treatment of opioid addiction. ihi
TRANSCRIPT

Treatment of Opioid Use Disorders
George Kolodner, M.D.
Chief Clinical Officer
Kolmac Outpatient Recovery Centers
Clinical Professor of Psychiatry
Georgetown and University Schools of Medicine
Overview
• Clinical Issues• Basics of Treatment• Recent History of Treatment• Specifics
• Biological• Psychological• Social
• Discussion
• Policy Issues
• Discussion
Substance Use Disorder
• A primary, chronic disease of brain reward, motivation, memory and related circuitry• Leads to characteristic biological, psychological, and social
manifestations
• Characterized by:• Inability to consistently abstain
• Impairment in behavioral control
• Craving
• Diminished recognition of significant problems with one’s behaviors and interpersonal relationships
• Dysfunctional emotional response
Distinguish Addiction From:• “Physical dependence”: signs and symptoms
experienced upon the abrupt discontinuation of a substance (withdrawal)• Can develop with non-addictive substances (steroids,
paroxetine)
• Stimulants are addictive without causing physical dependence
• “Dependence” eliminated from DSM-5
• Substances: act as the agent in the disease, but can be used safely by most people without resulting in addiction

Addictive Potential of a Drug:Increased by Fast CNS Onset and Offset
• Substance characteristics• Shorter half life• More pure
• Coca leaf vs. purified powder
• More lipophilic• Diazepam vs. chlordiazepoxide• Heroin vs. morphine
• Route of administration• Smoking > intravenous > nasal > oral
• Rush vs. high
• Genetic variability of user• Rapid metabolizers of nicotine addiction more likely

32
2317 15
11 9 95 4
Percentage of Substance Users WhoBecome Addicted, by Substance
Addiction Treatment Basics
• Treatment goal is recovery, not cure• “Recovering” not “ex-” or “reformed” addict• Return to safe use is statistically unlikely because underlying
vulnerability persists
• Abstinence -- not moderation, is the foundation• Includes other psychoactive substances
• Strategy: establish abstinence at outset and work to prevent relapse• Versus working with using patient toward abstinence
• Manage as a chronic illness, like hypertension and diabetes• Importance of long term follow up treatment• Respond to relapses with appropriate clinical intervention as
quickly as possible
Elements of Effective Treatment
• Separation from the substance
• Healing environment• Psycho-educational groups
• Cognitive-behavioral concepts
• Collaborate with community recovery support groups
• Include family, especially for adolescents and young adults
• Few medications available, but are useful

Treatment Settings
• Outpatient• Primary care
• Psychotherapy
• Structured program for withdrawal management and addiction rehabilitation
• Inpatient• Psychiatric hospital
• Medical hospital withdrawal management
• Residential addiction rehabilitation

Treatment of Opioid Use Disorders: Differences • Withdrawal symptoms tend to be more frequent,
severe, and protracted than with other substances
• Treatment without supportive medication has been less successful than for other substances• Controversy about the balance between therapy and
medication• Controversy about the role of agonist and antagonist
medication• Struggle with definition of “abstinence” and “recovery”
• Chronic pain may have been the trigger for use and can persist during recovery
Agonists and Antagonists
• Full agonist: attaches to opioid receptor and fully activates it• Opium, morphine, codeine, oxycodone (Oxycontin, Percocet), hydrocodone
(Vicodin), methadone
• Antagonist: attaches to opioid receptor and blocks it instead of activating it• Naloxone (“Narcan”)
• Reverses opioid overdose: immediate effect with short duration• Injectable or nasal preparation
• Naltrexone• Used for relapse prevention: long term (months to years)• Oral (“Revia”) or 1 month depot injection (“Vivitrol”)
• Partial agonist: attaches to opioid receptor, partially activates and blocks it• Buprenorphine (Suboxone, Zubsolv)


Recent History of Opioid Addiction Treatment
• 1960’s. Methadone• Restricted to specialized programs (OTPs)• Medication dispensed, not prescribed• Rich psychosocial context was gradually abandoned
• 1960’s. Residential therapeutic communities (TCs)• Opposed to use of methadone
• 1980’s. Alcoholism treatment programs expanded to include opioids• Most opposed methadone and buprenorphine
• 2003. Buprenorphine• Less restricted than methadone• Medication prescribed

Opioids For Addiction Treatment:A Change of Approach
• Methadone• 1937. Developed in Germany for pain
• 1971. Approved in USA for detoxification and maintenance of opioid addicts
• Highly restricted use – regulated programs (OTP)
• Now taken by about 250,000 patients in US
• Buprenorphine• 1978. Parenteral formulation for pain
• 2000 – 2003. Approval for addiction treatment
• Available for office based use by “waivered” physicians
• Now taken by about 1,000,000 patients in US

Methadone
• Actions• Normalizes the neuroendocrine alterations induced by short-acting opioids with minimal
psychoactive impairment• Blocks effect of other opioids
• Benefits• Overall reduction in mortality rates• Reduction in transmission of infectious diseases
• HIV, Hepatitis B and C• Reduction in crime• Driving not impaired on once daily dosing
• Included in World Health Organization list of essential medications
• “Current policy puts too much emphasis on protecting society from methadone, and not enough on protecting society from the epidemic of addiction, violence, and infections that methadone can help reduce.” IOM, 1995
Advantages of Buprenorphine
1. Safer from overdose than methadone• Ceiling on respiratory depression
• Benzodiazepines raise ceiling
2. Rarely causes euphoria unless taken IV• Partial mu agonist
3. Blocks most other opioids at low dose• High affinity for receptor sites
4. Long acting
5. For addiction treatment, physicians allowed to write prescriptions as Schedule III medication
• Physicians are not allowed to prescribe methadone or other opioids for addictions
Pregnancy: Buprenorphine vs. Methadone
• Same incidence of neonatal abstinence syndrome (NAS)
• Less severe NAS with buprenorphine• 89 % less medication
• 43% fewer hospital days
• More discontinuation of buprenorphine than methadone because of dissatisfaction with medication
• Methadone still the official standard of care

Antagonists• Naloxone (“Narcan”)
• Reverses opioid overdose
• Immediate effect with short duration
• Injectable or nasal preparation
• Naltrexone• Used for relapse prevention
• Long term (months to years)
• Oral (“Revia”) or 1 month depot injection (“Vivitrol”)

Kolmac Outpatient Treatment Model
• Accessibility• Time: evening or morning hours accommodate work or home responsibilities• Financial: covered by health insurance, 20% the cost of residential• Location: close to home and work sites• Minimal waiting: begin treatment within one business day
• 3 overlapping levels of care• Withdrawal management: 3 to 8 hours for 2 days• Intensive outpatient rehabilitation (“IOP”): 3 hours, tapering from 5 to 2
times/week over 8 weeks• Continuing care: 2 hours/day, 1 day/week
• Denser clinical staffing than hospital or residential treatment
• Expandable capacity• Establish new sites and new groups on existing sites

Motivational Interviewing
• A collaborative, goal-oriented style of communication with particular attention to the language of change
• Designed to strengthen personal motivation for and commitment to a specific goal…• By eliciting and exploring a person’s own reasons for change
• Within an atmosphere of acceptance and compassion
• Ambivalence is considered to be a normal and expected part of the process of change• “Denial” seen as the expression of a dysfunctional relationship and damaged
rapport
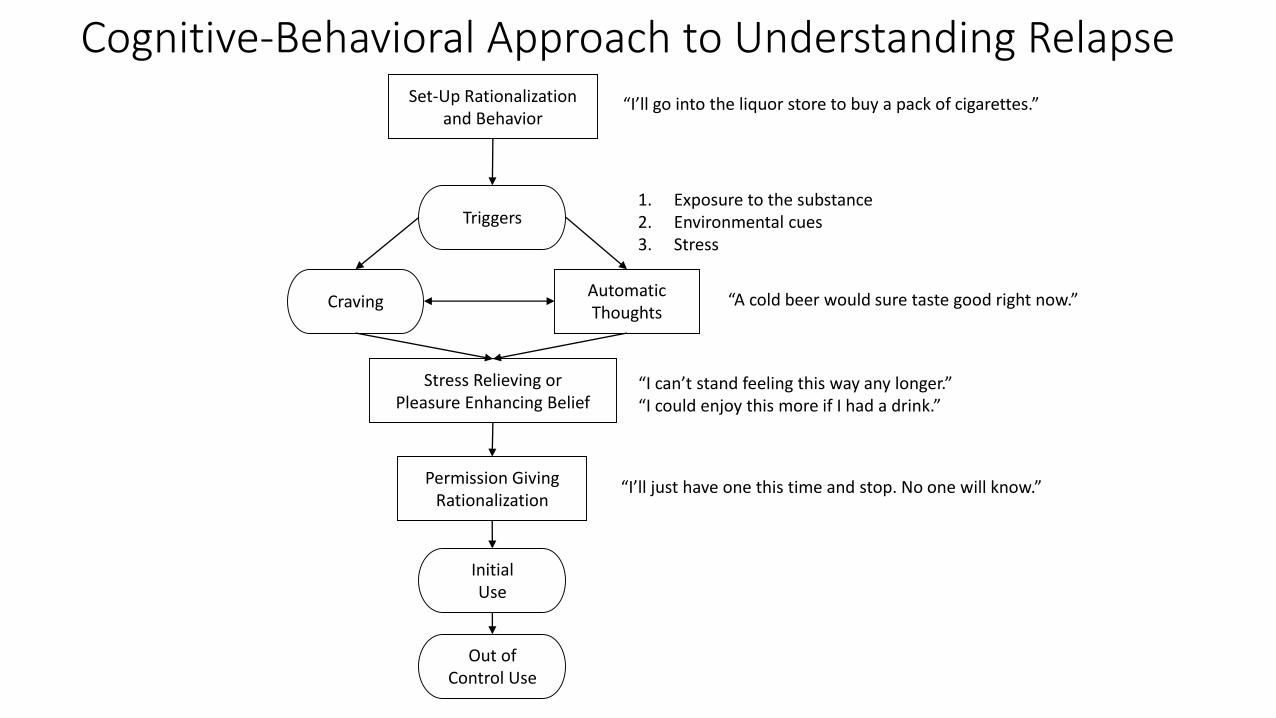
Set-Up Rationalizationand Behavior
Automatic Thoughts
Stress Relieving orPleasure Enhancing Belief
Triggers
Craving
InitialUse
Out ofControl Use
Permission Giving Rationalization
Cognitive-Behavioral Approach to Understanding Relapse“I’ll go into the liquor store to buy a pack of cigarettes.”
“A cold beer would sure taste good right now.”
“I can’t stand feeling this way any longer.”“I could enjoy this more if I had a drink.”
“I’ll just have one this time and stop. No one will know.”
1. Exposure to the substance2. Environmental cues3. Stress

RedLow in both % participation
and recovery relevance
Yellow
Low % participation
% S
po
nta
neo
us
Part
icip
atio
n
Group Psychotherapy Diagram
Recovery Relevance
Yellow
Low recovery relevance
Green Goals:• Maximize participation
and recovery relevance• Optimize emotional
depth

Non-Professional Support Groups
• 12-Step Fellowship• Alcoholics Anonymous, Narcotics Anonymous, Cocaine
Anonymous, Marijuana Anonymous, etc.• Biopsychosocial plus spiritual elements
• “Secular” organizations: Smart Recovery• Groups are fewer and smaller• Focus on cognitive rather than spiritual• Led by trained volunteer facilitator
• Religious organizations: Celebrate Recovery• Church based• Fastest growing segment of support community
Harm Reduction
• Needle exchange
• Protected use sites
• Heroin prescription

Discussion of Clinical Issues
Treatment Policy Issues
1. Opioid addiction is a complex issue that is seen in very different ways depending upon one’s interests and philosophies• Compare:
• Family member (parent, child, spouse)• Physician (surgeon, pain management, addiction specialist)• Pharmaceutical manufacturer of opioid medication• Criminal justice (prosecutor/defense attorney, police, prison guard)• Politician
2. The likelihood of policy change depends on achieving collaboration between these competing points of view• Policy change can be in either a productive or counter-productive direction
3. One historical theme has been the shifting balance between treatment and criminal justice

Harrison Anti-Narcotic Act (1914)
• Intent: To restrict the use of opioids and cocaine to legitimate medical purposes• Means: registration and taxation by Department of Treasury
• Actual effect: interpretation and enforcement criminalized opioid addicts and physicians• 25,000 physicians indicted: 3,000 jailed
• Viewed addicts as being criminals rather than having a medical disease
• Most physicians withdrew from treating this population
• Persists in Controlled Substances Act (1970)
Obstacles to Address
• Insurance coverage exclusion and limitations• Parity for behavioral health treatment
• Stigma of addiction• “Not in my back yard”
• Stigma against using opioid medications• “Just exchanging one drug for another.”
• Medical profession• Disinterest• Pessimism• Fueling the addiction by overly prescribing opioids
Community Opposition: Not In My Backyard

Changes Resulting From Collaboration
• 19th Century. Opioid prescription epidemic
• 1971. Heroin use by American soldiers during Vietnam War
• 2017. Banning the practice of prior authorization of buprenorphine

19th Century Opioid Prescription Epidemic
• 1870s – 80s: Overuse of hypodermic injection by physicians
• 1890’s – 1910s: Change to more balanced prescribing patterns through education and pressure by reform minded physicians and pharmacists• Occurred before 1914 passage of Harrison Anti-Narcotics Act
• NEJM 373:22, 2095-7, 2015. David Courtwright

Nixon: Heroin, Crime, and Vietnam War
• 1968. Campaigned on increasing “law and order”
• 1970. Rejected strategy to reduce crime by increasing access to treatment
• 1971. Reconsidered treatment strategy after reports of heroin use by American soldiers returning from Vietnam War
• Urine testing imposed on returning soldiers• Uniform Code of Military Justice suspended
• Vietnam success broke log jam over establishment of national treatment network
• Reduction of crime
• 1972. Loss of emphasis after re-election

Prior Authorization of Buprenorphine in Maryland• HB 887 proposed by Maryland delegate and addiction treatment
organizations to ban practice of prior authorization of buprenorphine• Argument: delays treatment without increasing care quality or reducing costs
• Opposed by insurance carriers• Concerns about setting precedent interfering with management of rising
medication costs
• March 1. Governor Larry Hogan declares state of emergency because of persistence of opioid problem in Maryland
• March 2. Insurance carriers drop opposition and testify in support of bill• Cost concern persists, but opioid issue deemed too important
