trauma imaging and intervention: jcms2015
TRANSCRIPT

Emergency Radiology: ���What We Can Offer In Trauma Care
Rathachai Kaewlai, MD Division of Emergency Radiology, Department of Radiology Ramathibodi Hospital, Mahidol University, Bangkok, Thailand Joint Conference in Medical Sciences, Centara Grand @CentralWorld, Bangkok, Thailand | 6 Jun 2015

Ramathibodi Emergency Radiology

Outline
Trauma care: time-conscious process
CT imaging of solid organs and vascular injuries Pan-scan Endovascular treatment in trauma

Trimodal Death Distribution due to injury
Image credit: ATLS, 9th edition

Trimodal Death Distribution due to injury
First Peak: Seconds to minutes Apnea, massive hemorrhage Prevention only
Image credit: ATLS, 9th edition

Trimodal Death Distribution due to injury
Second Peak: Minutes to hours SDH/EDH, hemopneumothorax Visceral bleeding Pelvic fracture “Golden Hour of Care”
Image credit: ATLS, 9th edition
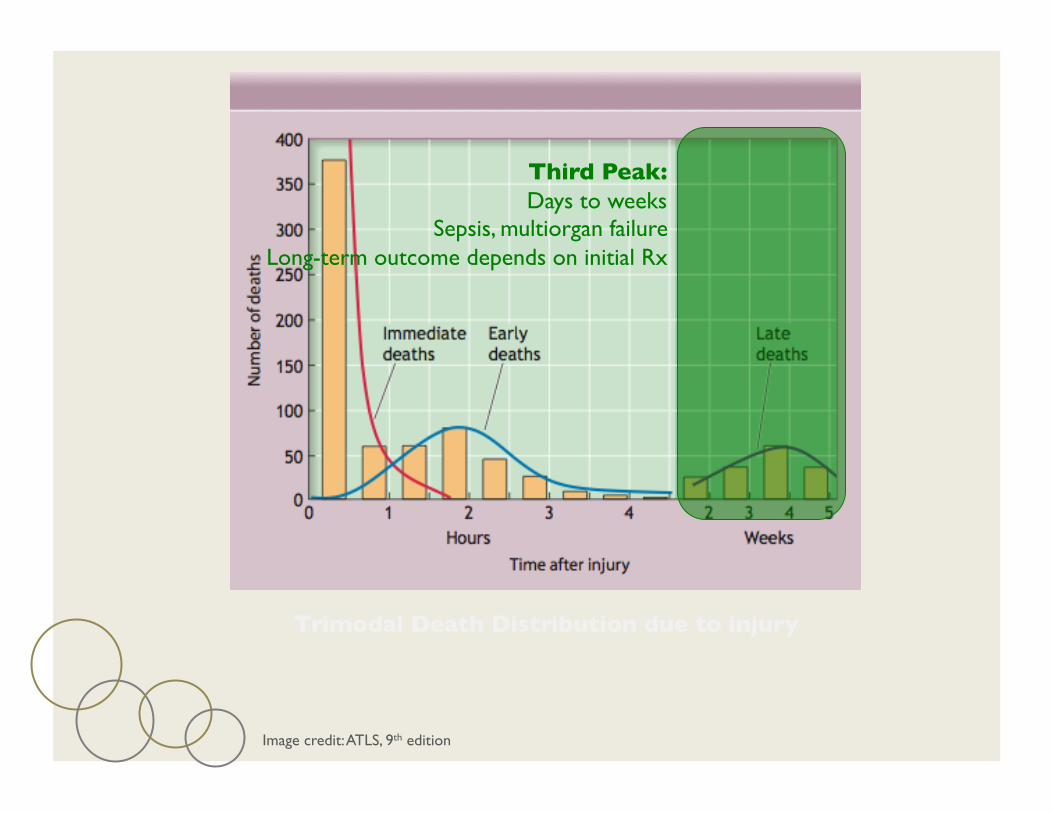
Trimodal Death Distribution due to injury
Third Peak: Days to weeks
Sepsis, multiorgan failure Long-term outcome depends on initial Rx
Image credit: ATLS, 9th edition

Initial Imaging Assessment and Management
AP chest radiograph
AP pelvic radiograph FAST
Spine x-ray
Extremity x-ray CT
Endovascular treatment

Time-conscious Care
Effective use of time to
- Obtain valuable information from imaging
- Minimize time spent
Valuable Information
Time

Trauma: Now It’s Time for CT
Quick
7-15 seconds (scanner time) 5-10 mins (in-room time) 15-20 mins (pan-scan)

Trauma: Now It’s Time for CT
Valuable
2D & 3D: easy to understand Accurate for traumatic injuries
Presence or absence
Grading Associated injuries
Epidural hematoma

Trauma: Now It’s Time for CT
Valuable
2D & 3D: easy to understand Accurate for traumatic injuries
Presence or absence
Grading Associated injuries
Lefort fractures

Trauma: Now It’s Time for CT
Valuable
2D & 3D: easy to understand Accurate for traumatic injuries
Presence or absence
Grading Associated injuries
Thoracic aortic injury

“Tuna Auction” at Tsukiji Fish Market
Image credit: Japan-Guide.com

16-year-old man with blunt head injury Epidural hematoma with significant mass effect
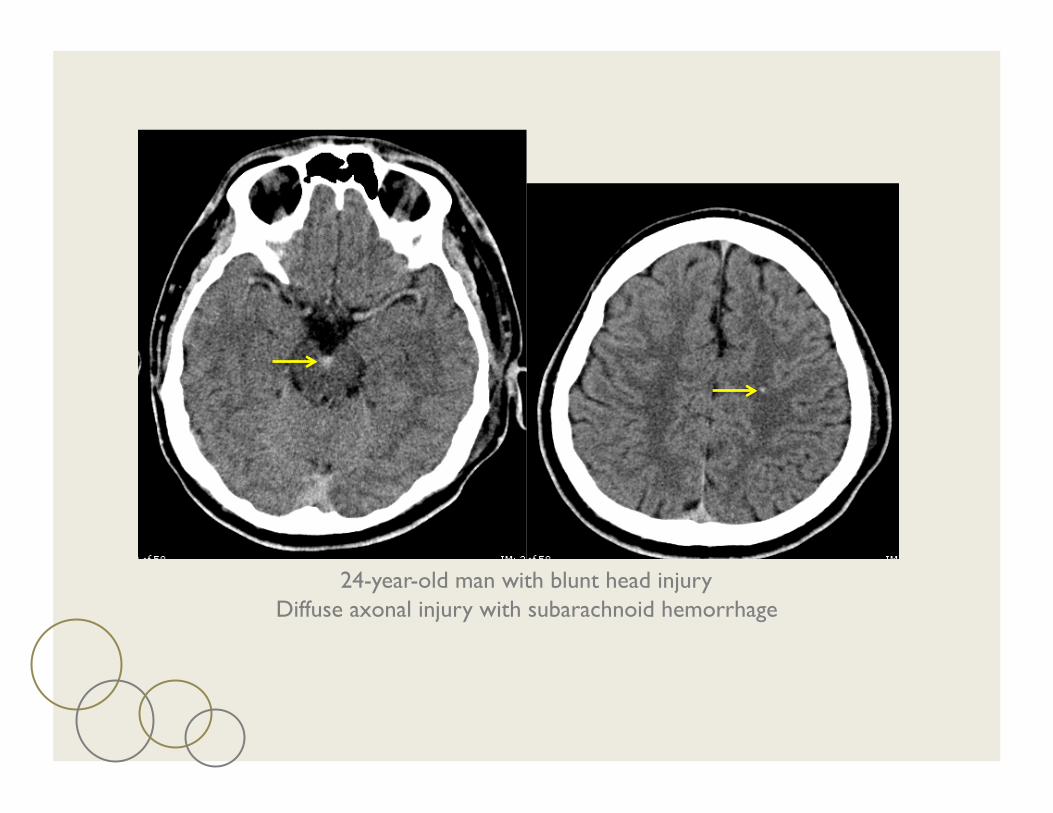
24-year-old man with blunt head injury Diffuse axonal injury with subarachnoid hemorrhage

80-year-old woman with neck trauma Burst fracture of C5
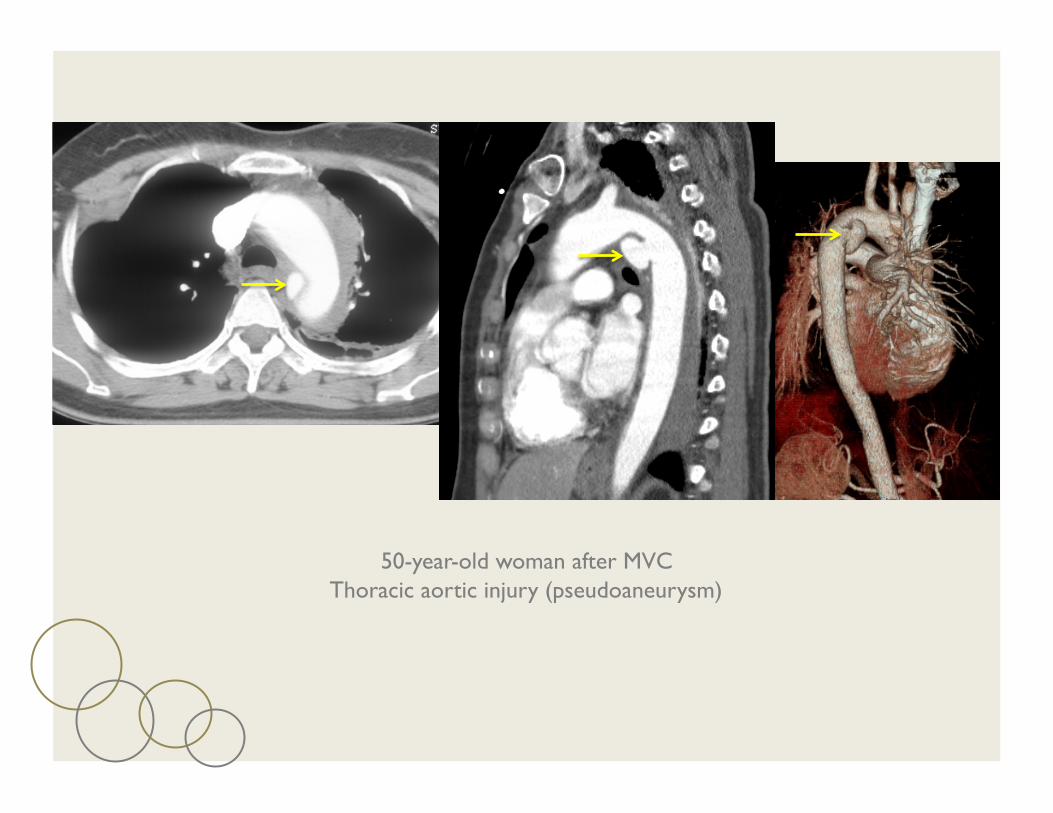
50-year-old woman after MVC Thoracic aortic injury (pseudoaneurysm)

Blunt left diaphragmatic rupture

Trauma CT
Selective or “Pan scan”
Pan scan = scanning from head to pelvis in one shot Pre-contrast head CT
Post-contrast neck, chest, abdomen and pelvis
Ramathibodi Protocol

“Pan Scan”
Indication based on severity of trauma and initial evaluations (clinical exam + FAST)
Ramathibodi Protocol

20-year-old woman
Non-contrast Head
Post-contrast Neck Post-contrast Chest, Abdomen

20-year-old woman, motorcycle vs. car SDH, vitreous hemorrhage, tonsillar herniation Pulmonary contusions, pneumothorax Buttock hematoma with active contrast extravasation

40-year-old man, motorcycle vs. car SDH, thoracic aortic injury, T-shaped acetabular fracture

40-year-old man with multiple trauma. Pulmonary contusions with active contrast extravasation, intrapulmonary chest tube, para-cardiac mediastinal hematoma with active contrast extravasation, splenic laceration with active contrast extravasation
“Pan Scan”
Should it replace other imaging in the primary survey (CXR, PXR, FAST and selective CT)?
CXR PXR FAST
Selective CT
Pan scan CT V

“Pan Scan”
Caputo ND, et al. J Trauma Acute Care Surg 2014
Dilemma continues…
Awaiting REACT-2 Trial (after 2016)

Trauma Angioembolization
Hemorrhage is the major preventable cause of trauma deaths within the first 48 hours of admission
55%
Death from blood loss in acute phase
Sauaia A, et al. J Trauma 1995

Trauma Angioembolization
Prolonged hypotension increases late deaths and long-term disability
Bloody vicious cycle Coagulopathy
Acidosis Hypothermia
Trauma.lbg.ac.at
Trauma Angioembolization
Advancement in catheter embolization system allows embolization of small target vessels with accuracy and speed – replacing the need for surgery

Embolic Materials
Image credits: neurointervention.blogspot.com, birthmarks.us, sterileeye.com
GELFOAM
PVA
COIL
GLUE

32-year-old woman after MVC Hepatic artery pseudoaneurysm within laceration
Coiling of pseudoaneurysm

39-year-old man after MVC Thoracic aortic injury with stent-graft placement

Conclusions
Radiology is helpful in both Dx and Rx of trauma
CT is the workhorse for detection of life-threatening injuries (bleeding), grading and guiding Rx
Endovascular Rx is emerging as a valuable option for “damage control” in actively bleeding patients, and treating traumatic vascular injuries

THANK YOU FOR ���YOUR ATTENTION!