tutorial bladder trauma
TRANSCRIPT

BLADDERTRAUMA
NOOR HAFIZAH BINTI HASSAN2007287236

REFERENCES:
1) SMITH’S GENERAL UROLOGY 17th ED
2) GUIDELINES ON UROLOGICAL TRAUMA,EUROPEAN ASSOCIATION OF UROLOGY, FEBRUARY 2003

INCIDENCE
o 10% of trauma: involve GU systemo Bladder trauma: 60-80% are due to BLUNT
TRAUMAo Highly associated with pelvic # (70-97%)o Most common complication of bladder
trauma → BLADDER RUPTURE (90%)
CAUSES OF BLADDER TRAUMA BLUNT TRAUMA (67-86%) MVA DECELERATING INJURY
PENETRATING INJURY (14-33%) HIGH VELOCITY GUNSHOT STAB WOUND
IATROGENIC MEDICAL PROCEDURE

CLASSIFICATION OF BLADDER INJURY
1) BASED ON FINDINGS ON CT CYSTOGRAPHY:

Grade II:Subtle intraperitoneal contrast material between small bowel loops
Grade III:Focal lenticular thickening of the bladder wall due to interstitial hematoma and likely muscular disruption

Grade IVa:Extravasated contrast material into confined to the perivesical space within extraperitoneal pelvis
Grade IVb:Complex extraperitoneal spread→ extension into rectus abdominis muscle as well as subcutaneous fascia
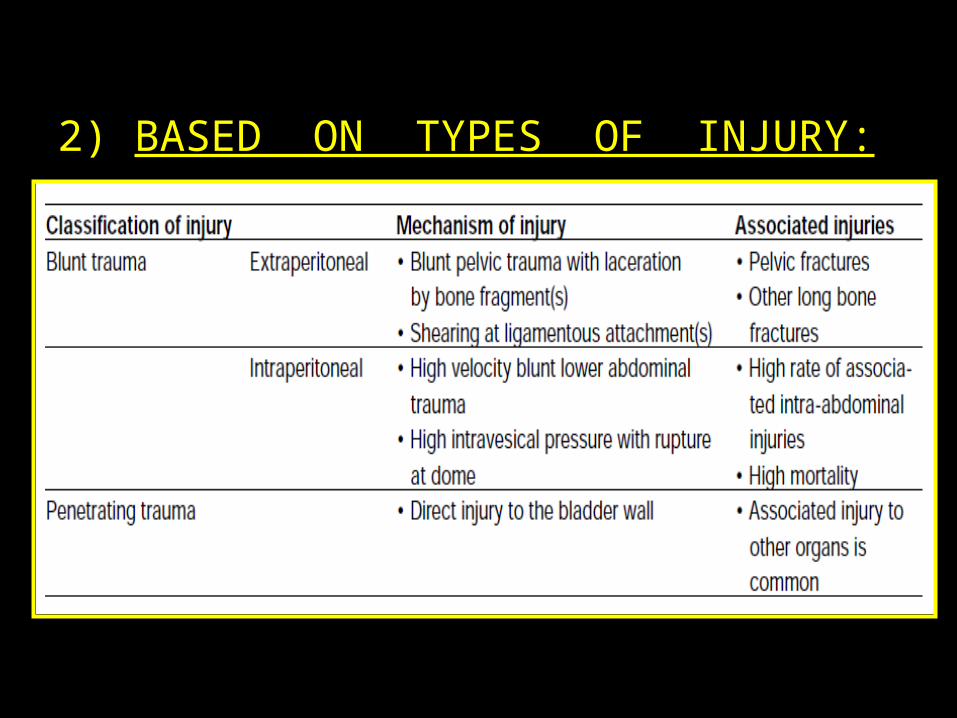
2) BASED ON TYPES OF INJURY:
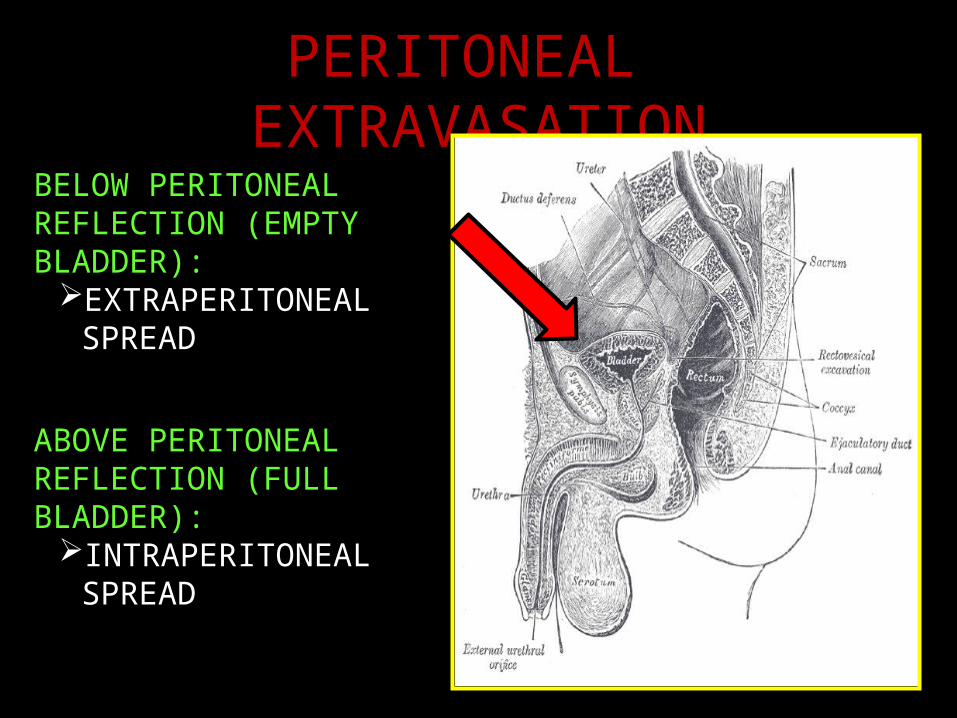
PERITONEAL EXTRAVASATION
ABOVE PERITONEAL REFLECTION (FULL BLADDER):
INTRAPERITONEAL SPREAD
BELOW PERITONEAL REFLECTION (EMPTY BLADDER):
EXTRAPERITONEAL SPREAD


EXTRAPERITONEAL BLADDERRUPTURE (80 %)
• Associated with pelvic fracture (80-100%)• Direct laceration of the bladder by the bony
fragments• > severe fracture, degree of bladder injury ↑• Cystographic finding: contrast extravasation
around base of bladder confined to perivesical space
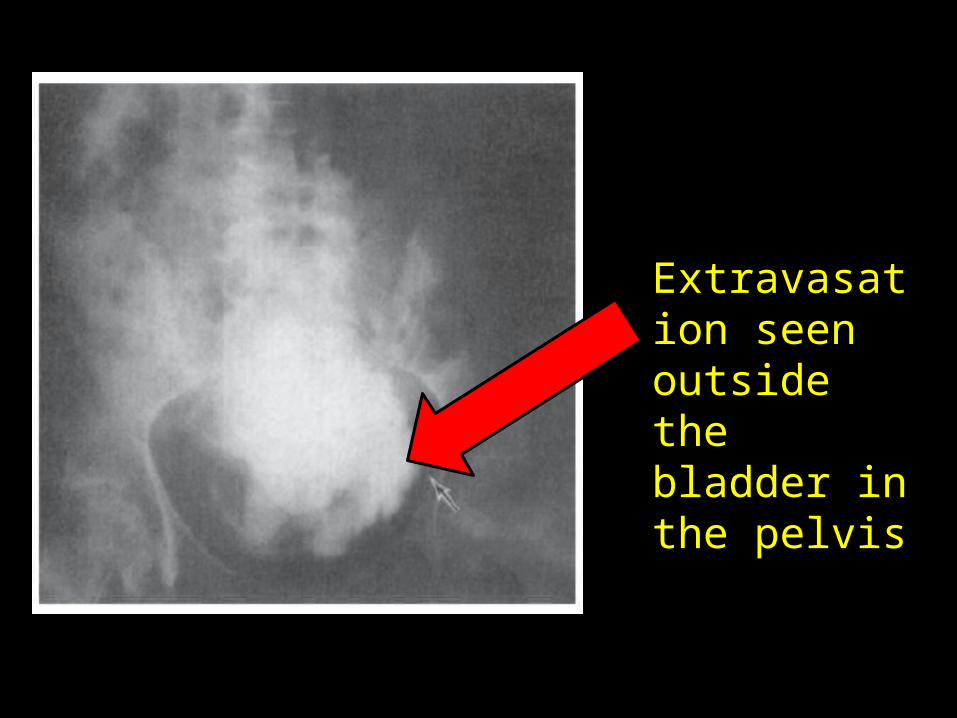
Extravasation seen outside the bladder in the pelvis
INTRAPERITONEAL BLADDERRUPTURE (20 %)
• Direct blow to a distended bladder• Full bladder → muscle fibers are widely
separated → entire bladder wall is thin → offer little resistance
• Injury → ↑ intravesical pressure → horizontal tear along intraperitoneal portion of bladder wall
• Cystographic finding: contrast extravasation into peritoneal cavity, lining loops of bowel
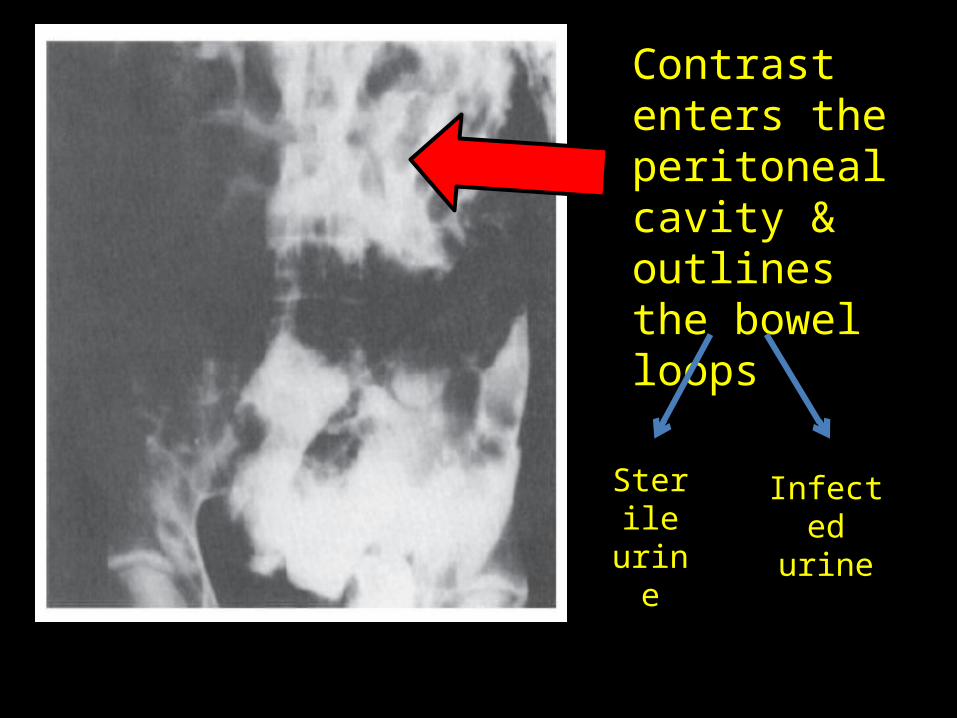
Contrast enters the peritoneal cavity & outlines the bowel loops
Sterileurine
Infectedurine

CLINICAL FEATURES
SYMPTOMS:– Gross hematuria – Abdominal tenderness– Others: inability to void, bruises over suprapubic
region
ON EXAMINATION:– Abdominal tenderness– Per rectal: to exclude rectal injury
: assess prostate position

INVESTIGATION
CYSTOGRAPHY• Gold standard for dx bladder rupture (85-100%)• Dx: injected contrast are out of the bladder• Require plain film, filled film and post-drainage
film• CT CYSTOGRAPHY: bladder is inadequately
distended to allow extravasation through perforated bladder

MANAGEMENT
1) IMMEDIATE MEASURES:– Treat shock and hemorrhage, if any– Catheterization: if blood noted at urethral
meatus, don’t insert Foley’s catheter → retrograde urethrogram
2) DETERMINE EXTENT OF PERITONEAL EXTRAVASATION : RETROGRADE CYSTOGRAPHY

EXTRAPERITONEAL RUPTURE:• Catheter drainage only, even in the presence of
extensive retroperitoneal or scrotal extravasation• Healing takes 10 days → 3 weeks• Surgical intervention?
bladder neck involvement presence of bone fragments in the bladder wall evacuation of pelvic hematoma/drainage of pelvic
abscess

INTRAPERITONEAL RUPTURE:• Always managed surgically:– Transperitoneal approach– Peritoneum closed carefully over the area of injury– All extravasated fluid should be removed– Bladder is closed in separate layer