treating chronic non-cancer pain in older people – more questions than answers?
TRANSCRIPT

R
Tt
Ha
b
a
ARA
KPCNEO
C
7
h0
Maturitas 79 (2014) 34–40
Contents lists available at ScienceDirect
Maturitas
jou rn al hom ep age: www.elsev ier .com/ locate /matur i tas
eview
reating chronic non-cancer pain in older people – More questionshan answers?
elen Gaskell a, Sheena Derryb, R Andrew Mooreb,∗
Department of Clinical Geratology, Oxford University Hospitals NHS Trust, John Radcliffe Hospital, Oxford, UKPain Research and Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, UK
r t i c l e i n f o
rticle history:eceived 16 June 2014ccepted 21 June 2014
eywords:ainhronicon-cancervidencelder person
a b s t r a c t
There is little evidence specifically relating to drug treatments for pain in older people, but much can beextrapolated from what we already know. The evidence about drug treatments for chronic non-cancerpain is changing, driven by major improvements in understanding of clinical trial analysis and by theadoption of patient-centered outcomes of proven economic benefit. There is clear evidence of lack of use-ful effect, or insufficient evidence of effect for a number of commonly used drugs, including paracetamol,topical rubefacients, low concentration topical capsaicin, and for strong opioids in chronic non-cancerpain. In musculoskeletal pain there is evidence of efficacy for NSAIDs, tramadol, and tapentadol, and inneuropathic pain for duloxetine, pregabalin, and gabapentin, with weak evidence for amitriptyline. Thenew perspective is of drugs that work well in a minority of patients, but hardly at all in the remainder.The goal of treatment is large reductions in pain, by 50% or more. This outcome, and only this outcome,
is associated with large benefits in terms of improved sleep, reduced depression, and large gains in func-tion and quality of life. It is not possible to predict which patient will benefit from which drug, but earlysuccess or failure appears to be predictive of long-term success or failure. The emphasis is on stoppingtreatments that do not work and switching to other drugs in the same or different class, so that anypotential future risk of treatment is balanced by very large and immediate benefit.© 2014 Elsevier Ireland Ltd. All rights reserved.
ontents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 351.1. What is CNCP and why is it important? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 351.2. Evidence on CNCP in older people? Can we extrapolate evidence from younger patients? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 351.3. There are significant developments in understanding data from clinical trials in treating CNCP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 351.4. Why are these developments important? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 361.5. What are the benefits and risks of medications used to treat CNMP in older people? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
1.5.1. Paracetamol (acetaminophen) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 371.5.2. NSAIDs (excluding paracetamol) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 371.5.3. Opioids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 371.5.4. Other medications. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
1.6. Questions and some answers for the patient/family/career/health professional/funder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
1.6.1. How can we treat CNCP effectively? . . . . . . . . . . . . . . . . . . . . . .1.6.2. How can we reduce risk of harm? . . . . . . . . . . . . . . . . . . . . . . . .1.6.3. How can we avoid unnecessary cost? . . . . . . . . . . . . . . . . . . . .∗ Corresponding author at: Pain Research and Nuffield Division of Anaesthetics, NuffieldLE, UK. Tel.: +44 1865 225674.
E-mail address: [email protected] (R.A. Moore).
ttp://dx.doi.org/10.1016/j.maturitas.2014.06.013378-5122/© 2014 Elsevier Ireland Ltd. All rights reserved.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
Department of Clinical Neurology, University of Oxford, The Churchill, Oxford OX3
H. Gaskell et al. / Maturitas 79 (2014) 34–40 35
2. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Contributors role . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Competing interests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Provenance and peer review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Acknowledgement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
. . . . . .
1
1
mtmsp
dtwiptAcn
tilsapaMry
pCcapdt
toepppt
1e
plm
w
from clinical trials in treating CNCP
Several recent insights show that much of the existing clinicaltrial evidence on CNCP may be unreliable as a guide to treatment.
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. Introduction
.1. What is CNCP and why is it important?
Chronic non-cancer pain (CNCP) is pain that is not caused byalignant disease and persists over a period of time. Although
here is no widely accepted definition of minimum duration, threeonths is often arbitrarily used to differentiate between acute or
ubacute pain (intermittent migraine, for example), and chronicain.
In older people CNCP is often associated with musculoskeletalisease, or conditions affecting the somatosensory nervous sys-em (neuropathic pain). In addition, pain in itself can be associatedith depression, impaired function in activities of daily living, and
ncreased mortality. Unfortunately it is a common problem foratients, their families/carers, health professionals and of coursehere are implications for delivery and cost of health care services.ssessment and treatment of pain in patients who cannot readilyommunicate (e.g. in dementia) are very important issues but willot be explored in this paper.
CNCP can be continuous; while it often varies in intensity overime, it is characterised by pain that is typically moderate or severen intensity over many years. Systematic reviews of CNCP preva-ence agree that chronic pain (usually defined conservatively intudies as moderate or severe pain lasting six months or more)ffects about 1 adult in 5 [1,2]. This is mostly musculoskeletalain (especially osteoarthritis), that increases with age [3], thoughtbout a third of older people with CNCP have neuropathic pain [1].ost people (66%) with CNCP have it for five years or longer: it
arely goes away spontaneously [4]. Over half of people aged 65ears or older in a study in the USA had bothersome pain [5].
The detrimental impact of CNCP on a whole range of associatedroblems, including quality of life and function, is immense [1].NCP has a greater negative impact on quality of life than any otherhronic condition for people living in the community [6]. There islso growing evidence that CNCP can affect the quantity of life [1],articularly in those with the most severe pain [7], or with walkingisability [8]; cardiovascular or respiratory death contribute mosto excess mortality.
This review concentrates on new thinking on drug therapy. Herehere is at least some evidence, but for intervention managementr complementary therapies, evidence is notable by its absence. Forxample, a broad review of interventional therapies for neuropathicain could make, at best, four very weak recommendations thatarticular treatments might work [9]. For complementary thera-ies and devices, there are many problems with the evidence, asypified by acupuncture [10].
.2. Evidence on CNCP in older people? Can we extrapolatevidence from younger patients?
There is clear evidence that CNCP is more prevalent in olderopulations, driven largely by osteoarthritis and other muscu-
oskeletal conditions [3]. Other surveys suggest that prevalenceay decline somewhat with age [4].As is often the case with conditions affecting patients with a
ide age range, there is little evidence on CNCP specifically in
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
older people, and much of the available data come from observa-tional studies. Reasons for the lack of inclusion of older patients inclinical trials in general have been discussed elsewhere; in CNCP,many trials recruit patients from specialist clinics in secondary careattended by relatively few older people. As a result, clinical tri-als in CNCP, particularly in osteoarthritis, often have a majority ofpatients of late middle age and some older patients but tend not toinclude many of the “oldest-old”.
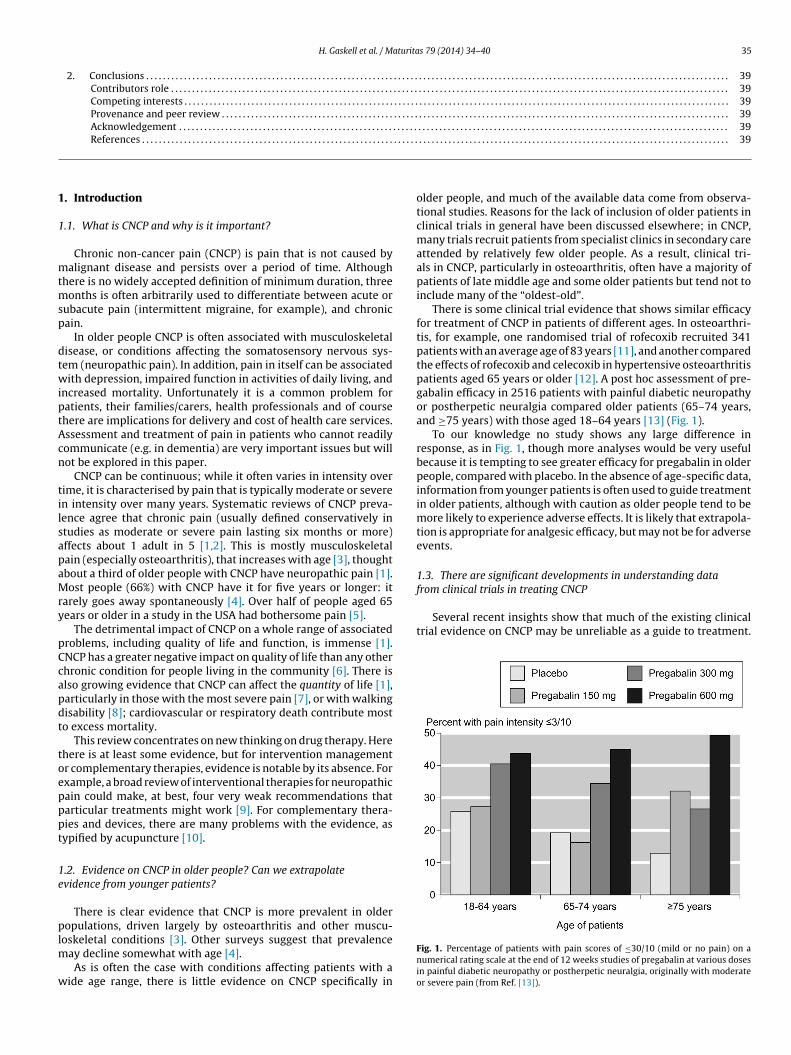
There is some clinical trial evidence that shows similar efficacyfor treatment of CNCP in patients of different ages. In osteoarthri-tis, for example, one randomised trial of rofecoxib recruited 341patients with an average age of 83 years [11], and another comparedthe effects of rofecoxib and celecoxib in hypertensive osteoarthritispatients aged 65 years or older [12]. A post hoc assessment of pre-gabalin efficacy in 2516 patients with painful diabetic neuropathyor postherpetic neuralgia compared older patients (65–74 years,and ≥75 years) with those aged 18–64 years [13] (Fig. 1).
To our knowledge no study shows any large difference inresponse, as in Fig. 1, though more analyses would be very usefulbecause it is tempting to see greater efficacy for pregabalin in olderpeople, compared with placebo. In the absence of age-specific data,information from younger patients is often used to guide treatmentin older patients, although with caution as older people tend to bemore likely to experience adverse effects. It is likely that extrapola-tion is appropriate for analgesic efficacy, but may not be for adverseevents.
1.3. There are significant developments in understanding data
Fig. 1. Percentage of patients with pain scores of ≤30/10 (mild or no pain) on anumerical rating scale at the end of 12 weeks studies of pregabalin at various dosesin painful diabetic neuropathy or postherpetic neuralgia, originally with moderateor severe pain (from Ref. [13]).

3 aturita
Noti
mwirronf
(
(
(
(
fessionals but unfortunately there is now concern about some med-ications previously thought to be good choices for older patients.
Box 1 provides information about drug treatments with evi-dence of lack of effect, no evidence of effect, or inadequate evidence
Box 1Drugs with evidence of lack of effectMusculoskeletal conditionsParacetamol for osteoarthritisStrong opioids for osteoarthritis and back painNeuropathic painLamotrigineOxcarbazepineTopiramateDrugs with no evidence or inadequate evidence of effectMusculoskeletal conditionsRubefacients for osteoarthritisLow concentration topical capsaicinNeuropathic painClenazepamPhenytoinVarproic acidCarbamazepineLacosamideLevetiracetam
6 H. Gaskell et al. / M
on-specialists may not be interested in details of CNCP trial design,r the methods of analysis and reporting of trial data. Because ofheir implications it is useful to highlight some significant changesn thinking in this field [14–18].
Pain is a subjective phenomenon and pain intensity cannot beeasured directly in the way that, say, one measures height oreight. In clinical practice and clinical trials, patients indicate the
ntensity of the pain they are experiencing by using a (validated)ating scale. Typically, results of clinical trials of pain treatments areeported as the mean (and standard deviation) of patients’ scoresn pain intensity rating scales at baseline and on treatment. But weow know that presenting data in this way gives a limited picture,
or the following reasons.
1) What patients want from CNCP treatmentTo misquote the English novelist Jane Austen, it might seem
to be a truth universally acknowledged, that a man (or woman)in pain must be in want of effective pain relief. What mattersto patients is 30% (or better, 50%) reduction in pain, or to expe-rience no worse than mild pain [14]. It may come as a surpriseto non-specialist readers that information in this form has onlyrecently begun to be reported in this way in clinical trials inpain treatment.
2) Heterogeneity in response to treatment for CNCPIt has become apparent that response to pain treatment varies
considerably from patient to patient. There are “responders”who gain good pain relief from a particular treatment, and“non-responders” who have little or no pain relief with thesame treatment, but relatively few who have an intermediateresponse. This phenomenon is seen with all different classes ofmedications and all types of CNCP (and also in acute pain andheadache). We learn little about this characteristic of responseto pain treatment when clinical trial results are reported usingmean values of pain intensity or pain relief, although wide dis-persion (large standard deviations) may suggest this.
3) Good response for pain means good response across the boardUnderstandably, patients also value the major improvement
in sleep, function, depression, and quality of life that occur whenCNCP is treated effectively. There is now a large literature thatdemonstrates that pain intensity reduction by 50% or more, ora final pain state of ≤30% of the maximum on any scale (forinstance, ≤3/10 on numerical rating scale, ≤30/100 on visualanalogue scale, mild or no pain on a categorical scale) equatingto no worse than mild pain is not only what patients want, butis also an outcome that delivers cost savings and quality of lifeimprovement [14].
4) Hidden complexities and pitfalls on trial analysisAnd these are not the only problems with interpretation of
data from clinical trials of treatment of CNCP. Typically, fewerthan half of patients will complete a study lasting 12 weeks,though it can be only a third with opioids. How to deal withmissing data when patients drop out of trials is a difficult prob-lem, and choice of data analysis technique may significantlyaffect the results obtained [17].
One technique commonly used in analysis of clinical trial datawhen patients do not complete a trial is “last observation car-ried forward” (LOCF). Using LOCF, when a patient drops out of atrial, the last recorded value of the outcome measure of interest(say, pain intensity) is used at all subsequent planned assess-ment times for that patient. With opioids, withdrawal is usuallywithin the first weeks of a 12-week trial, usually because ofadverse events; LOCF takes any analgesic effect at (say) 2 weeks,
and pretends it is present at 12 weeks. By contrast, in the“baseline-observation-carried-forward” (BOCF) technique thepain score at baseline is used to substitute for missing datafor that patient throughout the rest of the trial. The patient iss 79 (2014) 34–40
classified as a “non-responder” because there can be no painrelief if you do not take the tablets. Most clinical trials in CNCPuse the LOCF technique. Analysing such trial data using theBOCF technique can yield significantly different results [17].LOCF significantly overestimates drug efficacy where adverseevent withdrawals are high. For opioids in chronic muscu-loskeletal pain, the overestimation appears to be substantial forstrong opioids; LOCF says the drug works, while BOCF, which ismuch more relevant to clinical practice, says that it is unlikelyto be better than placebo.
1.4. Why are these developments important?
There are very few reports of clinical trials in treatment of CNCPin which the data are presented using the innovations describedabove. Interpretation of the results of older trials is uncertain. Thismeans that we now have limited high quality evidence from clin-ical trials in treatment of CNCP. Exceptions are duloxetine, whichhas been re-analysed using BOCF imputations and clinically usefulendpoints [18], pregabalin in fibromyalgia [19] and painful dia-betic neuropathy and postherpetic neuralgia combined [13], andsome NSAIDs in osteoarthritis [20], chronic low back pain [21], andankylosing spondylitis [22].
The key finding is that for any one drug some patients are likelyto respond well, and with attendant benefits in a range of othersymptoms and increases in quality of life and function, but only aminority will have that experience. Failure is the norm [23]. Duringclinical trials, it is usually apparent early – within one or two weeks– whether a drug is going to be a success for a particular patient.The best predictor of long-term benefit is short-term success [24].
1.5. What are the benefits and risks of medications used to treatCNMP in older people?
Medication to treat CNCP can be divided into several groups –paracetamol (acetaminophen), NSAIDs, opioids, and others includ-ing antidepressants and antiepileptic drugs. Many of the potentialhazards of these medications should be well known to health pro-
Low concentration topical capsaicinNortriptyline, desipramine, imipramine, and other TCAsVenlafaxineStrong opioids, oxycodone
aturita
os
dptaom
1
Hoppccsooci
pedbso
wio
dtaaob
1
wN
tpbirrouucaHlv
poc
H. Gaskell et al. / M
f effect. The evidence is derived mostly from Cochrane reviews,upplemented by individual patient data analyses.
Table 1 gives the number needed to treat (NNT) for a range ofrugs compared with placebo, using the outcome of at least 50%ain intensity reduction at trial end, usually about 12 weeks. Inhese analyses the ideal outcome is the BOCF outcome of pain reliefnd ability to keep taking the tablets (that is, not withdrawn). Somef these analyses do use LOCF, which is not ideal, but is unlikely toake a major difference in any of these analyses.
.5.1. Paracetamol (acetaminophen)Paracetamol is often suggested as a first-line treatment for CNCP.
owever, even when clinical trial evidence is considered in termsf previous, less stringent criteria, paracetamol is found to haveoor efficacy. In a Cochrane review, treatment of osteoarthritis witharacetamol was found to be associated with a statistically signifi-ant reduction in pain. But the effect was small and “of questionablelinical significance”, even though the doses used in many of thetudies were relatively high (4 g/day)[25]. This analysis includedne study of one week’s duration with a large effect size, and 97%f patients were in studies lasting 6 weeks or less. There is noonvincing evidence that paracetamol is any better than placebon osteoarthritis.
There have also been concerns about potential safety issues witharacetamol, including gastrointestinal and cardiovascular adverseffects. It might be argued that such problems are not necessarilyue to the medication itself, but reflect the fact that paracetamol haseen seen as a safer option in frail patients However, trial evidenceuggests otherwise [26]. Since paracetamol is in fact a weak NSAIDne might expect it to have adverse effects typical of this drug class.
In the USA, the US Food and Drug Administration has issuedarnings about the risk of inadvertent overdose when paracetamol
s taken either as a stand-alone formulation or in combination withther medication(s) [27].
In 2013 draft UK guidelines on the treatment of osteoarthritisid not recommend the use of paracetamol for osteoarthritis, buthe updated [28] guidelines stepped back from this advice, pending
review of medications available over-the-counter. Paracetamol is recommended first line treatment of acute and persistent pain inlder adults in some guidelines [29]; it is hard to see how this cane justified on efficacy or safety grounds.
.5.2. NSAIDs (excluding paracetamol)The efficacy of oral NSAIDs for chronic musculoskeletal pain is
ell established and supported in meta-analyses [20–22]. TopicalSAIDs offer benefits to some people with osteoarthritis [30].
The adverse effects are also well known, and include gas-rointestinal bleeding, heart and renal failure, and cardiovascularroblems. Much attention has been paid to cardiovascular issues,est described in a large meta-analysis [31]. There were small
ncreases in event rates in the overall analysis, and a subsequenteanalysis by patient age showed no evidence for a greater relativeisk of major vascular events with older age for coxibs, naproxen, orther traditional NSAIDs, and no trend was noted for symptomaticpper gastrointestinal events [32]. Large longitudinal studies of these of NSAIDs frequently do not find any increase in cardiovas-ular adverse events, but rather find reductions in them, and inll-cause mortality, sometimes in a dose dependent manner [33].arm from NSAID use is perhaps more subtle than we have been
ed to believe, but topical NSAIDs are much safer by virtue of theirery low systemic plasma concentrations.
In the light of more recent evidence on other analgesicsreviously thought to be safer, perhaps NSAID prescription forlder patients should be re-considered, at least for individualases. Whether or not the patient judges the predicted risks to be
s 79 (2014) 34–40 37
acceptable in return for relief of their symptoms should be a majorconsideration when prescribing an NSAID regimen.
1.5.3. OpioidsOpioids are arbitrarily classed as weak or strong depending
on their potency. Their prescribed use varies between countriesdepending on local regulation, particularly where strong opioidsare concerned. Addiction, abuse and diversion are of course majorconcerns with opioids, but are beyond the scope of this paper. Weconcentrate on developments in evidence on the therapeutic use ofopioids for CNCP. Opioid prescribing, and particularly prescribingof strong opioids, is rising [34–36].
Using the recent more stringent standards for interpreting clin-ical trial evidence, only tramadol is shown to have better efficacythan placebo for treating CNCP, both for osteoarthritis [37] andfor neuropathic pain [38]. There is little or no good quality evi-dence that strong opioids are effective in CNCP, and the evidencewe have is unconvincing for opioids generally [39] and specificallyfor oxycodone [40]. Tapentadol is probably an exception [41].
Codeine, alone or in combination with other medication, is com-monly used for CNCP although there are potential risks in patientswith impaired renal function. It is an interesting example where (atleast some of) the reasons are known explaining why there can bevariability in responses of individuals to a particular medication.Codeine is metabolised to morphine. About 10% of the Caucasianpopulation are “slow-metabolizers”; they typically gain little or nobenefit from codeine, and so are likely to be “non-responders” ina clinical trial of codeine. In the same population 2% are “ultra-metabolizers”, but in middle-eastern and Asian populations asmany as 20% or more can be ultra-metabolizers. The consequencesof codeine use in ultra-metabolizers can be very serious.
We do know that in older people (mean age 80 years) opioidscause much greater harm in terms of cardiovascular outcomes, frac-tures, hospital admission and all-cause mortality than traditionalNSAIDs and cyclooxygenase inhibitors [42]. All of which makes opi-oids perhaps the last rather than necessarily the first drugs to turnto.
1.5.4. Other medicationsAntiepileptic and antidepressant drugs are used to treat neuro-
pathic pain, often with some success. Fibromyalgia can sometimesrespond well to these drugs too. Fortunately we now have a numberof Cochrane reviews and overviews to help. The current picture isthat four drugs – amitriptyline, duloxetine, gabapentin, and prega-balin are effective in neuropathic pain [23,43,44]. Any might work,and current guidance is coalescing around trying each in turn untilsuccess if achieved. As with any CNS drug, CNS adverse events arelikely, especially in older people. These may include dizziness, falls,somnolence, confusion, gastro-intestinal and other symptoms.
Perhaps the one other treatment with evidence of efficacy is highconcentration topical capsaicin for some with postherpetic neural-gia [45]; low concentration topical capsaicin is probably ineffective[46].
1.6. Questions and some answers for thepatient/family/career/health professional/funder
1.6.1. How can we treat CNCP effectively?It is disconcerting to find that the validity of much of the evi-
dence that has guided CNCP treatment is now being questioned. Atthe very least, this offers an opportunity to stop using treatmentsthat raise false hope of pain relief but don’t work, leaving patients
in pain (and with associated negative effects such as poor quality oflife), families and carers distressed, health professionals frustratedby their inability to relieve symptoms, and funders wasting limitedresources on ineffective treatments.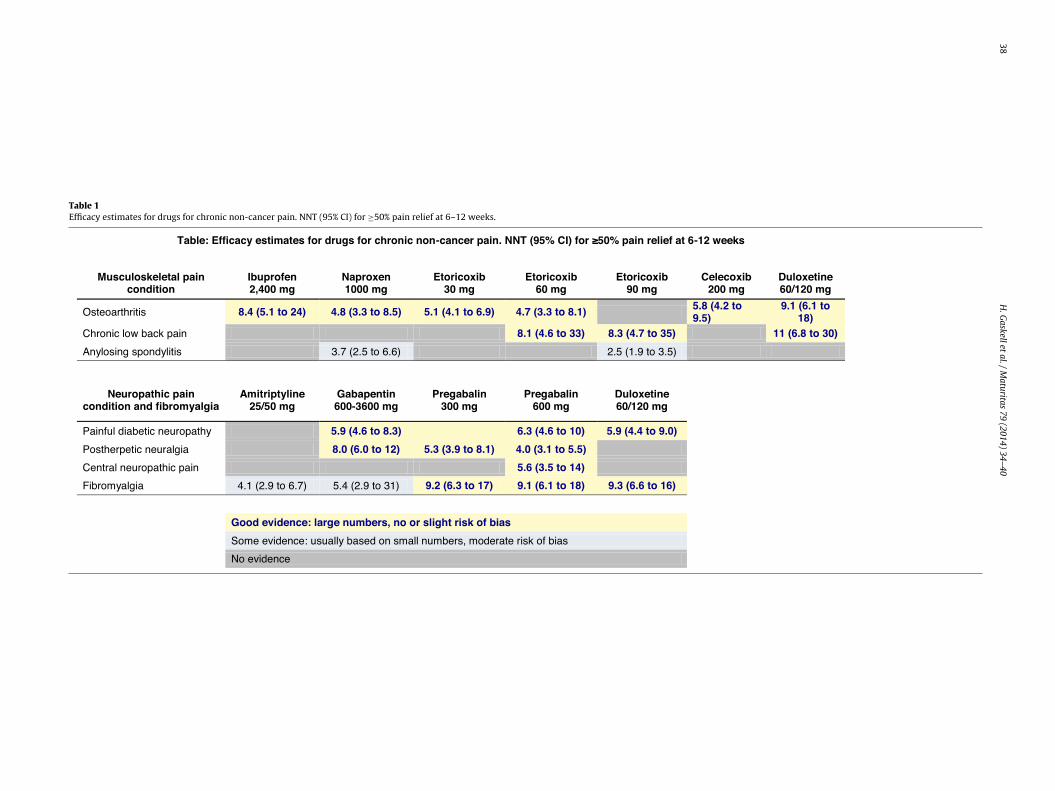
38
H.
Gaskell
et al.
/ M
aturitas 79
(2014) 34–40
Table 1Efficacy estimates for drugs for chronic non-cancer pain. NNT (95% CI) for ≥50% pain relief at 6–12 weeks.
Table: Effic acy estimates for drugs for chronic non-cancer pain. NNT (95% CI) for ≥50% pain relief at 6 -12 weeks
Musculoskeletal pain condition
Ibuprofen2,400 mg
Naproxen 1000 mg
Etoricoxib 30 mg
Etoricoxib 60 mg
Etoricoxib 90 mg
Celecoxib200 mg
Duloxetine 60/120 mg
Oste oarthritis 8.4 (5.1 to 2 4) 4.8 (3.3 to 8 .5) 5.1 (4.1 to 6 .9) 4.7 (3.3 to 8 .1) 5.8 (4.2 to 9.5)
9.1 (6.1 to 18)
Chronic low back p ain 8.1 (4.6 to 3 3) 8.3 (4.7 to 3 5) 11 (6. 8 to 3 0)
Anylosing spondylitis 3.7 (2.5 to 6. 6) 2.5 (1.9 to 3. 5)
Neuropathic pain conditio n and fibromyalg ia
Amitriptyline25/50 mg
Gabapentin600-3600 mg
Pregabalin 300 mg
Pregabalin600 mg
Duloxetine 60/120 mg
Painful diabetic neuropathy 5.9 (4.6 to 8 .3) 6.3 (4.6 to 1 0) 5.9 (4.4 to 9 .0)
Posth erpetic n euralgia 8.0 (6.0 to 1 2) 5.3 (3.9 to 8 .1) 4.0 (3.1 to 5 .5)
Central neuropat hic p ain 5.6 (3.5 to 14)
Fibromyalgia 4.1 (2.9 to 6. 7) 5.4 (2.9 to 31) 9.2 (6.3 to 1 7) 9.1 (6.1 to 1 8) 9.3 (6.6 to 16 )
Good e vidence: l arge numbers, no or s lig ht risk of bias
Some evidence: usually based o n small numbers, moderat e risk o f b ias
No evidence

aturita
apregtb
123
1
apbo5motmoiw
oe
•
•
wrc
1
eaGAtpn
cowat
r
H. Gaskell et al. / M
On the other hand we have firm evidence that some drugsre probably worth trying (NSAIDs in musculoskeletal pain, anderhaps tramadol; some antidepressants and antepileptics in neu-opathic pain, and perhaps tramadol). Other drugs are probablyither a waste of time (paracetamol) or may be ineffective and dan-erous (strong opioids). And we can be confident that success, inerms of major pain intensity reduction, should bring many otherenefits – and that is new.
There are three important messages:
. Good pain relief brings huge benefits to the patient.
. Only a minority of patients will benefit with any particular drug.
. Switching (and/or combining) drugs is often necessary to achievetreatment success
.6.2. How can we reduce risk of harm?Probably the most important thing in terms of benefit risk bal-
ncing is to be sure of the benefit. All too often patients takerescribed medication for pain without the intensity of their paineing much changed. In a recent survey of over 1000 patients withsteoarthritis in Europe, and on treatment prescribed by a doctor,5% still had moderate or severe pain [47]. This is not uncom-on, as other surveys have continued to demonstrate. Around 40%
f community-dwelling older people with chronic musculoskele-al pain hoped their physician would pay more attention to pain
anagement, more frequently in those with poor health, moderater severe pain, or those taking analgesics daily [48]. People tak-ng analgesics without good pain relief are at risk without benefit,
hich cannot be right.The balance between benefit and risk of harm from common,
r possibly rarer but more serious adverse events, depends on theffect of treatment on pain relief:
For patients with good pain relief, improved function and qualityof life, and tolerable adverse events, any increased risk of harmfrom treatment will be offset by large and immediate benefits. Itis possible to argue that the risks of not treating CNCP effectivelyare higher than the risks of treating it.For patients with pain relief but intolerable adverse events, orwith trivial pain relief and little improvement in quality of life,stop treatment and try another drug. This minimises exposure,and minimises risk of harm from a drug that does not work forthem.
Many younger people with chronic pain would anyway say theyould choose quite high risks of significant harm for even moderate
eductions in pain [49], and this is consistent with findings in otherhronic conditions.
.6.3. How can we avoid unnecessary cost?Younger people with inadequately treated chronic pain are
xpensive to manage, and much more expensive than those whore adequately treated. They might have 6–10 extra outpatient orP visits a year, have more days in hospital, and use more drugs.nnual healthcare costs for chronic pain patients are about 2.6
imes higher than for those without chronic pain, or with only mildain [14]. We do not have good data on older people, but there iso good reason to consider that it is much different.
People with adequately treated with CNCP may have higher drugosts than if they were not treated or inadequately treated, butverall healthcare expenditure is likely to be less. And even if itere not, the overall QALY gains with successful pain treatment
re between 0.1 and 0.3 in individual patients, making effectivereatment affordable in terms of cost per QALY.
Inadequate treatment is expensive (almost no QALY gain), andisky when there is no benefit. What is needed to prevent ongoing
[
s 79 (2014) 34–40 39
use is a stopping rule. In younger patients, not having at least 30%pain intensity reduction by 2–4 weeks is a simple marker of failure,and should result in stopping a treatment (with care to avoid awithdrawal reaction). For older patients, treatment may need moretapering of treatment dose “start low - go slow” but with regularreview so that patients are not left in pain [50].
2. Conclusions
The evidence about drug treatments for chronic non-cancer painis changing, driven by major improvements in understanding ofclinical trial analysis and by the adoption of patient-centered out-comes of proven economic benefit. The new perspective is of drugsthat work well in a minority of patients, but hardly at all in theremainder. Because it is not possible to predict which patient willbenefit from which drug, the emphasis is on stopping treatmentsthat do not work and switching to other drugs in the same or dif-ferent class. The good news is that early success appears to bepredictive of long-term success; early assessment of failure lim-its exposure and potential harm. But with older people, the generaladvice of staring with a low dose with frequent review still makessense, as long as pain assessment is the driver for success.
Contributors role
All contributors worked equally in assembling review data, andwriting and approving the manuscript.
Competing interests
None.
Provenance and peer review
Provenance and peer review: commissioned; externally peerreviewed.
Acknowledgement
The Oxford Pain Relief Trust provided institutional support.
References
[1] Moore RA, Derry S, Taylor RS, Straube S, Phillips CJ. The costs and consequencesof adequately managed chronic non-cancer pain and chronic neuropathic pain.Pain Pract 2014;14:79–94.
[2] van Hecke O, Austin SK, Khan RA, Smith BH, Torrance N. Neuropathic pain inthe general population: a systematic review of epidemiological studies. Pain2014;155:654–62.
[3] Elliott AM, Smith BH, Penny KI, Smith WC, Chambers WA. The epidemiology ofchronic pain in the community. Lancet 1999;354:1248–52.
[4] Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronicpain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain2006;10:287–333.
[5] Patel KV, Guralnik JM, Dansie EJ, Turk DC. Prevalence and impact of pain amongolder adults in the United States: findings from the 2011 National Health andAging Trends Study. Pain 2013;154:2649–57.
[6] Sprangers MA, de Regt EB, Andries F, van Agt HM, Bijl RV, de Boer JB. Whichchronic conditions are associated with better or poorer quality of life. J ClinEpidemiol 2000;53:895–907.
[7] Torrance N, Elliott AM, Lee AJ, Smith BH. Severe chronic pain is associatedwith increased 10 year mortality. A cohort record linkage study. Eur J Pain2010;14:380–6.
[8] Nüesch E, Dieppe P, Reichenbach S, Williams S, Iff S, Jüni P. All cause and diseasespecific mortality in patients with knee or hip osteoarthritis: population basedcohort study. Br Med J 2011;342:d1165.
[9] Dworkin RH, O’Connor AB, Kent J, Mackey SC, Raja SN, Stacey BR, et al. Inter-ventional management of neuropathic pain: NeuPSIG recommendations. Pain2013;154:2249–61.
10] Derry CJ, Derry S, McQuay HJ, Moore RA. Systematic review of systematicreviews of acupuncture published 1996–2005. Clin Med 2006;6:381–6.
4 aturita
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
0 H. Gaskell et al. / M
11] Truitt KE, Sperling RS, Ettinger Jr WH, Greenwald M, DeTora L, Zeng Q, et al. Amulticenter, randomized, controlled trial to evaluate the safety profile, tolera-bility, and efficacy of rofecoxib in advanced elderly patients with osteoarthritis.Aging (Milano) 2001;13:112–21.
12] Whelton A, Fort JG, Puma JA, Normandin D, Bello AE, Verburg KM, et al.Cyclooxygenase-2-specific inhibitors and cardiorenal function: a randomized,controlled trial of celecoxib and rofecoxib in older hypertensive osteoarthritispatients. Am J Ther 2001;8:85–95.
13] Semel D, Murphy TK, Zlateva G, Cheung R, Emir B. Evaluation of the safety andefficacy of pregabalin in older patients with neuropathic pain: results from apooled analysis of 11 clinical studies. BMC Fam Pract 2010;11:85.
14] Moore RA, Straube S, Aldington D. Pain measures and cut-offs – ‘no worse thanmild pain’ as a simple, universal outcome. Anaesthesia 2013;68:400–12.
15] Moore RA. What works for whom? Determining the efficacy and harm of treat-ments for pain. Pain 2013;154(Suppl. 1):S77–86.
16] Moore RA, Derry S, Wiffen PJ. Challenges in design and interpretation of chronicpain trials. Br J Anaesth 2013;111:38–45.
17] Moore RA, Straube S, Eccleston C, Derry S, Aldington D, Wiffen P, et al. Estimateat your peril: imputation methods for patient withdrawal can bias efficacy out-comes in chronic pain trials using responder analyses. Pain 2012;153:265–8.
18] Moore RA, Cai N, Skljarevski V, Tölle TR. Duloxetine use in chronic painful con-ditions – individual patient data responder analysis. Eur J Pain 2014;18:67–75.
19] Straube S, Derry S, Moore RA, Paine J, McQuay HJ. Pregabalin in fibromyalgia– responder analysis from individual patient data. BMC Musculoskelet Disord2010;11:150.
20] Moore RA, Moore OA, Derry S, Peloso PM, Gammaitoni AR, Wang H. Responderanalysis for pain relief and numbers needed to treat in a meta-analysis of etori-coxib osteoarthritis trials: bridging a gap between clinical trials and clinicalpractice. Ann Rheum Dis 2010;69:374–9.
21] Moore RA, Smugar SS, Wang H, Peloso PM, Gammaitoni A. Numbers-needed-to-treat analyses – do timing, dropouts, and outcome matter? Pooled analysisof two randomized, placebo-controlled chronic low back pain trials. Pain2010;151:592–7.
22] Peloso PM, Gammaitoni A, Smugar SS, Wang H, Moore RA. Longitudinalnumbers-needed-to-treat (NNT) for achieving various levels of analgesicresponse and improvement with etoricoxib, naproxen, and placebo in anky-losing spondylitis. BMC Musculoskelet Disord 2011;12:165.
23] Moore A, Derry S, Eccleston C, Kalso E. Expect analgesic failure; pursue analgesicsuccess. Br Med J 2013;346:f2690.
24] Bingham 3rd CO, Smugar SS, Wang H, Tershakovec AM. Early response to COX-2 inhibitors as a predictor of overall response in osteoarthritis: pooled resultsfrom two identical trials comparing etoricoxib, celecoxib and placebo. Rheuma-tology (Oxford) 2009;48:1122–7.
25] Towheed TE, Maxwell L, Judd MG, Catton M, Hochberg MC, WellsG. Acetaminophen for osteoarthritis. Cochrane Database Syst Rev2006;1:CD004257.
26] Doherty M, Hawkey C, Goulder M, Gibb I, Hill N, Aspley S, et al. A randomisedcontrolled trial of ibuprofen, paracetamol or a combination tablet of ibupro-fen/paracetamol in community-derived people with knee pain. Ann RheumDis 2011;70:1534–41.
27] Federal Register Notice Prescription Drug Products Containing Acetaminophen;Actions to Reduce Liver Injury From Unintentional Overdose – DocketNumber FDA-2011-N-0021-0001; 2014. http://www.regulations.gov/#!documentDetail;D=FDA-2011-N-0021-0001
28] National Institute for Health and Care Excellence. Osteoarthritis: Care and man-agement in adults. NICE clinical guideline 177; 2014 February.
29] Abdulla A1, Adams N, Bone M, Elliott AM, Gaffin J, Jones D, et al. Guidanceon the management of pain in older people. Age Ageing 2013;42(Suppl 1):i1–57.
[
s 79 (2014) 34–40
30] Derry S, Moore RA, Rabbie R. Topical NSAIDs for chronic musculoskeletal painin adults. Cochrane Database Syst Rev 2012;9:CD007400.
31] Coxib and traditional NSAID Trialists’ (CNT) Collaboration, Bhala N, EmbersonJ, Merhi A, Abramson S, Arber N, et al. Vascular and upper gastrointestinaleffects of non-steroidal anti-inflammatory drugs: meta-analyses of individualparticipant data from randomised trials. Lancet 2013;382:769–79.
32] Bhala N, Emberson J, Patrono C, Baigent C, CNT Collaborators. Coxibs and tra-ditional NSAIDs for pain relief – Authors’ reply. Lancet 2014;383:122.
33] Mangoni AA, Woodman RJ, Gaganis P, Gilbert AL, Knights KM. Use of non-steroidal anti-inflammatory drugs and risk of incident myocardial infarctionand heart failure, and all-cause mortality in the Australian veteran community.Br J Clin Pharmacol 2010;69:689–700.
34] Zin CS, Chen LC, Knaggs RD. Changes in trends and pattern of strong opioidprescribing in primary care. Eur J Pain 2014 April [Epub ahead of print].
35] Ruscitto A, Smith BH, Guthrie B. Changes in opioid and other analgesic use1995-2010: Repeated cross-sectional analysis of dispensed prescribing for alarge geographical population in Scotland. Eur J Pain 2014 May [Epub ahead ofprint].
36] Weisberg D, Stannard C. Lost in translation? Learning from the opioid epidemicin the USA. Anaesthesia 2013;68:1215–9.
37] Cepeda MS, Camargo F, Zea C, Valencia L. Tramadol for osteoarthritis: a sys-tematic review and metaanalysis. J Rheumatol 2007;34:543–55.
38] Hollingshead J, Dühmke RM, Cornblath DR. Tramadol for neuropathic pain.Cochrane Database Syst Rev 2006;3:CD003726.
39] McNicol ED, Midbari A, Eisenberg E. Opioids for neuropathic pain. CochraneDatabase Syst Rev 2013:8. CD006146.
40] Gaskell H, Moore RA, Derry S. Oxycodone for neuropathic pain and fibromyalgiain adults. Cochrane Database Syst Rev 2013;8. CD010692 [Full review submit-ted].
41] Lange B, Kuperwasser B, Okamoto A, Steup A, Häufel T, Ashworth J, et al. Efficacyand safety of tapentadol prolonged release for chronic osteoarthritis pain andlow back pain. Adv Ther 2010;27:381–99.
42] Solomon DH, Rassen JA, Glynn RJ, Lee J, Levin R, Schneeweiss S. The com-parative safety of analgesics in older adults with arthritis. Arch Intern Med2010;170:1968–76.
43] Wiffen PJ, Derry S, Moore RA, Aldington D, Cole P, Rice ASC, et al. Antiepilep-tic drugs for neuropathic pain and fibromyalgia – an overview of Cochranereviews. Cochrane Database Syst Rev 2013:11. CD010567.
44] Kalso E, Aldington DJ, Moore RA. Drugs for neuropathic pain. Br Med J2013;347:f7339.
45] Derry S, Sven-Rice A, Cole P, Tan T, Moore RA. Topical capsaicin (high concen-tration) for chronic neuropathic pain in adults. Cochrane Database Syst Rev2013:2. CD007393.
46] Derry S, Moore RA. Topical capsaicin (low concentration) for chronic neuro-pathic pain in adults. Cochrane Database Syst Rev 2012:9. CD010111.
47] Conaghan P, Peloso PM, Everett SV, Rajagopalan S, Black CM, Mavros P, et al.Inadequate pain relief and large functional loss among patients with kneeosteoarthritis: evidence from a prospective, multinational longitudinal studyof osteoarthritis real world therapies (SORT). Rheumatology 2014 [in press].
48] Karttunen NM, Turunen J, Ahonen R, Hartikainen S. More attention to pain man-agement in community-dwelling older persons with chronic musculoskeletalpain. Age Ageing 2014 May [Epub ahead of print].
49] Richardson CG, Chalmers A, Llewellyn-Thomas HA, Klinkhoff A, Carswell A,Kopec JA. Pain relief in osteoarthritis: patients’ willingness to risk medication-
induced gastrointestinal, cardiovascular, and cerebrovascular complications. JRheumatol 2007;34:1569–75.50] American Geriatrics Society Panel on Pharmacological Management of Persis-tent Pain in Older Persons. Pharmacological management of persistent pain inolder persons. J Am Geriatr Soc 2009;57:1331–46.