treatment of severe familial hypercholesterolemia pcsk9 ... · treatment of severe familial...
TRANSCRIPT
Treatment of severe Familial Hypercholesterolemia
PCSK9 inhibitors
Dr. Khalid Al-Waili, MD, FRCPC, DABCL
Senior Consultant Medical Biochemist & Lipidologist
Sultan Qaboos University Hospital
Identifying and Treating Severe Familial Hypercholesterolemia
October 14-15, 2017
Dubai, UAE
Disclosure
• Honoraria for consulting, research and
speaker activities from:
– Astra Zeneca, Pfizer, Sanofi/Regeneron.
Cardiovascular Disease (CVD) remains the biggest killer
worldwide
Reducing levels of low-density lipoprotein (LDL) cholesterol is
a cornerstone of the prevention of CVD.
Despite the proven efficacy of statins in lowering CV events,
many patients fail to reach recommended LDL-C goals
Background
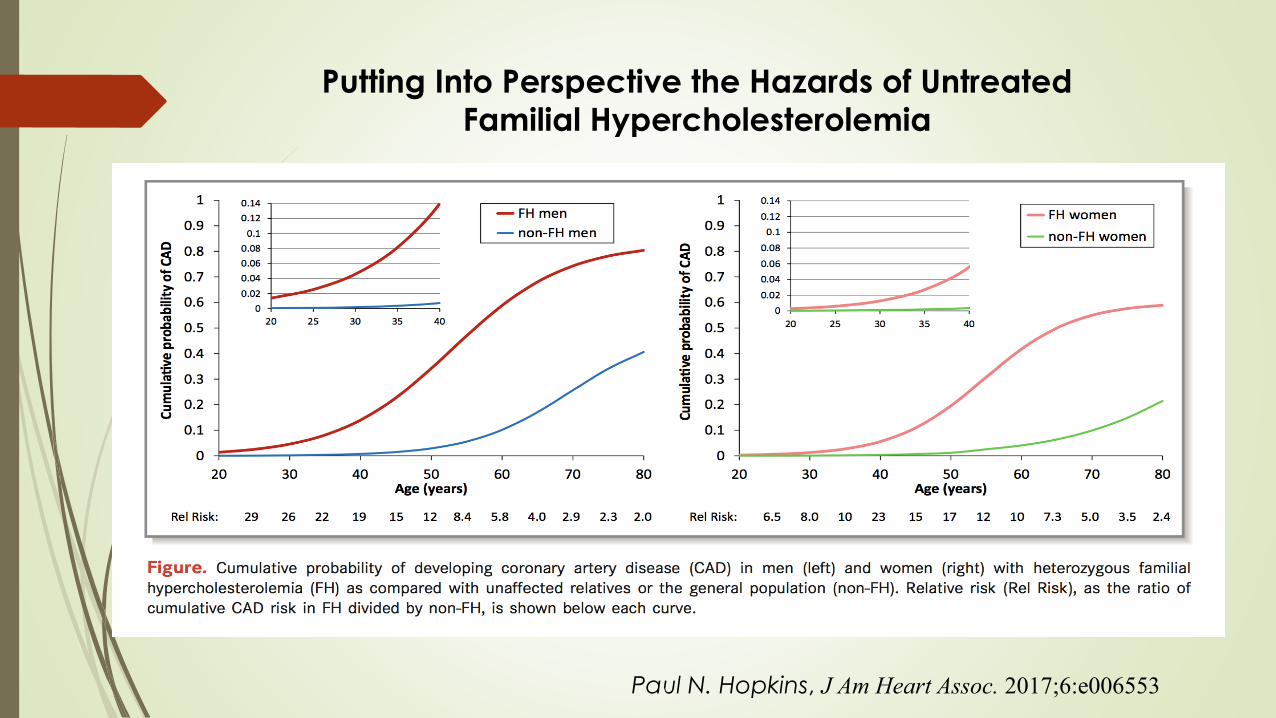
Putting Into Perspective the Hazards of Untreated Familial Hypercholesterolemia
Paul N. Hopkins, J Am Heart Assoc. 2017;6:e006553
Focus on treatment of blood cholesterol to reduce ASCVD risk
in adults
No LDL-C (and non–HDL-C) treatment goals
Statin centric
Identification of 4 patient groups most likely to benefit from
statin therapy
2013 ACC/AHA Guideline on the
Treatment of Blood Cholesterol
ACC=American College of Cardiology; AHA=American Heart Association; ASCVD=arteriosclerotic cardiovascular disease;
HDL-C=high-density lipoprotein cholesterol; LDL-C=low-density lipoprotein cholesterol.
Stone NJ et al. Circulation. 2013; doi:10.1161/01.cir.0000437738.63853.7a/-/DC1.
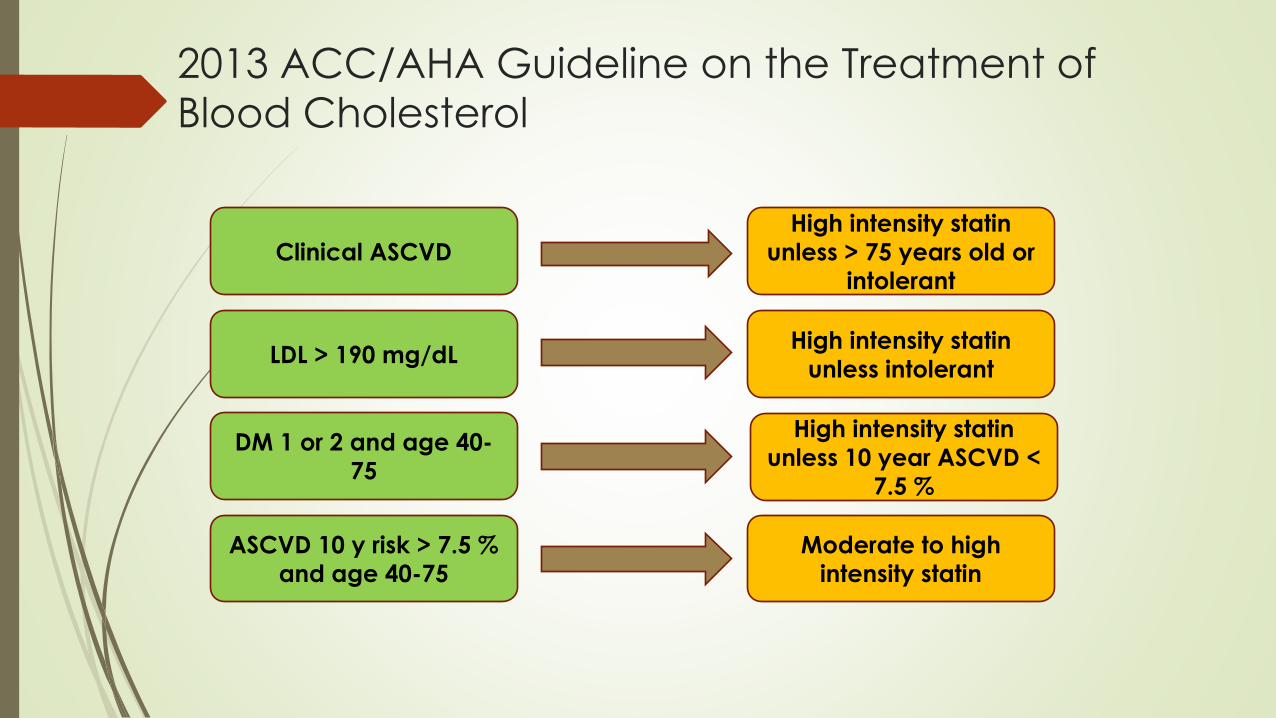
2013 ACC/AHA Guideline on the Treatment of
Blood Cholesterol
Clinical ASCVD
LDL > 190 mg/dL
DM 1 or 2 and age 40-
75
ASCVD 10 y risk > 7.5 %
and age 40-75
High intensity statin
unless > 75 years old or
intolerant
High intensity statin
unless intolerant
High intensity statin
unless 10 year ASCVD <
7.5 %
Moderate to high
intensity statin
The Actual Evidence
At that time Statin drugs are the only class with actual mortality and morbidity
benefits studied in randomized controlled trials
No RCT evidence that adjuncts to statin therapy add clinical benefit
Actually evidence to the contrary:
AIM HIGH: niacin added to statin when LDL < 80 mg/dL provides no benefit
ACCORD: adding fenofibrate to statin in patients with DM provides no
benefit
Focus Shift from LDL lowering to mortality and morbidity benefit
No evidence for target LDL levels in terms of ASCVD event risk reduction
High intensity statin therapy ( > 50 % LDL reduction) provides more clinical
benefit than moderate intensity therapy ( 30-50 % LDL reduction)
Are Statins Enough?
Statins are effective, potent, inexpensive and
generally well tolerated
Residual Risk
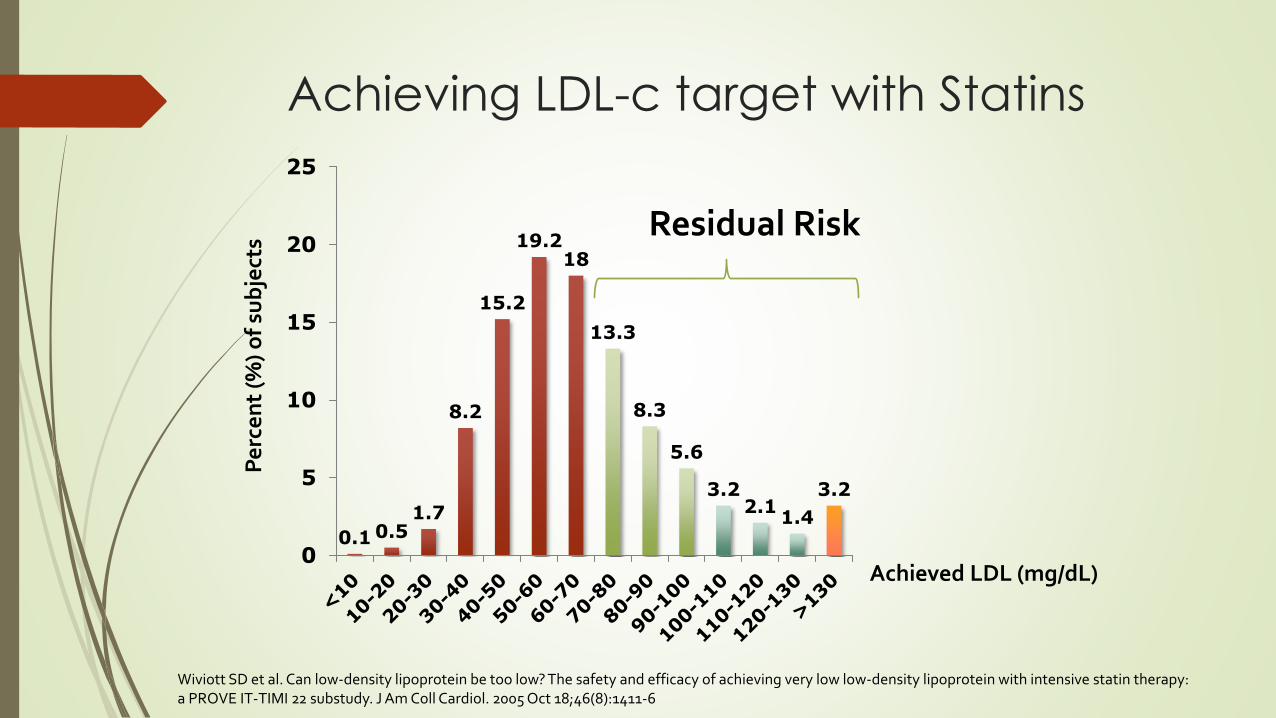
Achieving LDL-c target with Statins
Wiviott SD et al. Can low-density lipoprotein be too low? The safety and efficacy of achieving very low low-density lipoprotein with intensive statin therapy: a PROVE IT-TIMI 22 substudy. J Am Coll Cardiol. 2005 Oct 18;46(8):1411-6
0.10.51.7
8.2
15.2
19.218
13.3
8.3
5.6
3.22.11.4
3.2
0
5
10
15
20
25
Pe
rce
nt
(%)
of
sub
ject
s
Achieved LDL (mg/dL)
Residual Risk
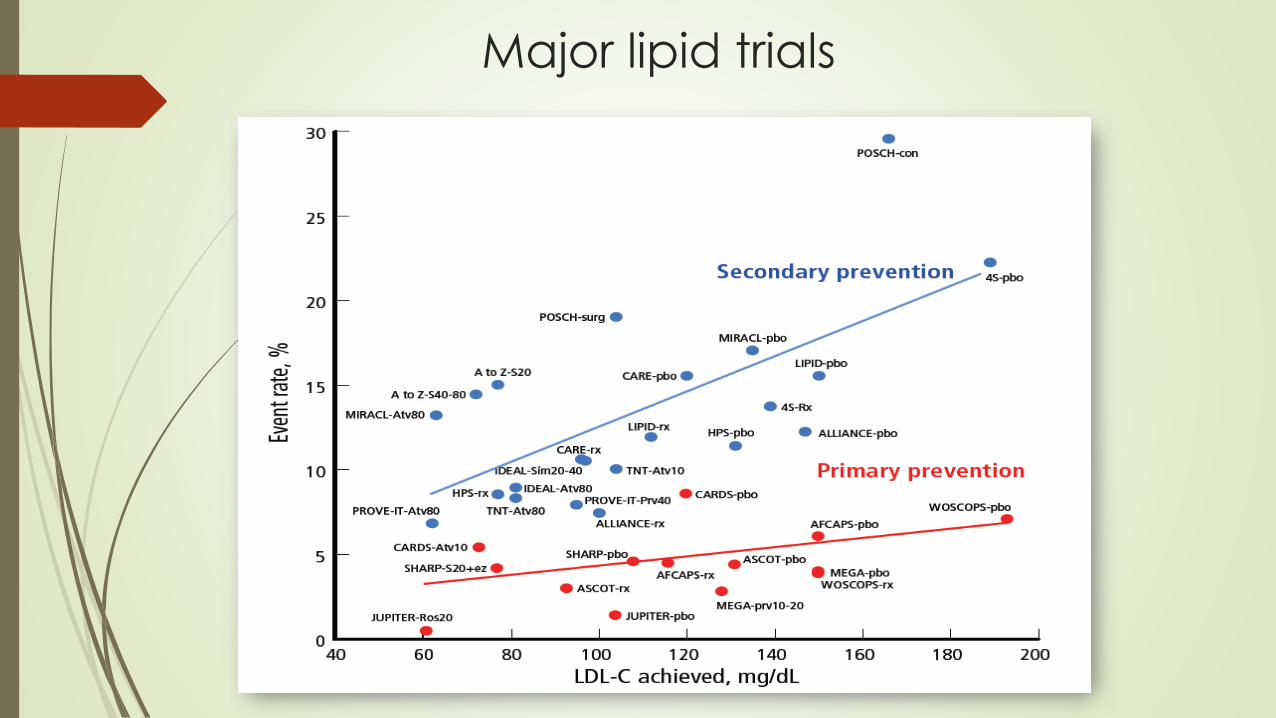
Major lipid trials
Is a low LDL better and is a low LDL-C safe ?
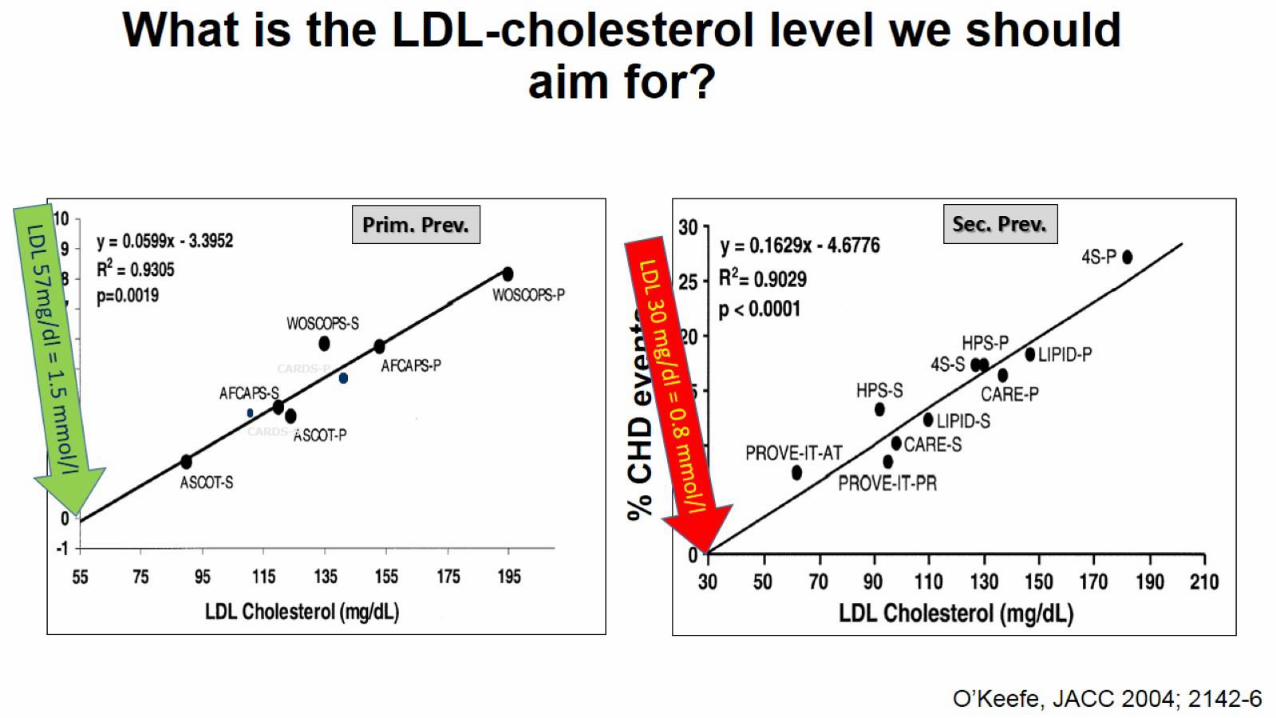
How low is too low LDL-c?
Persons born with defective PCSK9 gene have very low LDL
They are protected from CVD
No depression
No cognitive abnormalities
They are generally healthy
They have LDL-c <30mg/dL
Have no particular side effects
Appear to benefit from low LDL-c
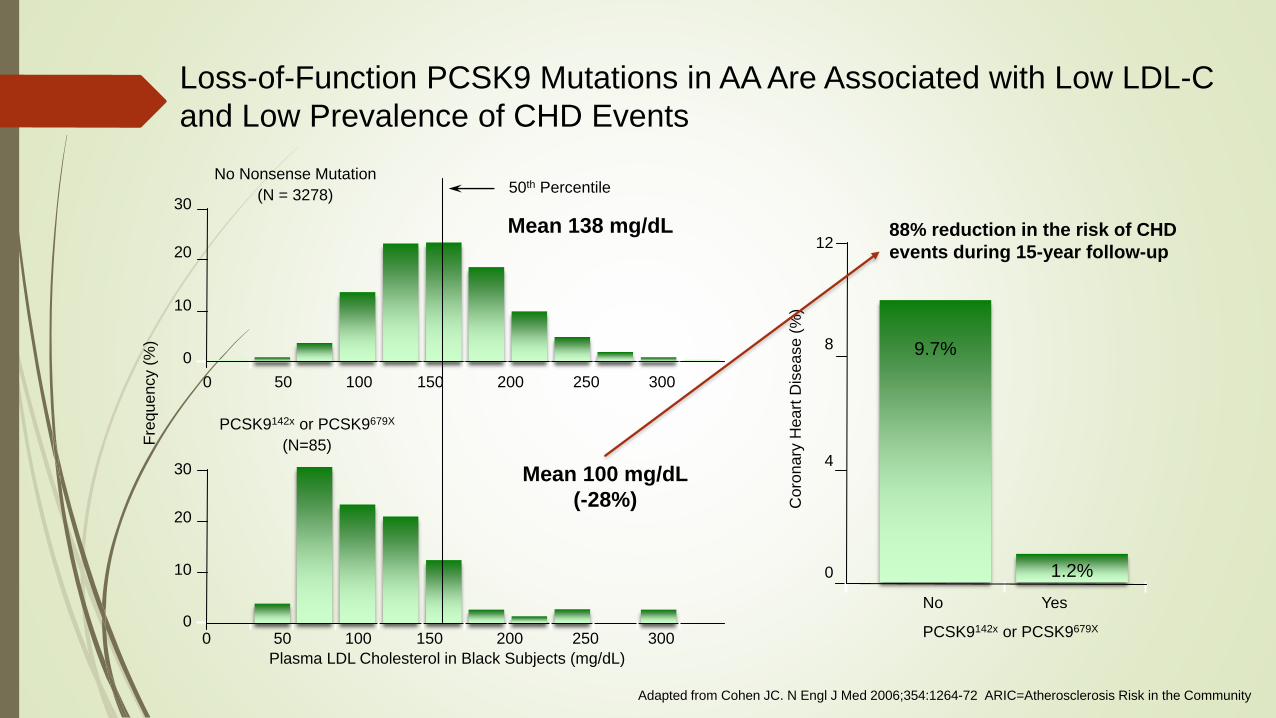
Loss-of-Function PCSK9 Mutations in AA Are Associated with Low LDL-C
and Low Prevalence of CHD Events
Adapted from Cohen JC. N Engl J Med 2006;354:1264-72 ARIC=Atherosclerosis Risk in the Community
30
20
10
09.7%
PCSK9142x or PCSK9679X
No Yes
12
8
4
0
0 50 100 150 200 250 300
30
20
10
00 50 100 150 200 250 300
No Nonsense Mutation
(N = 3278)50th Percentile
Plasma LDL Cholesterol in Black Subjects (mg/dL)
Fre
quency (
%)
1.2%
PCSK9142x or PCSK9679X
(N=85)
Coro
nary
Heart
Dis
ease (
%)
Mean 138 mg/dL
Mean 100 mg/dL
(-28%)
88% reduction in the risk of CHD
events during 15-year follow-up
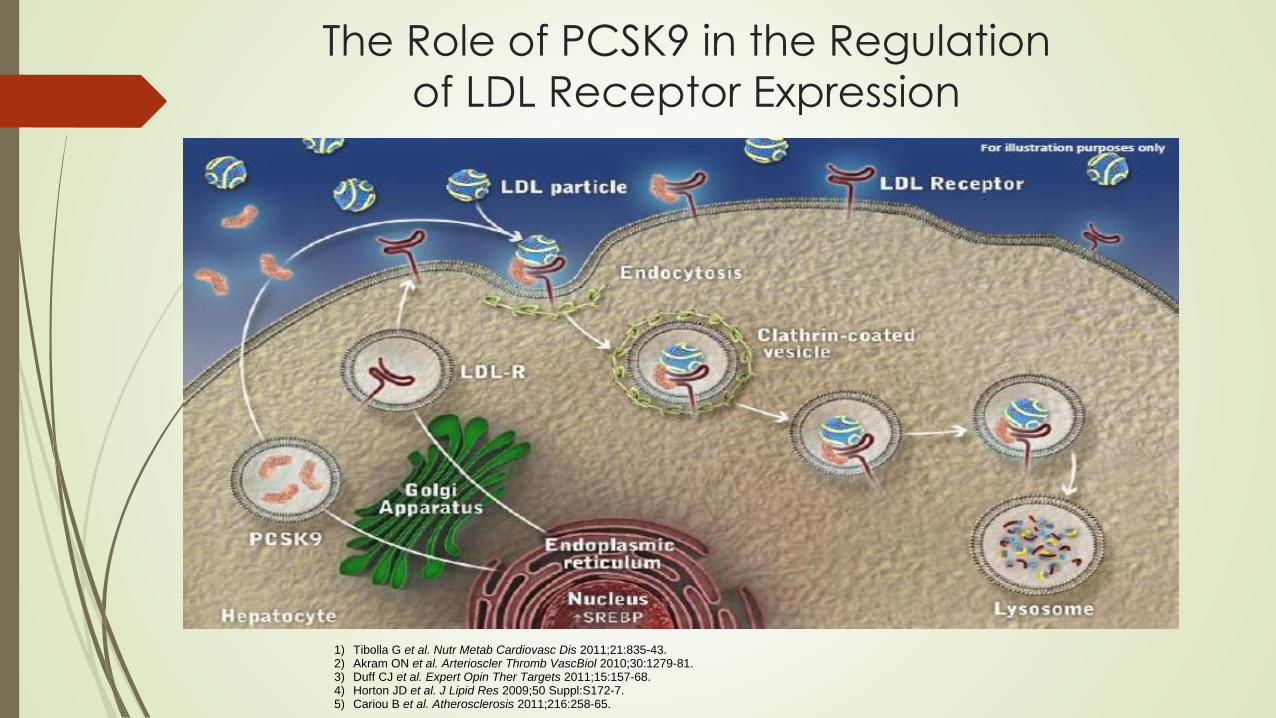
The Role of PCSK9 in the Regulation
of LDL Receptor Expression
1) Tibolla G et al. Nutr Metab Cardiovasc Dis 2011;21:835-43.2) Akram ON et al. Arterioscler Thromb VascBiol 2010;30:1279-81.3) Duff CJ et al. Expert Opin Ther Targets 2011;15:157-68.4) Horton JD et al. J Lipid Res 2009;50 Suppl:S172-7.5) Cariou B et al. Atherosclerosis 2011;216:258-65.
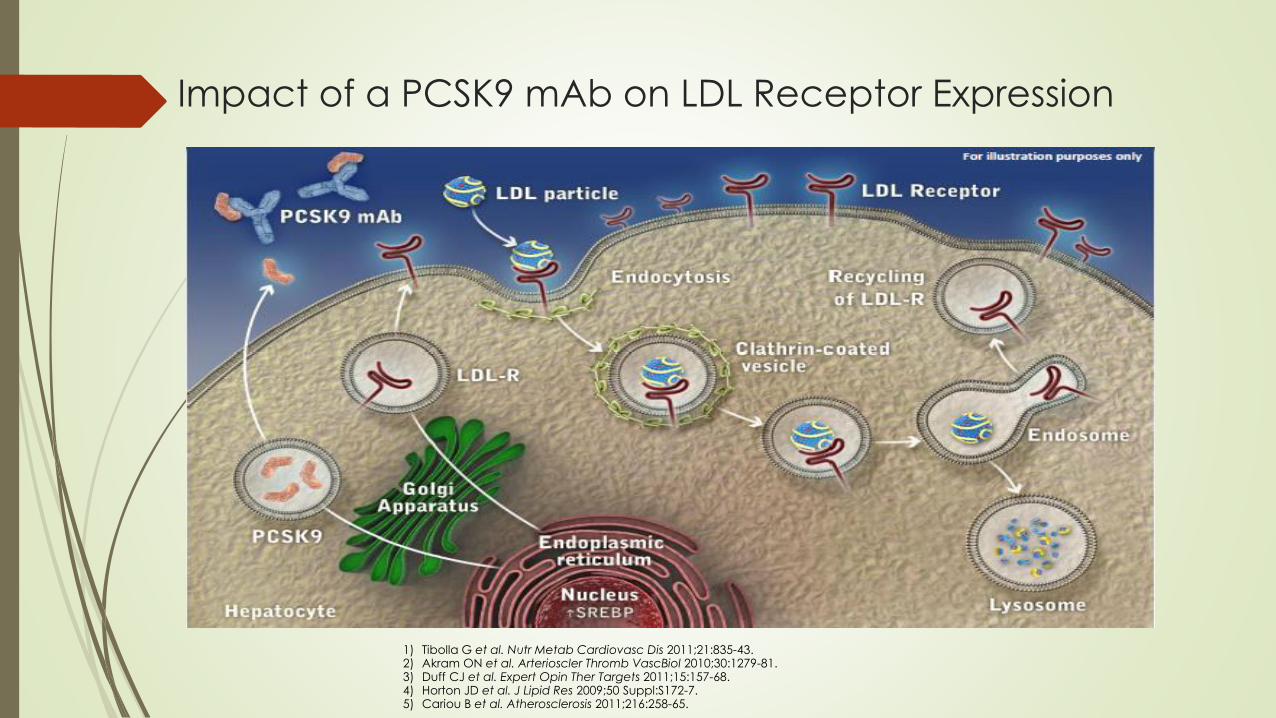
Impact of a PCSK9 mAb on LDL Receptor Expression
1) Tibolla G et al. Nutr Metab Cardiovasc Dis 2011;21:835-43.2) Akram ON et al. Arterioscler Thromb VascBiol 2010;30:1279-81.3) Duff CJ et al. Expert Opin Ther Targets 2011;15:157-68.4) Horton JD et al. J Lipid Res 2009;50 Suppl:S172-7.5) Cariou B et al. Atherosclerosis 2011;216:258-65.
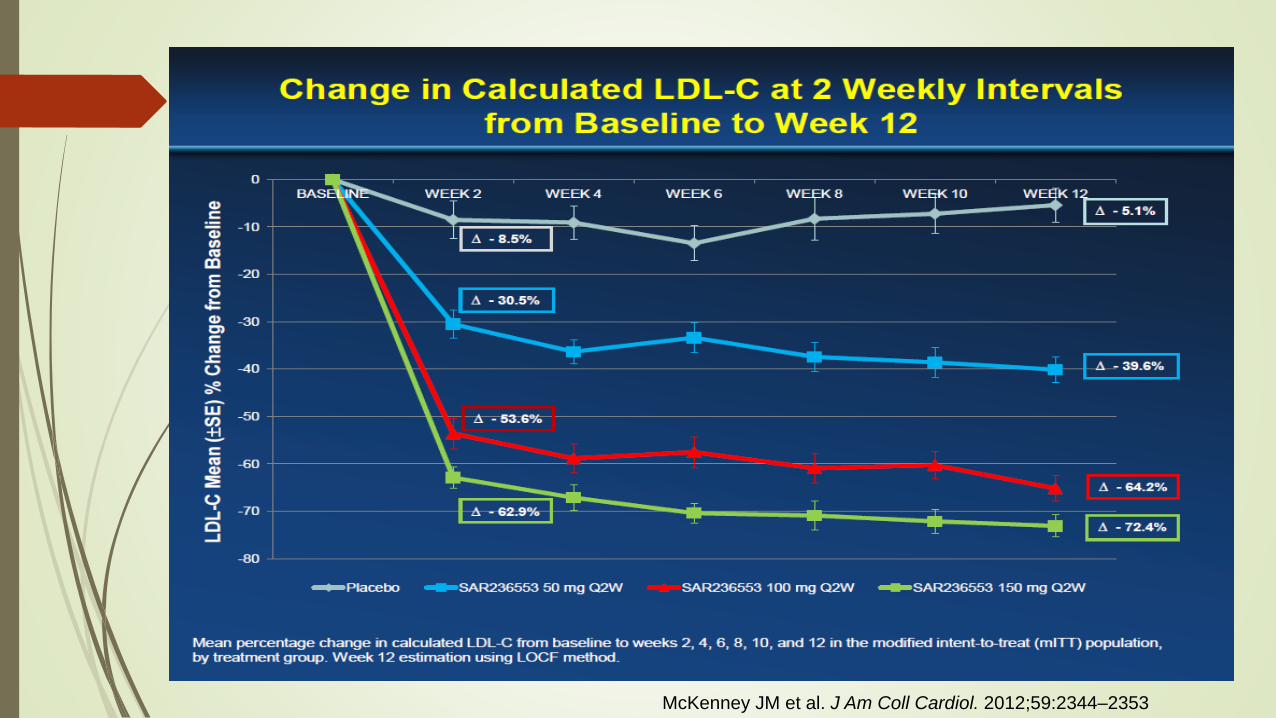
McKenney JM et al. J Am Coll Cardiol. 2012;59:2344–2353
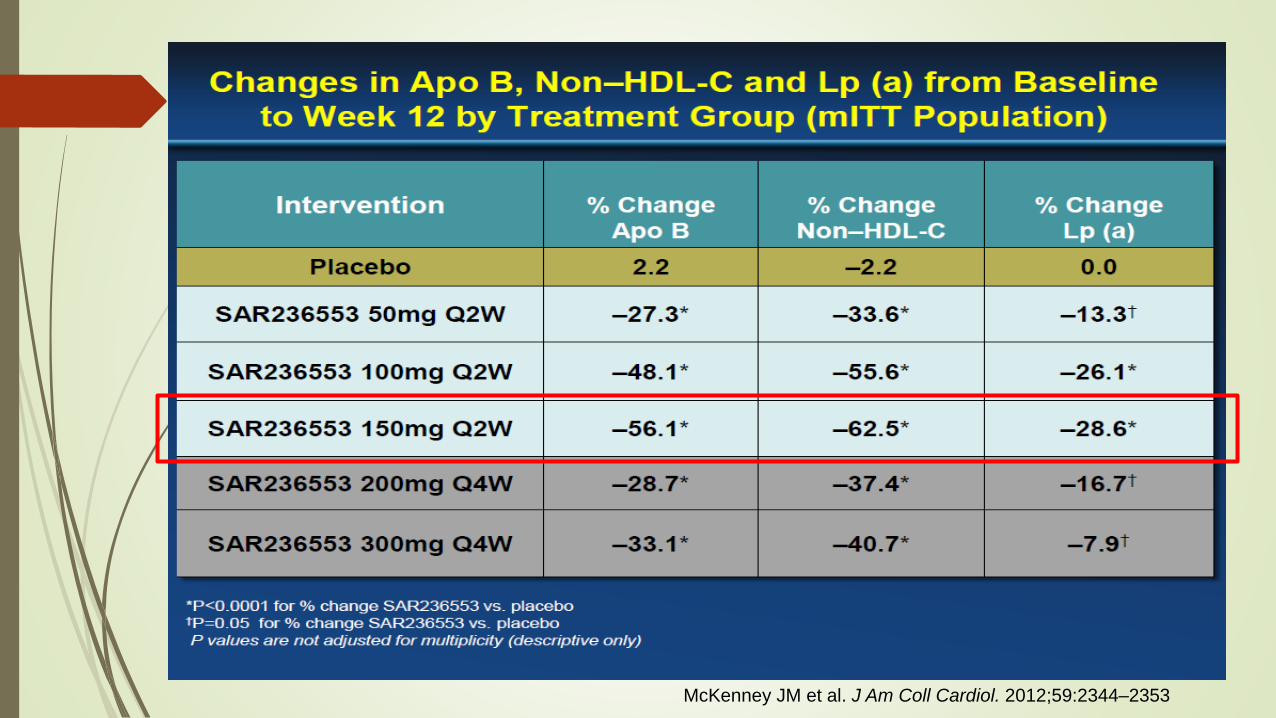
McKenney JM et al. J Am Coll Cardiol. 2012;59:2344–2353
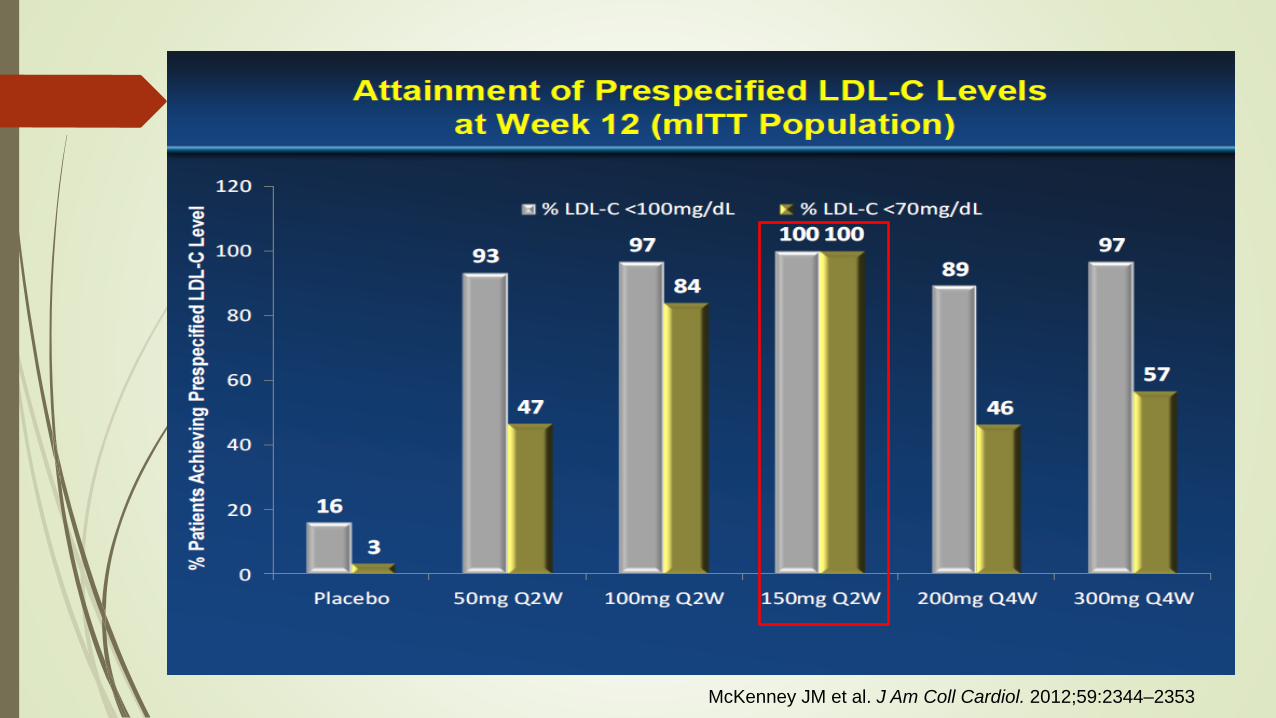
McKenney JM et al. J Am Coll Cardiol. 2012;59:2344–2353
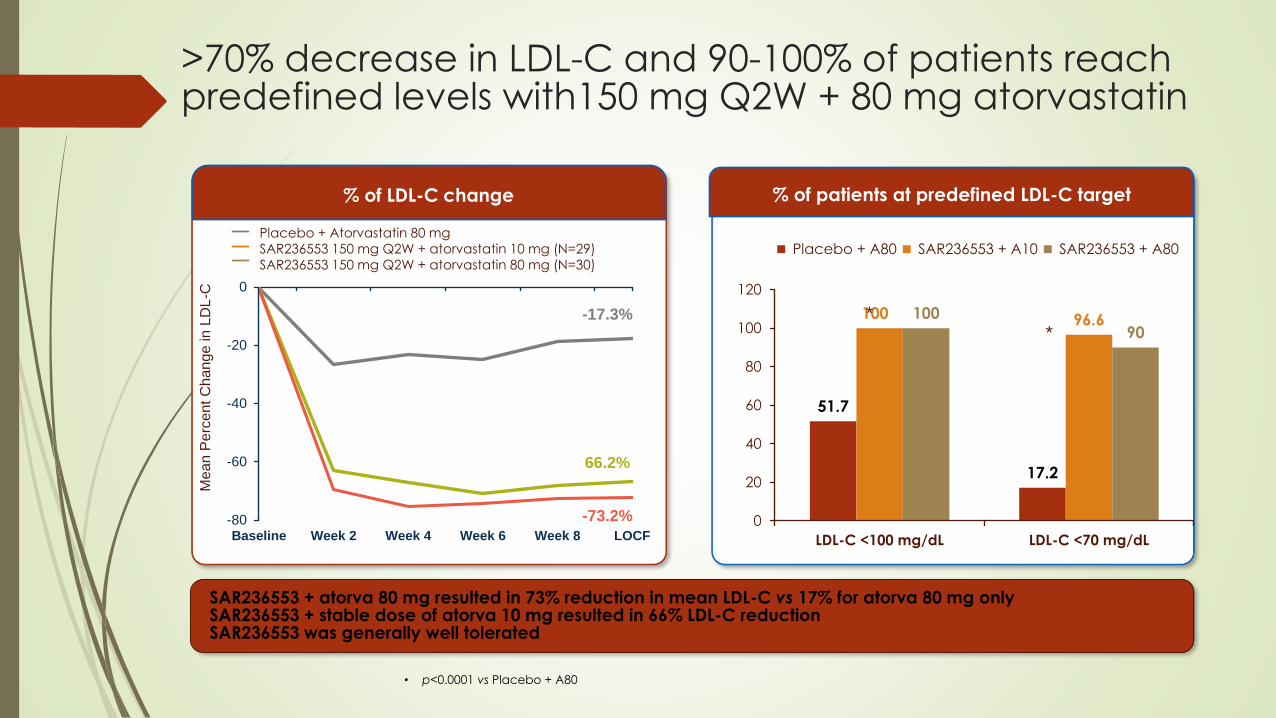
>70% decrease in LDL-C and 90-100% of patients reach predefined levels with150 mg Q2W + 80 mg atorvastatin
SAR236553 + atorva 80 mg resulted in 73% reduction in mean LDL-C vs 17% for atorva 80 mg onlySAR236553 + stable dose of atorva 10 mg resulted in 66% LDL-C reductionSAR236553 was generally well tolerated
% of LDL-C change % of patients at predefined LDL-C target
• p<0.0001 vs Placebo + A80
-80
-60
-40
-20
0
Baseline Week 2 Week 4 Week 6 Week 8 LOCF
-17.3%
66.2%
-73.2%
Placebo + Atorvastatin 80 mg
SAR236553 150 mg Q2W + atorvastatin 10 mg (N=29)
SAR236553 150 mg Q2W + atorvastatin 80 mg (N=30)
Mean P
erc
ent C
han
ge in
LD
L-C
51.7
17.2
100 96.6100
90
0
20
40
60
80
100
120
LDL-C <100 mg/dL LDL-C <70 mg/dL
Placebo + A80 SAR236553 + A10 SAR236553 + A80
**
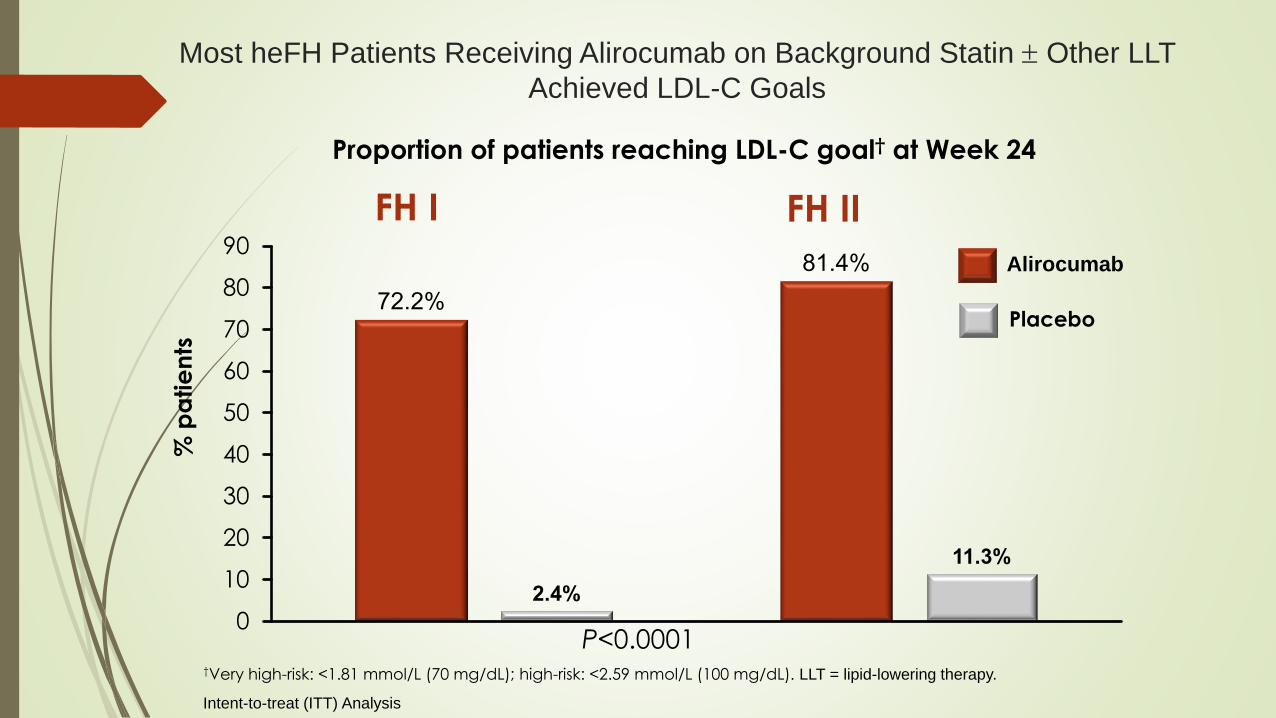
Most heFH Patients Receiving Alirocumab on Background Statin Other LLT
Achieved LDL-C Goals
72.2%
81.4%
2.4%
11.3%
0
10
20
30
40
50
60
70
80
90
P<0.0001
% p
atie
nts
Placebo
†Very high-risk: <1.81 mmol/L (70 mg/dL); high-risk: <2.59 mmol/L (100 mg/dL). LLT = lipid-lowering therapy.
Proportion of patients reaching LDL-C goal† at Week 24
FH I FH II
Alirocumab
Intent-to-treat (ITT) Analysis
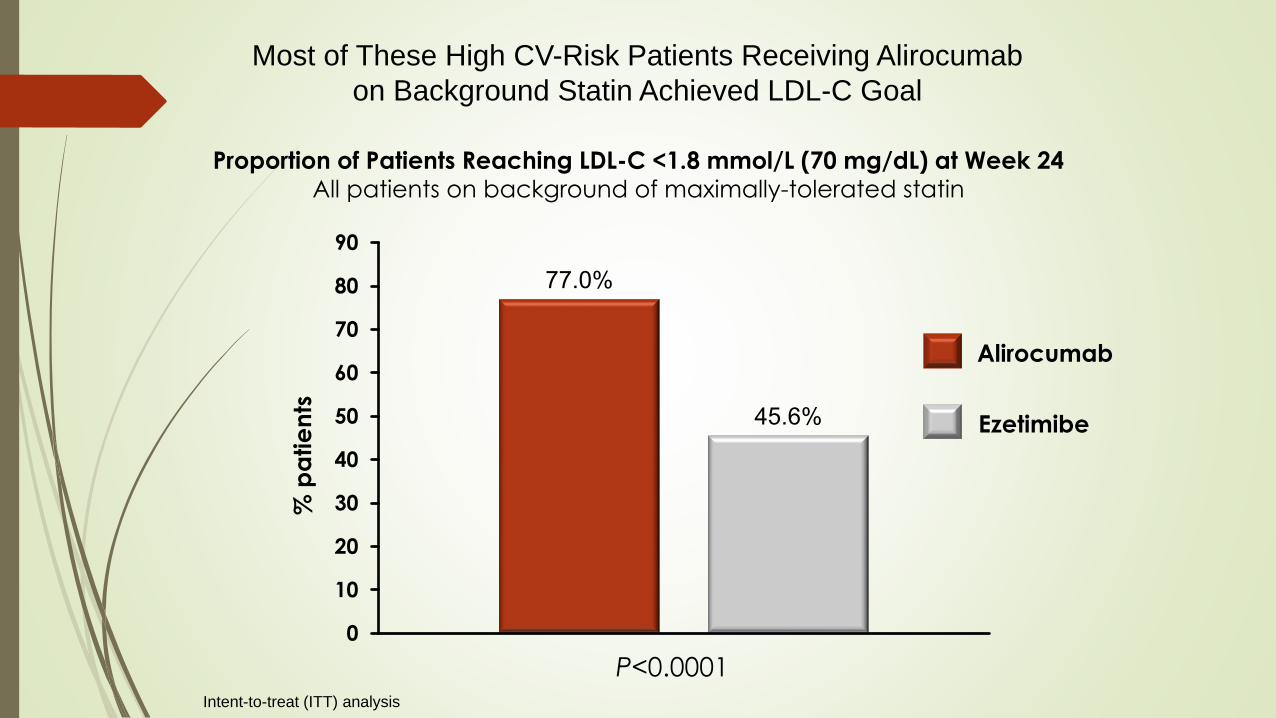
Most of These High CV-Risk Patients Receiving Alirocumab
on Background Statin Achieved LDL-C Goal
Proportion of Patients Reaching LDL-C <1.8 mmol/L (70 mg/dL) at Week 24All patients on background of maximally-tolerated statin
% p
atie
nts
77.0%
45.6%
0
10
20
30
40
50
60
70
80
90
P<0.0001Intent-to-treat (ITT) analysis
Ezetimibe
Alirocumab
Who Needs Benefit?
Very High LDL-C levels FH
Insufficient effects from statins
Statin side effects
Progression of Atherosclerosis
Alirocumab in Patients with Heterozygous
Familial Hypercholesterolemia Undergoing
Lipoprotein Apheresis: the ODYSSEY
ESCAPE Trial
Patrick M. Moriarty,1† Klaus G. Parhofer,2† Stephan P. Babirak,3 Marc-Andre Cornier,4
P. Barton Duell,5 Bernd Hohenstein,6 Josef Leebmann,7 Wolfgang Ramlow,8 Volker
Schettler,9 Vinaya Simha,10 Elisabeth Steinhagen-Thiessen,11 Paul D. Thompson,12
Anja Vogt,13 Berndt von Stritzky,14 Yunling Du,15 Garen Manvelian16
1Department of Internal Medicine, Division of Clinical Pharmacology, University of Kansas Medical Center, Kansas City, KS, USA; 2Medical Department II - Grosshadern, University of Munich, Munich, Germany; 3Metabolic Leader, LLC, Scarborough, MA, USA; 4Division
of Endocrinology, Metabolism, and Diabetes, Anschutz Health and Wellness Centre, Anschutz Medical Campus, Aurora, CO, USA; 5Knight Cardiovascular Institute, Oregon Health & Science University, Portland, OR, USA; 6Extracorporeal Treatment and Lipoprotein
Apheresis Center, Department of Internal Medicine III, University Hospital Carl Gustav Carus, Technische Universität Dresden, Dresden,
Germany; 7Apherese Zentrum Passau, Passau, Germany; 8Apheresis Center Rostock, Rostock, Germany; 9Apheresis centre,
Nehologisches Zentrum Göttingen GbR, Göttingen, Germany; 10Mayo Clinic, Rochester, MN, USA; 11Charite, Universitätsmedizin Berlin-
Campus Virchow-Klinikum, Berlin, Germany; 12Cardiology, Hartford Hospital, Hartford, CT, USA; 13Medizinische Klinik und Poliklinik IV,
LMU Klinikum der Universität München, Munich, Germany; 14Medical Department, Sanofi-Aventis Deutschland GmbH, Berlin, Germany; 15Regeneron Pharmaceuticals, Inc., Basking Ridge, NJ, USA; 16Regeneron Pharmaceuticals, Inc., Tarrytown, NY, USA
This study was funded by Sanofi and Regeneron Pharmaceuticals, Inc.†These joint authors contributed equally to this manuscript
Moriarty PM et al. Eur Heart J. 2016 (in press).
Key Inclusion Criteria
Diagnosis of HeFH by genotyping or clinical criteria (Simon Broome criteria or the WHO/Dutch
Lipid Network criteria)
Stable lipoprotein apheresis QW for ≥4 weeks or Q2W for ≥8 weeks
Background LLT, diet and exercise level stable for ≥8 weeks
Lipoprotein apheresis techniques: double membrane filtration, immunoadsorption, heparin-
induced LDL precipitation, direct adsorption of lipids, dextran sulfate adsorption (plasma) and
dextran sulfate adsorption (whole blood)
Key Exclusion Criteria
Diagnosis of homozygous FH
Lipoprotein apheresis schedule other than QW and Q2W
Key Inclusion and Exclusion Criteria
2
5
Moriarty PM et al. Eur Heart J. 2016 (in press).
WHO, World Health Oranisation.

Pre-apheresis LDL-C Over Time
Raw mean values are provided for baseline. SE, standard error.
26
Moriarty PM et al. Eur Heart J. 2016 (in press).
0
20
40
60
80
100
120
140
160
180
200
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
5.5
0 2 4 6 8 10 12 14 16 18
mg
/dL
Ave
rag
e L
DL
-C v
alu
e
(pre
-ap
here
sis
), m
ea
n (
SE
), m
mo
l/L
Week
Alirocumab 150 mg Q2W (n=41)
Placebo (n=21)
Apheresis rate varied from Week 7 onwards
192
mg/dL
175
mg/dL
185
mg/dL
90
mg/dL
110
mg/dL
191
mg/dL
LDL-C % change from baseline, LS mean (SE), %:
Week 6
Week 18
Alirocumab
-53.7 (2.3)
-42.5 (4.7)
Placebo
1.6 (3.1)
3.9 (6.3)
p-value versus placebo
<0.0001
<0.0001
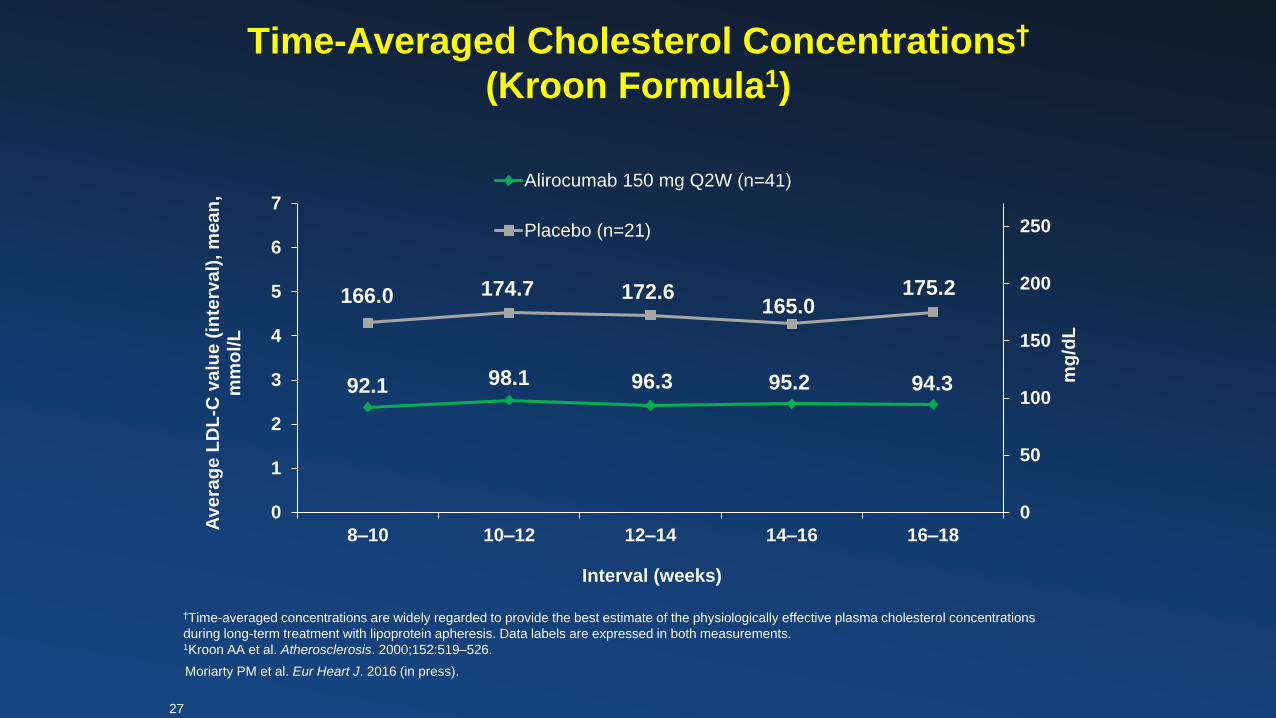
Time-Averaged Cholesterol Concentrations†
(Kroon Formula1)
†Time-averaged concentrations are widely regarded to provide the best estimate of the physiologically effective plasma cholesterol concentrations
during long-term treatment with lipoprotein apheresis. Data labels are expressed in both measurements.1Kroon AA et al. Atherosclerosis. 2000;152:519–526.
0
50
100
150
200
250
0
1
2
3
4
5
6
7
8–10 10–12 12–14 14–16 16–18
mg
/dL
Ave
rag
e L
DL
-C v
alu
e (
inte
rva
l), m
ea
n,
mm
ol/L
Interval (weeks)
Alirocumab 150 mg Q2W (n=41)
Placebo (n=21)
Moriarty PM et al. Eur Heart J. 2016 (in press).
27
166.0 174.7 172.6165.0
175.2
94.395.296.398.192.1
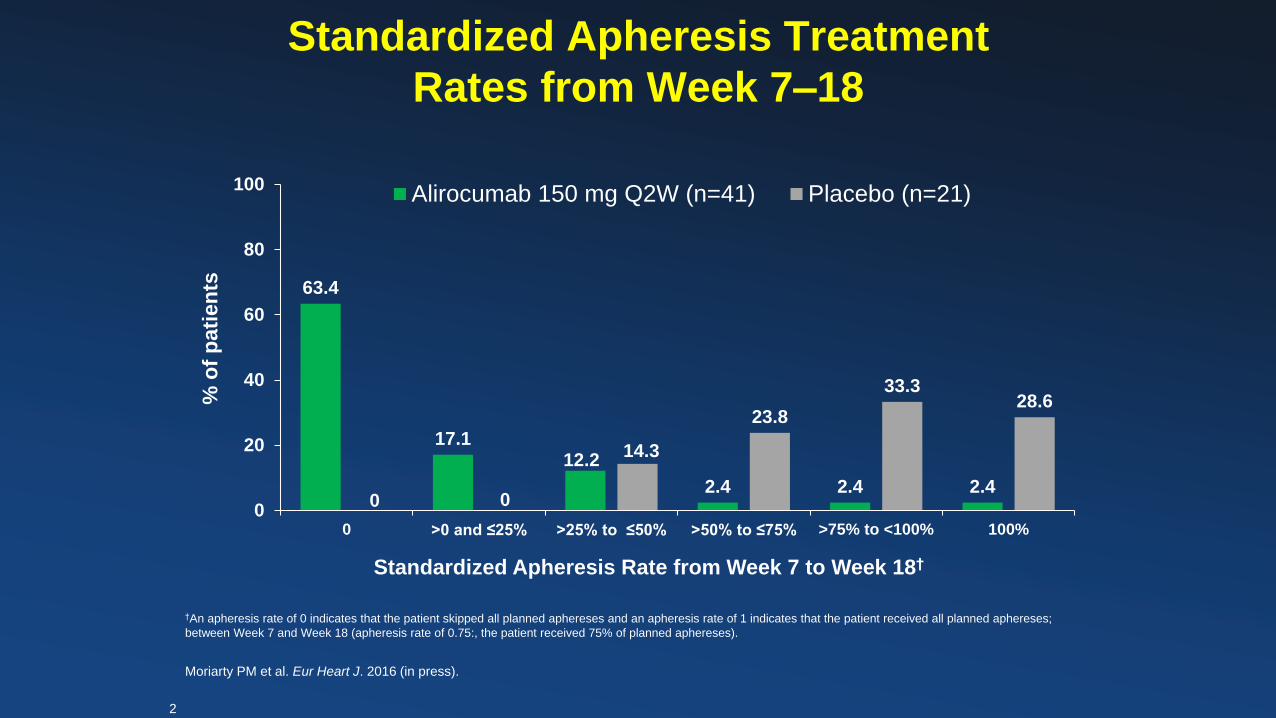
Standardized Apheresis Treatment
Rates from Week 7–18
63.4
17.112.2
2.4 2.4 2.40 0
14.3
23.8
33.328.6
0
20
40
60
80
100
0 >0 and ≤25% >25% to ≤50% >50% to ≤75% >75% to <100% 100%
% o
f p
ati
en
ts
Standardized Apheresis Rate from Week 7 to Week 18†
Alirocumab 150 mg Q2W (n=41) Placebo (n=21)
†An apheresis rate of 0 indicates that the patient skipped all planned aphereses and an apheresis rate of 1 indicates that the patient received all planned aphereses;
between Week 7 and Week 18 (apheresis rate of 0.75:, the patient received 75% of planned aphereses).
Moriarty PM et al. Eur Heart J. 2016 (in press).
2
8
Sabatine MS, et al. N Engl J Med. 2017 Mar 17. [Epub ahead of print]
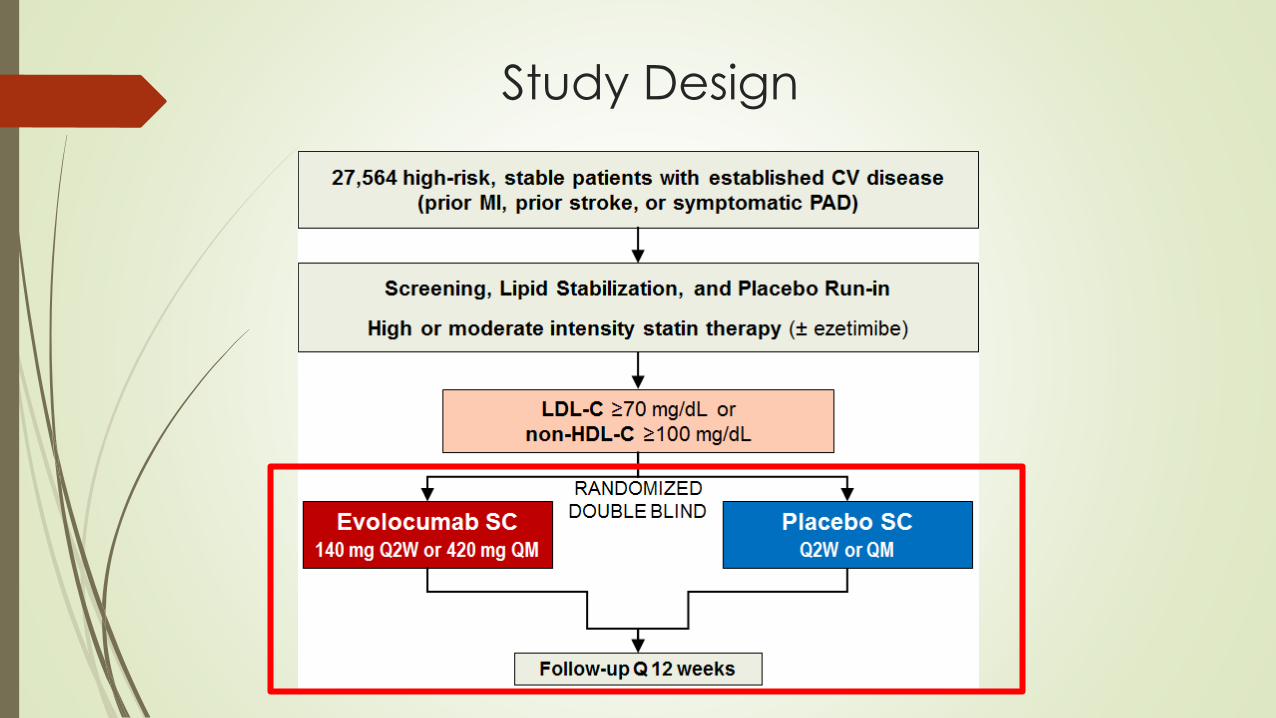
Study Design
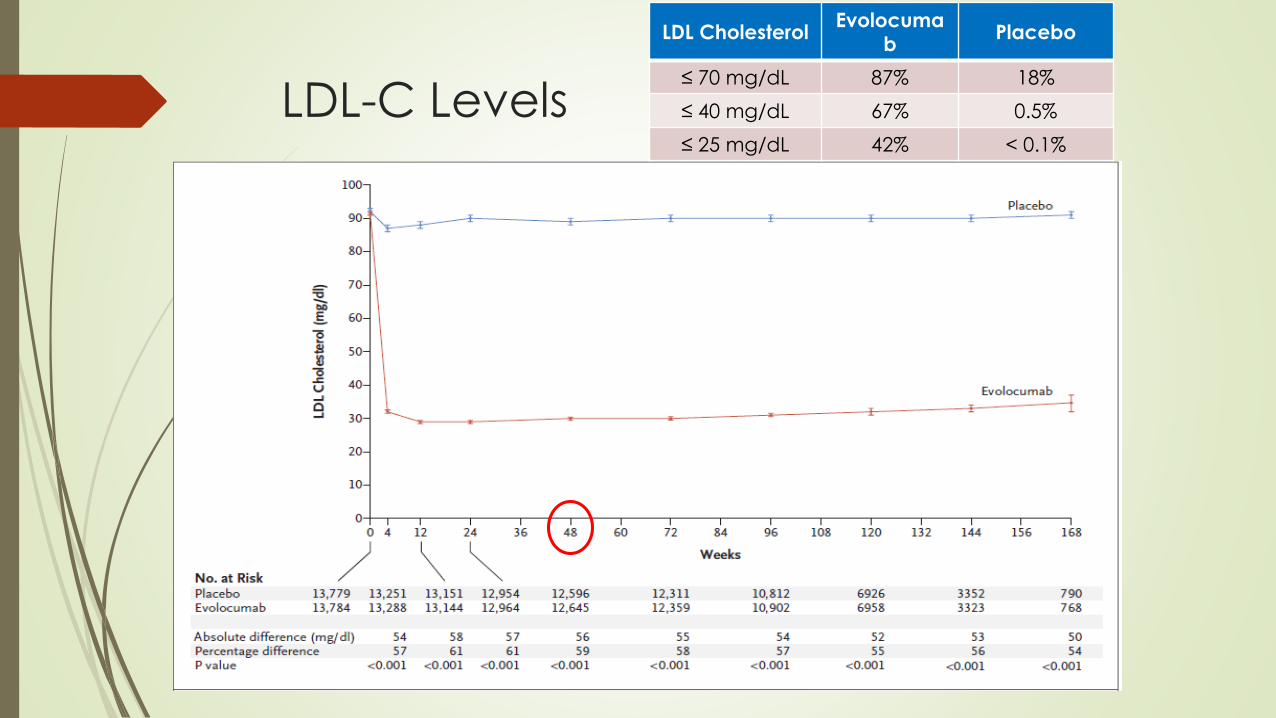
LDL-C Levels
LDL CholesterolEvolocuma
bPlacebo
≤ 70 mg/dL 87% 18%
≤ 40 mg/dL 67% 0.5%
≤ 25 mg/dL 42% < 0.1%
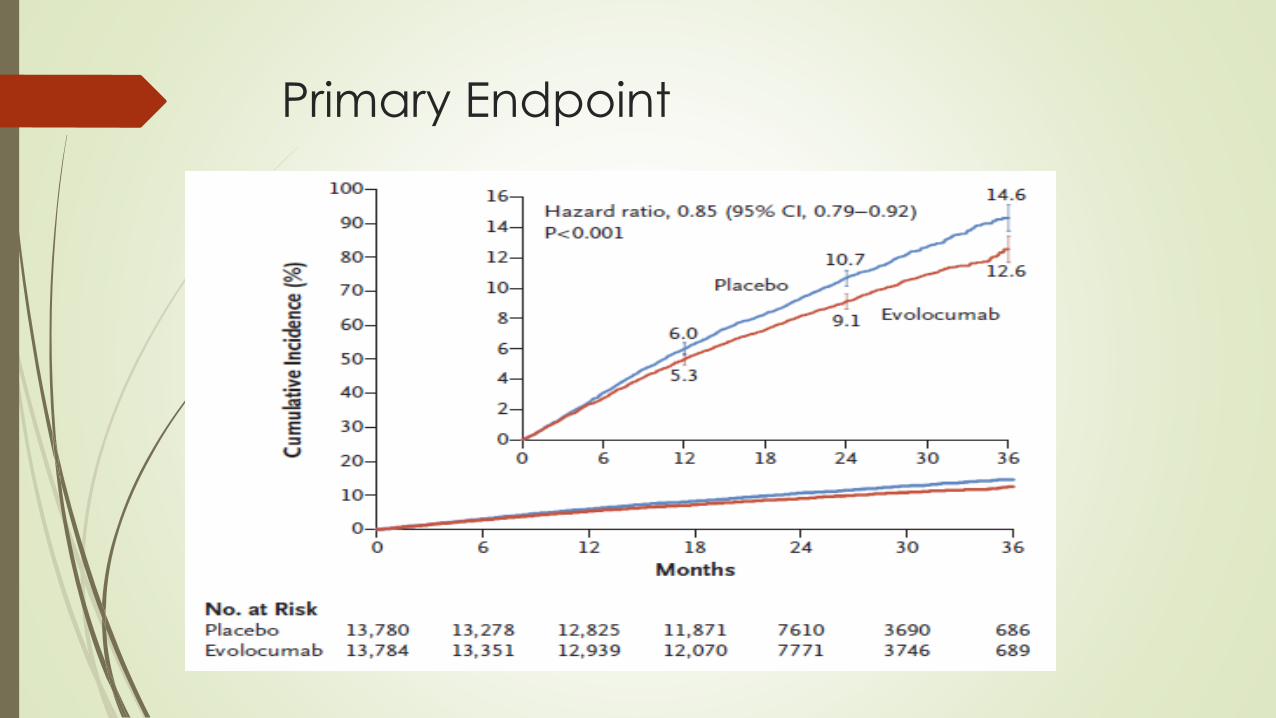
Primary Endpoint
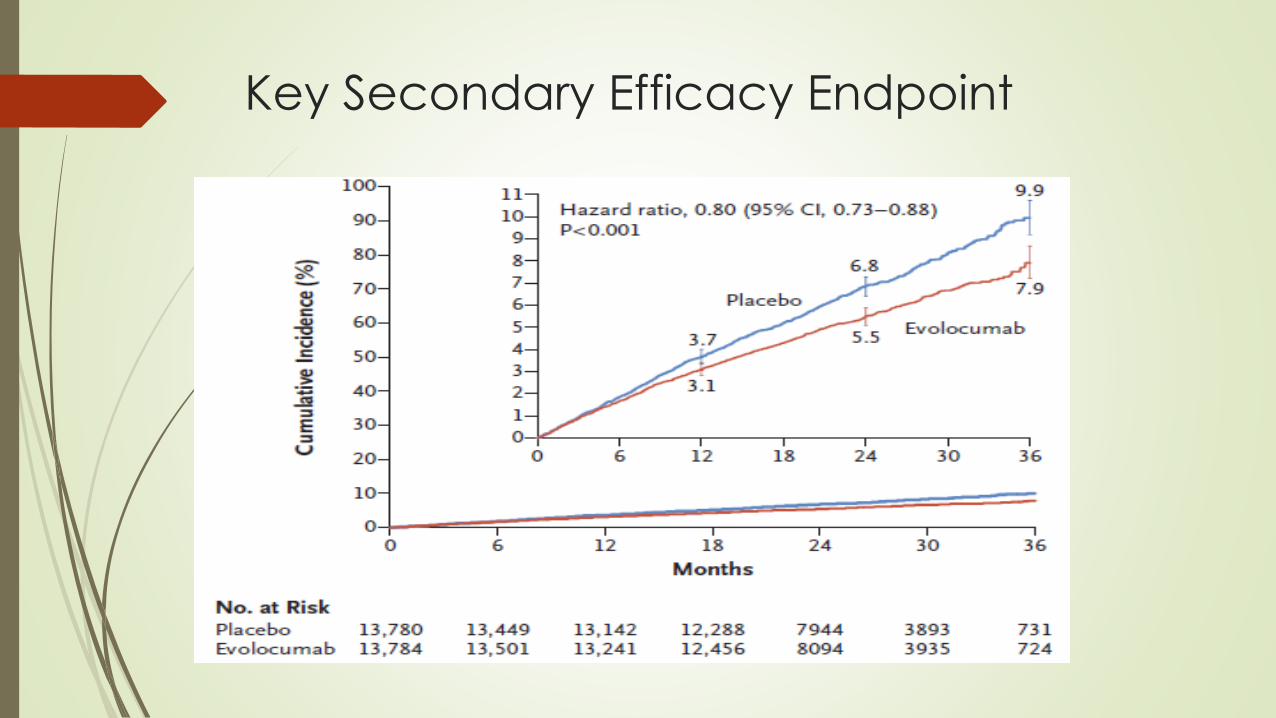
Key Secondary Efficacy Endpoint
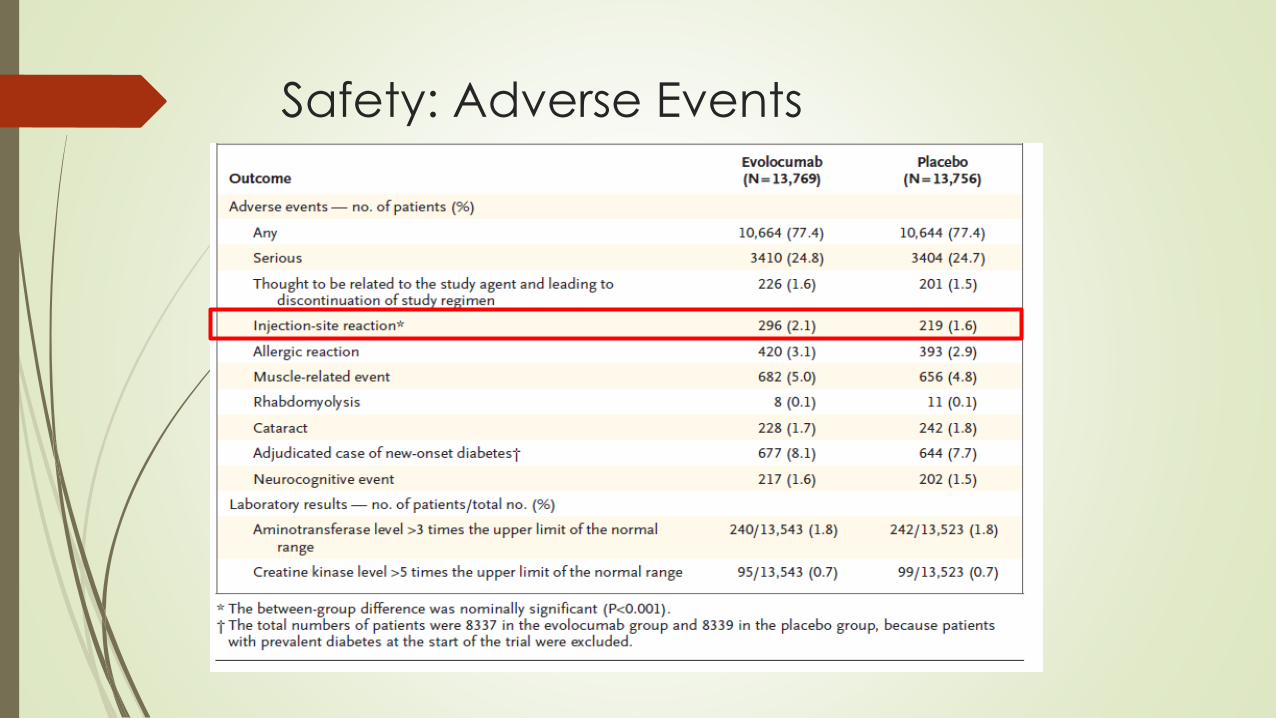
Safety: Adverse Events
Study Conclusions
When added to statin therapy, evolocumab lowered LDL
cholesterol levels by 59% from baseline compared to placebo,
from a median of 92 mg/dL to 30 mg/dL
risk of the primary composite endpoint by 15% and risk of
the key secondary endpoint by 20%
Magnitude of risk reduction shown to increase over time
No effect of additional LDL-C lowering on cardiovascular death
or all-cause mortality
Injection-site reactions were significantly higher in the
evolocumab group compared to the placebo group
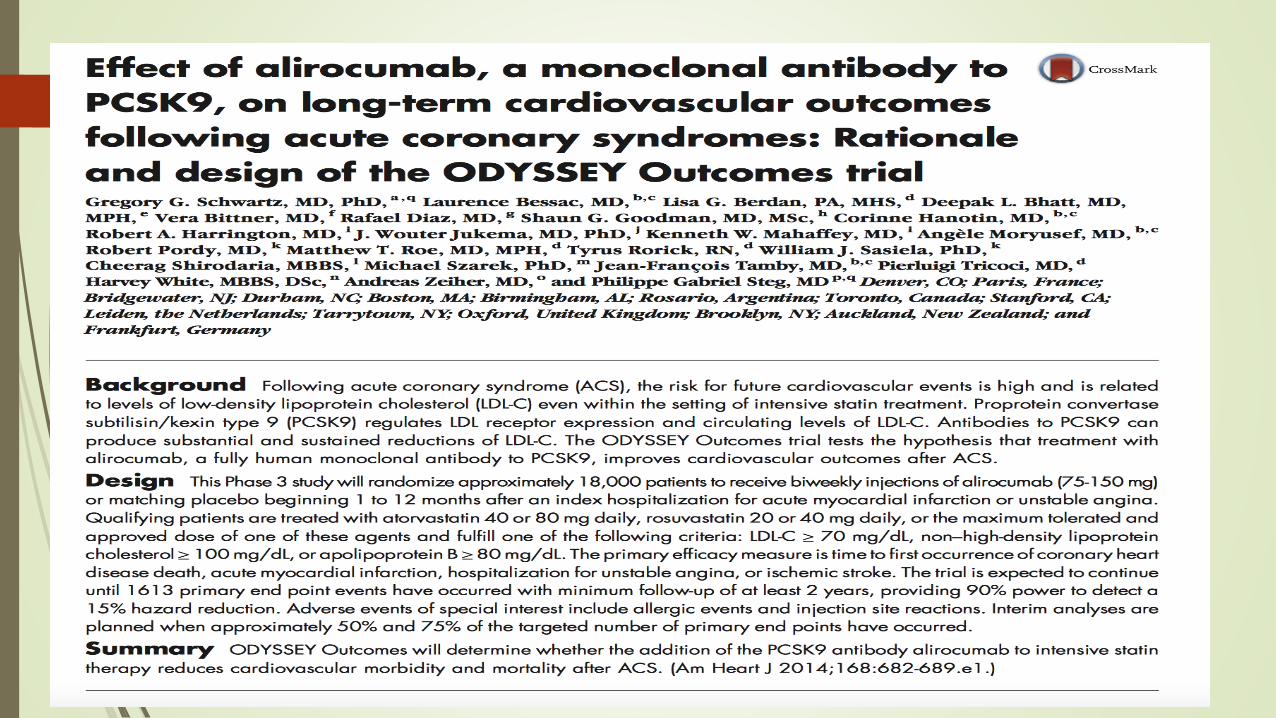
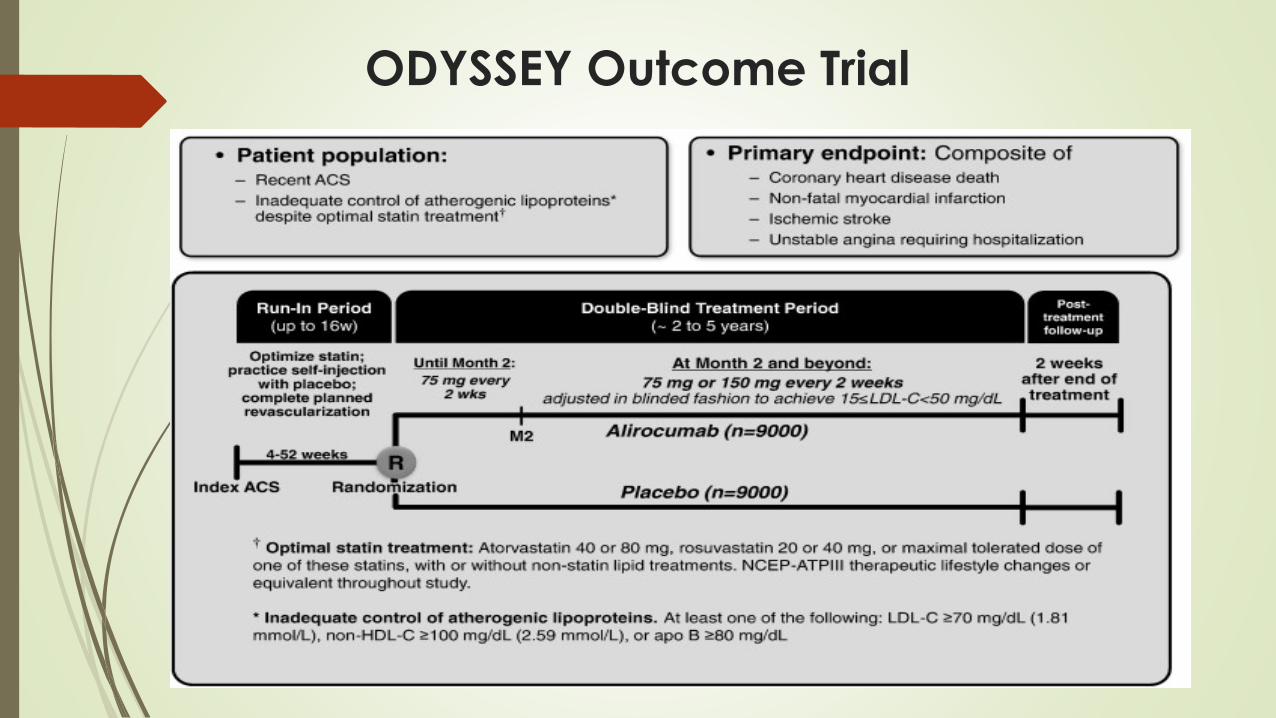
ODYSSEY Outcome Trial
Recommended Use of PCSK9I’s
Based on current guidelines, available evidence, and economic
considerations:
Patients with FH or ASCVD and statin resistance (on max dose) for
additional LDL lowering is a reasonable strategy.
Discuss with patient costs vs clinical benefit
In FH patients to avoid apheresis
2nd line to addition of ezetimibe for statin intolerant patients
No evidence to support use of PCSK9I’s as monotherapy or for arbitrary
reduction of statin dose
In complete statin intolerance, PCSK9I monotherapy should be
considered only after careful risk assessment and patient preference

Questions ?
39