treatment with olaparib monotherapy in the -...
TRANSCRIPT


Eric Pujade-Lauraine,1 Jonathan A Ledermann,2 Richard T Penson,3 Amit M Oza,4 Jacob Korach,5
Tomasz Huzarski,6 Andrés Poveda,7 Sandro Pignata,8 Michael Friedlander,9 and Nicoletta Colombo10
1Université Paris Descartes, AP-HP, Paris, France; 2University College London, London, UK; 3Massachusetts General Hospital and
Harvard University, Boston, USA; 4Princess Margaret Cancer Centre, Toronto, Canada; 5Sheba Medical Center, Tel Aviv University,
Tel Hashomer, Israel; 6Pomeranian Medical University, Szczecin, Poland; 7Instituto Valenciano de Oncología, Valencia, Spain; 8Istituto
Tumori Pascale di Napoli, Naples, Italy; 9University of New South Wales Clinical School, Prince of Wales Hospital, Randwick, Australia; 10University of Milan-Bicocca and Istituto Europeo Oncología (IEO), Milan, Italy
Funded by AstraZeneca; ClinicalTrials.gov number NCT01874353
Treatment with olaparib monotherapy in the
maintenance setting significantly improves
progression-free survival in patients with
platinum-sensitive relapsed ovarian cancer:
Results from the Phase III SOLO2 study

Verbal disclosure
• Eric Pujade-Lauraine reports advisory board membership and honoraria from AstraZeneca, and advisory board membership,
honoraria, and speaker’s bureau membership from Roche
• Jonathan A Ledermann reports honoraria from AstraZeneca, honoraria from Pfizer, and advisory roles from AstraZeneca,
Clovis Oncology, Pfizer, and Roche
• Richard T Penson reports honoraria, a consulting and advisory role, and receipt of research funding from AstraZeneca
• Amit M Oza reports a non-compensated advisory role and investigator role for AstraZeneca, Clovis Oncology, Tesaro, and
Pfizer
• Jacob Korach reports no disclosures
• Tomasz Huzarski reports no disclosures
• Andrés Poveda reports consulting and advisory roles from Advaxis, AstraZeneca, PharmaMar, and Roche
• Sandro Pignata reports honoraria from AstraZeneca, Roche, and PharmaMar
• Michael Friedlander reports honoraria and advisory roles from AstraZeneca, and Pfizer
• Nicoletta Colombo reports honoraria and advisory roles from AstraZeneca, Pfizer, Clovis Oncology, Roche, PharmaMar, and
Immunogen
AcknowledgmentsThe 295 patients and their families, and…
IDMC
R Ozols, J Vermorken
M Buyse
QoL Committee
E Pujade-Lauraine, F Hilpert,
M Friedlander, L Wenzel, E Lowe,
F Joly, V Gebsky, S Garnett, N Le Fur,
D Eek, R Bloomfield, T Morris,
A Fielding
Trial Steering Committee
E Pujade-Lauraine, P Harter, A Poveda,
R Penson, M Friedlander, G Sonke, N Colombo,
S Pignata, A Oza, K Fujiwara, G Girotto,
J Ledermann, I Vergote, J Korach, J-W Kim,
O Mikheeva, V Gebsky, E Lowe, A Fielding,
R Bloomfield
Study Sponsor:
AstraZeneca
P Pautier N Colombo A Clamp R Penson A Oza J Korach T Huzarski A Poveda Velasco
M Roigues S Pignata C Parkinson J Cosin D Ovencher A Amit M Sikorska A Prat Aparicio
J-P Lotz G Scambia J Ledermann R Penson M Plante L Helpman A Słowińska N Laínez Milagro
I Ray-Coquard M Nicoletto S Williams D O'Malley A Covens M Bidziński MP Barretina Ginesta
J Ioni R Sabbatini S Banerjee P Timmins H Hirte M Miedzińska A Tibau Martorell
C Dubot F Cognetti C Poole D Warshal S Welch A Casado Herraez
M-C Kaminsky E Dickson-Michelson P Bessette C Mendiola Fernández
A Lortholary N McKenzie MJ Rubio Pérez
F Joly G Roiguez JA Pérez Fidalgo
A Floquet D Armstrong
L Gladieff E Chalas
S Hamizi P Celano
K Behbakht
C Leath III
J Chan
MA Crispens
Australia Japan Germany Russia Netherlands South Korea Brazil Belgium
M Friedlander P Harter K Tamura A Lisyanskaya G Sonke J-H Kim E Filho I Vergote
C Scott T-W Park-Simon K Matsumoto S Tjulandin I Boere J-H Nam R Hegg H Denys
A Linda Mileshkin M Gropp-Meier M Mandai O Mikheeva P Ottevanger C-H Choi L Costa
A El-Balat T Saito R Lalisang J-W Kim G Queiroz
S Rothe K Takehara F Franke
T Reimer T Enomoto R Pereira
B Schmalfeldt H Watari G Borges
L Hanker Y Hirashima
F Thiel K Fujiwara
ARCAGYB Voltan, N Le Fur

Background
1. Ledermann JA et al 2012; 2. Ledermann JA et al 2014
• Olaparib is the first-in-class PARP inhibitor
• In a Phase II trial (Study 19), olaparib maintenance therapy (capsules) provided a
significant progression-free survival (PFS) improvement over placebo in all-comer
patients with platinum-sensitive, relapsed, high-grade serous ovarian cancer1
– The PFS benefit was greatest for patients with a BRCA1/2 mutation2
• SOLO2/ENGOT-Ov21 (NCT01874353) was a Phase III trial to confirm findings from
Study 19 in the BRCA1/2 mutation subgroup using the olaparib tablet formulation
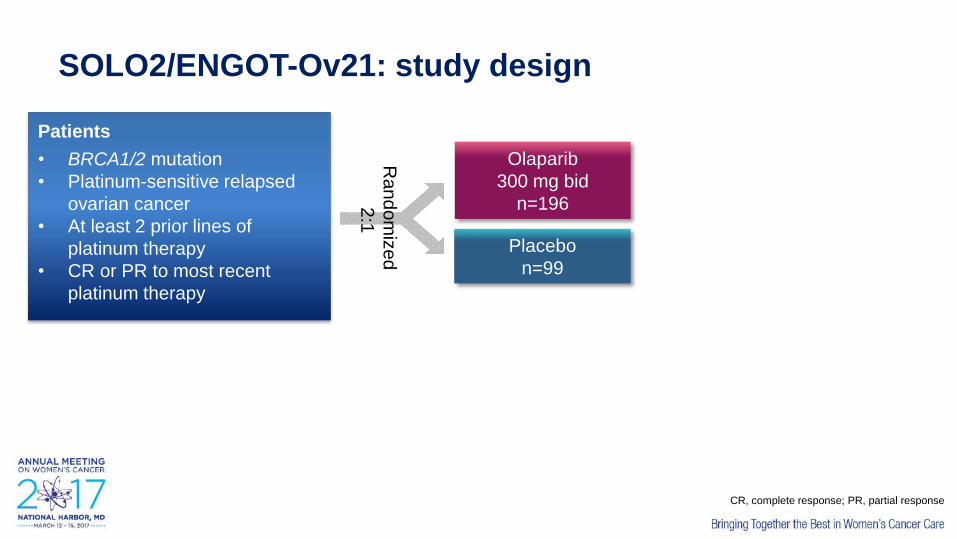
SOLO2/ENGOT-Ov21: study design
Placebo
n=99
Olaparib
300 mg bid
n=196
Patients
• BRCA1/2 mutation
• Platinum-sensitive relapsed
ovarian cancer
• At least 2 prior lines of
platinum therapy
• CR or PR to most recent
platinum therapy
Ra
nd
om
ize
d
2:1
CR, complete response; PR, partial response

SOLO2/ENGOT-Ov21: study design
Placebo
n=99
Olaparib
300 mg bid
n=196Primary endpoint
Investigator-assessed
PFS
Patients
• BRCA1/2 mutation
• Platinum-sensitive relapsed
ovarian cancer
• At least 2 prior lines of
platinum therapy
• CR or PR to most recent
platinum therapy
Ra
nd
om
ize
d
2:1
CR, complete response; PR, partial response

*Primary endpoint for HRQoL was trial outcome index (TOI) of the
FACT-O (Functional Assessment of Cancer Therapy – Ovarian)
Sensitivity analysis: PFS by blinded independent central review (BICR)
• Key secondary endpoints:– Time to first subsequent therapy or death (TFST), time to second progression (PFS2),
time to second subsequent therapy or death (TSST), overall survival (OS)
– Safety, health-related quality of life (HRQoL*)
SOLO2/ENGOT-Ov21: study design
Placebo
n=99
Olaparib
300 mg bid
n=196Primary endpoint
Investigator-assessed
PFS
Patients
• BRCA1/2 mutation
• Platinum-sensitive relapsed
ovarian cancer
• At least 2 prior lines of
platinum therapy
• CR or PR to most recent
platinum therapy
Ra
nd
om
ize
d
2:1

CharacteristicOlaparib
(n=196)
Placebo
(n=99)
Age, median (range) 56 (28–83) 56 (39–78)
Primary tumor type, n (%)
Ovarian 162 (82.7) 86 (86.9)
Fallopian tube or primary peritoneal 31 (15.8) 13 (13.1)
Other/missing 3 (1.5) 0
Prior platinum regimens, n (%)
2 lines 110 (56.1) 62 (62.6)
3 lines 60 (30.6) 20 (20.2)
≥4 lines 25 (12.8) 17 (17.2)
Platinum-free interval, n (%)6–12 months 79 (40.3) 40 (40.4)
>12 months 117 (59.7) 59 (59.6)
Response to platinum therapy, n (%)Complete response 91 (46.4) 47 (47.5)
Partial response 105 (53.6) 52 (52.5)
Demographic and baseline characteristics

No. at risk
Olaparib
Placebo196
99
182
70
156
37
134
22
118
18
104
17
89
14
82
12
32
7
29
6
3
0
2
0
0
0
100
90
80
70
60
50
40
30
20
10
0
Pro
gre
ssio
n-f
ree
su
rviv
al (%
)
Months since randomization
0 3 6 9 12 15 18 21 24 27 30 33 36
19.1
Olaparib
Placebo
5.5
Olaparib
(n=196)
Placebo
(n=99)
Events (%) 107 (54.6) 80 (80.8)
Median PFS, months 19.1 5.5
HR 0.30
95% CI 0.22 to 0.41
P<0.0001
PFS by investigator assessment
Median follow-up was 22.1 months in the olaparib group and 22.2 months for placebo

Months since randomization
Pro
gre
ssio
n-f
ree
su
rviv
al (%
)100
90
80
70
60
50
40
30
20
10
00 3 6 9 12 15 18 21 24 27 33
30.25.5
30
No. at risk
Olaparib
Placebo
196
99
176
62
148
26
128
18
112
16
103
14
88
14
82
11
30
6
28
5
3
0
1
0
Olaparib
(n=196)
Placebo
(n=99)
Events (%) 81 (41.3) 70 (70.7)
Median PFS, months 30.2 5.5
HR 0.25
95% CI 0.18 to 0.35
P<0.0001
PFS sensitivity analysis using BICR
Olaparib
Placebo

Secondary efficacy endpoints
27.9
7.1
18.4
Not reached
18.2
PFS2
0 10 20 30Median (months)
Olaparib
PlaceboData immatureOverall survival
Time to first
subsequent therapy,
or death (TFST)
Time to second
subsequent therapy,
or death (TSST)
HR 0.28
95% CI 0.21 to 0.38
P<0.0001
HR 0.50
95% CI 0.34 to 0.72
P=0.0002
HR 0.37
95% CI 0.26 to 0.53
P<0.0001
Median not reached
Median not reached

Characteristic, n (%)Olaparib
(n=195)
Placebo
(n=99)
Any AE 192 (98.5) 94 (94.9)
Any AE grade ≥3 72 (36.9) 18 (18.2)
Any SAE 35 (17.9) 8 (8.1)
Any AE leading to dose reduction 49 (25.1) 3 (3.0)
Any AE leading to discontinuation of study treatment 21 (10.8) 2 (2.0)
Any AE with an outcome of death 1 (0.5) 0
Total adverse events
AE, adverse event; SAE, serious adverse event

Most common hematologic adverse events
Event, n (%) Olaparib (n=195) Placebo (n=99)
All grades Grade ≥3 All grades Grade ≥3
Anemia* 85 (43.6) 38 (19.5) 8 (8.1) 2 (2.0)
Neutropenia* 38 (19.5) 10 (5.1) 6 (6.1) 4 (4.0)
Thrombocytopenia 16 (8.2) 0 3 (3.0) 1 (1.0)
MDS/AML: 4 cases in olaparib group (2.1%), including one case of CMML
4 cases in placebo group (4.0%)
*Grouped terms

Most common non-hematologic adverse events
All grades (frequency ≥20%)
Olaparib Placebo
100 75 50 25 0 0 25 50 75 100
Adverse events (%)
Dysgeusia 7.126.7
Headache 13.125.1
Decreased appetite 11.122.1
Nausea 33.375.9
Fatigue/asthenia 39.465.6
Vomiting 19.237.4
Constipation 23.220.5
Diarrhea 20.232.8
Abdominal pain 31.324.1
Grade ≥3 (frequency ≥2.5%)
Other AEs of interest
Elevated ALT: 10 patients in olaparib group (5.1%) vs 4 patients in placebo group (4.0%)
Elevated AST: 4 patients in olaparib group (2.1%) vs 4 patients in placebo group (4.0%)
2.6
1.02.6
2.04.1
3.0
1.0
2.6 3.0
0.5

Health-related quality of life: TOI of the FACT-O
TOI over first 12 months Olaparib (n=185) Placebo (n=94)
Change from baseline, adjusted mean −2.90 −2.87
TOI, trial outcome index;
FACT-O, Functional Assessment of Cancer Therapy – Ovarian
Estimated difference in adjusted means = −0.03 (95% CI −2.19 to 2.13, P=0.98)

Conclusions
• SOLO2 demonstrated a statistically significant PFS improvement in patients receiving
olaparib, by investigator assessment and BICR
• The PFS benefit was supported by a significant delay in TFST, PFS2 and TSST in the
olaparib group
• With the exception of anemia, toxicity was mostly low grade
• SOLO2 is the first Phase III trial of olaparib tablets as maintenance treatment and
showed a significant benefit in patients with platinum-sensitive, relapsed ovarian
cancer and a BRCA1/2 mutation

Additional slides

Olaparib better Placebo better
Subgroup analysis of PFSHazard ratio (95% CI)Subgroup

No. at risk
Olaparib
Placebo
196
99182
78
156
44
139
26
122
22
110
19
100
17
93
14
60
9
37
6
16
2
4
0
TDT: time to treatment discontinuation, or death
100
90
70
60
50
40
30
20
10
0
Pro
po
rtio
n o
f p
atie
nts
eve
nt
fre
e (
%)
Months since randomization
0 3 6 9 12 15 18 21 24 27 30 33
80
5.6 19.4
Olaparib
Placebo
Olaparib
(n=196)
Placebo
(n=99)
Events (%) 112 (57.1) 86 (86.9)
Median PFS, months 19.4 5.6
HR 0.31
95% CI 0.23 to 0.42
P<0.0001

TFST: time to first subsequent therapy, or death
Months since randomizationNo. at risk
Olaparib
Placebo196
99
190
92
176
65
155
33
139
26
130
23
122
20
107
19
64
11
40
6
16
2
4
0
100
90
80
70
60
50
40
30
20
10
0
No
t o
n f
irst su
bse
qu
en
t th
era
py (
%)
0 3 6 9 12 15 18 21 24 27 30 33
27.97.1
Olaparib
Placebo
Olaparib
(n=196)
Placebo
(n=99)
Events (%) 92 (46.9) 79 (79.8)
Median PFS, months 27.9 7.1
HR 0.28
95% CI 0.21 to 0.38
P<0.0001

PFS2: time to second progression, or death
Months since randomizationNo. at risk
Olaparib
Placebo
196
99
191
95
180
84
167
71
152
59
132
47
114
38
100
28
39
13
30
7
3
0
2
0
Pro
gre
ssio
n-f
ree
su
rviv
al 2
(%
)
Olaparib
Placebo
18.4
100
90
80
70
60
50
40
30
20
10
0
0 3 6 9 12 15 18 21 24 27 30 33
18.4
Olaparib
(n=196)
Placebo
(n=99)
Events (%) 70 (35.7) 49 (49.5)
Median PFS, months Not reached 18.4
HR 0.50
95% CI 0.34 to 0.72
P=0.0002

100
90
70
60
50
40
30
20
10
0
0 3 6 9 12 15 18 21 24 27 30 33 36
18.2
80
TSST: time to second subsequent therapy, or death
No
t o
n s
eco
nd
su
bse
qu
en
t th
era
py (
%)
Months since randomizationNo. at risk
Olaparib
Placebo
196
99
194
95
190
90
181
81
169
67
155
51
141
43
123
30
75
17
43
10
17
2
4
0
Months since randomization
Olaparib
(n=196)
Placebo
(n=99)
Events (%) 68 (34.7) 60 (60.6)
Median PFS, months Not reached 18.2
HR 0.37
95% CI 0.26 to 0.53
P<0.0001
0
0
Olaparib
Placebo

Hierarchy of statistical testing
• PFS is tested first using the full alpha. Subsequently, PFS2 is testedonly if PFS is statistically significant
• If PFS2 is significant at either the interim or final analyses, the fullalpha will be carried forward to OS
• Statistical significance will be declared at the interim analysis for PFS2if the one-sided P<0.0125
• Statistical significance will be declared at the interim analysis for OS if
the null hypothesis for PFS2 is rejected at the PFS analysis and the
observed P value for OS is P<0.0001
PFS
PFS2
OS
Multiple testing procedure
Supportive secondary endpoints: TDT, TFST, TSST
TDT, time to treatment discontinuation or death;
TFST, time to first subsequent therapy or death;
TSST, time to second subsequent therapy or death
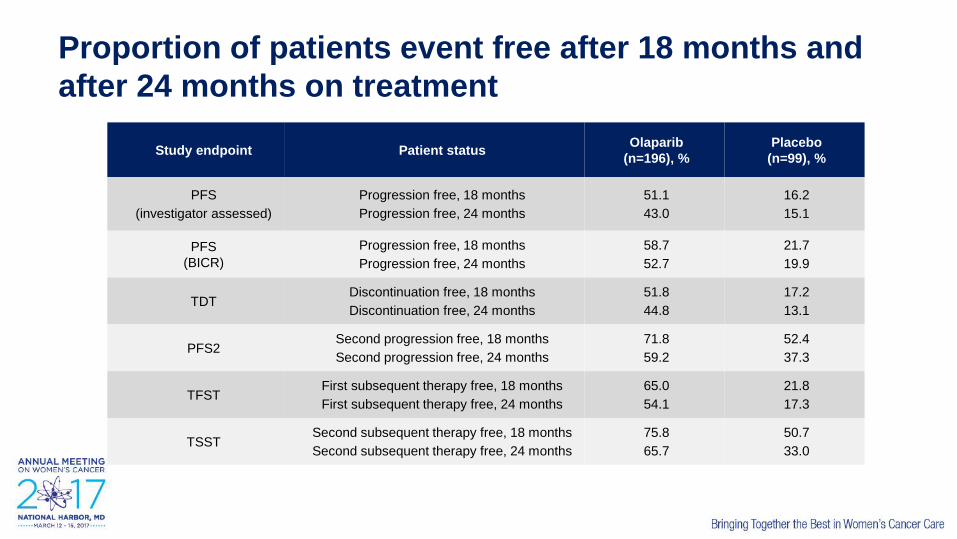
Proportion of patients event free after 18 months and
after 24 months on treatment
Study endpoint Patient statusOlaparib
(n=196), %
Placebo
(n=99), %
PFS
(investigator assessed)
Progression free, 18 months
Progression free, 24 months
51.1
43.0
16.2
15.1
PFS
(BICR)
Progression free, 18 months
Progression free, 24 months
58.7
52.7
21.7
19.9
TDTDiscontinuation free, 18 months
Discontinuation free, 24 months
51.8
44.8
17.2
13.1
PFS2Second progression free, 18 months
Second progression free, 24 months
71.8
59.2
52.4
37.3
TFSTFirst subsequent therapy free, 18 months
First subsequent therapy free, 24 months
65.0
54.1
21.8
17.3
TSSTSecond subsequent therapy free, 18 months
Second subsequent therapy free, 24 months
75.8
65.7
50.7
33.0

Key study dates
Study event Date
First subject in (FSI) 3 September 2013
Last subject in (LSI) 21 November 2014
Database lock (DBL) 19 October 2016