transverse incision for appendectomy
TRANSCRIPT
TRANSVERSE INCISION FOR APPENDECTOMY
LT. COMDR. SAM D. MURRAY
MEDICAL CORPS, UNITED STATES NAVAL RESERVE
T HE idea1 incision for appendectomy should give adequate exposure of the iIeoceca1 region, divide fascia and
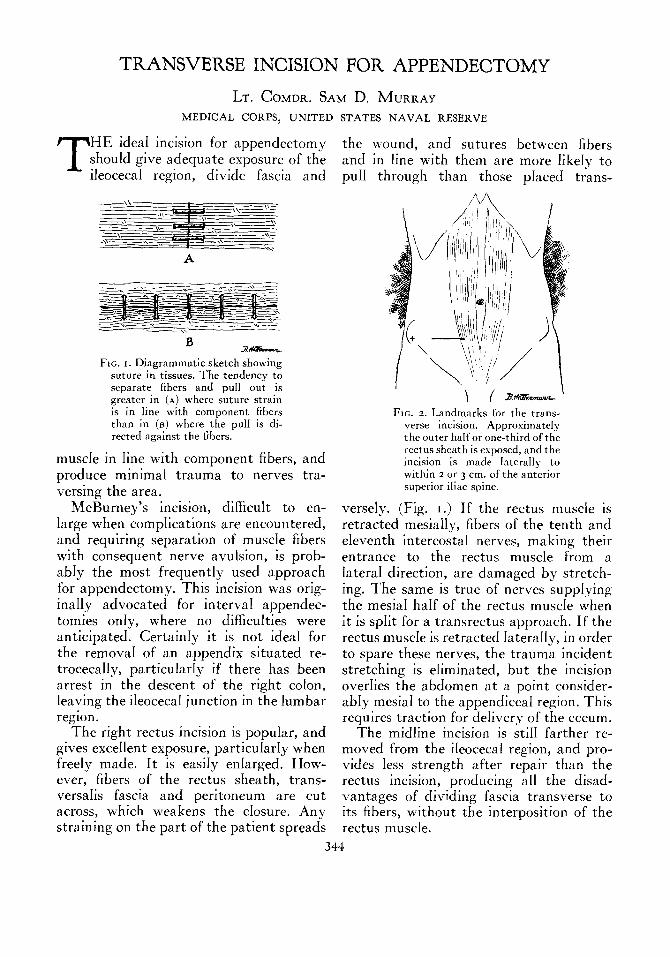
FIG. I. Diagrammatic sketch showing suture in tissues. The tendency to separate fibers and puI1 out is greater in (A) where suture strain is in line with component fibers than in (B) where the puI1 is di- rected against the fibers.
muscIe in Iine with component fibers, and produce minima1 trauma to nerves tra- versing the area.
McBurney’s incision, difficult to en- large when complications are encountered, and requiring separation of muscle fibers with consequent nerve avulsion, is prob- abIy the most frequentIy used approach for appendectomy. This incision was orig- inaIIy advocated for interva1 appendec- tomies onIy, where no diffrcuhies were anticipated. CertainIy it is not idea1 for the removal of an appendix situated re- trocecally, particuIarIy if there has been arrest in the descent of the right coIon, leaving the iIeoceca1 junction in the Iumbar region.
The right rectus incision is popular, and gives exceIIent exposure, particuIarIy when freeIy made. It is easiIy enIarged. How- ever, fibers of the rectus sheath, trans- versahs fascia and peritoneum are cut across, which weakens the cIosure. Any straining on the part of the patient spreads
the wound, and sutures between fibers and in Iine with them are more IikeIy to puIl through than those placed trans-
\I ( am- FIG. 2. Landmarks for the trans-
verse incision. Approximately the outer haIf or one-third of the rectus sheath is exposed, and the incision is made IateralIy to within z or 3 cm. of the anterior superior iliac spine.
versely. (Fig. I .) If the rectus muscIe is retracted mesially, fibers of the tenth and eIeventh intercostal nerves, making their entrance to the rectus muscle from a IateraI direction, are damaged by stretch- ing. The same is true of nerves suppIying the mesia1 haIf of the rectus muscle when it is spIit for a transrectus approach. If the rectus muscIe is retracted IateraIIy, in order to spare these nerves, the trauma incident stretching is ehminated, but the incision overIies the abdomen at a point consider- abIy mesial to the appendicea1 region. This requires traction for delivery of the cecum.
The midhne incision is stiI1 farther re- moved from the ileocecal region, and pro- vides Iess strength after repair than the rectus incision, producing a11 the disad- vantages of dividing fascia transverse to its fibers, without the interposition of the rectus muscIe.
344
NEWSERIESVOL.LXVIII. No. 3 Murray-Appendectomy American Journal of Surgery 345
The idea1 approach to the ceIomic cavity This type of incision opens the abdomen for appendectomy is the transverse incision directIy over the iIeoceca1 area, and fre- advocated by Rockey and Davis. Origi- quentIy the appendix is visuaIized as soon
FIG. 6.
a-
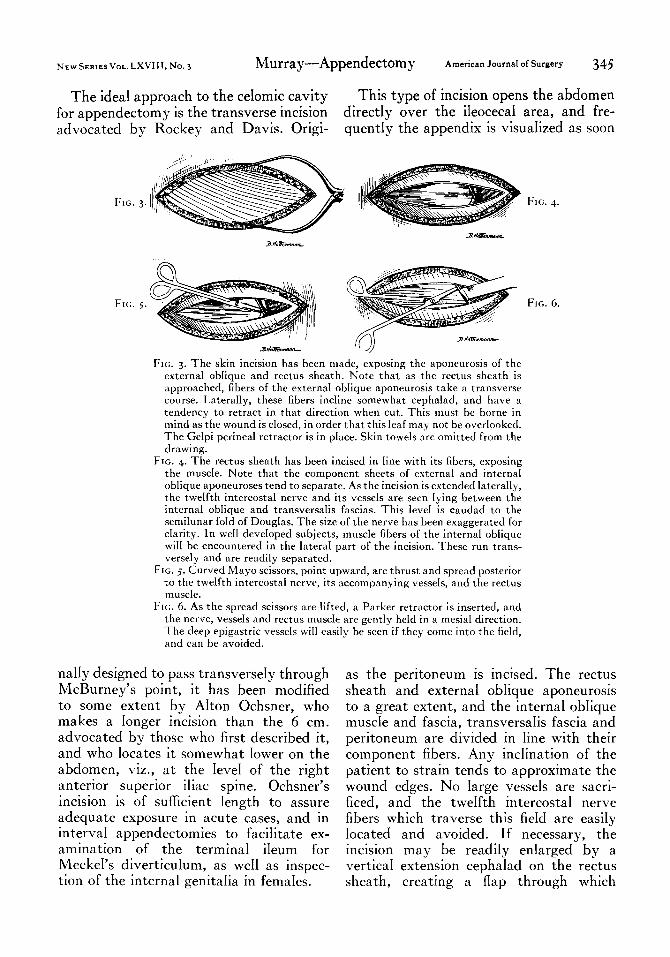
FIG. 3. The skin incision has been made, exposing the aponeurosis of the external oblique and rectus sheath. Note that as the rectus sheath is approached, fibers of the externa1 oblique aponeurosis take a transverse course. LateraIIy, these fibers incline somewhat cephalad, and have a tendency to retract in that direction when cut. This must be borne in mind as the wound is cIosed, in order that this leaf may not be overlooked. The GeIpi perineal retractor is in place. Skin towels are omitted from the drawing.
FIG. 4. The rectus sheath has been incised in line with its fibers, exposing the muscle. Note that the component sheets of external and internal obIique aponeuroses tend to separate. As the incision is extended IateraIly, the twelfth intercosta1 nerve and its vessels are seen Iying between the internal oblique and transversaIis fascias. This IeveI is caudad to the semilunar foId of Douglas. The size of the nerve has been exaggerated for clarity. In well deveIoped subjects, muscle fibers of the internal oblique will be encountered in the IateraI part of the incision. These run trans- versely and are readiIy separated.
FIG. 5. Curved Mayo scissors, point upward, are thrust and spread posterior to the twelfth intercosta1 nerve, its accompanying vessels, and the rectus muscIe.
FIG. 6. As the spread scissors are lifted, a Parker retractor is inserted, and the nerve, vesseIs and rectus musc1e are gently heId in a mesial direction. The deep eoigastric vesseIs will easily be seen if they come into the field, . .Y
and can be avoided.
naIIy designed to pass transverseIy through McBurney’s point, it has been modified to some extent by AIton Ochsner, who makes a Ionger incision than the 6 cm. advocated by those who first described it, and who locates it somewhat Iower on the abdomen, viz., at the IeveI of the right anterior superior iliac spine. Ochsner’s incision is of sufficient length to assure adequate exposure in acute cases, and in interval appendectomies to facilitate ex- amination of the terminal iIeum for MeckeI’s diverticuIum, as we11 as inspec- tion of the interna genitalia in femaIes.
as the peritoneum is incised. The rectus sheath and externa1 oblique aponeurosis to a great extent, and the interna obIique muscIe and fascia, transversaIis fascia and peritoneum are divided in Iine with their component fibers. Any inclination of the patient to strain tends to approximate the wound edges. No Iarge vesseIs are sacri- ficed, and the tweIfth intercosta1 nerve fibers which traverse this fieId are easiIy Iocated and avoided. If necessary, the incision may be readiIy enIarged by a vertica1 extension cephalad on the rectus sheath, creating a flap through which

346 American J0urnaI of Surgery -Murray-Appendectomy JUNE, "~45
adequate exposure has been provided for cholecystectomy incidenta to a mistaken diagnosis.
FIG. 7. Division of the peritoneum in line with its fibers, which arc transverse, completes the incision. It is not unusual to find the appendix lying in the wound.
The skin incision is made transversely from a point approximately over the center of the right rectus muscle to within 2 cm. of the right anterior superior iliac spine. (Fig. 2.) It is not unusual to encounter less than four superficial vessels requiring ligation. Subcutaneous tissue is divided to provide a clear view of the anterior rectus sheath and external obhque aponeurosis. (Fig. 3.) A GeIpi self-retaining peroneal retractor wiI1 be found usefu1 in keeping the skin edges apart.
The fascia is divided in line with the skin incision. As the rectus sheath is incised, the component external and internal ob- lique fascias wilI be seen to separate. (Fig. 4.) As the incision is carried IateralIy in we11 deveIoped subjects, muscIe fibers of the interna oblique will be encountered. These, however, run in line with the incision, and are easily separated. BIeedinp wiII be minimized if the handle of the scaIpe1 is used for this maneuver.
As the fascia at the IateraI border of the rectus sheath is divided, care shouId be exercised to avoid injury to the twelfth intercostal nerve and its concomitant vesseIs, which run between the interna ob- lique and transversaIis fascias. This is read- iIyseen, and shouId be inchrded in the Parker retractor used gentIy to hold rhe rectus muscle mesiaIIy. A pair of curved Mayo scissors thrust point upward and spread beneath the nerve and vesseIs wiII faciIitate the introduction of the rectractor. (Figs. 3 and 6.) As the rectus muscIe is Iifted
anteriorIy and mesialIy, the inferior epi- gastric vesseIs are in fuI1 view.
This IeveI is caudad to the semilunar fold of DougIas; hence only transversahs fascia and peritoneum remain to be incised. These structures are picked up and divided in Iine with the other incisions, viz., in a transverse manner. (Fig. 7,) EnIargement of the peritonea1 incision in either direction may be accomplished by tissue scissors under direct vision.
In cIosing, the peritoneum and trans- versaIis fascia are usuaIIy taken as one layer. When the rectus muscIe is allowed to faII back in pIace, it will be seen that much of the incision is covered. DeBakey has made the entire peritoneal opening posterior to the rectus muscle.
It wiI1 be found convenient when placing interrupted sutures, to have these cut to fourteen-inch lengths previousIy. The nurse should have severa loaded needle-holders avaiIabIe. As the sutures are inserted, the assistant gathers the ends, hoIding them in a sheaf. After the necessary number have been put in pIace, the assistant passes them back to the operator for tying, one at a time, making traction on the re- mainder. This approximates the wound edges, and greatly facilitates closure. When tying has been compIeted, the row of sutures is heId up and cut directly on the knots, Ieaving a minimum of thread in the wound.
The anterior rectus sheath is cIosed in one layer, care being taken that both the externa1 obbque and interna oblique com- ponents are incIuded. The cephaIad leaf of externa1 obIique aponeurosis has a tendency to retract and may be overlooked if care is not taken. Suturing as one layer continues unti1 the muscIe fibers of the internal oblique are encountered. If there has been a pronounced separation of fibers, a suture is inserted and tied IooseIy. The approximation of the fibers of the external obbque fascia is then continued IateraIIy. At this point the GeIpi retractor and skin toweIs are removed.

NEW SERIES VOL. LXVIII. No. 3 Murray-Appendectomy
SuperficiaI fascia is easiIy visualized by everting the skin edges, and is cIosed with interrupted sutures.
Approximation of the skin completes the procedure. The cosmetic effect, of minor importance from a surgical standpoint, sometimes warrants consideration, par- ticularly in young women. The transverse incision does not directly cross the skin lines of Langer in this region, and a thin scar results unless complications intervene.
The belt line is on a level with the iliac
crests, and consequentIy is completely cephalad to the scar, obviating the possi- bility of friction or pressure.
If drainage of the abdominal wall is indicated, rubber dam tissue may be in-
troduced laterally through the skin inci- sion, and directed in a mesial course to the peritoneum beneath the rectus muscle. This drains the entire incision.
CONCLUSION
The little used transverse incision for appendectomy may be made rapidly with Iittle damage to fascia, muscle, nerves or vessels. It produces excellent exposure, and is easily enlarged when necessary. It is readiIy cIosed even with the patient straining under a poor anesthetic. Fascia1 approximation with sutures transverse to component fibers provide a firm repair. The cosmetic effect is gratifying.
An unnecessary appendectomy should not be done during an abdominal
or pelvic operation which probably will be followed by some oozing of blood
into the peritoneal cavity. A sump drain is routineIy advisable if there is a
possibility of postoperative oozing both to indicate the presence and amount
of oozing and to keep the cavity free from blood and exudate. From “Principles and Practice of Surgery” by \\‘. U’avne Babcock
(Lea & Febiger).