two-stage hepatectomy for unresectable metastases :
DESCRIPTION
Two-Stage Hepatectomy for Unresectable Metastases :. R. Adam, D.A. Wicherts, R. Miller, R.J. de Haas, G. Bitsakou, E. Vibert, L.A. Veilhan, D. Azoulay, H. Bismuth, D. Castaing. Hôpital Paul Brousse, Université Paris-Sud, France. Resectable 10–20%. Non resectable 80–90%. 1-2%. 15–30 %. - PowerPoint PPT PresentationTRANSCRIPT
Two-Stage Hepatectomy Two-Stage Hepatectomy
for Unresectable for Unresectable
Metastases : Metastases :
Hôpital Paul Brousse, Université Paris-Sud, France
R. Adam, D.A. Wicherts, R. Miller,
R.J. de Haas, G. Bitsakou, E. Vibert, L.A. Veilhan,
D. Azoulay, H. Bismuth, D. Castaing
QuickTime™ et undécompresseur TIFF (non compressé)sont requis pour visionner cette image.
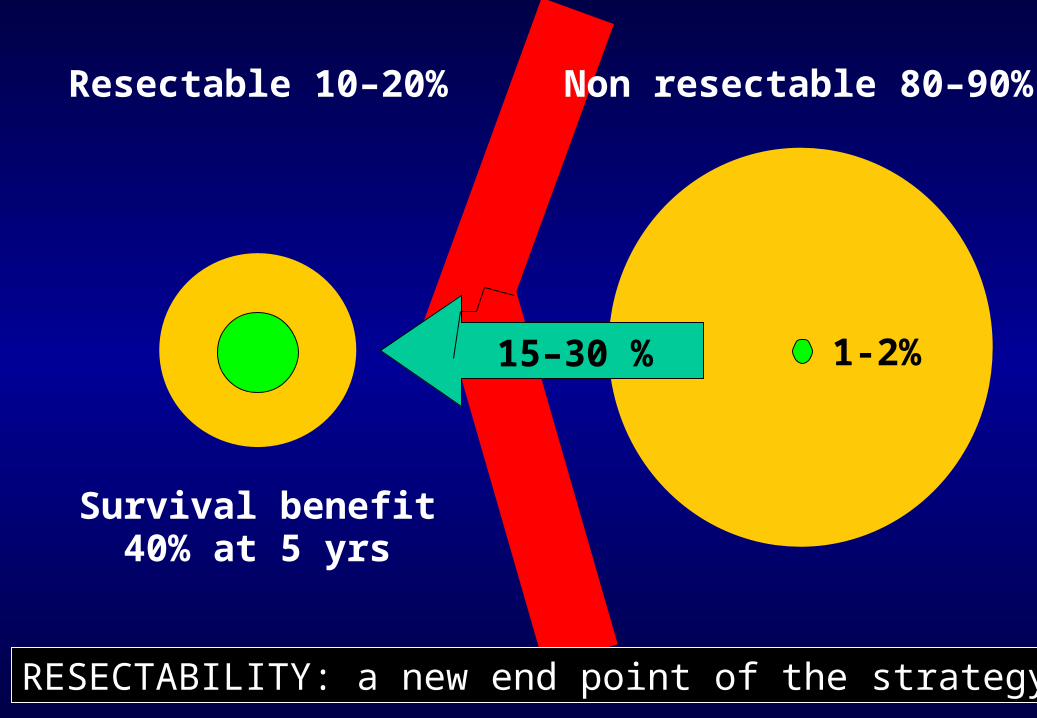
Survival benefit40% at 5 yrs
Resectable 10–20% Non resectable 80–90%
1-2%15–30 %
RESECTABILITY: a new end point of the strategy
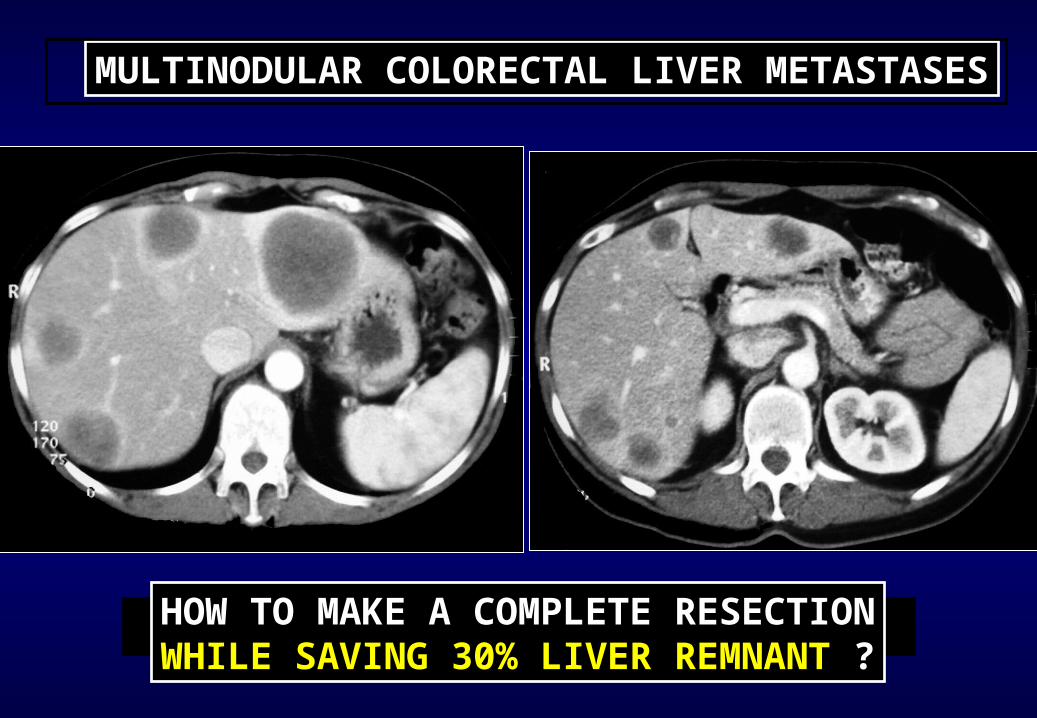
MULTINODULAR COLORECTAL LIVER METASTASES
HOW TO MAKE A COMPLETE RESECTIONWHILE SAVING 30% LIVER REMNANT ?
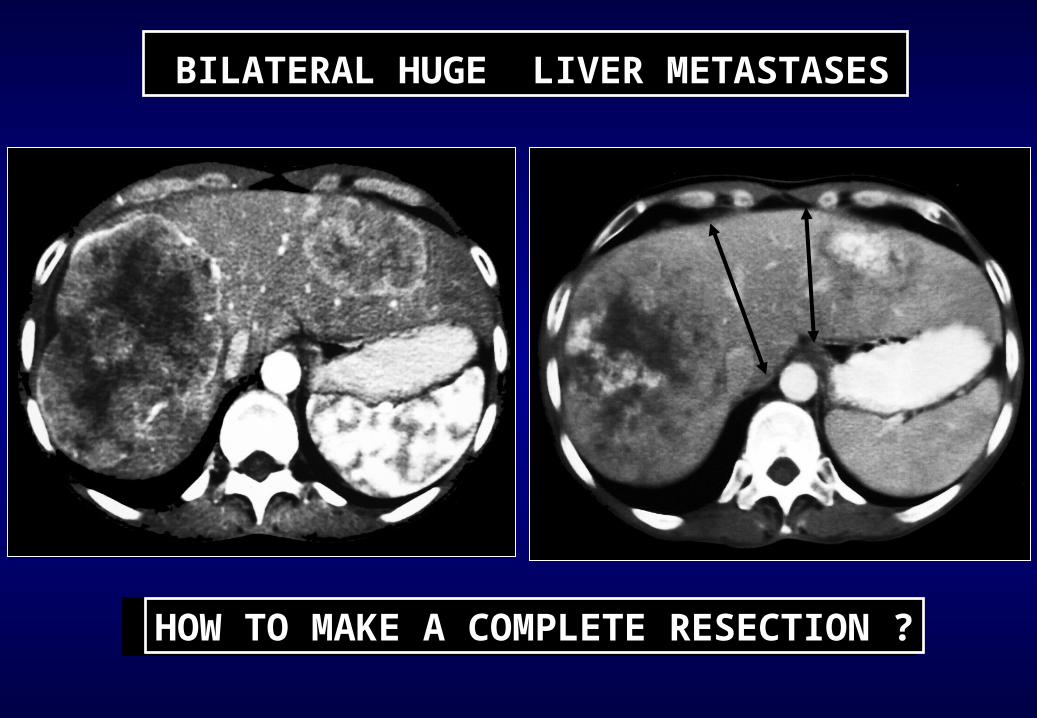
BILATERAL HUGE LIVER METASTASES
HOW TO MAKE A COMPLETE RESECTION ?
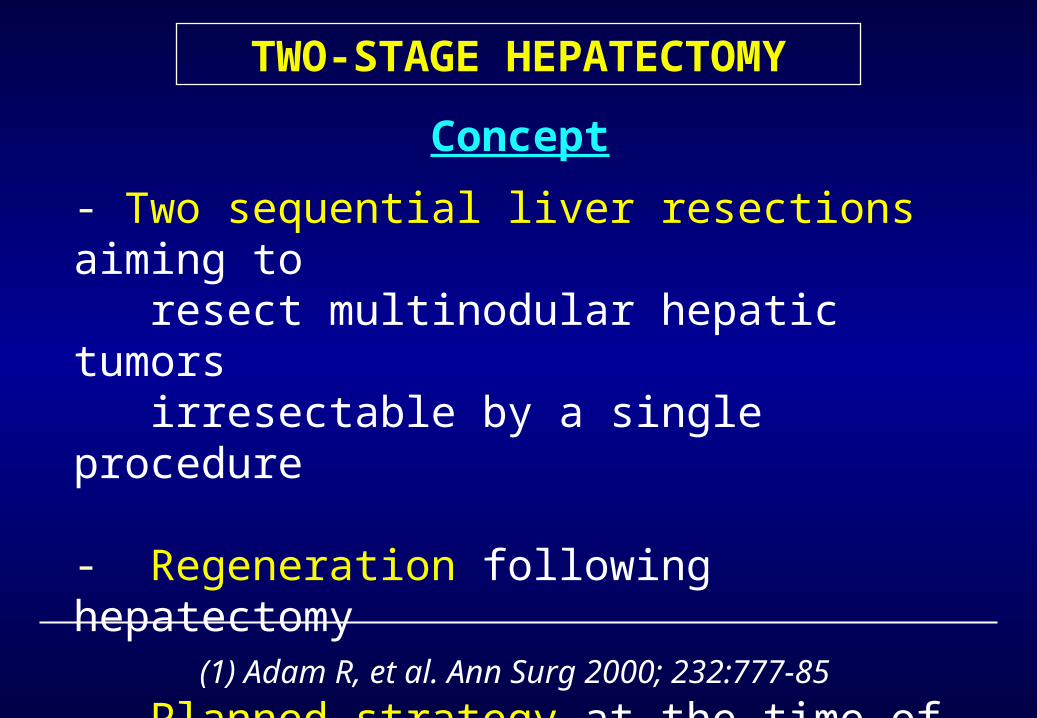
TWO-STAGE HEPATECTOMY
Concept
- Two sequential liver resections aiming to resect multinodular hepatic tumors irresectable by a single procedure
- Regeneration following hepatectomy
- Planned strategy at the time of 1st hepatectomy
- (1) Adam R, et al. Ann Surg 2000; 232:777-85

I
(1) Adam R, et al. Ann Surg 2000; 232:777-85
Two-Stage Hepatectomy
155 cc
440 cc
IVI
1
2
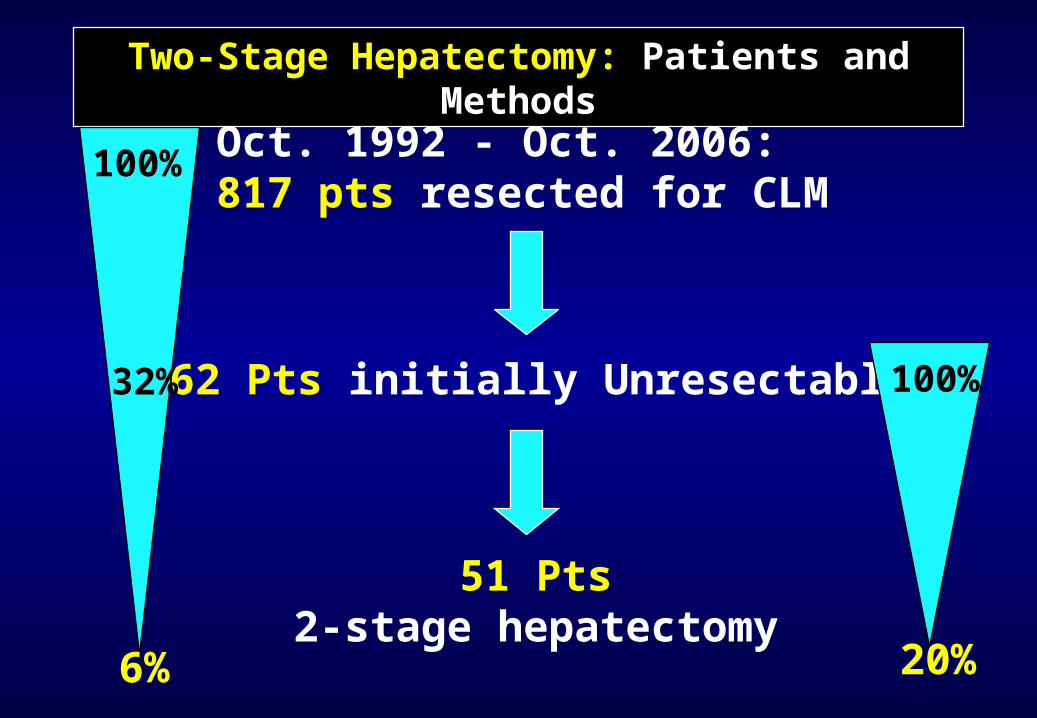
Oct. 1992 - Oct. 2006: 817 pts resected for CLM
Two-Stage Hepatectomy: Patients and Methods
51 Pts2-stage hepatectomy
262 Pts initially Unresectable
6%
32%
100%
100%
20%
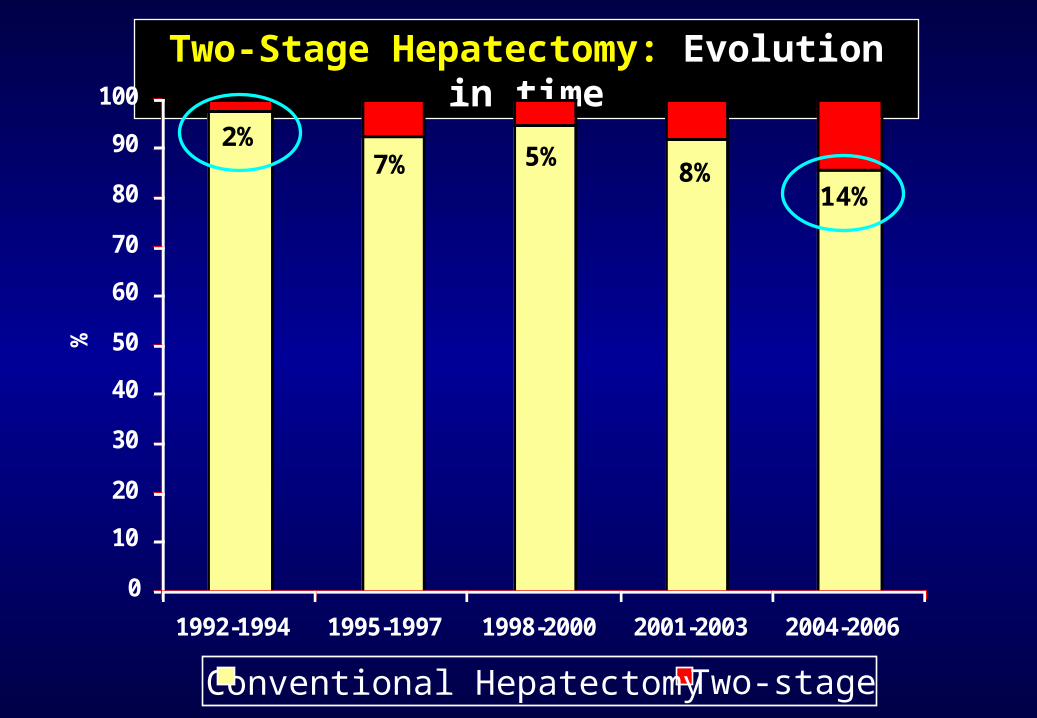
Two-Stage Hepatectomy: Evolution in time
0
10
20
30
40
50
60
70
80
90
100
1992-1994 1995-1997 1998-2000 2001-2003 2004-2006
%
Conventional HepatectomyTwo-stage
14%8%
5%7%2%
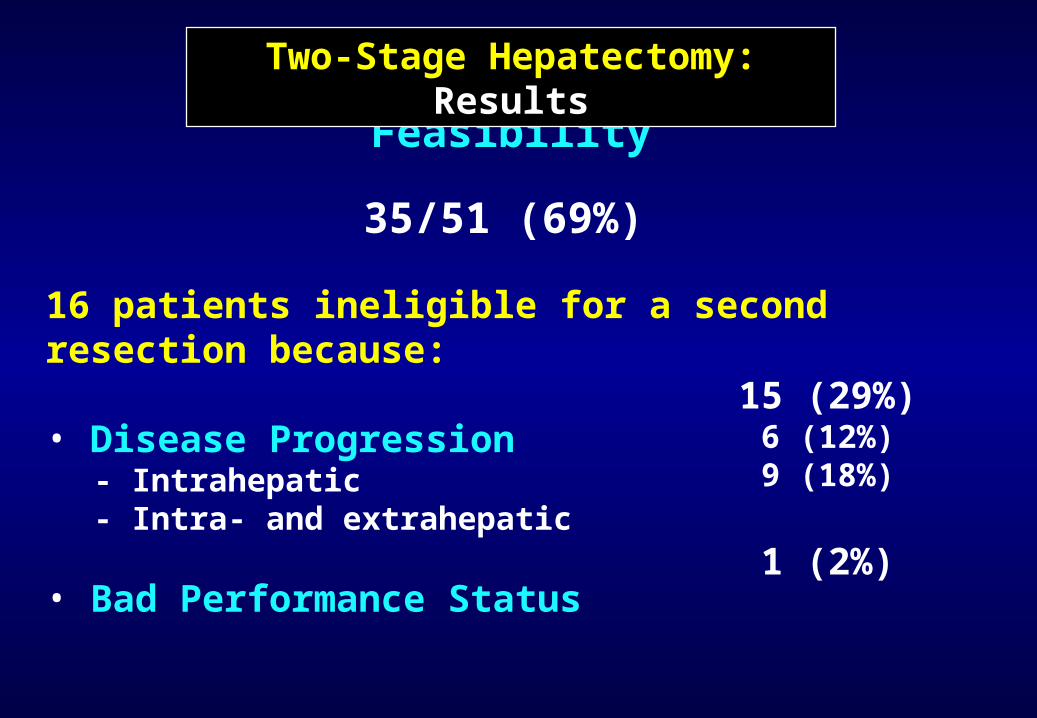
Feasibility
35/51 (69%)
16 patients ineligible for a second resection because:
• Disease Progression- Intrahepatic- Intra- and extrahepatic
• Bad Performance Status
15 (29%)6 (12%)9 (18%)
1 (2%)
Two-Stage Hepatectomy: Results
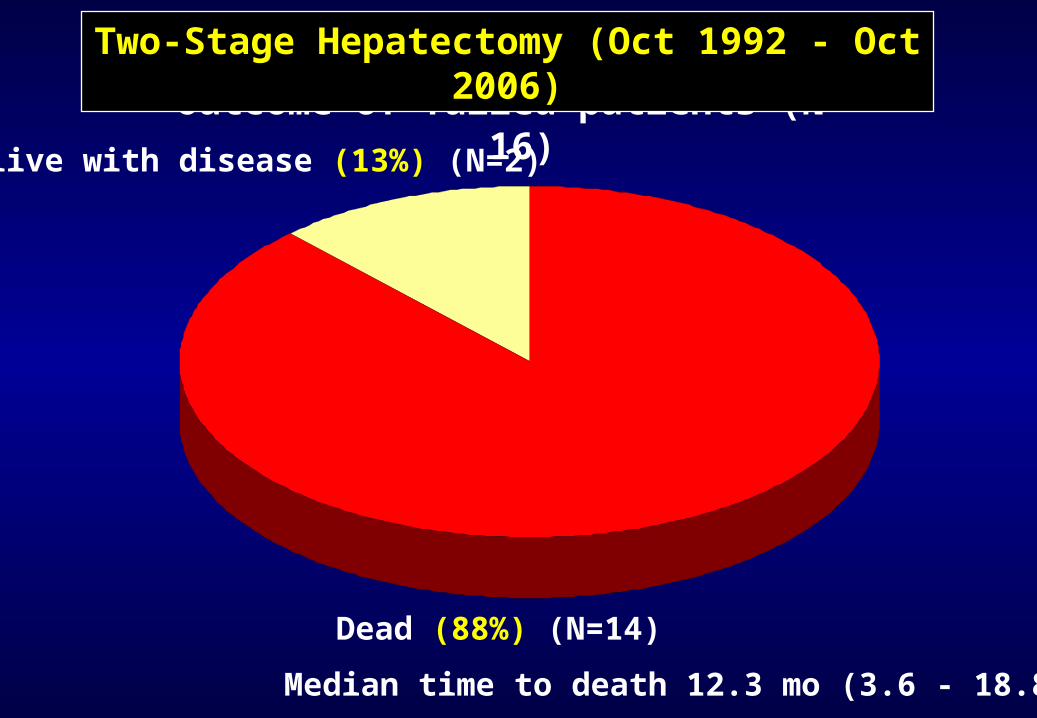
Outcome of failed patients (N = 16)
Two-Stage Hepatectomy (Oct 1992 - Oct 2006)
Dead (88%) (N=14)
Median time to death 12.3 mo (3.6 - 18.8)
Alive with disease (13%) (N=2)
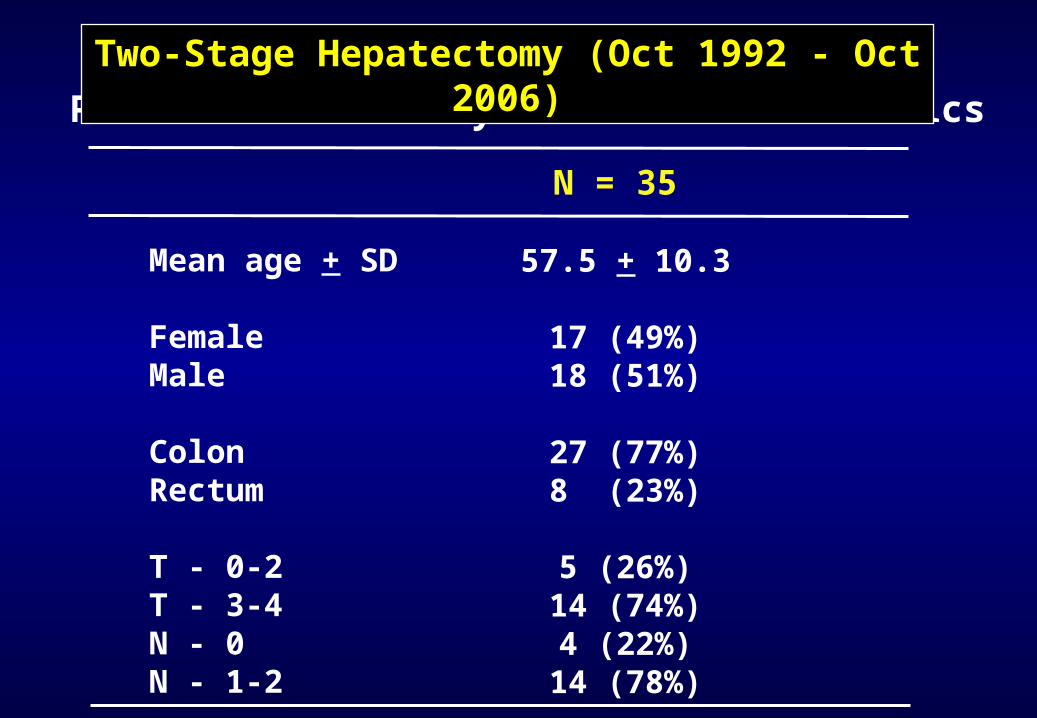
Patient and Primary tumor characteristics
Mean age + SD
FemaleMale
ColonRectum
T - 0-2T - 3-4N - 0N - 1-2
N = 35
57.5 + 10.3
17 (49%)18 (51%)
27 (77%)8 (23%)
5 (26%)14 (74%)4 (22%)14 (78%)
Two-Stage Hepatectomy (Oct 1992 - Oct 2006)
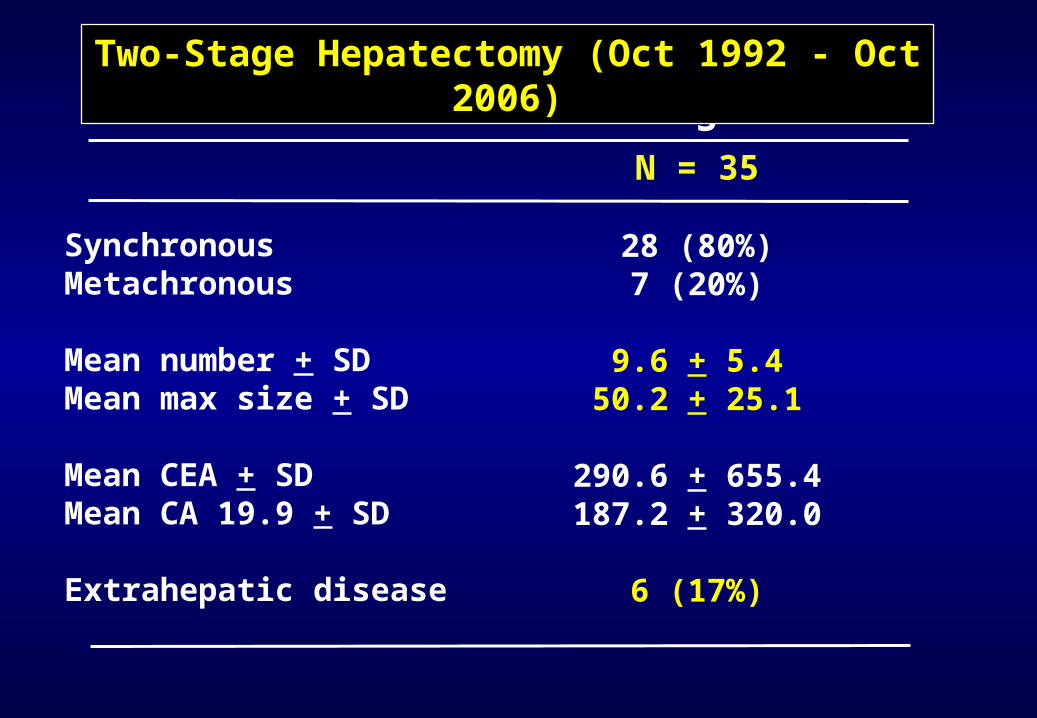
N = 35
28 (80%)7 (20%)
9.6 + 5.450.2 + 25.1
290.6 + 655.4187.2 + 320.0
6 (17%)
Liver Metastases Diagnosis
SynchronousMetachronous
Mean number + SDMean max size + SD
Mean CEA + SDMean CA 19.9 + SD
Extrahepatic disease
Two-Stage Hepatectomy (Oct 1992 - Oct 2006)
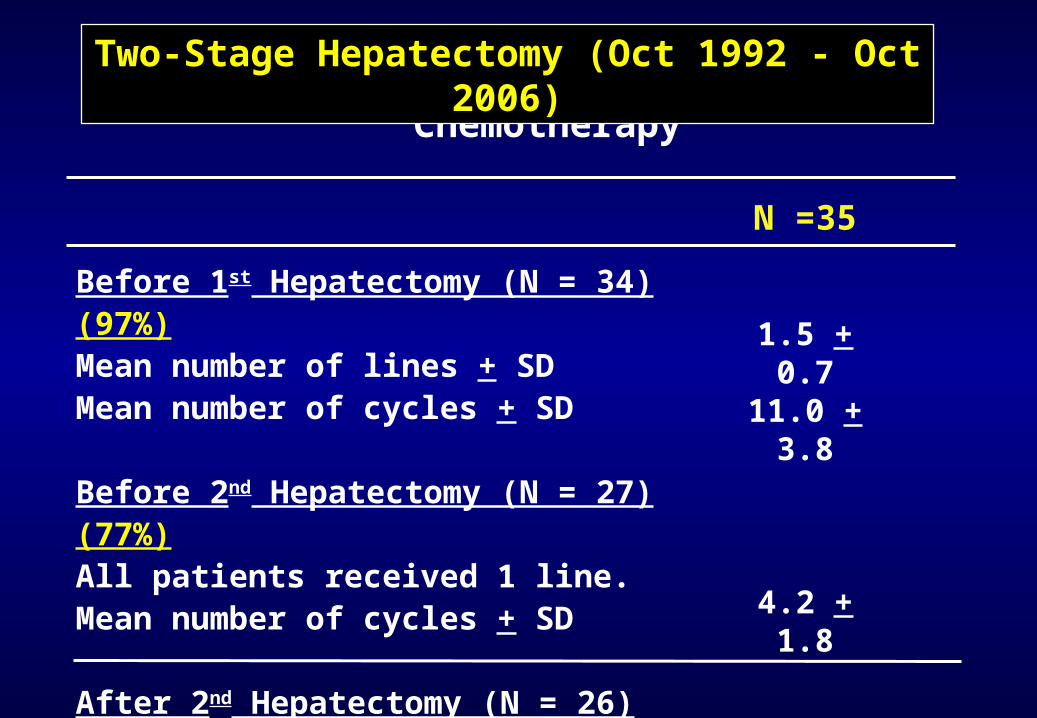
Chemotherapy
Before 1st Hepatectomy (N = 34) (97%)Mean number of lines + SDMean number of cycles + SD
Before 2nd Hepatectomy (N = 27) (77%)All patients received 1 line.Mean number of cycles + SD
After 2nd Hepatectomy (N = 26) (74%)
N =35
1.5 + 0.711.0 +
3.8
4.2 + 1.8
Two-Stage Hepatectomy (Oct 1992 - Oct 2006)
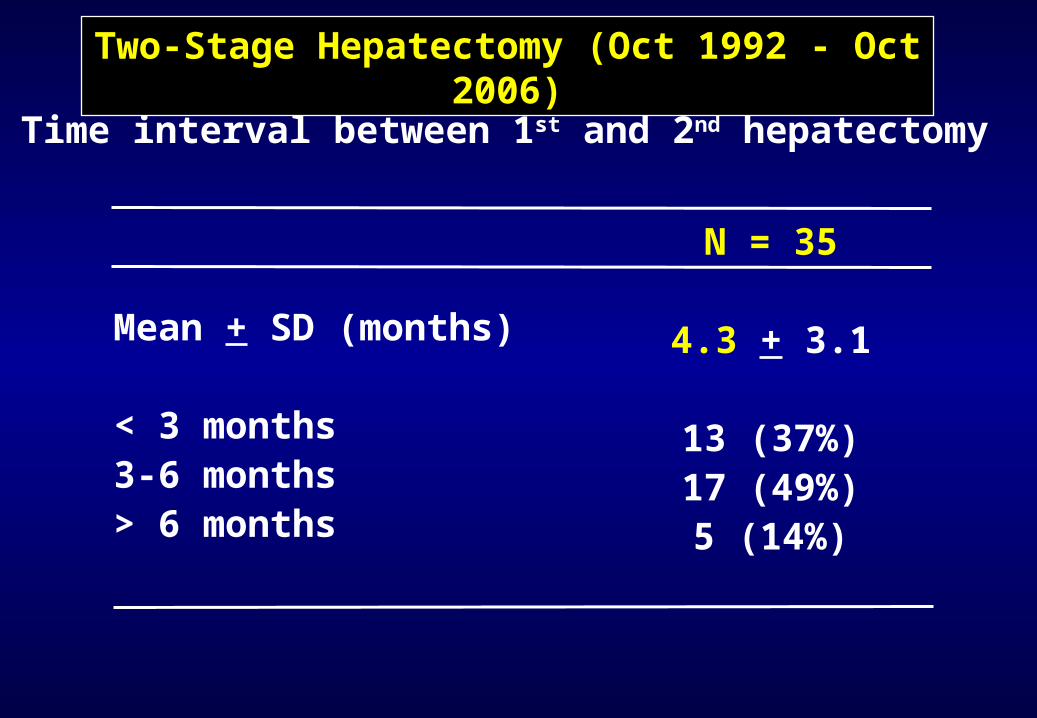
Time interval between 1st and 2nd hepatectomy
Mean + SD (months)
< 3 months3-6 months> 6 months
N = 35
4.3 + 3.1
13 (37%)17 (49%)5 (14%)
Two-Stage Hepatectomy (Oct 1992 - Oct 2006)
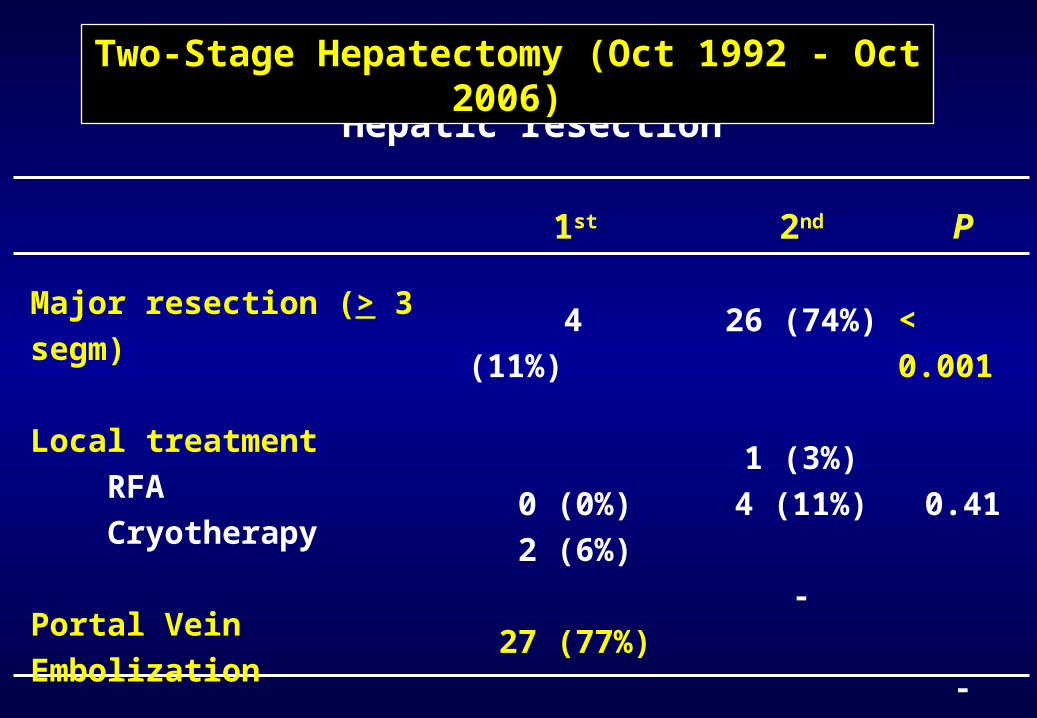
Hepatic resection
1st
4 (11%)
0 (0%)2 (6%)
27 (77%)
Major resection (> 3 segm)
Local treatment RFA Cryotherapy
Portal Vein Embolization
2nd
26 (74%)
1 (3%)4 (11%)
-
P
< 0.001
0.41
-
Two-Stage Hepatectomy (Oct 1992 - Oct 2006)
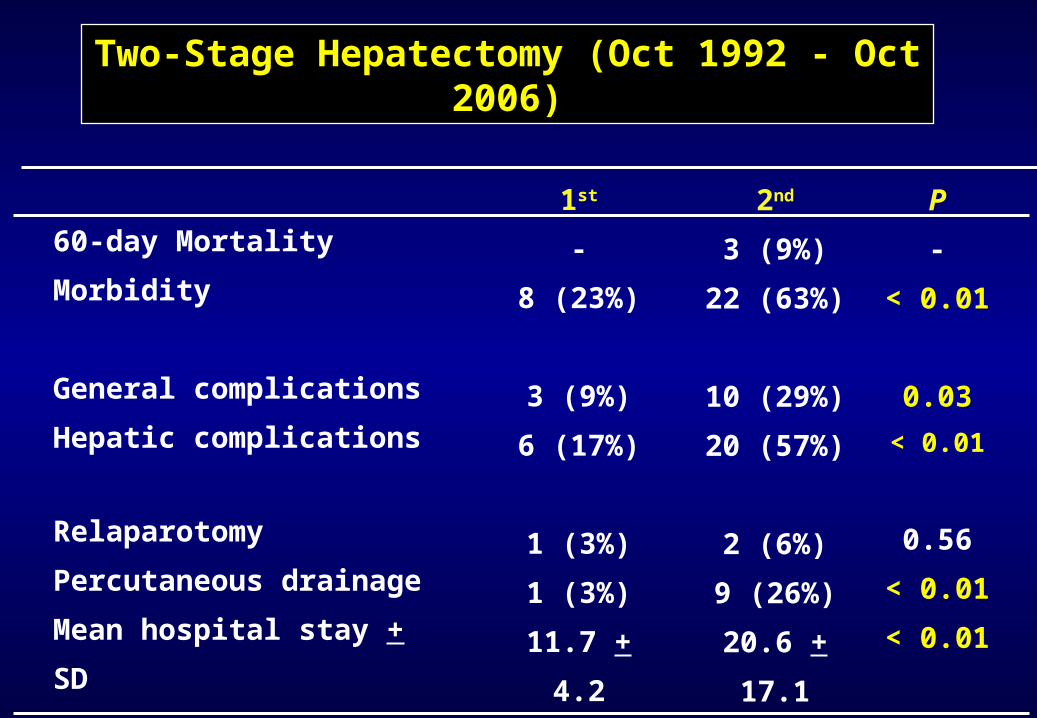
Short-term outcome
1st
-
8 (23%)
3 (9%)
6 (17%)
1 (3%)
1 (3%)
11.7 +
4.2
2nd
3 (9%)
22 (63%)
10 (29%)
20 (57%)
2 (6%)
9 (26%)
20.6 +
17.1
60-day Mortality
Morbidity
General complications
Hepatic complications
Relaparotomy
Percutaneous drainage
Mean hospital stay + SD
P
-
< 0.01
0.03
< 0.01
0.56
< 0.01
< 0.01
Two-Stage Hepatectomy (Oct 1992 - Oct 2006)
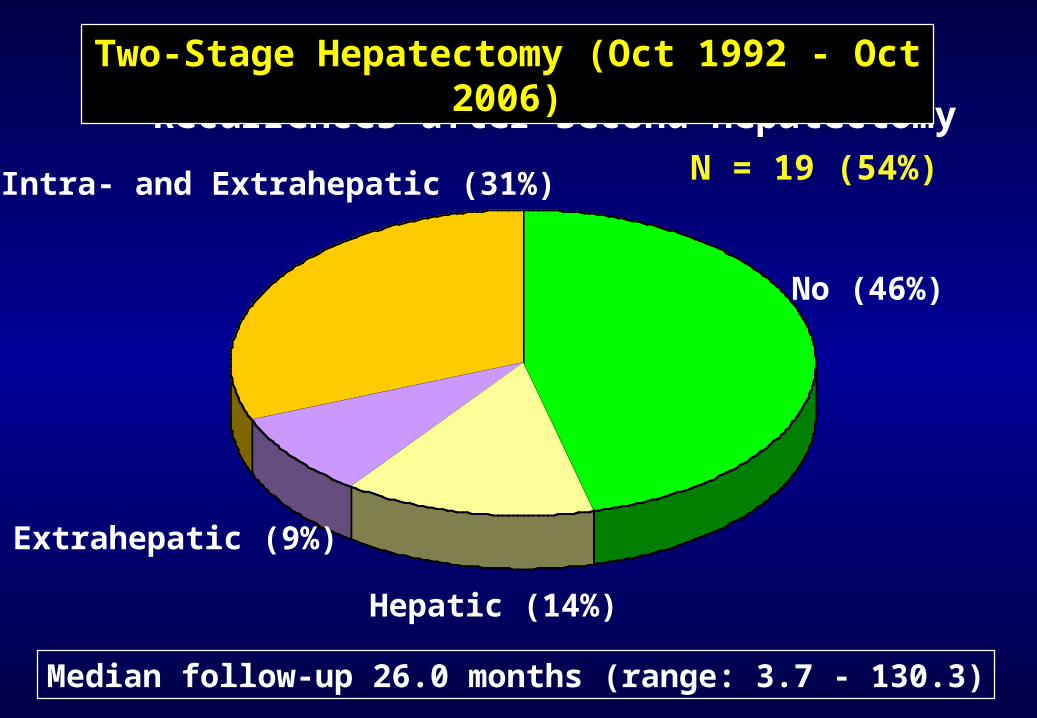
Recurrences after second hepatectomy
Two-Stage Hepatectomy (Oct 1992 - Oct 2006)
No (46%)
Hepatic (14%)
Extrahepatic (9%)
Intra- and Extrahepatic (31%)
Median follow-up 26.0 months (range: 3.7 - 130.3)
N = 19 (54%)
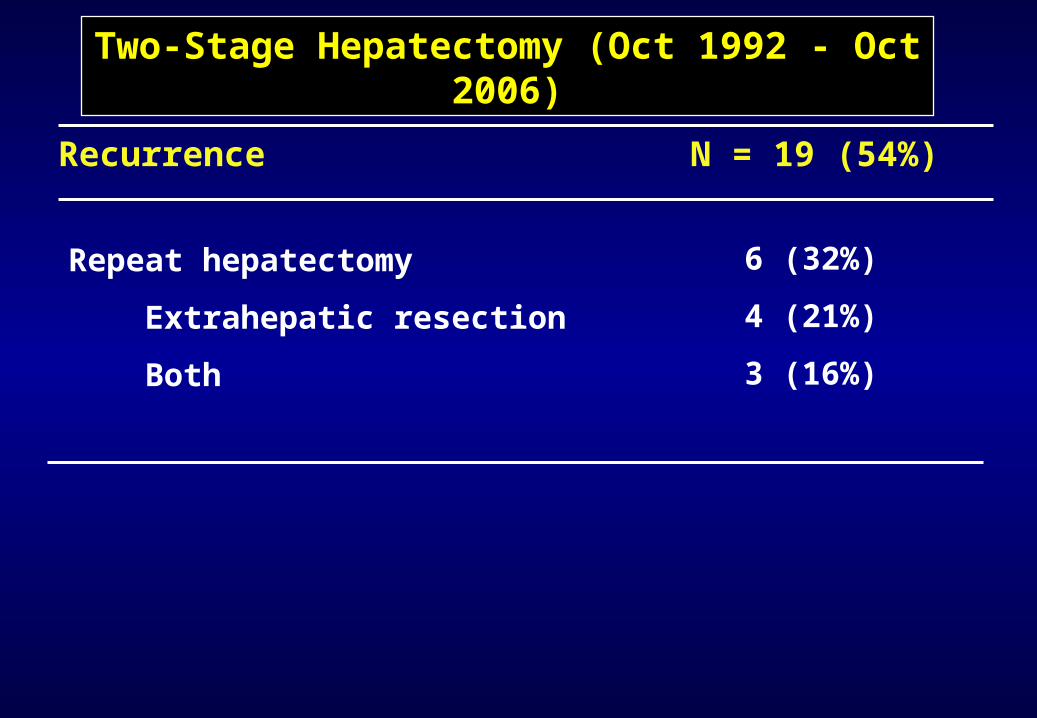
6 (32%)
4 (21%)
3 (16%)
Repeat hepatectomy
Extrahepatic resection
Both
Two-Stage Hepatectomy (Oct 1992 - Oct 2006)
N = 19 (54%)Recurrence
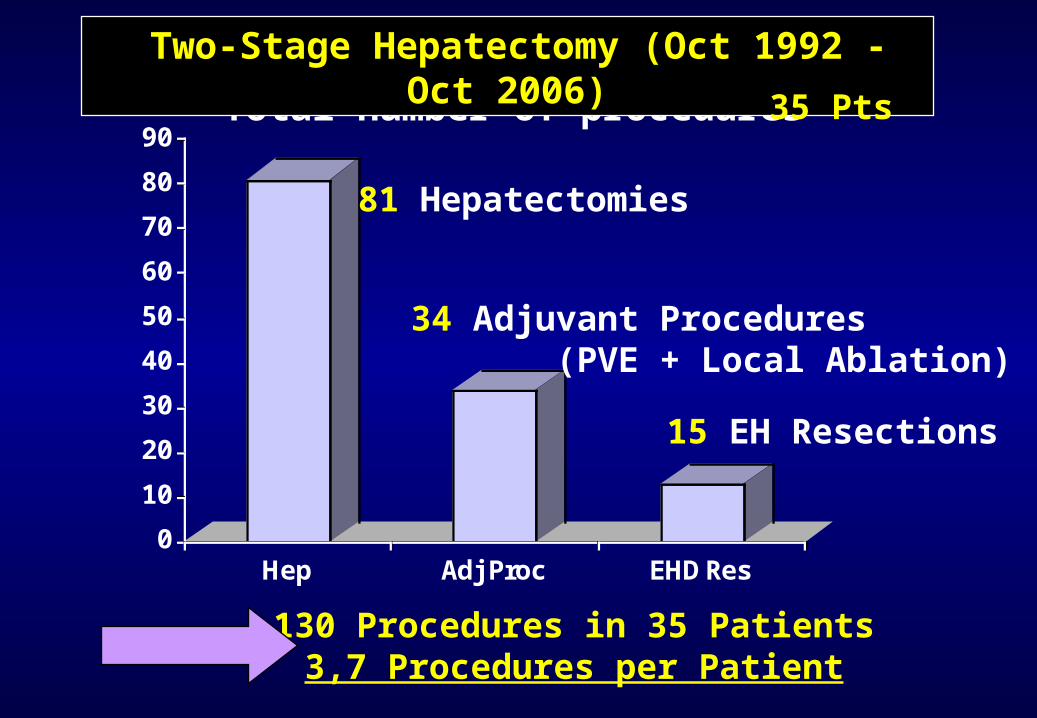
Total number of procedures
Two-Stage Hepatectomy (Oct 1992 - Oct 2006)
0
10
20
30
40
50
60
70
80
90
Hep Adj Proc EHD Res
81 Hepatectomies
34 Adjuvant Procedures (PVE + Local Ablation)
15 EH Resections
130 Procedures in 35 Patients3,7 Procedures per Patient
35 Pts
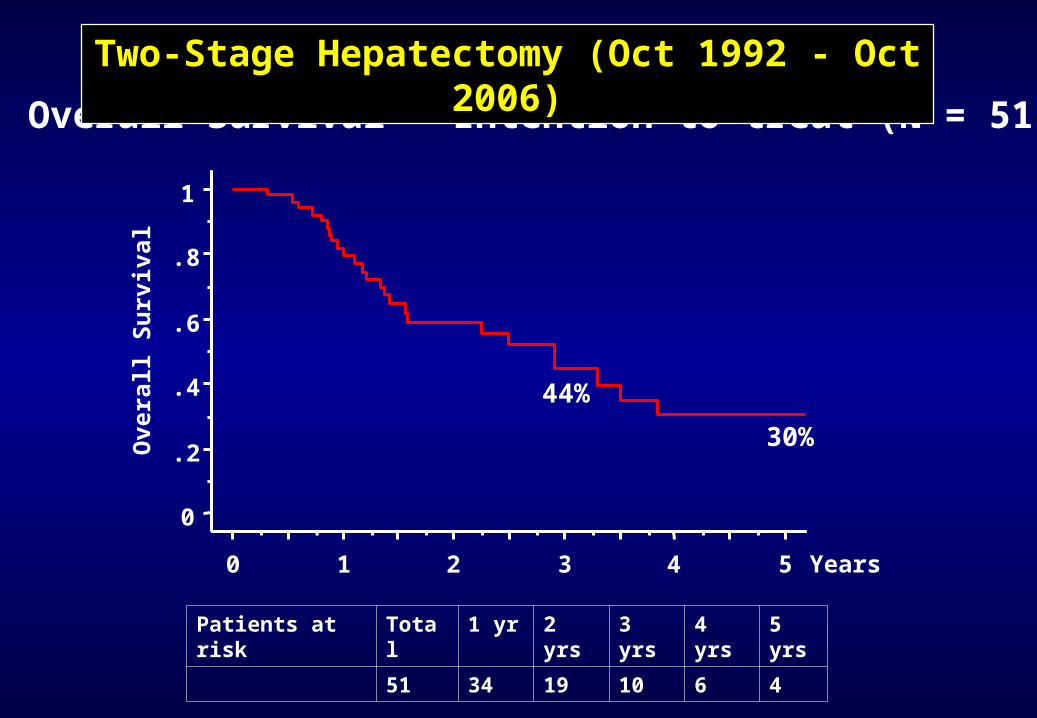
Overall Survival - Intention to treat (N = 51)
Patients at risk
Total 1 yr 2 yrs
3 yrs
4 yrs
5 yrs
51 34 19 10 6 4
0
.2
.4
.6
.8
1
Overa
ll S
urv
ival
0 1 2 3 4 5 Years
44%
30%
Two-Stage Hepatectomy (Oct 1992 - Oct 2006)
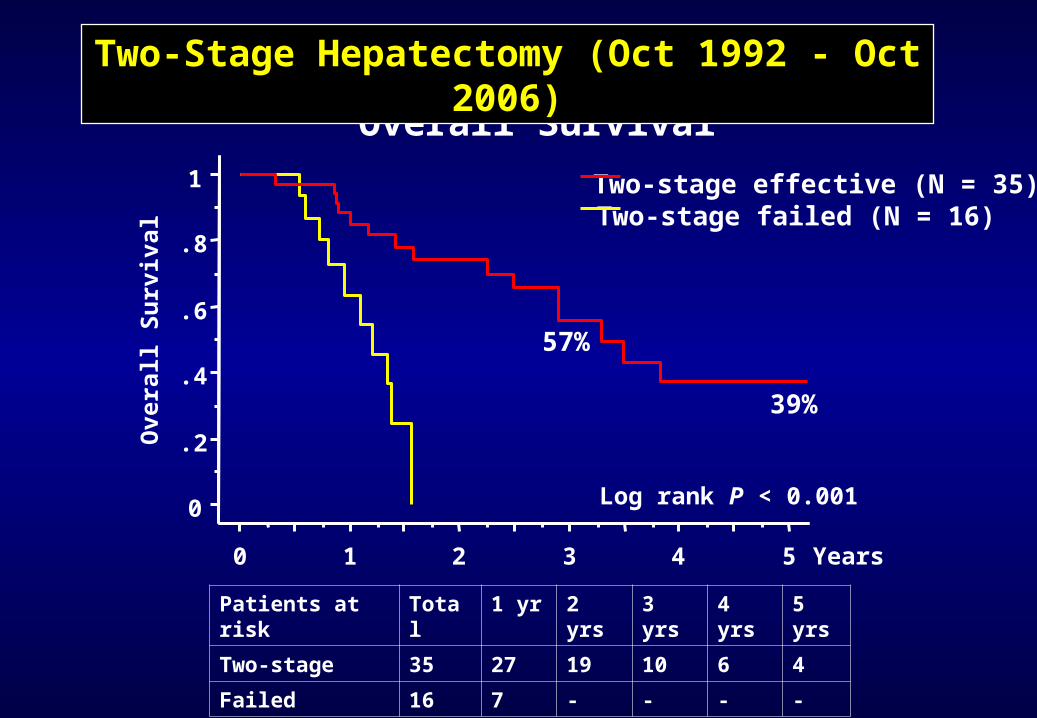
Overall Survival
Patients at risk
Total 1 yr 2 yrs
3 yrs
4 yrs
5 yrs
Two-stage 35 27 19 10 6 4
Failed 16 7 - - - -
0
.2
.4
.6
.8
1O
vera
ll S
urv
ival
0 1 2 3 4 5 Years
Two-stage effective (N = 35)Two-stage failed (N = 16)
Log rank P < 0.001
57%
39%
Two-Stage Hepatectomy (Oct 1992 - Oct 2006)
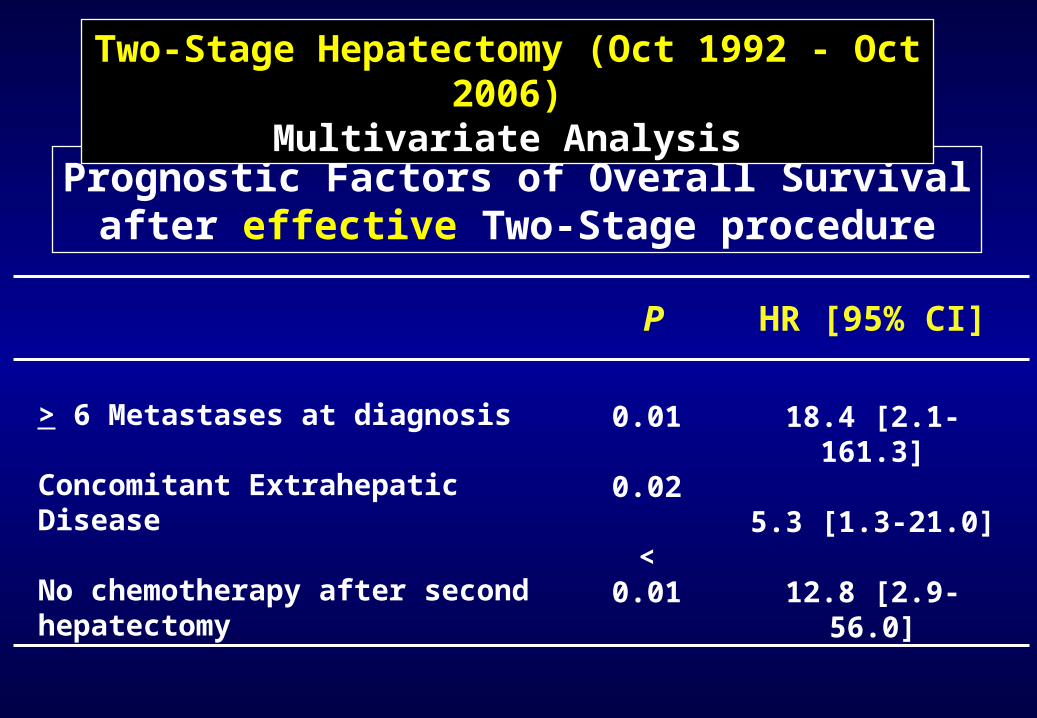
Prognostic Factors of Overall Survivalafter effective Two-Stage procedure
HR [95% CI]P
> 6 Metastases at diagnosis
Concomitant Extrahepatic Disease
No chemotherapy after second hepatectomy
0.01
0.02
< 0.01
18.4 [2.1-161.3]
5.3 [1.3-21.0]
12.8 [2.9-56.0]
Two-Stage Hepatectomy (Oct 1992 - Oct 2006)
Multivariate Analysis
Conclusions
1) Established strategy to increase resectability in selected patients with advanced bilobar disease
2) Feasibility rate: 69%
3) Second resection (more extensive) had higher morbidity than first resection
4) Five-year survival 39% for patients that completed the total strategy, close to that of patients with a single procedure.
Two-Stage Hepatectomy
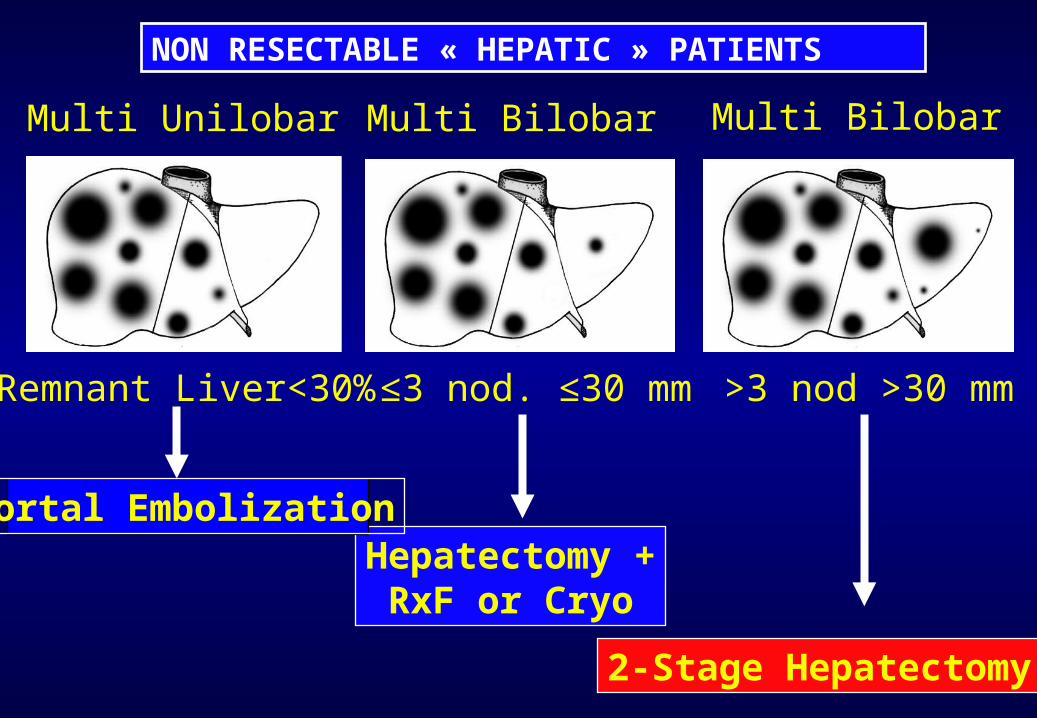
NON RESECTABLE « HEPATIC » PATIENTS
Multi Unilobar Multi Bilobar Multi Bilobar
Remnant Liver<30% ≤3 nod. ≤30 mm >3 nod >30 mm
Hepatectomy +RxF or Cryo
2-Stage Hepatectomy
Portal Embolization