Types of peritonitis and · PDF filePrimary Peritonitis . Bacteria may gain access to the peritoneal fluid from hematogenous or lymphogenous spread . Fever is most common presenting
63
Types of peritonitis and management J olita Auguste, PGY-5 SUNY Downstate Grand Rounds 11/3/2016 www.downstatesurgery.org
Types of peritonitis and management J olita Augus te, PGY-5 SUNY Downs tate Grand Rounds 11/3/2016
www.downstatesurgery.org
Case Presentation
xx year old patient pres ents to ED with complaints of one day of abdominal pain s ince his dis charge from an OSH. Patient was recently admitted to Hos pital 7 days prior for Colonos copy and s uffered a perforation. He was taken urgently to the OR and underwent an Exploratory laparotomy, s igmoid res ection with primary anas tomos is .
PMHx: HIV (viral load undetectable as per patient) PSHx: (1980s) Exploratory Laparotomy, small bowel resection with anastomosis for GSW; (10 days prior) Exploratory Laparotomy, sigmoid resection and anastomosis Meds: Atripla NKDA
www.downstatesurgery.org
Case Presentation
Vitals : afebrile, 106, 99/56
Labs : 12 142 99 17 123
16 262 4 23 1.16
37
6.2 36 166 Lactate 1.7
2.87 26 2.6 Coags : WNL
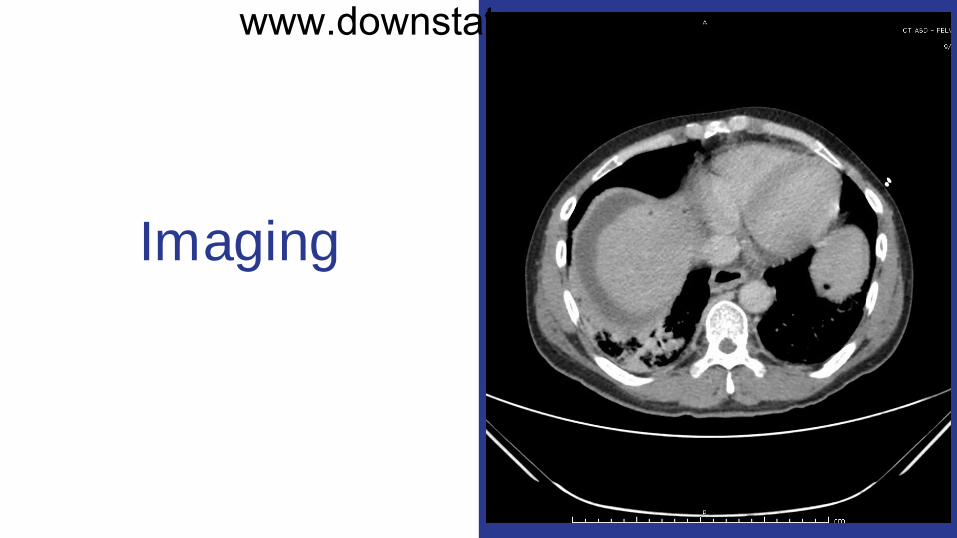
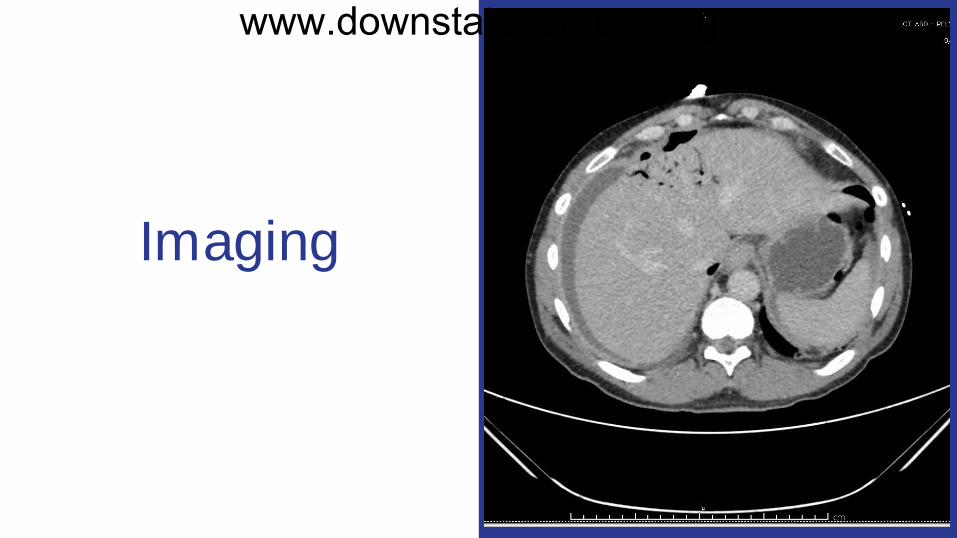
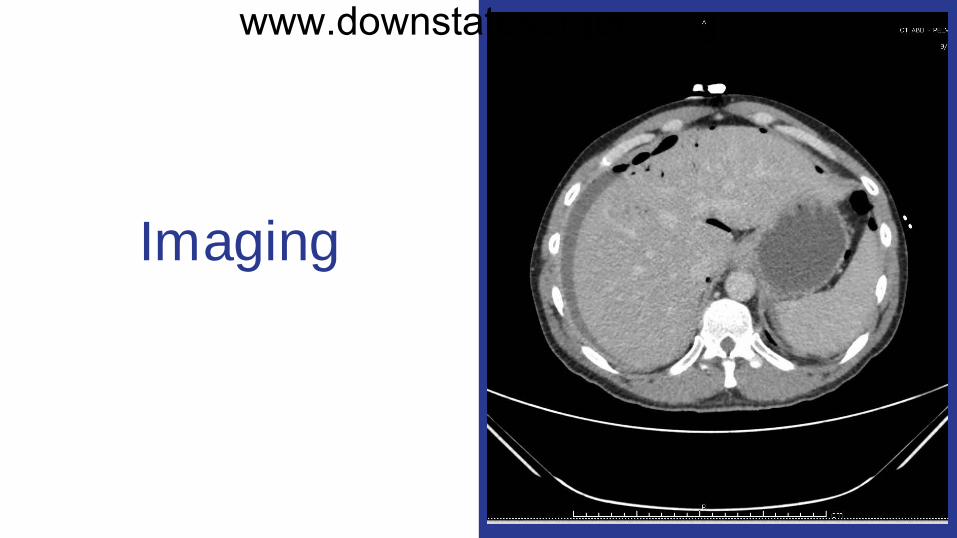
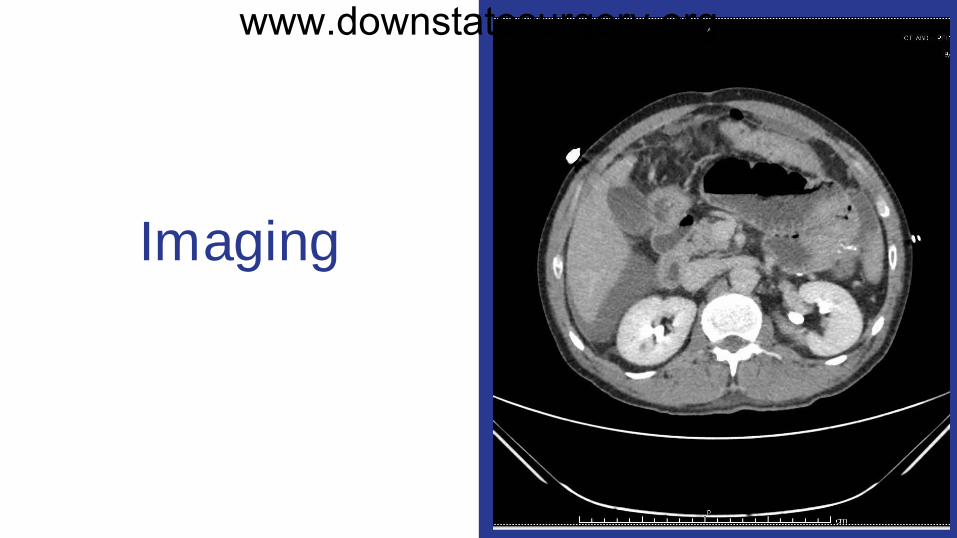
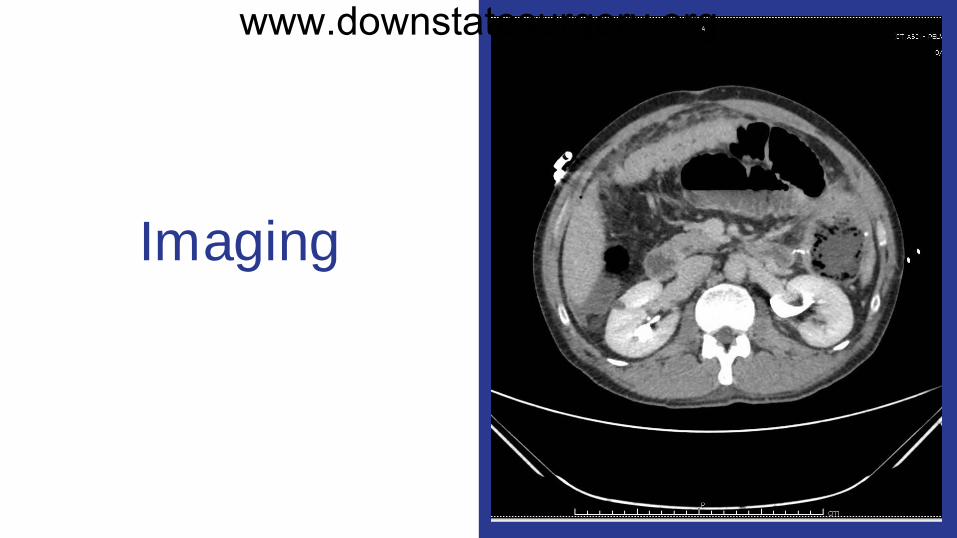
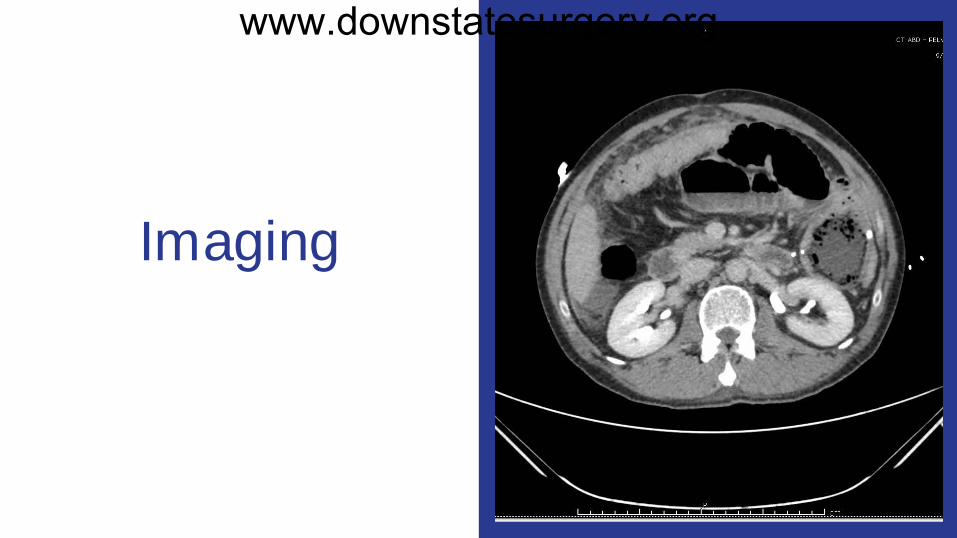
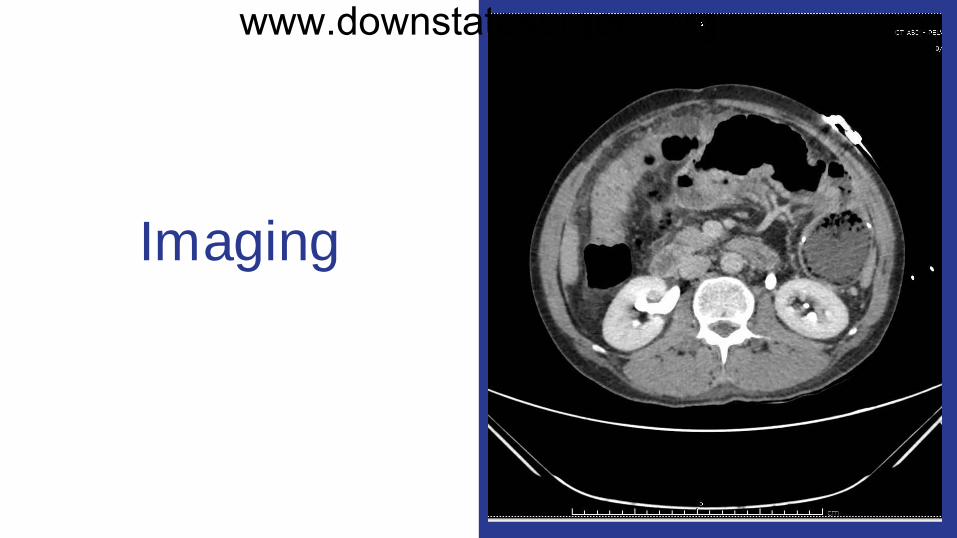
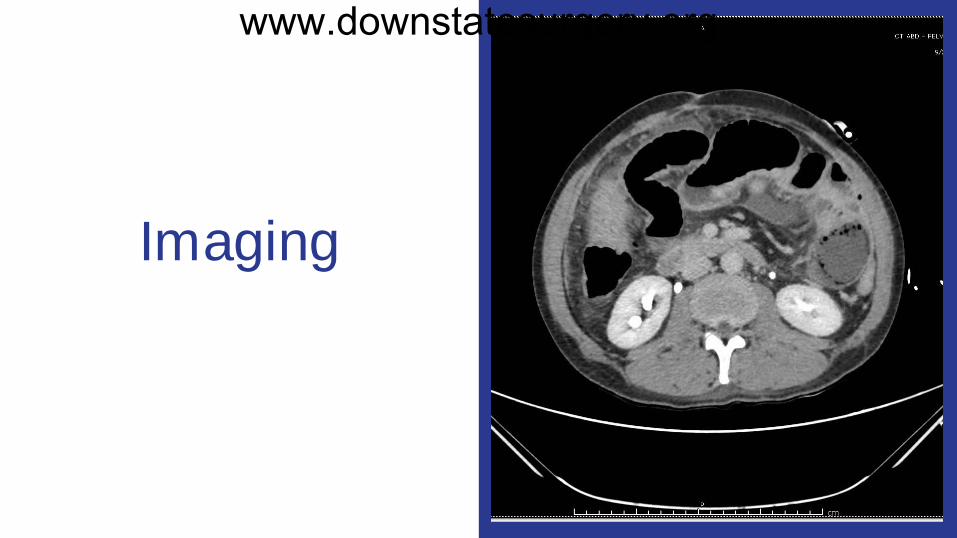
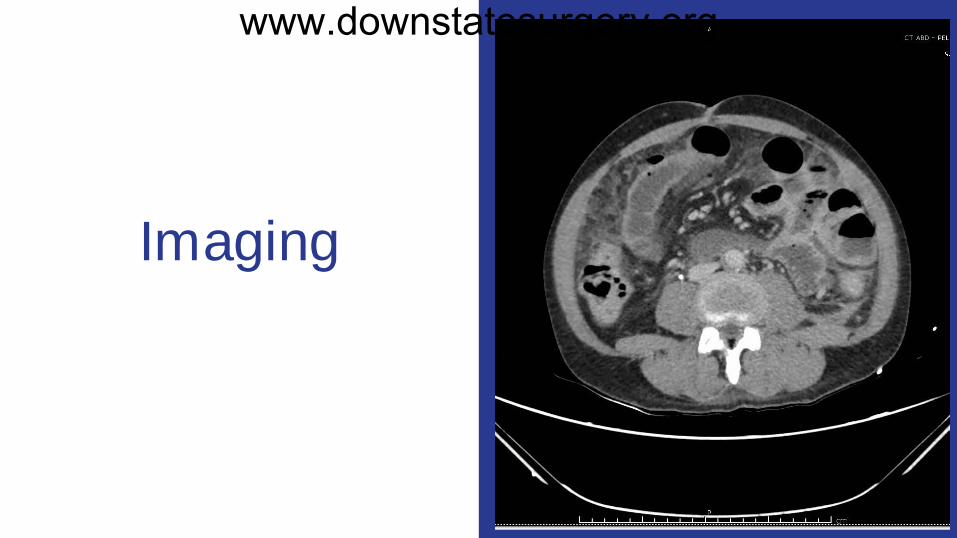
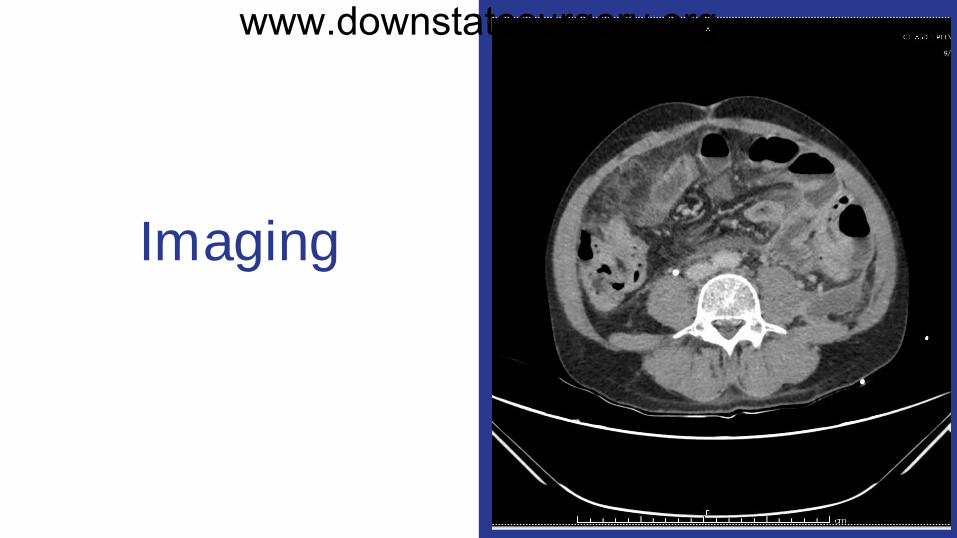
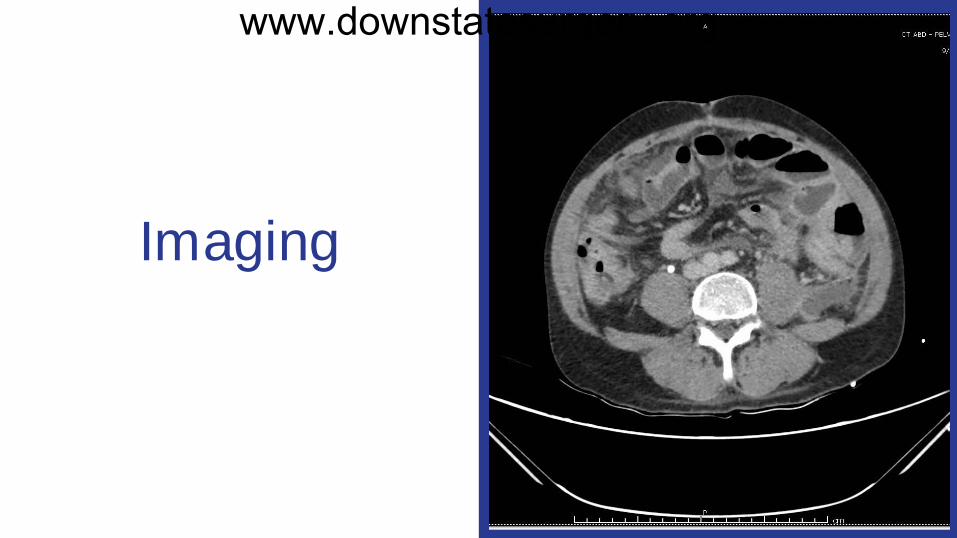
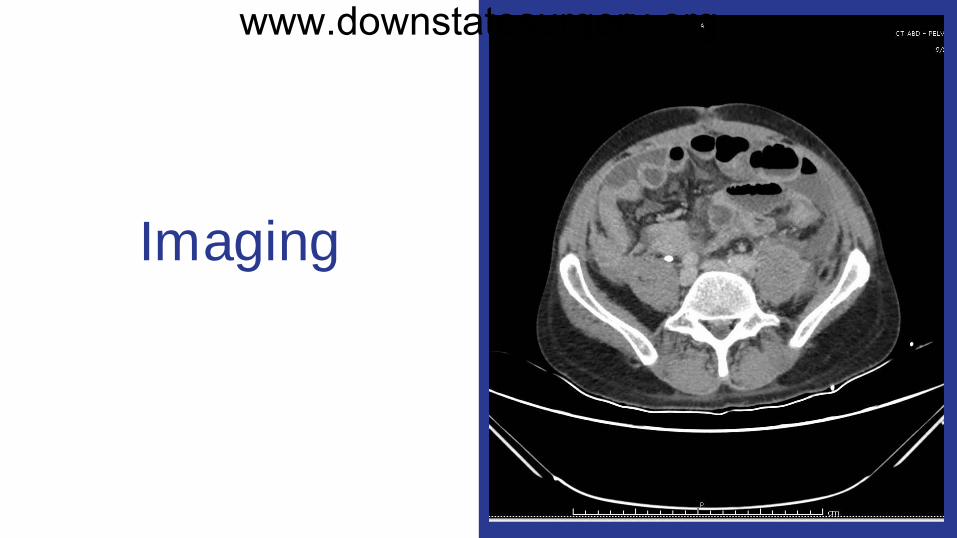
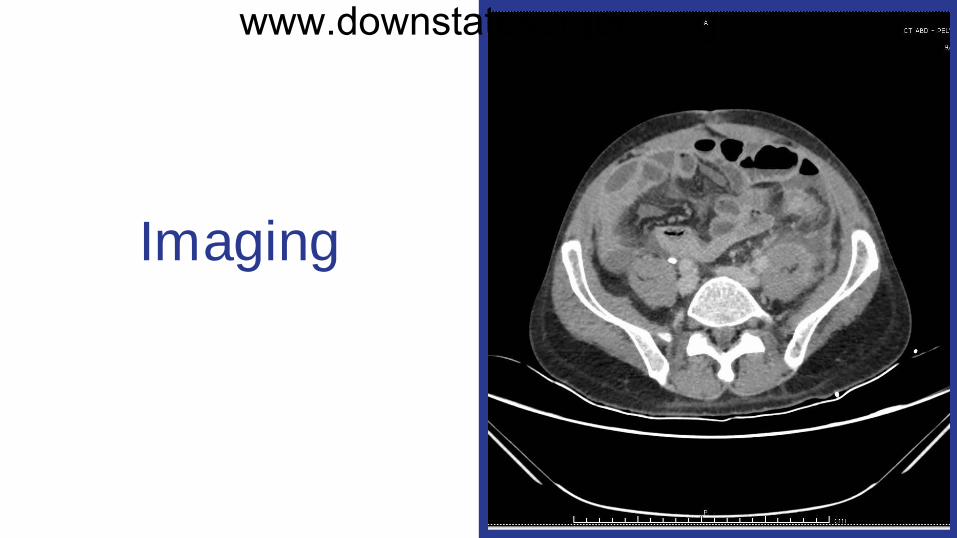
PE: Moderately distended, tender near incision site, wound had a 1 cm inferiorly which was being packed previously, serous drainage noted but no purulence Given 1L bolus and and Zosyn for presumed sepsis CT PE: negative for PE CT A/P: Small bowel obstruction likely secondary to adhesions. Small areas of pneumatosis intestinalis and portal venous gas, concerning for bowel ischemia. Free air and post surgical changes, compatible with known recent laparotomy.
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
Imaging
www.downstatesurgery.org
www.downstatesurgery.org
www.downstatesurgery.org
www.downstatesurgery.org
www.downstatesurgery.org
www.downstatesurgery.org
www.downstatesurgery.org
www.downstatesurgery.org
www.downstatesurgery.org
Hospital Course
HD # 1
Taken to OR for Exploratory Laparotomy, abdominal was hout, diverting loop ileos tomy creation, and pelvic drain placement
Findings : 1.5L of purulent/feculent fluid; multiple interloop abs ces s es
EBL: 50cc, IVF: 1500
POD # 1-2
Peritoneal fluid was pos itive for GNRs ; Zos yn was continued
NGT removed and patient advanced to clears
www.downstatesurgery.org
Hospital Course
POD # 4
WBC normalized, Micro res ulted with ESBL E coli, s witched to Meropenem
NPO for vomiting
POD # 5-6
Regular diet
Rehab cons ulted and recommended Acute rehab
POD # 8-12
J P drain removed
ID recommended 14 days IV Meropenem
Dis charged with VNS s ervices
www.downstatesurgery.org
Questions???
www.downstatesurgery.org
Peritonitis ● Inflammation of the peritoneal surface caused by irritants such a bile,
microorganisms, foreign bodies, or barium
www.downstatesurgery.org
Presenter
Presentation Notes
The main manifestations of peritonitis are acute abdominal pain, abdominal tenderness and abdominal guarding, which are exacerbated by moving the peritoneum, e.g., coughing (forced cough may be used as a test), flexing one's hips, or eliciting the Blumberg sign (a.k.a. rebound tenderness, meaning that pressing a hand on the abdomen elicits less pain than releasing the hand abruptly, which will aggravate the pain, as the peritoneum snaps back into place). A small amount of serous fluid is normally present in the peritoneal space, with a protein content (consisting mainly of albumin) of <30 g/L and <300 white blood cells (WBCs, generally mononuclear cells) per microliter.
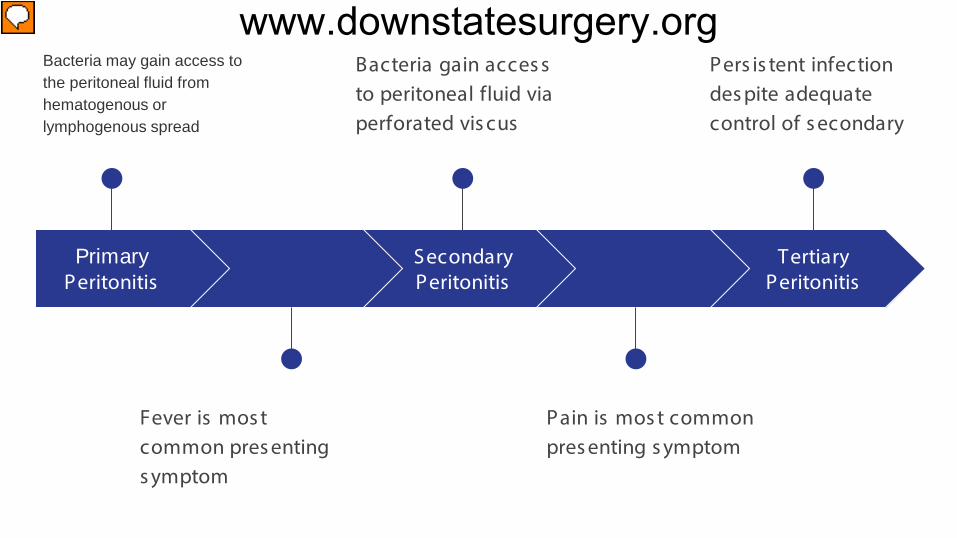
Primary Peritonitis
Bacteria may gain access to the peritoneal fluid from hematogenous or lymphogenous spread
Fever is mos t common pres enting s ymptom
Secondary Peritonitis
Bacteria gain acces s to peritoneal fluid via perforated vis cus
Pain is mos t common pres enting s ymptom
Tertiary Peritonitis
Pers is tent infection des pite adequate control of s econdary
www.downstatesurgery.org
Presenter
Presentation Notes
primary bacterial peritonitis (PBP) occurs most commonly in conjunction with cirrhosis of the liver (frequently the result of alcoholism). However, the disease has been reported in adults with metastatic malignant disease, postnecrotic cirrhosis, chronic active hepatitis, acute viral hepatitis, congestive heart failure, systemic lupus erythematosus, and lymphedema as well as in patients with no underlying disease. Although PBP virtually always develops in patients with preexisting ascites, it is, in general, an uncommon event, occurring in ≤10% of cirrhotic patients. The cause of PBP has not been established definitively but is believed to involve hematogenous spread of organisms in a patient in whom a diseased liver and altered portal circulation result in a defect in the usual filtration function. Organisms multiply in ascites, a good medium for growth. The proteins of the complement cascade have been found in peritoneal fluid, with lower levels in cirrhotic patients than in patients with ascites of other etiologies. The opsonic and phagocytic properties of PMNs are diminished in patients with advanced liver disease. Cirrhosis is associated with alterations in the gut microbiota, including an increased prevalence of potentially pathogenic bacteria such as Enterobacteriaceae. The most common manifestation for PBP is fever, which is reported in up to 80% of patients. Ascites is found but virtually always predates infection. Patients with ascites and fever, it is important to sample fluid. The finding of >250 PMNs/μL is diagnostic for PBP (exceptions for neutropenic patients), In PBP, a single organism is typically isolated; anaerobes are found less frequently in PBP than in secondary peritonitis, in which a mixed flora including anaerobes is the rule. In fact, if PBP is suspected and multiple organisms including anaerobes are recovered from the peritoneal fluid, the diagnosis must be reconsidered and a source of secondary peritonitis sought. Secondary: The organisms found almost always constitute a mixed flora in which facultative gram-negative bacilli and anaerobes predominate, especially when the contaminating source is colonic
www.downstatesurgery.org
Primary Peritonitis
Bacteria may gain access to the peritoneal fluid from hematogenous or lymphogenous spread
Fever is mos t common pres enting s ymptom
Secondary Peritonitis
Bacteria gain acces s to peritoneal fluid via perforated vis cus
Pain is mos t common pres enting s ymptom
Tertiary Peritonitis
Pers is tent infection des pite adequate control of s econdary
www.downstatesurgery.org
Presenter
Presentation Notes
Secondary: The organisms found almost always constitute a mixed flora in which facultative gram-negative bacilli and anaerobes predominate, especially when the contaminating source is colonic
www.downstatesurgery.org
www.downstatesurgery.org
www.downstatesurgery.org
Presenter
Presentation Notes
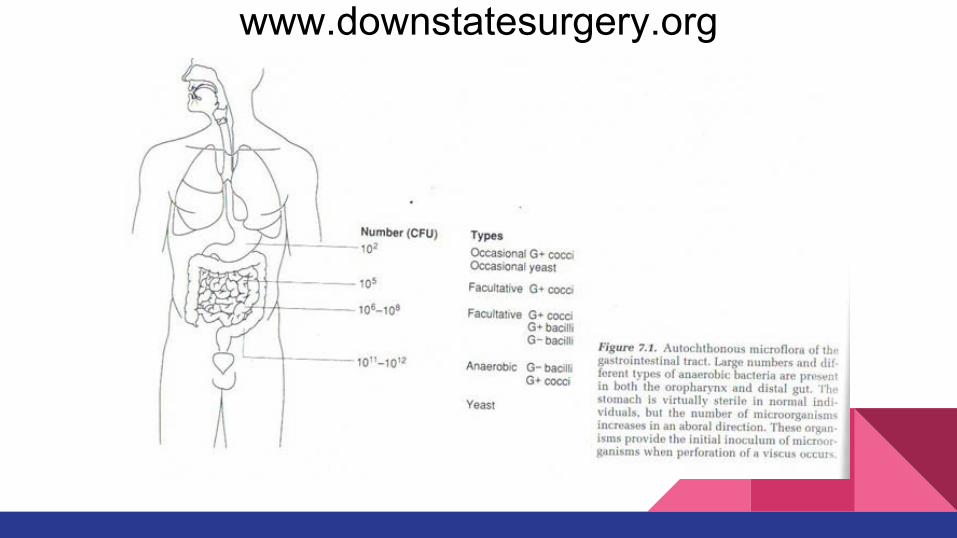
Gram-negative bacilli, particularly E. coli, are common bloodstream isolates, but Bacteroides fragilis bacteremia also occurs. The severity of abdominal pain and the clinical course depend on the inciting process. The organisms isolated from the peritoneum also vary with the source of the initial process and the normal flora at that site. Secondary peritonitis can result primarily from chemical irritation and/or bacterial contamination. For example, as long as the patient is not achlorhydric, a ruptured gastric ulcer will release low-pH gastric contents that will serve as a chemical irritant. The normal flora of the stomach comprises the same organisms found in the oropharynx but in lower numbers. Thus, the bacterial burden in a ruptured ulcer is negligible compared with that in a ruptured appendix. The normal flora of the colon below the ligament of Treitz contains ~1011 anaerobic organisms/g of feces but only 108 aerobes/g; therefore, anaerobic species account for 99.9% of the bacteria. Leakage of colonic contents (pH 7–8) does not cause significant chemical peritonitis, but infection is intense because of the heavy bacterial load.
Primary Peritonitis
Bacteria may gain access to the peritoneal fluid from hematogenous or lymphogenous spread
Fever is mos t common pres enting s ymptom
Secondary Peritonitis
Bacteria gain acces s to peritoneal fluid via perforated vis cus
Pain is mos t common pres enting s ymptom
Tertiary Peritonitis
Pers is tent infection des pite adequate control of s econdary
www.downstatesurgery.org
Presenter
Presentation Notes
Tertiary: can happen after any surgery for secondary: usually due to an array of host factors such as malnutrition; high APACHE II score, multi drug resistant organisms, immunocompromise. Surgical interventions have usually reached there limit in teritiary periotnitis (supportive care and antibiotics are mainstay therapy; but source control must be identified and affirmed) It is suspected that immunologic failure/paralysis is the primary cause of this process; defined as <30% HLA-DR monocytes activation. This decreased immunity causes a lack of host responsee and overwhlming sepsis.
Treatment
Primary: Antibiotics (Third gen Cephalos porin; Broad s pectrum PCN)
Secondary: Drainage (s urgical or percutaneous ) and definitive control of inciting agent
Tertiary: re operation often fails to reveal a s ource; newer s tudies us ing pro inflammatory s timulators (INF-Y or G-CSF) look promis ing
www.downstatesurgery.org
Presenter
Presentation Notes
Treatment for PBP is directed at the isolate from blood or peritoneal fluid. Gram’s staining of peritoneal fluid often gives negative results in PBP. Therefore, until culture results become available, therapy should cover gram-negative aerobic bacilli and gram-positive cocci. Third-generation cephalosporins such as cefotaxime (2 g q8h, administered IV) provide reasonable initial coverage in moderately ill patients. Broad-spectrum antibiotics, such as penicillin/β-lactamase inhibitor combinations (e.g., piperacillin/tazobactam, 3.375 g q6h IV for adults with normal renal function) or ceftriaxone (2 g q24h IV), are also options. Patients with PBP usually respond within 72 h to appropriate antibiotic therapy. Antimicrobial treatment can be administered for as little as 5 days if rapid improvement occurs and blood cultures are negative, but a course of up to 2 weeks may be required for patients with bacteremia and for those whose improvement is slow. Persistence of WBCs in the ascitic fluid after therapy should prompt a search for additional diagnoses. Secondary: Surgical can deal with 80% of events. Severe secondary dealt with either through staged laparotomies or open abdomen and continuous drainage