, Columbia University
Case Study 2: Pesticides and Integrated Pest Management
Prenatal Chlorpyrifos Exposure and Neurodevelopment: How Exposure to a Common Pesticide Can Damage the Developing Brain.....................................................................19Virginia Rauh, ScDProfessor and Deputy Director, Columbia Center for Children’s Environmental Health, Mailman School of Public Health, Columbia University
A Collaborative Effort to Evaluate the Impact of Integrated Pest Management in New York City Public Housing ...........................................................................................21Daniel Kass, MSPHAssistant Commissioner, Environmental Surveillance and Policy, New York City Department of Health and Mental Hygiene
Translating Science to Policy: Protecting Children’s Environmental Health
2
Case Study 3: Endocrine Disruptors
The Health Effects of Endocrine Disruptors on the Growth and Development of Children ...................................... 24Sandra Steingraber, PhDScholar in Residence, Division of Interdisciplinary and International Studies, Ithaca College
Translating Research Into Policy and Action
Translating Community-Based Research into Policy and Public Health Action.............................................................27Peggy ShepardExecutive Director, WE ACT for Environmental Justice
Conference Highlights: Roundtable Discussions*
Panel 1: Addressing Urban Air Pollution and Climate ChangeBrian Lehrer, MPH, ModeratorHost, WNYC and National Public Radio
Panel 1 Policy Recommendations ...................................................................................................................................................30
Rachel Miller MD, FAAAAI, Associate Professor of Medicine and Environmental Health Sciences (in Pediatrics) at New York–Presbyterian Hospital/Columbia University Medical Center
John Balbus, MD, MPH, Chief Health Scientist, Program Director at Environmental Defense Fund
Michel Gelobter, PhD, Chief Executive Officer, Cooler, Inc.
Rohit Aggarwala, PhD, Director, Office of Long-Term Planning and Sustainability, Mayor’s Office of Operations, City of New York
Cecil D. Corbin-Mark, MPhil, Deputy Director, WE ACT for Environmental Justice
Panel 2: Healthy Homes—Controlling Residential Pesticides and Consumer ProductsBrian Lehrer, MPH, ModeratorHost, WNYC and National Public Radio
Panel 2 Policy Recommendations...................................................................................................................................................35
Jay Feldman, MS, Executive Director, Beyond Pesticides
Philip Landrigan, MD, MSc, Director of the Children’s Environmental Health Center at the Mount Sinai School of Medicine
Robin Whyatt, DrPH, Professor and Deputy Director of the Columbia Center for Children’sEnvironmental Health, Mailman School of Public Health, Columbia University
Gina Solomon, MD, MPH, Senior Scientist, Natural Resources Defense Council (NRDC)
Erik Olson, Director of Chemical and Food Safety Programs, The Pew Charitable Trusts
Speakers and Panelists ............................................................................................................................................................................40
List of Key CCCEH Findings...................................................................................................................................................................43
Glossary of Terms ......................................................................................................................................................................................47
* Note: All case study and panel transcripts have been edited for length and clarity.
Additional materials, publications, and full videos of all the conference sessions are available online atwww.ccceh.org/conference09.
Table of Contents
3

On March 30, 2009, the Columbia Center forChildren’s Environmental Health (CCCEH) hosted aconference in collaboration with WE ACT forEnvironmental Justice (WE ACT), the Center’s leadcommunity partner. The symposium focused onthree major environmental health concerns affect-ing children: air pollution, pesticides, andendocrine disrupting chemicals in consumer prod-ucts. The purpose of the conference was to sharethe Center’s research findings and interventionsover the past ten years, and to discuss how such sci-entific findings can be translated into policies toadequately protect children’s health.
During the past ten years, the Center has beenconducting cohort studies in New York City, Poland,and China to identify the environmental and socialcontributors to childhood disease and developmen-tal disorders. Since 1998, CCCEH has followed acohort of over 700 Dominican and African-American mothers and children in NorthernManhattan and the South Bronx, and has partneredwith WE ACT and others to disseminate researchresults to community residents and policymakers.Community-academic partnerships such as this onehave demonstrated potential for improving envi-ronmental health. The conversion of New York City’sbus fleet to clean diesel, the installation by the EPAof permanent air monitors in Harlem and other“hot spots,” and legislation to restrict the use of toxicpesticides in New York City are among the initiativesfor which the partnership’s research and policywork has been given substantial credit. While therehave been successes in reducing exposure to envi-ronmental pollutants over the past ten years, thereis still much to be done in developing policies thatadequately protect children’s environmental health.
Air Pollution & Climate Change
Fossil fuel combustion by motor vehicles, residentialboilers, and power plants release a host of toxic pol-lutants including polycyclic aromatic hydrocarbons(PAH), fine particles, metals, sulfur and nitrogenoxides, and volatile organic compounds, whichinclude precursors to ozone. CCCEH research hasshown that prenatal exposures to PAH are associatedwith significantly reduced fetal growth, an increasedrisk of developmental and behavioral problems,reductions in IQ, asthma precursor symptoms, andchanges in gene expression associated with parentalreports of childhood asthma. Encouragingly, policy
changes supported by these and other findings haveresulted in cleaner air in New York City.Investigators at CCCEH have documented signifi-cant decreases in concentrations of airborne PAHexposure between 1998 and 2006 in our cohort.
Fossil fuel burning can also adversely affectchildren’s health through emissions of carbon diox-ide (CO2), the major climate-altering gas. Climatechange is likely to impact children’s health in a vari-ety of ways, including intensifying summer heatand worsening air quality, prompting earlier andmore intense allergy seasons, and increasing risksof mosquito-borne diseases like malaria and WestNile virus. Higher temperatures accelerate the for-mation of ozone and exacerbate the toxicity of airpollutants. Because of the close linkages betweenCO2 and other combustion-related air pollutants,policies aimed at mitigating global climate changewill also benefit local and regional air quality.Similarly, policies to address air quality locally willinfluence climate globally. An integrated policyapproach is clearly needed if we are to identify andcapitalize on win-win opportunities for climate andhealth. This approach must pay special attention topopulations that are more vulnerable to the healthimpacts of both climate change and air pollutionbecause of inadequate access to health care servic-es, quality housing, financial resources, and socialsupport networks. There is a disproportionate bur-den of adverse effects from air pollution and cli-mate change on disadvantaged communities in theUS and worldwide.
Residential Pesticides
The Center’s research has found links between pre-natal exposure to common residential pesticidesand adverse health outcomes. In our NYC cohort,high prenatal exposure to the organophosphatepesticide chlorpyrifos was associated with signifi-cant deficits in birth weight and birth length, aswell as developmental delay, increased risk forAttention-Deficit/Hyperactivity Disorder (ADHD)and other behavioral problems. Taken together,these findings indicate that residential use of chlor-pyrifos at pre-ban levels resulted in detectable andsometimes high levels of the chemical in umbilicalcord blood that were associated with neurobehav-ioral impairment.
This research has also shown that governmen-tal regulations such as the 2000-2001 EPA restric-
Translating Science to Policy: Protecting Children’s Environmental Health
4
Executive Summary
tions on residential use of chlorpyrifos and the pes-ticide diazinon succeeded in sharply lowering pre-natal exposures, and have had positive impacts onchildren’s health. Despite the residential ban onchlorpyrifos, however, agricultural applicationscontinue in the US and abroad. Citing CCCEH dataat a September 2008 public hearing, the EPA’sScientific Advisory Panel unanimously concludedthat chlorpyrifos may act as a neurotoxicant inhuman beings.
The Center’s research has also shown thatalternatives to the traditional use of residential pes-ticides are more effective and are less toxic.CCCEH, the NYC Housing Authority, and the NYCDepartment of Health and Mental Hygiene jointlyimplemented and evaluated an integrated pestmanagement (IPM) approach in NYC. IPM is anapproach that primarily involves improving sani-tary and structural conditions to deny pests food,water, and movement, and includes the judicioususe of pesticides after an evaluation of need and thehazard to human occupants. Investigators com-pared IPM to traditional practices with respect totheir impact on pests, allergens, pesticide use, andresident satisfaction in several representative publichousing developments. Apartments receiving IPMused fewer pesticides, had significantly lowercounts of cockroaches at three months, and hadgreater success in sustaining these benefits afterthree and six months. Residents of IPM apartmentsalso rated building services more positively. Thiswas just one example of using the results of scientif-ic research to change public health practice.
Endocrine Disruptors
Endocrine disrupting chemicals interfere with theproduction, release, transport, metabolism, bindingaction or elimination of the natural hormones in thebody responsible for the maintenance of homeosta-sis and the regulation of developmental processes.Recent studies indicate that when exposures occurat specific times in utero and/or in early life, infantand child development itself may be disrupted inways that can affect intelligence, reproductive devel-opment, the timing of puberty, fertility, and couldincrease the risks of obesity and cancer. The Center’sresearch on endocrine disrupting chemicals isfocusing on phthalates and bisphenol-A (BPA),
which are widely used in consumer products and infood and beverage containers. Exposures are ubiq-uitous. For example, in the sample of women andchildren in the CCCEH cohort evaluated thus far,100% were exposed to phthalates in the air theybreathed and 100% had residues of phthalates andBPA in their urine. High maternal phthalate expo-sure during pregnancy was associated with reducedgestational age.
Translating Science to Policy
Policy roundtables considered strategies for lever-aging scientific findings into policies that betterprotect environmental health. The first panel dis-cussed options for reducing pollution from fossilfuel burning in urban areas like New York City.Panelists considered proposals that would targetemissions from vehicles, residential heating fuels,and power plants. These included changes in infra-structure, such as renovating power plants withupdated technology, reforming transportation sys-tems to be both environmentally and financiallysustainable, and replacing residential boilers to uti-lize energy more efficiently while emitting fewerpollutants into the air. Other options included thereduction of diesel emissions through strongeridling regulations, retrofitting diesel fleets, and theuse of diesel particulate filters to reduce emissionsof black carbon.
Ensuring that the public is protected fromtoxic chemicals such as pesticides, phthalates, andBPA in the home and in common consumer prod-ucts is also an urgent matter. Panelists in the secondroundtable underscored the ineffectiveness of thecurrent Toxic Substances Control Act. They agreedthat comprehensive legislative reform at the federallevel is needed to require manufacturers to showthat chemicals are safe before marketing, ratherthan placing the burden on agencies and the publicto prove that each new chemical on the marketcauses harm before it is regulated. Labeling ofchemicals like phthalates, BPA, and other endocrinedisruptors in consumer products is needed toenable individuals to make informed decisions. Aconsumer-based approach to this problem, howev-er, is limited in effectiveness and cannot substitutefor regulation. When a chemical is removed fromthe market, safe substitutes must be available.
Conference Overview
5

Ten years ago, theColumbia Center forChildren’s EnvironmentalHealth (CCCEH) wasfounded with the goal ofpreventing environmental-ly related childhood diseaseand developmental disor-ders. We focused on therole of early-life exposureto pollutants and adversesocial conditions, whichwere suspected of beingamong the earliest deter-
minants of disease. Our ultimate goal was to docu-ment the effects of prenatal and childhood expo-sures and communicate our findings to helpreduce, and ultimately prevent, asthma, develop-mental disorders, and cancer in children.
Since 1998, we have been conducting interna-tional studies of pregnant women and their chil-dren in New York City, Poland, and China. We haveused an innovative research approach called“molecular epidemiology,” which combines tradi-tional epidemiological methods and environmentalmonitoring with the measurement of biomarkers(molecular changes that can be detected in blood orurine) to estimate children’s exposure to pollutantsand their risk of disease. In New York City, forexample, we have been following a cohort of over700 Dominican and African-American mothers andchildren in New York City’s Washington Heights,Harlem, and South Bronx neighborhoods, who aredisproportionately exposed to pollutant sourcessuch as diesel bus depots, major commercial road-ways, and deteriorated public housing.
In 2000, we convened our first conference todiscuss the serious health threats to children in NewYork City from environmental exposures, environ-mental justice, and the need for targeted research tofill the gaps in knowledge. We outlined our innova-tive research approach, our very early findings, andour plans for outreach and translation of results.
Since then, we have gathered compelling evi-dence of the multiple adverse health effects of early-life exposures to common urban pollutants. Ourfindings have identified links between specific healthhazards and their clinical consequences. The hazardsinclude prenatal exposure to air pollution from traf-fic and other combustion sources, second-hand
tobacco smoke, residential pesticides, and pest aller-gens. The health outcomes include significantlyreduced fetal growth, increased risk of developmen-tal and behavioral problems, respiratory symptomsand asthma, and increased cancer risk. We have alsolearned that exposure to multiple pollutants can leadto more detrimental health outcomes in childrenand that nutritional deficiencies, genetic predisposi-tion, and poverty can exacerbate pollutant effects.
In March 2009, we held a second conferencein collaboration with WE ACT for EnvironmentalJustice, our lead community partner, to report onour key findings, our intervention studies thatflowed from these findings, and to discuss ways totranslate this research into protective health policy.We have made significant gains in scientific knowl-edge over the past decade, which will be describedin this report. Working in collaboration with WEACT and other members of our CommunityAdvisory Board, we have applied our findings tointerventions and health education materials forparents, community members, health profession-als, and policymakers.
Much more remains to be done, however. Inthe coming years, we will address the longer-termconsequences of the pollutants we have been study-ing as well as the role of endocrine-disrupting chem-icals, such as bisphenol-A (BPA) and phthalates, inchildhood disease. These chemicals are ubiquitous inthe environment and have been linked to obesity andmetabolic disorders, as well as to other health prob-lems in children. We hope to better understand themechanisms involved in environmentally related dis-ease, such as epigenetic modifications (changes in agene’s expression but not its fundamental DNA struc-ture) and genotoxic mechanisms (DNA damage thatcan cause mutations). This knowledge will be valu-able in developing early warning indicators andinforming preventive policies.
We hope the conference proceedingsdescribed in this report will stimulate discussionand propel work forward for scientists, communityactivists, and policymakers as they identify andimplement policies to protect environmentalhealth. We also hope that it will inspire new allies inthe effort to protect children’s health.
—Frederica Perera, DrPHProfessor and Director,
Columbia Center for Children's Environmental Health
Translating Science to Policy: Protecting Children’s Environmental Health
6
Children’s Environmental Health: A Decade of Research

Most advocatesapproach theirmission in the spir-it of, “We are nothere to fear thefuture. We are hereto shape it.”
Over the past20 years, I havebeen proactivelyengaged in thegrassroots nationalenvironmental jus-tice movement,
which has redefined environment to embrace all thehabitats where we live, work, play, and go toschool. Movement organizers, advocates, and aca-demics have helped document that millions ofpeople in this nation do not have access to cleanair, clean water, a healthy home, a safe school, anda sustainable community. We are engaged in stud-ies that indicate that race, class, and income arekey determinants of health status, as are higherenvironmental and occupational exposures. Werealize that longevity is increasing for manyAmericans as mortality and morbidity increases forresidents in indigenous, and urban and rural com-munities of color and low income across thisnation and around the world.
We acknowledge that we live and work in acontext of race, class, and income as key determi-nants of health status, environmental protection,and how land-use burdens and benefits are distrib-uted. We understand that children, in their earlystages of development, are more vulnerable to envi-ronmental exposures, and that children of color aredisproportionately impacted by pollution and aremost disadvantaged. The dynamics of environmen-tal injustice have led to excess exposure to environ-mental hazards, communities devoid of green ben-efits, and a lack of community-based participationin democratic decision-making. It is these dynamicsthat have seized my attention, commitment, andenergy for the last 20 years.
The important news is that there is a growingawareness of community conditions that affect com-munity health and sustainability. There is evidencethat community engagement and participation is
translating research to policy and practice. It isreshaping the direction of many neighborhoods, cre-ating opportunities where it seemed there were none.
We realize that the most powerful factorsshaping health and disparities are social and eco-nomic determinants such as poverty and discrimi-nation. Community-wide environmental condi-tions influence health directly through toxins in air,water, soil, and building materials. Health dispari-ties are prominent in communities without accessto nutritious food, spaces for active living, effectivetransportation systems, but with ready access tounhealthy products like cigarettes, alcohol, and fastfoods. Combine these factors with lack of access toquality medical care, and we describe the landscapeof disparities in communities like NorthernManhattan and the South Bronx.
The results from the Center’s study here inNorthern Manhattan and the South Bronx are typi-cal of exposures being experienced by other envi-ronmental justice communities in NYC and acrossthis country. Like other communities, NorthernManhattan residents want and need to identifyenvironmental exposures that negatively impacttheir health and quality of life.
WE ACT’s 10-year partnership with theColumbia Center for Children’s EnvironmentalHealth has answered community questions aboutlevels of indoor and outdoor toxins and allergens.The collaboration has engaged residents, empower-ing them through trainings and evidence-basedenvironmental health campaigns to impact publicpolicy. The collaboration has enriched the scienceand increased capacity at the community and aca-demic levels. The Center’s research findings haveempowered residents and advocates to translate theresearch into policy and practice. I believe and Ihave observed that carefully designed Community-Based Participatory Research (CBPR) that is commit-ted to strong science, high level community involve-ment, engagement in policy steps and activities, andthe strategic use of study findings to help impactpolicy is an important contributor to the broaderstruggle for urban health and environmental justice.
—Peggy M. ShepardExecutive Director, WE ACT for Environmental Justice
Conference Overview
7
Partnership in Public Health Research: A Decade of Activism
I’m pleased that I have an opportunity to addressyou and meet with you so early in my tenure at EPA.I hope it underscores for you the importance that Iassign to these issues, to children’s health. It’s alsovery significant that we’re here in the middle of thisgreat city to talk about environmental protection.When we talk about the environment or environ-mentalism, it typically brings to mind sweepinglandscapes and stunning vistas, pristine beaches,mountains, but what usually doesn’t come to mindfor too many people still is an apartment buildingor a city block, an urban playground, parking lots.But that perception only tells part of the story. Youknow very well that our cities and urban communi-ties are home to some of the most significanthuman health and environmental issues that weface as a nation. That’s because environmental pro-tection is about human protection, it’s about pro-tecting our communities and our families, it’s aboutsafeguarding the places where Americans live andwork and play and learn. In that work, EPA and I asthe Administrator are committed to meeting peoplewhere they are.
You do not have to label yourself as an envi-ronmentalist, and I don’t believe that all of you herespend your days or nights thinking about wilder-ness preservation or sit up late at night, as too many
of us do lately, talking and strategizing on climatechange. But we’ve all come to the conclusion thatchildren’s health is worth fighting for. Maybe you’rea parent or a grandparent worried about lovedones, or maybe you’ve noticed that the kids in yourneighborhood can’t go outside and play in the sum-mer because it’s too dangerous to breathe the air.Maybe the work of our friends in the environmen-tal justice movement have moved you to action,people like WE ACT have gotten through to you.You understand that the children who get sick attwo and three times the average rate because theirair and water are dirty are often the same kids whouse emergency rooms as their primary healthcaremechanism. And you know that that drives uphealth costs for everyone, not to mention the strainit puts on working mothers and fathers who have tomiss work to care for their children.
Whatever reasons bring you here to thismoment, we share the common ground of chil-dren’s health protection. And I say again that EPA iscommitted to meeting you where you are andworking with you on the issues that we share. Thereare simply too many important issues where wecan’t wait for a quorum of the American people todecide that they are environmentalists before wemove forward with action. Children’s health is oneof those issues.
Ensuring that our children are not exposed totoxins and pollution or other environmentalthreats in their homes or in their schools or any-where else is central to our work at EPA. Children’shealth was one of the top issues that I laid out in myfirst day memo and sent to all employees in order toestablish priorities from day one. Children’s healthwas reinforced by our first lady, Michelle Obama,when she visited EPA last month and spoke to ourstaff. She charged each employee there with aresponsibility, saying simply that the health andsafety of our children is our top priority.
Children’s health was also the driving forcebehind one of our very first initiatives, the effort tomonitor dangerous particulate matter aroundschools. When USA Today published this story, par-ents all across the nation read about dangerous airin our schools; they read how children absorb toxicpollutants in the same quantities as adults, meaning
Translating Science to Policy: Protecting Children’s Environmental Health
8
Protecting Children’s Environmental Health
Lisa P. JacksonAdministrator, US Environmental Protection Agency
they ingest a much higher dose because of theirlower body weights; they read about how childrenare more vulnerable to asthma and other respirato-ry illnesses and susceptible to long-term complica-tions that can affect them throughout their entirelives. Then they sent their children to school won-dering, as any parent would, if they were puttingthem in harm’s way.
So in response to their concerns EPA has afundamental obligation to step in. We’ll work withtribes, states, and local officials to determine whichschools are exposed to high levels of toxic air pollu-tion. We have a strong focus on schools located nearlarge industries, big stacks, and in urban areaswhere we know there’s a coming together of issuesthat can affect children’s health. That will begin atsome schools in the coming weeks. Results will beavailable to the public as quickly as we can providethem so that the many concerned parents andhealthcare professionals, toxicologists, and riskassessors can get critical information they deserve,and so that we can all take action where it’s needed.But that’s just the beginning. We have importantobligations to look ahead and be proactive aboutpreventing and where necessary mitigating the par-ticular effects of climate change and those effectson children’s health and welfare. We need to stepup our efforts to assess and manage chemical riskespecially those in looking how they are particularlyharmful to children. As this Center has shown, pre-natal and early life exposures can have tragic life-long effects, and we must be diligent in preventingany possible dangers.
I’m also particularly concerned about elimi-nating disparities in environmental health and safe-ty from minorities and low income populations.You have all led the way on this, and I’m asking foryou to keep pushing. We need your help at EPA toelevate this issue to the mainstream so that we cancreate a sustainable and healthy environment forchildren and adults in every single community inour country.
These and many other issues—energy effi-ciency, public transportation, walkable neighbor-hoods, air quality, water quality, hazardous waste—are all important to children’s health protection.So I’m very proud today to announce some greatnews in our children’s health work. Starting todaywe have a new member on our team at EPA, PeterGrevatt. Peter will serve as our senior advisor forchildren’s environmental health. Peter brings tothe position a wealth of scientific, risk assessment,
environmental justice and children’s health expe-rience. …
Now given Peter’s background in science, Ithink I can speak for him, and I certainly know forme the theme of this meeting, translating scienceinto policy, is praiseworthy indeed. It makes mehappy not just because I’m a scientist, but becauseI’ve been working to communicate that sciencemust once again be the determining factor in EPA’sdecision making. If we return to science we willmake decisions on clean air and water that are
based on human health. It will lead us to placeswhere we can identify and articulate very clearlywhat it is we face and what it is we must do.
In just the past month we have begun thearduous process of reexamining previous decisionsmade at EPA largely because of questions aboutwhether science was trumped by politics. Wheneverthat happens it may be a momentary victory for oneside or the other, but it dilutes our effectiveness atEPA as an agency, it dilutes the American people’sability to look at EPA and see us as guardian of thethings they value, and it requires that we use ourtime and resources to look back when we absolutelyneed to be moving ahead.
Conference Highlights: Keynote Speakers
9
“… science must once again be the determining factor in EPA’sdecision making. If we return to science we will make decisionson clean air and water that are based on human health. It willlead us to places where we can identify and articulate veryclearly what it is we face and what it is we must do.”

The second guiding principle for us at EPA isthe rule of law. The lawsuits that follow EPA areprobably inevitable, but there have been someimportant times when lawsuits have crystallizedwhat we need to remember every day at EPA, andthat is that the laws are in place because Congress
decided and the people determined that environ-mental action was needed. If we don’t uphold theselaws then we have let the system down, but moreimportantly we are impacting and affecting people’shealth. When we don’t win a court case on particu-late matter or ozone, it’s sad for the lawyersinvolved but it’s tragic for human health.
Lastly, we must operate with unparalleledtransparency at EPA. Transparency will aid us inmaking sure that science and the law come first,and it will send a very clear signal to the Americanpeople that we work for them. I want everyone toknow who I meet with and what I’m talking about,and I want the American people to believe that EPAis its advocate. It’s extraordinarily important thatpeople believe they can get inside the walls of theEPA and that EPA is not governed by industry or anyone group or interest.
In closing, let me say that right now we haveextraordinary opportunities to protect publichealth and the environment, probably greater thanany other time in the history of the EPA. We’vemoved beyond the false choice between having agreen economy and having a green environment,and we have risen above many of the past dividesthat have often slowed down environmental pro-tection and set us back for years. Today in Congressand throughout the country there is tremendousbipartisan support for green jobs, smart growth,clean energy, a long list of ideas and innovationsthat will grow our economy and improve our plan-et. And we have the support of extraordinary peo-ple like you.
So when I speak to reporters and industryleaders, community members, stakeholders, I’vetried to send a clear, consistent message and it’s amessage that I give you in hopes that you will joinwith me in carrying it to everyone you work with.That message is that EPA is back on the job. I’masking you to keep doing exactly what you’redoing, continue to gather the best science, thenuse that information to organize and engage peo-ple in your communities, talk to parents aboutwhy this matters, show someone that whetherthey count themselves as an environmentalist ornot, clear air and clean water affects them and thepeople around them every day. Please educateyoung people so that they can carry the torch forthe next generation.
Translating Science to Policy: Protecting Children’s Environmental Health
10
“I’ve tried to send a clear, consistent message, and it’s a message that I give you in hopes that you will join with me incarrying it to everyone you work with. That message is that EPAis back on the job.”
Environmental health sciences provide criticalinvestments into children’s health. We’re interestedin prevention here, and that’s really the power ofenvironmental health. When I look at the missionof my Institute, it is to protect the American publicfrom diseases and health conditions associatedwith the environment. We need to remove thetoxic agents from human exposure before diseasehappens.
When we’re talking about environmentalhealth sciences and children’s health, we’re reallytalking about the issues of early prevention. Andwhat does early prevention get us? It gets us years,decades, a lifetime of improved health. It can leadto reductions in early mortality and morbidity. Itcan decrease the instances of fetal or childhoodexposures causing diseases in adulthood. You’vealready heard somewhat about that this morning,and I’m going to come back to the latent effects ofearly life exposures. It can improve the quality oflife. And, from an economic point of view, and weare always being asked to balance economic bene-fits with risks, it can decrease the expenditures onhealthcare while improving individual productivityin the schools and the workplaces throughout life.
I want to talk about a children’s success story,and that’s the story of lead. Lead as an additive wasremoved from gasoline in the mid-70s as well asfrom paint, and it started a downward trend.Actually, it was amazing. From 1976 to 1988 therewas a dramatic decline in the amount of lead meas-ured in children’s blood in the American popula-tion. I can tell you from a regulatory perspective noone expected that taking lead out of gasoline wouldbring about the very rapid decrease that ensued. Asa follow-up, CDC reported that the percent of chil-dren with elevated blood lead dropped from 9% in1988 to 1.4% in 2004.
When the regulatory limit of ten parts perdeciliter was set, the idea was that it was protectiveagainst the adverse effects of lead on child’s IQ. Butwhat we’re now understanding is that there appearsto be no safe level of lead. Even at lower levels, wecan still see relationships. It became harder to see theIQ effects (although you can see them on a popula-
tion basis), but we can see the behavioral effects asso-ciated with lead. I think this is a very important mes-sage to get out there—that we need to continue to bevigilant and to continue to reduce these exposures.
We’re all here really celebrating the success ofthe Centers for Children’s Environmental Health
and Disease Prevention program, and specificallythe marvelous program that exists here atColumbia. This is a federal partnership, and it’s thekind of thing the government can and should domore of. In this case, it’s a partnership betweenNIEHS and the US EPA. The overall goal of this part-nership was to establish a national network foster-ing communication, innovation, and researchexcellence in children’s environmental health inorder to reduce the burden of morbidity amongchildren as a result of exposure to harmful environ-mental agents.
We have 13 centers, 12 of which are co-fundedby NIEHS and EPA. These centers are addressing avariety of environmentally-related issues, and thefocus is to stimulate new and existing research on the
Conference Highlights: Keynote Speakers
11
The Promise: Children’s Environmental Health
Linda S. Birnbaum, PhD, DABT, ATSDirector, National Institute of Environmental Health SciencesNational Toxicology Program
“We need to remove the toxic agents from human exposurebefore disease happens.”

role of environment in the etiology of disease anddysfunction. All too often we’re looking for diseases,and what we really need to be looking at is puttingmore children in an at-risk category, whether it’s atrisk for their behavior, at risk for their intellectualsuccess, at risk for their future. We need to developnovel effective interventions and prevention strate-gies, and we heard about some of those this morn-ing. Again, it’s much better to prevent the problemthan to try to treat or cure it once it has occurred.
We need to promote the translation of basicresearch findings into applied intervention andprevention methods. We need to enhance theawareness of the public and medical professionalsof detection, treatment, and prevention—and I keepstressing prevention. I think the public partner-ships that these children’s centers have are really anexample for how the biomedical research establish-ment needs to be moving in the 21st Century.
I’m going to briefly give a couple of examplesof some of the different kinds of focuses that wehave in these environmental centers. You’ve alreadyheard somewhat about environmental health andasthma, which is still a work in progress. We knowthat the increase in asthma is really of epidemicproportions. Right now in the US we have at least 22million people with physician-diagnosed asthma,and 6 million of those people are children.Researchers funded by NIEHS within our Instituteand our intramural program have identified dustmites and roach allergens, cockroaches, as commontriggers in initiating asthma and asthmaticepisodes. These environmental agents not only cancause the disease, they exacerbate and promote it.Here you have two opportunities for prevention.The first is to stop the disease from ever happening,which is the best. The second is to stop it frombeing reintroduced or progressing.
Many of the centers, like this one, are explor-ing the roles of outdoor pollution as well as indoorpollution, and the role of maternal smoking. We’realso understanding that there are genetic suscepti-
bilities. What we’re looking at in many cases areinteractions between the epigenome and environ-mental exposure in the induction of these diseases. Iknow that here at Columbia you’re looking at pollu-tants from vehicle exhaust, indoor residential heat-ing and power generation, and finding that many ofthese pollutants may actually alter the structure ofDNA and chromosomes in the womb.
The increased susceptibility of the developingorganism is well known. In utero, infantile, andpubertal stages are all times of rapid growth andextensive differentiation. It’s at these times that youhave opportunities for initiation of lesions and pro-motions of altered cells. We all know that develop-ment is a highly integrated process. The idea of latenteffects of early exposure comes from some key epi-demiological work done in the United Kingdom,which is known as the “Barker Hypothesis.” This isthe growing body of research that suggests that manychronic adult diseases and disorders, including asth-ma, diabetes, obesity, even heart disease for exam-ple, can be traced back to exposures that occur inutero or during early childhood.
I just want to briefly mention some of thework that NIEHS is doing related to early expo-sures. NIEHS is partnering with the NationalCancer Institute in funding four breast cancer andthe environment research centers that are investi-gating the impact of prenatal and childhood expo-sures on mammary gland development, and on thepotential of exposures to alter risk of breast cancerin adulthood.
In addition to asthma and cancer, another keyissue is neurodevelopment and neurological dis-eases. We support basic research to determine themechanisms and pathways by which toxicants candisrupt the developing brain. A point that I shouldmake is that brain development does not stop atbirth. It does not stop at two years of age. In fact,there’s growing evidence that, in humans, the braincontinues to develop until about 25 years of age (sowhen you’re dealing with your teenagers and youknow that they’re not full adults, it’s true.)Neurotoxicants being studied by NIEHS-sponsoredresearch includes a variety of metals, such as lead,mercury and manganese, pesticides, tobaccosmoke, and a whole bunch of persistent organicpollutants such as PCBs. In the past we have studiedthe dioxins, and it’s a success of the regulatoryagency that dioxin levels have gone way down. Butnow there’s a lot of focus on polybrominateddiphenyl ethers (PBDEs) and other brominated
Translating Science to Policy: Protecting Children’s Environmental Health
12
“We need to promote the translation of basic research findingsinto applied intervention and prevention methods. We need toenhance the awareness of the public and medical professionalsof detection, treatment, and prevention—and I keep stressingprevention. I think the public partnerships that these children’scenters have are really an example for how the biomedicalresearch establishment needs to be moving in the 21st Century.”

flame retardants, which we’re finding in exponen-tially increasing levels in our environment and inour people. They’ve been put there to provide firesafety. I’m not terribly concerned about going up insmoke, but I am concerned about what’s happeningto our population by exposure to these compounds.
In addition to looking at early life exposureand development neurotoxicity, we’re also lookingat the associations with neurodegenerative syn-dromes. Autism is clearly a neurodevelopmentalcondition. I should mention we shouldn’t just betalking about “autism,” just like we don’t just talkabout “cancer.” We’re talking about a spectrum ofdisorders, and they may have different and multiplecauses when you talk about autism spectrum. We’redealing with Attention-Deficit/HyperactivityDisorder (ADHD). Again, this is not one condition—there are multiple conditions and multiple causes.We are also looking at adult onset diseases, such asParkinson’s disease and Alzheimer’s. Again, thesemay be rooted in early environmental exposures.Many of our NIEHS centers focus on neurodevelop-mental outcomes.
I want to come back to autism now because weknow that there is an epidemic of autism in the popu-lation, and it cannot all be explained by changes inclassification of the disorder or better diagnosis. Oneof our children’s centers that really focuses on that isat the University of California at Davis, which is con-ducting the first large-scale epidemiologic study ofchildren with autism, looking at a wide range of envi-ronmental exposures and effects on early develop-ment of over 1,000 California children. At the sametime, we have NIEHS-sponsored investigators lookingat new and improved animal and cellular models forautism and ADHD. This will help us determine howneurotoxic substances may impact both brain devel-opment and behavior. Interestingly, we have tendedto think about the immune system and allergies, orresponses to certain other stressors. The immune sys-tem plays a key role in brain development as well, andthere appear to be interactions. If you have one autis-tic child or if there’s autism in a family there is clearlysome kind of both genetic and environmental suscep-tibility factors going on here. One of the most excitingthings we’re doing is enrolling mothers of autisticchildren who are pregnant with a subsequent child tolook at prenatal, neonatal, and early postnatal expo-sures to see if we can pick up an association in thismore susceptible population.
The other thing I want to mention is that in2006 Congress passed the Interagency Autism Act,
which provides for a national strategy on dealingwith autism and autism-based research. I serve onthe coordinating committee for that, along with theheads of National Institutes of Child Health andDevelopmental and Neurological Disorders, andMental Health, for example. This is also a coordi-nating committee that not only involves the leadersof the research community, but involves citizens’action groups and advocacy groups so we can worktogether to move faster in dealing with these seri-ous environmental diseases.
Endocrine disruptors are exogenous agentsthat interfere with the production, release, trans-port, metabolism, binding action or elimination ofthe natural hormones in the body responsible forthe maintenance of homeostasis and the regulationof developmental processes.
One point I want to make is that what is nor-mal for me may not be normal for you. We all haveour own balance of different hormones in our dif-ferent systems. What is normal has a distribution. Iused to talk about in the dioxin field where we knewthat exposure to dioxin could reduce circulatingtestosterone levels by 10%—for a male who is in theaverage of that, or the mean of that distribution, a10% reduction means nothing. But for a male who’sat the low end, a 10% reduction can make him infer-tile. When we’re talking about exogenous chemicalsthat are endocrine disruptors, they’re not addingonto a control of 0. They’re adding onto a back-ground that already exists. Depending on wherethat background is, it may cause a problem for somepeople and not for other people.
Environmental exposures to endocrine dis-ruptors are suspected of being associated with theearlier and earlier puberty we’re finding in younggirls, with increasing incidences of genital malfor-mation that are being detected in the population,and with the dramatic increase in testicular cancerin males. This is not only in our country, it is prettymuch worldwide. NIEHS has supported a numberof studies, both experimental and epidemiologicalstudies, looking at endocrine disruptor activities.
For example, BPA, which you heard men-tioned this morning, is often called a weak environ-mental estrogen. But weak is context-dependent. It
Conference Highlights: Keynote Speakers
13
“As we move into the 21st Century, we’re beginning to realizethat the developmental period is a critical time for disruption,not only by endocrine disrupting agents but by other toxicants.”
may be weak in terms of its ability to work onnuclear estrogen receptors, but it is equipotentwhen it comes to the newly-discovered membraneestrogen receptors. And BPA is only one of a pletho-ra of environmental endocrine disruptors, or in thiscase environmental estrogens, which act in an addi-tive fashion. So when we look at one compound at a
time we may miss the boat. Nevertheless, BPA inexperimental studies clearly causes changes in themammary gland and in the development that weretime and dose dependent. …
As we move into the 21st Century, we’re begin-ning to realize that the developmental period is acritical time for disruption, not only by endocrinedisrupting agents but by other toxicants. We’rebeginning to emphasize the use of perinatal dosing
regimes in our toxicology and carcinogenicity stud-ies. We’re also focusing on the important under-standing that it’s not so much what you get on a dailybasis but it’s what’s really in your bodies that’s reallyimportant. For some chemicals, which are persistentand biocumulative, you are what you’ve beenexposed to for the last month, year, multiple years.For other things, it could be very much what you’regetting on a daily basis. But if we want to compareour animal data to our human data we have to lookat the internal dose. That has been kind of a lateunderstanding in the field. …
So when we talk about children’s health, insome ways our children’s health is a report card onwhat the future adult health of the American popu-lation will look at. Kids, along with the ill and theelderly, are the most vulnerable parts of our popu-lation. The lives of our children are our most cher-ished and prized responsibilities. Our children’shealth reflects how we are doing both as a nationand the world. May our report cards give usincreasingly A’s in this area.
Translating Science to Policy: Protecting Children’s Environmental Health
14
“The lives of our children are our most cherished and prizedresponsibilities. Our children’s health reflects how we are doingboth as a nation and the world.”

Air pollution from the burning of fossil fuelsadversely affects children’s health in many ways. InNew York City (NYC), major sources are local-trans-portation vehicles, including buses, trucks, andautomobiles. Diesel fuel is a particularly importantsource of pollutants. Nationwide, coal burning iswidely used in power generation and industry, andis a major contributor to air pollution. These pollu-tants can be locally generated as well as transportedto NYC from areas upwind. The complex mix ofpollutants in urban ambient air includes polycyclicaromatic hydrocarbons (PAH), fine particles, sulfurand nitrogen oxides, mercury, and other metalsfrom fossil fuel burning.
We know from many lines of research that thedeveloping fetus, infant, and young child are espe-cially susceptible to effects of toxic pollutants, andalso to psychosocial and other physical stressors suchas heat. Compared to older children and adults, thevery young have less efficient systems to detoxifychemicals or repair damage; and their rapid growthand higher rates of cell proliferation put them atgreater risk. Over the span of their lives there is moretime for cancer and other serious chronic diseases,such as cardiovascular and neurodegenerative dis-eases, to develop. We are now aware that harmfulearly-life exposures can affect health over the lifecourse, not only in childhood, but also in adoles-cence and in middle and older age. We are alsobeginning to understand that early exposures canresult in heritable effects across generations.
There is an urgent need to prevent environ-mentally-related disease, in NYC and elsewhere.
High rates of low birth weight, developmentaldelay, and asthma in children were obvious to usten years ago. They are even more obvious now. InCCCEH’s Mothers & Newborns study in NorthernManhattan and the South Bronx, we have found a30% incidence of asthma and a high incidence ofdevelopmental problems. African-American popu-lations have much higher rate of low birth weightand preterm delivery than other populations. In theUS, rates of developmental disorders, asthma, andcertain childhood cancers have been increasing inrecent decades. Common environmental exposuresare known or suspected of contributing to thisincrease, along with adverse social conditions,genetic susceptibility, and nutritional deficits.
Studies & Design
The Center has been carrying out longitudinal studiesof mothers and children in NYC, Poland, and China,as well as a study of health effects in the aftermath ofthe World Trade Center disaster. All these cohortstudies are complementary because they are investi-gating common pollutants using the same molecularmethods. These methods involve the analysis of bio-
Conference Highlights: Presentations
15
Impact of Prenatal Exposure to Air Pollution from Traffic and Other Fossil Fuel Combustion Sources on Children’s Health and Development
Frederica Perera, DrPH Professor and Director, Columbia Center for Children’s Environmental Health, Mailman School of Public Health, Columbia University
Figure 1
Case Study 1: Air Pollution and Climate Change
This case study focused on the effects of fossil-fuel related air pollution on children’s health, and the linkages between fossil fuelcombustion, climate change, and human health. Dr. Frederica Perera discussed the Center’s findings about the health effects ofprenatal and early-life exposure to air pollution from traffic in New York City, which include low birth weight, respiratoryeffects, neurodevelopmental disorders, and potentially increased cancer risk. Dr. Patrick Kinney then reviewed the effects ofglobal climate attributable to carbon dioxide (CO2, one of the main greenhouse gases) on children’s health. The predictedeffects in children of global warming caused by CO2 from fossil fuel combustion include heat stroke, increased risk of infectiousdisease, allergies and asthma, and malnutrition from food shortages. These two pathways of health effects are closely related,and interact with each other (see Figure 1). Reducing fossil fuel pollution in New York City and across the country will thereforehave multiple, complementary benefits..
logic samples like umbilical cord blood, urine or pla-cental tissue for biologic markers indicating the levelof pollutant exposure, the preclinical damage result-ing from the exposure, or genetic or nutritional sus-ceptibility to the exposure. The biomarkers areembedded in population studies—an approachknown as molecular epidemiology. Our study popula-tions include young, healthy, non-smoking womenrecruited during pregnancy. A total of 2,000 mothersand 2,000 children have been enrolled in these stud-ies. Our largest study is in NYC, where over 700African-American and Dominican mother-child pairsliving in Harlem, Washington Heights, and the SouthBronx have been enrolled.
We use a molecular epidemiologic approach in allour studies to better document the early warning signsof disease risk or susceptibility. Two examples of bio-markers include epigenetic changes and chemical-DNAadducts, which can be measured in blood. When epige-netic changes occur, the structure of DNA is notchanged, but the expression of the gene is altered. Sincegene expression is tightly choreographed during earlydevelopment, unprogrammed epigenetic changes canresult in developmental and health problems. DNA-adducts are formed by the direct interaction of a chemi-cal (such as PAH) with DNA. Adducts are considered amarker of potentially increased cancer risk because theycan lead to mutation and even to cancer.
In the NYC study, as in the other cohorts, we havetaken repeat measures of exposure, biomarkers, andoutcomes from pregnancy into childhood. Exposureassessment is done through personal and residentialair monitoring. We obtain extensive questionnairedata, as well as geographic information about neigh-borhood-level characteristics (see Figure 2). In ouranalyses, we control for factors that could confoundassociations between the pollutants of concern andhealth effects, such as socioeconomic status and age.
CCCEH Research Results
We have found that exposure to pollution in the air iswidespread in our NYC cohort—100% of pregnantmothers were exposed to PAH in air; 40% were alsoexposed to environmental tobacco smoke (ETS); and40% of mothers reported experiencing materialhardship during pregnancy. This is clearly a popula-tion in which both physical toxicants and psychoso-cial stressors are prevalent.
DNA adducts were detected in 40% of thematernal and newborn cord bloods. We also com-pared the levels of PAH-DNA adducts in maternal andcord blood within and across our NYC, World TradeCenter, Polish, and Chinese study populations.Despite the natural protection that the placenta pro-vides in reducing fetal exposure, levels of DNA dam-age in mothers and children were similar withineach population. This finding indicates that the fetusmay be significantly more susceptible to DNA dam-age from air pollution than adults.
Prenatal exposure to PAH measured by personalbackpack air monitors or by PAH-DNA adducts incord blood was associated with reduced birth weightand head circumference among African-Americansand, across the entire population, with developmen-tal delays at age 3, attentional and behavioral prob-lems, and reduced IQ scores at age five. Prenatal PAHexposure in conjunction with postnatal exposure tosecondhand smoke was associated with increased res-piratory symptoms. We have also found that an epige-netic alteration in cord blood that was associated withprenatal PAH exposure was a predictor of subsequentchildhood asthma. This was the first such report.Finally, we have found that prenatal PAH exposurewas linked to significantly higher frequency of stablechromosomal alterations in newborns.
Conclusions
Our scientific findings have serious implications forchildren’s health, but there is also good news in thatdata such as ours can spur action that yields imme-diate benefits. In NYC, for example, we have seenthat personal prenatal exposure to PAH in ourcohort declined significantly in recent years as aresult of NYC’s efforts to clean up its fleet of buses,restrict idling, and reduce congestion. As shown inFigure 1, children’s health doubly benefits fromcurbing of fossil fuel combustion emissions. In con-clusion, our findings underscore the critical need toidentify risks from early-life environmental expo-sures as a key to prevention of childhood diseaseand developmental impairment.
Translating Science to Policy: Protecting Children’s Environmental Health
16Figure 2
Case Study 1 : Air Pollution and Climate Change
17
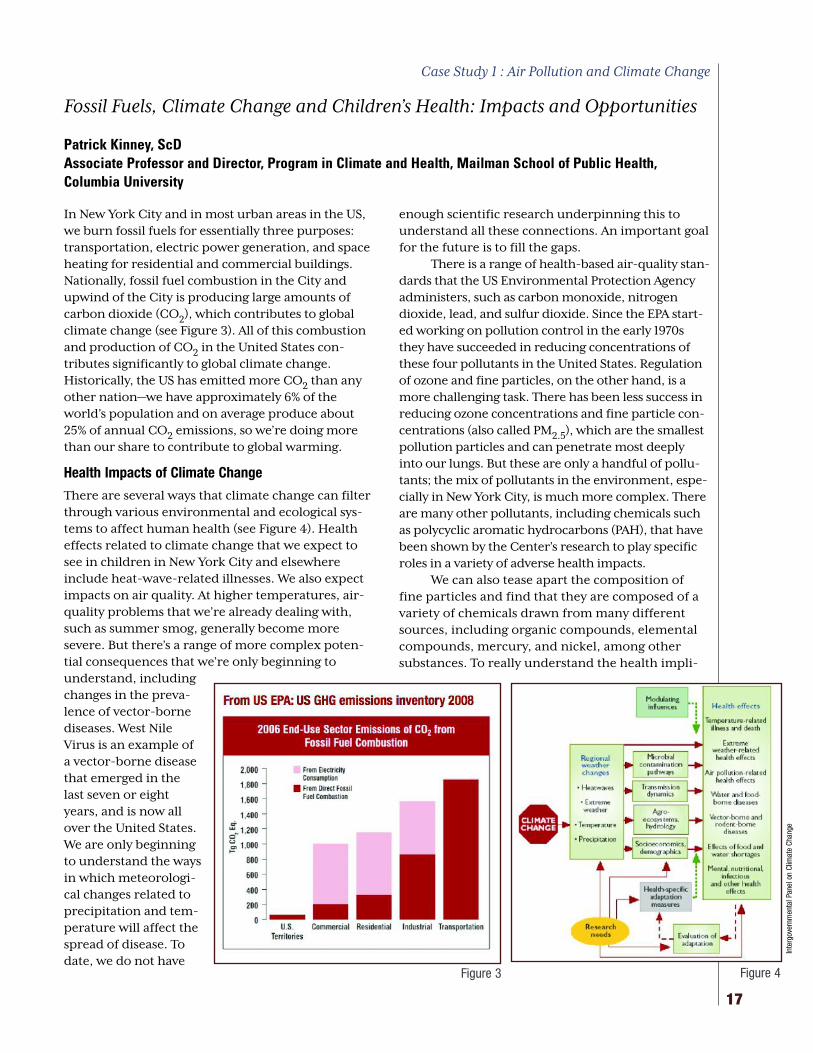
In New York City and in most urban areas in the US,we burn fossil fuels for essentially three purposes:transportation, electric power generation, and spaceheating for residential and commercial buildings.Nationally, fossil fuel combustion in the City andupwind of the City is producing large amounts ofcarbon dioxide (CO2), which contributes to globalclimate change (see Figure 3). All of this combustionand production of CO2 in the United States con-tributes significantly to global climate change.Historically, the US has emitted more CO2 than anyother nation—we have approximately 6% of theworld’s population and on average produce about25% of annual CO2 emissions, so we’re doing morethan our share to contribute to global warming.
Health Impacts of Climate Change
There are several ways that climate change can filterthrough various environmental and ecological sys-tems to affect human health (see Figure 4). Healtheffects related to climate change that we expect tosee in children in New York City and elsewhereinclude heat-wave-related illnesses. We also expectimpacts on air quality. At higher temperatures, air-quality problems that we’re already dealing with,such as summer smog, generally become moresevere. But there’s a range of more complex poten-tial consequences that we’re only beginning tounderstand, includingchanges in the preva-lence of vector-bornediseases. West NileVirus is an example ofa vector-borne diseasethat emerged in thelast seven or eightyears, and is now allover the United States.We are only beginningto understand the waysin which meteorologi-cal changes related toprecipitation and tem-perature will affect thespread of disease. Todate, we do not have
enough scientific research underpinning this tounderstand all these connections. An important goalfor the future is to fill the gaps.
There is a range of health-based air-quality stan-dards that the US Environmental Protection Agencyadministers, such as carbon monoxide, nitrogendioxide, lead, and sulfur dioxide. Since the EPA start-ed working on pollution control in the early 1970sthey have succeeded in reducing concentrations ofthese four pollutants in the United States. Regulationof ozone and fine particles, on the other hand, is amore challenging task. There has been less success inreducing ozone concentrations and fine particle con-centrations (also called PM2.5), which are the smallestpollution particles and can penetrate most deeplyinto our lungs. But these are only a handful of pollu-tants; the mix of pollutants in the environment, espe-cially in New York City, is much more complex. Thereare many other pollutants, including chemicals suchas polycyclic aromatic hydrocarbons (PAH), that havebeen shown by the Center’s research to play specificroles in a variety of adverse health impacts.
We can also tease apart the composition offine particles and find that they are composed of avariety of chemicals drawn from many differentsources, including organic compounds, elementalcompounds, mercury, and nickel, among othersubstances. To really understand the health impli-
Fossil Fuels, Climate Change and Children’s Health: Impacts and Opportunities
Patrick Kinney, ScD Associate Professor and Director, Program in Climate and Health, Mailman School of Public Health,Columbia University
Figure 4Figure 3
Inte
rgov
ernm
enta
l Pan
el o
n Cl
imat
e Ch
ange
Translating Science to Policy: Protecting Children’s Environmental Health
18
cations, and also the climatological relationships,we need to fully examine the constituent elementsof the particles.
Climate impacts and human health impactsfrom air pollution are two sides of the same coin.When we burn fossil fuels we know that the toxicemissions have immediate impacts on children’shealth. At the same time, we also emit carbon dioxidethat is diffusing globally and contributing in importantways to climate change, which has a variety of adversehealth impacts. Climate change itself can influence airpollution, resulting in direct health effects
Projected Effects of Climate Change
I also want to mention the New York Climate andHealth Project, a project started at Columbia that wasdesigned to examine whether climate change couldhave adverse effects on human health, particularly inthe New York region. First, we developed a modelingsystem that took global climate change models andlinked them with regional climate and air qualitymodels. We do not know exactly how global anddomestic policy will evolve for the next 50 to 100years, so we looked at a range of potential scenariosfor greenhouse gas growth. We looked at several dif-ferent time slices: the 2020s, 2050s, and 2080s.
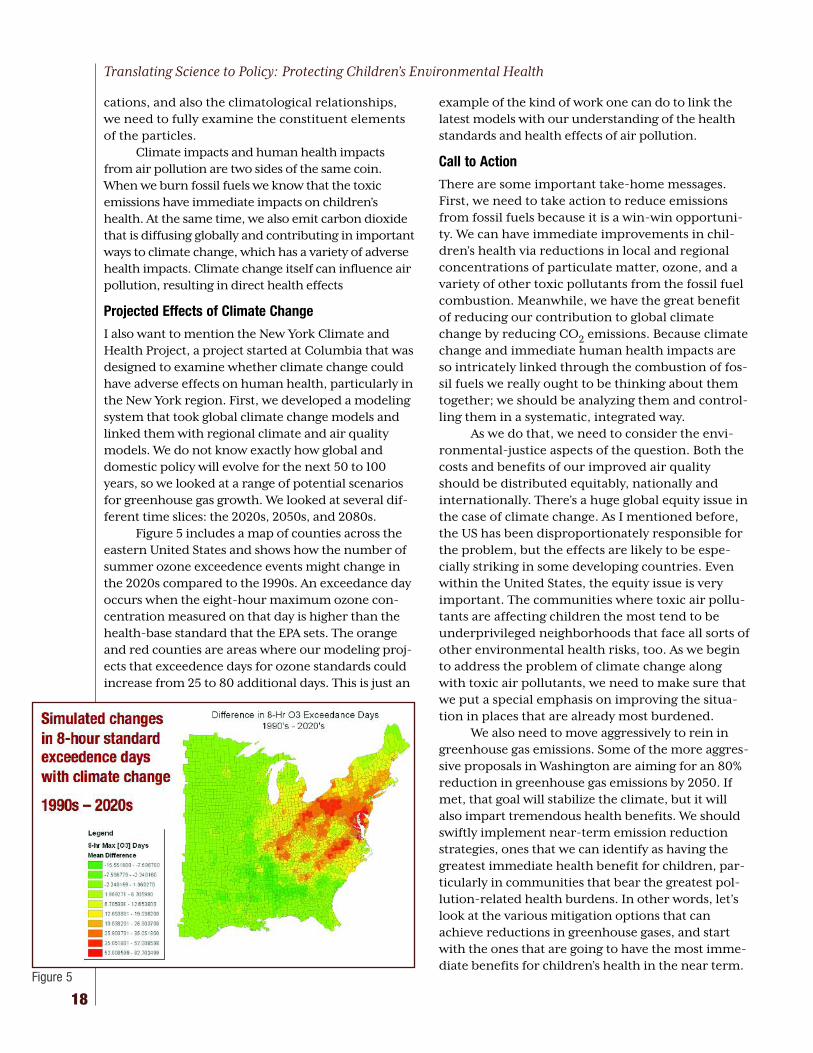
Figure 5 includes a map of counties across theeastern United States and shows how the number ofsummer ozone exceedence events might change inthe 2020s compared to the 1990s. An exceedance dayoccurs when the eight-hour maximum ozone con-centration measured on that day is higher than thehealth-base standard that the EPA sets. The orangeand red counties are areas where our modeling proj-ects that exceedence days for ozone standards couldincrease from 25 to 80 additional days. This is just an
example of the kind of work one can do to link thelatest models with our understanding of the healthstandards and health effects of air pollution.
Call to Action
There are some important take-home messages.First, we need to take action to reduce emissionsfrom fossil fuels because it is a win-win opportuni-ty. We can have immediate improvements in chil-dren’s health via reductions in local and regionalconcentrations of particulate matter, ozone, and avariety of other toxic pollutants from the fossil fuelcombustion. Meanwhile, we have the great benefitof reducing our contribution to global climatechange by reducing CO2 emissions. Because climatechange and immediate human health impacts areso intricately linked through the combustion of fos-sil fuels we really ought to be thinking about themtogether; we should be analyzing them and control-ling them in a systematic, integrated way.
As we do that, we need to consider the envi-ronmental-justice aspects of the question. Both thecosts and benefits of our improved air qualityshould be distributed equitably, nationally andinternationally. There’s a huge global equity issue inthe case of climate change. As I mentioned before,the US has been disproportionately responsible forthe problem, but the effects are likely to be espe-cially striking in some developing countries. Evenwithin the United States, the equity issue is veryimportant. The communities where toxic air pollu-tants are affecting children the most tend to beunderprivileged neighborhoods that face all sorts ofother environmental health risks, too. As we beginto address the problem of climate change alongwith toxic air pollutants, we need to make sure thatwe put a special emphasis on improving the situa-tion in places that are already most burdened.
We also need to move aggressively to rein ingreenhouse gas emissions. Some of the more aggres-sive proposals in Washington are aiming for an 80%reduction in greenhouse gas emissions by 2050. Ifmet, that goal will stabilize the climate, but it willalso impart tremendous health benefits. We shouldswiftly implement near-term emission reductionstrategies, ones that we can identify as having thegreatest immediate health benefit for children, par-ticularly in communities that bear the greatest pol-lution-related health burdens. In other words, let’slook at the various mitigation options that canachieve reductions in greenhouse gases, and startwith the ones that are going to have the most imme-diate benefits for children’s health in the near term.
Figure 5
19
Chlorpyrifos is a broadband organophosphateinsecticide, typically used as an insecticide for agri-cultural purposes, but has also been employed tocontrol pests in residential and commercial set-tings. It is also registered for use on farms. This isthe same substance that was initially introduced asa nerve gas in warfare, so it would seem reasonableto expect that it might be harmful to human beings.
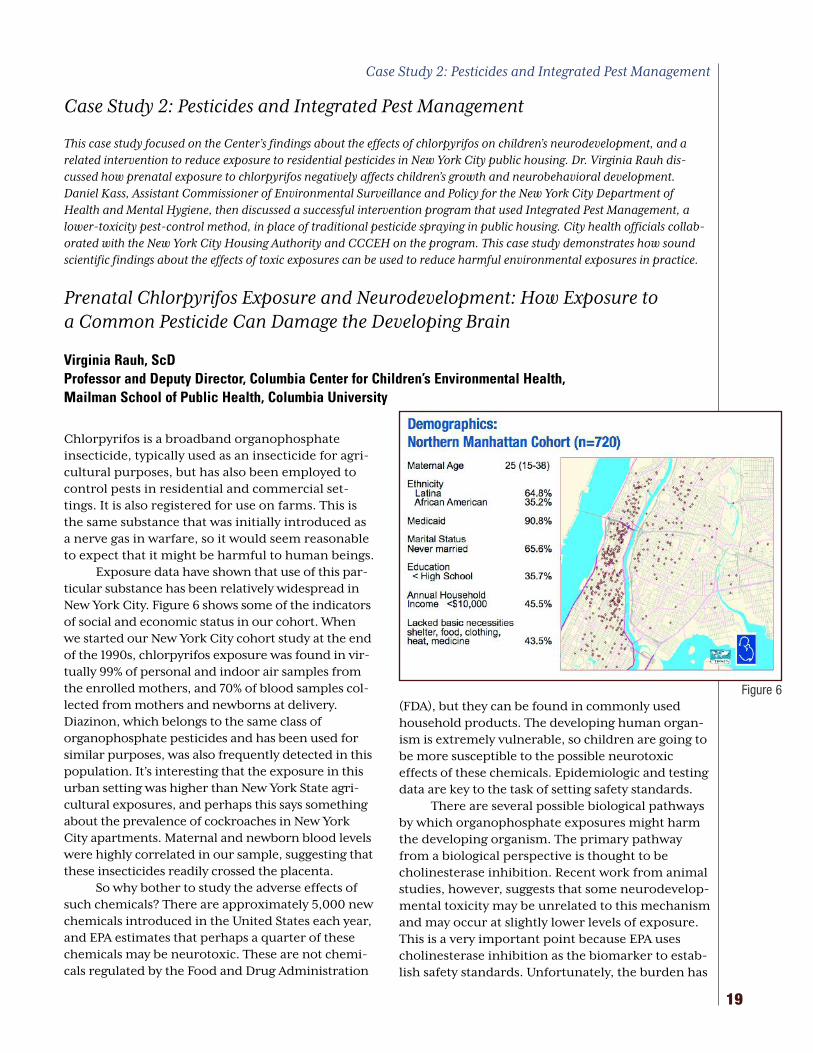
Exposure data have shown that use of this par-ticular substance has been relatively widespread inNew York City. Figure 6 shows some of the indicatorsof social and economic status in our cohort. Whenwe started our New York City cohort study at the endof the 1990s, chlorpyrifos exposure was found in vir-tually 99% of personal and indoor air samples fromthe enrolled mothers, and 70% of blood samples col-lected from mothers and newborns at delivery.Diazinon, which belongs to the same class oforganophosphate pesticides and has been used forsimilar purposes, was also frequently detected in thispopulation. It’s interesting that the exposure in thisurban setting was higher than New York State agri-cultural exposures, and perhaps this says somethingabout the prevalence of cockroaches in New YorkCity apartments. Maternal and newborn blood levelswere highly correlated in our sample, suggesting thatthese insecticides readily crossed the placenta.
So why bother to study the adverse effects ofsuch chemicals? There are approximately 5,000 newchemicals introduced in the United States each year,and EPA estimates that perhaps a quarter of thesechemicals may be neurotoxic. These are not chemi-cals regulated by the Food and Drug Administration
(FDA), but they can be found in commonly usedhousehold products. The developing human organ-ism is extremely vulnerable, so children are going tobe more susceptible to the possible neurotoxiceffects of these chemicals. Epidemiologic and testingdata are key to the task of setting safety standards.
There are several possible biological pathwaysby which organophosphate exposures might harmthe developing organism. The primary pathwayfrom a biological perspective is thought to becholinesterase inhibition. Recent work from animalstudies, however, suggests that some neurodevelop-mental toxicity may be unrelated to this mechanismand may occur at slightly lower levels of exposure.This is a very important point because EPA usescholinesterase inhibition as the biomarker to estab-lish safety standards. Unfortunately, the burden has
Prenatal Chlorpyrifos Exposure and Neurodevelopment: How Exposure toa Common Pesticide Can Damage the Developing Brain
Virginia Rauh, ScDProfessor and Deputy Director, Columbia Center for Children’s Environmental Health, Mailman School of Public Health, Columbia University
Case Study 2: Pesticides and Integrated Pest Management
This case study focused on the Center’s findings about the effects of chlorpyrifos on children’s neurodevelopment, and arelated intervention to reduce exposure to residential pesticides in New York City public housing. Dr. Virginia Rauh dis-cussed how prenatal exposure to chlorpyrifos negatively affects children’s growth and neurobehavioral development.Daniel Kass, Assistant Commissioner of Environmental Surveillance and Policy for the New York City Department ofHealth and Mental Hygiene, then discussed a successful intervention program that used Integrated Pest Management, alower-toxicity pest-control method, in place of traditional pesticide spraying in public housing. City health officials collab-orated with the New York City Housing Authority and CCCEH on the program. This case study demonstrates how soundscientific findings about the effects of toxic exposures can be used to reduce harmful environmental exposures in practice.
Figure 6
Case Study 2: Pesticides and Integrated Pest Management

rested on academic communities and centers likeour own to determine whether there are dangers tothe developing brain via other pathways, and toexamine the relevant levels of exposure and effectsfrom these pathways.
Health Effects
There have been a number of findings to date sug-gesting adverse effects of chlorpyrifos exposure onthe developing child. In 2004, Dr. Robin Whyatt andCenter investigators showed that early exposure dur-ing the prenatal period to chlorpyrifos resulted in a150-gram reduction in birth weight in the infants ofwomen who were highly exposed. The 200-gramreduction in birth weight associated with activematernal smoking in pregnancy is considered adevelopmentally meaningful reduction in birthweight, and the chlorpyrifos effect is comparable.Importantly, the affected children appeared to begrowth restricted. This means that, rather than beingborn early, these children may have completed gesta-tion but did not grow normally. In fact, the infants inour cohort whose mothers were highly exposed tochlorpyrifos in utero were twice as likely to be bornbelow the tenth percentile in size for gestational age.
In 2001, EPA phased out and banned the saleof chlorpyrifos for all residential and indoor use.However, many agricultural uses are still permitted.The residents of farming communities, and theagricultural workers themselves, continue to beexposed. Exposure also occurs through residues onfood. Replacement pesticides are now being used,in particular pyrethroids and carbamates, for pestcontrol in homes and apartments. The long-term
effects of chlorpyrifos on children and adolescentsare still unknown.
Following EPA’s regulatory action, we foundthat chlorpyrifos levels in air and blood samplesbegan to drop immediately. It was amazing to seethe average exposure levels drop among pregnantwomen in this New York City cohort. We had directevidence that the levels of chlorpyrifos werereduced in the air that was breathed as well as inumbilical cord blood samples. Both measuresdropped precipitously over the period immediatelyfollowing the ban.
To touch upon a few of the highlights from theCenter’s pesticide research, we examined children’sdevelopmental progress over the first three years oflife. The Bayley Scales of Infant Development are abroadband test of child development, and showedsignificant deficits associated with high exposure.By 36 months, children with high pesticide expo-sure were starting to fall off developmentally by 3 to5 points, on average, as compared to those with lowexposure. The size of this deficit is educationallymeaningful in the early preschool years, and in factcan push whole groups of children into the devel-opmentally delayed category. We saw the same kindof findings in motor and mental development.
Another worrisome finding concerned possi-ble effects in the neurobehavioral domains. Wefound evidence that a higher proportion of exposedchildren were showing attention deficit problems,as compared to those with lower exposure. Theseproblems included hyperactivity and impulsivity.The nature of these attentional problems is not yetclear, and we are continuing to follow the childrento ages when the clinical assessment of behaviorproblems is more reliable. We also found evidencethat some children had developmental problemsrelated to socialization and self-regulation.
We have continued to follow the children overthe course of the last few years. The bulk of childrenare now reaching the 5-year age range and some havereached 9-10 years of age. Figure 7 shows the develop-mental trajectory. At 7 years of age we’re already find-ing some deficits in the areas of working memory. Thismight be expected if the primary mechanism is affect-ing attention and self-regulation, with possible effectson full-scale IQ measures. These types of deficits couldaffect learning and school performance. We are nowworking to better understand these functional andbehavioral results with new studies, including throughthe use of MRI (magnetic resonance imaging) to iden-tify possible anatomical changes in the brain that mayaccompany these functional disturbances.
Translating Science to Policy: Protecting Children’s Environmental Health
20
Figure 7

21
When we first launched this joint integrated pestmanagement program I am about to describe,1 wesuspected that cockroaches would be a commonproblem. We now know from our own Departmentof Health survey that this is true. But contrary tourban myth, not every New Yorker is subject to thepests. Based on our survey work, 30% of New YorkCity residents have cockroaches in their household(see Figure 8). The disparities by income and raceare enormous. The same patterns of disparity arealso apparent when looking at mice. Slightly fewerhouseholds—about 25%—report mice in their build-ings. In these housing-related conditions, incomeand race and ethnicity are predictive of dispropor-tionate burden.
The same disparate patterns apply to the meth-ods by which households try to control pests. Aboutone in five families in New York use aerosol prod-ucts like sprays or bombs and foggers, but their useis especially common among low-income, non-White populations in New York City. This is partlydue to the fact that these families receive less profes-sional pest control, and because they have morepests. In addition to legal, commercial pesticidesbeing used, people sometimes use illegal pesticidesto control pests.
Study Design
With funding from EPA and the City Council, weestablished a valuable collaboration among the NewYork City Housing Authority (NYCHA)’s TechnicalServices Department, the Health Department, andthe Columbia Center for Children’s EnvironmentalHealth. New York City has the largest housingauthority in North America. It is home to at least400,000 residents, has 180,000 apartments in 340developments, and includes 2,600 buildings. Thehousing authority represents 8.3% of all of New York
City’s rental apartments and a substantial portion ofthe population. If we could influence better pestcontrol in this type of institution, we felt that wecould pave the way for expansion across both gov-ernmental agencies and into the private sector.
Our study addressed three critical questions:1) whether an integrated pest management (IPM)approach was superior to traditional, pesticide-based approaches at reducing pest populations,particularly cockroaches and mice; 2) whether IPMwas more effective at reducing residents’ own use ofhazardous pesticides; and 3) whether IPM was effec-tive at reducing exposure to key cockroach andmouse allergens.
This program was conducted in two neighbor-hoods within New York City: East Harlem, inManhattan; and Bushwick, in Brooklyn. Both neigh-borhoods have high rates of asthma, relative toboth the city’s and the nation’s average. The essen-tial design of the study involved comparing anintervention group of buildings to a control groupof buildings. Our intervention occurred in 13 build-ings in 280 apartments.
We performed the IPM intervention in theexperimental buildings, while allowing traditionalpest control to continue in the control buildings.
A Collaborative Effort to Evaluate the Impact of Integrated Pest Management in New York City Public Housing
Daniel Kass, MSPHAssistant Commissioner, Environmental Surveillance and Policy, New York City Department of Health and Mental Hygiene
Figure 8
Case Study 2: Pesticides and Integrated Pest Management
1. Kass D, McKelvey W, Carlton E, Hernandez M, Chew G, Nagle S,Garfinkel R, Clarke B, Tiven J, Espino C, Evans D. Effectiveness ofan integrated pest management intervention controlling cock-roaches, mice, and allergens in New York City public housing.Environmental Health Perspectives, 117(8): 1219-1225, 2009.

Traditional pest control as generally practiced by theHousing Authority and private landlords ofteninvolves a combination of professional pesticide useand residents’ own use of chemicals. Sometimes,traditional pest control means no pest control serv-ices at all. A combination of interviews, objectivemeasures of pests by trapping, residents’ self-report-ed sightings of pests, and tracking the frequency ofimprovement or deterioration of conditions allowedus to assess the status of residences in terms of pestcontrol at three points in time: baseline, threemonths, and six months.
Unemployed residents within public housingwere hired to form an integrated pest managementteam. We trained them and arranged for them to belicensed by the State to be pesticide applicators. Theintervention involved very simple but labor-inten-sive approaches for deep cleaning, including HEPA-vacuuming wall cavities (HEPA vacuums contain aspecial filter that is able to trap very fine dust parti-cles.) The goal was to reduce both pests and allergenbuild-up by caulking and sealing cracks andcrevices; patching holes in walls with careful use ofgel baits, containers, and boric acid in wall cavities;and providing safer cleaning supplies to residentsthemselves. Due to our limited resources, we didnot provide extensive residential education.
Results
Baseline results showed that cockroach levels meas-ured by the number trapped weekly were higher inthe IPM group than in the control group. At threeand six months after the intervention began, therewas a significant decline in the median weeklytrapped cockroaches in kitchens in the intervention
group, whereas we saw a pattern of growth andthen modest reduction in control apartments—essentially little change at all (see Figure 9).
Success in our intervention was defined aseither substantially reducing within an apartmentthe number of cockroaches, or staying cockroachfree over time. The IPM intervention apartmentswere three times more likely to show successfulreductions in pests than control apartments. Thestudy also asked about residents’ own sightings ofcockroaches, to assess how people felt about theintervention’s impact. In the IPM apartments, therewas a sharp and sustained decline of sightings at 3and 6 months. In the control apartments, there wasno change at 3 months, and some decline at 6months. Changes in the levels of allergens were alsoevaluated in the apartments. Though the programconfined its interventions to kitchens and bath-rooms, we found meaningful reductions in cock-roach allergens in bedrooms. Bedrooms in IPMapartments at 3 months had just 60% the levels ofcontrol apartments, and 40% their levels at 6months.
We also tracked individual’s self-reported useof legal and illegal pesticide products. Figure 10shows a decline in use of these products amongpeople who received IPM services, and very littlechange in the use of such products by people incontrol apartments. If people continued to havecockroaches at the end of the intervention, theywere more likely to continue to use these products.If we can reduce pests, we ultimately reduce the useof hazardous products.
There are some important limitations to thisstudy. It employed a quasi-experimental design,which limits the generalizability of the findings. Wedid not randomize the selection of buildings, butwe tried to match them within a development.
NYCHA was more likely to visit control apart-ments to spray or offer to spray pesticides.Normally, a significant proportion of residentsrefuse or do not make their homes available forthese scheduled visits. Given the nature of thisstudy, however, it is likely the NYCHA reached agreater proportion of control apartments thanwould otherwise be expected.
Because residents within a development share aresident association, we believe that the informationabout this program was spread from experimental tocontrol groups, perhaps lessening the estimation ofthe intervention’s impact, since the control groupmay have benefited from IPM techniques too.
Translating Science to Policy: Protecting Children’s Environmental Health
22
Figure 9
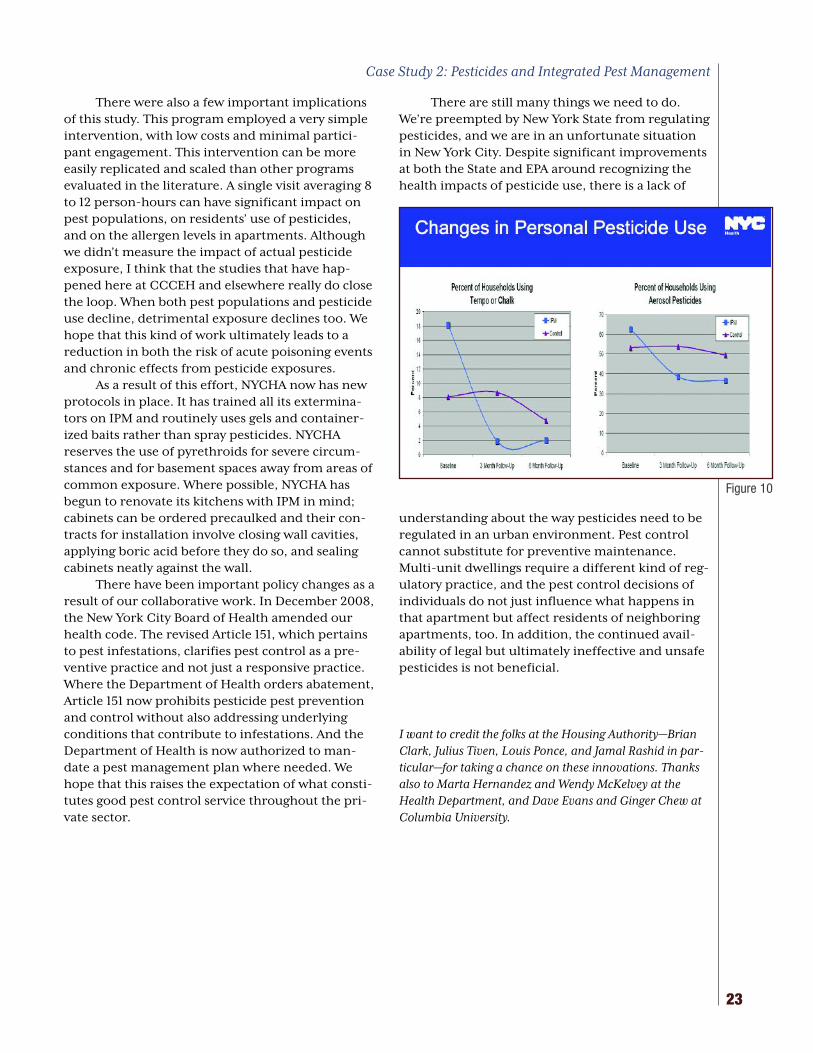
There were also a few important implicationsof this study. This program employed a very simpleintervention, with low costs and minimal partici-pant engagement. This intervention can be moreeasily replicated and scaled than other programsevaluated in the literature. A single visit averaging 8to 12 person-hours can have significant impact onpest populations, on residents’ use of pesticides,and on the allergen levels in apartments. Althoughwe didn’t measure the impact of actual pesticideexposure, I think that the studies that have hap-pened here at CCCEH and elsewhere really do closethe loop. When both pest populations and pesticideuse decline, detrimental exposure declines too. Wehope that this kind of work ultimately leads to areduction in both the risk of acute poisoning eventsand chronic effects from pesticide exposures.
As a result of this effort, NYCHA now has newprotocols in place. It has trained all its extermina-tors on IPM and routinely uses gels and container-ized baits rather than spray pesticides. NYCHAreserves the use of pyrethroids for severe circum-stances and for basement spaces away from areas ofcommon exposure. Where possible, NYCHA hasbegun to renovate its kitchens with IPM in mind;cabinets can be ordered precaulked and their con-tracts for installation involve closing wall cavities,applying boric acid before they do so, and sealingcabinets neatly against the wall.
There have been important policy changes as aresult of our collaborative work. In December 2008,the New York City Board of Health amended ourhealth code. The revised Article 151, which pertainsto pest infestations, clarifies pest control as a pre-ventive practice and not just a responsive practice.Where the Department of Health orders abatement,Article 151 now prohibits pesticide pest preventionand control without also addressing underlyingconditions that contribute to infestations. And theDepartment of Health is now authorized to man-date a pest management plan where needed. Wehope that this raises the expectation of what consti-tutes good pest control service throughout the pri-vate sector.
There are still many things we need to do.We’re preempted by New York State from regulatingpesticides, and we are in an unfortunate situationin New York City. Despite significant improvementsat both the State and EPA around recognizing thehealth impacts of pesticide use, there is a lack of
understanding about the way pesticides need to beregulated in an urban environment. Pest controlcannot substitute for preventive maintenance.Multi-unit dwellings require a different kind of reg-ulatory practice, and the pest control decisions ofindividuals do not just influence what happens inthat apartment but affect residents of neighboringapartments, too. In addition, the continued avail-ability of legal but ultimately ineffective and unsafepesticides is not beneficial.
I want to credit the folks at the Housing Authority—BrianClark, Julius Tiven, Louis Ponce, and Jamal Rashid in par-ticular—for taking a chance on these innovations. Thanksalso to Marta Hernandez and Wendy McKelvey at theHealth Department, and Dave Evans and Ginger Chew atColumbia University.
23
Case Study 2: Pesticides and Integrated Pest Management
Figure 10

Translating Science to Policy: Protecting Children’s Environmental Health
24
…. Translating the empirical evidence of a serioussystematic problem into a rational public policy hasone set of challenges when the public is aware andfamiliar with the problem. It has another set of chal-lenges when the public is largely unaware that theproblem exists, or at least is not conversant with thescope of the problem. Nowhere in pediatric environ-mental health is that more true than endocrine dis-ruption. I say this with a particular sadness, becauseas an ecologist and a public scientist I’ve beenresearching and writing about endocrine disruptionfor 15 years, as have my esteemed colleagues.
In spite of the media attention that this workhas received and in spite of the Congressional brief-ings and the testimonies and town hall meetings andgrand rounds that we’ve all done, most people stillconsider their hormones as a private, innate, inti-mate, interior part of themselves, and not a signal-ing mechanism, a tuning fork, that responds to mes-sages streaming in from the environment that we
inhabit. Nor is it common knowledge that commonchemical contaminants at vanishingly small concen-trations can interfere with natural signals control-ling human development in pregnancy, infancy,childhood, and adolescence. Chemicals used infarming have demonstrable links to early pregnancyloss. For example, the pesticide methoxychlor isknown to interfere with para-hormonal signals thatguide embryonic implantation in the uterus.
Let me be specific. When a woman who wantsto get pregnant and is having a tough time of it goesto the pharmacy to purchase a home ovulation pre-dictor kit in an attempt to increase the efficacy ofher efforts, does she, as she reaches for the box onthe shelf, think about weed control in cornfields?She should. The weed killer Atrazine, the numbertwo pesticide used in the US, which is banned foruse in Europe because it is an endocrine disrupter,is used for this purpose. It’s known to interfere witha hormone from the pituitary to the ovary that gov-erns ovulation. When this woman finds out that shehas endometriosis and decides to undergo laparo-scopic surgery, does she ask herself as she slipsunder the anesthesia, “Hmm, I wonder about thepossible connection between my painful periodsand our nation’s waste disposal practices.” Sheshould. Municipal waste incineration is a leadingsource of dioxin, which is a chlorinated hydrocar-bon that has been linked in primates toendometriosis. If she does succeed in achievingpregnancy only to suffer the acute and particulargrief of miscarriage, does she call her mother to talkabout agriculture? She might.
If this woman carries her pregnancy into thethird trimester only to give birth prematurely andspends the first days of her new life as a mother pray-ing in the neonatal intensive care unit over an incu-
The Health Effects of Endocrine Disruptors on the Growth and Development of Children
Sandra Steingraber, PhDScholar in Residence, Division of Interdisciplinary and International Studies, Ithaca College
Case Study 3: Endocrine Disruptors
This case study focused on the health effects of early-life exposure to phthalates and bisphenol-A, two synthetic chemicalscommonly found in plastics and consumer products that interfere with the body’s endocrine system. These chemicals canmimic or block naturally occurring hormones in the body, and thus are capable of disrupting early development. An abbrevi-ated version of Dr. Steingraber’s remarks appear here. The full transcript is available online at www.ccceh.org/conference09.

25
bator, does she start to wonder about nail polish?Does she ask herself whether the date of her child’sbirthday might have anything to do with our nation’sfailure to regulate endocrine disruptors in cosmeticsand personal care products? She might. Phthalatesare the latest chemical to join DDT and PCBs and theclub of chemicals with the power to shorten humangestation. In the case of PCBs we even understandthe mechanism. PCBs can alter the way calcium flowsthrough uterine muscle tissue, through the calciumchannels, overriding the balance of estrogen andprogesterone that prevent taut muscle tissue fromcontracting in late pregnancy. Calcium is needed formuscular contractions. Pre-term birth is the leadingcause of disability in the United States.
If her child is a son and he’s diagnosed with agenital malformation, un-descended testicles orhypospadias, does the mother start to wonderabout building material specs? She could, becausephthalates are also a compound in vinyl, which is abuilding material, and is known to shorten urogeni-tal distance and be a male reproductive toxicant.
If her child is a daughter who grows up into afourth grader and one night is taking a bath andlooks up at her mother and says, “Mama, there’ssomething hard that hurts inside my chest.” Andthe mother discovers that the lump in her ten-year-old chest is a breast bud, and says, “Well, honey,you’re just growing your breasts,” and the daughtercries and says, “But I’m not ready for that,” does themother think about the world’s plastics manufac-turing? She might. Bisphenol-A is a plasticizer usedto prevent polycarbonate from cracking. It’s foundin the urine of most schoolgirls at levels capable ofaccelerating sexual maturation in female juvenilerats, and early puberty is an outcome of bisphenol-A exposure in mammal studies.
I am the author of a monograph on the envi-ronmental contributions to early puberty in girls(“The Falling Age of Puberty in US Girls.”1) I spenttwo years studying the neuroendocrinology ofpubertal onset, and I tried as a parent to do every-thing right. In spite of my work and the work of OurStolen Future and WE ACT and many in this room,there is still low public awareness about the exqui-site communion between our neuroendocrine sys-tem and the ecological world. There’s a huge cultur-al blindness because, in this culture, we see healthas an individual thing—as if we were all captains ofour own health boats—and if we do see larger forces
at work, we attribute them to genetics or to lifestyle.The idea that the environment might be another legof that triangle of genetics, lifestyle, and environ-ment is not evident to most people still.
Our public policy around endocrine disruptorscan’t wait for a public education campaign to bringthe whole populace up to speed on this and createthe cultural sea change that would be necessary to
recognize the communion between our bodies andthe environment. Policy needs to precede and serveas that educator. In this, I think the example of sec-ondhand smoke is a good one for us. When New YorkState banned public smoking a few years ago, itserved to de-normalize tobacco smoke.
In some cases—and this is probably the mostcontroversial thing I say—I believe that public educa-tion in the absence of decent public policy actuallyworks at cross-purposes. For the past eight years,we’ve had no real chance to make meaningfulnational environmental health policy, nor eveninvest in basic science. The Bush administrationworked to defund the National Children’s Study, forexample. (Happily, it failed.) Into the breach steppedadvocacy groups that tried to educate the publicabout endocrine disruption. They directed theirefforts at parents, whom they addressed as shoppersand consumers—not as citizens. Hence, toxicitybegan to be seen as a choice. Nonprofit advocacygroups provided us with websites on lead and cad-mium in children’s toys. We were offered websiteson safe cosmetics. We were told how to avoidformaldehyde in plywood and why to avoid vinylshower curtains. We were urged not to microwave inplastic. Vigilant parenting replaced meaningfulchemical policy reform. That task required thatevery parent become a chemical engineer and a riskassessor. We became our own regulatory agencies.
And there was a backlash against this. Mostrecently Peggy Orenstein, an otherwise very thought-ful journalist who writes for The New York TimesSunday magazine, wrote an article called “ToxicParadox.” In it, she describes her reaction to being
1. Available on the Breast Cancer Fund website:http://www.breastcancerfund.org/site/c.kwKXLdPaE/b.3266509/k.27C1/Falling_Age_of_Puberty_Main_Page.htm
Case Study 3: Endocrine Disruptors
“Our public policy around endocrine disruptors can’t wait for apublic education campaign to bring the whole populace up tospeed on this and create the cultural sea change that would benecessary to recognize the communion between our bodies andthe environment. Policy needs to precede and serve as thateducator.”

Translating Science to Policy: Protecting Children’s Environmental Health
26
presented with evidence of dangerous air pollutionnear her child’s school. Already worn out from tryingto keep harmful pesticides and harmful toys awayfrom her child, her response is to kill the messenger.
Sociologist Rebecca Altman wrote a counter-point to that essay in Environmental Health News. Shepoints out the plight of parents who have gonegreen at home only to recognize the modest effectsof their actions for kids overall means that we haveto feverishly scan the internet for green products toavoid headline-grabbing chemicals, only to learnthat research implicates another chemical andanother product, so that our efforts become onlypartial solutions until they’re finally part of theproblem, too, because we don’t want to hear any-thing more about air pollution because we’ve hadit. We’ve already used up all our anxiety about this,trying to find the right lunchbox.
I’m going to close now by talking about somenew science. And here I’m going to speak from theperspective of a mother of two school-aged chil-dren, one a son and one a daughter. I’ll start withphthalates, which are a male reproductive toxicantand therefore a pediatric heath threat to my son,Elijah, who is seven.
Phthalates provide car interiors with theirunmistakable new-car smell. You’ve all smelledphthalates. They are an ester of 1,2-benzenedicar-boxylic acid. They’re used to soften plastic, namelya form of plastic called vinyl, which is 50% chlorineby weight. There are many kinds of phthalates.Those with high molecular weights are used invinyl. Those with lower molecular weights are anoily substance used in perfumes and hair spray andpersonal care products.
Phthalates have as their target of endocrinedisruption the testicle. They are linked to lowersperm concentration and motility.2 Earl Gray’s labat EPA has looked closely at phthalates and explicat-ed the vulnerability of the fetal male genital tract toendocrine disruption by phthalates. Gray and histeam looked at a birth defect called hypospadias, inwhich the urethra does not roll up and have itsopening at the tip of penis but rather along theshaft somewhere.3 There’s a name called phthalate
syndrome for this combination of different kinds ofmale reproductive disorders. It’s one subset ofwhat’s called testicular dysgenesis syndrome, whichis a frightening phrase for a mother to say.
One billion pounds of phthalates are manu-factured each year. Researchers here at theColumbia Center for Children’s EnvironmentalHealth, as part of their Mothers and NewbornsStudy in Harlem and the Bronx, persuaded verypregnant women in the last trimester to wear abackpack containing a personal air monitor. Themonitors measured actual levels of phthalates inthe air that women breathed during pregnancy. Theresearchers found that almost 100% of these womenhad phthalates in their personal air samples. Mosttroubling: one form of phthalate, DEHP, was associ-ated with shorter gestation.
Perfume use is linked to higher level of uri-nary metabolites of phthalates in women of repro-ductive age. We need to know how much phthalatescome to us from inhalation and by ingestion infood. What we do know is that 95% of us havephthalates in our urine.
Bisphenol-A is a plasticizer used to softenpolycarbonate. It’s used in food and beverage con-tainers. The CDC estimates that bisphenol-A isfound in 92.6% of Americans’ urine. It’s higher inchildren and teenagers than in adults. A pilot studyby Mary Wolff found bisphenol-A routinely in theurine of six- to eight-year-old girls.4 Bisphenol-Awas first synthesized in 1891 as a pharmaceuticalestrogen, but DES, Diethylstilbestrol, was found tobe more potent so bisphenol-A was abandoned forthat purpose. It has been linked to diabetes andobesity, and early puberty, which in turn is linkedto increased risk of breast cancer. Early puberty isalso linked to increased risk of violent victimizationduring adolescence, increased risk for depressionand substance abuse, and early sexual initiation.Bisphenol-A triggers early onset of sexual matura-tion in female rodents and stimulates breast devel-opment. The stimulation of breast development isthe target of bisphenol-A. In animals studiesbisphenol-A exposure in infancy makes breast tis-sue more sensitive to estrogens at puberty. …
2.Hauser R et al. “Altered semen quality in relation to urinary concentrations of phthalate monoester and oxidative metabolites.”Epidemiology. 2006 Nov 17(6):682-91.
3. Wilson VS et al. “Phthalate ester-induced gubernacular lesions are associated with reduced insl3 gene expression in the fetal rattestis.” Toxicol Lett. 2004 Feb 2:146(3):207-15.
4. Wolff MS et al. Pilot study of urinary biomarkers of phytoestrogens, phthalates, and phenols in girls. Environmental HealthPerspectives. 2007 Jan 115(1):116-21.

27
Studies tell us that race, class, and income are keydeterminants of health status, as well as higherenvironmental and occupational exposure. Yet,despite the fact that longevity is increasing formany Americans, mortality and morbidity hasincreased for others. One concern in addressingexpanding health disparities is that the emphasis isnot on primary prevention.
The good news is that there is a growingawareness of community conditions for health. Werealized that the most powerful factors shapinghealth and disparities are social and economicdeterminants. First, we have root factors of povertyand discrimination that play out at the communitylevel. Then there are community-wide environ-mental conditions that influence health directlythrough toxins in air, water, soil, and buildingmaterials. Indirectly, those affected by health dis-parities tend to live in environments without accessto nutritious food, spaces for active living, effectivetransportation systems, but they have ready accessto unhealthy products like cigarettes, alcohol, andfast foods. Combine these factors with lack of accessto quality medical services and we have a good pic-ture of the landscape of health disparities for com-munities like Northern Manhattan and the SouthBronx. The results from the Center’s study here aretypical of exposures being experienced by otherenvironmental justice communities around NewYork City and around the nation.
As a long time environmental justice advocate,I know that race and socioeconomic status areimportant risk factors locally and globally for pre-dicting the location of noxious facilities, the levelsof exposure, health disparities, and the effects ofclimate change. The dynamics of environmentalinjustice have led to excess exposure to environ-mental hazards, community devoid of green bene-fits, and lack of participation in democratic deci-sion-making that affects the lives of residents. It’sthese dynamics that have seized my attention, mycommitment and energy over the last 20 years.
When I first began organizing around theseissues in 1985, I recognized that the lack of scientificliteracy, information, and context was and contin-ues to be a factor that contributes to the inaction of
policymakers and to the systemic exclusion of low-income communities of color from decision mak-ing. As a result, WE ACT was founded in 1988 toinstitutionalize advocacy and organizing inNorthern Manhattan, to build community power, toimprove environmental health, policy and protec-tion in communities of color. We believe that we’rehaving impact on the field through new models ofcommunity-based environmental action, combin-ing community organizing with policy initiatives atthe local, state and federal levels. We have helpedadvance the perception and reality that it can bebeneficial to work with affected communitieswhether the goal is to document environmentalexposures, intervene in housing hazards, or devel-op a waterfront park for active living the way wenow have at 125th Street and the Hudson.
To address some of these concerns, the envi-ronmental justice movement has raised its voicewith disempowered communities and we’ve takenaction to develop the community capacity tobecome effective stewards of healthy homes andhealthy schools. We organized residents to engagedirectly in the design and implementation of solu-tions that make sense, solutions that lead to sus-tainable homes and healthy schools, and schoolsthat we will not allow to be built on brownfield siteswith no environmental review, the situation wenow have with the City refusing to allow environ-mental review on leased sites.
Translating Research Into Policy and Action
Translating Community-Based Research into Policy and Public Health Action
Peggy ShepardExecutive Director, WE ACT for Environmental Justice

So we have a moral obligation to help stop thebad stuff, as reported in a recent New York Times arti-cle on green groups and diversity. But guess what?When we stop the bad stuff and impact the politicalwill, we will bring the good stuff, too. And that par-adigm has sparked the new green economy,renewed investment in our built environment, andcatalyzed exciting new collaborations that are mak-ing a difference. By taking action, families andadvocates who supported a lead poisoning bill in2004 helped improve the potential for many of our
children. Over 90% of new lead poisoning cases arechildren of color living in the ten worst neighbor-hoods for lead poisoning risk. By taking action, WEACT stopped the City from reopening and triplingthe size of Manhattan’s only 24-hour marine trans-fer station (MTS) that would have drawn 300 dieseltrucks per day to West Harlem. “We have the lion’sshare, not the fair share,” we said, and the Mayorheard that and he changed course in developing theCity’s solid waste plant. As a result, the City hasagreed to work with WE ACT and Community Board9 to organize residents in a planning charette forthe community reuse of the 27,000 square foot MTSfacility in the Hudson River. That marine transferstation will now be transferred to the ParksDepartment by Department of Sanitation, and thatfacility, adjacent to the new West Harlem waterfrontpark, will be renovated to community use. Lookingback, if it were not for the hundreds of residentswho mobilized around the operations of the NorthRiver Sewage Treatment Plant back in the ‘80s and‘90s, the City would not have committed $55 mil-lion to fix the plant, to stop the odors and emissionsthat were making people sick, and WE ACT mightnot be here as a partner with the Children’s Center.
It was that campaign to stop odors and emis-sions from North River that were making kids andfamilies sick that led to the community demandinghealth studies to understand their exposure to pollu-tants. It has been the air quality data on exposure andoutcomes that has led to the MTA using cleaner fuels,hybrid technology, and diesel retrofits on all its buses.The MTA has the largest fleet in the nation, and hous-es one-third of that fleet in northern Manhattanneighborhoods. WE ACT’s 18-year campaign, “CleanFuel, Clean Air, Good Health,” has made a difference
in New York City’s public health, and the data fromtwo Columbia centers and the help of allies likeEnvironmental Defense Fund and the NaturalResources Defense Council have helped us create realchange here in this community.
Ten years ago WE ACT began a partnership withthe Children’s Center. Earlier we had begun workingwith researchers like Pat Kinney and Mary Northridgeand the NIEHS Center for Health in NorthernManhattan to engage residents in documenting expo-sure of students in the West Harlem community todiesel. That collaboration yielded important data forthe community as well as four peer-reviewed pub-lished articles on air quality and the value of academiccommunity partnerships. It has been a rewardingexperience to educate youth as field technicians toengage in community-based participatory researchand to co-author articles in our work.
Now, fortunately, the ten years of work withthe Children’s Center has yielded answers aboutenvironmental exposures that community resi-dents have wanted to know. This data has addressedour concerns. These research findings haveempowered residents and advocates, and the part-nership was chosen as one of ten KelloggFoundation case studies that was authored byMeredith Minkler and published in the New YorkAcademy of Medicine’s “Journal of Urban Health.” Itfound that carefully designed community-basedparticipatory research that is committed to strongscience, high level community involvement,engagement in policy steps and activities, and thestrategic use of study findings to help impact policycan be an important part of the broader struggle forurban health and environmental justice. The papercited accomplishments like the partnership’s role inthe conversion of New York City’s bus fleet to cleandiesel, and the installation by the EPA of permanentair monitors in Harlem and other hotspots.
With Columbia researchers, we have devel-oped a daylong training for 60 community healtheducators, and over 300 community residents havegraduated from a six-week environmental healthand justice leadership training program. We’ll con-tinue working with our graduates in a new stake-holder collaborative supported by EPA’s CARE pro-gram that will identify, prioritize and reduce risksin northern Manhattan communities.
During these years, WE ACT has also beenprincipal investigator on several NIEHS grants thathave allowed us to develop relationships with aca-demics and to build our capacity to engage in com-munity-based research, and advise the Center on
Translating Science to Policy: Protecting Children’s Environmental Health
28
“I believe we need a clear dialogue between researchers andpractitioners aimed at highlighting the role of communityconditions in shaping health disparities.”

29
communication with participants and on other eth-ical issues. We have been able to hire staff withadvanced degrees in environmental health and sci-ence, and provide technical assistance with ourlocal, regional and national environmental justicecommunity. And we have leveraged additionalfunding for our partnerships from foundations thatunderstand the importance of building healthycommunities with residents.
By making environmental data and researchaccessible and relevant to community residentsthrough City-wide campaigns, such as Our Housingis Our Health, that translate relevant findings intopractice and policy, the partnership helps ensurethat City policies related to environmental healthand indoor air quality are informed by the latestand most relevant research. Through the campaign,member groups around the City are linking theirorganizing and advocacy work with legal strategiesacross traditionally very separate fields, such as civilrights, land use, housing, environmental and publicpolicy, to change policy in housing violations thatcontribute to poor indoor air quality and an epi-demic of respiratory disease. One campaignachievement was getting the City’s health and hous-ing agencies together in the same room so that theycould develop consistent guidelines for mold reme-diation. We developed a report on mold in housing,“The Silent Epidemic,” with the Public Advocate’soffice, and we held state government accountableto implementing a state mold task force that hadbeen legislated but never created.
Center findings have been employed in secur-ing support from council members for passage ofLocal Law 36 on pesticide notification and LocalLaw 37 on Pesticide Use Reduction Act. We havehelped achieve legislative aims, such as the DieselEmission Reduction Act of 2006, and we’re workingto strengthen the state’s anti-idling regulations forschool buses and to hasten the use of the best alter-native technology for school bus conversions, thedirtiest vehicles on the road.
Most recently the Just Green statewide coali-tion that WE ACT helped to develop and convenehas facilitated a legislative initiative in the StateSenate on bisphenol-A, and we are working withour local State Senator, Bill Perkins, who will intro-duce a bill on comprehensive chemical policyreform. So these are some changes we can believein and get behind. “Where we live, work, play, go toschool”—you hear that a lot now. That’s the way the
environmental justice movement redefined theenvironment 18 years ago. Our vision and agendafor the coming decade places communities at thecenter of dialogue, planning, action and change.
What are some of the lessons I would like toshare with you? I’ve learned that community-basedparticipatory research partnerships are critical tounderstanding place-based exposure of families,getting the expertise of affected residents, and forstudying cumulative risk and synergistic effects ofpollution. We need to ensure translation of researchfindings to participants, and to community resi-dents. We need to make sure that our communitiesunderstand government regulations and mobilizefor policy reform. We need to expand the capacityand training of low-income communities of color toimprove children’s health, and we need to developnew partners across interdisciplinary sectors. Andwe must ask ourselves how do we lay the ground-work for a movement to reduce health disparities? Ibelieve we need a clear dialogue betweenresearchers and practitioners aimed at highlightingthe role of community conditions in shaping healthdisparities. We need to make houses and apart-ments healthy homes by examining the built envi-ronment where poverty, environmental conditions,and poor design combine to cause or exacerbatedisease. We need to build health considerations intoland use, zoning, permitting, community design,and other urban planning decisions that shape thelong-term nature of our built environment. And weneed to study the concept of health impact assess-ments being tried out in San Francisco, where thecommunity identifies its idea of the physical andsocial characteristics of healthy neighborhoods andthen the city develops a process to incorporatethose elements as goals of the rezoning process.
We need to focus on the long view and askourselves: Are we living longer, healthier lives, arewe building strong human communities, are wehanding down to our children a world that is dete-riorating or a place whose natural heritage is beingrevitalized? Those are key questions that representgreat challenges but also great opportunities. It hasbeen my pleasure and excitement to be here todayto really look at the breadth and scope of what wehave learned over the last ten years and to summa-rize that for you and to talk to you about how wehave been able to translate this wonderful researchinto policy.
Translating Research Into Policy and Action

Translating Science to Policy: Protecting Children’s Environmental Health
30
Brian Lehrer, MPH, Host,The Brian Lehrer Show,WNYC Radio, am820, 93.9fm
It is my honor to be at this con-ference. This is truly a new dayin the United States for oppor-tunities to make environmentalpolicy. The Obama administra-tion knows that they have awindow of opportunity rightnow. It would seem logical tome that they try to use thepolitical capital that they have,and the honeymoon period
that a new administration has, to do as much asthey can. This is the perfect time to be having thisconference to talk about the intersection of scienceand policy. I’m delighted to moderate two greatpanels today.
Rachel Miller MD, FAAAAI, Associate Professor of Medicine and Environmental Health Sciences (in Pediatrics) at New York–Presbyterian Hospital/Columbia University Medical Center
As a lung physician I think that it’s important tokeep in mind the statistics about asthma.Approximately nine million children have a lifetimeasthma diagnosis. We are aware that there is unfor-tunately a substantial disparity in susceptibilityaccording to socioeconomic groups, which is closelyrelated to ethnicity. Also keep in mind that therewere approximately 3,780 deaths from asthma inthe US in one year, which calculates to about tenpeople a day who die from asthma annually.
On the brighter side, due to advances in treat-ment, between 1990 and 2000 asthma hospitalizationsin New York City have actually decreased by 17%, whichexceeds the 13% reduction that had been seen nation-wide during this same time interval. And very fortu-nately, there actually has been a 35% decrease in pedi-atric admissions for asthma between 1997 and 2000.
Living in areas with high volumes of traffic hasbeen associated with respiratory problems andasthma in children. In particular, exposure to dieselemissions is a big focus of our medical research.This includes reports that higher levels of fineambient particulate matter, which includes dieselexhaust emissions, has been associated withdecreased lung function among children living incities, including New York. Higher diesel exposurehas been associated with a greater likelihood ofdeveloping allergies. In addition to diesel and par-ticulate matter, other air pollutants have been asso-ciated with respiratory problems. These includeexposure to polycyclic aromatic hydrocarbons(PAH), nitrogen dioxide, and ozone and sulfur diox-ide. PAH have been associated with higher rates ofcough, wheeze, and possible asthma and ear infec-tions in infant children. Prenatal exposure to nitro-gen dioxide has been associated with impaired lungfunction. Ozone and sulfur dioxide have been asso-ciated with emergency room visits for asthma.
There are many mechanisms as to why air pol-lution may be a problem for breathing and for thelung. We know from a number of studies that airpollution exposure, meaning air pollution exposureprenatally in the womb and also shortly thereafterwhen the lungs are continuing to develop, can actu-ally affect lung development. There have been anumber of immune changes that have been associ-ated with air pollution exposure, including effectson our overall inflammatory response, the differen-tiation of some of our immune cells, and the pro-duction of some of our mediators, such as cytokine,as well as processes related to oxidative stress. I’dalso like to mention that diesel exposure has beenassociated with changes in airway remodeling,which refers to what we think are permanentchanges in the cell structure of our lungs that dieselpollution may induce.
There is some good news that I’d like to high-light, in which we’re able to document improve-
Panel 1: Addressing Urban Air Pollution and Climate Change
This panel discussed viable options for reducing the effects of air pollution and climate change in urban areas like New YorkCity. Panelists discussed policy proposals that would target sources of air pollution that contribute to climate change andmore immediate adverse health outcomes (discussed in the cases studies), such as reducing vehicle emissions and idling.Others suggested changes in infrastructure, such as repowering power plants with cleaner fuel alternatives and replacingboilers in homes to utilize energy more efficiently and emit fewer pollutants in the air. Several panelists noted the dispropor-tionate burden of adverse effects from air pollution and climate change on disadvantaged communities. In light of the bigchallenge presented by urban air pollution and climate change, the panelists emphasized the need to work together to advo-cate for effective policy changes at the city, state, and federal levels.

31
ments. One large study inSwitzerland documentedsignificant declines in ambi-ent exposure to particulatematter over an 11-year peri-od between 1991 and 2002.This was associated withimprovements in lung func-tion. Furthermore, CCCEHhas documented reductionsin the ambient levels of PAHfrom 1998 to 2006 in ourNYC cohort. In addition toour research, we translateour findings throughnewsletters, through med-ical associations, andthrough review articles so wecan get this information out to doctors and familiesand parents and legislators. There’s clearly muchmore that we need to do, however.
John Balbus, MD, MPH, Chief Health Scientist,Program Director, Environmental Defense Fund
My comments will address the policy interventionsthat can be taken to get at this complex intersectionof urban life, climate change, and children’s harm-ful exposures to air pollution. New Yorkers as agroup have the smallest carbon footprint per per-son in America, yet they still breathe some of themost polluted air east of California. A lot of thatpollution wafts in from the west from coal-firedpower plants and industrial facilities, but a lot of achild’s exposure in the City comes from very localsources, such as school buses, trucks on the street,highways nearby, and building chimneys. How dowe get at that nexus of greenhouse gas reductionand protecting children’s health from these harmfulair pollutants? It’s not necessarily the easiest thing.Obviously there’s some relatively low-hanging fruitthat we have in terms of fuel efficiency and buildingefficiency. I’m not going to talk a lot about them,but reducing carbon dioxide really requires shiftingour complete transportation-energy infrastructureaway from fossil fuels. That’s a big policy question.There’s a lot that needs to be done.
What I want to do in three to five minutes is tokeep it really simple, and I’m going to boil it down tothree letters: DPF. It stands for a diesel particulatefilter. If you place a DPF on the tailpipe of a dieselengine, it takes out about 90% of the diesel particu-late, most of which is made out of black carbon.There is a bill that was passed several years ago—the
Diesel Emissions Reduction Act—which authorized$500 million for putting diesel filters on existingdiesel engines. It was one of those semi-fundedmandates. A lot of that money wasn’t actually appro-priated, but $300 million has been appropriated inthe Stimulus Bill, and EPA has just announced grantsfor localities, cities, and states to apply for dieselreductions. So that’s a way to get at all of these exist-ing diesel engines that aren’t going away anytimesoon that are in the meantime spewing out a lot ofharmful pollution and black carbon.
We’ve been hearing a lot about black carbonfrom a health perspective, especially its respiratoryimpacts. There are also some alarming neurodevel-opmental impacts that seem to be associated withblack carbon, and good studies are being done out ofthe Harvard School of Public Health looking at traf-fic-associated black carbon exposures and decreasedneurodevelopment. There’s also a lot of new scienceand concern about black carbon as a greenhouse gas.People are saying that black carbon is the second-strongest contributor to global warming after carbondioxide. It’s much shorter-lived, so it doesn’t have thesame implications long-term, but in the near term itseems to have a very significant impact, and it may bea very important bridge between a carbon-based anda non-carbon-based energy system.
Although New Yorkers have a very small car-bon footprint in terms of CO2 per capita, we candefinitely shrink the black carbon footprint. Indoing so, we not only score a big win for children’senvironmental health, especially in areas that arehardest hit by asthma and exposure to diesel pollu-tion, but we also can do a short-term, much-need-ed fix on global warming.
Panel 1: Addressing Urban Air Pollution and Climate Change
Panelists R. Miller, J. Balbus, R. Aggarwala, M. Gelobter, and C. Corbin-Mark

Translating Science to Policy: Protecting Children’s Environmental Health
32
There are other things that need to be done.One of the other obvious low-hanging fruits in a citylike New York is doing away with engine idling, andthe City is taking this up, having just signed into law amuch tougher one-minute idling law. Enforcing thislaw saves fuel, saves money, and saves children’slungs. We’re also working with New York City to try toclean up the dirty fuels that are used in buildings. We
worked for a long time to get the gasoline cleaner andto get the sulfur content of diesel cleaner, but build-ings in New York are burning some of the dirtiestfuels. Shifting from the number 4 and 6 heating oils,which have high pollutant content, to cleaner types offuels are policies that really are low-hanging fruit.They can be done very quickly at the local level in acity like New York, or in any city around the country.
Bigger issues require addressing our trans-portation system, addressing transportation effi-ciency, and moving toward non-motorized forms oftransportation whenever possible. These are veryimportant for children’s health and for reduction ofgreenhouse gases.
It is a lot to do, but there are so many win-winsituations out there that are good for the economy,good for children’s health, and good for long-termsustainability. We really have to seize this opportuni-ty, seize the funding mechanisms that have just beenput into place, and start acting on them. We reallyneed to keep children at the center of our concernsand at the center of our plans about climate changeand air pollution. Not only are they especially vul-nerable to the harmful effects of tailpipe andsmokestack pollution, but they and their childrenare going to have to live on the planet that we leaveto them, so we’ve got to make that the atmosphere isas clean as it can be both in terms of greenhousegases and in terms of toxic air pollutants.
Michel Gelobter, PhD, CEO, Cooler, Inc.
I have five points to discuss how we can achieve someof these changes. First of all, I’d like to say that it’s ourtime to fix this problem. We’re at an unprecedentedmoment of debt accumulation, as we’re all aware,unfortunately. The bailout is likely to leave each andevery American with a $75,000 debt. It’s better thanIceland, where they have a million dollar per capita
debt, but it’s huge. At the level of climate, we each emit12 times more than we should. In this country, weshould be able to have a sustainable, stable atmosphereand climate. We’re at a moment when it has becomeclear that we’ve been managing our resources com-pletely unsustainably, borrowing from the future, andcontinuing to do so to dig ourselves out of the econom-ic and environmental holes we’ve dug ourselves into.I’m sure people at this conference are aware that fossilfuels are like cigarettes or tobacco for the planet as awhole. They take money out of our communities, theypollute our environment, they lead to all the impactsand effects on children’s health, and they waste ourlives and our resources. The first point is that this is thetime to act on the kinds of things we’re talking about atthis conference, and we have a grave responsibilitythat’s tied to the crisis in our country today.
The second is that there is a tremendousopportunity in working on climate change becauseit’s one of the few issues where there’s almost acomplete confluence between justice and efficiency.Climate change is a problem of justice, inter- andintragenerationally. Some people have used more ofthe atmosphere than they had a right to, than wassustainable, and are precluding the use of thatatmosphere and those resources for others, haveprecluded it, and will continue to do unless we takeaction. So it’s clearly a justice problem.
But the second point is if you solve it by sort ofhanding a lot of capital to the polluters—for exam-ple, giving permits to polluters in a cap and tradesystem—I call it paying the pusher for the cure.That’s not an efficient solution. It’s one that wastescapital and it’s one in which there will be tremen-dous credit default swaps, which will not work. Theright way to do it is to make us all owners of thesolution, make us all owners of the capital we haveto invest to move away from fossil fuels, and makeus all owners of the right to emit by charging pol-luters, making them pay, and making sure that theresources we get from those charges go back to ourcommunities in ways that help us transition to aclean energy future.
The fourth point is not to let them make usown the problem. A lot of us in this field believe it’sgoing to be so difficult. That’s true—it will be hardfor those of us who are activists. But the world wewant and the world we’re headed toward will bemuch better. Let’s take, for example, the war inIraq, which was about oil. It’s estimated that thatwar will have cost $3.5 trillion. What’s $3.5 trillion?$3.5 trillion equates to a $100,000 piece of land witha $250,000 home on it, $60,000 worth of furniture,
“We need to keep children at the center of our concerns and atthe center of our plans about climate change and air pollution.Not only are they especially vulnerable to the harmful effects oftailpipe and smokestack pollution, but they and their children are going to have to live on the planet that we leave to them.”
and a $40,000 car in the garage for each and everyperson in the State of New York. Having spent that,there would still be enough money left to build 250libraries at a cost of $10 million, and 500 schools ata cost of $20 million apiece. The rest of the moneycould be placed in an interest-bearing account tofund 10,000 teachers, 10,000 librarians, and 10,000nurses at an annual salary of $65,000 apiece, andstill we’d have enough money left to pay each andevery resident in the State of New York $8,500 ayear, not just this year, but forever. That’s $3.5 tril-lion. So the next time someone tells you that wherewe’re headed is hard, you tell them about how hardwhat we’re doing today is.
And finally, the last point is to hold hands. Thesolution really is a battle between a 90-minute com-mute in a car to a tract home, and walking. Those ofyou who live in New York get to do this every day,walking to school with your kids, five fingers inyour fingers, or linking arms with your partner asyou walk to and from work. It’s about community,and it’s about the five fingers on your hands.
Rohit Aggarwala, PhD, Director, Office of Long-TermPlanning and Sustainability, Mayor’s Office ofOperations, City of New York
I have two broader issues I’d like to discuss. One is tobuild on something John said about the low-hangingfruit. I think one of the things we all have to bear inmind is that the low-hanging fruit is still pretty highup, and it requires a certain amount of work to get.And as Michel said, the real challenge here is goingafter the areas where solutions can clean the air, canpromote justice, can protect the planet, and can alsopay for themselves and save us money.
The remarkable thing is how many of thoseopportunities we as a society, as a nation, as a City,leave on the table because organizing ourselves toget there, even when the economics makes sense,can be very difficult. Here are a couple of examples.One is in power plants. We are committed to explor-ing and bringing large amounts of renewable energyto the City, but we do know that’s some time away.There are shorter-term opportunities that involvefossil fuels, but involve far less fossil fuels than wecurrently have. And yet we face, both within the Cityand due to the regulatory structure that the Stateimposes, tremendous obstacles to things such as therepowering of power plants where you can replace anatural gas turbine that’s 30 years old, install a newone, get more power out of it, have half as muchcarbon emissions, half as much natural gas con-sumption, and 90% less criteria pollutants emitted
from that power plant. The economics makes senseif you look at it in one way, but when you take intoaccount the way electricity prices are set, you’ve gotto get a number of people aligned in order to makethose opportunities a reality for the City.
And yet opportunities can be very powerful.We did our carbon inventory for New York City andlooked at the years from 2005 to 2007. The single-largest improvement in our carbon footprint wasthe opening of the new power plant in Astoria. It’ssurprising to think that a big 500-megawatt fossilfuel power plant contributed a 5% reduction in NewYork City’s entire carbon footprint. But it’s truebecause it pushed obsolete, less-efficient power sup-plies out of our supply stack.
We also know that there are huge opportuni-ties to make our buildings more efficient. By chang-ing light bulbs, insulating pipes, fine tuning boilers,and doing things that may not require much in theway of capital investment, individuals could get a 5%reduction in energy consumption, 5% less pollutionin the air, and reduce the amount of electricity weconsume. Overall, these simple changes can lead toa reduction in fossil fuels. Yet we still have tremen-dous barriers in the way leases are structured, in theway our incentives are organized, in the way our taxcode is organized, and in the way we do not requirethese things citywide to achieving them.
I think one of the things I have learned in thepast two or three years now is that we have to thinkabout this differently. I think some of the opportu-nities that we’ve been exploring, with theEnvironmental Defense Fund and with WE ACT andwith others, show that we are now more comfort-able with the idea of pushing people to places theyought to go. I also think as a City, we are focusedmost on those places that save us money, clean theair, and reduce carbon to start.
Cecil D. Corbin-Mark, MPhil, Deputy Director,WE ACT for Environmental Justice
Just for basics, how are air pollution and climatechange linked, and how does that connect to ourpublic health? In terms of climate change, the sunheats the Earth, and two-thirds of that heat getsabsorbed in the Earth and the remainder returns tothe atmosphere. The greenhouse gas effect is aresult of our production systems, transportationsystems, and our energy systems. These systems areputting gases into the air that essentially trap moreof that heat than the planet was designed to con-tain. Some of those gases are produced by thingslike diesel buses that burn diesel fuel and put car-
33
Panel 1: Addressing Urban Air Pollution and Climate Change
Translating Science to Policy: Protecting Children’s Environmental Health
34
bon into the air, or power plants that may be inyour neighborhoods that also put fossil fuels intothe air. In terms of climate, we’re seeing someimpacts like heat waves and impacts that are caus-ing more respiratory illnesses.
For more than a decade now, we’ve been in apartnership with the CCCEH and other research
centers at Columbia. CCCEH research findings haveshown that the abundance of diesel pollution inNorthern Manhattan and the South Bronx is directlylinked to decreasing circumference of heads of thebabies in our communities, lower birth weight, andearly onset of asthma and other types of respiratoryillnesses. This is not a surprise to many of the resi-dents that we organized with. We know that ourcommunities are more polluted and are moreadversely impacted with health outcomes, includingasthma and low birth weight. We also know thatthese health outcomes contribute to other types ofsocial problems, including poor performance inschools.
WE ACT has taken up the challenge of figuringout how to take those scientific research findings thatwe’ve done in partnership with residents in the com-munity and with our research team, and translatethem into policies that create changes that bringabout a cleaner environment and reduce some of thenegative impacts of climate change. We’ve taken someof those findings and created policy vehicles like theEnvironmental Justice Leadership Forum, which iscomposed of 30-plus organizations across the UnitedStates, and across 16 states and the District ofColumbia. Through that forum, we are trying toimpact the national debate on climate policy.
What are we looking for in terms of the out-comes of that policy debate? We’re looking to havepolicies that place public health at the center of theclimate change debate. Why? Because we know thateven in rich countries like the United States it’s thepoorest and the most vulnerable communities thatwill ultimately feel the harshest effects of climate
change, or are feeling them already. In NorthernManhattan, we are looking for policies that will rec-ognize that we already have particular health bur-dens, and that we need to be able to put those healthburdens into the climate change policy framework.
At the state level, we’re also looking at theRegional Greenhouse Gas Initiative, which is a com-pact made up of the 11 northeastern states. It createsa system where they’re trading pollutants. They havehad two auctions already. We’re looking at the rev-enue that is being generated in that process, whichcould help address some of the public health issuesin communities that we know are on the forefrontline of climate change. We’re also looking at creatingresources that will help convert boilers in our com-munity, because we know that the boilers in ourbuildings burn some of the dirtiest fuel. And lastly,on the city level, we have been working with PlaNYC2030 to look at how we can generate a public healthdiscussion about climate change. We are placingsome of our communities at the forefront of the ini-tiatives that the Mayor’s office has developed, alongwith the advisory body on PlaNYC 2030.
I’d like to raise the issue of climate policy andpublic health. In the focus on climate change, we’veactually lost sight of the fact that we have significantlaws in place to help deal with criteria pollutants.Those are pollutants like PM2.5 that come from thecombustion of things like diesel. One of the things thathas happened is we’ve lost sight of regulating thoseparticular pollutants. We believe that before we getthrust into a climate change policy that is only focusedon carbon, we need to recognize that there are co-pol-lutants in our communities that make us equally as ill.These are the things that need to be linked in the longrun for us.
I think Michel was right when he said we have ahistorical opportunity to deal with this challengebefore us. Dr. Martin Luther King talked about theurgency of now. The other thing that he said shortlyafter that was not to allow ourselves to be tranquilizedby the pill of gradualism. I believe that if we don’t seekbold solutions with regards to this, if we don’t take thepolicy findings that are coming out of the Center andthe community-based research approach that we doand really translate them into bold issues that putpublic health at the center of climate change, reduceurban air pollution, and recognize that some commu-nities are more vulnerable than others, we will bedoomed to the pill of gradualism.
“Even in rich countries like the United States it’s the poorest andthe most vulnerable communities that will ultimately feel theharshest effects of climate change, or are feeling them already.In Northern Manhattan, we are looking for policies that willrecognize that we already have particular health burdens, andthat we need to be able to put those health burdens into theclimate change policy framework.”

35
Jay Feldman, MS, Executive Director,Beyond Pesticides
My thesis today is that, as a result of what we’veheard here today and what the scientific literaturesupports, we need to shatter the conventional wis-dom that drives pesticide policy—that toxic pesti-cides are necessary to our quality of life, food pro-duction, public health and environmental manage-ment. We’re sort of in between the age of riskassessment and the precautionary principle. Weneed to move with some urgency to the transfor-mation of public policy toward precaution. Todaywe’re looking at pesticide policies that are driven byrisk assessments, despite the fact that there areknown uncertainties associated with risk assess-ments. We don’t know much about mixtures, wedon’t know much about inert ingredients orendocrine disruptors, as you heard. We don’t knowmuch about the inverse dose response curve. Weassume that dose makes the poison. We do very lit-tle under risk assessment to look at the dispropor-tionate effects on people of color and those withelevated risk factors. We’re not looking at low doseor sub-lethal effects.
Policymakers continue to advance changes inrisk assessment. Improving a bad situation, however,does not achieve the environmental public healthgoals that we hear about from people who are livingin communities at risk. Consider the disproportion-ate risk of kids in New York City. African-Americaninner city children suffer elevated asthmatic condi-tions caused or triggered by pesticide products thatmeet the current health-based risk assessment stan-dards. African-Americans are four to six times morelikely than whites to die from asthma. Therefore anytime our policies allow regulators to permit uses of
pesticides with known asthma or respiratory effects,our policies essentially impact the African-Americancommunity disproportionately.
Noted English epidemiologist Austin BradfordHill actually got us to start thinking about the pre-cautionary principle back in the ’60s when he said,“All scientific work is incomplete. Whether it is obser-vational or experimental, all scientific work is liableto be upset or modified by advancing knowledge.That does not confer upon us a freedom to ignorethe knowledge we already have or to postpone theaction that appears to be demanded at a given time.”This same conclusion was reached in the recent bookwritten by Philip Shabecoff, former New York Timesreporter, and Alice Shabecoff, Poison Profits—The ToxicAssault on Our Children, in which the authors refer tothe industry and its co-conspirator EPA—that’s theauthors’ characterization—that their actions amountto crimes against children. Too often we let our senseof what is possible politically cloud our sense of whatis scientifically appropriate or really necessary.
Panel 2: Healthy Homes—Regulating Residential Pesticides and Consumer Products
Panel 2: Healthy Homes—Regulating Residential Pesticides and Consumer Products
This roundtable considered how best to ensure that the public is protected from toxic chemicals like phthalates and BPA inthe home and in common consumer products. A common refrain was the ineffectiveness of the current Toxic SubstancesControl Act, and the need for comprehensive legislative reform at the federal level. According to the US GovernmentAccountability Office (GAO), fewer than 200 chemicals out of the 82,000 on the market have been required to be testedunder the current law, and EPA has assessed fewer than 2% of the chemicals that are in its inventory.
There was strong support for the proposed Kid-Safe Chemicals Act, introduced in the previous Congress, because itincludes a range of systematic reforms instead of relying on a chemical-by-chemical approach to regulation. Panelistsunderscored the need to reverse the burden of proof so that the chemical industry is responsible for establishing the safetyof their chemicals, rather than requiring the public sector to prove that each new chemical causes harm before it is regulat-ed. Panelists suggested requiring labeling of chemicals like phthalates and other endocrine disruptors in consumer productsso individuals can make informed decisions in the absence of other restrictions. Regardless of the policy solutions imple-mented, there is an ongoing need to promote safe substitutes when a chemical is removed from the market. They also notedthat, with a new presidential administration, environmental health policy is now at a critical crossroads.
Panelists E. Olson, G. Solomon, R. Whyatt, P. Landrigan, and J. Feldman
Now we’ll hear a lot on this panel perhaps, andhave heard somewhat throughout this conference,about health-based standards, but the underlyingrisk assessments that those standards are based onstill drive the use of unnecessary toxic substances.And this is where I transition to alternative prac-tices. We heard earlier from the city health officialsand others who talked about IPM, integrated pestmanagement. As a policy we have to look into howit is put into action. But these ideas embrace cau-tion—that in the face of inadequate knowledge weneed to prevent use and advance precaution.
EPA has something they call the PesticideStewardship Program. It’s a grant program thatworks with the users of pesticides. In that program,the agency is advancing this concept of risk mitiga-tion, or reducing risk. In contrast, policies like theone in New York City, or San Francisco’s precaution-ary risk policy, or the pesticide-free parks policy inWichita, Kansas, or the Washington, DC policy thatstopped the spraying for West Nile Virus because ofelevated asthma rates in the city—all of these policiesare essentially embracing the notion of precaution.
So what policies should we be looking at interms of models? The model that I look to is theOrganic Foods Production Act, which is a law Ihelped write. It’s aimed at avoiding the vulnerabili-ties that lead to pest problems, proper fertilization,inter-cropping, rotations, establishing acceptablematerials, biological controls, pheromones, traps,and ensuring certification, enforcement and demo-cratic decision making. This can be applied to homeuse products as well in the context of IPM, definingpractices and acceptable least-toxic chemicals to beused only as a last resort.
How do I know this can be done? Because I’mworking with people in the private sector that areactually doing it. In public housing projects inGary, Indiana, and Portsmouth, Virginia, they havedone the same thing that we’re told is being donein New York, which is to reduce pesticide use andcreate a higher percentage of pest-free units—going from 6% in Portsmouth, Virginia, to 80%after the adoption of an integrated pest—manage-ment program.
Here’s my bottom line: we’re seeing aroundthe country and in Europe the adoption of policiesthat link the availability of safer alternatives to thecancellation of pesticides. The striking absence of
this link, knowing that alternatives are available, inthe Kid-Safe Chemicals Act, which we’ll talk aboutlater, is troubling to me. Risk assessment withoutsafer substitutes is bad policy in the 21st century.Finally, we must join together to effect a transfor-mation at this historic time. Science can and shouldinform this transformation and drive home theurgency of embracing green practices.
Philip Landrigan, MD, MSc, Director of the Children’s Environmental Health Center,Mount Sinai School of Medicine
Knowing all that we know about pesticides, whatare the strategies that we as a society can adopt toreduce exposures? I tend to think that control of atoxic exposure such as pesticides ought to proceedon three levels. There are steps that need to betaken at the national level having to do with pesti-cide registration standard setting; there are stepsthat need to be taken at the state or the city level;and there are steps that people can take in theirown homes, pursuing the maxim that a parent isthe CEO in their own home and there are thingsthey can do, sometimes alone, sometimes in part-nership with city and national authorities.
In that last vein about control of pesticides atthe most local level, in the home, I’d like to tell youabout something we did a few years ago a couple ofmiles from here in East Harlem. We basicallyundertook a very rigorous evaluation in the EastHarlem community to see if integrated pest man-agement could be successful in a mostly poor, 90%minority community. We partnered with twoneighborhood health centers that are about tenblocks apart in East Harlem. We introduced IPM tothe parents who were attending one, and a veryvigorous fire-safety and accident-prevention pro-gram to parents in the other. After a year we intro-duced everything to everyone. For the first year wefollowed the two groups of parents to see whetherIPM could make a difference. When a mom whowas pregnant came in to the clinic for her prenatalcare we offered to provide her IPM. If she agreedwe sent a handyperson out to the home to teachthe mom and the family about how to clean upfood residues. The person also spent a couple ofhours closing cracks and crevices in the apartment,the portals through which the cockroaches enteredthe apartment.
We evaluated levels of pesticides in the homesthat participated in the IPM program and comparedthem to levels of pesticides in the homes thatreceived conventional pesticide spraying. We also
Translating Science to Policy: Protecting Children’s Environmental Health
36
“Risk assessment without safer substitutes is bad policy in the 21st century.”

37
engaged in the wonderfully salubrious exercise ofconducting roach censuses, which we did by takinga sticky pad about the size of this piece of paper andsticking it under the sink once a month for 24 hoursand actually doing a body count and seeing howmany roaches accumulated.
We found three things. First, the homes thatswore off chemical pesticides and went to integrat-ed pest management decreased their indoor con-tamination by chemical pesticides by 90%. Second,in homes that went to IPM there was a 50% reduc-tion in the numbers of roaches as actually countedcompared to the homes that used traditional pestcontrol, which had no reduction in roach counts. Ithink all the traditional pesticides do is chase theroaches from one apartment to another. It’s like thecoming and going of the tide. Finally, there was vir-tually no cost difference between the two. Therewas a one-time $25 cost per unit to bring thehandyperson in to do the repairs, and then afterthat the costs were equal. So it works. It’s doable. Itwas the model that the City adopted when theyembarked on the larger program that Dan Kass pre-sented this morning. It’s something that I commendto you and wish you well with.
Robin Whyatt, DrPH, Professor and Deputy Director,Columbia Center for Children’s Environmental Health,Mailman School of Public Health
Phthalates are ubiquitous, and virtually everybodyin the United States is exposed daily to multiplephthalates. They’re used as plasticizers to makeplastic soft. They’re also very sticky chemicals sothey’re used to hold scent and are in all kinds ofscented products. There are phthalates in virtuallyall perfumes. They’re used in time-released pills, inpesticide formulations, household cleaners, nailpolish, hairspray, air fresheners, tablecloths, floortiles, shower curtains, raincoats, baby pants, uphol-stery in both home and car, synthetic leather, floorfiles, food wraps, raincoats, carpets, and that’s justto name a few sources. So you can see why we allhave so much exposure to them.
So what are we going to do about it? Well,first there’s some good news. In August 2008,Congress passed the Product Safety ImprovementAct that banned six phthalates from children’s toys(defined as toys for children ages birth through 12years). There has also been a lot of state actiontaken and recently proposed. Industries in theUnited States have also taken steps to removephthalates from products. SC Johnson recentlyannounced that they would remove phthalates
from their fragrance products and, equally excit-ing to me, they also said that they were going tostart listing the ingredients on their air care andhome cleaning products. Phthalates are not listedin any products at this point. That’s true of most ofthe endocrine disruptors.
Despite this good news, we have a long way togo. First, the ban that was just passed on children’stoys does nothing about exposures during pregnan-cy, a window of major susceptibility. Regulation ofphthalates in the United States is a real mishmash,with multiple agencies and very little coordinationamong them. The FDA is responsible for regulationof phthalates in cosmetics and also in medicationswith time-release properties. EPA regulates phtha-lates in pesticides. The Consumer Product SafetyCommission is responsible for regulating phthalatesin children’s toys and in other consumer products.
And while there are alternatives to phthalates,there are enormous data gaps. That brings me to mytwo solutions. First, we need to amend the ToxicSubstances Control Act. I think that’s desperatelyneeded and overdue. I think we should make it com-parable to the European Union (EU) Registration,Evaluation, Authorisation and Restriction ofChemicals (REACH) regulation. In fact, most of thecompanies that are selling products in the UnitedStates are also selling them in the European market.One of the reasons that the US ban on phthalates intoys was successful was because the companies thatwere affected had already removed the phthalatesfrom these toys because a ban had already beenpassed in Europe.
These are global markets that affect eachother, so I think the two statutes should be compa-rable. REACH is an EU regulatory initiative onchemicals and their safe use. It is based on the pre-cautionary principle, and shifts the burden awayfrom requiring regulatory agencies to make thecase that a compound is harmful in order toremove it from the market. Instead, it requires theindustries to make the case that the compound issafe as a condition of registration. It also requirestesting of chemicals. REACH is only addressinghigh-production chemicals. But it’s still an enor-mous step forward.
Second, we need to require labeling of ingre-dients on consumer products. At this point, if youwant to avoid phthalates in products, there’s no wayfor you to tell whether a shampoo, hair spray, soapor other product that you’re picking up off the shelfcontains phthalates as part of the ingredients.
Panel 2: Healthy Homes—Regulating Residential Pesticides and Consumer Products

Gina Solomon, MD, MPH, Senior Scientist,Natural Resources Defense Council (NRDC)
It’s interesting and challenging to pull together thethreads of discussion today and to bring the scienceout into the public policy arena. Jay Feldman talkedabout exposure reduction, and the importance ofreducing exposure before all the scientific evidenceis complete. That was done in California in 2005when research came out of Sweden showing PBDE(polybrominated diphenyl ether) flame retardants
in breast milk. Studies from the US, including fromCalifornia, soon followed, showing that these chem-icals increased logarithmically over time. A dramaticincrease means that, whether or not there are healtheffects right now, at some point there will be a prob-lem. Concern was compounded by the fact thatthese chemicals looked structurally very much likePCBs. So there was legislation passed to ban PBDEsin California. That was a good decision, since newerscience has confirmed the toxicity of the PBDEs.
That legislative success was followed the nextyear by the realization that, well, okay, that’s great,we pat ourselves on the back, but now what? Whatchemicals are coming out to replace these chemi-cals? What chemicals are being added to consumerproducts instead? This is something that policyadvocates in environmental health have faced formany years. We call the problem “whack a mole”—when you finally club some toxic chemical down,something else pops up to replace it. That was theimpetus for the creation of the CaliforniaBiomonitoring Program, which has focused on try-ing to identify new emerging contaminants. Itfocused initially on emerging flame retardants,which include chemicals like tetrabromo-bisphe-nol-A and chlorinated tris, which was banned foruse in children’s sleepwear in the 1970s because it iscarcinogenic. Tris was only banned in sleepwear,and now is turning up in sofa cushions and all kindsof other things. Monitoring and detecting chemicalsin the environment and in people can be an impor-tant trigger for action.
It was fabulous to get phthalates out of chil-
dren’s toys, and that legislation moved initially fromthe city of San Francisco to statewide California in abill sponsored by the Breast Cancer Fund, to a fed-eral bill. But what’s replacing the phthalates in toys?We need to stay ahead of the curve. Policyapproaches that can support science, by movingbiomonitoring ahead and better understandingchemical toxicity, are good approaches.
There’s a third approach that’s been used quitea lot in public policy: consumer campaigns to edu-cate the public about alternatives. Robin mentionedsome of NRDC’s work on air fresheners. We weretrying to figure out where all these phthalates inpeople were coming from. Since we knew thatphthalates are in fragrances, we decided to take alook at air fresheners, and yes, we found phthalates.And yes, some change has happened as a result.Walgreen’s immediately pledged to take phthalatesout of their air fresheners. SC Johnson recently fol-lowed suit. But that kind of approach has problemsbecause there are still plenty of air fresheners on themarket that have phthalates. Most don’t list theiringredients. Air fresheners are one source of phtha-lates but there’s still a panoply of other sources. If wehave to go hunting under every rock, just lookingblindly for the sources of exposure, it’s going to takeus way too long to protect families and kids.
The ultimate solution isn’t just a chemical-by-chemical approach, and it’s not an approach thatfocuses on targeting companies and doing con-sumer product campaigns. It’s an approach thatchanges the whole system that governs the way thatchemical policy is put together at the federal levelin this country. True reform gives people the infor-mation they need to protect themselves, but alsophases out bad actor chemicals and improves theway chemicals are assessed so that there is nolonger the need to gather huge amounts of infor-mation before any action can be taken. Real chemi-cal policy reform may be just around the corner,and scientists should support it.
Erik Olson, Director of Chemical and Food SafetyPrograms, The Pew Charitable Trusts
Someone earlier said that this has been a historicconference, and I have to agree with that. I thinkthat no one who listened to Lisa Jackson or LindaBirnbaum today could fail to be impressed withhow much the leadership of the country haschanged and how important it is to have senior gov-ernment officials talking about the issues in a waythat indicates that they are going to listen to the sci-ence. It’s really impressive to hear them make com-
Translating Science to Policy: Protecting Children’s Environmental Health
38
“The ultimate solution isn’t just a chemical-by-chemicalapproach, and it’s not an approach that focuses on targetingcompanies and doing consumer product campaigns. It’s anapproach that changes the whole system that governs the way that chemical policy is put together at the federal level in this country.”

39
mitments about moving forward with the toxic-chemical policy agenda.
I believe we’ve actually made some significantprogress. But what we have not made progress on,or as much progress as we need to, is on this hugemountain of evidence that’s been accumulating.The research that we saw presented this morning isreally compelling. It’s very rare that you see anintervention, a policy intervention, tracked, andyou see direct, immediate impacts from that. That’swhat I think that Dursban (chlorpyrifos) studyshowed, and that’s why I quote it so often when I’mup on the Hill. It’s very similar to what happenedwhen we phased out lead in gasoline, where yousaw almost immediate benefits in terms of bloodlead levels. Here you see almost immediate benefitsto the pregnant women and to their children whono longer were being exposed to this chemical.That is compelling stuff, and I think we really needto be supporting that kind of research because itfeeds into the policy arena very effectively, and it’shard to deny that it’s important.
So that’s the good side of the story. I want totalk about the bad side of the story, and how badour toxic chemical policy is just briefly. For those ofyou who are interested in this I would commend toyour attention a couple of GAO (GovernmentAccountability Office) reports that were done in thelast couple of years. They provide informationabout the 1976 law called the Toxic SubstancesControl Act, or what our former colleague AlMeyerhoff used to call the Toxic ChemicalConversation Act, because it only required ongoingconversations and no action. That law has essential-ly been a failure. What we know is that there arenow 82,000, plus or minus, chemicals in com-merce. Guess how many of those EPA has been ableto regulate under the Toxic Substances Control Act?Five out of 82,000. This is according to GAO. Thelast one that was regulated under that act was in1990—19 years ago, according to GAO. Fewer than200 chemicals out of 82,000 have been required tobe tested under this law, according to GAO. EPA hasassessed fewer than 2% of the chemicals that are inthe inventory. Even if you look at the most highlyproduced chemicals, the high-production-volumechemicals of which over a million pounds are madea year, according to GAO, 7% have even the six basictoxicity studies, so 93% do not. Now maybe that’schanged slightly in the last couple of years, but thebottom line is that we don’t know much about the
chemicals that are in virtually everything in thisroom, that we’re all being exposed to and our kidsare being exposed to, almost every day.
This highlights the need for comprehensivereform of the Toxic Substances Control Act. Weneed to be able to take effective regulatory action.First, we need a systematic review of all new andexisting chemicals. We can’t grandfather existingchemicals, which the previous law did. Secondly, weneed to look at the entire spectrum of healtheffects. We need to look at cancer, developmentaleffects, immunotoxicity, endocrine effects, and soon. We can’t limit ourselves just to one or twoeffects. Third, we absolutely have to have a standardthat protects children and vulnerable populations.We’ve learned from the Food Quality Protection Act,a law passed in 1996, that when you have a relativelytough standard, if there are people willing to sueEPA and be watchdogs on it, you can actually makeprogress. And that’s what happened. Dursban(chlorpyrifos) didn’t magically disappear; it tookvery difficult and sustained work and a tough stan-dard in the law. Fourth, we need to reverse the bur-den of proof so that the chemical industry isresponsible for proving the safety of their chemi-cals. Fifth, we need to make sure that public healtheffects data is made public, that there is a right toknow in the public, and that this information is
shared and not claimed as confidential. Lastly, weneed to improve our exposure information. Weneed to have more biomonitoring data and aneffective program that ensures that we know whatour children are being exposed to, and what we areall being exposed to.
I think all of those components are in the Kid-Safe Chemicals Act, which was introduced in theprevious Congress by Congressman Waxman andCongresswoman Solis, who’s now in our Cabinet,and by Senator Lautenberg and Senator Boxer andothers, that I hope will be improved and reintro-duced in not too long a period. I think that’s thekind of reform we’re going to need. It’s not going tobe enacted this week or next month, but it’s thekind of reform we have to seriously discuss. I thinkwe actually have to go beyond where Europe is atthis point and reach for the stars.
Panel 2: Healthy Homes—Regulating Residential Pesticides and Consumer Products
“We need to reverse the burden of proof so that the chemicalindustry is responsible for proving the safety of their chemicals.”

Translating Science to Policy: Protecting Children’s Environmental Health
40
Rohit T. Aggarwala, PhD is Director of theNew York City Mayor’s Office of Long-TermPlanning and Sustainability. This office wascharged with the creation of PlaNYC: AGreener, Greater New York, a comprehensivesustainability plan consisting of 127 separateinitiatives to green New York City. Dr.Aggarwala is now charged with implement-ing the plan and supporting other effortsrelated to the sustainability of New York City.Under his leadership the City has begunimplementing over 90% of the 127 initiativesin PlaNYC, including regulations to make theCity’s taxicabs and black car fleets clean,planting a million trees throughout the fiveboroughs and overseeing the investment of$80 million a year to reduce City govern-ment’s greenhouse gas. A native ofManhattan, NY, Dr. Aggarwala holds BA,MBA, and PhD degrees from ColumbiaUniversity, as well as a master’s from QueensUniversity in Ontario. Prior to joining theBloomberg administration for the City,Aggarwala was a management consultant atMcKinsey & Company. During the ClintonAdministration, he worked at the FederalRailroad Administration.
John M. Balbus, MD, MPH is the Chief HealthScientist for Environmental Defense Fund(EDF). He has authored studies and lectureson global climate change and health, trans-portation-related air pollution, the toxiceffects of chemicals, and regulatoryapproaches to protecting susceptible sub-populations. Recent publications include theClimate Change Science Program’s Synthesisand Assessment Product 4.6, for which hewas a chapter co-author, and the EDF Report“Are We Ready? Preparing for the PublicHealth Challenges of Climate Change.” Dr.Balbus is a member of the EPA ScienceAdvisory Board, the National ResearchCouncil’s Board on Environmental Studiesand Toxicology and the EPA Children’s HealthProtection Advisory Committee. He receivedhis AB degree in Biochemistry from HarvardUniversity, his MD from the University ofPennsylvania, and his MPH from the JohnsHopkins School of Public Health.
Linda S. Birnbaum, PhD, DABT, ATS, isDirector of the NIEHS and the NationalToxicology Program (NTP). Prior to herappointment as NIEHS Director, Dr.Birnbaum was a senior advisor at theEnvironmental Protection Agency (EPA),where she has served for 16 years as directorof the Experimental Toxicology Division. Sheis a board certified toxicologist and hasserved as a federal scientist for nearly 29years—the first 10 of those at NIEHS — first asa senior staff fellow at the NTP, then as aprincipal investigator and research microbi-ologist, and finally as a group leader for theInstitute’s Chemical Disposition Group. The
author of more than 600 peer-reviewedpublications, book chapters, abstracts andreports, Dr. Birnbaum’s research focuses onthe pharmacokinetic behavior of environ-mental chemicals; mechanisms of actions oftoxicants, including endocrine disruption;and linking of real-world exposures toeffects. She is also an adjunct professor inthe School of Public Health, the ToxicologyCurriculum, and the Department ofEnvironmental Sciences and Engineering atthe University of North Carolina, ChapelHill, as well as in the Integrated ToxicologyProgram at Duke University. Dr. Birnbaumearned her MS and PhD in microbiologyfrom the University of Illinois, Urbana.
Cecil D. Corbin-Mark, MPhil, is the DeputyDirector of WE ACT for Environmental Justice.He is the former Vice-President of his neigh-borhood association, and the former Chair ofthe Landmarks Preservation Committee of hisCommunity Planning Board. Mr. Corbin-Markeither currently sits on, or has in the past servedon, the following environmental boards, coali-tions and committees: New York Jobs withJustice, Center for Environmental Health,Urban Wet Weather FACA for the EPA, the NewYork State DEC Urban Air Toxic Committee,New York State Cumulative Risk AssessmentWork Group, New York City DEP Water QualityCitizen Advisory Committee, Manhattan SolidWaste Advisory Board, Clean Air Network,Association for Clean Water Action, CleanProducts/Clean Production Network,Environmental Justice Fund, Organization ofWaterfront Neighborhoods, the NYCEnvironmental Education Advisory Council. Heis also a member of the Steering Committee forthe Northeast Environmental Justice Network.He received his undergraduate degree in politi-cal science at Hunter College, CUNY, and hisgraduate degree in political science at OxfordUniversity in the United Kingdom.
Jay Feldman, MS, Executive Director ofBeyond Pesticides, is a cofounder of theorganization and has served as its directorsince 1981. Mr. Feldman has helped to buildBeyond Pesticides’ capacity to assist localgroups and impact on national pesticide andalternatives policy. He has tracked specificchemical effects, regulatory actions, pesticidelaw, and safe pest management. Publicationsinclude numerous Beyond Pesticides’ publi-cations, including Taking Toxics Out of HealthCare, Ending Toxic Dependency, Safer Schools, TheSchooling of State Pesticide Laws, Pole Pollution,Poison Poles, Voices for Pesticide Reform, A Failureto Protect, Safety at Home, and Unnecessary Risks,and numerous articles on pesticides andschools, food safety and agriculture, farm-worker protection, landscape management,children and related issues. Mr. Feldmanprovides testimony regularly before the USCongress. He is the author of the School
Environment Protection Act; co-author,Organic Farming Act, and contributor to theOrganic Foods Production Act. He has a mas-ter’s in Urban and Regional Planning fromVirginia Polytechnic Institute and a BA fromGrinnell College.
Linda P. Fried, MD, MPH, Dean and DeLamarProfessor of the Mailman School of PublicHealth, introduced keynote speaker LisaJackson. Dr. Fried is a leader in the fields ofepidemiology and geriatrics, and has dedi-cated her career to the science of healthyaging, particularly the prevention of frailtyand disability, and the design of generativehealth-promoting roles for older adults. Dr.Fried co-founded Experience Corps, a com-munity-based senior volunteer program thatboth serves the academic success of publicschool children and is a health promotionprogram for older adults. Dr. Fried is therecipient of numerous awards, including theAPHA Archstone Award, the Maxwell PollackAward of the Gerontological Society ofAmerica, and the American GeriatricsSociety’s Henderson Award for career con-tributions to research on aging. Previously,Dr. Fried served as the Mason F. LordProfessor of Geriatric Medicine at JohnsHopkins University and held joint appoint-ments in the Bloomberg School of PublicHealth and the School of Nursing. Shedirected The Johns Hopkins MedicalInstitutions’ Center of Excellence for AgingResearch, the Center on Aging and Health,and the Division of Geriatric Medicine andGerontology. Dr. Fried received her MDfrom Rush Medical College in Chicago andher MPH from Johns Hopkins.
Michel Gelobter, PhD, is the founder ofCooler, Inc., a for-profit, social venture thatprovides easy ways for consumers and retail-ers to address the global warming impact ofgoods and services. Dr. Gelobter brings over25 years of experience working on climatechange, and led the national think-tank,Redefining Progress, in designing the world’smost aggressive climate legislation, signedinto California law in August 2006. He hasbeen a Congressional Black Caucus Fellowwith the US House of Representatives Energyand Commerce Committee; Director ofEnvironmental Quality for the City of NewYork, and an Assistant Commissioner for itsDepartment of Environmental Protection;and founder and director of theEnvironmental Policy Program at ColumbiaUniversity’s School of International andPublic Affairs. He serves on the AdvisoryBoard of Vice-President Al Gore’s Alliancefor Climate Protection, and the Board of theNatural Resources Defense Council amongothers. He earned his PhD, MS, & BS inEnergy and Resources from UC Berkeley andis an alumnus of Deep Springs College.
Speakers and Panelists

41
Lisa P. Jackson, Administrator of the USEnvironmental Protection Agency, leads astaff of approximately 18,000 professionalsdedicated to protecting the public health andenvironment of all Americans. She was nom-inated to lead the Agency by President BarackObama on Dec. 15, 2008 and confirmed bythe Senate on Jan. 23, 2009. She is the firstAfrican American to serve in that position.Administrator Jackson lists among her priori-ties reducing greenhouse gas emissions,improving air quality, managing chemicalrisks, cleaning up hazardous waste sites, andprotecting America’s water. Before becomingEPA’s Administrator, Jackson served as Chiefof Staff to New Jersey Governor Jon S.Corzine. Prior to that, she was appointed byGovernor Jon S. Corzine to be Commissionerof the state’s Department of EnvironmentalProtection (DEP) in 2006. WhileCommissioner, Jackson was known for heradvocacy for reducing greenhouse gases,aggressively addressing pollution, and havingan open and honest dialogue with stakehold-ers in the public policy process. She was alsonoted for ensuring that underserved com-munities received fair environmental protec-tion under the law. Jackson joined N.J. DEP in2002, serving as Assistant Commissioner forCompliance and Enforcement followed byLand Use Management before becomingCommissioner. Prior to joining N.J. DEP, sheworked for 16 years as an employee of the USEPA. Jackson is a summa cum laude graduateof Tulane University’s School of ChemicalEngineering and earned a master’s degree inchemical engineering from PrincetonUniversity.
Daniel Kass, MSPH, is Assistant Commissionerfor the Bureau of Environmental Surveillanceand Policy at the NYC Department of Healthand Mental Hygiene, which provides epidemi-ologic, analytic, policy analysis and other serv-ices, promotes public awareness of environ-mental health, and works on a variety ofurban environmental concerns. Mr. Kass alsoserves as the Principal Investigator on theagency’s Environmental Public HealthTracking grant, a CDC effort to enhance envi-ronmental surveillance. Mr. Kass overseesNew York City’s Local Law 37 pesticide usereduction program, and has worked since1998 to promote and evaluate safer pest con-trol in urban settings. Mr. Kass was formerlyDirector of Evaluation for the NYC ChildhoodAsthma Initiative and Deputy Director forEnvironmental & Occupational DiseaseEpidemiology. Before joining the Department,he founded and directed the Hunter CollegeCenter for Occupational and EnvironmentalHealth. In 2008, he and other staff at BESPreceived the US EPA Regional Children’sEnvironmental Health Champion Award fortheir work in understanding and preventingexposures to methylmercury. He earned a ScBdegree from Brown University and MSPHdegree from the UCLA School of PublicHealth, and completed doctoral studies atNYU’s Wagner School.
Patrick Kinney, ScD, is Associate Professorand the Director of the program in climateand health at the Mailman School of PublicHealth. Dr. Kinney’s teaching and researchaddress issues at the intersection of globalenvironmental change, human health, andpolicy, with an emphasis on the publichealth impacts of climate change and airpollution. His work in the 1990s on airquality and environmental justice inNorthern Manhattan and the South Bronxled to important new insights into theimpacts of diesel vehicle emissions on localair quality. He has carried out numerousstudies examining the human health effectsof air pollution, including studies of theeffects of ozone and/or particulate matteron lung health and on daily mortality inlarge cities. More recently, he developed anew interdisciplinary research and teach-ing program at Columbia examining thepotential impacts of climate change onhuman health. Dr. Kinney earned his doc-torate at the Harvard School of PublicHealth, where he studied the effects of airpollution on lung function in children aspart of the Harvard Six Cities Air Pollutionand Health Study.
Philip J. Landrigan, MD, MSc, the Ethel WiseProfessor and Chair of the Department ofCommunity and Preventive Medicine at Mt.Sinai, is a pediatrician, epidemiologist, andinternationally recognized leader in publichealth and preventive medicine. He hasbeen a member of the faculty of MountSinai School of Medicine since 1985, Chairof the Department of Community andPreventive Medicine since 1990, and he isthe Director of the Mt. Sinai Children’sEnvironmental Health Center. He servedfor 15 years as an Epidemic IntelligenceService Officer and medical epidemiologistat the Centers for Disease Control andPrevention (CDC) and the National Institutefor Occupational Safety and Health(NIOSH). He has also chaired committees atthe National Academy of Sciences (NAS).The NAS report that he directed on pesti-cides and children’s health was instrumen-tal in securing passage of the Food QualityProtection Act, the only environmental lawin the United States that contains explicitprovisions for the protection of children. In1997-1998, Dr. Landrigan served as SeniorAdvisor on Children’s Health to theAdministrator of the US EPA and wasinstrumental in helping to establish a newOffice of Children’s Health Protection atEPA. He has published more than 500 sci-entific papers and 5 books. Dr. Landriganreceived his undergraduate degree fromBoston College, his medical degree fromHarvard Medical School, a Diploma ofIndustrial Health from the University ofLondon, and a Masters of Science inOccupational Medicine degree from theLondon School of Hygiene and TropicalMedicine.
Brian Lehrer is host of “The Brian LehrerShow,” WNYC Radio’s daily call-in program,covering politics and life, locally and globally.The show airs weekdays from 10 a.m. to noonon WNYC 93.9 FM, AM 820 and wnyc.org.“The Brian Lehrer Show” was recognized witha 2007 George Foster Peabody Award for“Radio That Builds Community Rather ThanDivides.” Time Magazine has called Lehrer’sshow “New York City’s most thoughtful andinformative talk show.” He also hosts a weeklytelevision program on CUNY-TV, “BrianLehrer Live” featuring issue-oriented webvideo. In addition to the Peabody, Lehrer haswon numerous awards, including fourAssociated Press New York Broadcasters “BestInterview” Awards since 2000. He has hostedhis eponymous program, originally called“On The Line,” since its inception in 1989.Prior, he was an anchor and reporter for theNBC Radio Networks, and an award-winningauthor and documentary producer. Lehrerholds master’s degrees in public health fromColumbia University and journalism fromOhio State University and a bachelor’s inmusic and mass communications from theState University of New York at Albany.
Rachel L. Miller, MD, FAAAAI is an AssociateProfessor of Medicine and EnvironmentalHealth Sciences (in Pediatrics) at NewYork–Presbyterian Hospital/ColumbiaUniversity Medical Center. She is also DeputyDirector of Columbia Center for Children’sEnvironmental Health (CCCEH). As Directorof the CCCEH Asthma Project, her researchfocuses on mechanisms for the onset of asth-ma. Her clinical work specializes in the treat-ment of asthma and allergies. A majoremphasis of her research is the role of prena-tal and early postnatal exposure in later pedi-atric and adolescent asthma risk. Additionalareas of research include identifying novelgenetic by environment interactions and epi-genetic by environment interactions impor-tant to the onset of asthma. She received herundergraduate degree from HarvardUniversity, and her medical degree from NewYork University.
Erik D. Olson is the Director of Chemical andFood Safety Programs at the Pew CharitableTrusts. He was deputy staff director and gen-eral counsel of the Senate Committee onEnvironment and Public Works untilNovember 2008, and has 25 years of experi-ence in environmental policy and consumeradvocacy. Mr. Olson is responsible for con-sumer product safety, including efforts toimprove food safety, overhaul toxic chemicalregulatory programs to better protect chil-dren and other vulnerable people, andestablish safeguards for emerging risks inconsumer products. During his Senatetenure, he worked on environmental issuesand on health threats from toxic chemicals,playing a key role in major environmentallegislation and hearings on global warming,toxic chemicals, children’s environmentalhealth, clean air, drinking water, clean water
Speakers and Panelists

Translating Science to Policy: Protecting Children’s Environmental Health
42
and environmental justice, among otherissues. He also helped to negotiate the leadand phthalates provisions enacted in theConsumer Product Safety Improvement Actof 2008, and the green buildings and greenschools provisions of the EnergyIndependence and Security Act of 2007.Prior to his Senate work, Erik worked for 15years at the Natural Resources DefenseCouncil, where he held various positionsincluding advocacy center director, publichealth program director and a senior attor-ney. He previously served as counsel for theNational Wildlife Federation’s environmentalquality program for five years, and as anattorney for EPA’s Office of General Counsel,working on hazardous waste and waterissues. He graduated from the University ofVirginia School of Law, and from ColumbiaCollege of Columbia University.
Frederica P. Perera, DrPH, is a Professor at theMailman School of Public Health, where sheserves as Director of the Columbia Centerfor Children’s Environmental Health and ofthe Disease Investigation ThroughSpecialized Clinically-Oriented Ventures inEnvironmental Research (DISCOVER)Center. Dr. Perera pioneered the field ofmolecular epidemiology, beginning withstudies of cancer and is now applying molec-ular techniques within studies of pregnantwomen and their children. Her areas of spe-cialization include prevention of environ-mental risks to children, molecular epidemi-ology, cancer prevention, environment-sus-ceptibility interactions in cancer, develop-mental damage, asthma, and risk assess-ment. She is the author of over 200 publica-tions and has received numerous honors,including: First Irving J. Selikoff CancerResearch Award, The Ramazzini Institute(1995); Newsweek, The Century Club Award(1997); First Children’s Environmental HealthAward, The Pew Center for Children’s Healthand the Environment (1999); DistinguishedLecturer, National Cancer Institute,Occupational and Environmental Cancer(2002); Doctoris Honoris Causa, JagiellonianUniversity, Krakow, Poland (2004);Children’s Environmental Health ExcellenceAward, US Environmental Protection Agency(2005); and CEHN (Children’sEnvironmental Health Network) Award(2008). Dr. Perera received her undergradu-ate degree from Harvard University and hermaster’s and doctoral degrees in publichealth from Columbia University.
Virginia Rauh, ScD, MSW, is a Professor ofClinical Population and Family Health at theMailman School of Public Health, andDeputy Director of Columbia Center forChildren’s Environmental Health. Dr. Rauhhas been working in the field of perinatalepidemiology since 1982. Her expertise is inthe area of low birth weight and pretermdelivery, particularly with respect to socioe-conomically disadvantaged and minoritypopulations. At the Columbia Center for
Children’s Environmental Health her workfocuses on the adverse impact of exposureto air pollutants, including second handsmoke and pesticides; pregnancy and childhealth; and the susceptibility of disadvan-taged populations to environmental haz-ards. She is working with other Columbiafaculty to study the effects of the WorldTrade Center disaster on pregnant womenand newborns. Dr. Rauh is currently princi-pal investigator for the Manhattan Site ofthe National Children’s Study. She is the pri-mary instructor for the Child Health coursewithin the Heilbrunn Department ofPopulation and Family Health. She holds anMSW from Smith College and an ScD fromHarvard University.
Peggy Shepard is the Executive Director andco-founder of WE ACT for EnvironmentalJustice, also known as West HarlemEnvironmental Action. Founded in 1988 inWest Harlem, WE ACT works to build com-munity power to improve environmentalhealth, policy and protection in communitiesof color. She is a recipient of the 2008 JaneJacobs Lifetime Achievement Award from theRockefeller Foundation, the 10th AnnualHeinz Award for the Environment, and theDean’s Distinguished Service Award from theColumbia Mailman School of Public Healthin 2004. WE ACT is a nationally recognizedorganization in the field of community-basedparticipatory research in partnership withthe Mailman School of Public Health atColumbia University. Ms. Shepard is a mem-ber of the National Children’s Study FederalAdvisory Committee to the NationalInstitutes of Health. Ms. Shepard served asguest editor of an Environmental HealthPerspectives monograph, AdvancingEnvironmental Justice Through Community-BasedParticipatory Research, April 2002, and is co-author of “Promoting Environmental HealthPolicy Through Community BasedParticipatory Research: A Case Study fromHarlem, New York,” published in the Journalof Urban Health, Bulletin of the New YorkAcademy of Medicine, Jan. 2006.
Sandra Steingraber, PhD, is an ecologist,author and cancer survivor. Dr. Steingraber iscurrently a Distinguished Visiting Scholar atIthaca College. She is the author of Post-Diagnosis, a volume of poetry, and co-authorof a book on ecology and human rights inAfrica, The Spoils of Famine. She has taughtbiology at Columbia College, Chicago, heldvisiting fellowships at the University ofIllinois, Radcliffe/Harvard, and NortheasternUniversity, and served on President Clinton’sNational Action Plan on Breast Cancer. Dr.Steingraber is an internationally recognizedexpert on the environmental links to cancerand human health. Dr. Steingraber’s highlyacclaimed book, Living Downstream: An EcologistLooks at Cancer and the Environment presentscancer as a human rights issue. Her newwork, Having Faith: An Ecologist’s Journey toMotherhood, explores the intimate ecology of
motherhood. Most recently, she has con-tributed to What We Do Now, an anthology ofindividual manifestos outlining a series ofpassionate new ideas for living. Dr.Steingraber has won many awards for herwork. Several interviews with Dr. Steingraberhave appeared in The Chicago Tribune, USAToday, The Cleveland Plain Dealer, on NationalPublic Radio, “The Today Show,” and “Now”with Bill Moyers. She received her doctoratein biology from the University of Michiganand master’s degree in English from IllinoisState University.
Gina Solomon, MD, MPH, is a Senior Scientistat the Natural Resources Defense Council(NRDC) and an Associate Clinical Professor ofMedicine at the University of California atSan Francisco (UCSF) where she is also theDirector of the Occupational andEnvironmental Medicine Residency Programand the Associate Director of the UCSFPediatric Environmental Health SpecialtyUnit. Her work has included over 40 scientif-ic papers, book chapters, and reports on airpollution, pesticides, global warming, andother environmental and occupationalthreats to health. Dr. Solomon serves on theUS EPA Science Advisory Board DrinkingWater Committee, the National ToxicologyProgram Board of Scientific Counselors, andthe California Scientific Guidance Panel forbiomonitoring. Dr. Solomon attended med-ical school at Yale University and received herpostgraduate training in internal medicine,public health, and occupational and environ-mental medicine at Harvard University.
Robin M. Whyatt, DrPH, is Professor ofClinical Environmental Health Sciences atthe Mailman School of Public Health and isDeputy Director of the Columbia Center forChildren’s Environmental Health. Herresearch focus is on the effects of environ-mental exposures on women and children,including the developing fetus. Dr. Whyatt’sparticular focus is on the extent of exposureto non-persistent pesticides (organophos-phates, carbamates and pyrethroids) andphthalates during pregnancy among thisminority cohort. She is also collaboratingwith the Centers for Disease Control on thevalidation of biomarkers of prenatal expo-sures to contemporary-use chemicals. Shehas served on a number of federal commit-tees, including the National Academy ofScience Committee on HumanBiomonitoring for Environmental Toxicants,for the US EPA on children’s environmentalhealth issues including considerations ofdevelopmental changes in behavior andanatomy when assessing exposures to chil-dren, and on a framework for assessinghealth risks of environmental exposures tochildren. She also served as co-chair of thechemical exposures workgroup for theNational Children’s Longitudinal CohortStudy. She received her MPH and DrPH fromColumbia University.

43
Mothers & Newborns Study,Northern Manhattan / South Bronx
The Center’s largest study focuses on 725 African-American and Latino women and their childrenwhose health is monitored from birth througheleven years of age. Exposure beginning in thewomb to polycyclic aromatic hydrocarbons (PAH)from traffic-related air pollution, pesticides in com-mon home pest-control products, and pest allergensin the home can result in asthma and other respira-tory symptoms, delays in cognitive development,and changes at the molecular level that couldincrease children’s cancer risk. These pollutants cancross the placenta and expose the developing fetusto chemical contamination. Children are more vul-nerable to environmental exposures than adultsbecause their bodies are still developing, and theyare less able to clear toxins from their systems.
Exposures of concern in this study includePAH in ambient air pollution, secondhand smoke,pesticides, endocrine-disrupting chemicals such asphthalates and bisphenol-A, and indoor pest aller-gens. PAH are a group of chemicals released into theair during the incomplete burning of fossil fuelssuch as gasoline, diesel, coal, and other organicsubstances. Secondhand smoke gets into the airwhen tobacco products are burned in cigarettes,cigars, and pipes. This smoke contains thousands oftoxic chemicals, many of which are known to becancer-causing. Harmful pesticides can be inhaledfollowing the use of spray pesticides indoors, andyoung children also have greater exposure becausethey spend more time on the floor where pesticidesare commonly applied. Plastics and other consumerproducts contain chemicals that mimic or blocknatural hormones and thus are capable of disrupt-ing early development. Exposure to pest allergensfrom cockroaches, dust mites, and rodents can
cause serious allergic and asthmatic reactions.Following is a summary of key findings from the
Center’s research study:
Exposure• All pregnant women in the study and their babies
are exposed to multiple common pollutants thatcan harm fetal and child development, affect res-piratory health, or increase cancer risk. Exposuresinclude air pollution, pesticides used in homes,and secondhand smoke [1-3].
• PAH from air pollution were detected in 100% ofthe personal air samples [4].
• There was widespread phthalate exposure duringpregnancy among the study participants.Phthalates were detected in 99%-100% of maternalpersonal air samples. Levels of exposure weregenerally higher among CCCEH cohort womenthan among women of reproductive age (18-40years) sampled through the National Health andNutrition Examination Survey (NHANES) [5].
Fetal Growth and Neurobehavioral DevelopmentCCCEH research has shown that prenatal exposuresto PAH, pesticides, and secondhand smoke arelinked to reduced fetal growth and developmentalproblems in children. These findings have impor-tant implications for health and learning abilitybecause early developmental delays and attention-al/behavioral problems such as Attention-Deficit/Hyperactivity Disorder (ADHD) can affectlater school performance.
PAH
• Prenatal exposure to PAH reduced birth weightand head circumference in African-Americanbabies born to women who were more highlyexposed to the air pollutants [4]. Several studieshave reported that reduction in head circumfer-ence at birth or during the first year of life corre-
CCCEH Key Findings & Interventions
1. Perera FP, Rauh V, etal. Effects of transplacental exposure to environmental pollutants on birth outcomes in a multi-ethnic popula-tion. Environmental Health Perspectives, 111(2): 201-5, February 2003.
2. Whyatt RM, Rauh VA, et al. Prenatal insecticide exposures, birth weight and length among an urban minority cohort. EnvironmentalHealth Perspectives, 112(10):1125-32, 2004.
3. Perera FP, Rauh V, et al. Molecular evidence of an interaction between prenatal environmental exposures on birth outcomes in amultiethnic population. Environmental Health Perspectives, 112(5):626-30, 2004.
4. Perera FP, Rauh V, et al. Effects of transplacental exposure to environmental pollutants on birth outcomes in a multi-ethnic popu-lation. Environmental Health Perspectives, 111(2): 201-5, February 2003.
5. Adibi JJ, Whyatt RM, et al. Characterization of phthalate exposure among pregnant women assessed by repeat air and urine sam-ples. Environmental Health Perspectives, 116(4):467-73. April 2008.
For a comprehensive list and the full text of all CCCEH publications, please visit: www.ccceh.org/papers.html
CCCEH Key Findings & Interventions

Translating Science to Policy: Protecting Children’s Environmental Health
44
lates with poorer cognitive functioning and schoolperformance in childhood.
• Children with high prenatal exposure to PAH hadsignificantly lower test scores at age 3 on theBayley test for cognitive development and weremore likely to be developmentally delayed [6].
• Prenatal exposure to PAH at levels encountered inNYC air can adversely affect child IQ scores at 5years of age. After adjustment for potential con-founders, highly exposed children had full-scaleand verbal IQ scores that were 4.31 and 4.67 pointslower compared to less exposed children. Thesereductions are similar to the effects of low-levellead exposure [7].
Pesticides
• Prenatal exposure to two household pesticides,chlorpyrifos and diazinon, which transfer easilyfrom the mother to her fetus, reduced birthweight by an average of 6.6 ounces—the equivalentof weight reduction seen in babies born to womenwho smoked [8].
• Children prenatally exposed to high levels ofchlorpyrifos were significantly more likely thanchildren exposed to low levels to experience delayin both psychomotor and cognitive development,and to show symptoms of attentional disorders,ADHD, and pervasive personality disorder at age 3.Although the EPA banned residential use of chlor-pyrifos in 2001, this pesticide is still widely used inagriculture [9].
• Pyrethroid insecticides appear to be replacing theorganophosphorus insecticides like chlorpyrifosand diazinon for residential pest control amongthe cohort. Levels of permethrin, a commonpyrethroid insecticide, and piperonyl butoxide, apyrethroid synergist, have increased in personalair samples collected during pregnancy. Also fol-lowing the 2000-2001 EPA restrictions, both
reporting of cockroaches in the home and use ofspray pesticides during pregnancy have increased.Insect resistance to pyrethroids may be one possi-ble explanation for these trends [10].
Secondhand Smoke
• Children prenatally exposed to secondhandsmoke—especially children experiencing materialhardship (unmet basic needs of food, clothing, andhousing)—had significantly reduced scores on testsof cognitive development at two years of age [11].
Phthalates
• Prenatal exposure to the phthalate DEHP was asso-ciated with shorter gestation. Gestational age wasshorter by 1.1 days for each log-unit increase inmetabolite concentrations and averaged 5.1 daysless among the most exposed. Given inconsisten-cies with prior findings in other study popula-tions, additional research is warranted [12].
Asthma RiskChildhood asthma in urban communities is a seri-ous disease that accounts for a significant propor-tion of emergency room visits, hospitalizations, anddeaths. Asthma is a chronic disease of the lungs andairways that causes difficulty breathing, and occursmost commonly in people who become sensitizedto certain allergens in our environment. Differentpeople with asthma react to different triggers.Common triggers include air pollution, dieselexhaust, environmental tobacco smoke, cockroachparticles, dust mites, cat or dog dander, and mold.These exposures may also contribute to the earlydevelopment of the disease.
• Over half the babies in the study have been bornwith an immune response to cockroach proteinsthat may increase the risk of asthma in certainchildren [13].
6. Perera FP, Rauh VA, et al. Effect of prenatal exposure to airborne polycyclic aromatic hydrocarbons on neurodevelopment in thefirst three years of life among inner-city children. Environmental Health Perspectives, 114(8):1287-92, August 2006.
7. Perera FP, Li Z, et al. Prenatal Airborne Polycyclic Aromatic Hydrocarbon Exposure and Child IQ at Age 5. Pediatrics, publishedonline July 20, 2009.
8. Whyatt RM, Rauh VA, et al. Prenatal insecticide exposures, birth weight and length among an urban minority cohort. EnvironmentalHealth Perspectives, 112(10):1125-32, 2004.
9. Rauh VA, Garfinkel R, et al. Impact of prenatal chlorpyrifos exposure on neurodevelopment in the first three years of life amonginner-city children. Pediatrics, 2006.
10. Williams M., Rundle, A., et al. Changes in pest infestation levels, self-reported pesticides use and permethrin exposure duringpregnancy following the 2000-01 US EPA restriction of organophosphates, Environmental Health Perspectives, Vol 116, 1681-8, 2008.
11. Rauh VA, Whyatt RM, et al. Developmental effects of exposure to environmental tobacco smoke and material hardship amonginner-city children. Journal of Neurotoxicology and Teratology, 26(3):373-85, 2004.
12. Whyatt RM, Adibi JJ, et al. Prenatal di(2-ethylhexyl) phthalate exposure in relation to length of gestation among a cohort of inner-city mothers and their newborns. Pediatrics, in press.
13. Miller RL, Chew G, et al. Prenatal exposure, maternal sensitization, and sensitization in utero to indoor allergens in an inner-citycohort. American Journal of Respiratory and Critical Care Medicine, 164(995-1001), 2001.
45
• Pest infestation, allergen levels, and pesticide useare higher among women and babies living in themost deteriorated housing [14].
• Combined prenatal exposure to airborne PAH andpostnatal secondhand smoke results in theincreased likelihood of respiratory symptoms atone and two years of age that may be associatedwith increased asthma risk [15].
• In the Center’s evaluation of the New York CityHousing Authority’s intervention to reduce toxicpesticide use in public housing, high cockroachand mouse allergen levels were significantly asso-ciated with asthma prevalence among childrenand adults [16].
• Developing antibodies to cockroach and mouseproteins is associated with a greater risk forwheeze, hay fever, and eczema in preschool chil-dren as young as three years of age [17].
• CCCEH has linked epigenetic alterations associat-ed with prenatal exposure to PAH in cord bloodwith parental report of asthma by age 5.Epigenetic changes may disrupt the normal func-tioning of genes by affecting how they areexpressed, but do not cause structural changes ormutations in the genes [18].
Cancer RiskThis study is finding that exposure to air pollutionduring pregnancy is associated with genetic damagein babies before they are even born. This type ofgenetic damage has been generally associated withincreased cancer risk later in life.
• Approximately 40% of babies in the study wereborn with DNA damage associated with PAH. Inother studies such damage has been tied to anincreased risk of cancer. Of particular concern,
newborns had higher (approximately 10-fold) lev-els of adducts than mothers per unit of estimatedexposure, indicating greater fetal susceptibilityand potential risk from these pollutants [19].
• Prenatal exposure to PAH was linked to structuralchanges in babies’ chromosomes. Such geneticalterations have been related in other studies toincreased risk of cancer in children and adults[20].
Interventions and Impact on Policy
• From its inception, the Center has worked in part-nership with, and provided data to, a CommunityAdvisory Board of health service and environmen-tal advocacy organizations in Northern Manhattanand the South Bronx, including WE ACT forEnvironmental Justice (WE ACT). With WE ACT,the Center developed the Healthy Home HealthyChild (HHHC) community education campaign in2000. The campaign provides families, physicians,and their patients with practical tips for reducingharmful environmental exposures and protectingchildren’s health, and information on clean aircampaigns in the community. HHHC has also pro-vided training workshops for community leadersand health professionals.
• CCCEH data on the health effects of air pollutionhave been used by local and national groups tosupport clean air policies in New York City. From1998 to 2006, PAH levels from personal monitor-ing of pregnant mothers in the cohort decreasedsignificantly over time [21].
• CCCEH estimated the economic burden of oneaspect of developmental delays associated withprenatal secondhand smoke exposure—EarlyIntervention Services—to be over $50 million per
14. Rauh V, Chew G, et al. Deteriorated housing contributes to high cockroach allergen levels in inner-city households. EnvironmentalHealth Perspectives, 110 (suppl.2):323-327, 2002.
15. Miller RL, Garfinkel R, et al. Polycyclic aromatic hydrocarbons, environmental tobacco smoke, and respiratory symptoms in aninner-city birth cohort. Chest, 136, 1071-78, 2004.
16. Chew G, Carlton E, et al. Determinants of cockroach and mouse exposure and associations with asthma among families and theelderly living in New York City public housing. Annals of Allergy, Asthma and Immunology, 2006.
17. Donohue KM, Al-alem U, et al. Anti-cockroach and anti-mouse IgE are associated with early wheeze and atopy in an inner-citybirth cohort. Journal of Allergy and Clinical Immunology, 122(5):914-20, November 2008.
18. Perera F, Tang W-Y, et al. Relation of DNA Methylation of 59-CpG Island of ACSL3 to Transplacental Exposure to AirbornePolycyclic Aromatic Hydrocarbons and Childhood Asthma. PLoS ONE 4(2): e4488. February 2009.
19. Perera FP, Rauh V, et al. Molecular evidence of an interaction between prenatal environmental exposures on birth outcomes in amultiethnic population. Environmental Health Perspectives, 112(5):626-30, 2004.
20. Bocskay KA, Tang D, et al. Chromosomal aberrations in cord blood are associated with prenatal exposure to carcinogenic poly-cyclic aromatic hydrocarbons. Cancer Epidemiology, Biomarkers & Prevention, 14(2):506-11, February 2005.
21. Narvaez R., Hoepner L, et al. Spatial and temporal trends of polycyclic aromatic hydrocarbons and other traffic-related airbornepollutants in New York City, Environmental Science and Technology, 42:7330-35, 2008.
CCCEH Key Findings & Interventions

Translating Science to Policy: Protecting Children’s Environmental Health
46
year for New York City Medicaid births and $99million per year for all New York City births [22].
• Governmental regulations such as the 2000-2001EPA restrictions on residential use of theorganophosphorous insecticides, chlorpyrifos anddiazinon, have positive impacts on children’shealth. These regulations significantly reduced useof and exposure to these compounds during preg-nancy [23].
• Despite a regulatory ban on residential use ofchlorpyrifos, agricultural applications continue inthe US and abroad. In September 2008, at a publichearing of the EPA’s Scientific Advisory Panel,Federal Insecticide, Fungicide and Rodenticide Act(“Scientific Issues Associated with Chlorpyrifosand PON1”), the Panel unanimously recommendedthat EPA accept the epidemiologic evidence thatchlorpyrifos may act as a neurotoxicant in humanbeings. The panel cited CCCEH data as epidemio-logically sound and recommended that the Agencyattempt to use the cohort data to inform the riskassessment process.
• CCCEH conducted a pilot intervention usingIntegrated Pest Management (IPM) to reduce pestinfestations and residential insecticide exposuresamong pregnant women living in New York City.Residential IPM is a pest-control method that min-imizes exposure to toxic pesticides in the homethrough the use of lower-toxicity pesticides, suchas sticky traps, bait stations, and gels; cleaning;and repairing leaks and holes. Insecticides meas-ured in indoor air samples and in maternal cordblood decreased significantly after the interven-tion. These pilot data suggest that IPM is an effec-tive strategy for reducing pest infestation levelsand the internal dose of insecticides during preg-nancy [24].
• CCCEH has collaborated with the New York CityHousing Authority (NYCHA) and the New YorkCity Department of Health (NYCDOH) in thedevelopment, implementation, and evaluation ofIntegrated Pest Management (IPM) interventionsin public housing. The evaluation has shown thatIPM is more effective than the conventional use ofmore toxic pesticides in reducing levels of cock-roach and cockroach allergens in apartments [25].
• WE ACT incorporates Center findings into regulareducation seminars, promotes health events, andsupports and translates institutional research forthe education of Northern Manhattan residents.The organization developed a citywide network,Our Housing is Our Health, which is comprised ofseveral organizations collaborating to empowercommunities to mitigate health effects of environ-mental exposures related to poor-quality housing.WE ACT has also organized a number of briefings,presentations, case-studies for publication, andtestimony to public interest groups and govern-ment agencies.
• Other recent impacts of WE ACT’s work in NewYork City, informed in part by CCCEH research,include:
— The introduction of the Asthma Free Housing Actby Public Advocate Betsy Gotbaum and CityCouncil member Rosie Mendez in April 2008. Thebill seeks to improve indoor air quality in thehomes of NYC asthma sufferers;
— The coordination of the inaugural taskforcemeetings on rodent control with NY State SenatorBill Perkins; and
— The organization of several successful communityworkshops throughout Northern Manhattan on top-ics ranging from lead poisoning to pest infestation.
22. Miller T, Rauh VA, et al. The economic impact of early life environmental tobacco smoke exposure: early intervention for develop-mental delay. Published Online, Environmental Health Perspectives, July 11, 2006.
23. Whyatt RM, Rauh VA, et al. Prenatal insecticide exposures, birth weight and length among an urban minority cohort.Environmental Health Perspectives, 112(10):1125-32, 2004.
24. Williams MK, Barr DB, et al. An intervention to reduce residential insecticide exposure during pregnancy among an inner-citycohort. Published Online, Environmental Health Perspectives, July 27, 2006.
25. Kass D, McKelvey W, et al. Effectiveness of an integrated pest management intervention controlling cockroaches, mice, and aller-gens in New York City public housing. Environmental Health Perspectives, 117(8): 1219-1225, 2009.

47
Allergen: Any substance that induces an allergy: com-mon allergens include pollen, grasses, dust, and somemedications.
Attention-Deficit/Hyperactivity Disorder: One of themost common childhood disorders that can continuethrough adolescence and adulthood. Symptomsinclude difficulty staying focused and paying atten-tion, difficulty controlling behavior, and hyperactivity(over-activity).
Autism Spectrum Disorder (ASD): A developmental andbehavioral syndrome that consists of certain combina-tions of characteristically autistic traits.
Biomarker: A component in a biological substance(blood, DNA, saliva, breast milk, hair, etc.) used toindicate exposure to, or early biological effect of, anenvironmental chemical, or susceptibility to disease.
Bisphenol-A (BPA): An industrial chemical used tomake polycarbonate plastic resins, epoxy resins, andother products.
Carbamates: A group of chemical pesticides.
Cell proliferation: Cell growth and multiplication.
Chloropyrifos: An organophosphate pesticide widelyused before an EPA ban on household use in 2001.
Cholinesterase inhibition: An action that prevents thebreakdown of the neurotransmitter acetylcholine byacetylcholinesterase, so that high levels of acetyl-choline accumulate at reactive sites, increasing theaction of this neurotransmitter.
Chromosome aberrations: Any change in the normalstructure or number of chromosomes. This may resultin physical or mental abnormalities.
Climate change: Modification of Earth’s climate overtime brought about as a result of changes in theatmosphere as well as interactions between the atmos-phere and various other geologic chemical, biological,and geographic factors within the Earth system.
Cohort: Group of people participating in a researchstudy.
Community-based participatory research (CBPR): A col-laborative approach to research that equitablyinvolves community and academic investigators in theresearch process and recognizes the unique strengthsthat each brings, particularly with the goal of achiev-ing social change, to improve health outcomes andeliminate health disparities.
Cord blood: Blood from a newborn’s umbilical cord.When analyzed, cord blood can indicate allergens andother substances to which an infant was exposedbefore birth.
Developmental disorder (or disability): A delay or prob-lem in a child’s development involving the brain ornervous system. These include learning disabilities,Attention Deficit/Hyperactivity Disorder (ADHD), andother behavioral and cognitive dysfunctions.
Diesel particulate filter (DPF): A device designed toremove diesel particulate matter or soot from theexhaust gas of a diesel engine.
Dioxins: Chemical contaminants that are formed dur-ing combustion processes such as waste incineration,forest fires, and backyard trash burning, as well asduring some industrial processes. They are associatedwith cancer, and reproductive and developmentalproblems, and an increased risk of heart disease anddiabetes.
DNA adduct: This forms as a result of DNA binding to agenotoxic chemical. It reflects exposure to specificcarcinogens, and is a marker of cumulative unre-paired DNA damage.
DNA methylation: The chemical modification of DNAinvolving the addition of a methyl group (a combina-tion of one carbon atom and three hydrogen atoms).This methylation has the potential to alter geneexpression without changing the underlying DNAsequence.
Ecosystem: A system formed by the interaction of acommunity of organisms with their environment.
Endocrine disruptor: Substance that can mimic or dis-rupt the action of naturally occurring hormones witheffects on development and reproduction.
Endometriosis: The presence of uterine lining in otherpelvic organs, especially the ovaries, characterized bycyst formation, adhesions, and menstrual pains.
Environmental justice: The fair treatment and mean-ingful involvement of all people regardless of race,color, national origin, or income with respect to thedevelopment, implementation, and enforcement ofenvironmental laws, regulations, and policies.
Environmental pollutant: Substance present in theenvironment (indoor or outdoor) that can have a neg-ative effect on health and development. Common pol-lutants include pesticides, polycyclic aromatic hydro-carbons (PAH) produced by combustion of organicmaterials, particulate matter (also from fossil fuelsand other combustion including diesel exhaust), envi-ronmental tobacco smoke, lead, and mercury.
Environmental tobacco smoke (ETS): Smoke generatedfrom the burning end of a cigarette, pipe, or cigar, andsmoke that is exhaled by smokers.
Glossary of Terms
Glossary of Terms

Translating Science to Policy: Protecting Children’s Environmental Health
48
Epigenome: Collection of chemical modificationsthroughout the human genome (i.e. genetic materials)that influence gene expression.
Epigentic changes: Heritable alternations in geneexpression that do not change the DNA sequence.
Genetic susceptibility: An inherited increase in the riskof developing a disease.
Global warming: An increase in the Earth’s averageatmospheric temperature caused by an accumulationof greenhouse gases.
Greenhouse gases: Gases that trap heat in the atmos-phere, such as carbon dioxide and ozone. Some green-house gases occur naturally; others are created andemitted solely through human activities.
In utero: In the uterus; unborn.
Hypospadias: A developmental anomaly of the urethrain which a part of the urethral canal is open on theundersurface of the penis or on the perineum.
Integrated pest management (IPM): A safer, low-toxicityapproach to keeping homes free of pests and toxic pes-ticides. Examples of IPM methods include: sealing pestentry points in the home with caulking compoundsand/or metal screens; using low-toxicity, citrus-basedcleaning products to remove food debris and greasestains; and placing glue traps, gels and bait stations forcockroaches and sticky traps for mice throughout thekitchen, bathroom, and any problem areas.
Intelligence quotient (IQ): The ratio of tested mental ageto chronological age, usually expressed as a quotientmultiplied by 100.
Longitudinal birth-cohort studies: Typically long-termobservational studies; often following mothers duringpregnancy and/or babies from birth through severalstages of the developmental.
Magnetic resonance imaging (MRI): The use of a nuclearmagnetic resonance spectrometer to produce elec-tronic images of specific atoms and molecular struc-tures in solids, especially human cells, tissues, andorgans.
Metabolites: Biological by-products of metabolism.Often used as a biomarker to confirm exposure toenvironmental factors.
Molecular epidemiology: A science that focuses on thecontribution of potential genetic and environmentalrisk factors, identified at the molecular level, to theetiology, distribution and prevention of disease withinfamilies and across populations.
Neurodevelopmental disorder: An impairment of thegrowth and development of the brain or central nerv-ous system.
Neuroendocrinology: The study of the anatomical andphysiological interactions between the nervous andendocrine systems.
Neurotoxic pesticides: Pesticides that alter the normalfunctioning of the nervous system.
Organophosphate: Any of several organic compoundscontaining phosphorus, some of which are used asfertilizers and pesticides.
Ozone: An unstable form of oxygen found naturally inthe stratosphere and troposphere. At ground level it isconsidered an air pollutant having harmful effectsupon the respiratory system.
Particulate matter (PM): The summation of airbornemolecules, both solid and liquid, that remain suspend-ed in air. These molecules vary in toxicity due to theirsize (e.g., PM10, PM2.5) and/or composition.
Pesticides: Chemicals used to kill pests, especially insects.
Phthalates: Chemicals used to soften plastics in manyconsumer products, including children’s toys, plasticcontainers, and personal care products. Phthalates canseep out of these products, and studies have shownthat phthalates can disrupt the endocrine system,which is the body’s system of regulating hormones.
Polybrominated diphenyl ethers (PBDE): A potentiallytoxic bioaccumulating flame retardant substancefound in many household products (e.g., electronics,furniture).
Polychlorinated biphenyl (PCB): Any of a family of verystable industrial compounds used as lubricants, heat-transfer fluids, and plasticizers. The manufacture anduse of PCBs has been restricted since the 1970sbecause they are very harmful to humans and theenvironment.
Polycyclic aromatic hydrocarbons (PAH): A carcinogenicorganic molecule produced from the burning of organ-ic substances such as coal, garbage, oil, and cigarettes.
Pyrethroid: Any of several synthetic compounds simi-lar to pyrethrin, used as an insecticide.
Risk assessment: An estimate of the likelihood ofadverse effects that may result from exposure to cer-tain health hazards.
Toxic Substances Control Act (TSCA): A federally-man-aged law that gives EPA broad authority to regulate themanufacture, use, distribution in commerce, and dis-posal of chemical substances.
We would like to thank the women and children participating in CCCEH studies.
We would also like to thank the following individuals:
CCCEH Key Investigators: H. Andrews, S. Chillrud, K. Donohue, D. Evans, R. Garfinkel, I. Goldstein, J. Herbstman, L. Hoepner, P. Kinney, S.A. Lederman, G. Lovasi, R. Miller, M. Orjuela, M. Patel, M. Perzanowski, F. Perera, V. Rauh, A. Rundle, B. Sheares, P. Shepard, D. Tang, R. Whyatt, S. Wang, M. Williams.
Mothers & Newborns and Sibling Study Research Workers: F. Arias, G. Badia, L. Calero, D. Diaz, B. Plaza, M. Reyes, C. Tobon.
CCCEH Staff & Technicians: K. Bernabe, S. Chu, T. Dasgupta, A. Divjan, S. Edwards, E. Evans, C. DeLeon, F. Hafeeez, D. Holmes, S. Hsu, L. Hua, F. Hua, I. Ibrahimagic, X. Jin, I. Jung, A. Just, K. Kern, M. Kurzon, K. Lane, J. Li, C. Lin, H. Lu, R. Martinez, S. Mehta, K. Moors, B. Obeng, M. Rosa, A. Schneider, I. Suen, A. Tse, J. Yu, L. Qu, M. Quaratino, J. Yu, M. Yung, N. Velez de Villa, W. Wang, H. Zhang, D. Zhu.
WE ACT: O. Dotson-Newman, P. Shepard.
CUMC Genetics Lab: D. Warburton, C. Cujar, T. Tubo, X. Liu. NCI: S. Chanock.University of Cincinnati: S.M. Ho, W. Tang. CDC: D. Barr, T. Bernert, A. Calafat, L. Needham, R. Schleicher, A. Sjodin.NIEHS: D. Bell, G. Pittman.Institute for Cancer Research, London: A. Ford, M. Greaves, D. Phillips.Jagiellonian University in Krakow: W. Jedrychowski.Children’s Hospital of Chongqing Medical University: T-Y Li.
Conference Photographer: J. Ramirez.Conference Report: K. Lane, S. Mehta; designed by A. Garland.

COLUMBIA CENTERFOR CHILDREN’SENVIRONMENTALHEALTH
MAILMAN SCHOOL OF PUBLIC HEALTHColumbia Universitywww.ccceh.org
printed on recycled paper