tratamientosnuevospara el manejode la...
TRANSCRIPT

Tratamientos Nuevos Para el Manejo de La Hiperlipemia
Israel Hartman MD FACEProfesor Asistente de Medicina Interna
Departamento de EndocrinologiaUniversity of Texas Southwestern Medical Center
Dallas Texas
La Necesidad
• Eficacia Limitada de las estatinas• Tolerabilidad• Fallo de llegar a las metas establecidas
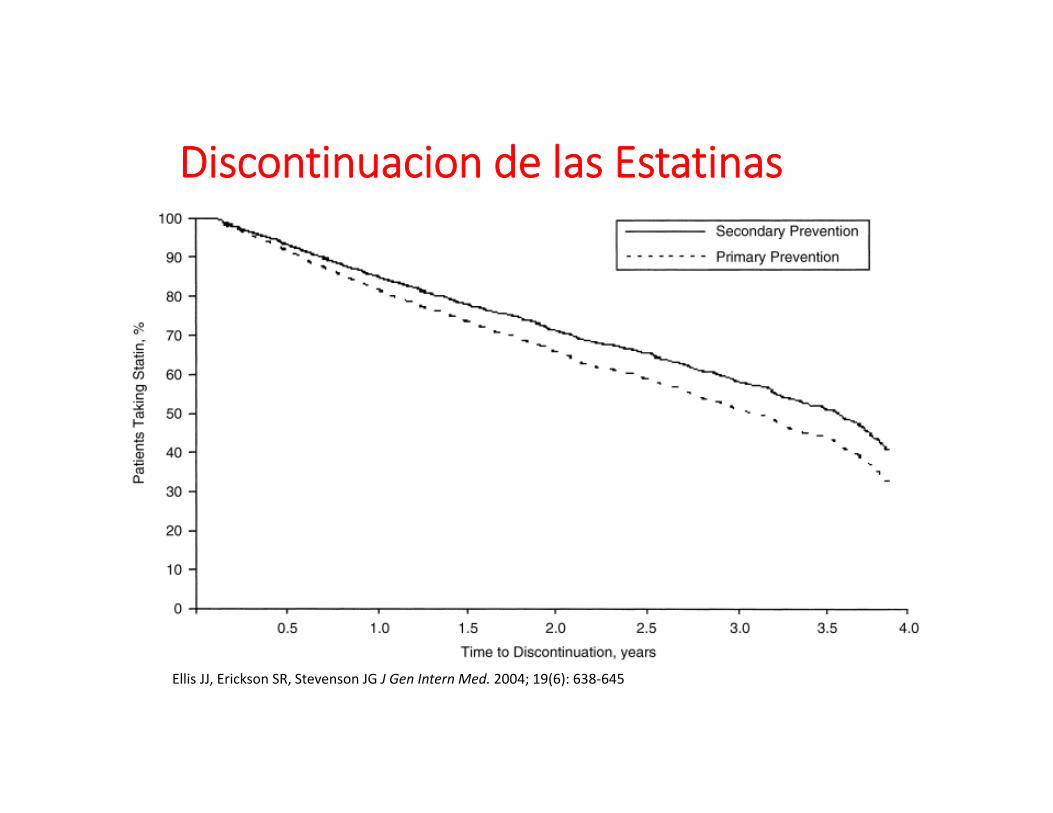
Discontinuacion de las Estatinas
Ellis JJ, Erickson SR, Stevenson JG J Gen Intern Med. 2004; 19(6): 638‐645

Riesgo Cardiovascular Residual en los estudios Clinicoscon Estatinas
0
5
10
15
20
25
30
Placebo
Statin
Secondary High‐risk Primary
N 4444 9014 4159 20,536 6595 6605
ΔLDL ‐35% ‐25% ‐28% ‐29% ‐26% ‐25%
Major coron
ary he
art d
isease even
ts (%
)

Tratamiento de“Dislipemia resistente al Tratamiento”
Procedimientos• LDL Apheresis
Farmacos• Lomitapide• (Juxtapid ®)
• Mipomersen• (Kynamro®)
• Alirocumab(Praluent®)
• Evolocumab(REPATHA)
Aprobados
AnacetrapibEvacetrapib
Futurostratamientos

Caso Clinico
• Hombre de 60 A referido por hiperlipemiarefractaria
• 3V CABG a los 28 A • Redo CABG a los 38 A• Angina and PCI LCx 2010• PCI SVG to LAD 2012
Caso Clinico
• Padre, madre y dos hermanos con historia de hiperlipemia severa
• Fue tratado con plasmaferesis en los 80’s hasta el el año2010 , Luego de esto se reuso a recivir mas tratamiento
• Tiene una funcion ventricular normal, tiene una vidaactiva
• Tolera el tratamiento con Atorvastatina 40mg y ezetamibapero no tolero una dosis mas alta

• Profil lipidico (en Lipitor 40 mg + Zetia 10 mg)
• Examen fisico : Xantomas tuberosos en el aquiles
Cual es el diagnostico ?
TC: 452TG: 238HDL: 43LDL: 362
Hyperlipemia Familiar
• Hiperlipemia Familiar Homozigota• Ambos padres y hermanos afectados• Elvacion extrema de el LDL (en tratamiento > 300 mg/dl, Sin tratar LDL > 500)
• Xantoma tuberoso es diagnostico

Hyperlipemia Familiar
• Herencia Autosoma Dominante• Prevalencia 1/500 heterozigotos (LDL 250‐500)• Homozigotos: Complicaciones y muerte <20 A (LDL > 600‐1000)
• Mutaciones geneticas en el Receptor LDL Y la interaccion con el APO B
• Sin tratar el riesgo de enfermedad cardiovascular es > 30% antes de los 40 A, > 50% a los 50 A
• 125 x el riesgo de los sujetor de la misma edad• Xantomas Tendinosos• No responden a dieta y ejercicio
Pediatrics;97:619‐28

Nabil G. Seidah et al. Circ Res. 2014;114:1022-1036
PCSK9

PCSK9: Fisiologia
Dadu, R. T. & Ballantyne, C. M. (2014) Lipid lowering with PCSK9 inhibitorsNat. Rev. Cardiol. doi:10.1038/nrcardio.2014.84

PCSK9 mAbAlirocumab(Praluent)
Evolucumab(Repatha)
Bococizumab*
Manufacturer Amgen Regeneron/Sanofi PfizerFDA Approval July 25, 2015 August 27, 2015
Approved doses (SQ q2 wks)
140 mg/1mL pen
* Currently in phase III trials
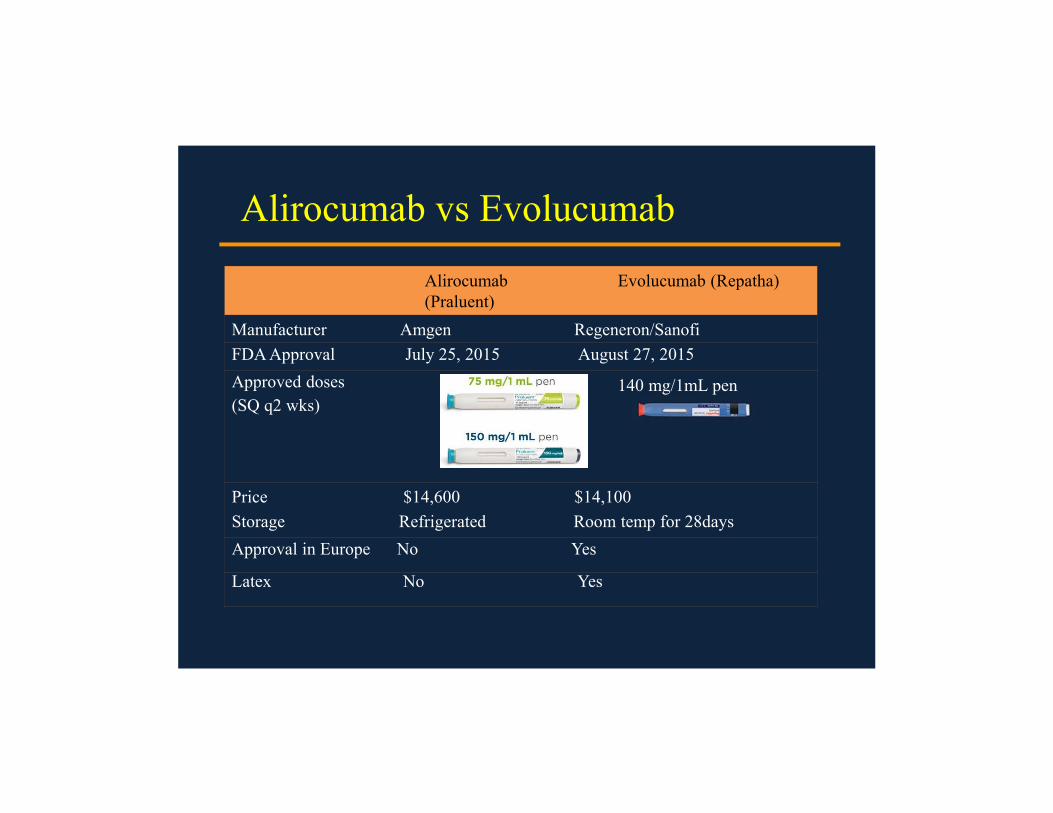
Alirocumab vs Evolucumab
Alirocumab(Praluent)
Evolucumab (Repatha)
Manufacturer Amgen Regeneron/SanofiFDA Approval July 25, 2015 August 27, 2015Approved doses (SQ q2 wks)
140 mg/1mL pen
Price $14,600 $14,100Storage Refrigerated Room temp for 28daysApproval in Europe No Yes
Latex No Yes

Indicationes
Adjunto a dieta y ejercicio y dosis maximaTolerada de estatina Para el manejo de adultoswithCon Hiperlipemia Familiar o Enfermedad
Cardiovascular
Note: evolocumab(Repatha) is also approved for use in patients with homozygous FH
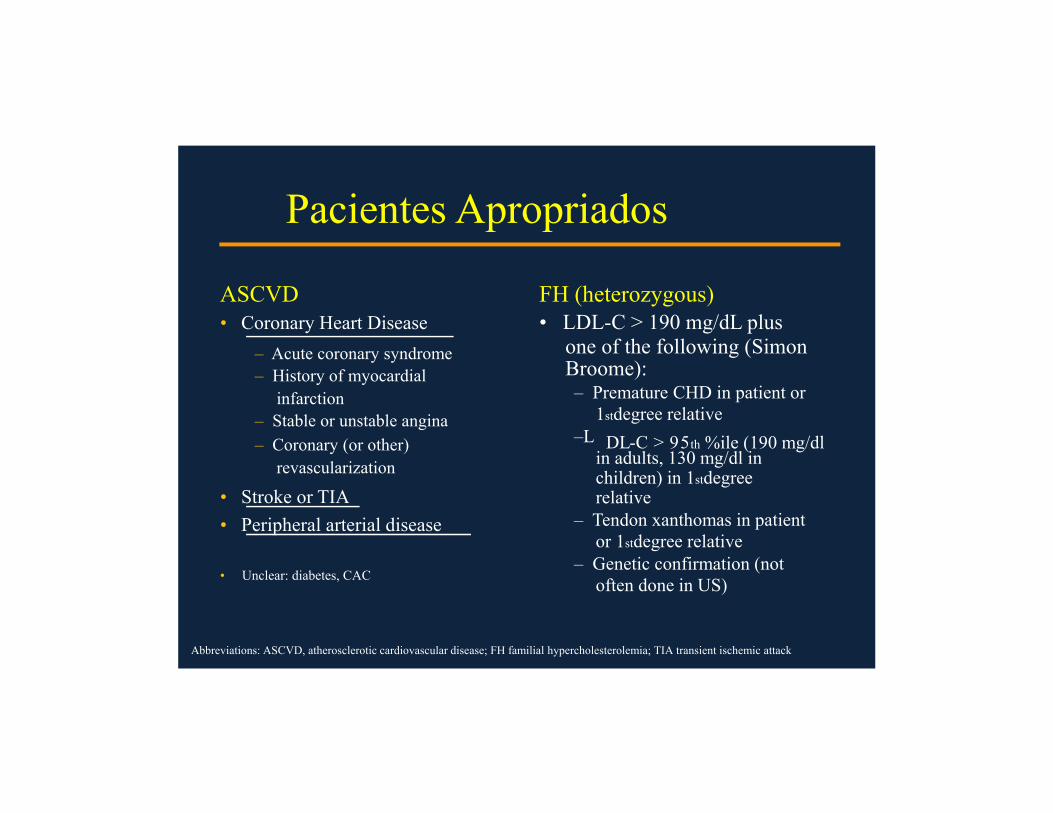
Pacientes Apropriados
ASCVD• Coronary Heart Disease
– Acute coronary syndrome– History of myocardial
infarction– Stable or unstable angina– Coronary (or other)
revascularization
• Stroke or TIA• Peripheral arterial disease
• Unclear: diabetes, CAC
FH (heterozygous)• LDL-C > 190 mg/dL plus
one of the following (Simon Broome):– Premature CHD in patient or
1stdegree relative–L DL-C > 95th %ile (190 mg/dl
in adults, 130 mg/dl in children) in 1stdegree relative
– Tendon xanthomas in patient or 1stdegree relative
– Genetic confirmation (not often done in US)
Abbreviations: ASCVD, atherosclerotic cardiovascular disease; FH familial hypercholesterolemia; TIA transient ischemic attack
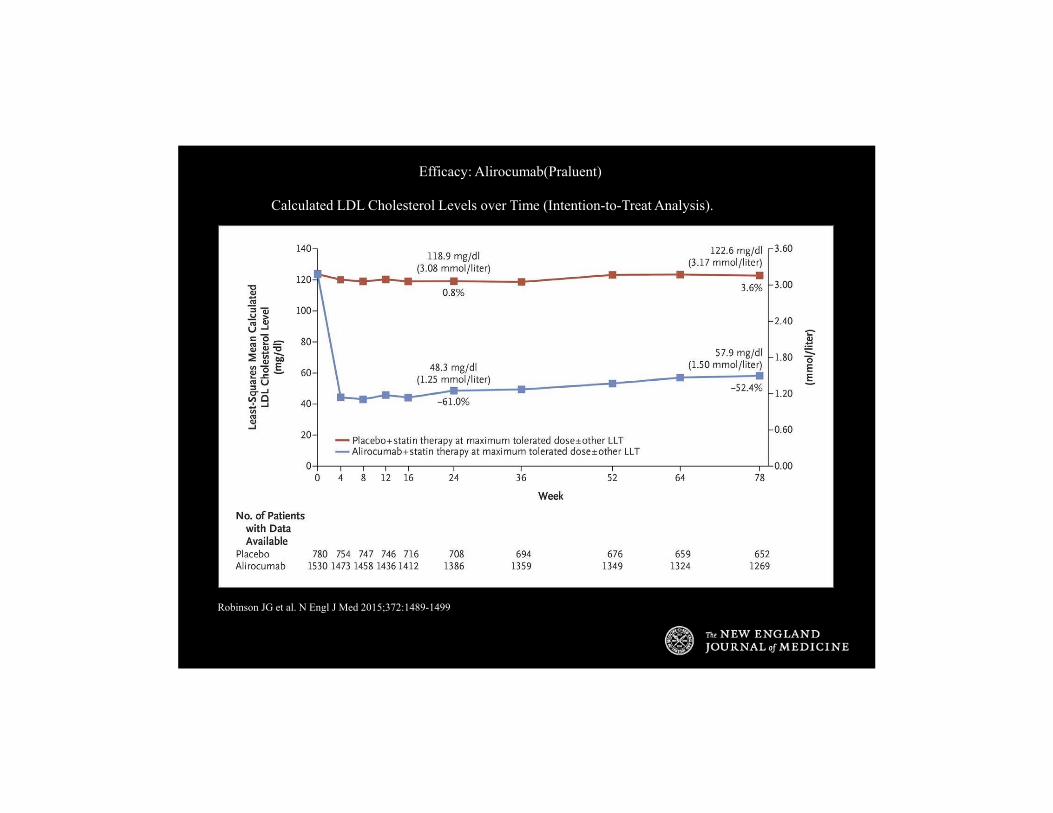
Efficacy: Alirocumab(Praluent)
Calculated LDL Cholesterol Levels over Time (Intention-to-Treat Analysis).
Robinson JG et al. N Engl J Med 2015;372:1489-1499

Efficacy of Evolocumab(Repatha): LDL-C
Sabatine MS et al. N Engl J Med 2015;372:1500-1509
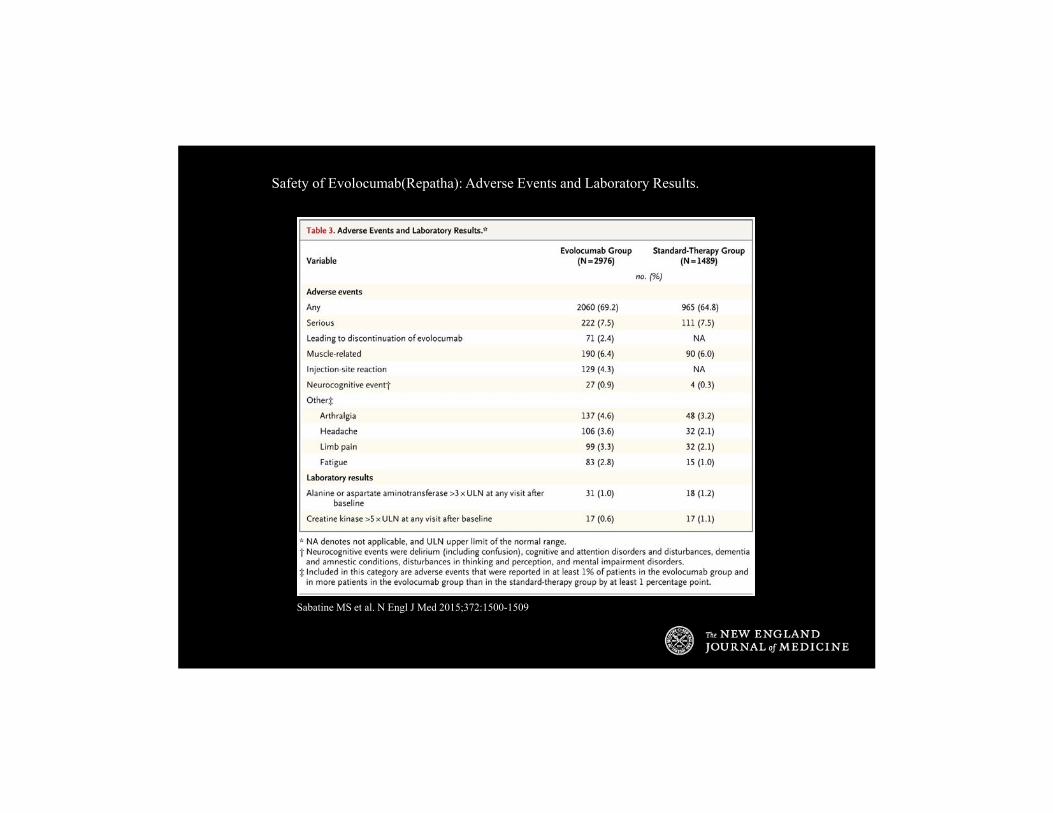
Safety of Evolocumab(Repatha): Adverse Events and Laboratory Results.
Sabatine MS et al. N Engl J Med 2015;372:1500-1509

PCSK9i En pacientesintolerantes a Estatinas
• PCSK9 mAb Aprobado para pacientes en“En Dosis Maximas de Estatina”–Interpretacion Variable:
• Dosis Alta/ Potencia (e.g. atorva80 mg diario)
• Dosis Maxima que el paciente puede tolerar(e.g. atorva10 mg de dia de por medio)• No nececidad de estatina si el paciente esIntolerante?

Figure 4. Kaplan–Meier estimates for time to first skeletal muscle–related AE (predefined as myalgia, muscle spasms, muscular weakness, musculoskeletal stiffness, or muscle fatigue). AE, adverse event; ALI, alirocumab; ATV, atorvastatin; CI, confidence interva...
Patrick M. Moriarty, Paul D. Thompson, Christopher P. Cannon, John R. Guyton, Jean Bergeron, Franklin J. Zieve, Eric Bruckert,
Terry A. Jacobson, Stephen L. Kopecky, Marie T. Baccara-Dinet, Yunling Du, Robert Pordy, Daniel A. GipeEfficacy and safety of alirocumab vs ezetimibe in statin-intolerant patients, with a statin rechallenge arm: The ODYSSEY
ALTERNATIVE randomized trialJournal of Clinical Lipidology, Volume 9, Issue 6, 2015, 758–769
http://dx.doi.org/10.1016/j.jacl.2015.08.006

GAUSS‐2
• Patients intolerant to at least 2 statins
• Randomly assigned to evolocumab vsezetimibe
• 12‐wk treatment• LDL‐C lowering ‐56% vs. ‐18%
Stroes E, Colquhoun D, Sullivan D, et al. J Am Coll Cardiol. 2014; 63:2541
EvolocumabMENDEL‐2
• Hypercholesterolemia – relatively low CAD risk
• No history of statin intolerance
• Placebo vs ezetimibevs evolocumab
• 12‐week treatment• LDL‐C lowering ‐1% vs. ‐18% vs. 57%
Koren MJ, Lundqvist P, Bolognese M, et al. J Am Coll Cardiol. 2014; 63:2531
Date of download: 7/8/2016 Copyright © 2016 American Medical Association. All rights reserved.
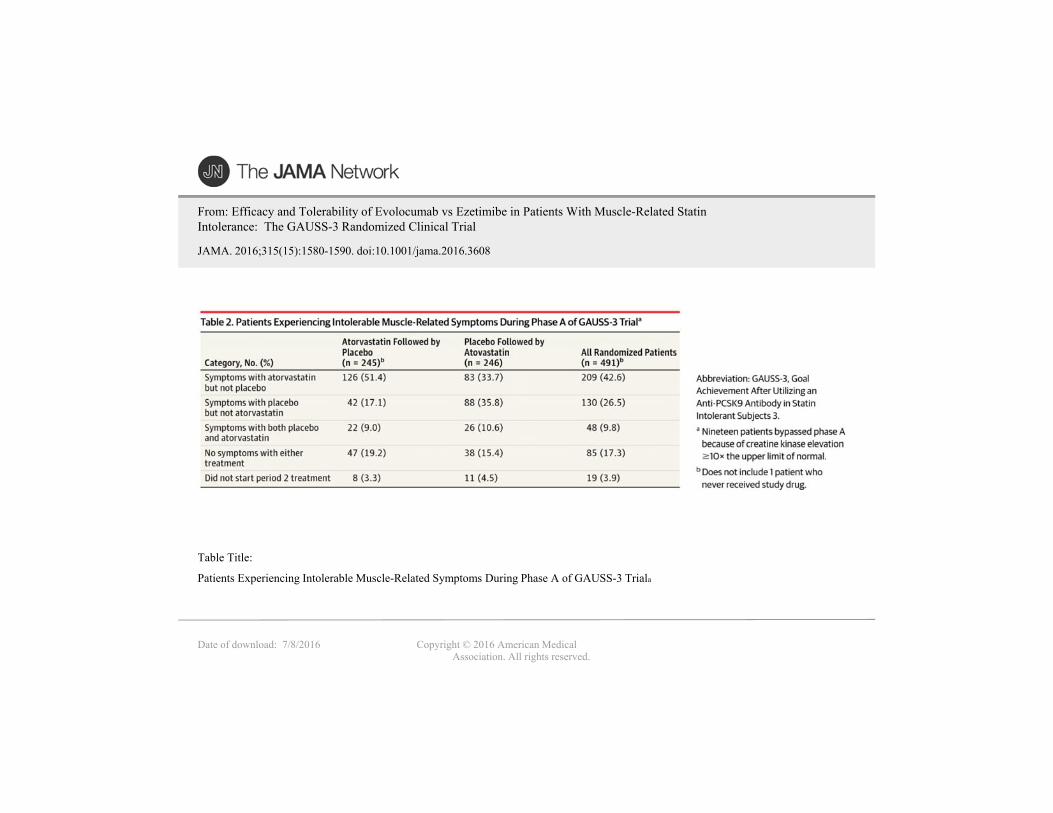
From: Efficacy and Tolerability of Evolocumab vs Ezetimibe in Patients With Muscle-Related Statin Intolerance: The GAUSS-3 Randomized Clinical Trial
JAMA. 2016;315(15):1580-1590. doi:10.1001/jama.2016.3608
Patients Experiencing Intolerable Muscle-Related Symptoms During Phase A of GAUSS-3 Triala
Table Title:
Date of download: 7/8/2016 Copyright © 2016 American Medical Association. All rights reserved.
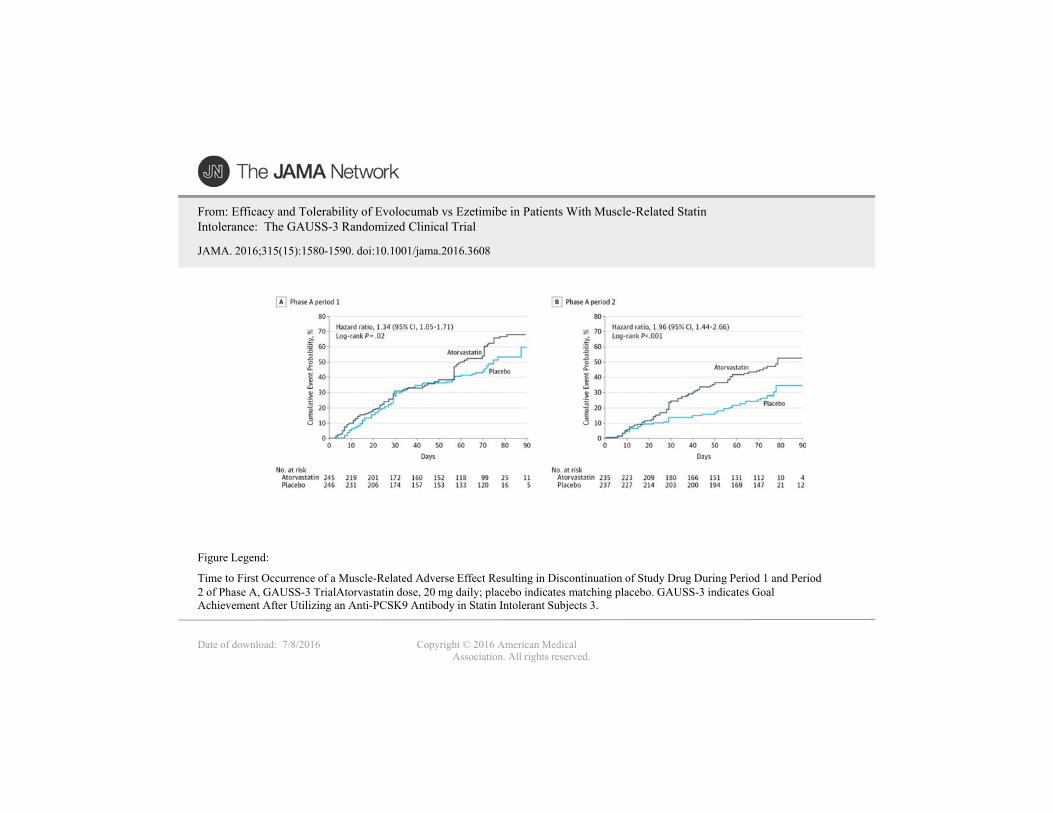
From: Efficacy and Tolerability of Evolocumab vs Ezetimibe in Patients With Muscle-Related Statin Intolerance: The GAUSS-3 Randomized Clinical Trial
JAMA. 2016;315(15):1580-1590. doi:10.1001/jama.2016.3608
Time to First Occurrence of a Muscle-Related Adverse Effect Resulting in Discontinuation of Study Drug During Period 1 and Period 2 of Phase A, GAUSS-3 TrialAtorvastatin dose, 20 mg daily; placebo indicates matching placebo. GAUSS-3 indicates Goal Achievement After Utilizing an Anti-PCSK9 Antibody in Statin Intolerant Subjects 3.
Figure Legend:
Date of download: 7/8/2016 Copyright © 2016 American Medical Association. All rights reserved.
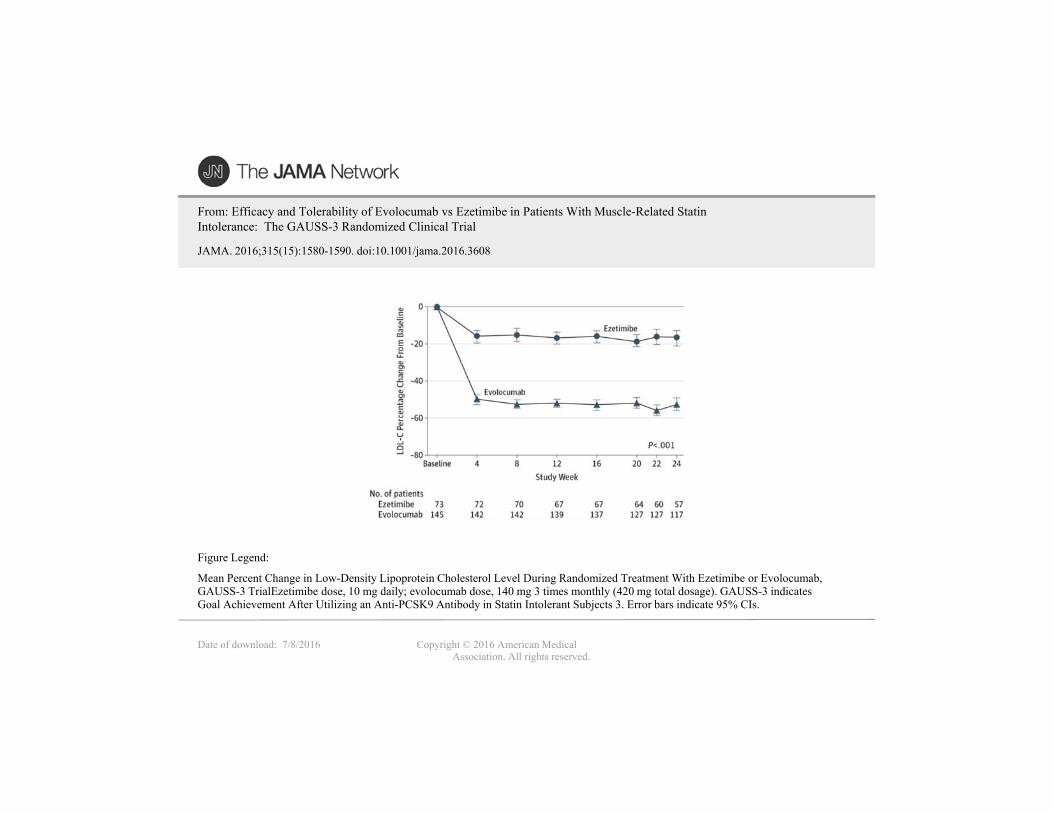
From: Efficacy and Tolerability of Evolocumab vs Ezetimibe in Patients With Muscle-Related Statin Intolerance: The GAUSS-3 Randomized Clinical Trial
JAMA. 2016;315(15):1580-1590. doi:10.1001/jama.2016.3608
Mean Percent Change in Low-Density Lipoprotein Cholesterol Level During Randomized Treatment With Ezetimibe or Evolocumab, GAUSS-3 TrialEzetimibe dose, 10 mg daily; evolocumab dose, 140 mg 3 times monthly (420 mg total dosage). GAUSS-3 indicates Goal Achievement After Utilizing an Anti-PCSK9 Antibody in Statin Intolerant Subjects 3. Error bars indicate 95% CIs.
Figure Legend:
SUMARIO• PCSK9 INH aumenta la cantidad de
LDLRs
• PCSK9 inh reducen el reduce LDL-C en un
50-60% con un perfil de seguridad favorable
• En 3 estudios clinicos en pacientes intolerantes
a las estatinas, bajaron efectivamente el LDL con
efectos secundarios comparables a ezetamidaPCSK9 inhibitors lower LDL-C effectively and
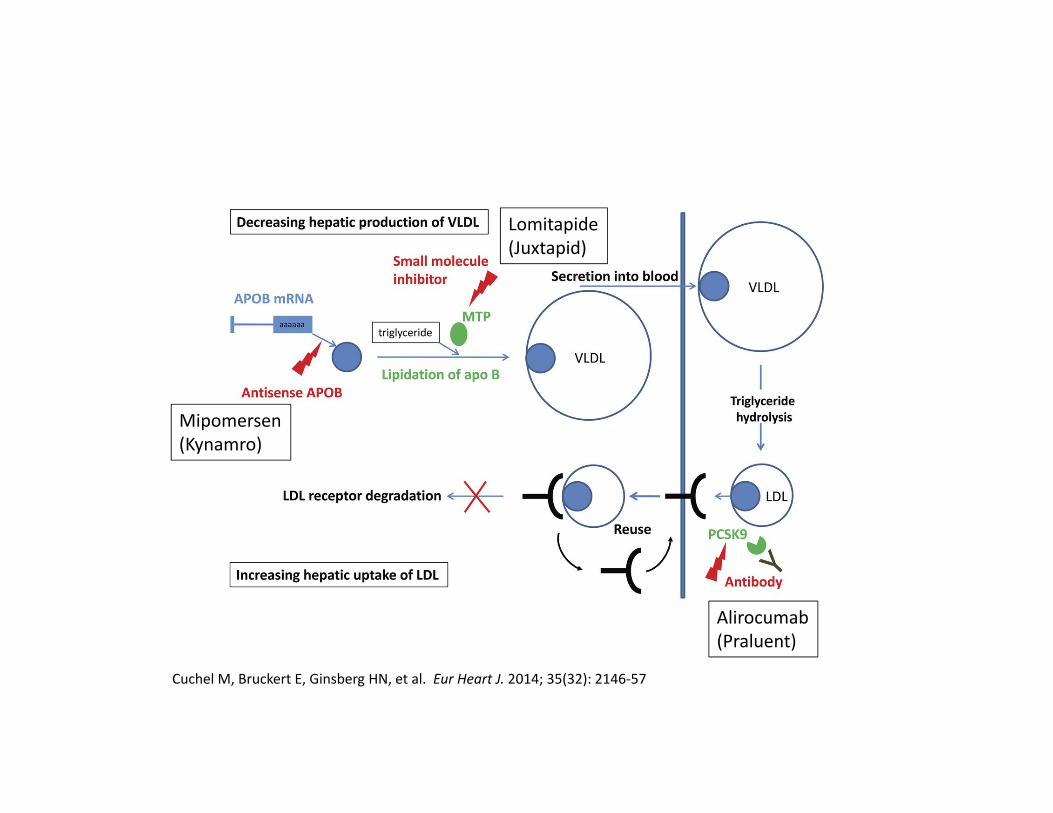
Cuchel M, Bruckert E, Ginsberg HN, et al. Eur Heart J. 2014; 35(32): 2146‐57
Mipomersen(Kynamro)
Lomitapide(Juxtapid)
Alirocumab(Praluent)

Juxtapid: LomitapideDosis oral diariaMTP inhibitor (microsomal transfer protein)Aprovado en pacientes en aferesis

Lomitapide – Eficacia
Decreased LDL‐C by 51% and apo B by 56% Cuchel M, Bloedon LT, Szapary PO, et al. N Engl J Med. 2007; 356:148

Lomitapide – Seguridad• Efectos Secundarios
• Sintomas GI• Elevacion de transaminasas
• Acumulacion de grasa hepatica
Lomitapide – Uso clinico• HF Homozigota• Agregada a dieta, estatinas o aferesis• Para pacientes que reusan o no son candidatos a aferesis u otros tratamientos
Mipomersen – FarmacologiaKynamro ®
• OligonucleotidoAntisensorcomplementario a la region codificadora de RNA de el APO B
• FDA‐Aprobada / Enero2013
• En HF

Mipomersen: Antisense Strand
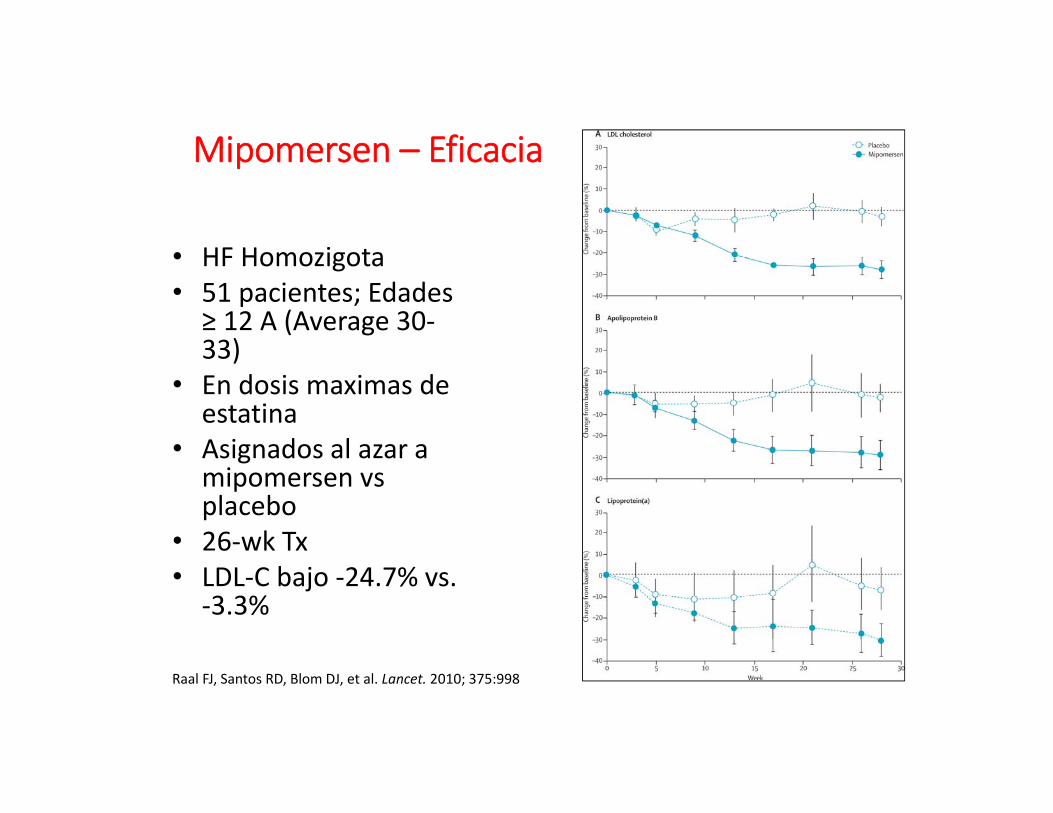
Figure 2
The Lancet 2010 375, 998-1006DOI: (10.1016/S0140-6736(10)60284-X) Raal FJ, Santos RD, Blom DJ, et al. Lancet. 2010; 375:998
• HF Homozigota• 51 pacientes; Edades
≥ 12 A (Average 30‐33)
• En dosis maximas de estatina
• Asignados al azar a mipomersen vs placebo
• 26‐wk Tx• LDL‐C bajo ‐24.7% vs.
‐3.3%
Mipomersen – Eficacia

Mipomersen – eficacia• Statin‐intolerant patients at high CAD risk• 33 patients• Mipomersen vs. placebo • 26 weeks • LDL‐C lowering ‐47%Visser ME, Wagener G, Baker BF, et al. Eur Heart J. 2012; 33:1142
• No FH and CAD or high CAD risk• 158 patients• Mipomersen vs. placebo as add‐on to statins• 26 weeks • LDL‐C lowering ‐36.9% vs. ‐4.5%Thomas GS, Cromwell WC, Ali S, et al. J Am Coll Cardiol. 2013; 62: 2178

Mipomersen – Seguridad• Efectos secundarios
• Reacccion al sitio de inyeccion• Sintomas gripales• Aumento de funcion hepatica

Mipomersen• 200 mg Sq wk• Aprovado en pacientes con HF

LDL Aferesis ‐ Pocedimiento
Thompson GR, Catapano A, Saheb S, et al. Curr Opin Lipidol. 2010; 21:492
• Removimientoextracorporal del APO B circulante
• Varios metodos• Semanal o bisemanal l
Blood withdrawal
Cells Plasma
Apo B containing lipoproteins
Waste line
Lower Apo B Plasma
Back to patient

LDL Aferesis – Seguridad• Efectos secundarios mas comunes
• Hypotencion• Anemia• Nausea• Flushing• Cefalea
• Necesida de acceso venoso• AV fistula / Central venous port
Thompson GR, Catapano A, Saheb S, et al. Curr Opin Lipidol. 2010; 21:492

LDL Aferesis ‐ Recomendaciones• Recomendaciones de el pane de la associacion de Lipidologos
• Pacientes que no responden adecuadamente al tratamiento luego de 6 meses
• HF Homozigota con LDL ≥ 300 mg/dl (or non‐HDL ≥ 330 mg/dl)
• FH Heterozigota con LDL ≥ 300 mg/dl (or non‐HDL ≥ 330 mg/dl) and 0‐1 risk factors
• HF Heterozigota con LDL ≥ 200 mg/dl (or non‐HDL ≥ 230 mg/dl)and ≥ 2 risk factors or lp(a) ≥ 50 mg /dl
• HF Heterozigota con LDL ≥ 160 mg/dl (or non‐HDL ≥ 190 mg/dl) and established CAD, other CV disease, or diabetes
Goldberg AC, Hopkins PN, Toth PP J Clin Lipidol. 2011; 5 S1

Anacetrapib and Evacetrapib – FarmacologiaCETP Inhibidores
• Aumento en HDL‐C • Reduccion en LDL‐C y apoB• Reduccion en lp(a)
TG
TGCholesterol
Cholesterol
VLDLHDL
LDL

Anacetrapib
• REALIZE ‐ efficacy • REVEAL – CV endpoints
Evacetrapib
• ACCENTUTAE ‐efficacy
• ACCELERATE – CV endpoints
clinicaltrials.gov – acc. July 2015

GRACIAS