travellers' health 2
TRANSCRIPT

Travelers’ HealthPart 2
(Post-Travel Evaluation)By
Mohammed Ezz El-din Abd El-monemAssistant Lecturer of Tropical Medicine & Gastroenterology
Faculty of Medicine, Assiut UniversityEmail: [email protected]

General Approach to the Returned Traveler

THE POST-TRAVEL EVALUATION
•Most post-travel infections become apparent soon after travel, but because incubation periods vary, some syndromes can present months to years after initial infection.
•When evaluating a patient with a probable travel-related illness, the clinician should consider this items:

Important elements of a medical history in an ill returned traveler• Severity of illness• Travel itinerary and duration of travel• Timing of onset of illness in relation to
international travel• Past medical history and medications• History of a pre-travel consultation• Travel immunizations• Adherence to malaria chemoprophylaxis• Individual exposures
• Type of accommodations• Insect precautions taken (such as
repellent, bed nets)• Source of drinking water• Ingestion of raw meat or seafood or
unpasteurized dairy products• Insect or arthropod bites• Freshwater exposure (such as swimming,
rafting)• Animal bites and scratches• Body fluid exposure (such as tattoos,
sexual activity)• Medical care while overseas (such as
injections, transfusions)

Travel Itinerary• The itinerary is crucial to formulating a differential diagnosis, because
potential exposures differ depending on the region of travel.
• A 2013 study from the GeoSentinel Surveillance Network found a distinct pattern of diagnoses depending on the region of the world visited. In travelers to sub-Saharan Africa presenting with fever, malaria was the most common specific diagnosis. On the other hand, febrile patients who traveled to Latin America or Southeast Asia were much more likely to have dengue.
• The duration of travel is also important, since the risk of a travel-related illness increases with the length of the trip.
Timing of Illness in Relation to Travel•Most ill travelers will seek medical attention within 1 month
of return from their destination, because most common travel-related infections have short incubation periods.
• Occasionally, however, infections such as schistosomiasis, leishmaniasis, or tuberculosis can manifest months or even years later.
• Therefore, a detailed history that extends beyond a few months before presentation can be helpful.

Illnesses associated with fever presenting in the first 2 weeks after travel
• Systemic febrile illness with initial nonspecific symptoms
MalariaDengueTyphoid feverRickettsial diseases (such as scrub typhus, relapsing fever)East African trypanosomiasisAcute HIV infectionLeptospirosis
• Fever with central nervous system involvement
Meningococcal meningitisMalariaArboviral encephalitis (such as Japanese encephalitis virus, West Nile virus)East African trypanosomiasisAngiostrongyliasisRabies

• Fever with respiratory complaints
InfluenzaBacterial pneumoniaAcute histoplasmosis or coccidioidomycosis, Legionella pneumoniaQ feverMalariaTularemiaPneumonic plague
• Fever and skin rash
DengueMeaslesVaricellaSpotted-fever or typhus group rickettsiosisTyphoid feverParvovirus B19MononucleosisAcute HIV infection
Underlying Medical Illness• Comorbidities can affect the susceptibility to infection, as
well as the clinical manifestations and severity of illness.
• An increasing number of immunosuppressed people (due to organ transplants, immune-modulating medications, HIV infection, or other primary or acquired immunodeficiencies) are international travelers.

Vaccines Received and Prophylaxis Used• The history of vaccinations and malaria chemoprophylaxis should be reviewed
when evaluating an ill returned traveler.
• Although adherence to malaria chemoprophylaxis does not rule out the possibility of malaria, it reduces the risk and increases the chance of an alternative diagnosis.
• Fever and a rash in a traveler without an up-to-date measles vaccination would raise concern about measles.
• The most common vaccine preventable diseases found in a large 2010 GeoSentinel study of returned travelers included enteric fever (typhoid and paratyphoid), viral hepatitis, and influenza. More than half of these patients with vaccine-preventable diseases were hospitalized.

Individual Exposure History• Knowledge of the patient’s exposures during travel, including insect bites, contaminated
food or water, or freshwater swimming, can also assist with the differential diagnosis.
• In addition to malarial parasites, mosquitoes can transmit viruses (such as dengue virus, yellow fever virus, and chikungunya virus) and filarial parasites (such as Wuchereria bancrofti).
• Depending on the clinical syndrome and location of exposure, a history of a tick bite could suggest a diagnosis of tickborne encephalitis, African tick-bite fever, or other rickettsial infections.
• Tsetse flies are large, and their bites are painful and often recalled by the patient. They can carry Trypanosoma brucei, the protozoan that causes African sleeping sickness.

• Freshwater swimming or other water contact can put the patient at risk for schistosomiasis, leptospirosis, and other diseases.
• The purpose of the patient’s trip and the type of accommodations can also influence the risk for acquiring certain diseases.
• Travelers who visit friends and relatives are at higher risk of malaria, typhoid fever, and certain other diseases because, compared with tourists, they stay longer, travel to more remote destinations, have more contact with local water sources, and are less likely to seek pre-travel advice.
• Someone backpacking and camping in rural areas will also have a higher risk of certain diseases than those staying in air-conditioned hotels.

COMMON SYNDROMES• The most common clinical presentations after travel to developing
countries include systemic febrile illness, acute diarrhea, and dermatologic conditions.
• Respiratory complaints and eosinophilia are also conditions of importance in returning travelers.
• Fever in a traveler returning from a malaria-endemic country needs to be evaluated immediately.

Respiratory Complaints• Respiratory complaints are frequent among returned travelers and are typically associated
with common respiratory viruses.
• Influenza is among the most common vaccine-preventable diseases associated with international travel.
• Severe respiratory symptoms—especially associated with fever—in a returned traveler should alert the physician to common infectious diseases such as seasonal influenza, bacterial pneumonia, and malaria but could also suggest more unusual entities, such as Legionnaires’ disease.
• Emerging respiratory infections such as Middle East respiratory syndrome (MERS) and H7N9 avian influenza should be in the differential if the travel history is appropriate and respiratory symptoms do not have a clear alternative diagnosis. In these suspected cases, local public health authorities and CDC should be alerted immediately.

• Delayed onset and chronic cough after travel could be tuberculosis, especially in a long-term traveler or health care worker.
• Other uncommon infections causing respiratory illness after travel to specific regions are histoplasmosis, coccidioidomycosis, Q fever, plague, tularemia, and melioidosis.
• Helminth infections that produce pulmonary disease include strongyloidiasis, paragonimiasis, and schistosomiasis.

Eosinophilia• Eosinophilia in a returning traveler suggests a possible helminth infection. • Allergic diseases, hematologic disorders, and some viral, fungal, and protozoan infections can
also cause eosinophilia.
• Fever and eosinophilia can be present during pulmonary migration of parasites, such as hookworm, Ascaris, and Strongyloides.
• Acute schistosomiasis, or Katayama syndrome, is also a cause of fever and eosinophilia and can be associated with pulmonary infiltrates.
• Other parasitic infections associated with eosinophilia include chronic strongyloidiasis, visceral larval migrans, lymphatic filariasis, and acute trichinellosis.

MANAGEMENT• Most post-travel illnesses can be managed on an outpatient basis, but
some patients, especially those with systemic febrile illnesses, may need to be hospitalized.
• Severe presentations, such as acute respiratory distress, mental status change, and hemodynamic instability, require inpatient care.
• Clinicians should have a low threshold for admitting febrile patients if malaria is suspected. Confirmation of diagnosis can be delayed, and complications can occur rapidly.

• Management in an inpatient setting is especially important if the patient may not reliably follow up or when no one is at home to assist if symptoms worsen quickly.
• Consultation with an infectious disease physician is recommended in severe travel-related infections, when management is complicated, or when the diagnosis remains unclear.
• A travel medicine or infectious disease specialist should be involved in cases that require specialized treatment, such as neurocysticercosis, severe malaria, and leishmaniasis, among others.

Fever in Returned Travelers
INITIAL FOCUS• The initial focus in evaluating a febrile returned traveler
should be on identifying infections that are rapidly progressive, treatable, or transmissible.
• In some instances, public health officials must be alerted if the traveler may have been contagious while traveling or infected with a pathogen of public health importance (such as yellow fever) at the origin or destination.

USE OF HISTORY, LOCATION OF EXPOSURE, AND INCUBATION TO LIMIT DIFFERENTIAL DIAGNOSIS
• A large proportion of illnesses in returned travelers is caused by common, cosmopolitan infections (such as bacterial pneumonia or pyelonephritis), so these must be considered along with unusual infections.
• Because the geographic area of travel determines the relative likelihood of major causes of fever, it is essential to identify where the febrile patient has traveled and lived.

Common causes of fever, by geographic area
GEOGRAPHIC AREA COMMON TROPICAL DISEASE CAUSING FEVER OTHER INFECTIONS CAUSING OUTBREAKS OR CLUSTERS IN TRAVELERS
Caribbean Dengue, malaria (Haiti) Acute histoplasmosis, leptospirosis, chikungunya
Central America Dengue, malaria (primarily Plasmodium vivax) Leptospirosis, histoplasmosis, coccidioidomycosis
South America Dengue, malaria (primarily P. vivax) Bartonellosis, leptospirosis, enteric fever, histoplasmosis
South-central Asia Dengue, enteric fever, malaria (primarily non-falciparum) Chikungunya
Southeast Asia Dengue, malaria (primarily non-falciparum) Chikungunya, leptospirosis
Sub-Saharan AfricaMalaria (primarily P. falciparum), tickborne rickettsiae (main cause of fever in southern Africa), acute schistosomiasis, filariasis
African trypanosomiasis, chikungunya, enteric fever, filariasis

• Details about activities (such as freshwater exposure in schistosomiasis-endemic areas, animal bites, sexual activities, tattoos, or local medical care with injections) and accommodations in areas with malaria (bed nets, window screens, air conditioning) during travel may provide useful clues.
• Preparation before travel (such as hepatitis A vaccine or yellow fever vaccine) will markedly reduce the likelihood of some infections, so this is a relevant part of the history.
• A history of travel and residence should be an integral part of every medical history.

• Because each infection has a characteristic incubation period (although the range is extremely wide with some infections), the time of exposures needs to be defined in different geographic areas.
• This knowledge will allow the clinician to exclude some infections from the differential diagnosis.
• Most serious febrile infections manifest within the first month after return from tropical travel, yet infections related to travel exposures can occasionally occur months or even >1 year after return.
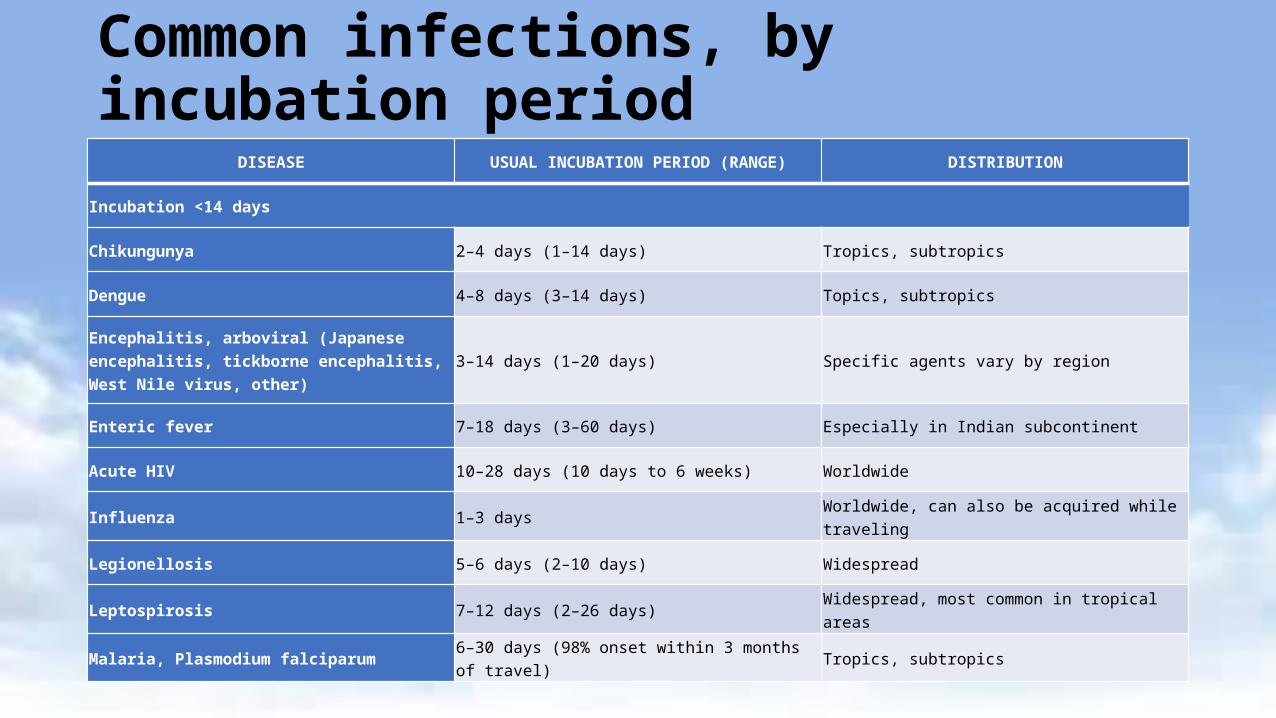
Common infections, by incubation period
DISEASE USUAL INCUBATION PERIOD (RANGE) DISTRIBUTION
Incubation <14 days
Chikungunya 2–4 days (1–14 days) Tropics, subtropics
Dengue 4–8 days (3–14 days) Topics, subtropics
Encephalitis, arboviral (Japanese encephalitis, tickborne encephalitis, West Nile virus, other) 3–14 days (1–20 days) Specific agents vary by region
Enteric fever 7–18 days (3–60 days) Especially in Indian subcontinent
Acute HIV 10–28 days (10 days to 6 weeks) Worldwide
Influenza 1–3 days Worldwide, can also be acquired while traveling
Legionellosis 5–6 days (2–10 days) Widespread
Leptospirosis 7–12 days (2–26 days) Widespread, most common in tropical areas
Malaria, Plasmodium falciparum 6–30 days (98% onset within 3 months of travel) Tropics, subtropics

Malaria, P. vivax 8 days to 12 months (almost half have onset >30 days after completion of travel) Widespread in tropics and subtropics
Spotted-fever rickettsiae Few days to 2–3 weeks Causative species vary by region
Incubation 14 Days to 6 Weeks
Encephalitis, arboviral; enteric fever; acute HIV; leptospirosis; malaria See above incubation periods for relevant diseases See above distribution for relevant diseases
Amebic liver abscess Weeks to months Most common in developing countries
Hepatitis A 28–30 days (15–50 days) Most common in developing countries
Hepatitis E 26–42 days (2–9 weeks) Widespread
Acute schistosomiasis (Katayama syndrome) 4–8 weeks Most common in sub-Saharan Africa
Incubation >6 weeks
Amebic liver abscess, hepatitis E, malaria, acute schistosomiasis See above incubation periods for relevant diseases See above distribution for relevant diseases
Hepatitis B 90 days (60–150 days) Widespread
Leishmaniasis, visceral 2–10 months (10 days to years) Asia, Africa, Latin America, southern Europe, and the Middle East
Tuberculosis Primary, weeks; reactivation, years Global distribution, rates and levels of resistance vary widely

FINDINGS REQUIRING URGENT ATTENTION• Presence of associated signs, symptoms, or laboratory findings can focus attention on
specific infections.
• Findings that should prompt urgent attention include hemorrhage, neurologic impairment, and acute respiratory distress.
• Even if an initial physical examination is unremarkable, it is worth repeating the examination, as new findings may appear that will help in the diagnostic process (such as skin lesions or tender liver).
• Although most febrile illnesses in returned travelers are related to infections, the clinician should bear in mind that other problems, including pulmonary emboli and drug hypersensitivity reactions, can be associated with fever.

Common clinical findings and associated infections
COMMON CLINICAL FINDINGS INFECTIONS TO CONSIDER AFTER TROPICAL TRAVEL
Fever and rash Dengue, chikungunya, rickettsial infections, enteric fever (skin lesions may be sparse or absent), acute HIV infection, measles
Fever and abdominal pain Enteric fever, amebic liver abscess
Undifferentiated fever and normal or low white blood cell count Dengue, malaria, rickettsial infection, enteric fever, chikungunya
Fever and hemorrhage Viral hemorrhagic fevers (dengue and others), meningococcemia, leptospirosis, rickettsial infections
Fever and eosinophilia Acute schistosomiasis, drug hypersensitivity reaction, fascioliasis and other parasitic infections (rare)
Fever and pulmonary infiltrates Common bacterial and viral pathogens, legionellosis, acute schistosomiasis, Q fever, leptospirosis
Fever and altered mental status Cerebral malaria, viral or bacterial meningoencephalitis, African trypanosomiasis, scrub typhus
Mononucleosis syndrome Epstein–Barr virus infection, cytomegalovirus infection, toxoplasmosis, acute HIV
Fever persisting >2 weeksMalaria, enteric fever, Epstein-Barr virus infection, cytomegalovirus infection, toxoplasmosis, acute HIV, acute schistosomiasis, brucellosis, tuberculosis, Q fever, visceral leishmaniasis (rare)
Fever with onset >6 weeks after travel Plasmodium vivax or ovale malaria, acute hepatitis (B, C, or E), tuberculosis, amebic liver abscess
Bruising or unusual bleeding (without previous injury)Persistent diarrheaPersistent vomiting (other than air or motion sickness)JaundiceParalysis of recent onset
• Fever accompanied by any of the following syndromes deserves further scrutiny, because it may indicate a disease of public health importance:
Skin rash Difficulty breathing Shortness of breath Persistent cough Decreased consciousness
• People who travel to visit friends and relatives (VFRs) often do not seek pre-travel medical advice and are at higher risk for some diseases than other travelers.
• A review of GeoSentinel Surveillance Network data showed that a larger proportion of immigrant VFRs than tourist travelers presented with serious (requiring hospitalization), potentially preventable travel-related illnesses.

CHANGE OVER TIME• Clinicians have access to resources on the Internet that provide information about
geographic specific risks, disease activity, and other useful information, such as drug-susceptibility patterns for pathogens.
• Infectious diseases are dynamic.
• Common infections in returned travelers may be seen at unexpected times of the year.
• Travelers may acquire infections caused by common bacteria that are unusually resistant.
• In most studies, a specific cause for fever is not identified in about 25% of returned travelers.

KEEP IN MIND• Initial symptoms of life-threatening and self-limited infections can be
identical.
• Fever in returned travelers is often caused by common, cosmopolitan infections, such as pneumonia and pyelonephritis, which should not be overlooked in the search for more exotic diagnoses.
• Patients with malaria may be afebrile at the time of evaluation but typically give a history of fever or chills.
• Malaria is the most common cause of acute undifferentiated fever after travel to sub-Saharan Africa and to some other tropical areas.

• Malaria, especially P. falciparum, can progress rapidly. Diagnostic studies should be done promptly and treatment instituted immediately if malaria is diagnosed.
• A history of taking malaria chemoprophylaxis does not exclude the possibility of malaria.
• Patients with malaria can have prominent respiratory (including acute respiratory distress syndrome), gastrointestinal, or central nervous system findings.
• Dengue is the most common cause of febrile illness among people who seek medical care after travel to Latin America or Asia.
• Viral hemorrhagic fevers are important to identify but are rare in travelers; bacterial infections, such as leptospirosis, meningococcemia, and rickettsial infections, can also cause fever and hemorrhage and should be always be considered because of the need to institute prompt, specific treatment.
• Sexually transmitted diseases, including acute HIV, can cause acute febrile infections.
• Consider infection control, public health implications, and requirements for reportable diseases.

Persistent Travelers’ Diarrhea

• Although most cases of travelers’ diarrhea are acute and self-limited, a certain percentage of travelers will develop persistent (>14 days) gastrointestinal symptoms.
• The pathogenesis of persistent travelers’ diarrhea generally falls into one of the following broad categories:
Persistent infection or coinfection with a second organism not targeted by initial therapy.
Previously undiagnosed gastrointestinal disease unmasked by the enteric infection.
A postinfectious phenomenon.

PERSISTENT INFECTION• Most cases of travelers’ diarrhea are the result of bacterial infection
and are short-lived and self limited. Travelers may experience prolonged diarrheal symptoms if they are immunosuppressed, are infected sequentially with diarrheal pathogens, or are infected with protozoan parasites.
• Giardia is by far the most likely persistent pathogen to be encountered.
• Suspicion for giardiasis should be particularly high when upper gastrointestinal symptoms predominate.

• Untreated, symptoms may last for months, even in immunocompetent hosts.
• The diagnosis can often be made through stool microscopy, antigen detection, or immunofluorescence.
• However, as Giardia infects the proximal small bowel, even multiple stool specimens may fail to detect it, and a duodenal aspirate may be necessary for definitive diagnosis.
• Given the high prevalence of Giardia in persistent travelers’ diarrhea, empiric therapy is a reasonable option in the clinical setting after negative stool microscopy and in lieu of duodenal sampling.

• Other intestinal parasites that may cause persistent symptoms include Cryptosporidium species, Entamoeba histolytica, Isospora belli, Microsporidia, Dientamoeba fragilis, and Cyclospora cayetanensis.
• Individual bacterial infections rarely cause persistence of symptoms, although persistent diarrhea has been reported in children infected with enteroaggregative or enteropathogenic Escherichia coli and among people with diarrhea due to Clostridium difficile.

• C. difficile–associated diarrhea may follow treatment of a bacterial pathogen with a fluoroquinolone or other antibiotic, or may even follow malaria chemoprophylaxis.
• This is especially important to consider in the patient with persistent travelers’ diarrhea that seems refractory to multiple courses of empiric antibiotic therapy.
• The initial work-up of persistent travelers’ diarrhea should always include a C. difficile stool toxin assay.
• Treatment of C. difficile infection is with metronidazole, oral vancomycin, or fidaxomicin, although increasing reports of resistance to the first 2 drugs have been noted.

• Persistent travelers’ diarrhea has also been associated with tropical sprue and Brainerd diarrhea.
• These syndromes are suspected to result from infectious diseases, but specific pathogens have not been identified.
• Tropical sprue is associated with deficiencies of vitamins absorbed in the proximal and distal small bowel and most commonly affects long-term travelers to tropical areas.
• Investigation of an outbreak of Brainerd diarrhea among passengers on a cruise ship to the Galápagos Islands of Ecuador revealed that diarrhea persisted from 7 to more than 42 months and did not respond to antimicrobial therapy.
UNDERLYING GASTROINTESTINAL DISEASE• In some cases, persistence of gastrointestinal symptoms relates to
chronic underlying gastrointestinal disease or susceptibility unmasked by the enteric infection. Most prominent among these is celiac disease.
• Idiopathic inflammatory bowel disease, both Crohn disease and ulcerative colitis, may be seen after acute bouts of travelers’ diarrhea.
• Colorectal cancer should be considered, particularly in patients
passing occult or gross blood rectally or with the onset of a new iron-deficiency anemia.
POSTINFECTIOUS PHENOMENA• In a certain percentage of patients who present with persistent
gastrointestinal symptoms, no specific source will be found.
• Patients may experience temporary enteropathy following an acute diarrheal infection, with villous atrophy, decreased absorptive surface area, and disaccharidase deficiencies.
• This can lead to osmotic diarrhea, particularly when large amounts of lactose, sucrose, sorbitol, or fructose are consumed.
• Use of antimicrobial medications during the initial days of diarrhea may also lead to alterations in intestinal flora and diarrhea symptoms.

• Occasionally, the onset of symptoms of irritable bowel syndrome (IBS) can be traced to an acute bout of gastroenteritis.
• IBS that develops after acute enteritis has been termed postinfectious
(PI)-IBS.
• To be labeled PI-IBS, symptoms should follow an episode of gastroenteritis or travelers’ diarrhea if the work-up for microbial pathogens and underlying gastrointestinal disease is negative.

EVALUATION• Three or more stool examinations should be performed for ova and
parasites, including acid-fast stains for Cryptosporidium, Cyclospora, and Isospora; Giardia antigen testing; C. difficile toxin assay; and a D-xylose absorption test to determine if nutrients are being properly absorbed.
• Patients may also be given empiric treatment for Giardia infection. • If underlying gastrointestinal disease is suspected, an initial evaluation
should include serologic tests for celiac and inflammatory bowel disease. Subsequently, other studies to visualize both the upper and lower gastrointestinal tracts, with biopsies, may be indicated.
MANAGEMENT• Dietary modifications may help those with malabsorption.
• If stools are bloody or when disease is caused by C. difficile, antidiarrheal medications such as loperamide or diphenoxylate should not be used in children and should be used cautiously, if at all, in adults.
• Probiotic medications have been shown to reduce the duration of persistent diarrhea among children in some settings.
• Antimicrobial medications may be useful in treating persistent diarrhea caused by parasites.
• Nonabsorbable antibiotics may help if small intestinal bacterial overgrowth accompanies the symptom complex.

Skin & Soft Tissue Infections in Returned Travelers

• Skin problems are among the most frequent medical problems in returned travelers.
• The largest case series of dermatologic problems in returned travelers from the GeoSentinel Surveillance Network showed that cutaneous larva migrans, insect bites, and bacterial infections were the most frequent skin problems in ill travelers who sought medical care, making up 30% of the 4,742 diagnoses.

Skin lesions in returned travelers, by cause
SKIN LESION PERCENTAGE OF ALL DERMATOLOGIC DIAGNOSES (N = 4,742)
Cutaneous larvae migrans 9.8
Insect bite 8.2
Skin abscess 7.7
Superinfected insect bite 6.8
Allergic rash 5.5
Rash, unknown origin 5.5
Dog bite 4.3
Superficial fungal infection 4.0
Dengue 3.4
Leishmaniasis 3.3
Myiasis 2.7
Spotted-fever group rickettsiae 1.5
Scabies 1.5
Cellulitis 1.5
• Skin problems generally fall into either of the following categories:
Those associated with fever, usually a rash or secondary bacterial infection (cellulitis, lymphangitis, bacteremia, toxin mediated).
Those not associated with fever.
•Most skin problems are minor and are not accompanied by fever.
• Diagnosis of skin problems in returned travelers is based on the following:
Pattern recognition of the lesions: papular, macular, nodular, linear, or ulcerative
Location of the lesions: exposed versus unexposed skin surfacesExposure history: freshwater, ocean, insects, animals, or human
contactAssociated symptoms: fever, pain, pruritus
• It is important to recognize that skin conditions in returned travelers may not have a travel related cause.

PAPULAR LESIONS• Insect bites, the most common cause of papular lesions, may
be associated with secondary infection or hypersensitivity reactions.
• Onchocerciasis may occur in long-stay travelers living in rural sub-Saharan Africa and, rarely, Latin America. It usually manifests as a generalized pruritic, papular dermatitis.

NODULAR OR SUBCUTANEOUS LESIONS, INCLUDING BACTERIALSKIN INFECTIONS• Bacterial skin infections may occur more frequently after
bites and other wounds in the tropics, particularly when good hygiene cannot be maintained. Organisms responsible are commonly Staphylococcus aureus or Streptococcus pyogenes.
•Myiasis presents as a painful lesion similar to a boil. It is caused by infestation with the larval stage of the African tumbu fly (Cordylobia anthropophaga) or the Latin American bot fly (Dermatobia hominis).

• Tungiasis is caused by a sand flea (Tunga penetrans).
• Loa loa filariasis occurs rarely in long-term travelers living in rural sub-Saharan Africa.
• Gnathostomiasis is a nematode infection found primarily in Southeast Asia and less commonly in Africa and Latin America. Infection results from eating undercooked or raw freshwater fish.

MACULAR LESIONS• Macular lesions are common and often nonspecific and may be due to
drug reactions or viral exanthems. Superficial mycoses, such as tinea versicolor and tinea corporis, may also present as macular lesions.
• Tinea versicolor, due to Malassezia furfur (previously Pityrosporumovale).
• Tinea corporis (ringworm) may be caused by a number of different superficial fungi.
• Lyme disease, a tickborne infection with Borrelia burgdorferi, is common in North America, Europe, and Russia.

LINEAR LESIONS• Cutaneous larva migrans, a skin infection with the larval
stage of dog or cat hookworm (Ancylostoma braziliense).
• Larva currens (running larva) due to cutaneous migration of filariform larvae of Strongyloides stercoralis.

• Lymphocutaneous spread of infection occurs when organisms spread along superficial cutaneous lymphatics. Examples include sporotrichosis, Mycobacterium marinum infection (associated with exposure to water), leishmaniasis, bartonellosis (cat-scratch disease), Nocardia infection, tularemia, melioidosis, and blastomycosis.
• Phytophotodermatitis is a noninfectious condition that results from interaction of natural psoralens, most commonly from spilled lime juice, and ultraviolet radiation from the sun.

SKIN ULCERS• Ulcerated skin lesions may result from Staphylococcus infections or may
be the direct result of an unseen spider bite.
• The necrotic ulcer of anthrax is often surrounded by edema and usually results from handling animal hides or products.
• Rarely, a painless destructive ulcer with undermining edges may result from infection with Mycobacterium ulcerans (Buruli ulcer).
• Of particular concern is the ulcer (or less commonly, nodule) caused by cutaneous leishmaniasis.

MISCELLANEOUS SKIN INFECTIONS• Skin Infections Associated with WaterM. marinum, Aeromonas spp., Plesiomonas spp., Edwardsiella tarda, Erysipelothrix rhusiopathiae, Vibrio vulnificus, and Pseudomonas aeruginosa
• Skin Infections Associated with BitesS. aureus; α-, β-, and γ-hemolytic streptococci; several genera of gram-negative organisms; and a number of anaerobic microorganisms; Pasteurella multocida, and Capnocytophaga canimorsus

FEVER AND RASH• Fever and rash in returned travelers are most often due to a viral infection.
• Dengue is caused by 1 of 4 strains of dengue viruses. The disease is transmitted by a primarily day-biting Aedes mosquito often found in urban areas, and its incidence continues to increase.
• Chikungunya, a virus transmitted by a primarily day-biting Aedes mosquito, has recently caused major outbreaks of illness in southeast Africa, South Asia, the Americas, and the Caribbean.
• South African tick typhus, or African tick-bite fever (Rickettsia africae), is the most frequent cause of fever and rash in southern Africa. Transmitted by ticks.

• Rocky Mountain spotted fever (RMSF), although uncommon in travelers, is an important cause of fever and rash because of its potential severity and the need for early treatment. This tickborne infection is found in the United States, Mexico, and parts of Central and South America.
• The category of fever with rash is large, and providers caring for ill travelers should also consider the following diagnoses: enteroviruses, such as echovirus and coxsackievirus; hepatitis B virus; measles; Epstein-Barr virus; cytomegalovirus; typhus; leptospirosis; syphilis; and HIV.

Screening Asymptomatic Returned Travelers

• CDC has no official guidelines or recommendations for screening asymptomatic international travelers.
• Recommendations for screening the asymptomatic traveler are necessarily based on opinion and common sense, rather than convincing evidence.

• The following may serve as a general guideline:
For the asymptomatic short stay (<3–6 months) traveler, the yield of screening is low and should be directed by specific risk factors revealed in the history.
A history of prolonged (>2 weeks) digestive symptoms during travel can suggest protozoal infection.
Exposure to fresh water in a region endemic for schistosomiasis, especially in Africa, merits serologic screening, with the addition of stool and urine examination in the case of high-intensity exposure.

Serology for Strongyloides should be considered in those who have a high risk of skin exposure to soil likely to be contaminated with human feces, usually those with a history of frequently walking barefoot outdoors.
A sexual history should be obtained. Work in a health care setting or other area at high risk for TB may merit screening.
For longer-stay travelers, as the overall yield of screening increases it becomes less useful to rely on history for selective testing.
The emphasis should be on those with the longest stays and the most problematic sanitary conditions.
In some cases, employers may require certain tests, partly for reasons
of liability. Stool examinations are usually done, although they serve mostly to
provide a psychological reassurance. Serologic testing for schistosomiasis and strongyloidiasis should be
done in those reporting some level of risk.

Eosinophil counts are usually done, although results should be interpreted cautiously. Screening for sexually transmitted infections should be offered to all except those with the most convincing absence of risk.
Mantoux or interferon-γ release assay (IGRA) tests should be limited to those who have worked in a health care or similar setting, orwho have had intimate and prolonged contact with residents of an endemic area for ≥ 6 months.
Possible exposure to bloodborne pathogens should be assessed. Any other screening should be guided by exceptional exposures or knowledge about local outbreaks.
