trauma skeletal radiology -...
TRANSCRIPT

Trauma Skeletal Radiology
Hand & Wrist
L J Brimicombe
Suspected trauma
Indicate the following
on the request form: Side involved and body part
Mechanism of injury
Exact site of focal tenderness related
to a specific bone or joint
(IRMER requirement)
Incomplete/Inadequate requests
without all the above information
may not be processed.
If clinical findings remain unexplained
recheck that imaging for the area of clinical
concern has been requested with the
relevant and appropriate clinical
Information
Appropriate further management
? Need for delayed imaging/fracture clinic
referral
P
R
O
T
O
C
O
L
P
R
O
T
O
C
O
L

Systematic Film Evaluation
Alignment
Bones
Cartilage
Soft Tissue
Evaluate the ABC’S!

Alignment
Bowing
Normal position of bones
Spaces between bones
Symmetry
Angulations

Bones
Periosteal Reaction
Anomalies in the cortex, breaks, overlaps &
steps.
Changes in trabecular pattern
Changes in densities

Cartilage
Look for avulsion fractures
Misalignment
Effusions
Soft Tissue
1. Defect on normal contours
2. Obvious swelling
3. Foreign body (e.g. glass) in soft tissues
4. A fluid/solid interface (lipohaemoarthrosis)
5. A gas/fluid interface (perferation)

Finger Nail Bed Injury

Avulsions of the Medial and/or Lateral Co-lateral Ligaments

Avulsion From the Insertion of the Volar Plate

Avulsion of the Extensor Tendon

Swan Neck Deformity
Swan neck deformity is a
condition in which the
distal joint (behind the
nail) of the finger goes into
flexion and the proximal
joint goes into extension.

Boutonniere Deformity
Initially, the
finger is painful
and swollen
around the PIP
joint.
The PIP joint
may not
straighten out
completely
under its own
power.
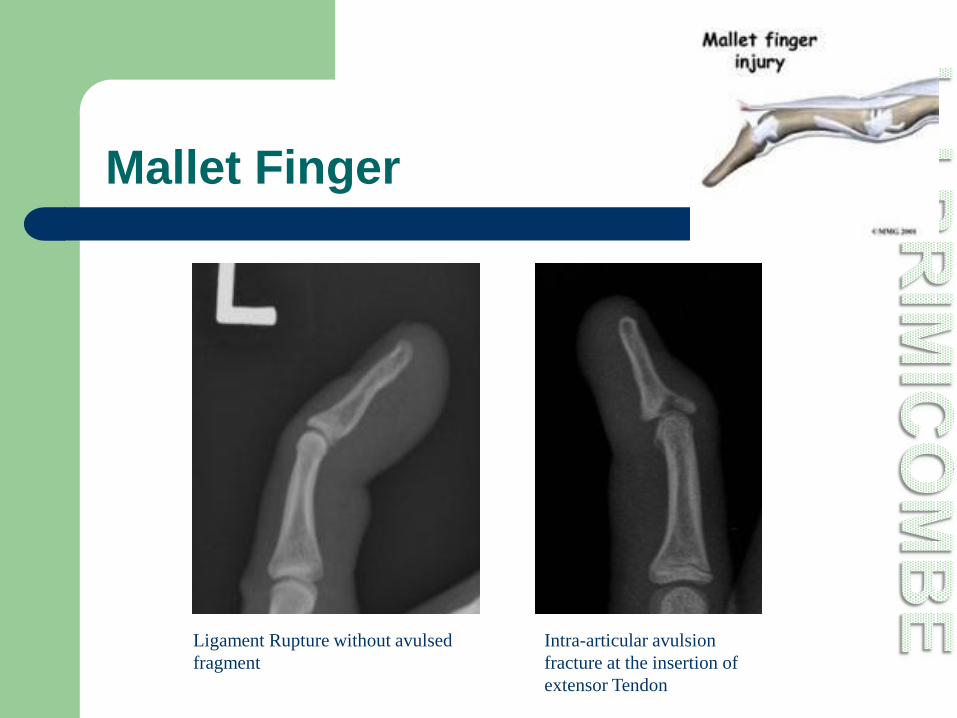
Mallet Finger
Intra-articular avulsion
fracture at the insertion of
extensor Tendon
Ligament Rupture without avulsed
fragment

Dislocation

Fracture Dislocation Coaches Finger
• Named after baseball coaches
• Most common hand injury in
athletes, especially among those
who play ball-handling sports
• Most cases, the dislocation happens
because the fingers are bent
backward when an athlete tries to
catch a ball or block a shot.
• Proximal interphalangeal joint
dislocations can happen when an
athlete’s fingers are twisted or bent
by an opponent.

Boxers Fracture
Blow from a “roundhouse" motion, fractures 4th or 5th or both

Fighter’s Fractures
• Instead of using a
"roundhouse" motion,
the blow comes straight
from the body
• This is typical of a skilled
fighter
• The 2nd Metacarpal is
fractured.

Dislocation Carpometacarpal joint
Most common are 4th and 5th metacarpals
Associated with fractures at the base of
affected metacarpal or an adjacent one
When a fracture of hamate is seen it is likely to
have an associated dislocation of the 5th
metacarpal joint.

Hand Less Obvious Fractures
If a base of 5th is suspected an AP rather than PA view and a
reverse oblique can be useful

Trapezio-Trapezoidal Junction
Oblique View

Carpel Arcs
I. Smooth curve outlining
the proximal convexities
of the scaphoid, lunate
and triquetrum.
II. Traces the distal
concave surfaces of the
same bones
III. Follows the main
proximal curvatures of
the capitate and hamate.

Disruption of arc I
There is disruption
of arc I at the lunate
triquetral joint
Suggestive of a
triquetral fracture
A posterior
fragment maybe
seen on the lateral

Disruption of Arc II
There is a step in the
scapho-lunate joint
and the luno-triquetral
joint is seen on the
left.
Terry Thomas Sign

Disruption Arch III
There is an
abnormal step off
at the capito-
hamate joint.
Hamate Fracture
AP rather than PA
view advised

Hand – Fracture Dislocations

Hand – Associated Fractures
Fracture of Hamate With an associated fracture through
the base of the 4th metacarpal

Thumb Attachments

Thumb – Bennetts Fracture Dislocation
Unstable
An oblique intra-articular fracture at the base of
the 1st metacarpal,
The abductor pollicis longus muscle pulls the
main body away.

Thumb – Rolando’s Highly Unstable
Similar to the Bennett’s fracture-dislocation,
but this intra articular fracture is comminuted.
Extra-articular fractures are stable!
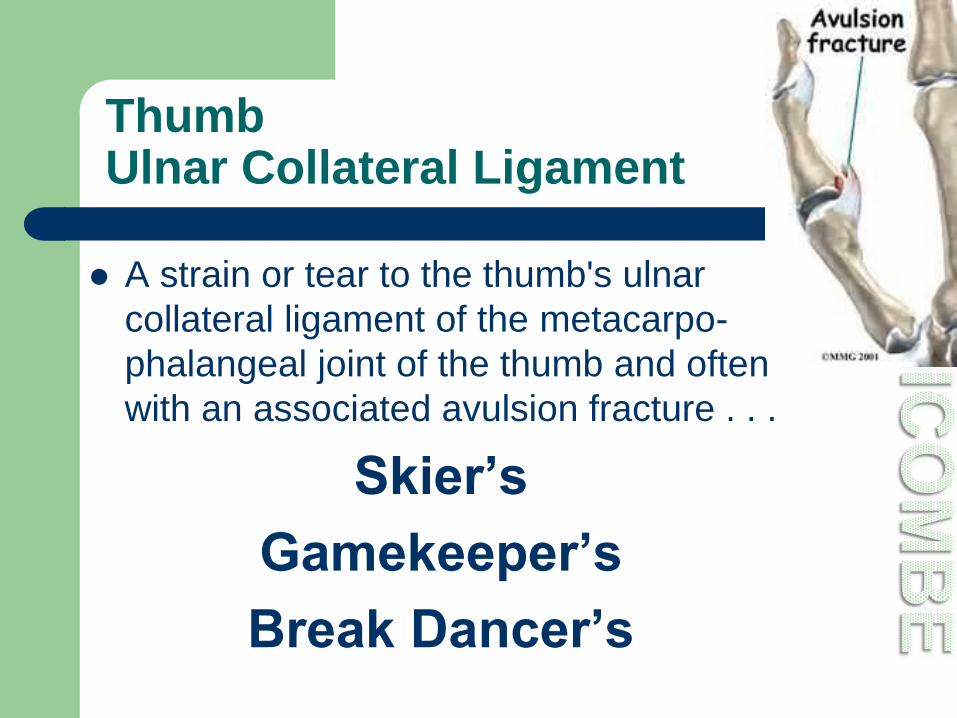
Thumb Ulnar Collateral Ligament
A strain or tear to the thumb's ulnar
collateral ligament of the metacarpo-
phalangeal joint of the thumb and often
with an associated avulsion fracture . . .
Skier’s
Gamekeeper’s
Break Dancer’s

Gamekeeper’s Thumb
• Injury occurs breaking rabbits necks
between the ground and the
gamekeeper's thumb and index
fingers.
• A valgus force was placed onto the
abducted MCP joint, leading to the
injury
• Resulting in instability, accompanied
by pain and weakness of the pinch
grasp.

Skier’s Thumb
• Usually results from a fall on an
outstretched hand that continues
to hold the ski pole.
• A valgus force is placed onto the
abducted MCP joint, leading to
injury
• Resulting in instability,
accompanied by pain and
weakness of the pinch grasp.
• May comprise up to 50% of
injuries to hand in skiers

Break Dancer’s Thumb
A valgus force is placed
onto the abducted MCP
joint, leading to injury
A valgus force was placed
onto the abducted MCP
joint, leading to the injury
Resulting in instability,
accompanied by pain and
weakness of the pinch
grasp.

Dislocated 1st Carpometacarpal

Eaton Littler Views
Stress views of thumbs
Osteoarthritis to bases
of 1st metacarpal-carpal
joint
Often shows
subluxation of the joint

Wrist Anatomy

Wrist Anatomy

Normal Wrist Angulation
Normal palmer tilt of the radial
articular surface
If the tilt is not present suspect
an impacted fracture

Normal Wrist Allignment
ANT.
Wrist
A fall on the out-stretched hand (FOOSH) tends to result in specific
injuries depending on the general age of the patient:
4-10years – Torus fracture of the distal radial metaphysis
11-16years – Salter-Harris II fracture involving the physeal plate
17-40years – Scaphoid fracture
Over 40years – Colles-type fracture

Radial Styloid Process Fractures
Fractures are common
due to blunt trauma
directly to the radial
styloid process
Fractures are oblique,
intra-articular and are
usually minimally
displaced

Chauffeur Fracture
A vertical fracture of the radial
styloid process
Typically a blow to the back of
the wrist
Name comes from trying to
start an old-fashioned car with
a hand crank resulted in it
rapidly spinning backwards
out of the driver's grasp and
striking the back of the wrist
Displacement is uncommon

Barton’s Fracture – Dorsal Type
A comminuted intra-articular
fracture of the distal radius,
(shearing fracture) extending
through the dorsal aspect to
the articular surface, and not
to the volar aspect.
Dorsal rim and carpus are
displaced dorsally and
proximally
There can be associated
carpal subluxation /
dislocation.

Reverse Barton’s – Volar Type
A comminuted intra-
articular distal radial
fracture with volar
displacement
Volar rim maintains
relationship with the
carpus, both displace
proximally (blue)
Fracture of radial styloid
process with loss of
radial definition (yellow)

Die Punch
Blue arrow indicates the
depressed fragment of the
lunate fossa.
Note: an articular step-off.
Yellow arrow indicates a
subtle fracture of the radial
styloid process.
There is no disruption of
carpal arc.
EASILY OVERLOOKED!

Wrist – Smith’s
Occur in younger patients
Resulting from high energy
trauma on the volar flexed wrist.
Fracture through the distal 5cm of
radius
An associated fracture through
the ulna styloid process
Anterior displacement of the distal
fragment

Colles’
A fracture of the distal metaphysis of the
radius with dorsal angulation and
displacement leading to a ‘dinner fork
deformity'.
An associated fracture of the ulna styloid
process
Frequently with advancing age and in
women with osteoporosis.
In many cases extra-articular,
uncomplicated and stable fracture
It can be intra-articular.
Look for signs of instability:
– Intra-articular radiocarpal or distal radial
ulna junction extension of the fracture
– Radial shortening
– Loss of radial inclination

Colles an insufficient description ?
Extension into the radiocarpal
joint and the distal radioulnar
joint
Displacement of the articular
fragments (blue arrow)
Radial shortening and loss of
radial inclination resulting in
distal ulna abutting the lunate
(yellow arrow)
Fracture of ulnar styloid

Scaphoid Appearance

Importance of Ulna Deviation
The shape of the
scaphoid changes
with movement of
the wrist.
In ulnar deviation
the scaphoid
elongates to fill the
space between the
radial styloid and
the trapezium
Without With

Scaphoid – most common carpus fracture the majority are waist type
Waist Scaphoid # Often non-displaced
Difficult to see initially
At 10-14 days demonstrates sclerosis
or re-absorption at the fracture line
Important to pick up! As the blood supply enters at the waist and can be disrupted resulting
in delayed union or avascular necrosis of the waist and proximal pole.

Scaphoid Blood Supply

Scaphoid – Distal Pole
•Fractures at the distal
pole are usually avulsion
injuries.
•The distal pole has its
own blood supply, so
healing is quick.
A child’s scaphoid injury

Scaphoid Importance of the 10/14 day rule
1st Presentation 14 days later

Scaphoid Ruptured Scapho-Lunate Ligament
Terry Thomas Sign
Clench Fist View
Demonstrates this well

Scaphoid - Children
7yrs & Below Scaphoid NOT ossified
Younger than 12yrs Dedicated scaphoid views not
necessary. Injuries NOT adult
type and can be
clearly seen on a ulna deviated PA
Wrist.

Triquetral- 2nd most common fracture in carpus
Posterior fragment
seen on the Lateral view

Hamate Fractures
Associated with fracture-dislocations
at the base of the 4th and 5th metacarpals.
(as mentioned before)
Important to spot but often subtle.
Check the cortex of the hamate,
particularly on an oblique view.
Ensure there is a 2mm joint space with
the adjacent metacarpals on the PA view

Pisiform Fractures
A reverse oblique
shows the pisiform
Pisiform Fractures are
occasionally seen due
to direct trauma

Carpus Fractures
Isolated fractures to the other carpus are rare:
Lunate
Capitate
Trapezium
Trapezoid

Obvious seen, subtle overlooked
A Scaphoid and Capitate fracture
Plus a Peri-lunate dislocation.

Differentiation between Lunate and Peri-Lunate Dislocations
The key is what is centred
over the radius.
– If the capitate is centred over the
radius and the lunate is
displaced anteriorly, it is a lunate
dislocation.
– If lunate is centred over the
radius and the capitate is
displaced posteriorly, it is a peri-
lunate dislocation

Lunate Dislocation
• Lunate loses its
articulation with both the
capitate and the radius
• Lunate displaces
anteriorly with up to
90 degrees rotation
• The capitate remains
aligned with the radius
but sinks proximally
Triangular
Appearance
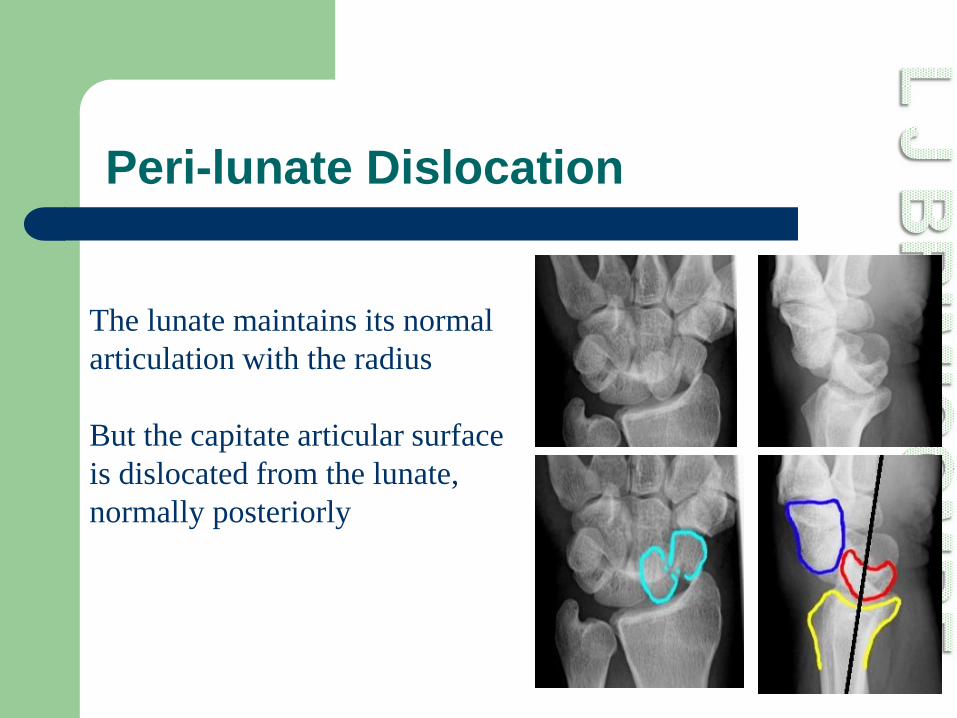
Peri-lunate Dislocation
The lunate maintains its normal
articulation with the radius
But the capitate articular surface
is dislocated from the lunate,
normally posteriorly

Midcarpal Dislocation
The lunate tilts anteriorly
but is not dislocated from
the radius
The capitate is dislocated
from the lunate but not as
posterially as seen in a
perilunate dislocation

Forearm – Galeazzi Fracture Dislocation
•Fracture of the Radius
•Dislocation of the distal
Radio-ulna joint
Normal Abnormal

Zone of Vulnerability
If one abnormality if
detected with the
zone there is
possibly another
within the zone, be it
fracture, dislocation
or both.
