typhoid fever by pcr by dr. safia 2012.doc - pdfmachine ...mmc.gov.bd/downloadable file/typhoid...
TRANSCRIPT

Comparison of different test methods including
polymerase chain reaction for early and reliable
diagnosis of typhoid fever
Dr. Safia Sultana MBBS
Department of Microbiology Mymensingh Medical College
Mymensingh, Bangladesh January 2012
id971609 pdfMachine by Broadgun Software - a great PDF writer! - a great PDF creator! - http://www.pdfmachine.com http://www.broadgun.com
TO WHOM IT MAY CONCERN
This is to certify that Dr. Safia Sultana, a student of thesis part of M Phil (Microbiology) has
completed the thesis entitled �Comparison of different test methods including polymerase
chain reaction for early and reliable diagnosis of typhoid fever� in the Department of
Microbiology, Mymensingh Medical College under my guidance and supervision and this is
up to my satisfaction. Her protocol was approved by protocol approval committee of the
Department of Microbiology and Ethical review committee of Mymensingh Medical College.
Mymensingh December 05, 2011
Professor Dr. Md. Akram Hossain Head of the Department of Microbiology
Mymensingh Medical College Mymensingh, Bangladesh
Declaration
I hereby declare that the whole work submitted as a thesis entitled �Comparison of different
test methods including polymerase chain reaction for early and reliable diagnosis of
typhoid fever� in the department of the microbiology, Mymensingh Medical College, Dhaka
University, from July 2010 to June 2011 for the Degree of Master of philosophy is the result
of my own investigation and was carried out under the supervision of Professor Dr. Md.
Akram Hossain.
I, further declare this thesis or part thereof has not been concurrently submitted for the award
of any Degree or Diploma anywhere.
Dr. Safia Sultana Signature of the Candidate

ACKNOWLEDGEMENT
All praises belongs to Almighty Allah, the most merciful, the most beneficent and the most
kind for giving me the opportunity, courage and enough energy to carry out and complete the
entire thesis work.
I am very grateful and deeply indebted to my honourable teacher and guide Professor Dr. Md.
Akram Hossain, Head of the Department of Microbiology, Mymensingh Medical College. It
is my great pleasure to express my deepest regards and whole hearted indebtedness to him for
his inspiring encouragement, continuous guidance, active cooperation, constant supervision,
valuable suggestions, constructive criticism and help in carrying out this work successfully.
I am grateful and express thanks to the honorable members of the Ethical Review Committee
for giving kind approval to my research protocol. I am obliged to Professor Md. Aminul
Haque Principal of Mymensingh Medical College, Mymensingh for his kind permission to
conduct the thesis.
I would like to express my deepest regards and gratitude to my respected teacher Dr. Md.
Ashraful Alam, Assistant Professor, Department of Microbiology, Mymensingh Medical
College, Mymensingh, for his constructive criticism in correcting this thesis with his wise
advice and active cooperation in correcting the manuscript.
I owe my gratitude to respected teacher Md Chand Mahamud, Assistant Professor,
Department of Microbiology, Mymensingh Medical College, Mymensingh for valuable
advice and cordial cooperation.
I am cordially expressing my respect and complements to Dr. Shaymol Kumar Paul,
Assistant Professor, Department of Microbiology, Mymensingh Medical College,
Mymensingh, for his cordial cooperation, and thoughtful suggestions in my thesis work.
I also grateful to Professor Nobumichi Kobayashi, Sapporo Medical University of Japan for
providing with us primers of PCR and technical assistance for this study and also greatful to
Professor Jalaluddin Ashraful Hoque, Professor of BIRDEM and Ibrahim medical college for
sponsoring blood culture tube.
I owe my gratitude to Professor Abu Ahmed Saleh, Professor of microbiology, BSMMU, for
supplying reference strain of Salmonella typhi.
I like to express gratitude to all other teachers, M.Phil students, laboratory technologist and
other staffs of Microbiology department, Mymensingh Medical College, Mymensingh for
their constant help and sincere cooperation during the entire study period.
I also grateful to Alamin, for his active help in computer typing, data entry and sincere
cooperation during the entire study period. I like to express gratitude to Dr. Aklima Sultana,
medical officer of pathology, BSMMU for kind help in my study period.
I express my gratitude to my parent, who always inspired me for higher studies and is my
constant source of inspiration and encouragement in every step of my life.
I remained incomplete if I do not express whole hearted thanks and gratitude to my
husband Dr. Mohammed Abdoullah Al Maruf for sparing me so much time in this job from
all sorts of social and family responsibilities and sharing my pain and pleasure. I would like
to express my heartiest affection for my sons, Mikail Abid and Yousuf Aryan who had been
deprived of my care and attention during the thesis work.

I remained incomplete if I do not express wholehearted thanks and gratitude to my beloved
mother in law Jahanara Begum her blessings, affectionate support and spearing me so much
time in this job from all sorts of social and familial responsibilities.
Lastly I am indebted to all those persons from whom I have collected samples. May Allah
give them better rewards. Thanks again.
Mymensingh, January, 2012 Dr. Safia sultana
CONTENTS
Page No.
LIST OF TABLES VI

LIST OF FIGURES VII
LIST OF ABBREVIATIONS VIII
SUMMARY X
INTRODUCTION 1
CHAPTER 1: HYPOTHESIS 5
OBJECTIVES 6
CHAPTER 2: REVIEW OF LITERATURE 7
CHAPTER 3: MATERIALS AND METHODS 54
CHAPTER 4: RESULTS 68
CHAPTER 5: DISCUSSION 90
CHAPTER 6: CONCLUSION AND RECOMMENDATIONS 98
CHAPTER 7: LIMITATION 99
CHAPTER 8: LIST OF REFERENCES 100
CHAPTER 9: PHOTOGRAPH i
CHAPTER 10: APPENDICES xii
LIST OF TABLES
Table No. Title Page No.
1 Age group distribution of suspected cases of typhoid fever. 71
2 The socio-demographic characteristics of study population 73

3 Rate of isolation of S. typhi among study cases 76
4 Relationship of blood culture positivity with duration of fever
of the cases
77
5 Antibiotic usage by the blood culture-negative suspected
cases of typhoid fever
78
6 Results of ICT for identification of IgM antibody of S. typhi 81
7 Sensitivity and specificity of ICT for diagnosis of typhoid
fever.
83
8 Results of polymerase chain reaction (PCR) for identification
of flagellin gene of S. typhi
84
9 Comparison of culture and PCR methods for identification of
S. typhi
85
10 Sensitivity and specificity of blood culture in study population 88
11 Diagnostic accuracy of PCR for diagnosis of typhoid fever 89
LIST OF FIGURES
Figure No. Title Page No.
1 Presenting complaints by the suspected cases of typhoid
fever.
69
2 Age group distribution of study population 70
3 Sex pattern of study population. 72
4 Different test performed for diagnosis of typhoid fever. 75
5 Antimicrobial susceptibility pattern of the Salmonella
typhi isolates
79
6 Antibody detection among suspected cases by ICT
method.
82
7 Comparison of positivity of Blood culture and PCR for
diagnosis of typhoid fever.
86
LIST OF ABBREVIATIONS
ATCC American Type Culture Collection
BMAC Bone-marrow-aspirate culture
BP Base pair
CIE Counter current Immunoelectophoresis
CLSI Clinical and Laboratory Standards Institute
CMIR Cell-mediated immune responses
DDW Deionized distilled water
DNA Deoxyribonuclic acid
DSCC Duodenal string-capsule culture
DTH Delayed-type hypersensitivity response
EDTA Ethylene diamine tetraacetic acid
EIA Enzyme Immunoassay
ELISA Enzyme-linked immunosorbent assay
et al. et alia ( and others )
FAE Follicle-associated epithelium
GALT Gut-associated lymphoid tissues
HLA Human leucocyte antigen
ICDDRB International Center for Diarrrhoeal Diseses and Research Bangladesh,
ICT Immunochromatography test
IROMPs Iron-regulated outer-membrane protein
Kb Kilobyte
Kda Kilo dalton
LDC Lysine decarboxylase
LMI Leucocyte migration inhibition test
MDR Multidrug resistant
MDRTF Multi Drug Resistant typhoid fever
MHC Major Histocompatibility Complex
OMPs Outer membrane proteins
PCR Polymerase chain reaction
PPs Peyer's patch
rEPA Recombinant Pseudomonas aeruginosa exotoxin
RPHA Reverse Passive Haemagglutination assay
Rpm Rotation per minute
SIADH Syndrome of inappropriate release of antidiuretic hormone
SPI Salmonella pathogenecity island
SPS Sodium polyanethol sulfonate
SPV Salmonella plasmid virulence
Taq Thermus aquaticus
TBE Tris/Borate/EDTA
TTSSs Type III Secretion Systems
USDA The United States Department of Agriculture
VICPS Capsular polysaccharide vi antigens

SUMMARY
Background
Typhoid fever, caused by Salmonella typhi, is an important cause of morbidity and mortality
among all age groups in many developing countries including Bangladesh. A rapid and
reliable method for the detection of S. typhi is essential for early diagnosis. The blood culture
though less sensitive and technically demanding is the gold standard method for diagnosis of
typhoid fever. In addition, the disease is diagnosed serologically by the Widal test and other
methods, which have limitations of sensitivity and specificity. The most promising recently
published method is polymerase chain reaction (PCR) based amplification of DNA from the
blood samples of typhoid fever patients.
Objective
Keeping in mind the above considerations, the study was designed- (i) to detect IgM antibody
to S. typhi specific antigen by Immunochromatographic (ICT) method, (ii) to isolate the S.
typhi by lytic centrifugation method of blood culture and (iii) to detect flagellin gene of S.
typhi using appropriate primers by a nested PCR directly from blood sample.
Methodology
The study was carried out in the department of Microbiology, Mymensingh Medical College,
Mymensingh between July, 2010 and June, 2011 including 200 individuals of different age
and sex. Of them, 150 were clinically suspected cases of typhoid fever and 25 were febrile
non-typhoid controls, and remaining 25 were apparently healthy controls. Specimens of
whole blood were collected from each of the cases and controls following universal safety
precautions. The collected samples were tested by culture, ICT and PCR and then results
were analyzed using appropriate statistical methods.
Results
Among the 150 suspected typhoid fever cases, PCR showed maximum positive result 133
(88.7%) followed by ICT for IgM 106(70.7%) and blood culture 23(15.3%). All culture
positive cases were positive by PCR and among 127 culture negative cases, 110(86.5%) were
also positive by PCR. Neither of the controls was positive by PCR or blood culture. At first
week of illness, out of 23 culture positive samples, 14 were positive by the ICT (IgM). Out of
127 cultures negative cases 92 were positive by ICT (IgM). The sensitivity, specificity of
PCR (100%, 100%) using blood culture as gold standard and ICT (77.4%, 82.3%) using PCR
as a gold standard was calculated.
Conclusion
In the present study, the PCR appears to be highly sensitive and specific and superior to
blood culture. So it is recommended to take necessary steps for setup and start PCR at least in
the tertiary care hospitals. The ICT remains one of the easily accessible, cheap and simple
method with moderate sensitivity for the diagnosis of typhoid fever, especially in the resource
poor countries like Bangladesh. Analyzing the findings of the study it is concluded that ICT
and PCR are the suitable methods for diagnosis of typhoid fever.

Introduction
Typhoid fever, caused by Salmonella typhi, is widely recognized as a major public health
problem in many developing countries. The disease emerged as an important infectious
disease in the early 19th century. It is endemic in the Indian subcontinent including
Bangladesh, South-East and Far- East Asia, the middle East, Africa, central and South
America (Jenkins and Gillespie 2009). It is a systemic infection and is transmitted through
the faecal oral route by the consumption of contaminated water and food, particularly raw or
undercooked meat, poultry, eggs and milk. The consumption may occur either directly from
person-to-person or by ingestion of food or water contaminated with faeces or urine carrier as
well as through flies (Singh 2001). The disease may occur in all ages, with the highest
incidence found particularly in children (Anggraini, Handoyo and Aryati 2004). In addition
infection is most common in young children and elderly with peak incidence in summer and
fall (Jerrold and Turner 2010). It is therefore, presumed that typhoid fever is a major health
problem in all those parts of the world where safe drinking water and sanitation is inadequate.
There was an estimation that typhoid fever caused more than 21 million illnesses and more
than 216,000 deaths in the world during 2000 (Crump, Luby and Mintz 2004). A previous
study from Pakistan in 2006 revealed an incidence rate of 170/100,000 (using blood culture)
whereas a serology based incidence rate was 710/100,000 (using Typhidot) (Siddiqui et al.
2006). The incidence of cases of bacteraemic typhoid fever in Bangladesh per year was found
390/100,000 in 2001. In the same investigation, the incidence of typhoid fever among the
children per year was 210/100,000 children of >5 years of age and 1870/100,000 of <5 years
of age (Brooks et al. 2005).
Enteric fevers including typhoid fever occur only in the humans, which may turn into a
severe infection progressing to complications and death. Persons with typhoid fever carry the
causative agent S. typhi in their bloodstream and intestinal tract. S. typhi is uniquely adapted
to humans and carriers represent the sole source of these organisms for a short period of time
(convalescent carrier) or chronic carriers who shed the organism for longer than 1 year
(Zwadyk 1992).
Since all the signs and symptoms of typhoid fever are nonspecific, a definitive diagnosis of
the disease depending on the clinical presentation alone is very difficult. Therefore,
laboratory-based investigations are essential for supporting the diagnosis of typhoid fever.
Several different techniques are used for the diagnosis of the disease. The �gold standard� for
diagnosis of typhoid fever is the isolation of S. typhi from appropriate samples including
blood, bone marrow aspirates, stool, urine and rose spots (Gasem et al. 1995; Wain et al.
2001). A lytic centrifugation technique of blood culture has some added advantage over
conventional method to reduce the isolation time (Old 2006; Betly et al. 2010). Serologic
diagnostic tests for typhoid fever by immunochromatographic test (ICT) are good alternatives
(Bhutta and Mansurali 1999) and PCR identification of the S. typhi specific gene (e,g-
flagellin gene) are the better techniques.
Drug resistance in S. typhi is of considerable importance to both clinicians and
microbiologists and poses a major problem for public health authorities. The emergence of
antibiotic resistant strains of the bacteria is closely linked to the irrational use of antibiotic in
treating human infections; especially ciprofloxacin resistance to commonly used antibiotics
such as chloramphenicol, ampicillin and cotrimoxazole has been reported from different parts
of world including India (Gautam et al. 2002). A study in Bangladesh reported showed a
gradual change in resistance to ampicillin and cotrimoxazole among S. typhi. In the same
study, the rate of resistance to cotrimoxazole, ampicillin and chloramphenicol decreased from
59.6 to 5.6% of the organisms over a 3 years period (Asna and Haq 2000). For this reason,

antimicrobial susceptibility test is essential to see the changing trend of antibiogram of
circulating strains in the community.
In the perspective of Bangladesh, it is presumed that the diagnosis of typhoid fever is usually
based on clinical presentation as well as Widal test, both of which are associated with
numerous limitations. The diagnosis of typhoid fever on clinical presentations alone is
difficult, as the presenting symptoms are diverse and similar to those observed with other
febrile illnesses, especially during the first weeks of the infection (Jenkins and Gillespie
2009). On the other hand, ICT method for detection of S. typhi antibodies is a simple and
rapid diagnostic test. The test simultaneously detects and differentiates the IgG and IgM
antibodies to S. typhi specific-antigen in whole blood (Ismail, Kader and Ong 1991). The
detection of IgM reveals acute typhoid fever in the early phase of infection, the IgG detection
reveals late phase as well as the carriage of infection, while the detection of both IgG and
IgM suggests acute typhoid in the middle phase of the infection (Saha et al. 1999; Choo et al.
1999).
The development of molecular methods for diagnosis of infectious diseases, including
typhoid fever has improved the sensitivity and specificity of diagnosis. One of the molecular
methods, Polymerase chain reaction (PCR) is the most sensitive and rapid method to detect
microbial pathogens in clinical specimens (Massi et al. 2003). In particular, when the specific
pathogen is difficult to culture in vitro or requires a long cultivation period, the diagnostic
value of PCR appears very significant (Kumar et al. 2002). Among the various PCR
techniques, nested PCR assay was used in the early diagnosis of typhoid fever (Prakash et al.
2005). The nested PCR has good potential to be a rapid tool for the definitive diagnosis of
typhoid fever and is superior to conventional methods of PCR (Ali et al. 2009). The nested
PCR had greatest diagnostic value for detection of S. typhi among all the diagnostic tests used
and also had higher efficacy in detecting the disease than other methods like the Widal test,
blood and urine cultures (Ambati, Nath and Das 2007).
The present study was designed to identify the cases of typhoid fever employing the
techniques of blood culture, serology and molecular methods keeping in mind the commonly
occurring problems and to overcome them. For this reason, blood culture was done by lytic
centrifugation method to cut short the length of isolation of S. typhi. Antimicrobial
susceptibility test was done in the present study to see the susceptibility pattern of circulating
strains in Bangladesh. The ICT method has been shown to be cheap, less time-consuming,
applicable for field use, easy to perform and highly sensitive and specific for detection of
antibodies in patients with typhoid fever. Considering this, the ICT method was applied for
the detection of S. typhi specific IgM antibodies in blood samples of the present study. The
nested PCR method was included in the present study as a tool for diagnosis of typhoid fever
and was compared to blood culture and serology.

Hypothesis
Polymerase chain reaction is highly sensitive, specific and superior to other available
methods for diagnosis of typhoid fever.

Objectives
General Objective:
To compare different test methods including polymerase chain reaction (PCR) for early and
reliable diagnosis of typhoid fever.
Specific objectives:
1. To isolate S. typhi by lytic centrifugation method of blood culture and to test
antimicrobial susceptibility of S. typhi isolates by disk diffusion method.
22.. To detect IgM and IgG antibodies to S. typhi-specific antigen by
immunochromatographic test (ICT).
3. To detect flagellin gene of S. typhi by a nested polymerase chain reaction from blood
samples.
4. To compare results of the test methods used for diagnosis of typhoid fever.
Review of literature
Typhoid fever caused by Salmonella typhi is a disease of global distribution. It is
characterized by insidious onset of sustained fever, headache, malaise, anorexia, relative
bradycardia, constipation or diarrhoea, and nonproductive cough. Epidemics are more
common in spring and summer; sporadic in other seasons (CDC 1997; Crum 2003). It is
continues to be a health major problem in many developing countries where there is poor
standard of personal hygiene and prevalence of contaminated food, safe drinking water and
sanitation is inadequate (Lifshitz 1996; House et al. 2001).
Background and history of typhoid fever
Until the first quarter of the 19th century, typhoid fever was not recognized as a separate
clinical entity and was often confused with other prolonged febrile illness of typhus fever of
rickettsial origin. �Typhos in Greek means smoke and typhus fever got its name from smoke
that was believed to cause it. Typhoid means typhus like and thus the name was given to this
disease. Although typhoid fever was first discovered by Willis in 1643 (cited in collier�s
Encyclopedia 1989), it was mistakenly understood to be typhus fever for a long time. Gerhard
in 1837 (cited in collier�s Encyclopedia 1989), distinguished the two illnesses and invented
the name typhoid fever which means typhus like fever. The causative organism was
visualized in tissue sections from Peyer�s patches and spleen of infected patients by Ebertt in
1880 and named it as Salmonella typhosum and was grown in pure culture by Gaffky in 1884
(Topley and Wilson 1990).
The significance of water contamination in the spread of the disease was first recognized by
Budd in 1856. As a young practitioner in North Devon (is a local government district in
Devon, England) his observations provided one of the greatest milestones in the development

of hygiene. He for the first time proved that the disease is infectious and spread through
patients� faeces. He further discovered that milk and water played an important role in the
transmission of typhoid fever (Topley and Wilson 1990).
Mary Mallon also known as Typhoid Mary was the first person in the United States to be
identified as a healthy carrier of typhoid fever. She became the first American carrier to be
identified and traced. She was a cook in New York. Some believed she was the source of
infection for several hundred people. Over the course of her career as a cook, she is known to
have infected 53 people, three of whom died from the disease. Public health authorities told
Mary to give up working as a cook or have her gall bladder removed; Mary quit her job but
returned later under a false name. She was detained and quarantined after another typhoid
outbreak. Mallon spent the rest of her life in quarantine. Six years before her death, she was
paralyzed by a stroke. On November 11, 1938, aged 69, she died of pneumonia. She was still
infectious on the day of her death. An autopsy found evidence of live typhoid bacteria in her
gallbladder. Her body was cremated; the ashes were buried at Saint Raymond's Cemetery in
the Bronx (Wikipedia 2011).
Epidemiology
Mode of transmission
Typhoid fever is a systemic infection caused primarily by S. typhi and is transmitted through
the fecal oral route by the consumption of contaminated meat, poultry, eggs and milk.
Infection is most common in young children and elderly with peak incidence in summer and
fall (rainy season) (Jerrold and turner 2010). The infection is transmitted by ingestion of food
or water contaminated with faeces. The disease is transmitted by either directly through hands
soiled with faeces or urine of cases or carriers or indirectly by ingestion of contaminated
water, milk, food or through flies. Contaminated ice, ice-cream and milk products are rich
sources of infection (Singh 2001).
Two hospital based case-control studies from Vietnam found that risk of infection was related
to recent contact with a typhoid infected person, lack of education and drinking untreated
water (Luxemburger et al. 2001; Tran et al. 2005).
Depending on age, 1% - 5% of patients become chronic carriers, harbouring S. typhi in the
gall bladder (WHO 2003). Chronic typhoid carrier status may be responsible for the
endemicity and outbreaks of the disease in the region. High prevalence of typhoid carriers
occurs in patients with biliary, gastrointestinal and other related disease (Vaishnovi et al.
2005).
World wide distribution
Typhoid fever caused by S. typhi is widely recognized as a major public health problem in
many developing countries. The disease is endemic in the Indian subcontinent including
Bangladesh, South-East and Fareast Asia, the Middle East, Africa, Central and South
America (Jenkins and Gillespie 2009).
Crump et al. estimated the global burden of typhoid fever and showed that 21.6 million cases
of illnesses and 0.2 million cases of death were by typhoid fever during 2000 (Crump, Luby
and Mintz 2004). They also identified the regions with high incidence of typhoid fever
(>100/100000 caser per year) including South-East and South-central Asia. Other regions of
medium incidence (10-100/100000 cases/per year) included rest of Asia, Africa, Latin
America, the Caribbean and Oceania (except Australia and New Zealand) and region low
incidence (<10/100000 cases/year) of typhoid fever included Europe, North America and
the rest of the developed world. In contrast to that seen in rich countries, typhoid fever
remains an important cause of illness in developing world where annual incidences in Papua
New Guinea and Indonesia may reach 1200/100,000 population (Crump, Luby and Mintz
2004).
It is commonly observed that the majority of patients, 60% - 90% are treated as out patients
and therefore, hospital based studies was underestimate true incidence. The annual typhoid
incidence (per 100,000 person years) among 5-15 year-olds age group varied from 24.2 and
29.3 in sites in Viet Nam and China, respectively, to 180.3 in the site in Indonesia; and to
412.9 and 493.5 in sites in Pakistan and India, respectively (Ochiai et al. 2008). In a study
during 2000-2001 among children in an urban slum Bangladesh, the overall incidence of
typhoid fever was 390 cases per 100,000 populations per year. The incidence among >5 years
was 210 per 100,000 per year and among children <5 years the rate was 1870 per 100,000 per
year (Brooks et al. 2005).
Another study conducted by Sinha et al. 63 culture-positive typhoid fever cases were
detected. The incidence rate of typhoid per 1000 person-years was 27.3 at age under 5 years,
11.7 at 5-19 years, and 1.1 between 19 and 40 years. The difference in the incidence of
typhoid fever between those under 5 years and those aged 5-19 years was significant (Sinha
et al. 1999).
The organism Salmonella typhi
Historical background
The genus Salmonella was named after Daniel Elmer Salmon, an American veterinary
pathologist. Although Theobald Smith was the actual discoverer of the bacterium (Salmonella

enterica Var. cholerasuis) in 1885. As Dr. Salmon was the administrator of the United States
drug administration (USDA) research program, and thus the organism was named after him.
Smith and Salmon had been searching for the cause of common �hog cholera� and proposed
this organism as the causal agent. Later research, however, showed that this organism (now
known as Salmonella enterica) rarely causes enteric symptoms in pigs and was thus not the
agent they were seeking (Which was eventually shown to be a virus). However related
bacteria in the genus Salmonella were eventually shown to cause other important infectious
diseases (Wikipedia 2011).
Salmonella Nomenclature:
Salmonella nomenclature is complicated. Initially each Salmonella species was named
according to clinical consideration e,g. S. typhimurium (mouse typhoid fever), S. Cholerasuis
(hog cholera) (Kauffmann 1941)(Cited in Wikipedia 2011). Later, molecular findings led to
the hypothesis that Salmonella consisted of only one species (Leminor and Popoff 1987).
The terminology introduced by White and modified by Kauffman accorded specific rank to
each antigenically distinguishable Salmonella type and the convention was established that
each new type should be named after the place in which it was first isolated. The first
published table contained some 20 serotypes. The current number in about more than 2500
serotypes (Moreno et al. 2009).
The antigenic formulae of Salmonella serotype are defined and maintained by the World
Health Organization (WHO) collaborating centre for Reference and Research of Salmonella
at the Pasteur institute, Paris, France, and new serotype have been listed in annual updates of
the Kauffman�White scheme (Popoff, Bockemüh and Brenner 2000).
Morphology
These are Gram negative, motile, non spore forming, non capsulated bacilli measuring 2-4 x
0.6 µm. Most strain are motile due to presence of peritrichous flagella except S. gallinarum
and S. pullorum which are non motile. They may possess fimbriae (Chacraborty 2003). Most
strains of most serotypes form type 1 fimbriae (Mannose � Sensitive, haemagglutinating); S.
gallinarum, S. pullorum and a few strains of other serotypes form type2 fimbriae (non-
haemagglutinating) and most S. paratyphi A strains are non-fimbriate. S. typhi also
synthesizes type IV pili and such pili are important in adherence to or invasion of human
intestinal cells (Zhang et al. 2000).
Antigenic structure of Salmonella typhi
The O and H antigens are the major antigens used to serotype the Salmonella. The O antigens
are Similar to the O antigens of other Enterobacteriaceae but H antigens are different in that
they are diphasic. i.e, the H antigens can exist in either of two major antigenic phases. Phase
1 (Specific phase) and phase 2 (non specific phase). Phase 1 antigens are shared by only a
few organisms and react only with homologous antigens but phase 2 antigens are shared by
many organisms and react with heterologous antisera (Zwadyk 1992).
O antigens or somatic antigens
The O antigens are the most surface exposed lipopolysaccharide (LPS) component and
displays enormous structural variability, resulting in a large variety of serotypes (Reeves
1993). These somatic antigens represent the side-chains of repeating sugar units projecting
outwards from the lipopolysaccharide layer on the surface of the bacterial cell wall.
The O antigens are heat stable being unaffected by heating for 2.5 hour at 1000c and alcohol
stable. The O antigens are unaffected by suspension of the bacteria in 0.2% formaldehyde
(Old 2006). Antibodies to O antigens are predominantly IgM and tend to agglutinate O
antigens in granular masses. The presence and proper Chain length distribution of the O
antigens polysaccharide are essential for serum resistance of S. typhi but not for invasion of
epithelial cells (Hoare et al. 2006).
H (Flagellar) Antigens
These antigens represent determinant groups on the flagellar protein. They are heat�labile
and alcohol labile, but are well preserved in 0.04 � 0.2 % formaldehyde. Heating at
temperature above 600C detaches the flagella from the bacteria and detachment of all flagella
is achieved by heating for 30 minute at 100°c. The deflagellated bacteria are inagglutinable
by H antibodies but the detached flagella remain immunogenic and suspensions of bacteria to
be used for the production of O antisera should be freed from detached flagella by
centrifugation and washing or by inactivation by heating for 2.5 hour at 1000C (Old 2006).
Vi � antigen
S. typhi also produces a group 1 exopolysaccharide known as the vi antigen; which is made of
a homopolymer of high molecular mass (Virlogeux and Popoff 1996) and form a capsular
structure. The vi antigen is found in virtually all clinical isolates from patients with acute
typhoid infection. It protect S. typhi against complement mediates lysis as well as
phagoaytosis (Kossack et al. 1981).
M antigens
It is a loose extracellular polysaccharide slime consisting of colanic acid. It occurs in a
serologically similar form in various unrelated enterobacteria, including serotypes of S. typhi
and many stains of E. coli and resembles the vi antigen in preventing agglutination by O
antibodies (Old 2006).
R antigens

In S-R mutation the O antigens are lost and new R antigens revealed at the bacterial surface.
The R variant bacteria tend to out grow the parenteral S bacteria during serial culture in the
laboratory. They form rough colonies, and are autoagglutinable in saline and sensitive to
killing by complement because they are autoagglutinable and lack serotype specificity, they
are unsuitable for serologic tests (Old 2006).
Fimbrial antigens
The type 1 fimbriae formed by most strains of S. typhi bear antigens that determine
agglutination by sera containing anti-fimbrial antibodies. Fimbriae are not found in young (6-
24 hours old) broth cultures, but can be found in 24-48 hours old broth cultures (Old 2006).
Determinants of pathogenecity
Whether an infection with S. typhi leads to a disease largely depends on the virulence of the
strain and the constitution of the host. The virulence of the strain is determined by So-called
virulence factors. S. typhi is a complex organism that produces a variety of virulence factors.
These include surface antigens, factors contributing to invasiveness, endotoxin, cytotoxin and
enterotoxin (Zwadyk 1992).
Whereas a number of virulence factors of S. typhi have been identified only recently, others
have been studied for decades. These latter virulence factors i, e, virulence plasmids, toxin,
fimbriae and flagella are therefore referred to as classic virulence factors (Asten and Dijk
2005).
Surface Antigen
a) O antigen
The ability of S. typhi to attach to host receptors cells and to survive intracellularly may be
due to O antigenic side chain. The O antigen of S. typhi apparently is important in
determining the susceptibility of some serotypes to complement, to host cationic proteins and
to an interaction with host macrophages. Organisms with intact O antigens are more resistant
to the complement mediated killing of normal serum. The resistance to killing by normal
serum probably is due to the shielding of the complement activating lipid A and LPS core
polysaccharides by the polysaccharides of the O antigen (Zwadyk 1992).
b) Vi antigen
The capsular polysaccharide vi antigens (VICPS) is an essential virulence factor and also a
protective antigen of S. typhi (Tang et al. 2003). The vi antigen is found in virtually all
clinical isolates from patients with acute typhoid infection. It protects S. typhi against
complement mediate lysis as well as phagocytosis (Kossack et al. 1981).
c) Fimbrial antigen
S. typhi synthesizes type IV pilli and such pilli are important in adherence to or invasion of
human intestinal cells (Zhang et al. 2000).
d) Outer membrane protein (OMP)
Act as virulence factor such as 55 KDa outer membrane protein from short chain fatty acids
exposed to S. typhi induces apoptosis in macrophages (Chander et al. 2006).
Invasive ness
Unlike most bacteria, which rely on receptor mediated endocytosis to invade a target cell, S.
typhi utilizes a complex process known as bacterial mediated endocytosis, where bacterial
proteins enter the host cell and manipulate signaling cascades that control cytoskeletal

architecture membrane trafficking and gene expression, all of which force the host to
endocytose S. typhi (Ohi and Miller 2001).
The target cell for S. typhi is the macrophage. The ability of S. typhi to survive in
macrophages is due to the production of bacterial proteins that enable the organism to
withstrand both the oxygen-dependent and the non oxygen-dependent killing mechanisms of
these professional phagocytic cells. The oxygen-dependent mechanisms include the
production of hydrogen peroxide and super oxide. The oxygen independent mechanisms
include the production of antibacterial, cationic proteins known as defensins (Zwadyk 1992).
Endotoxin
Endotoxin may play a role in the pathogenesis of S. typhi infections, especially during the
bacteremic stages of typhoid fever. The fever is produced by the endotoxin acting directly
and indirectly through the release of endogenous pyrogens from leukocytes. Endotoxin
activation of the chemotactic properties of the complement system may cause the localization
of leukocytes in the classic lesions of typhoid fever (Chakraborty 2003).
Virulence plasmid
Certain Salmonella carry a large, low copy number plasmid that contains virulence genes.
Virulence plasmids are required to trigger systemic disease; their involvement in the enteric
stage of the infection is unclear. Salmonella virulence plasmids are heterogeneous in size (50-
90kb), but all share a 7.8 kb region, SPV, required for bacterial multiplication in the
reticuloendothelaial system (Rotger and Casadesus 1999).
Cultural Characteristics
Salmonellae are aerobic and facultatively anaerobic. They grow on simple laboratory media
in temperature range 150c - 450c, optimally at 370c, and require enrichment of the minimal
medium with one or more amino acids or vitamins e.g, cystin or Nicotinamide; most S. typhi
strains require tryptophan (Old 2006).
On Nutrient agar
The colonies of most strains are moderately large 2-3 mm in diameter after 24 hours at 370c.
They are grey white, Moist Circular discs with a smooth convex surface and entire edge (Old
2006).
On Blood agar
S. typhi produce grey white 2-3 mm in diametre colonies. Some strain produce mucoid
colonies (Cheesbrough 2010).
Peptone water and Nutrient broth
In liquid media most strains give abundant growth with uniform turbidity. A thin surface
pellicle usually forms on prolonged incubation, Rough (R) variants, which have a
hydrophobic a granular deposit and a thick pellicle (Old 2006).
Mac Conkey�s agar
After 18-24 hour at 370c the colonies are pale yellow or nearly colour less, 1-3 mm in
diameter and easily distinguished from the pink red calories of lactose fermenting commensal
coliform bacilli e.g. � Escherichia coli (Richard and Thompson 2007; Cheesbrough 2010).
Salmonella � Shigella agar (SS agar)
SS agar is highly selective medium formulated to inhibit the growth of most coli form
organisms and permit the growth of species of Salmonella and shigella from environmental
and clinical specimens. The high bile salts concentration and sodium citrate inhibit all Gram
positive bacteria and many Gram negative organisms, including coliforms (Old 2006).
Enrichment media
These are liquid media used to assist the isolation of S. typhi from faeces, sewage, food stuffs
and other materials containing a mixed bacterial flora. The enriched culture is placed on
selective and/or differential media, usually after 24 hours of incubation (Richard and
Thompson 2007; Cheesbrough 2010).
Tetrathionate broth
Enriches S. typhi and sometimes shigellae but permits the growth of proteus species.
Selenite F broth
It is the most commonly used enrichment medium for specimens that may contain either
salmonella or shigellae. It is excellent for S. typhi and S. Dublin. It is not suitable particularly
for isolation of S. paratyphi A and S. choleraesuis (Old 2006; Richard and Thompson 2007).
Immune response
The nature of protective immunity in typhoid fever in man is not well understood. The
development of the humoral immune response to O, H, and Vi antigens of S. typhi has been
regularly demonstrated during and after typhoid fever as well as after TAB vaccination
(Kumer et al. 1774).
The development of specific humoral antibody response as well as CMIR in patients with
typhoid fever at various stages of their illness. These immune responses are correlated with
the clinical picture and specific CMIR give protection against typhoid fever (Sarma et al.
1977).
Cell mediated immune response (CMIR)
The cell-mediated immune response in typhoid fever develops almost invariably during the
second week of illness in uncomplicated cases while it was often negative in complicated
cases (Sarma et al. 1977).
Cell-mediated immunity was assessed by the leucocyte migration inhibition tests (LMI), and
developed in all cases with typhoid fever. Positive LMI was evident in the first week of the
illness and was maintained during the evolution of disease and in some patients was still
present after a year. It also developed at the end of 3 weeks in TAB vaccinated subjects
(Dham and Thompson 1982). Positive LMT is associated with good clinical recovery (Sarma
et al. 1977).
A studies have shown that, iron-regulated outer-membrane protein (IROMPs) expressed by
S.typhi induce a cellular immune response against infection through Th1 and Th2 type cells
(Sood et al. 2005). The cellular immune response induced by IROMPs resulted in an
enhanced DTH (delayed-type hypersensitivity response) and exhibited a significant increase
the ratio of CD4+/CD8+ cells and increased production of interleukin (IL-2) and interferon
(IFN) in early period and in the late period of the study, increased production of IL-
4_producing cells. The increase in the lymphocytes in Peyer�s patches (PPs) might have
caused the increase in the secretory immunoglobulin A (sIgA). Therefore, it is speculated that
immunization with IROMPs may evoke peripheral as well as mucosal immunity against S.
typhi infection (Sood et al. 2005). The uncomplicated cases of typhoid fever were found to
have and intact CMIR as compared to the complicated cases (Rajagoplan, Kumar and
Malaviya 1982).
Humoral immune response

The humoral response to S. typhi is important for protective immunity against typhoid fever,
as indicated by the protection obtained with killed cell vaccines and component vaccines
(outer membrane proteins, Vi antigen) in animals and human beings (Aron et al. 1993).
Although antibodies to S. typhi O, H, and Vi antigen appear to be involved in protection
against S. typhi infection, it is unknown whether such antibodies mediate protection, act in
conjunction with other adaptive responses, or serve as a surrogate for the presence of other,
more dominant protective immune responses e.g. cell-mediated immunity (Sztein 2007).
Anti-O-polysaccharide chain antibody titres are lower at the first week and increase up to the
third week of the infection. On the other hand, antilipid A antibody levels, which are already
higher at the beginning of the disease, progressively augment during the following weeks
(Mastroianni et al. 1989).
The antibodies and cellular reactively developed almost simultaneously but there was no
correlation between the agglutination titres and LMI positivity. Typhoid patients also showed
significantly raised serum IgM and IgA levels and increased concentrations of secretory IgA
in their saliva (Dham and Thompson 1982). The antibodies appeared after the 1st week of
illness and the titres gradually increased during the following days. Chloramphenicol therapy
did not interfere with antibody production and antibody titres did not correlate with the
severity of typhoid fever (Sarma et al. 1977).
S. typhi IROMP have also been observed to have immunogenic potential and are able to
stimulate antibody-mediated protection at systemic and mucosal levels (Sood et al. 2005). For
protection against Salmonella spp. both antibody and cell-mediated immune (CMI) responses
are considered to be important. The O antigen (O9, 12 serotype) is most relevant to protection
against typhoid fever; other antigens include the virulence capsule antigen and some outer
membrane proteins (Viret et al. 1999).
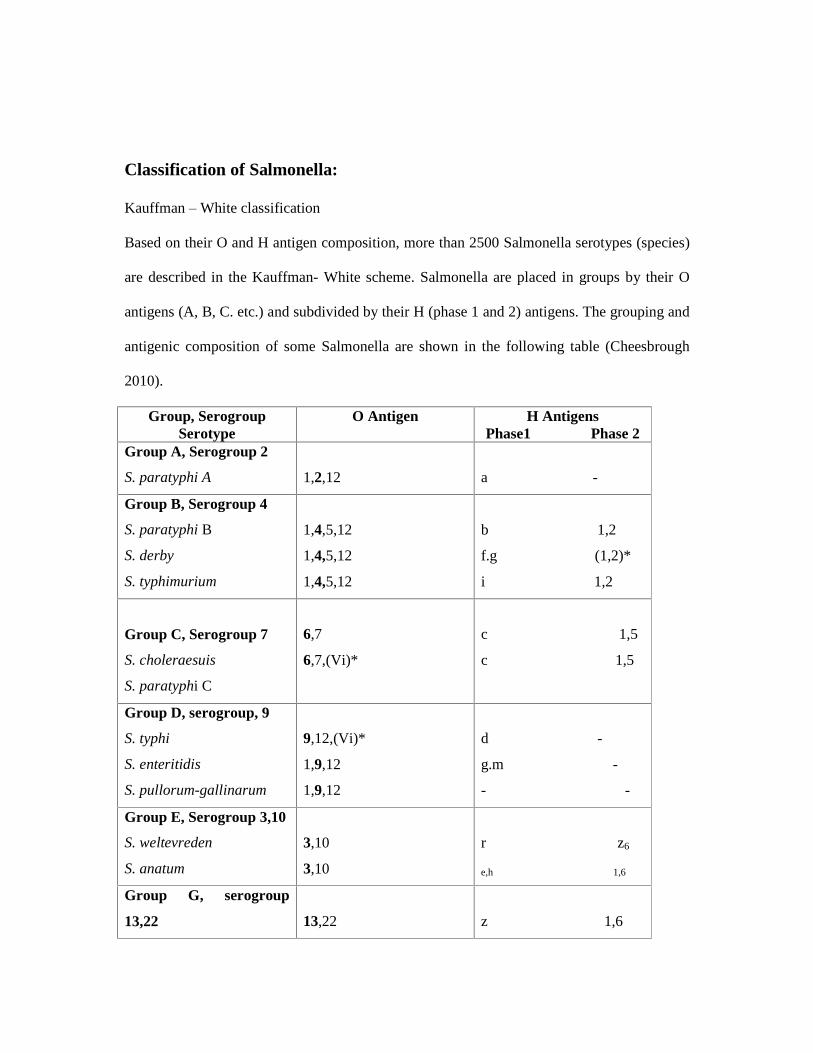
Classification of Salmonella:
Kauffman � White classification
Based on their O and H antigen composition, more than 2500 Salmonella serotypes (species)
are described in the Kauffman- White scheme. Salmonella are placed in groups by their O
antigens (A, B, C. etc.) and subdivided by their H (phase 1 and 2) antigens. The grouping and
antigenic composition of some Salmonella are shown in the following table (Cheesbrough
2010).
Group, Serogroup Serotype
O Antigen H Antigens Phase1 Phase 2
Group A, Serogroup 2
S. paratyphi A
1,2,12
a -
Group B, Serogroup 4
S. paratyphi B
S. derby
S. typhimurium
1,4,5,12
1,4,5,12
1,4,5,12
b 1,2
f.g (1,2)*
i 1,2
Group C, Serogroup 7
S. choleraesuis
S. paratyphi C
6,7
6,7,(Vi)*
c 1,5
c 1,5
Group D, serogroup, 9
S. typhi
S. enteritidis
S. pullorum-gallinarum
9,12,(Vi)*
1,9,12
1,9,12
d -
g.m -
- -
Group E, Serogroup 3,10
S. weltevreden
S. anatum
3,10
3,10
r z6
e,h 1,6
Group G, serogroup
13,22
13,22
z 1,6
S. Poona
S. cubana
1,13,23 z29 -
Brackets indicate that the antigen may present or absent. Note:The O Antigen in bold type is common to all members of the group.
Pathogenesis
Natural infection of typhoid fever occurs by ingestion of contaminated food followed by
penetration of salmonella typhi through the intestinal mucosa. Disease production is
dependent on several factors: i) number of organisms swallowed, ii) state of gastric acidity
and iii) possession of vi antigen by the organisms (Jenkins and Gillespie 2009). Studies
involving human volunteer showed that only 25% of people become infected on ingestion of
105 organisms, with the infection rate increasing to 95% when the infecting dose increases to
109 viable organisms (Zwadyk 1992).
Many factors influence the infective dose. The vehicle of ingestion also matters. Organisms
in water and other drinks may be carried through the stomach relatively rapidly, and thus
escape the effect of the gastric acid. Similarly, the administration of antacids, or the effects of
gastric resection, reduces the infective dose (Lewis 1997).
After ingestion, organisms enter the lumen of intestine. They are able to multiply. Some of
bacteria attach to the microvilli of the ileal mucosa by means of adhesions on the bacterial
surface, which adhere specifically to mannose-containing receptors on the epithelium. S.
typhi crosses the intestinal mucosal barrier after attachment to the microvilli by a complex
mechanism involving membrane ruffling, acting rearrangement, and internalization in an
intracellular vacuole (Bhutta 2008). Attachment is followed by degeneration of the microvilli
to form breaches in the cell membrane through which S. typhi enter the cell (Lewis 1997).
Gastric acidity is an important defense against enteric infections and gastric hypo acidity
from any cause will allow a greater number of organisms to enter the small intestine (Jones,
Ghori and Falkaw 1994).
From the submucosa, invading bacteria are taken up by macrophages and the organisms
travel to mesenteric lymph nodes. After a brief period of multiplication in the lymph nodes,
the organisms enter blood stream via thoracic duct causing transient primary bacteraemia.
The organisms are then transported to the liver and spleen. After a period of further
multiplication in these organs, huge numbers of organisms enter the blood stream and onset
of clinical illness due to Secondary bacteraemia. During this secondary bacteraemia, which
continues for the greater part of illness and involvement of gall bladder Peyers patches in the
lower small intestine, have important clinical significance (Jenkins and Gillespie 2009).
Invasion of the Peyers patches occurs either during the primary intestinal infection or during
the secondary bacteraemia and further seeding occurs through infected bile. The Peyers
patches become hyperplasic with infiltration of chronic inflammatory cells. Later necrosis of
the superficial layer leads to formation of irregular, ovoid ulcers along the long axis of the
gut, so that stricture does not occur after healing. When an ulcer erodes into a blood vessel,
severe haemorrhage results and transmural perforation leads to peritonitis (Jenkins and
Gillespie 2009).
The clinical syndrome of fever and systemic symptoms is produced by a release of
proinflammatory cytokines (IL-6, IL-1ß, and TNF-Ü) from infected cells. In addition to the
virulence of the infecting organisms, host factors and immunity may also play an important
role in predisposition to infection (Bhutta 2008).

Molecular basis of pathogenesis
To be effective pathogens, salmonellae must be able to invade epithelial cells for organisms
to cause enteric fever they have to be adapted to survive inside cells of the reticulo-
endothelial system.
Epithelial invasion
Membranous or microfold cells, commonly referred to as M cells, are specialized epithelial
cells of the gut-associated lymphoid tissues (GALT). M cells form part of the follicle-
associated epithelium (FAE) which overlies the Peyers Patches and other lymphoid
aggregates (Miller et al. 2007).
The target of S. typhi invasion is the M cell but must cross epithelial later to achieve this
(Jones, Ghori and Falkaw 1994). S. typhi invade the intestinal epithelial cells by a complex
mechanism which includes triggering active rearrangements, formation of pseudopodia and
phagocytosis of the bacterium into the cells. Membrane ruffling then returns to normal after
the bacterium has invaded. The ruffling- internalization process is controlled by a type III
secretion system encoded by genes found in the inv locus (Collazo and Galan 1997). These
genes are located on a pathogenecity island SPI -1(Salmonella pathogenecity island 1) which
encodes all of the genes necessary for the invasion of intestinal epithelial cells and induction
of intestinal secretory and inflammatory responses (Galan 2001).
Intracellular survival
S. typhi causing typhoid fever must be able to survive and replicate within the host
macrophage system. Once inside these locations they are shielded from the effect of
immunity, but to do this they must overcome the nutrient poor environment within the
macrophage and defeat its bactericidal mechanisms. The PhoP-PhoQ two-component
regulatory system is required for the virulence of S. typhi in humans. PhoP-PhoQ plays a
more significant role in resistance of the organisms to deoxycholic and chenodeoxycholic
acids than in resistance to other bile acids or detergents (VanVelkinburgh and Gunn 1999).
Salmonella genes necessary for survival inside macrophages are constituents of a two
component response regulator termed phoP/ phoQ. Genes activated by this phoP/ phoQ are
known as pag genes of which pag A �C have been characterized. The pag genes are
expressed within the macrophage phagosome and are required for survival within it (Behlau
and Miller 1993; Pegues et al. 1995).
Complication: Intestinal perforation and bleeding
Typhoid perforation of the intestinal wall is an important complication of typhoid fever. It is
seen rarely, but shows a high mortality and morbidity. It usually occurs when sloughs
overlying the Peyer�s patches are separated during the late second or early third week of the
illness (Atamanalp et al. 2007; Jenkins and Gillespie 2009).
Typhoid fever leads to hyperplasia in the reticuloendothelial system. In addition necrosis and
ulceration may limited to the Peyer�s patches (Hosoglu et al. 2004; Saxena, Basu and Sharma
2007). While typhoid fever often affects the terminal ileum, in rare cases, the jejunum and
caecum may also be involved (Eggleston, Santoshi and Singh 1979).
Typhoid encephalopathy
Typhoid encephalopathy, often accompanied by shock, is associated with a high mortality.
Patients may display the �typhoid� facies, a thin, flushed face with a staring, apathetic
expression. Mental apathy may progress to an agitated delirium, frequently accompanied by
tremor of the hands, tremulous speech and gait ataxia, and then muttering delirium,
twitchings of the fingers and wrists (subsultus tendinum), agitated plucking at the bedclothes
(carphology), and a staring, unrousable stupor (coma vigil) (Parry et al. 2002).
The mechanisms responsible for the neurological manifestations of typhoid fever have been
variously described. Possible mechanisms implicated are hyperpyrexia (>43°C), fluid and
electrolyte disturbances, typhoid neurotoxin, vasculitis with peri-vascular cuffing,
autoimmune mechanism, pressure effect on blood vessels resulting in cerebral infarction and
acute disseminated encephalomyelitis (Vidyasagar et al. 2004).
Hepatobiliary manifestation of typhoid fever
Mild jaundice may occur in typhoid fever due to hepatitis, cholangitis, cholecystitis or
haemolysis. Biochemical changes indicative of hepatitis have been observed during the acute
stage (Khosla 1990). The spectrum of hepatic injury in typhoid fever has been studied in
children aged below 18 years. Among 100 children with confirmed typhoid fever, 29 had
moderate hepatitis (Balasubramanian et al. 2010).
Typhoid fever in pregnancy
Typhoid fever in pregnancy may be complicated by miscarriage; although antimicrobial
treatment has made this less common (Seoud et al. 1988). Pregnancy is a risk factor for and
affects typhoid disease expression, typhoid fever does not appear to affect pregnancy
outcome (Sulaiman and Sarwari 2007). A study described by Hasbun and others found that
the hepatic dysfunction occurred in 10 cases out of 32 women with typhoid fever during
pregnancy. This was associated with late diagnosis and maternal and perinatal complications.
Hepatic dysfunction in typhoid fever during pregnancy must be interpreted as a severe
damage of cell function with potential progress to maternal multisystemic failure and
perinatal death (Hasbun, Osorio and Hasbun 2006).
Complications of typhoid fever in children
Bacteraemia by Salmonella typhi in younger children can have serious consequences and
potentially fatal outcomes. Typhoid fever in children can lead to intracranial infections
(meningitis, focal brain abscesses) and osteomyelitis with sickle cell disease. Reactive
arthritis may follow Salmonella gastroenteritis in children with HLA �B27 antigen.
Complications of typhoid fever in children include anicteric hepatitis, bone marrow
suppression, paralytic ileus, myocarditis, psychosis, cholecystitis, osteomyelitis, peritonitis,
pneumonia and syndrome of inappropriate release of antidiuretic hormone (SIADH) (Malik
2002).
Intestinal haemorrhage and perforation is infrequent among children. Other reported
complications include fatal bone marrow necrosis, disseminated intravascular coagulation,
haemolytic uraemic syndrome, pyelonephritis, nephritic syndrome, meningitis, endocarditis,
parotitis, orchitis, and suppurative lymphadenitis (Bhutta 2008).
Relapse and Carriers
Two types of relapse in case of typhoid fever have been reported such as early and late
relapse. An early relapse occurs in 5 to 10 percent of patients, usually two to three weeks
after the resolution of fever. Reinfection may also occur and can be distinguished from
relapse by molecular typing of the causative agent (Wain et al. 1999; Parry et al. 2002).
Late relapse of typhoid fever may occur in some patients (10-20%), several weeks later or
after apparent recovery. There is usually an afebrile period between the first and second
episode of fever which may be a few days to a few weeks. Clinical manifestations and course
of the disease are usually milder and shorter than the primary attack (Joshi 2001).

There are two types of carrier have been identified. Carrier of S. typhi are either convalescent
carriers who secrete the organism for a limited period of time after apparent clinical cure, or
chronic carriers in whom persistent excretion of S. typhi in stool or urine can be detected a
year after clinical illness. Chronic faecal carriers occur more commonly than do chronic
urinary ones (Singh 2001).
It is reported that 1% - 5% of those infected become chronic carriers (WHO 2003) and carrier
status persists throughout the life of a person. High prevalence of typhoid carriers occur in
patients with biliary, gastrointestinal and other related disease (Vaishnovi et al. 2005). Apart
from this, it may be responsible for deaths due to hepato biliary cancer. Faecal carriage is
more frequent individual with gall bladder disease and is most common in women over 40
(Vaishnavi et al. 2005). Chronic Carriage lead to an increased risk of carcinoma of the gall
bladder, Pancreas and Large bowel (Parry et al. 2002).
Laboratory diagnosis
Laboratory diagnosis of typhoid fever is based on isolation and identification of Salmonella
typhi from a suitable clinical specimen such as blood, stool, urine, bone marrow, and
duodenal aspirate by culture, detection of S. typhi-specific antibodies by serological test and
antigen by immunological test and identification of nucleic acid by Polymerase chain reaction
(Pearson and Guerrant 1995).
Isolation of the organism
Culture isolation of the S. typhi remains the most effective diagnostic procedure in suspected
typhoid fever. Where culture is available, typhoid fever may account for two thirds of cases
of community acquired septicaemia admitted to hospital (Hoa et al. 1998). Blood has been
the mainstay of culture for S. typhi since 1900. S. typhi maximally isolated from blood in the
first week of disease; from faeces in the second and subsequent weeks and urine in the third
and fourth weeks (Old 2006).
The various culture methods available are: 1. Blood culture 2. Clot cultures 3.Faeces culture
4. Bone marrow culture 5. Urine culture 6. Bile culture 7. Duodenal aspirate culture.
Blood Culture
Blood culture is the gold standard diagnostic method for diagnosis of typhoid fever (Parry et
al. 2002). The sensitivity of blood culture is highest in the first week of the illness and
reduces with advancing illnesses (Ananthanarayan and Panikar 1999). The organisms may be
recovered from bloodstream at any stage of the illness, but are most commonly found during
the first 7-10 days and during relapses (Lewis 1997).
Blood culture is the method of choice and has the great advantage over culture from the
faeces, urine or bile. It is showing not only that patient is infected with the bacillus but that
the infection is active (Parker 1990). Though it is gold standard, the yield of blood culture is
quite variable. In the untreated patient, blood culture is usually positive in about 80% during
first week and declining 20% - 30% later in the course of the disease (Jenkins and Gillespie
2009). Sensitivity of cultures can be affected by antibiotic treatment of the patient, inadequate
sampling, type of culture medium, lengths of incubation, and variations of bacteraemia in the
patients. In addition, Salmonella cultures take 4-7 days for isolation and identification of the
organisms (Miller and Pegues 2000).

Adequate volumes of medium should be used in blood culture system to avoid negative
results. A study finding suggested that 50 ml of medium was adequate for 8 ml of blood,
presumably because of very low degrees of bacteraemia in some patients (Watson 1978).
If whole blood is to be cultured, it is essential to prevent bactericidal effects of serum either
by adequate dilution of the sample in an adequate medium volume or by inhibition of serum
bactericidal factors. Sodium polyanethol sulfonate (SPS) and bile salt inhibit this bactericidal
effect (Parker 1990).
The SPS in concentration of 0.025% to 0.03% is the best anticoagulant for blood. It is also
anticomplementary and antiphagocytic, and interferes with the activity of some anti microbial
agents, notably amino glycosides (Betly et al. 2010). A study was reported that SPS aids in
early recovery of S. typhi and S. Paratyphi A from blood cultures (Escamilla et al. 1985).
Taking samples of blood on several occasions may improve the results of culture (Le and
Hoffman 1999).
Three types of blood cultures have been in use such as i) traditional or conventional blood
culture ii) lysis centrifugation iii) automated blood culture (Collee and Marr 2006).
Traditional or conventional technique
Tryptone soya broth, bile broth or glucose broth, brain heart infusion broth are usually used
for conventional methods of blood culture.
The media is incubated aerobically at 37°c. Subculture should be done on Mac conkey�s agar,
blood agar media daily for 1 week and checked for turbidity, gas formation and other
evidence of growth after 1, 2, 3 and 7 days. For days 1, 2 and 3 only bottles showing signs of
positive growth are cultured on agar plates. On day 7 all bottles should be sub-cultured before
being discarded as negative (Watson 1978).

Automated technique
Modern blood culture techniques (automated) permit the bacteriological confirmation of
typhoid fever in a higher proportion of cases. These systems employ equipment that
automatically detects an early sign of bacterial growth in a special blood culture bottle
(Collee and Marr 2006). An isolation rate of 92% of blood culture with the Bactec 460
Radiometric system using a blood: broth ratio of 1:6 was found in a study (Duthie and French
1990).
Lysis centrifugation
Lysis centrifugation system consists of a tube containing anticoagulant (SPS), EDTA, and
saponin. After the tube is filled with blood during phlebotomy, the contents are mixed and
centrifuged and the resulting pellet is inoculated onto agar media taking all aseptic measures.
The system effectively recovers S. typhi from blood specimen (Richard and Thompson 2007).
The benefit of this system include; i) the more rapid and greater recovery of the organism; ii)
the presence of actual colonies for direct identification and susceptibility testing after initial
incubation; iii) the ability to quantify the colony forming units present in the blood; iv) rapid
detection of polymicrobial bacteraemia; and v) possible recovery of intracellular
microorganisms caused by lysis of host cells. Limitation of the method is high rate of
possible contamination (Betly et al, 2010).
Clot culture
The blood clot culture was found to be much more sensitive for S. typhi than whole blood
culture. Bacterial growth was significantly faster in cultures of blood clot compared to whole
blood. The rapid confirmation of the aetiological agent would facilitate an early institution of
appropriate antimicrobial therapy, thereby reducing clinical morbidity, especially in an
endemic population (Mantur et al. 2007).
Blood clot from which serum has been removed often gives a positive result when a similar
volume of whole blood yields no growth (Parker 1990). A method of clot culture with
streptokinase has been recommended (Watson 1956). An amount of 8 ml quantities of venous
blood is taken from patient and allowed to clot in sterile screw capped universal containers.
The separated serum is removed. The medium used consists of a Wilson and Blair agar slope
in a 120 ml bottle to which is added 15 ml of streptokinase bile salt broth. The streptokinase
causes rapid clot lysis with release of bacteria trapped in the clot. The cultures are then
incubated and positive results may be obtained in less than 24 hours (Watson 1956). Clot
culture is more sensitive than blood cultures with isolation rate of 92% and the clot technique
has many advantages over conventional whole blood culture, both in reliability and in cost
(Watson 1978).
Culture of the mononuclear cell �Platelet Fraction of Blood
The moderate or low sensitivity of blood culture is probably due to low concentration of S.
typhi (<10 bacteria per ml) in cells of the blood of patients with typhoid fever. Virtually all
intracellular S. typhi are found within only mononuclear cells (MNC) and platelets. By the
method of culture of mononuclear cells (MNC) and platelets fraction of blood from typhoid
patients is subjected to density gradient centrifugation to isolate the mononuclear cells.
Colonies of S. typhi were present in all mononuclear cell�platelet layer�positive cultures
within 18 hours of plating and were identified within an additional 10 minutes by a co-
agglutination technique. In contrast, identification of all positive culture by conventional
blood culture required 3 days (Rubin et al. 1990).
Bone marrow culture
Salmonella typhi is an intracellular pathogen in the reticuloendothelial cells of the body
including the bone marrow. The overall sensitivity of bone marrow cultures ranges from 80-
95% and is good even in the late phase of the disease and despite prior antibiotic therapy
(Parry et al. 2002).
Bone marrow aspirates are know to yield a higher rate of positive cultures than peripheral
blood in typhoid fever cases (Gilman et al. 1975; Farooqui et al. 1991) Bone marrow culture
may give a positive result when blood culture fails, particularly in patients admitted to
hospital while on antibiotic treatment. As a result unlike blood culture bone marrow culture is
highly (90%) sensitive (Lesser and Miller 2005). Another study reported that the
concentration of S. typhi in the bone marrow was found considerably higher than in
peripheral blood (Wain et al. 2001). In the bone marrow there were over 10 times more
bacteria than in peripheral blood. it seems likely to the positively rate of a 1 ml bone marrow
culture is equivalent to the result of 10 ml of peripheral blood (Wain et al. 2001). The
invasive nature of bone marrow aspiration discourage from its use as a first line investigation
for diagnosis of typhoid fever (Kundu 2006).
Stool Culture
In typhoid fever, stool cultures are usually positive from the second week of the infection.
Stool is usually plated on desoxycholate- citrate agar and also inoculated into fluid
enrichment media such as tetrathionate or selenite broth. The limitation of liquid of medium
is that the growth of fluid enrichment medium is subcultured appropriate medium for proper
identification. Suspicious colonies from culture plates are tested directly for the presence of
salmonella O antigens by slide agglutination and subcultured to peptone water for
determination of H antigen structure and for further biochemical analysis (Lewis 1997).
Urine Culture
Urine cultures are not recommended for diagnosis in view of poor sensitivity (Parry et al.
2002) (Gilman et al. 1975). Bacteria are not excreted continuously and therefore, several
specimens may need to be cultured before organisms can be isolated (Chessbrough 2010).
In typhoid fever, urine cultures are usually positive from the third week of the infection. The
centrifuged urine deposit is plated on desoxycholate- citrate agar and is also inoculated into
fluid enrichment media such as tetrathionate or selenite broth. The growth of fluid enrichment
medium is subcultured appropriate medium for proper identification (Lewis 1997).
Duodenal string � Capsule Culture
Duodenal string test was found to be a simple, non-invasive and a reliable test which when
used in combination with blood culture could identify almost all cases of typhoid fever
irrespective of duration of fever and prior use of antibiotics (Antony et al. 1993).
Duodenal content cultures have been proved to be more sensitive (86%) in diagnosis than
bone marrow (75%) and more effective than blood (42%) and stool (26%) cultures in
recovery of S. typhi. The sensitivity of duodenal content cultures was found not modified by
the duration of illness at admission or by previous antibacterial therapy (Benavente et al.
1984).
Culture of duodenal aspirate is important in the detection of typhoid carriage. Individuals can
excrete S. typhi in the bile and yet be undetected by stool culture (Madanagopalan et al.
1975). Because of patient�s discomfort and the time required for tube placement, duodenal
aspiration has not been widely used (Gilman and Rechard 1976).
Antibody detection tests (serology)
Widal test
The information regarding Widal test has been noted in Britannica encyclopaedia. The Widal
agglutination test was introduced as a serologic technique to aid in diagnosis of typhoid fever.
The test was named after Georges Fernand Isidore Widal, a French physician and
bacteriologist. In 1896, Widal developed a procedure for diagnosing typhoid fever based on
the fact that antibodies in the blood of an infected individual cause the bacteria to bind
together into clumps (the Widal reaction) (Encyclopaedia Britannica 2011).
The test was based on demonstrating the presence of agglutinin (antibody) in the serum of an
infected individual, against the H (flagellar) and O (somatic) antigens of Salmonella typhi
(Jenkins and Gillespie 2009).
The �O� antigen is the somatic antigen of S. typhi and is shared by S. paratyphi A, S.
paratyphi B, other Salmonella species and other members of the Enterobacteriaceae family
(Rodrigues 2003). Antibodies against the O antigen are predominantly IgM, rise early (appear
on day 6-8) in the illness and disappear early (Rodrigues 2003). The H antigens are flagellar
antigens of S. typhi, paratyphi A and paratyphi B. Antibodies to H antigens are both IgM and
IgG, rise late (on days 10-12) in the illness and persist for a longer time (Olopoenia and King
2000; Rodrigues 2003).
Serological diagnosis relies classically on the demonstration of a rising titre of antibodies in
paired samples at an interval of 10�14 days (Parry et al. 1999). In typhoid fever, however, a
four- fold rise after 2 weeks in not always demonstrable, even in blood culture confirmed
cases. This situation may occur when the acute phase sample is obtained late in the natural
history of the disease, because of high levels of probable background antibodies in an
endemic region, or because in some individuals the antibody response is blunted by the early
administration of an antibiotic (Schroeder 1968).

There is a controversy about the predictive value of O and H antibodies for diagnosis of
enteric fever. Some authorities claim that O antibodies have superior specificity and positive
predictive value (PPV) because these antibodies decline early after an acute infection
(Schroeder 1968).
It can be negative in up to 30% of culture- proven cases of typhoid fever. The purity and
standardization of antigens used for the Widal test is a major problem and often results in
poor specificity and poor reproducibility of test results (Olopoenia and King 2000).
Followings are the causes of a positive Widal agglutination test: i) the patient being tested has
typhoid fever; ii) previous immunization with Salmonella antigen; iii) cross-reaction with
non-typhoidal Salmonella; iv) infection with other enterobacteriaceae ; v) other diseases such
as dengue, schistosomal infection, chronic liver disease associated with raised globulin
levels; and vi) disorders such as rheumatic fever, rheumatoid arthritis, multiple myeloma,
nephritic syndrome and ulcerative colitis (Cheesbrough 2010). False negativity is one of the
obstructive features of the Widal test. Hosoglu et al conducted a study to evaluate the
associated factors with Widal test negativity in an endemic area. Widal test negativity was
retrospectively analyzed by them among culture-proven typhoid fever cases. The potential
features including age, gender, previous antibiotic usage, duration of symptoms, leucopoenia,
haematocrit value, and erythrocyte sedimentation rate (ESR) were evaluated for association
with Widal test negativity (Hosoglu et al. 2008).
It has been shown that the antibody response to the O antigen of S. typhi was markedly
reduced in acute episodes of malaria compared to controls and that humoral immunity is
transiently impaired (Greenwood et al. 1972). In a recent study, subjects with dual infection
of malaria and typhoid fever had significantly higher rates of nausea, vomiting, abdominal

pain, and diarrhoea�the common features of enteric fever (Khan et al. 2005). In the last two
decades, this relationship between the two diseases has been reported in studies from Africa
and India (Ammah et al. 1999; Ohanu et al. 2003; Kanjilal et al. 2006).
A study conducted in Cameron found that the number of fever cases diagnosed as malaria-
typhoid fever co-infection were actually overestimated (Ammah et al. 1999).
Immunochromatographic method
ICT has been studied in many countries and they found significantly higher sensitivity and
specificity (Jesudason, Esther and Mathai 2002; Pastoor et al. 2008; Anusha, Ganesh and
Lalitha 2011). An evaluation of ICT (Typhidot) in India was found to be 100% sensitive and
80% specific compared to a blood culture as �gold standard� (Jesudason, Esther and Mathai
2002).
Haemagglutination (HA) Tests
Many researchers have evaluated the usefulness of HA tests in different countries. In a study
from India, the anti-LPS HA test showed a sensitivity of 60% and specificity of 98.2%. The
positive predictive value and negative predictive value were 66.7% and 96.7% respectively.
In the same study, the haemagglutination inhibition test targeted Salmonella antigens and was
found useful for helping the early detection of S. typhi in culture (Shukla, Patel and Chitinnis
1997). In another study, a Reverse Passive Haemagglutination Test (RPHA) was designed for
the detection of S. typhi antigen. The test was found to be 70% sensitive and 92% specific for
acute typhoid fever diagnosis (Kalhan et al. 1998).
Countercurrent Immunoelectophoresis (CIE)

This test is based on electrophoresis and the visualization of the precipitin band of antigen-
antibody complexes that form. The sensitivity is similar to that of the Widal test and the
procedure may be quicker if tests are batched (about one hour for a gel), but bands are often
difficult to see, the cost is higher than that of the Widal, and some studies conclude that CIE
has a low sensitivity with Vi antigen. A panel of antigens (somatic (O), flagellar (H) and
capsular polysaccharide (Vi) antigens of S. typhi is recommended for rapid diagnosis of
typhoid fever (Sharma et al. 1979).
Other serological test
In view of the limitations of the Widal test and need for a cheap and rapid diagnostic method,
several attempts to develop alternative serologic tests have been made. These include rapid
dipstick assays, dot enzyme immuno-assays and agglutination inhibition tests.
Antibody detection:
Dot Enzyme Immunoassay (EIA) test
A dot enzyme immunoassay that detects IgG and IgM antibodies against a 50 KD outer
membrane protein, distinct from the somatic (O), flagellar (H) or capsular (Vi) antigen of
Salmonella typhi is commercially available as Typhidot (Gasem et al. 2002). commercially it
is available in two different properties, i) The Typhidot M that detects only IgM antibodies of
S. typhi has been reported to be slightly more specific in a couple of studies (Choo et al.
1999; Hatta et al. 2002).
ii) Typhidot® test detects specific IgM and IgG antibodies to S. typhi. It has undergone full-
scale multinational clinical evaluation of its diagnostic value (Ismail, Kader and Ong 1991).
In areas of high endemicity, where the rate of S. typhi transmission is high, the detection of
specific IgG increases. The IgG can persist for more than two years after typhoid fever
Infection (Choo et al. 1997; Bhutta and Mansurali 1999). The detection of specific IgG can
not differentiate between acute and convalescent cases (Choo et al. 1999). Furthermore, false
positive results attributable to previous infection may occur. On the other hand, IgG positivity
may also occur in the event of current reinfection. In cases of reinfection there is a secondary
immune response with a significant boosting of IgG over IgM, such that the later can not be
detected and its effect is masked. A possible strategy for solving this problem is to enable the
detection of IgM by ensuring that it is unmasked (Bhutta 1996).
IgM dipstick test
A rapid dipstick assay for the detection of S. typhi-specific IgM antibodies in serum and
whole blood samples was previously reported and the sensitivity and specificity was
evaluated (Gasem et al. 2002; Hatta et al. 2002; House et al. 2005).
The dipstick assay may thus also be useful for the serodiagnosis of culture-negative patients
with clinical signs and symptoms consistent with typhoid fever. The advantages of the
dipstick assay are that the result can be obtained on the same day allowing a prompt
treatment, that only a small volume of serum is needed, and that no special laboratory
equipment is needed to perform the assay. The stability of the reagents of the dipstick and the
simplicity of the assay allows its use in places that lack laboratory facilities (Hatta et al.
2002).
Antigen detection tests
There is clearly a demand for a simple diagnostic test for typhoid fever. An ideal test is
reliable, simple, and affordable for the countries where the need is the greatest. Many of the

affected countries are poor, and some places do not have electricity. The antigen detection,
rather than antibody detection, could provide such a test (Wain and Hosoglu 2008).
Protein and Vi antigens
Enzyme immuno-assay, counterimmune electrophoresis and co-agglutination tests to detect
serum or urinary somatic/flagellar/Vi antigens of S. typhi have been evaluated (Fadeel et al.
2004; Kalhan et al. 1999). Sensitivity of Vi antigen had been found to be superior than
somatic and flagellar antigen, had been reported as ranging from 50-100% in different studies
(Fadeel et al. 2004; Kalhan et al. 1999; Rao et al. 1999). Similarly, specificity estimates have
been reported to vary from 25% -90%. The suboptimal and variable sensitivity and specificity
estimates, inability to detect S. paratyphi infection and Vi antigen negative strains of S. typhi
are serious limitations of the Vi antigen detection tests. S. typhi antigen can be detected in the
urine of some typhoid patients by co-agglutination test (West, Richens and Howard 1989). A
monoclonal antibody specific for group D Salmonellae antigen 9 was used in an indirect
enzyme-linked immunosorbent assay (ELISA) for detecting the antigen in urine specimens
collected from patients with clinical typhoid fever in Jakarta, Indonesia. The ELISA had a
sensitivity of 95% in identifying patients in whom S. typhi was isolated from blood cultures,
73% in patients in whom S. typhi was isolated from stool specimens, and 40% in patients in
whom the organism was isolated from bone marrow cultures, but specificity varies from 25-
90% (Chaicumpa et al. 1992).
Molecular methods
The molecular method for diagnosis of typhoid fever has been evolved to overcome the
limitations of cultures and serologic tests. Many authors have explored the use of polymerase
chain reaction (PCR) for detecting specific DNA sequence of the organisms present in
clinical specimens. The PCR as a diagnostic modality for typhoid fever was first evaluated in

1993 when Song et al successfully amplified the flagellin gene of S. typhi in all cases of
culture proven typhoid fever and from none of the healthy controls. By using two pairs of
primers evaluated in the study by Song et al, amplification of the flagellin gene of S. typhi
confirmed the presence of the organism in the patient�s blood (Song et al. 1993).
The PCR has been used to enable diagnosis of typhoid fever within few hours and more
specific and sensitive than blood cultures.In addition nested PCR has been shown promising
results. These results show that the nested PCR has good potential to be a rapid tool for the
definitive, differential diagnosis of typhoid and is superior to conventional methods (Ali et al.
2009).
The nested PCR resulted in amplified fragments that were visible after agarose gel
electrophoresis. The whole procedure to identify S. typhi DNA in the blood by agarose gel
electrophoresis took only 16 hours, demonstrating the PCR to be a specific and rapid method
for the early diagnosis of typhoid fever (Song et al. 1993). Frankel et al. amplified flagellin
gene sequences specifically from S. typhi (Frankel et al. 1989).
Massi in the year 2005 conducted a study to establish the nested PCR for DNA detection of S.
typhi in the urine of patients with suspected typhoid fever. This research was used 107 urine
samples from patients suspected with typhoid fever which were examined with nested PCR
using two primer pairs with the final amplification result of 343 basepair (bp). This study
reported that 64 (59%) urine samples were positive with S. typhi DNA. This research
concluded that nested PCR specifically from urine specimen can be used as an alternative
method in diagnosis and management of typhoid fever (Massi et al. 2005).
Kumar et al used blood samples from 40 clinically suspected cases of typhoid fever, and
found 20 of 20 culture positive and 12 of 20 culture negative cases to be positive by PCR in
Delhi, India (Kumar et al. 2002). Using single primer in South Sulawesi, Indonesia, 46 of 73
(63.0%) blood samples collected from patients with clinically suspected typhoid fever were
positive by PCR compared to 13.7% positive by blood culture (Massi et al. 2003). In
Varnassi, India, nested PCR was again better 53 of 57 (73.0%) were positive than blood
culture 17 of 53 (32%) were positive on specimens from 63 clinical typhoid fever cases
(Prakash et al. 2005).
A large, well-designed study in Indonesia investigated 131 patients with a clinical diagnosis
of typhoid fever and diagnosed the cases by blood culture and PCR from blood (84.5%) and
urine samples (69.3%). The PCR diagnosis was found more sensitive than the blood culture
(61.8%) (Hatta and Smith 2007).
A study from Nepal on specimens from 71 children with suspected typhoid fever reports
82.7% positivity for PCR from blood and urine, showing similar results for each specimen
and PCR results were much higher than blood culture (26.9%). In Pakistan, 55 cases of
suspected typhoid fever and a control group of 20 healthy persons were diagnosed by PCR
from blood samples and blood culture. The PCR and blood culture gave 58.2% and 14.5%
positivity, respectively showing significantly better results by PCR (Haque et al. 2001).
Again in Pakistan, a multiplex PCR targeting five different genes for differential diagnosis of
typhoidal pathogens has been developed for use directly on clinical blood samples. Of 42
multiplex PCR-positive blood samples, 35 were positive for S. typhi and two for S. Paratyphi
A and interestingly remaining 5 patients were found to have mixed infection (Ali et al. 2009).
Moreover, some patients with culture negative typhoid fever were PCR positive suggesting
that PCR diagnosis of typhoid fever may have superior sensitivity than cultures. Over the
next 10 years, a handful of studies have reported PCR methods targeting the flagellin gene,
somatic gene, Vi antigen gene, 5S-23S spacer region of the ribosomal RNA gene, invA gene
and hilA gene of S. typhi for diagnosis of typhoid fever (Prakash et al. 2005; Jimenez and
Castro 2004; Haque et al. 2001; Cocolin et al. 1998). These studies have reported excellent
sensitivity and specificity when compared to positive (blood culture proven) and healthy
controls. The time required for diagnosis has been less than 24 hours (Kundo et al. 2006).
Chaudhry et al. developed standardization of PCR for the detection of S. typhi in typhoid
fever. The PCR technique was used for detection of S typhi in blood or clot cultures from 84
patients clinically suspected of having typhoid fever, and from 20 healthy controls. Twenty
five of 84 samples from clinically suspected cases were positive by PCR; four of which were
culture negative. No amplification was seen in samples from patients who were culture
positive for organisms other than S. typhi or from controls. The time taken for each sample
for PCR analysis was less than 48 hours, compared with three to five days for blood or clot
culture. The PCR was found to appear to be a promising diagnostic test for typhoid fever
(Chaudhry et al. 1997).
Multiplex PCR has been successfully applied for differential diagnosis of many diseases
caused by viruses, bacteria, fungi, and parasites (Rithidech, Dunn, and Gordon 1997; Hirose
et al. 2002). The multiplex PCR technique was evaluated by Ali et al directly on blood
samples of 60 clinically suspected cases of typhoid fever. The PCR detected typhoidal
species in 42 cases, only 17 of which were culture positive. The presence of Salmonella in
these samples was confirmed with genus-specific primers (Kidgell et al. 2002). Quick
multiplex PCR-based detection method was developed for early diagnosis of typhoid fever,
using specific genetic markers of S. typhi. Primers of tyv gene, flag gene, viaB gene and ratA
gene confirmed the specificity and sensitivity of the PCR. The serum samples of the
suspected typhoid patients were taken directly for PCR without culturing the organism and
extracting genomic DNA. Overall diagnosis required 2 hours which is the least time ever
reported for a PCR based method. The sensitivity of the method was up to 5 famtogram (fg)
genomic DNA. The genetic markers were specific and the four pairs of primers give selective
amplification and differentiate S. typhi from closely related S. typhimurium (Kumar et al.
2010).
Antimicrobial resistance of S. typhi
Most drug resistance is the result of a genetic change in the organism caused either by a
chromosomal mutation or the acquisition of a plasmid or transposon (Winstaniey and Hart
2001; Levinson 2010). Plasmid-mediated resistance is more common in multidrug resistant
(MDR) typhoid fever and occurs with a high frequent rate (Levinson 2010). In 1948,
chloramphenicol became the standard antibiotic for treating typhoid fever (Woodward et al.
1948; Kidgell et al. 2002). Emergence of S. typhi strains resistant to chloramphenicol was
reported in 1970 cited in Rahman et al (Rahman et al. 2006) then subsequently resistance to
ampicillin and co-trimoxazole emerged soon (Morshed et al. 1986; Parry and Threlfall 2008).
Toward the end of the 1980s and the 1990s, S. typhi developed resistance simultaneously to
all the drugs that were then used as first-line treatment (chloramphenicol, trimethoprim,
sulfamethoxazole, and ampicillin (Mirza, Beeching and Hart 1996). The MDR S. typhi being
resistant to three of the first-line antimicrobials emerged sporadically (Goldstein et al. 1986).
First documented outbreak of multidrug resistance occurred in Malaysia in 1984 (Sharma et
al. 1979). Since then the MDR S. typhi spread throughout south-east Asia and China, where
they became endemic (Ling and Chang 1984). Outbreaks of infections with these strains
occurred in India (Threlfal et al. 1992; Shanahan et al. 1998), Pakistan (Bhutta 1996;
Shanahan et al. 2000), Bangladesh (Saha et al. 1996), Vietnam (Hoa et al. 1998), the Middle
East (Lancet 1990), and Africa (Kariuki et al. 2000) . In most cases, resistance to
chloramphenicol, ampicillin and cotrimoxazole was transferable on plasmid, either

individually or all together (Goldstein et al. 1986; Mirza, Beeching and Hart 1996; Mirza et
al. 2000; Connerton et al. 2000; Wain et al. 2001). Plasmids are extrachromosomal
supercoiled loops of DNA that were probably originally derived from bacterophages (Sinha
et al. 1999; Levinson 2010). When greater than 40 kbp in size the plasmids are able to
transfer the carrying genes from host bacterium to others by conjugation.
The plasmids found in S. typhi are of two major types. First as pH CM2 cryptic plasmid
which can carry gene encoding mechanisms of DNA metabolism and replication and
virulence are found in Asia but not in Africa. Second, type approximately 140-180 kbp self
transferable plasmid. Large resistant plasmids are built up by the addition of resistant gene
encoded on integrons and transposons (Levinson 2010). These large plasmids can then be
transferred to and from enteric gram negative bacterium such as Echerichia coli, Klebsiella
pneumoniae and S. enterica, especially when antimicrobials are being administered
(Levinson 2010).
Chomosomally acquired quinolone resistance in S. typhi has been found in different parts of
Asia (Park 1999; Rahman et al. 2006; Levinson 2010) which may be the consequence of wide
spread indiscriminate use of these drugs. Resistance rarely emerges during the course of
treatment (Schwalbe et al. 1990). There have been sporadic reports of high-level resistance to
ceftriaxone (minimal inhibitory concentration [MIC], 64 mg per liter) in S. typhi and S.
paratyphi A (Saha et al. 1999; Bhutta, Farooqui and Sturm 1992), although these strains are
very rare. S. typhi strains with reduced susceptibility to fluoroquinolones have become a
major problem in Asia (Wain et al. 1997; Brown et al. 1997; Threlfall and Ward 2001a). An
outbreak of typhoid with such strains in Tajikistan in 1997, caused illness in 8000 people in a
six-month period and 150 deaths. Although they were reported to be susceptible to
fluoroquinolones, by disk testing with the use of recommended break points, these organisms
were resistant to nalidixic acid and the MIC of fluoroquinolones for these strains was 10

times that for fully susceptible strains. This reduction in susceptibility results in a poor
clinical response to treatment (Wain et al. 1997; Threlfall et al. 1999).
Quinolone resistance is frequently mediated by single point mutations in the quinolone-
resistance� determining region of the gyrA gene, characteristically occurring at position 83 of
the DNA gyrase enzyme (changing serine to phenylalanine) and position 87 (changing
aspartate to tyrosine or glycine) (Wain et al. 1997; Brown et al. 1999). In other
Enterobacteriaciae, higher levels of quinolone resistance have been associated with additional
mutations in the gyrA gene, mutations in other Topoisomerase genes, or alterations in
fluoroquinolone uptake. No such mutations have been reported yet in S. typhi, although there
are sporadic reports of fully fluoroquinolone-resistant isolates (Mehta, Randhawa and
Mohapatra 2001). Because the clinical response to fluoroquinolones in patients infected with
nalidixic acid�resistant strains is greatly inferior to the response in those infected with
nalidixic acid�susceptible strains (Threlfall, Skinner and Ward 2001b).
Treatment of multidrug resistant (MDR) S. typhi infection
The MDR S. typhi infections are those caused by the organism resistant to chloramphenicol,
ampicillin, and cotrimoxazole (trimethoprim�sulphamethoxazole). Emergence of drug
resistance is a major challenge in the treatment of typhoid fever (Bhutta 2008).
The MDR cases began to appear around 1990 (Rahman et al. 2007). In 1992, 40% of the
isolates were MDR (Hoque et al. 1992). Studies from Institute of child and maternal health
(ICMH) in Dhaka (1994) and BSMMU (1992) revealed similar pattern, while isolates were
equally sensitive to ciprofloxacin and ceftriaxone (Saha 1994).
WHO recommends in the year 2003 ciprofloxacin and ofloxacin for MDR cases and
azithromycin, third generation cephalosporin and high dose older generation fluroquinolones
in nalidixic acid resistant cases (WHO 2003). Resistance to azithromycin and ceftriaxone is
rarely reported and this is if they can be used as empirical therapy in enteric fever (Islam et
al. 2007; William et al. 2001). Azithromycin is a macrolide azolide antibiotic with relatively
poor in vitro activity against S. typhi. However, the antibiotic is concentrated 50-100 fold
inside cells such as macrophages, where the S. typhi reside usually. It also has a long half life
(68 hours) and is thus given as a once-daily regimen. In a study in Bangladesh, 94% cure rate
with azithromycin was observed. An Indian study showed 88% response with once daily
azithromycin for 7 days, where 100% of the cases were disease free after 14 days therapy
(Butler, Sridhar and Daga 1999).
The MDR S.typhi isolates with reduced susceptibility to fluoroquinolones indicated by
resistance to nalidixic acid have caused epidemics and become endemic in southern Viet
Nam during the 1990s. Short courses of ofloxacin have proved acceptable for treating MDR
or nalidixic acid sensitive isolates of S. Typhi (Parry et al. 2002).
Prevention of typhoid fever
Typhoid fever is a food and waterborne disease and the main preventive measure is to ensure
access to safe water and water. Adequate water treatment, waste disposal, and protection of
food supply from contamination are important public health measures. Typhoid can be
transmitted by chronic carriers who do not apply satisfactory food � related hygiene practices.
These carriers should be excluded from any activities involving food preparation and serving
(Bhutta 2008; Zwadyk 1992).
Vaccination
Vaccination in high-risk areas is a potential control strategy recommended by WHO for the
short-to-intermediate term. Two safe and efficacious typhoid vaccines, the injectable Vi
polysaccharide and the oral Ty21a, have been licensed; and new, improved candidate
vaccines are currently being tested. This vaccine is licensed in 56 countries in Africa, Asia,
Europe; South America, and the USA However; typhoid vaccination has not been
implemented as a routine public health measure in most typhoid-endemic countries (WHO
2003).
Inactivated whole-cell typhoid vaccine
Vaccines of this type were introduced in 1896 (WHO 2005). Their efficacy was established
only in 1960 in controlled trials in the Cochrane countries of Yugoslavia, the Soviet Union,
Poland, and Guyana. The 1998 version of the vaccine demonstrated that two doses of this
type of vaccine resulted in 73% efficacy over three years .Different methods of inactivating
cells of S. typhi have been used to prepare these vaccines: acetone-inactivated, alcohol-
inactivated, or heat inactivated and phenol preserved. In field trials, the vaccine has been
associated with fever and systemic reactions in 9% to 34% of the recipients, and with short
absences from work or school in 2% to 17% of the cases (WHO 2000). Therefore, the
inactivated whole cell typhoid vaccine is considered unsuitable for use as a public health
vaccine and although licensed, it is no longer available for use. The old parenteral killed
whole cell vaccine was effective but produced strong side effects because of
lipopolysacharide (LPS) (Garmory, Brown and Titball 2002).
Vi polysaccharide vaccine
The Vi polysaccharide vaccine is given as a single parenteral dose. Protection was found to
begin seven days after injection and maximum protection reached 28 days after injection
when the highest antibody concentration was obtained (Garmory, Brown and Titball 2002).

The vaccine is approved for persons aged over two years. Revaccination is recommended
every three years. Mild local adverse reactions was found to occur including 17% of adult
vaccinees and 86.7% of child vaccines experience local pain at the injection site, although
these reactions are usually transient and mild (Garmory, Brown and Titball 2002).
In field trials conducted in Nepal and South Africa, where the disease was endemic and attack
rates reached 900/100000, the protective efficacy was 72%, one and half years after
vaccination (Acharya et al. 1987) and was found 55% three years after a single dose
(Klugman et al. 1996). In another field trial in South Africa, 10 years after immunization,
58% of the vaccines still had protective level of antibodies of over 1 ìg/ml. (Keddy et al.
1999). In efficacy trials conducted in Chiang Su and Guangxi, China, in 1995 and 1997
respectively, with a locally produced Vi vaccine, 72% protection was obtained by vaccination
(Yang et al. 2001). A protective efficacy of 70% was reported in a population vaccinated
before or during an outbreak situation in the same country (Yang and Kilgore 2001). It is
mainly used by travelers, visiting areas at high risk of typhoid fever because of the presence
of multidrug-resistant strains (Jegathesan 1983).
Ty2la vaccine
The live oral vaccine Ty21a is available as enteric coated capsule or liquid formulation. It
elicits protection as from 10-14 days after the third dose. It is approved for use in children
aged at least 5 years or older and adults. A booster dose is needed every 5 years for people
who remain at risk. Travelers should be revaccinated annually, and those living in disease
endemic areas, every three years (Khan 2005; Black et al. 1990).
In randomized, controlled field trials in Area Norte and Area Occidente of Santiago, Chile, 2
(Norte) or 3 (Occidente) doses of live oral typhoid vaccine Ty21a in enteric-coated capsules
conferred protection against confirmed S. typhi disease (53% efficacy in Norte; 67% efficacy

in Occidente) during 3 years of follow-up. There was also a trend in each trial showing
protection against S. paratyphi B disease (56% efficacy in Norte; 42% efficacy in Occidente)
(Levine et al. 2007). The use of vaccines in the control of typhoid fever has had mixed
results. The most promising was an oral vaccine of an attenuated typhoid bacillus, TY21a. In
a field trial in Alexandria, Egypt, involving 32,000 children, the infection rate was 0/100,000
in the vaccinated group as compared to 126/100,000 in the placebo group and 133/100,000 of
non-vaccinated group (Zwadyk 1992).
Future vaccines (Vi-rEPA vaccine)
A new modified Vi vaccine conjugated to a nontoxic recombinant Pseudomonas aeruginosa
exotoxin A (rEPA) has also been evaluated in a randomized controlled trial among children
aged two to five years. This vaccine has the potential of being immunogenic in infants under
the age of two (Parry et al. 2002). Research continues to develop more effective typhoid
vaccines. It is concentrated on two main efforts. The first is development of new parenteral
Vi polysaccharide protein conjugate vaccines, which are expected to produce higher antibody
titres following initial and booster immunizations. The second effort is to genetically
attenuate strains of S. typhi to achieve high immunogenicity, while at the same time rendering
the strain nonpathogenic (Garmory, Brown and Titball 2002). Vi-rEPA vaccine has enhanced
immunogenecity in adults and in children aged 5-14 years and has induced a booster response
in children aged 2-4 years (Kossaczka et al. 1999). In a double-blind randomized control trial,
11091 Vietnamese children aged 2-5 years, were given two injections of Vi- rEPA separated
by six weeks (Lin et al. 2001). No serious side effects observed. The efficacy after 27 months
of active surveillance was 91.2%. Passive surveillance in the 16 months since the study ended
showed 88% efficacy.


Materials and methods
Type of study: The study was designed as Descriptive type of comparative study.
Place of study:
The study was carried out in the Department of Microbiology Mymensingh Medical College,
Mymensingh.
Period of study:
The study was carried out from 1st July 2010 to 30th June 2011.
Sampling technique:
Non probability purposive type of sampling.
Data collection, recording and analysis:
A set of questionnaire was used for each of the cases and controls. All the relevant
information (history, clinical and laboratory findings) of every cases were systematically
recorded in a pre-designed data sheet (Appendix I). The data were analyzed in computer
using appropriate program.
Study population:
One hundred and fifty (150) cases and fifty (50) age sex matched controls were studied.
Sample size determination:

In this study, the sample size was calculated by the following formula:
2
2
d
pqzn
In this study, sample size was taken 150, due to limitation of budget, resource and time.
Subjects/Cases:
All febrile patients suspected of typhoid fever attending at out patient departments (OPD) of
Medicine and Paediatrics unit of MMCH were included in this study. The suspicion was
made by characteristics presentation of typhoid fever by the medical officer working at the
relevant OPD�s.
Inclusion criteria for cases:
1. Fever, characteristics for typhoid fever for 3 days or more, irrespective of antibiotic
treatment.
2. Any other additional presentation suggestive of typhoid fever like headache, anorexia,
nausea, vomiting, abdominal discomfort with diarrhea, soft enlarged spleen, coated
tongue, toxic look and relative bradycardia.
3. Individuals of both sexes representing all ages.
Exclusion criteria of the cases:
1. Fever with any obvious focus for other infection such as urinary tract infection, otitis
media etc.
2. History of immunization with typhoid vaccines.
The control group:
A total of 50 age and sex- matched controls of which 25 were healthy control individuals
with no recent history of fever and 25 were sick suffering from non-typhoidal febrile illness.
Consent taking:
Informed written consent was taken from each patient or from guardian of the minor patients
before his/her entry into the study (Appendix II).
Socioeconomic condition:
Socio-economic conditions of the study population were ascertained on the basis of their
monthly income of the patients or their guardians from all possible sources. The cases and
controls were classified into three groups:
i. Low income group (Up to 15,000 TK. /month.)
ii. Middle income group (15,000-50,000 TK. /month.)
iii. Upper income group (>50,000 TK. /month.)
Laboratory procedures
Specimen collection and storage:
Whole blood 10 ml for adults and 6 ml for children.
Venous blood was collected aseptically following universal safety precaution. For this
purpose:
i) Wearing a sterile disposable glove, the puncture area was washed with iodine and
70% alcohol.
ii) With a sterile disposable syringe, 10 ml of blood in case of adult and 6 ml in case of
children were collected.
iii) Of the collected sample, 8 ml for adults and 4 ml for children were transferred in
heparinized tube for blood culture.
iv) From the remaining blood sample, 1 ml of was transferred in a tube with EDTA for
PCR and immediately would be refrigerated at -200C for molecular study.
v) Remaining blood was transferred in another clean tube for ICT.
Blood culture by lytic centrifugation method:
The aseptically collected blood sample in an amount of 8 ml in case of adult and 4 ml in case
of children were collected in heparinized tube containing lytic solution which was made in
our laboratory (Appendix III) for initial processing. Blood sample were mixed well by
inverting the tube 3-5 times to mix blood with lytic solution and mixture were shaked,
vortexed and centrifuged at 3000 rpm for 30 minutes. After centrifugation, the supernatant
were discarded and 1ml of the deposit containing the pathogen is vigorously vortexed and
entire sediment were directly inoculated onto blood agar and Mac Conkey agar media
(Appendix IV). The inoculated culture plates were immediately placed in an incubator at
370C for 24 - 48 hours. After proper incubation colonies if any as Salmonella typhi were
identified by colony morphology, Gram staining, motility test and relevant method of
biochemical tests (Richard and Thompson 2007; Cheesbrough 2010).
Colony morphology:
MacConkey agar: Produce non lactose fermenting colonies of 1-3 mm in diameter, colonies
are pale yellow or nearly colour less.
Blood agar: The colonies of S. typhi were moderately large 2-3 mm in diameter after 24 hours
at 370C. They were non haemolytic, grey-white, moist circular discs with a smooth convex
surface and entire edge.
Salmonella � Shigella agar (SS agar): In SS agar medium, Colonies of S. typhi were colorless
with or without black centers.
Gram�s staining
Gram�s staining was done for morphological identification of S. typhi. A drop of distilled
water was taken on the middle of a clear glass slide. Then a colony of S. typhi (young culture)
was transferred with a sterilized inoculating wire loop on the drop of water. Then a very thin
smear was prepared on the slide by spreading specimen uniformly. The smear was fixed by
passing it over the flame for two or three times. Then Gram�s staining was done (Appendix-
V) and S. typhi was found to be Gram negative short bacilli.
Motility test:
It was done by hanging drop preparation and by using Motility indole urease (MIU) medium.
In MIU medium, S. typhi were motile and Urease and indole negative. In hanging drop
preparation, S. typhi were motile.
Biochemical tests:
S. typhi were presumptively identified using triple sugar iron (TSI) medium, citrate utilization
test and oxidase test.
On Triple sugar iron agar medium (TSI)
The subculture of S. typhi in TSI medium was inoculated by using a sterile straight wire to
stab into the butt first and then use the same wire to streak slope in a zig-zag pattern. Then the
medium were incubated at 370C for 24 hours.
S. typhi in TSI medium was identified by following findings:
- Pink-red (alkaline) slope and yellow (acid) butt, indicating fermentation of glucose
but not lactose.
- No cracks in the medium (if serotype produces gas from glucose fermentation, it is (S.
Para typhi A)
- Blackening in the medium due to H2S production (only a small amount of blackening
is seen with S. typhi).
Citrate utilization test:
By using a sterile straight wire, first streak the slope with a saline suspension of S. typhi and
then stab the butt. Then the medium were incubated at 350C for 48 hours. S. typhi were citrate
negative, it was identified that there was no color change in the medium.
Oxidase test (Cheesbrough, 2010)
Objective: To distinguish S. typhi from Pseudomonas species.
A piece of filter was placed in a clean petridish and 2 to 3 drops of 1% freshly prepared
oxidase reagent (tetramethyl-p-phenylene diamine dihydrocloride) was added. With a sterile
glass rod 1 or 2 colonies of the test organism was taken and rubbed on the filter paper.
Development of blue- purple colours within 10 seconds indicates positive test. Pseudomonas
aeruginosa was used as positive control and Escherichia coli as negative control.
Antimicrobial susceptibility test by disk diffusion method
All the isolated S. typhi were put into antibiotic susceptibility test by Kirby-Bauer disk
diffusion technique as per recommendation of the Clinical and Laboratory Standards Institute
(CLSI 2010). Panel of antibiotics were used � namely chloramphenicol, cotrimoxazole,
amoxycillin, ciprofloxacin, cephradine, gentamicin, ceftriaxone, azithromycin and nalidixic
acid. All tests were performed on Muller-Hinton agar (Appendix VI) media. The surface was
lightly and uniformly inoculated by sterile cotton swab stick. Prior to inoculation, the swab
stick was dipped into bacterial suspension having visually equivalent turbidity to 0.5
McFarland standards (Appendix VII). The swab stick then took out and squeezed on the wall
of the test tube to discard extra suspension. Inoculated plates were incubated at 35 to 370C for
24 hours. On the next day, plates were read by taking measurement of zone of inhibition.
Inhibition zones were measured in millimeter (mm) by using a ruler over the surface of the
plate with the lid open. The plates were hold a few inches above a black, non-reflecting
background and illuminated with reflected light. Results were recorded and graded as
Resistant (R) and Sensitive (S) according to the reference zone of inhibition for particular
antibiotic (CLSI 2010).
Standardization of the disk
In order to standardize the disk potency, a representative disk was tested against the reference
strains of S. typhi ATCC 19430. The zone of inhibition was compared with standard value as
recommended by CLSI (2010).
Serological tests:
Detection of Salmonella typhi antibody
Immunochromatographic test (Typhoid IgG/IgM combo rapid test ® USA) is a rapid assay
for the detection of S. typhi antibody in whole blood/serum specimen.
Principle of the test: Detection of S. typhi antibody by ICT is a qualitative test. The ICT
utilizes a unique combination of monoclonal antibody/colloidal gold dye conjugate and a
polyclonal antibody immobilized on the solid phase. This was selectively identifying S. typhi
antibody associated S. typhi infection with a high degree of sensitivity and specificity.
As the specimen follows through the absorbent pad in the sample well and through the
antigen/colloidal gold complex any S. typhi antibody present in the sample binds to the
conjugate forming an antigen/antibody complex. The sample and dye complex continue to
migrate along the membrane to the immobilized polyclonal antibody. In the presence of S.
typhi, the polyclonal antibody captures the complex. This forms a visible pink/purple band in
the test area of the card. If no antibody is present, there is no line in the area. The remaining
complex continues to migrates to another immobilized antibody on the membrane in the
control area of the card and is captured which then forms a band indicating proper
performance of the test.
The test cassette consists of � A colored conjugate pad containing recombinant S. typhi H
antigen and O antigen conjugated with colloid gold (Typhoid conjugates) and rabbit IgG gold
conjugates.
A nitrocellulose membrane strip containing two test bands (T1 and T2 bands) and a control
band. The T1 band is pre-coated with monoclonal anti human IgM for the detection of IgM
anti- S. typhi, T2 band is pre coated with reagents for the detection of IgG anti S. typhi and
the C band is pre-coated with goat anti rabbit IgG.
Reagent
1. Test strip
2. Sample Diluent
3. Positive Control

Procedural note:
All specimens or reagents were brought to room temperature (18-250) prior to testing and Foil
pouch was not opened until ready to perform the test.
Assay procedure
Step 1: Place the test device on a clean, flat surface.
Step 2: Be sure to label the device with specimen�s ID number.
Step 3: For whole blood test
One drop of whole blood (about 40-50 µl) was put to the sample well of the test unit, then
add 1 drop (about 35-50 ìl) of sample diluent immediately. The test unit was kept for 15
minutes. Results were read after 15 minutes. Result was not interpreted after more than 15
minutes. Positive results can be visible in as short as 1 minute.
Interpretation of ICT was given in (Appendix �VIII) (Photograph-12)
Polymerase chain reaction for detection of S. typhi directly from blood
sample:
Processing of blood samples and PCR amplification:
Three major steps:
Extraction of DNA from blood samples.
Amplification of DNA in thermal cycler.
Electrophoresis and then documentation under UV light.
DNA extraction from blood:
Extraction of DNA from blood samples (1ml) was carried out by modified lysis buffer
method. One ml EDTA containing blood was centrifuged by micro-centrifuge at 13000 rpm
for 5 minutes. Supernatant was discarded. Then 1 ml 0.2% Triton X-100 (Appendix-IX) was
added to the pellet. The mixture was vortexed, incubated at room temperature for 10 minutes
and centrifuged at 13000 rpm for 10 minutes. Supernatant was decanted. One ml 0.2% Triton
X-100 was added to the pellet again, vortexed and centrifuged at 13000 rpm for 10 minutes.
Then washed with 1 ml nuclease free water, centrifuged for 3 minutes and supernatant
discarded. The pellet was resuspended in 30 µl nuclease free water. Boiled for 10 minutes at
990C then centrifuged for 3 minutes. Supernatant was used as template for PCR (Jimenez and
Castro 2004; Nagarajan et al. 2009).
Preparation of reaction mixture
Sterile micro-centrifuge tubes (1.5ml) were taken and the tubes were labeled with date and
identification number. A total volume of 50 µl master mixture including 1 µl sample in which
included 10 x buffers, primer mixture, deoxy nucleoside triphosphate, taq polymerase and
PCR water.
Preparation of master mixture for each reaction (50 µl) contained:
10 x buffers - 5µl
2.5 micro mol deoxy nucleoside triphosphate - 4µl
25 Pico mol of each primer mix- 1µl (STI =0.5 µl, ST2 =0.5 µl)
2units of Taq DNA polymerase - 0.5µl
DDW/PCR water - 38.5µl
DNA sample - 1µl
Polymerase chain reaction for detection of S. typhi directly from blood sample DNA
amplification was carried out as described by Nagarajan et al. 2009 with some modification.
A mixture consisting of 5µl of 10X Ex Taq buffer (Takara, Japan), 4µl 2.5 mM dNTP mix

(2.5 mM each of dATP, dCTP, dGTP and dTTP, Takara, BIO INC, Japan), 38.5 µl of DDW
was taken in a 1.5 ml of micro centrifuge tube. Then 0.5 µl (25 pmol) each of gene specific
forward (STI) and reverse (ST2) primers were added. Afterwards 1µl of extracted DNA was
added and finally 0.5 µl Taq polymerase (Takara, BIO INC, Japan) was added and contents
of tube mixed well by pipetting. The tubes were placed in a thermal cycler and allowed to run
by the following protocol by Massi and others, Ambati and others with some modification
(Massi et al. 2003; Ambati, Nath and Das 2007).
Protocol of thermal cycles:
Denaturation at 940C for 30 seconds.
Primer annealing at 540C for 30 seconds.
Extension at 72 0C for 1 minute.
Final extension at 720C for 5 minutes.
Above step were repeated for 30 cycles in an automated DNA thermal cycler (Eppendorf,
Germany). Final extension was done at 720C for 5 minutes. The PCR products were run in
1% agarose gels stained with ethidium bromide and visualized under the UV transilluminator.
In nested PCR, the amplified product of the first PCR is used as template. In the second
amplification (nested PCR), a second set (ST3 and ST4) of primer was added to the reaction
mixture (50 µl). The tube was kept in a thermal cycler and allowed to run for 30 cycles as
well as the same protocol of the first round PCR.
Primer used for PCR:
30 cycles
For nested PCR oligonucleotide primers as first described by Song et al. 1993 and used by
Massi et al. 2003 and Ambati and others 2007. The sequences from 5' to 3' ends of these
oligonucleotide primers were as follows:
Designation- sequence (5' to 3') Target gene Amplicon size
ST1- 5'-TAT GCC GCT ACA TAT GAT GAG-3' Flagellin gene 495 bp
ST2 - 5'-TTA ACG CAG TAA AGA GAG-3'
Above primers were used for first round PCR to amplify 495 bp sequence of flagellin gene.
Designation- sequence (5' to 3') Target gene Amplicon size
ST3- 5'-ACT GCT AAA ACC ACT ACT-3' Flagellin gene 364 bp
ST4 - 5`-TGG AGA CTT CGG TCG CGT AG-3'
Above pairs of primers were used for second round PCR to amplify a 364 bp sequence of
flagellin gene.
Agarose gel electrophoresis:
The PCR product was analyzed in 1% agarose gel by electrophoresis for 35 minutes to detect
specific band.
Preparation of agarose gel:
One percent agarose gel was prepared by melting 3 gm agarose in 200 ml of diluted TBE
buffer (1:4) using microwave woven. The agarose was allowed to cool about 500C and was
poured into gel electrophoresis unit with spacers and comb. After solidification of the gel, the
comb was removed and wells were formed. During electrophoresis, gel was placed in a
solution containing Tris- EDTA- borate buffer (TBE buffer) and ethidium bromide
(0.5µg/ml) in the horizontal electrophoresis chamber.
Loading and Running of the sample:
Five µl of amplified product was mixed with 2.0 µl gel loading dye. The mixture was slowly
loading into the well using disposable micropipette tips. Marker DNA of known size (100 bp
ladder) was loaded in one well to determine the size of amplified PCR products.
Electrophoresis was carried out at 100 volts for 35 minutes in 1% agarose gel, prestained with
ethidium bromide in a submarine gel apparatus (Mupid 2 plus submarine electrophoresis,
Japan).
Visualization /documentation under Transilluminator
Following electrophoresis, amplified product, the bands (495 bp in first round and 364 bp in
second round of nested PCR) of the sample of the study was visualized by
transilluminator.The amplicon size was determined by comparing position of amplicon in
respect to that of a 100 bp ladder that was loaded in adjacent well and simultaneously
electrophoresed. And the gel was photographed by a digital camera and was transferred data
to computer for further documentation.
Interpretation
PCR positive: Samples were scored as positive when a PCR product of 495 bp could be
detected in first round PCR.
In nested PCR, samples were scored as positive when a PCR product of 364 bp could be
detected.
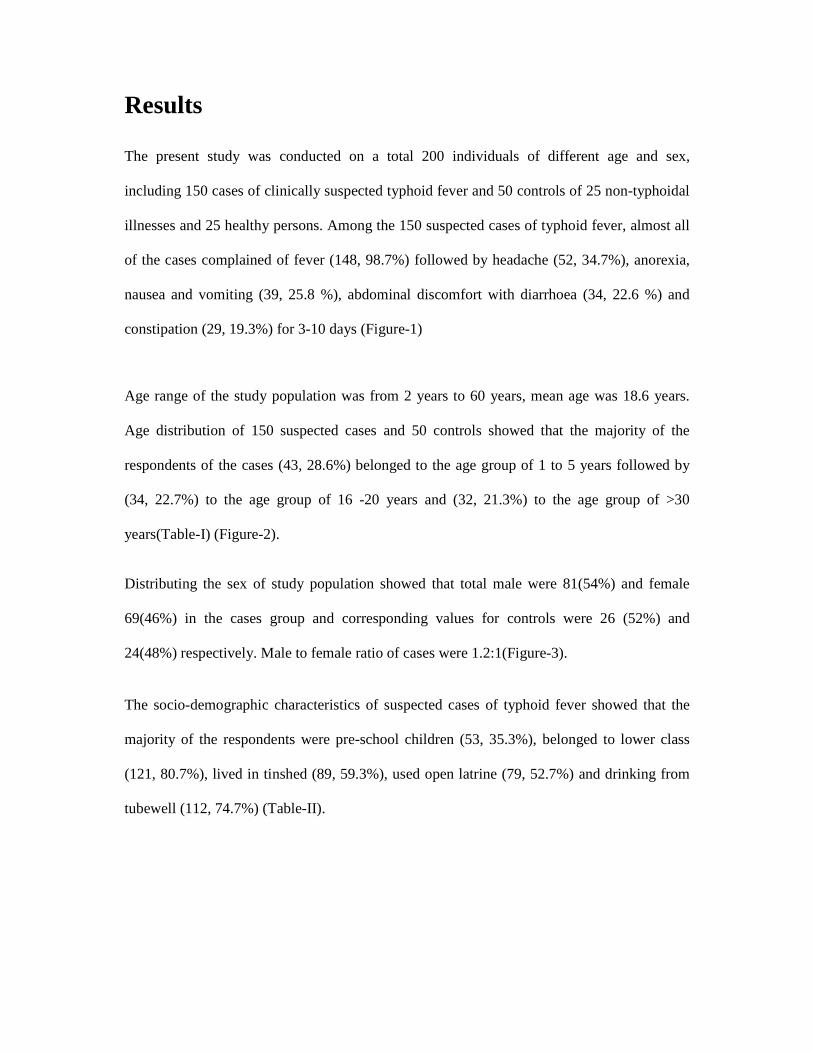
Results
The present study was conducted on a total 200 individuals of different age and sex,
including 150 cases of clinically suspected typhoid fever and 50 controls of 25 non-typhoidal
illnesses and 25 healthy persons. Among the 150 suspected cases of typhoid fever, almost all
of the cases complained of fever (148, 98.7%) followed by headache (52, 34.7%), anorexia,
nausea and vomiting (39, 25.8 %), abdominal discomfort with diarrhoea (34, 22.6 %) and
constipation (29, 19.3%) for 3-10 days (Figure-1)
Age range of the study population was from 2 years to 60 years, mean age was 18.6 years.
Age distribution of 150 suspected cases and 50 controls showed that the majority of the
respondents of the cases (43, 28.6%) belonged to the age group of 1 to 5 years followed by
(34, 22.7%) to the age group of 16 -20 years and (32, 21.3%) to the age group of >30
years(Table-I) (Figure-2).
Distributing the sex of study population showed that total male were 81(54%) and female
69(46%) in the cases group and corresponding values for controls were 26 (52%) and
24(48%) respectively. Male to female ratio of cases were 1.2:1(Figure-3).
The socio-demographic characteristics of suspected cases of typhoid fever showed that the
majority of the respondents were pre-school children (53, 35.3%), belonged to lower class
(121, 80.7%), lived in tinshed (89, 59.3%), used open latrine (79, 52.7%) and drinking from
tubewell (112, 74.7%) (Table-II).
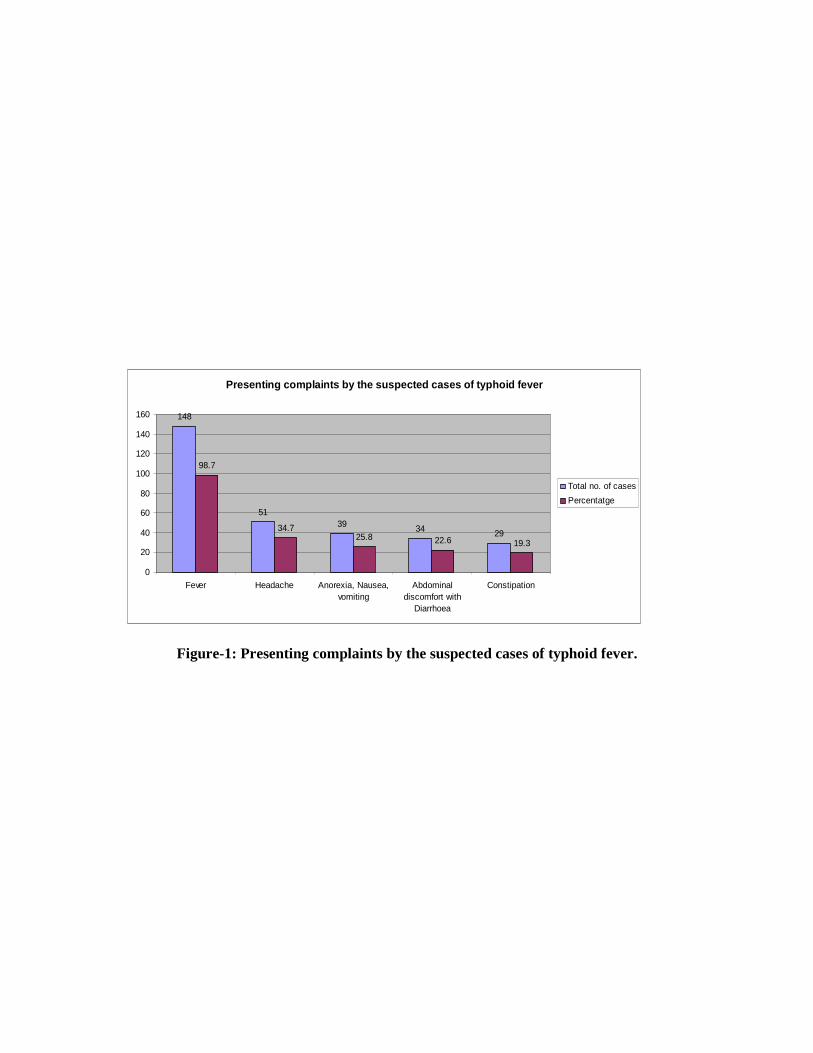
Presenting complaints by the suspected cases of typhoid fever
148
5139 34 29
98.7
34.725.8 22.6 19.3
0
20
40
60
80
100
120
140
160
Fever Headache Anorexia, Nausea,vomiting
Abdominaldiscomfort with
Diarrhoea
Constipation
Total no. of cases
Percentatge
Figure-1: Presenting complaints by the suspected cases of typhoid fever.
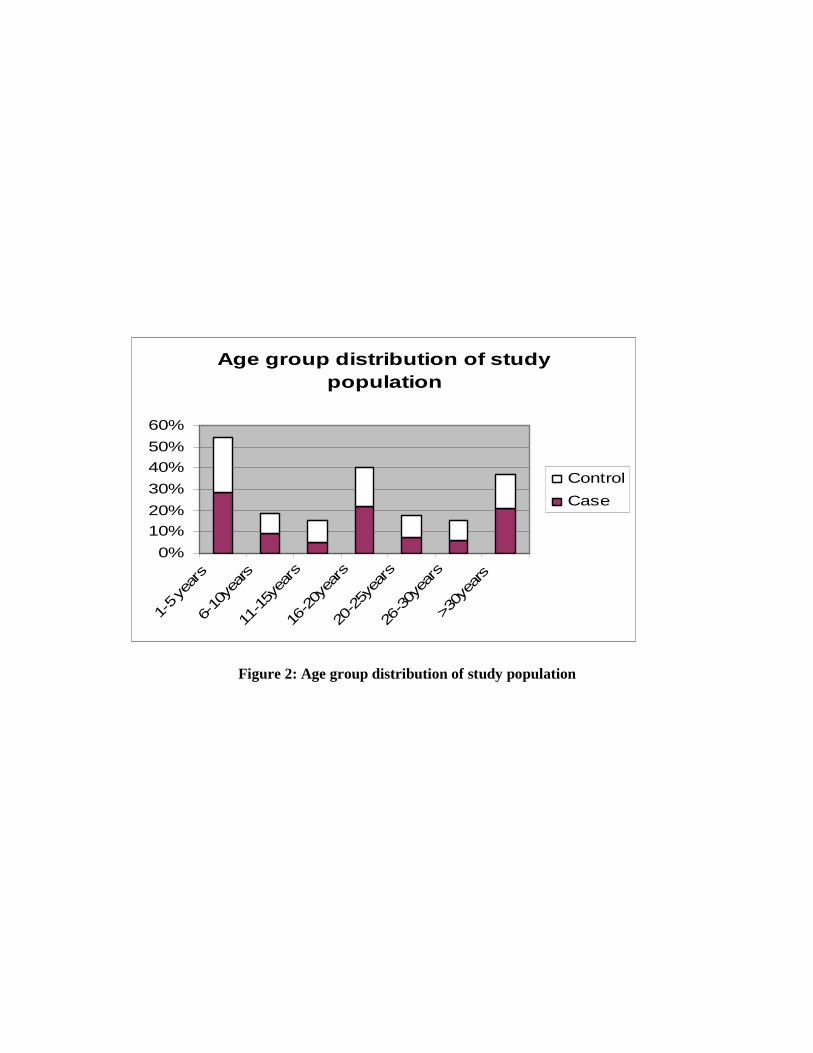
Age group distribution of study population
0%
10%
20%
30%
40%
50%
60%
1-5 ye
ars
6-10
years
11-15y
ears
16-20y
ears
20-25y
ears
26-30y
ears
>30y
ears
Control
Case
Figure 2: Age group distribution of study population

Table I: Age group distribution of suspected cases of typhoid fever
Age in years No of cases (%)
1 - 5 43 (28.6%)
6 - 10 14 (9%)
11 - 15 8 (5.3%)
16 - 20 34 (22.7%)
21 - 25 12 (7.7%)
26 - 30 7 (4.7%)
>30 33 (21.3%)
Male female ratio 1:1.2

Sex pattern of suspected cases of typhoid fever
54%
46% Male
Female
Sex pattern of control group
52%
48%Male
Female
Figure-3: Sex pattern of study population.

Table-II: The socio-demographic characteristics of study population (n=150)
Factors Number of cases (%)
Illiterate 26 (17.3)
Pre-school 53 (35.3)
Primary level 31 (20.7) Education status
Secondary level or higher 36 (24)
Lower class (Up to Tk. 15,000/=) 121(80)
Middle class (Tk. 15,000-50,000/=) 26(17.3) Socio-economic class as per monthly income
Upper class (Tk. >50,000/=) 03(2.0)
Tin shed 89 (59.3)
Mud house 35 (23.3)
Tin shed building 20 (13.3) Housing condition
Building 06 (4)
Tube well 112 (74.7)
Municipal Supply 35 (23.3) Source of drinking water
Ponds water 3 (2)
Figures in parenthesis indicate percentage.

Among the three investigations performed for the diagnosis of typhoid patients, polymerase
chain reaction showed maximum 133(88.7%) positive result followed by
Immunochromatography (ICT) test 106 (70.7%) and blood culture 23(15.3%) (Figure-4).
Among 150 blood samples from the suspected cases, 23(15.3%) were positive for Salmonella
typhi by blood culture. None of the healthy controls was positive by blood culture. The
highest rate of blood culture positivity for S. typhi 09(39.1%) was found among 1 to 5 years
of age group followed by 5(21.8%) among 6 to 10 years (Table-III).
By observing the relationship of blood culture positivity and duration of illness, it was found
that all of the samples yielding positive result were collected from the cases complaining of
3-7 days of fever (Table-IV).
Considering the relationship of antibiotic usage with the results of blood culture of the
suspected cases of typhoid fever, it was found that none of the blood culture positive cases
taken any antibiotic during the episode and majority of the blood culture negative cases gave
history of taking different antibiotics for variable periods (Table-V).
Antimicrobial susceptibility pattern of S. typhi isolates (n=23) showed that the highest
number (73.9%) of isolates were sensitive to chloramphenicol, followed by cotrimoxazole
(69.6%), ceftriaxone (60.9%), gentamicin (52.2%), ceftazidime (47.8%) and azithromycin
(43.5%) (Figure-5).

Results of three tests performed typhoid fever
15.30%
70.70%
88.70%84.70%
29.30%
11.30%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Blood culture ICT PCR
Positive
Negative
Figure-4: Different test performed for diagnosis of typhoid fever.
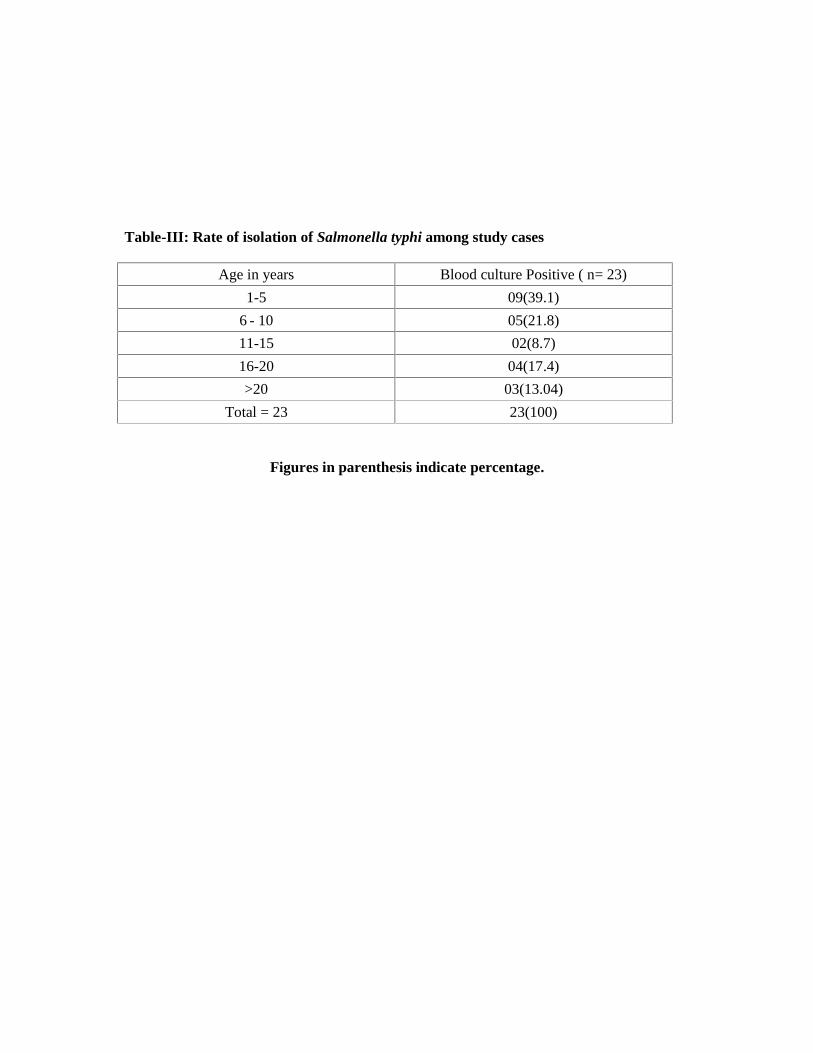
Table-III: Rate of isolation of Salmonella typhi among study cases
Age in years Blood culture Positive ( n= 23)
1-5 09(39.1)
6 - 10 05(21.8)
11-15 02(8.7)
16-20 04(17.4)
>20 03(13.04)
Total = 23 23(100)
Figures in parenthesis indicate percentage.

Table-IV: Relationship of blood culture positivity with duration of fever of the cases
No. (%) of patients and duration of illness in days Result of blood culture 1-3 4-7 8-10 11-14
Positive 1(0.7%)* 22(14.7%) 0(0%) 0(0%)
Negative 01(0.7%) 96(64%) 26 (17.3%) 2 (1.3%)
*The case was presenting with fever for 3 days.

Table-V: Antibiotic usage by the blood culture-negative suspected cases of typhoid fever
Antibiotic Dosage schedule Duration of intake
(days) No. (%) of cases
Ciprofloxacin 100-500 mg twice
daily 2-7 23 (25.9%)
Cotrimoxazole 960 mg twice
daily 2-5 14 (22.2%)
Tetracycline 250 mg twice
daily 2-7 9(5.6%)
Azithromycin 500 mg single 3 18 (14.8%)
Amoxycillin 250-500mg thrice
daily 3-5 13(13.0%)
Levofloxacin 500 mg single 3-7 17 (5.6%)
Cephradin 250 mg thrice
daily 6 16 (1.9%).
*17 patients taken some drugs but cannot mentioned the name properly.
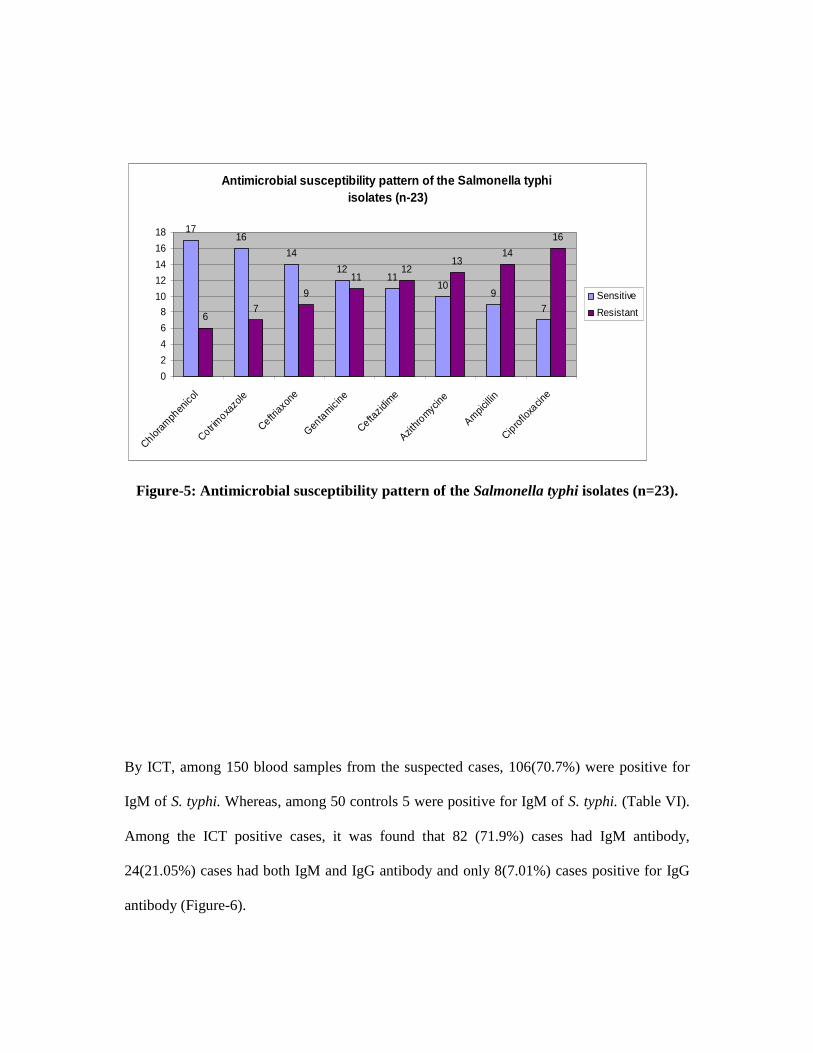
Antimicrobial susceptibility pattern of the Salmonella typhiisolates (n-23)
1716
14
1211
109
76
7
9
1112
1314
16
0
2
4
6
8
10
12
14
16
18
Chloram
phen
icol
Cotrimoxa
zole
Ceftriax
one
Genta
micine
Ceftazid
ime
Azithr
omycine
Ampic
illin
Cipro
floxa
cine
Sensitive
Resistant
Figure-5: Antimicrobial susceptibility pattern of the Salmonella typhi isolates (n=23).
By ICT, among 150 blood samples from the suspected cases, 106(70.7%) were positive for
IgM of S. typhi. Whereas, among 50 controls 5 were positive for IgM of S. typhi. (Table VI).
Among the ICT positive cases, it was found that 82 (71.9%) cases had IgM antibody,
24(21.05%) cases had both IgM and IgG antibody and only 8(7.01%) cases positive for IgG
antibody (Figure-6).

By observing the relationship between ICT and PCR, it was found that 103 cases were both
ICT (IgM) and PCR positive (Table�VII), 3 samples (clotted blood) were ICT positive but
PCR negative.
The ICT (IgM) was positive in 14(60.9%) out of 23 culture positive typhoid cases. Sensitivity
and specificity of ICT was 77.4% and 82.3% respectively by considering PCR as gold
standard (Table VII).
Among 150 blood samples from the suspected cases, subjected to PCR, 133(88.7%) showed
positive results for flagellin gene of S. typhi, and all of the 50 blood samples from the
controls were negative by PCR (Table IX). The samples of the cases showing negative
results with blood culture (n=127) were also tested by PCR and 110 (86.5%) of them were
positive by the PCR (Table X). The rate of positivity by PCR (88.7%) was found to be much
higher than blood culture (15.3%) method (Figure- 7).
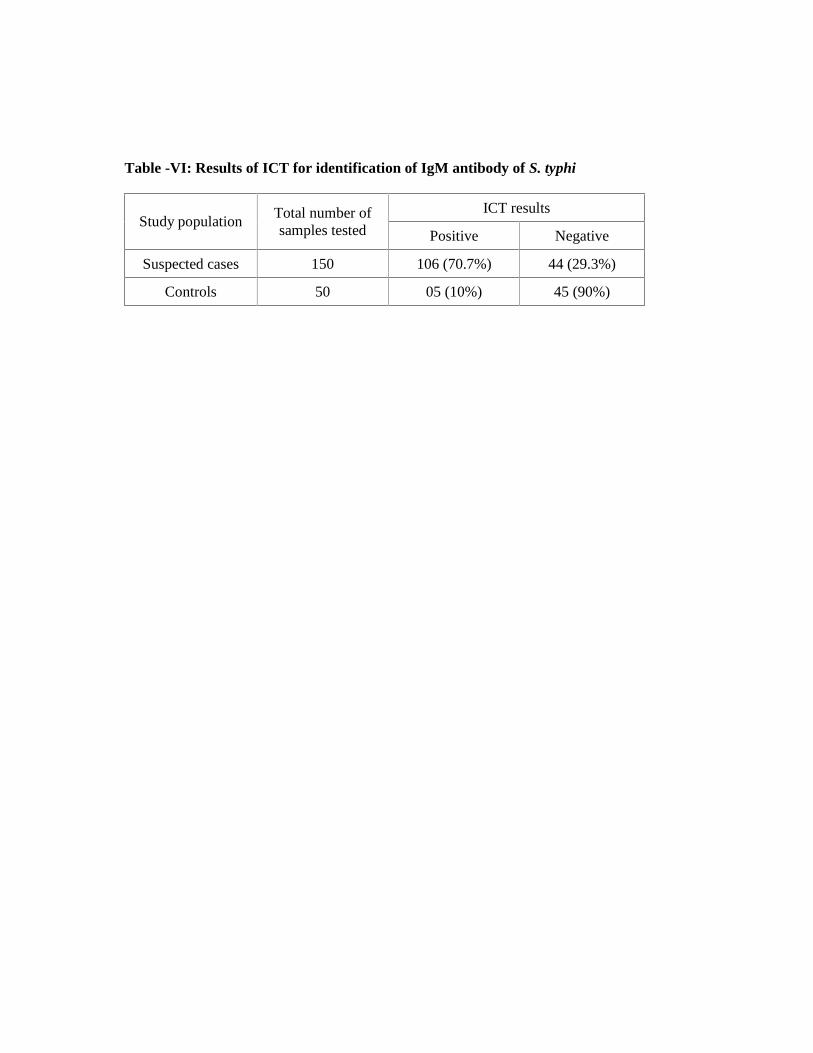
Table -VI: Results of ICT for identification of IgM antibody of S. typhi
ICT results Study population
Total number of samples tested Positive Negative
Suspected cases 150 106 (70.7%) 44 (29.3%)
Controls 50 05 (10%) 45 (90%)
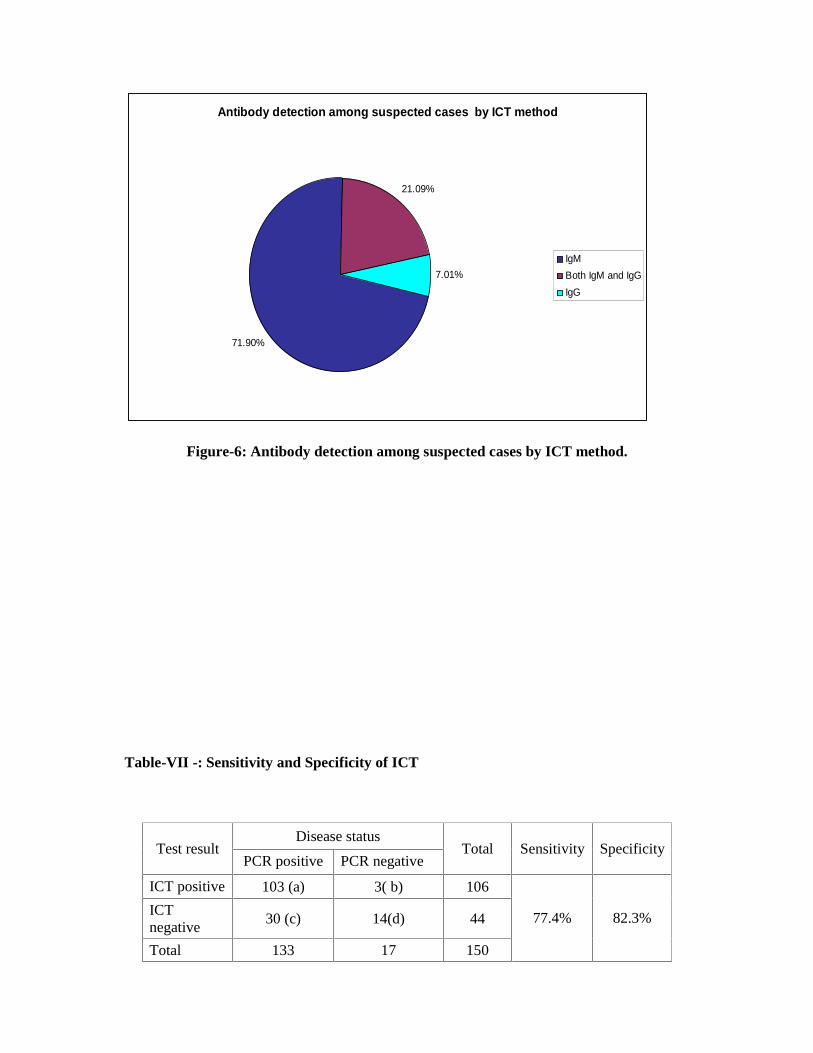
Antibody detection among suspected cases by ICT method
71.90%
21.09%
7.01%
IgM
Both IgM and IgG
IgG
Figure-6: Antibody detection among suspected cases by ICT method.
Table-VII -: Sensitivity and Specificity of ICT
Disease status Test result
PCR positive PCR negative Total Sensitivity Specificity
ICT positive 103 (a) 3( b) 106
ICT negative 30 (c) 14(d) 44
Total 133 17 150
77.4% 82.3%

N.B: Sensitivity and specificity was calculated by the following formula considering PCR as
gold standard
Sensitivity= 100 x a/a+c, Specificity = 100 x d/b+d.
Positive predictive value = a x 100 / a+b = 97.2%
Negative predictive value = d x 100 / c+d =31.8%
a = True positive, b = False positive, c = False negative and d = True negative.
PPV = Positive predictive value; NPV = Negative predictive value

Table-VIII: Results of polymerase chain reaction (PCR) for identification of flagellin
gene of S. typhi
PCR results Study population
Total number of samples tested Positive Negative
Suspected cases 150 133 (88.7) 17 (11.3)
Controls 50 00 (00) 50 (100)
Figures in parenthesis indicate percentage.

Table-IX: Comparison of culture and PCR methods for identification of Salmonella
typhi
No(%) of cases showing culture results PCR results
Positive Negative Total
Positive 23(100) 110(86.7) 133(88.7)
Negative 0(0) 17(13.3) 17(11.3)
Total 23(100) 127(100) 150(100)
Figures in parenthesis indicate percentage.
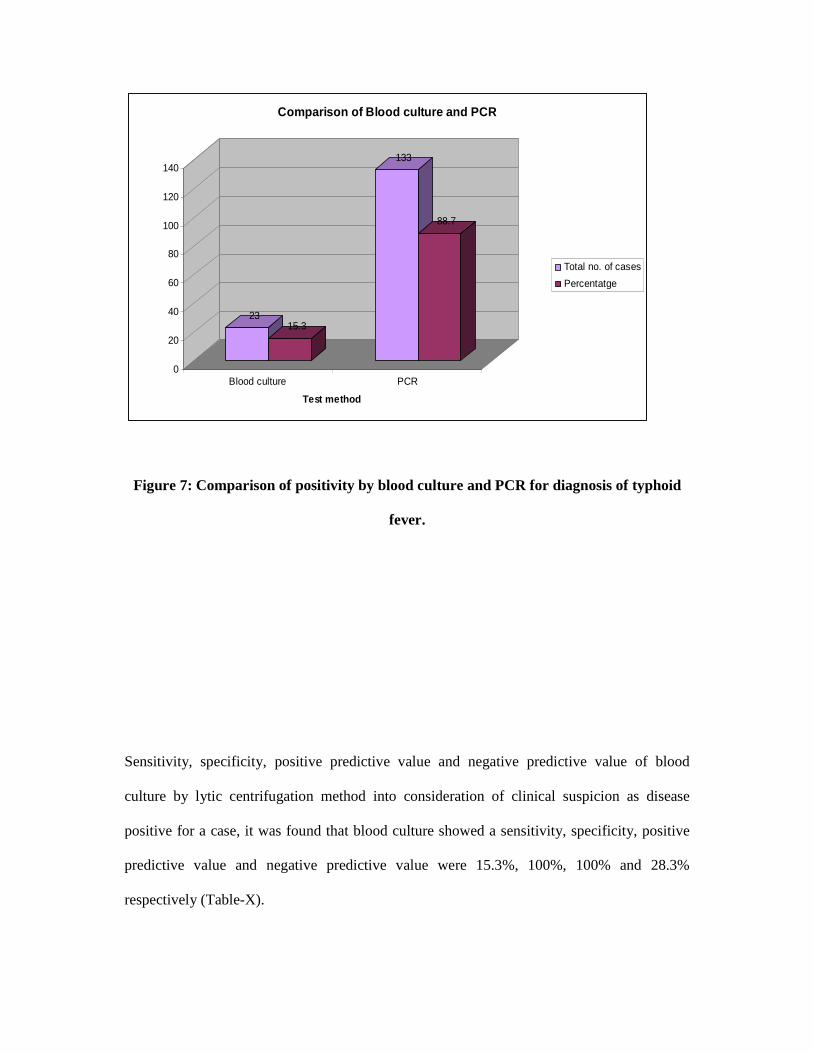
2315.3
133
88.7
0
20
40
60
80
100
120
140
Blood culture PCR
Test method
Comparison of Blood culture and PCR
Total no. of cases
Percentatge
Figure 7: Comparison of positivity by blood culture and PCR for diagnosis of typhoid
fever.
Sensitivity, specificity, positive predictive value and negative predictive value of blood
culture by lytic centrifugation method into consideration of clinical suspicion as disease
positive for a case, it was found that blood culture showed a sensitivity, specificity, positive
predictive value and negative predictive value were 15.3%, 100%, 100% and 28.3%
respectively (Table-X).
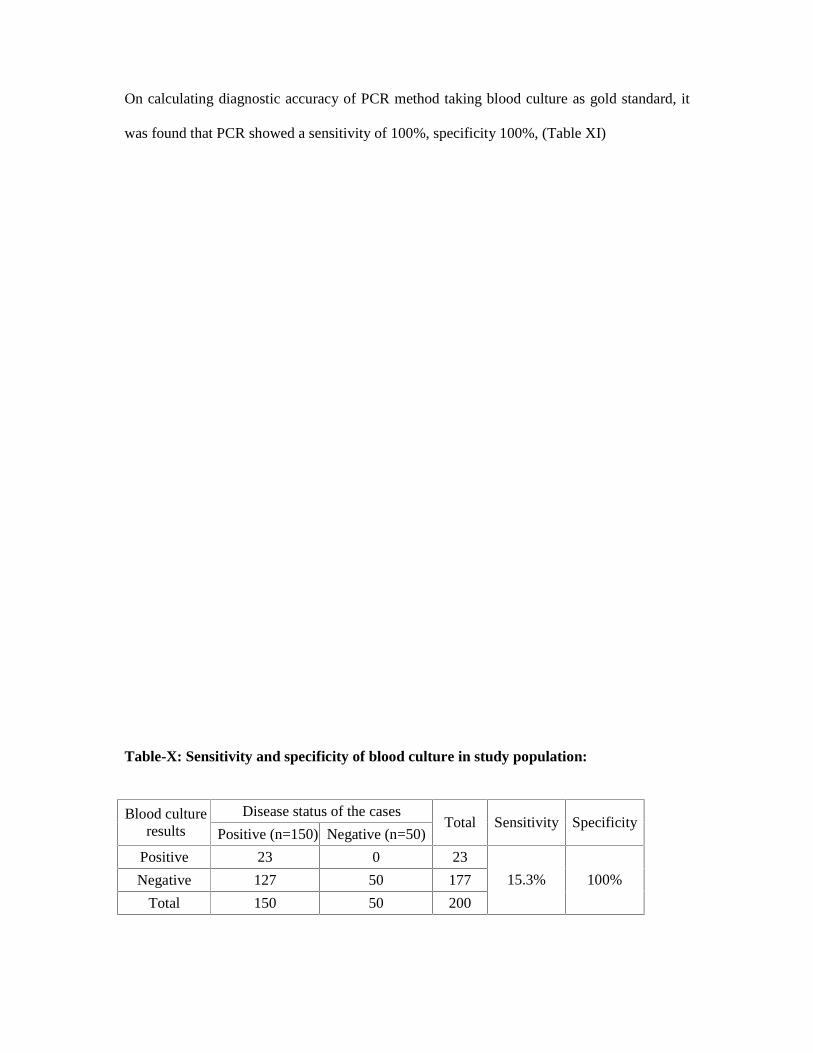
On calculating diagnostic accuracy of PCR method taking blood culture as gold standard, it
was found that PCR showed a sensitivity of 100%, specificity 100%, (Table XI)
Table-X: Sensitivity and specificity of blood culture in study population:
Disease status of the cases Blood culture
results Positive (n=150) Negative (n=50) Total Sensitivity Specificity
Positive 23 0 23
Negative 127 50 177
Total 150 50 200
15.3% 100%
N.B: Sensitivity and specificity was calculated by the following formula
Sensitivity= 100 x a/a+c, Specificity = 100 x d/b+d.
a = True positive, b = False positive, c = False negative and d = True negative.
PPV = Positive predictive value; NPV = Negative predictive value
Positive predictive value = a x 100 / a+b = 100%
Negative predictive value = d x 100 / c+d =28.3%.
Table-XI: Diagnostic accuracy of PCR for diagnosis of typhoid fever
PCR results No(%) of cases showing culture results Total
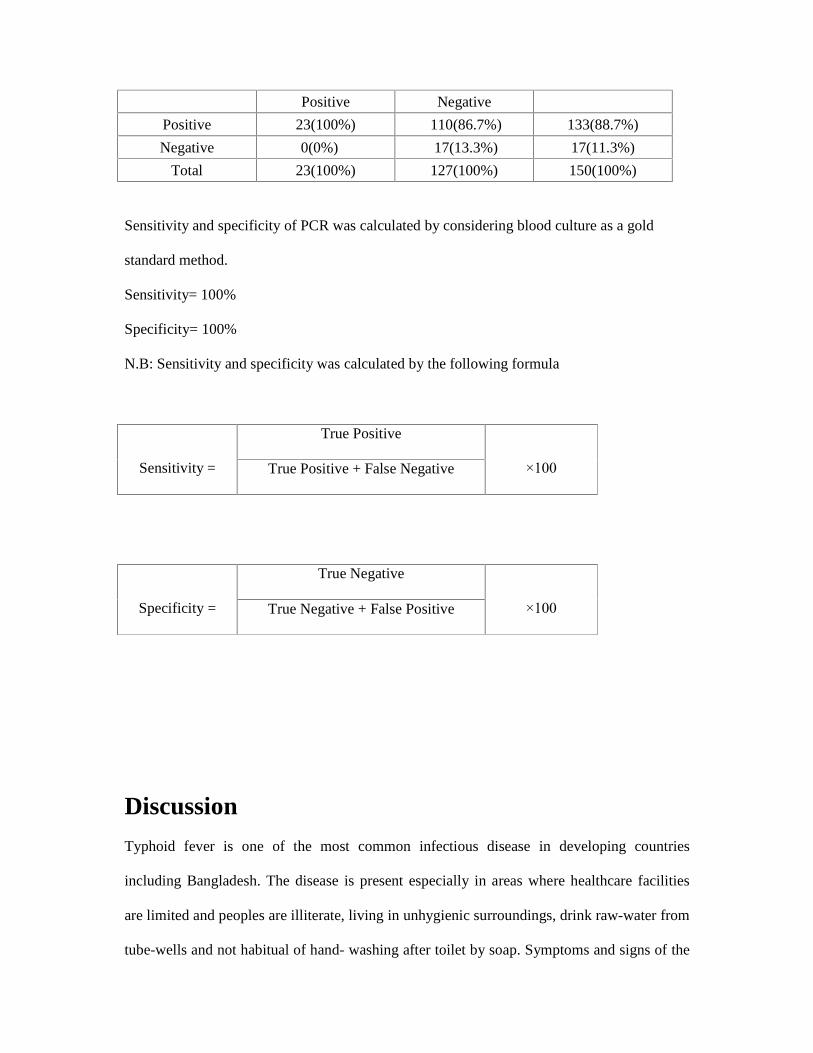
Positive Negative
Positive 23(100%) 110(86.7%) 133(88.7%)
Negative 0(0%) 17(13.3%) 17(11.3%)
Total 23(100%) 127(100%) 150(100%)
Sensitivity and specificity of PCR was calculated by considering blood culture as a gold
standard method.
Sensitivity= 100%
Specificity= 100%
N.B: Sensitivity and specificity was calculated by the following formula
True Positive
Sensitivity = True Positive + False Negative
×100
True Negative
Specificity = True Negative + False Positive
×100
Discussion
Typhoid fever is one of the most common infectious disease in developing countries
including Bangladesh. The disease is present especially in areas where healthcare facilities
are limited and peoples are illiterate, living in unhygienic surroundings, drink raw-water from
tube-wells and not habitual of hand- washing after toilet by soap. Symptoms and signs of the
disease are non-specific and laboratory tests are essential for diagnosis. Early and reliable
diagnosis of the disease is not only important in relieving patients� suffering, but also
necessary to avoiding life threatening complications including perforation of the intestine.
In the present study, 200 purposefully selected individuals were investigated including 150
clinically suspected cases of typhoid fever and 50 controls (25 non-typhoid febrile illnesses
and 25 healthy individuals). The disease affected all ages, however most of the cases (28%)
of the study were in the age group of 1�5 years (Table I). This findings correlates with the
observation made by Saha and associates who found that children between 2-3 years of age
are most susceptible age group (35.6%) (Saha et al. 2003). Almost similar study done by
Brooks and others showed that the prevalence of typhoid fever in children of under 5 years
were much higher than other age group (Brooks et al. 2005). The child aged group < 5 years
were more prone to infection, which may be due to a lack of immunity transferred by
mothers� milk or the non consumption of potable drinking water as is the common practice in
rural areas (Saha et al. 2003).
In present study, among 150 clinically suspected typhoid cases 54% were male and 46% were
female. Another study done by Butler and others also showed similar result that infection rate
was slightly higher in male (Butler et al. 1991). Butler expressed his opinion that greater
exposure of male to contaminated food and water out side the home might be region of higher
rate of infection among this population.
The socio-demographic characteristics of suspected cases of typhoid fever in this present
study showed that the majority of the respondents were pre-school children (53, 35.3%) and
(26, 17.3%) were illiterate, belonged to lower class (121, 80.7%), used open latrine (79,
52.7%) and drinking from tubewell (112, 74.7%) (Table II). Similar findings also have been
reported by Sur and others showing that the illiteracy rates were highest in the cases of
typhoid fever. In the same study unhygienic latrines were the main sources of spreading
typhoid diseases and the sanitation condition of low income areas was remarkably poor (Sur
et al. 2007). Lack of safe drinking water and unhygienic sanitation are believed to contribute
the transmission of typhoid fever (Jenkins and Gillespie 2009). It has been observed that the
water and sewage pipelines lie close together in the slum areas of Bangladesh and they are
prone to leakage and cross-contamination. In addition most of the people cannot afford the
sanitary latrines in Bangladesh due to poverty which further carries the risk of exposure to
Salmonella typhi.
In the present study, blood culture, ICT and nested PCR were studied. The nested PCR
showed maximum (133 out of 150, 88.7%) positive result followed by ICT (106, 70.7%) and
blood culture (23, 15.3%). All of the culture positive cases were positive by PCR and among
culture negative cases 86.5% were positive by PCR. Almost similar study was done in Delhi,
India, and used blood samples from 40 clinically suspected cases of typhoid fever, and found
100% of culture positive (n=20) and 75% (15/20) of culture negative cases positive by PCR
(Kumar et al. 2002).
In the present study, among 150 clinically diagnosed typhoid fever cases 23(15.3%) showed
positive blood culture for S. typhi (Table III). Similar finding was also reported by Begum
and associates in Bangladesh in 2007, where they found an isolation rate of S. typhi was 14%
(Begum et al. 2009). Saha and others from Kolkata in 2003 found an isolation rate of S. typhi
was 21.1% (Saha et al. 2003). Hossain (2001) from Bangladesh reported an isolation rate of
S. typhi was 16.67% (Hossain 2001). The relative low sensitivity of the blood culture in
diagnosing typhoid fever is a common phenomenon. It may be due to indiscriminate use of
antibiotics and difficulties in obtaining adequate volume of blood for culture from children
(Bhutta and Mansurali 1999; Mohanty and Ramana 2007). Blood culture has the promise of
diagnosis in the first week and is very specific, but its sensitivity is poor due to various
factors. Sensitivity of cultures can be affected by antibiotic treatment, type of culture
medium, length of incubation and variations of bacteraemia (Gilman et al. 1975; Miller and
Pegues 2000).
In this study, the highest rate of positive blood culture for S. typhi 09(39.1%) was found
among 1 to 5 years of age group followed by 5(21.8%) among 6 to 10 years (Table-III).
Another similar study by Saha and others from Bangladesh showed that the majority (54.5%;
213 of 391) of S. typhi isolates were from children who were younger than 5 years, and 27%
(105 of 391) were from children in the first 2 years of life. They also mentioned that the
isolation rate was highest (17.4%, 68 of 486) in the second year of life (Saha et al. 2001).
In present study, majority of the blood culture negative cases gave history of taking different
antibiotics for variable periods. Antibiotic treatment prior to collection of sample inhibits the
growth on blood cultures (Gasem et al. 1995; Cheesebrough 2010). Similar finding were
found by Lin and others, where they showed that the S. typhi was recovered from 5.3% of
patients with prior antibiotic intake versus 5.8% without prior antibiotics (Lin, Ho and Bay
2000).
In this study, the majority (73.9%) of isolates of S. typhi were sensitive to chloramphenicol,
followed by cotrimoxazole (69.6%). There have been some reports of the reemergence of the
sensitivity of S. typhi to chloramphenicol and other first line drugs. Bhatia and others reported
that the highest (96%) sensitivity of Salmonella typhi to chloramphenicol in India (Bhatia,
Mathur and Arora 2007). Another study by Yashavanth and Vidyalakshmi found that the re-
emergence of chloramphenicol (97.4%) sensitivity among the strain of S. typhi pathogens in
Mangalore in 2007 (Yashavanth and Vidyalakshmi 2010).
In present study, some isolates of S. typhi were found resistant to ciprofloxacin and nalidixic
acid. Nalidixic acid-resistant (NAR) S. typhi with decreased susceptibility to ciprofloxacin is
now endemic in India and neighbouring countries, constituting a threat to global health
(Chandel et al. 2000; Threlfall and Ward 2001a; Hakanen et al. 2001).
Another study from Bangladesh showed that the decreased susceptibility to ciprofloxacin was
detected in 24 (18·2%) out of 132 randomly selected strains during 1990�2002 (Rahman et al.
2006). Fluoroquinolones, especially ciprofloxacin, have been in use for more than 18 years
and have remained an important weapon against S. typhi. In spite of this, in recent years,
several reports have appeared worldwide concerning reduced activity of ciprofloxacin against
S. typhi (Wain et al. 1997; Chandel et al. 2000; Threlfall and Ward 2001a; Hakanen et al.
2001). In perspective of Bangladesh, ciprofloxacin is commonly used in case of typhoid fever
may be due to ciprofloxacin continues to be the mainstay in the treatment of typhoid fever as
it is orally effective and economical.
In this study, 40% of isolates of S. typhi were found resistant to ceftriaxone. Third generation
cephalosporins have been recommended as an alternative to quinolone treatment in enteric
fever and several physicians have claimed good results with them, particularly with
ceftriaxone (Girgis et al.1995a). As consequences of extensive use of ceftriaxone and other
third generation cephalosporin, resistance is being reported with increasing frequency all over
the world. Another study by Saha and others reported about the highly ceftriaxone resistant
strain of S. typhi in Bangladesh (Saha et al. 1999).
ICT has been studied in many countries and they found significantly higher sensitivity and
specificity (Jesudason, Esther and Mathai 2002; Pastoor et al. 2008; Anusha, Ganesh and
Lalitha 2011). An evaluation of ICT (Typhidot) in India was found to be 100% sensitive and
80% specific compared to a blood culture as �gold standard� (Jesudason, Esther and Mathai
2002). In present study, sensitivity and specificity of ICT in suspected typhoid cases were
found 77.4% and 82.3% respectively. In another study from India by Nakhla and others
showed almost similar type of result that the sensitivity and specificity of ICT (IgM) was
80% and 71.4% respectively (Nakhla et al. 2011). Abdoel and associates showed that the
sensitivity of ICT improved with the duration of illness from 30.8% for samples collected
during the first 4-5 days of illness to 45.5% for samples collected between days 7 and 9, and
to 84.6% for the samples collected more than 9 days after the onset of illness (Abdoel et al.
2007).
In this study, out of 127 cultures negative typhoid cases 92 (72.5%) were positive by ICT
method. Almost similar types of results were also reported by Anggraini and others, where
they showed that ICT (IgM) positive 66% among culture negative but clinically diagnosed
typhoid fever (Anggraini Handoyo and Aryati 2004). In another study from Pakistan showed
that only 28% (7 out of 25) of culture negative typhoid fever cases were ICT (IgM) positive
(Bhutta and Mansurali 1999). The lower detection rate in that study may be explained by the
reason that the study was conducted on random selection rather than the clinically diagnosed
typhoid fever cases.
In this study, out of 23 culture positive cases, 9 (39.1%) were negative for ICT (IgM).
Although these patients may have had antibodies at a lower titre. It is well recognized that

patients with blood culture-confirmed typhoid fever may have a negative antibody response
throughout the course of their illness. This lack of antibody response among such patients has
been attributed to short duration of illness (3-7 days, Table-IV). Seropositivity increased with
duration of illness and seroconversion was observed in the majority of typhoid patients with a
negative IgM result for the first collected serum sample. Seropositivity in the IgM increased
from less than 30% for samples collected during the first week of illness to over 95% for
samples collected from patients ill for more than 9 days (Hatta et al. 2002).
Among 106 ICT (IgM) positive cases, 3 cases showed negative result by PCR due to clotting
of blood because of delayed processing. Thirty PCR positive cases showed negative result by
ICT (Table-VII). The false negative ICT in this case was probably due to the failure of ICT to
detect antibodies the because antibody titre did not yet reach the detectable level in these
patients.
In the present study the rate of diagnosis of typhoid fever by the PCR was 88.7% compared
with blood culture, where it was 15.3%. The rate of positivity of the nested PCR using 1 ml
of blood appears to be higher than that of blood culture performed with 8 ml blood samples.
The results show that nested PCR method can be an alternative tool to confirm clinical
diagnosis of typhoid fever. The finding of the PCR results is consistent with the previous
observations, which showed that the same nested PCR, as well as other PCRs for typhoid
fever, had higher sensitivities than blood culture (Haque et al. 2001; Kumar et al. 2002; Massi
et al. 2003; Prakash et al. 2005; Hatta and Smit 2007). In Varnassi, India, Prakash and others
used the nested PCR with a different DNA extraction method and reported nested PCR was
again better (53 positive of 57 samples, 73.0%) than blood culture (17 positive of 53 samples,
32.0%) (Prakash et al. 2005). In another study, in Pakistan, 55 cases of suspected typhoid
fever were diagnosed by the PCR and blood culture, gave 58.2% and 14.5% positivity,
respectively, showing significantly better results by PCR (Hoque et al. 2001). A large, well-
designed study in Indonesia by Hatta and Smith reported a sensitivity of 61.8% by blood
culture and 84.5% by PCR from blood samples (Hatta and Smit 2007). A study from Nepal
reported sensitivity of PCR 82.7% which is much higher than blood culture (26.9%) (Ambati
et al. 2007). Another study in South Sulawesi, Indonesia, showed 63.0% were positive by
PCR compared to 13.7% positive by blood culture (Massi et al. 2003).
In this study, nested PCR was used to yield 364 bp amplicon specific for flagellin gene of S.
typhi. This was preferred because hypervariable region VI of the flagellin gene is unique for
S. typhi and its amplification was found to provide 100% specificity (Frankel, 1994; Song et
al. 1993). In an alternative, targetting Vi gene, gives false-positive results, because of the
presence of the gene in another salmonella namely S. paratyphi C as well (Hashimoto et al.
1995).
Among the suspected typhoid cases in the present study, PCR was able to detect S. typhi in
88.70% of the blood samples and none of the healthy controls was positive. The rate of
detection by PCR was significantly higher (p<0.001 each) than blood culture. The low rate of
detection by blood culture is probably due to antibiotics taken by the patients before sample
collection. Antibiotics are freely available in Bangladesh over the counter without
prescription and many of the patients reported to have antibiotics before collection of
samples.
It is, therefore, concluded that the PCR method was much superior to blood cultures yielding
very high sensitivity and specificity. Although the PCR method requires extensive
infrastructure and specialized skilled personnel, and cannot be made available everywhere,
especially in developing countries, it can be made available to the reference centres for
utilizations by other healthcare facilities following referral system. In fact, due to the rapid

and definitive diagnosis, hospital admission of the patient can be avoided, reduce patients�
suffering, save working days and unnecessary expenditure on unrelated and misdirected
treatment which may be many times more than the cost of PCR.

Conclusion and recommendations Analyzing the findings of the present study, it can be concluded that typhoid fever remain to
be as an endemic disease in this locality. All the signs and symptoms of the disease are
nonspecific common with other acute febrile illnesses; a definitive diagnosis of the disease is
required for treatment and to prevent transmission. The ICT and PCR can be the suitable
method for rapid diagnosis of typhoid fever. Detection of antibody (IgM) from whole blood
by ICT method is more easy, non-invasive and highly sensitive and specific method. Thus,
Detection rate of antibody by ICT method is quite satisfactory, so this test can be applicable
for field level use. So, efforts should be made to establish antibody (IgM) detection from
whole blood by ICT method at field level, especially in the endemic areas of Bangladesh.
It is, therefore, concluded that the PCR method was much superior to other method yielding
very high sensitivity and specificity. Although the PCR method requires extensive
infrastructure and specialized skilled personnel, and cannot be made available everywhere,
especially in developing countries, it can be made available to the reference centres for
utilizations by other healthcare facilities following referral system. So it is strongly
recommended to take necessary steps for setup and start PCR at least in the tertiary care
hospitals.


Comparison of different test methods including polymerase
chain reaction for early and reliable diagnosis of typhoid
fever

List of references
Abdoel, TH, Pastoor, R, Smits, HL, Hatta, M 2007, Laboratory evaluation of a simple and
rapid latex agglutination assay for the serodiagnosis of typhoid fever, Transaction of Royal
Society of Tropical Medicine and Hygiene, vol. 101, pp. 1032-1038.
Acharya, VI, Lowe, CU, Thapa, R, Gurubacharya, VL, Shrestha, MB, Cadoz, M et al. 1987,
Prevention of typhoid fever in Nepal with the Vi capsular polysaccharide of Salmonella typhi,
A preliminary report, New England Journal of Medicine, vol. 317, pp. 1101-1104.
Ali, A, Haque, A. Sarwar, Y, Mohsin, M, Bashir, S, Tariq, A et al. 2009, Multiplex PCR for
differential diagnosis of emerging typhoidal pathogens directly from blood samples,
Epidemiology and Infection, vol. 137, pp. 102�107.
Ambati, SR, Nath, G, Das, BK 2007, Diagnosis of typhoid fever by polymerase chain
reaction, Indian Journal of Pediatric, vol. 74, pp. 909-913.
Ammah, A, Akenji, NT, Ndip, R, and Deas, JE 1999, An update on concurrent malaria and
typhoid fever in Cameroon, Transaction of Royal Society of Tropical Medicine and Hygiene,
vol. 2, pp. 127�129.
Ananthanarayan, R and Panikar, CKJ 1999, in Textbook of Microbiology, Chennai, Orient
Longman, pp. 244-249.
Anggraini, R, Handoyo, I and Aryati 2004, DOT- EIA typhoid test using Omp salmonella
typhi local phage type antigen to support the diagnosis of typhoid fever, Folia Medica
Indonesiana, vol. 40, no. 1, pp. 10-20.
Antony, TJ, Patwari, AK, Anand, VK, Pillai, PK, Aneja, S, Sharma, D et al. 1993, Duodenal
string test in typhoid fever, Indian Pediatrics, vol. 30, no. 5, pp. 643-647.
Anusha, R, Ganesh, R and Lalitha, J 2011, Comparison of a rapid commercial test,
Enterocheck WB, with automated blood culture for diagnosis of typhoid fever, Annals of
Tropical Paediatrics: International Child Health, vol. 31, no. 3, pp. 231-234.
Aron, L, Faundez, G, Gonzalez, C, Roessler, E and Cabello, F 1993, Lipopolysaccharide
independent radioimmuno precipitation and identification of structural and in vivo induced
immunogenic surface proteins of Salmonella typhi in typhoid fever, Vaccine, vol. 11, pp. 10-
17.
Asna, SMZA and Haq, JA 2000, Decrease of antibiotic resistance in Salmonella typhi
isolated from patients attending hospitals of Dhaka City over a 3 year period, International
Journal of Antimicrobial Agents, vol. 16, no. 3, pp. 249-251.
Asten, AJV and Dijk, JEV 2005, Distribution of "classic" virulence factors among
Salmonella spp, FEMS Immunology and Medical Microbiology, vol. 44, pp. 251-259.
Atamanalp, SS, Aydinli, B, Ozturk, Oren, D, Basoglu, M, Yildirgan, MI et al. 2007, Typhoid
intestinal perforations: twenty-six year experience, World Journal of Surgury, vol. 31, pp.
1883-1888.
Balasubramanian, K, Kaarthigey, AN, Srinivas, S, and Rajeswari, R 2010, Serum ALT:
LDH Ratio in Typhoid Fever and Acute Viral Hepatitis, Indian paediatrics, vol. 47, pp. 339-
341.
Begum, Z, Hossain, MA, Shamsuzzaman, AK, Ahsan, MM, Musa, AKMahmud, MC 2009,
et al. Evaluation of Typhidot (IgM) for Early Diagnosis of Typhoid Fever, Bangladesh
Journal of Medical Microbiology, vol. 03, no. 1, pp. 10-13.
Begum, Z, Hossain, MA, Musa, AK, Shamsuzzaman, AK, Mahmud, MC, Ahsan, MM et al.
2009, Comparison between DOT EIA IgM and Widal test as early diagnosis of typhoid fever,
Mymensingh Medical Journal, vol. 18, no. 1, pp. 13-17.
Behlau, I and Miller, SI 1993, A PhoP-repressed gene promotes Salmonella typhimurium
invasion of epithelial cells, Journal of bacteriology, vol. 175, no. 14, pp. 4475-4484.
Benavente, L, Gotuzzo, E, Guerra, J, Grados, O, Guerra, H, Bravo, N et al. 1984, Diagnosis
of typhoid fever using a string capsule device, Transaction of the Royal Society of Tropical
Medicine and Hygiene, vol. 78, no. 3, pp. 404-406.
Betly, A, Daniel, FF, Alice, SS, Weissfeld editors, 2010, Blood stream infection, in Baily and
Scott�s Diagnostics Microbiology, Mostby, Missouri, USA, 12th edition, pp. 865-880.
Bhatia, JK, Mathur, AD and Arora, MM 2006, Reemergence of Chloramphenicol Sensitivity
in Enteric Fever, Medical Journal Armed Forces of India, vol. 63, pp. 212-214.
Bhutta, ZA 1996, Impact of age and drug resistance on mortality in typhoid fever, Archives
of Disease in Childhood, vol. 75, pp. 214-217.
Bhutta, ZA 2008, Salmonella in Nelson Textbook of peadiatric, vol.1, 18th edition, Kliegman,
Behrman, Jenson, Stanton editors, India, Saunders, Elsevier, pp.1182-1191.
Bhutta, ZA and Mansurali, N 1999, Rapid serologic diagnosis of paediatric typhoid fever in
an endemic area: a prospective comparative evaluation of two dot-enzyme immunoassays and
the Widal test, American Journal of Tropical Medicine and Hygiene, vol. 61, pp. 654-657.
Bhutta, ZA, Farooqui, BJ and Sturm, AW 1992, Eradication of a multiple drug resistant
Salmonella paratyphi A causing meningitis with ciprofloxacin, Journal of Infection, vol. 25,
pp. 215-219.
Bhutta, ZA, Naqvi, SH and Suria, A 1991, Chloramphenicol therapy of typhoid fever and its
relationship to hepatic dysfunction, Journal of Tropical Pediatrics, vol. 37, pp. 320-322.
Black, RE, Levine, MM, Ferreccio, C, Clements, ML, Lanata, C, Rooney, J et al. 1990,
Efficacy of one or two doses of Ty21a Salmonella typhi vaccine in enteric-coated capsules in
a controlled field trial, Vaccine, vol. 8, pp. 81-84.
Brooks, AW, Hossain, A, Goswami, D, Sharmin, AT, Nahar, K, Alam, K et al. 2005,
Bacteraemic Typhoid fever in children in an urban slum, Bangladesh, Emerging Infectious
Disease, vol. 11, no. 2, pp. 326-329.

Brown, JC, Shanahan, PM, Jesudason, MV, Thomson, CJ, Amyes, SG 1996, Mutations
responsible for reduced susceptibility to 4-quinolones in clinical isolates of multi-resistant
Salmonella typhi in India, Journal of Antimicrobial and Chemotherapy, vol. 37, pp. 891-900.
Butler, T, Islam, A, Kabir, I, Jones, PK 1991, Patterns of morbidity and mortality in typhoid
fever dependent on age and gender: review of 552 hospitalized patients with diarrhea, Review
of infectious Disease, vol. 13, no. 1, pp. 85-90.
Butler, T, Sridhar, CB and Daga, MK 1999, Treatment of typhoid fever with azithromycin
versus chloramphenicol in a randomized multicentertrial in India, Journal of Antimicrobial
and Chemotherapy, vol.18, pp. 245-248.
Callazo, CM and Galan, JE 1997, the invasion associated type III protein secretion system in
salmonella �a review, Gene, vol. 192, pp. 15-23.
CDC 1997, Case Definitions for Infectious Conditions under Public Health Surveillance,
MMWR, 46(RR-10), http://www.cdc.gov/mmwr/preview/mmwrhtml/ 00047449.htm, pp. 1-55.
Chaicumpa, W, Ruangkunaporn, Y, Burr, D, Nguan CM, Echeverria, P 1992, Diagnosis of
typhoid fever by detection of Salmonella typhi antigen in urine, Journal of Clinical
Microbiology, vol. 30, pp. 2513-2515.
Chakraborty, P 2003, Salmonella, in a text book of microbiology, 2nd edition, new central
book agency, Calcutta, pp. 327-337.

Chandel, DS, Chaudhry, R, Dhawan, B, Paudey, A and Dey, AB 2000, Drug-resistant
Salmonella enterica serotype Paratyphi A in India, Emerge Infectious Diseases, vol. 6, pp.
420�421.
Chander, H, Majumdar, S, Sapru, S and Rishi, P 2006, 55 kDa outer-membrane protein from
short-chain fatty acids exposed Salmonella enterica serovar Typhi induces apoptosis in
macrophages, Antonie van Leeuwenhoek, vol. 89, no. 3-4, pp. 317-323.
Chaudhry, R, Laxmi, BV, Nisar, N, Ray, K, Kumar, D 1997, Standardisation of polymerase
chain reaction for the detection of Salmonella typhi in typhoid fever, Journal of Clinical
Pathology, vol. 50, pp. 437-439.
Chessbrough, M 2010, District laboratory practice in tropical countries, Part-2, New York,
USA, Cambridge University, pp. 184- 186.
Chinh, NT, Parry, CM, Diep, TS, Wain, J, White, NJ, Farrar, JJ et al. 2000, A randomised
controlled comparison of azithromycin and ofloxacin for multidrug-resistant and nalidixic
acid resistant enteric fever, Antimicrobial Agents and Chemotherapy, vol. 44, pp. 1855-1859.
Choo, KE, Davies, TME, Ismail, A, Ong, KH 1997, Longevity of antibody responses to a
Salmonella typhi specific outer membrane protein: Interpretation of a dot enzyme
immunosorbent assay in an area of high typhoid fever endemicity, American Journal of
Tropical Medicine and Hygiene, vol. 57, no. 6, pp. 656-659.
Choo, KE, Davis, TM, Ismail, A, Ibrahim, TTA, Ghazali, WN 1999, Rapid and reliable
serological diagnosis of enteric fever: comparative sensitivity and specificity of Typhidot and
Typhidot-M tests in febrile Malaysian children, Acta Tropica, vol. 72, pp. 175-183.
CLSI 2010, Performance Standards for Antimicrobial Susceptibility Testing, Twentieth
Informational Supplement, CLSI Document M100-S20, Wayne, PA: Clinical and Laboratory
Standards Institute, vol. 30, no. 15, pp. 1-7.
Cocolin, L, Manzano, M, Astori, G, Botta, GA, Cantoni, C, Comi, G et al. 1998, A highly
sensitive and fast non-radioactive method for the detection of polymerase chain reaction
products from salmonella serovars, such as Salmonella typhi, in blood specimens, FEMS
Immunology and Medical Microbiology, vol. 22, pp. 233-239.
Collee, JG and Marr, W 2006, Culture of bacteria, in Mackie and Cartney, Practical Medical
Microbiology, Collee JG, Fraser, AG, Marmion, BP and Simmons, A editors, 14th edition,
Curchill Livingstone, India, pp. 121-124.
Collier�s Encyclopedia 1989, vol. 22, Macmillian Educational copany, Collier. Inc Londone
and NewYork.
Connerton, P, Wain, J, Hien, TT, Ali, T, Parry, CM, Chinh, NT et al. 2000, Epidemic typhoid
in Vietnam: molecular typing of multiple antibiotic-resistant Salmonella enterica serotype
typhi from four outbreaks, Journal of Clinical Microbiology, vol. 38, pp. 895-897.
Crum, NF 2003, Current trends in typhoid fever, Current Gastroenterology Report, vol. 5,
no.4, pp. 279-286.

Crump, JA, Luby, SP and Mintz, ED 2004, the global burden of typhoid fever, Bulletin of
World Health Organization, vol. 82, pp. 346-353.
Dham, SK and Thompson, RA 1982, Studies of cellular and humoral immunity in typhoid
fever and TAB vaccinated subjects, Clinical and Experimental Immunology, vol. 48, pp. 389-
395.
Dhanjee, A, Sheikh, MA, Yaqub, M, Alam, SE 1999, Orelox (cefodoxime) in typhoid fever,
Journal of the Pakistan Medical Association, vol. 49, pp. 8-9.
Duthie, R and French, G 1990, Comparison of methods for the diagnosis of typhoid fever,
Journal of Clinical Pathology, vol. 43, pp. 863-865.
Eggleston, FC, Santoshi, B and Singh, CM 1979, Typhoid perforation of the bowel,
Experiences in 78 cases, Annals of Surgery, vol. 190, pp. 31-35.
Encyclopedia Britannica 2011, Fernand-Isidore Widal, Online, Web. 25 Apr. 2011.
<http://www.britannica.com/EBchecked/topic/643157/Fernand-Isidore-Widal>. (accessed 28
April 2008).
Escamilla, J, Santiago, LT, Uylangco, CV and Cross, JH 1985, Evaluation of Sodium
Polyanethol Sulfonate as a Blood Culture Additive of Salmonella typhi and Salmonella
paratyphi A, Journal of clinical Microbiology, vol. 18, pp. 380-383.

Fadeel, MA, Crump, JA, Mahoney, FJ, Nakhla, IA, Mansour, AM, Reyad, B et al. 2004,
Rapid diagnosis of typhoid fever by enzyme-linked immunosorbent assay detection of
Salmonella serotype typhi antigens in urine, American Journal of Tropical Medicine and
Hygiene, vol. 70, pp. 323-328.
Farooqui, BJ, Khurshid, M, Ashfaq, MK and Khan, MA 1991, Comparative yield of
Salmonella typhi from blood and bone marrow cultures in patients with fever of unknown
origin, Journal of Clinical Pathology, vol. 44, pp. 258�259.
Frankel, G, Newton, SMC, Schoolnik, GK and Stocker, BAD 1989, Unique sequences in
region VI of the flagellin gene of Salmonella typhi, Molecular Microbiology, vol. 3, pp.
1379-1383.
Frenck, RW, Nakhla, I, Sultan, Y 2000, Azithromycin versus ceftriaxone for the treatment of
uncomplicated typhoid fever in children, The Journal of Infectious Diseases, vol. 31, pp.
1134-1138.
Galan, JE 2001, salmonella interactions with host cells: Type iii secretion at work, Annual
Review of Cell and Developmental Biology, vol. 17, pp. 53� 86.
Garmory, HS, Brown, KA, and Titball, RW 2002, Salmonella vaccines for use in humans:
present and future perspectives, FEMS microbiology reviews, vol. 26, no. 4, pp. 339�353.

Gasem, MH, Dolmans, WM, Isbandrio, BB, Wahyono, Keuter, HM, Djokomoeljanto, R et al.
1995, Culture of Salmonella typhi and Salmonella paratyphi from blood and bone marrow in
suspected typhoid fever, Tropical Geographical Medicine, vol. 47, 164-167.
Gasem, MH, Smits, HL, Goris, MG and Dolmans, WM 2002, Evaluation of a simple and
rapid dipstick assay for the diagnosis of typhoid fever in Indonesia, Journal of Medical
Microbiology, vol. 51, pp. 173-177.
Gautam, V, Gupta, NK, Choudhary, U, Arora, DR 2002, Sensitivity pattern of Salmonella
serotypes in Northern India, The Brazilian Journal of Infectious Diseases, vol. 6, pp. 281-
287.
Gilman, R, Terminel, M, Levine, M, Mendoza, PH and Hornick, RB 1975, The relative
efficacy of blood, urine, rectal swab, and rose spot cultures for recovery of S. typhi in typhoid
fever, Lancet, vol. 1, pp. 1211-1213.
Gilman, RH and Richard, BH 1976, Duodenal Isolation of Salmonella typhi by String
Capsule in Acute Typhoid Fever, Journal of Clinical Microbiology, vol. 3, no. 4, pp. 456-
457.
Girgis, NI, Sutan, Y, Hammad, O, Farid, Z 1995a, Comparison of the efficacy, safety and
cost of cefixime, ceftriaxone and aztreonam in the treatment of multidrug resistant
Salmonella typhi septicemia in children, The Pediatric Infectious Disease Journal, vol.14, pp.
603-605.

Girgis, NI, Tribble, DR, Sultan, Y, Farid, Z 1995b, Short course chemotherapy with cefixime
in children with multidrug resistant Salmonella typhi septicemia, Journal of Tropical
Pediatrics, vol. 4, pp. 364-365.
Goldstein, FW, Chumpitaz, JC, Guevara, JM, Papadopoulo, B, Acar, JF, Vieu, JF et al. 1986,
Plasmid-mediated resistance to multiple antibiotics in Salmonella typhi, Journal of Infectious
Disease, vol. 153, pp. 261-266.
Gotuzzo, E, Frisancho, O, Sanchez, J, Liendo, G, Carrillo, C, Robert E et al. 1991,
Association between the acquire immunodeficiency syndrome and infection with Salmonella
typhi or Salmonella paratyphi in an endemic typhoid area, Archive of International Medicine,
vol. 151, pp. 381-382.
Greenwood, BM, Bradley-Moore, AM, Bryceson, AD, Palit, A 1972, Immunosuppression in
children with malaria, Lancet, vol. 1, pp. 169-172.
Hakanen, A, Kotilainen, P, Huovinen, P, Helenius, H and Siitonen, A 2001, Reduced
fluoroquinolone susceptibility in Salmonella enterica serotypes in travelers returning from
Southeast Asia, Emerge Infectious Disease, vol. 7, pp. 996�1003.
Haque, A, Ahmad, J, Qureshi, JA 1999, Early detection of typhoid by polymerase chain
reaction, Annals of Saudi Medicine, vol. 19, pp. 337�340.
Haque, A, Ahmed, N, Peerzada, A, Raza, A, Bashir, S, Abbas, G et al. 2001, Utility of PCR
in diagnosis of problematic cases of typhoid, Japanese Journal of Infectious Disease, vol. 54,
pp. 237-239.
Hasbun, JH, Osorio, R and Hasbun, A 2006, Hepatic Dysfunction in Typhoid Fever During
Pregnancy, Infectious Diseases in Obstetrics and Gynecology, vol. 2006, pp. 1�2.
Hashimoto, Y, Itho, Y, Fujinaga, Y, Khan, AQ, Sultana, F, Miyake, M et al. 1995,
Development of nested PCR based on the ViaB sequence to detect Salmonella typhi, Journal
of Clinical Microbiology, vol. 33, pp. 775-777.
Hatta M and Smits HL 2007, Detection of Salmonella typhi by nested polymerase chain
reaction in blood, urine, and stool samples, American Journal of Tropical Medicine and
Hygiene, vol. 76, pp. 139-143.
Hatta, M, Goris, MG, Heerkens, E, Gooskens, J and Smits, HL 2002, Simple dipstick assay
for the detection of Salmonella typhi-specific IgM antibodies and the evolution of the
immune response in patients with typhoid fever, American Journal of Tropical Medicine and
Hygiene, vol. 66, pp. 416-421.
Hirose, K, Itoh, K, Nakajima, H, Kurazono, T, Yamaguchi, M, Moriya, K et al. 2002,
Selective amplification of prt (rfbS), viaB tyv (rfbE),, and fliC genes by multiplex PCR for
identification of Salmonella enterica serovars typhi and Paratyphi A, Journal of Clinical
Microbiology, vol. 40, pp. 633-636.

Hoa, NTT, Diep, TS, Wain, J, Hien, TT, Smith, MD, Amanda, L et al. 1998, Community-
acquired septicaemia in southern Viet Nam: the importance of multidrug-resistant Salmonella
typhi, Transaction of the Royal Society of Tropical Medicine and Hygiene, vol. 92, pp. 503-
508.
Hoare, A, Bittner, M, Carter, J, Alvarez, S, Zaldívar, M, Bravo, D et al. 2006, The Outer
Core Lipopolysaccharide of Salmonella enterica serovar typhi Is Required for Bacterial
Entry into epithelial Cells, Infection and Immunity, vol. 74, pp. 1555-1564.
Hoffman, SL, Punjabi, NH, Kumala, S, Moechtar, MA, Pulungsih, SP, Rivai, AR et al. 1984,
Reduction of mortality in chloramphenicol-treated severe typhoid fever by high-dose
dexamethasone, The New England Journal of Medicine, vol. 310, pp. 82-88.
Hoffman, SL, Punjabi, NH, Rockhill, RC, Sutomo, A, Rivai, AR, Pulungsih, SP et al. 1984,
Duodenal string-capsule culture compared with bone-marrow, blood and rectal-swab cultures
for diagnosing typhoid and paratyphoid fever, Journal of Infectious Disease, vol. 149,
pp.157�161.
Hoque, SS, Alam, AN, Islam, MR, Khan, MR 1992, Recent advances in the treatment of
typhoid: with special emphasis on multidrug resistant Salmonella typhi in Bangladesh,
Bangladesh Journal of Child Health, vol. 16, pp. 15-19.
Hosoglu, S, Aldemir, M, Akalin, S, Geyik, MF, Tacyildiz, IH, Loeb, M et al. 2004, Risk
factors for enteric perforation in patients with typhoid Fever, American Journal of
Epidemiology, vol. 160, pp. 46-50.

Hosoglu, S, Bosnak, V, Akalin, S, Geyik, MF, Ayaz, C 2008, Evaluation of false negativity
of the Widal test among culture proven typhoid fever cases, The Journal of Infection in
Developing Countries, vol 2, no. 06, pp. 475-478.
Hosssain, MS 2001, Comparative study of Widal test and DOT enzyme immunoassay for
early sero diagnosis typhoid fever, (Thesis), Bangabandhu Sheikh Mujib Medical University
Dhaka, Bangladesh.
House, D, Bishop, A, Parry, C, Dougan, G and Wain, J 2001, Typhoid fever: pathogenesis
and disease, Current Opinion of Infectious Disease, vol. 14, no. 5, pp. 573-578.
House, D, Chinh, NT, Diep, TS, Parry, CM, Wain, J, Dougan, G et al. 2005, Use of paired
serum samples for serodiagnosis of typhoid fever. Journal of Clinical Microbiology, vol. 43,
pp. 4889-4890.
Islam, MN, Rahman, ME, Rouf, MA, Islam, MN, Khaleque, MA, Siddika, M et al. 2007,
Efficacy of azithromycin in the treatment of childhood typhoid fever, Mymensingh Medical
Journal, vol. 16, no. 2, pp. 149-153.
Ismail, A, Kader, ZSA and Ong, KH 1991, Dot enzyme immunosorbant assay for the
serodiagnosis of typhoid fever, The Southeast Asian Journal of Tropical Medicine and Public
Health, vol. 22, pp. 563-566.
Jegathesan, M 1983, Phages types of Salmonella typhi isolated in Malaysia over the 10 year
period 1970-1979, The Journal of Hygiene, vol. 90, no. 1, pp. 91-97.
Jenkins, C and Gillespie, SH 2009, Salmonella Infections in Gordon, C, Cook and Zumla, AI
editors, in Manson�s Tropical Diseases, 22nd edition, China, Saunders, Elsevier, pp. 931-952.
Jerrold, R and Turner 2010, The gastrointestinal tract: Salmonellosis, in Kumar, V, Abbas,
AK, Fausto, and Aster, JC, editors, Robins and Cotran Pathologic Basis of Disease, 8th
edition India, Elsevier, p. 801.
Jesudason, M, Esther, E, Mathai E 2002, Typhidot test to detect IgG & IgM antibodies in
typhoid fever, Indian Journal of Medical Research , vol. 116, pp. 70-72.
Jimenez, SMM and Castro, CN 2004, Validation of a PCR for diagnosis of typhoid fever and
salmonellosis by amplification of the hilA gene in clinical samples from Colombian patients,
Journal of Medical microbiology, vol. 53, pp. 875-878.
Jones, BD, Ghori, N and Falkaw, S 1994, Salmonella typhimurium initiates murine infection
by penetrating and destroying the specialized epithelial M cells of the Peyer's patches,
Journal of experimental medicine, vol. 180, pp. 15-23.
Joshi, YK 2001, Symposium: typhoid fever, Journal, Indian Academy of Clinical Medicine,
vol. 2, no. 1 and 20, pp 12-15.
Kalhan, R, Kaur, I, Singh, RP and Gupta, HC 1999, Latex Agglutination Test (LAT) for the
diagnosis of typhoid fever, Indian Pediatrics, vol. 36, pp. 65-68.
Kanjilal, SD, Dutta, A, Mondal, RK, Chakravorti, S 2006, Uncomplicated falciparum malaria
complicated by Salmonella septicaemia: cause not coincidence, Journal of Indian Medical
Association, vol. 104, no.11, pp. 646, 648.
Kariuki, S, Gilks, C, Revathi, G, Hart, C 2000, Genotypic analysis of Multidrug-resistant
Salmonella enterica serovar typhi, Kenya, Emerge Infectious Disease, vol. 6, pp. 649-651.
Kauffmann, F 1941, Die Bakteriologie der Salmonella-Gruppe, Einar Munksgaard,
Copenhagen.Kauffmann, F. 1941.
Keddy, KH, Klugman, KP, Hansford, CF, Blondeau, C, Bouveret, Lecam, NN 1999,
Persistence of antibodies to the Salmonella typhi Vi capsular polysaccharide vaccine in South
African school children ten years after immunization, Vaccine, vol. 17, pp. 110-113.
Khan, MA, Mekan, SF, Abbas, Z, Smego, RA 2005, Concurrent malaria and enteric fever in
Pakistan, Singapore Medical Journal, vol. 46, pp. 635-638.
Khan, MR and Hoque, SS 1992, Emergence of multi-drug resistant Salmonella typhi A need
for therapeutic reappraisal, Bangladesh Journal of Child Health, vol. 16, pp. 1-3.
Khan, MR, 2005, Immunization and infectious disease, in Essence of paediatrics, 3rd edition,
Asian colour printing, Dhaka, p. 654.
Khosla, SN 1990, Typhoid hepatitis, Postgraduate Medical Journal, vol. 66, no, 781, pp.
923-925.
Kidgell, C, Reichard, U, Wain, J, Linz, B, Torpdahl, M, Dougan, G et al. 2002, Salmonella
typhi, the causative agent of typhoid fever, is approximately 50,000 years old, Infection,
Genetics and evolution, vol. 2, pp. 39-45.
Klugman, K, Hendrick, J, Koornhof, J, Robbins, JB, Le Cam N 1996, Immunogenicity,
efficacy and serological correlate of protection of Salmonella typhi Vi capsular
polysaccharide vaccine three years after immunization, Vaccine, vol. 1, no. 5, pp. 435-438.
Kossack, RE, Guerrant, RL, Densen, P, Schadelin, J, Mandell, GL 1981, Diminished
neutrophil oxidative metabolism after phagocytocis of virulent Salmonella typhi, Infection
and Immunity, vol. 31, pp. 674-678.
Kossaczka, Z, Lin, F, Ho, V, Thuy, N, Bay P, Thanh, T, Khiem, H et al. 1999, Safety and
immunogenicity of Vi conjugate vaccines for typhoid fever in adults, teenagers, and 2- to 4-
year-old children in Viet Nam, Infection and immunity, vol. 67, pp. 5806-5810.
Kumar, A, Arora, V, Bashamboo, A and Ali, S 2002, Detections of Salmonella typhi by
polymerase chain reaction: implification in diagnosis of typhoid fever, Infection Genetics
Evolution, vol. 2, pp. 107-110.
Kumar, A, Balachandran, Y, Gupta, S, Khare, S, Suman et al. 2010, Quick PCR based
diagnosis of typhoid fever using specific genetic markers, Biotechnology Letter, 32, pp. 707-
712.
Kumar, R, Malaviya, AN, Murthy, RGS, Venkataraman, M and Mohapatra, LN 1974,
Immunological study of typhoid: immunoglobulins, C3, antibodies and leucocyte migration
inhibition in patients with typhoid fever and TAB-vaccinated individuals, Infection and
Immunity, vol. 10, p. 1219.
Kundu, R, Ganguly, N, Ghosh, TK, Yewale, VN, Shah, RC, Shah. NK 2006, IAP Task Force
Report: Diagnosis of Enteric Fever in Children, Indian Pediatrics, vol. 43, no. 10, pp. 875-83.
Le, TP and Hoffman, SL 1999, Typhoid fever, in Tropical Infectious Diseases, Principles,
Pathogena and practice, Guerrent, RL, Walker, DH, weller, PF editors, Churchill
Livingstone, Philadelphia, vol. 1, pp. 277-290.
Leminor, L and Popoff, MY 1987, Request for an Opinion, Designation of Salmonella
enterica sp. nov., nom. rev., as the type and only species of the genus Salmonella,
International Journal of Systemic Bacteriology, vol. 37, pp. 465-468.
Lesser, CF and Miller, SI 2005, Salmonellosis, in Harrison�s principle of internal Medicine,
16th edition, Kasper, DL, Fauel, AS, Longo, DL, Braunwald, E, Hauser, SL, Jameson, J
editors, McGraw- Hill Medical publishing Division, New York, vol. 1, pp. 897-902.
Levine, MM, Ferreccio, C, Black, RE, Lagos, R, Martin SO, and William, C, Blackwelder,
CW 2007, Ty21a Live Oral Typhoid Vaccine and Prevention of Paratyphoid Fever Caused by
Salmonella enterica Serovar Paratyphi B, Clinical Infectious Diseases, vol. 45, pp. 24-28.

Levinson, W 2010, Review of medical microbiology and immunology, 11th edition, New
York, Lange, pp. 85-93.
Lewis, MJ 1997, Salmonella, in Medical Microbiology, Greenwood, D, Slack, R and
Pebtherer, J, editors, 15th edition, ELST, USA, pp. 252-261.
Lifshitz, EI 1996, Travel trouble: typhoid fever- A case presentation and review, Journal of
American Collaborative Health, vol. 45, no. 3 pp. 99-105.
Lin, FY, Ho, VA, Bay, PV et al. 2000, The Epidemiology of typhoid fever in the Dong Thap
province, Mekong Delta region of Vietnam, American Journal of Tropical Medicine and
Hygiene, vol. 62, no. 5, pp. 644�648.
Lin, FY, Ho, VA, Khiem, HB, Trach, DD, Bay, PV, Thanh, TC et al. 2001,The efficacy of a
Salmonella typhi Vi conjugate vaccine in two to five years old children, New England
Journal of Medicine, vol. 344, pp. 1263-1269.
Luxemburger, C, Chau, MC, Mai, NL, Wain, J, Tran, TH, Simpson, JA et al. 2001, Risk
factors for typhoid fever in the Mekong delta, southern Viet Nam: a case-control study,
Transactions of the royal Society of Tropical Medicine and Hygiene, vol. 95, no. 1, pp. 19-23.
Madanagopalan, N, Subramaniam, S, Panchanadaer, M, Rao, P and Suniti, S 1975, Detection
of enteric carriers by upper small intestinal aspirate studies, Journal of Tropical Medicine and
Hygiene, vol. 78, pp. 123-125.

Malik, AS 2002, Complications of bacteriologically confirmed typhoid fever in children. J
Trop Pediatr, vol. 48, pp. 102-108.
Malik, AS and Malik, RH 2001,Typhoid fever in Malaysian children, Medical Journal of
Malaysia, vol. 56, pp.478- 90.
Mantur, BG, Bidari, LH, Akki, AS, Mulimani, MS, Tikare, NV 2007, Diagnostic yield of
blood clot culture in the accurate diagnosis of enteric fever and human brucellosis, Clinical
laboratory, vol. 53, no. 1-2, pp. 57-61.
Massi, MN, Shirakawa, T, Gotoh, A, Bishnu, A, Hatta, M, Kawabata, M et al. 2003, Rapid
diagnosis of typhoid fever by PCR assays using one pair of primers from flagellin gene of S.
typhi, Journal of Infection and Chemotherapy, vol. 9, pp. 233-237.
Massi, MN, Shirakawa, T, Gotoh, A, Bishnu, A, Hatta, M, Kawabata, M 2005, Quantitative
detection of Salmonella enterica serovar typhi from blood of suspected typhoid fever patients
by real-time PCR, International Journal of Medical Microbiology, vol. 295, pp. 117-120.
Mastroianni, DCM, Jirillo, E, Simone, CD, Grassi, PP, Maffione, AB, Catino, AM et al.
1989, Humoral and cellular immune responses to salmonella typhi in patients with typhoid
fever, Journal of Clinical Laboratory Analysis, vol. 3, pp. 191 � 195.

Mehta, G, Randhawa, VS, Mohapatra, NP 2001, Intermediate susceptibility to ciprofloxacin
in Salmonella typhi strains in India, European Journal Clinical Microbiology and Infectious
Disease, vol. 20, pp. 760-761.
Miller, H, Zhang, J, KuoLee, R, Patel, GB, Chen, W 2007, Intestinal M cells: The fallible
sentinels?, World J Gastroenterol, vol. 13, no. 10, pp. 1477-1486
Miller, IS and Pegues, DA 2000, Salmonella species, including Salmonella typhi, in Mandell,
Douglar and Bennetts principles and practice of infectious disease, Mandell, GL, Bennett,
JE, Dolin, R, editors, 5th edition, Philadelphia, Churchill Livingstone, pp. 2344-2263.
Mirza, S, Kariuki, S, Mamun, KZ, Beeching, NJ, Hart, CA 2000, Analysis of plasmid and
chromosomal DNA of multidrug-resistant Salmonella enterica serovar typhi from Asia,
Journal of Clinical Microbiology, vol. 38, pp. 895-897.
Mirza, SH, Beeching, NJ, and Hart, CA 1996, Multi-drug resistant typhoid: a global problem,
Journal of Medical Microbiology, vol. 44, pp. 317-319.
Mohanty, SK and Ramana, KV 2007, Single and Unpaired Sera Tube Widal Agglutination
Test in Enteric Fever, The Saudi Journal of Gastroenterology, vol. 13, p. 213.
Moreno, S, Yesim, S, Andrea, I, Lorin, D, Warnick, Wiedmann, M et al. 2009,
Emergence,Distribution, and Molecular and Phenotypic Characteristics of Salmonella
enterica Serotype 4,5,12:I, Foodborne pathogens and disease, vol. 6, no.4, pp. 407-415.
Morshed, MG, Khan, WA, Khan, HZ, Akbar, MS 1986, Multiple drug resistant S. typhi in
Bangladesh (letter), Journal of Diarrhoeal Diseases Research, vol. 4, p. 24.
Nagarajan, AG, Karnam, G, Lahiri, A, Allam, US, Chakravortty, D et al 2009, Reliable
means of diagnosis and serovar determination of blood borne salmonella strains. Quick PCR
Amplification of Unique Genomic Loci by Novel primer sets, Journal of Clinical
Microbiology, vol. 47, no. 8, pp. 2435-2441.
Nakhla, I, Mohammady, ElH, Mansour, A, Klena, JD, Hassan, K, Sultan, Y, Pastoor, R,
Abdoel, TH, Smits, H 2011,Validation of the Dri-Dot Latex agglutination and IgM lateral
flow assays for the diagnosis of typhoid fever in an Egyptian population, Diagnostic
Microbiology and Infectious Diseases, vol.70, no. 4, pp. 435-41.
Ochiai, RL, Acosta, CJ, Danovaro-Holliday, MC, Baiqing, D, Bhattacharya, SK, Agtini, MD
et al. 2008, A study of typhoid fever in five Asian countries: disease burden and implication
for controls, Bulletin of world health organization, vol. 86, pp. 260-268.
Ohanu, ME, Mbah, AU, Okonkwo, PO, Nwagbo, FS 2003, Interference by malaria in the
diagnosis of typhoid using Widal test alone, West African Journal of Medicine, vol. 22, pp.
250-252.
Ohi, ME, and Miller, SI 2001, Salmonella: A Model for Bacterial Pathogenesis, Annual
Review Medical, vol. 52, pp 259�274.
Old, DC 1990, Salmonella, in Topley and Wilsons, Principles of Bacteriology, Virology and
Immunity, 8th edition, Parker, MT, Collier, LH, Edward, A edition, A division of Hodders and
Stoughton, London Melbourne Auckland, vol. 2, pp. 469-493.
Old, DC 2006, Salmonella infection, in Mackie and McCartney, Practical Medical
Microbiology, 14th edition, Collee, JG , Fraser, AG, Marmion, BP, Simons, A editors,
Churchil Livingston, New York, pp. 385-402.
Olopoenia, LA and King, AL 2000, Widal agglutination test�100 years later: Still plagued by
controversy, Postgraduate Journal of medicine, vol. 76, pp. 80-84.
Park, K 1999, Textbook of preventive and social medicine, 17th edition, Jabalpur: Banarsidas
Bhonet publishers, p. 178-181.
Parker, MT 1990, enteric infections: typhoid and paratyphoid fever, in Topley and Wilson�s
Microbiology and Microbial infections, 8th edition. Collies, L, Balows, A, Susman, M.
Arnold, editors, London, vol. 3, pp. 423-446.
Parry, CM and Threlfall, EJ 2008, Antimicrobial resistance in typhoidal and nontyphoidal
salmonellae, Current Opinion of Infectious Disease, vol. 21, no. 5, pp. 531-538.
Parry, CM, Hoa, NTT, Diep,TS, Chinh, JNT Vinh, H 1999, Value of a single tube widal test
in a diagnosis of typhoid fever in Vietnam, Journal of Clinical Microbiology, vol. 37, no. pp.
2882�2886.
Parry, CM, Hien, TT, Dougan, G, White, NJ, Farrar, JJ 2002, Typhoid fever, New England
Journal of medicine, vol. 347, no. 22, pp. 1770�1782.
Pastoor, R, Hatta, M, Abdoel, TH, Smits, HL 2008, A simple, rapid, and affordable point-of-
care test for the serodiagnosis of typhoid fever, Diagnostic Microbiology and Infectious
Disease, vol. 61, no. 2 , pp. 129-134.
Pearson, RD and Guerrant, RL 1995, Enteric fever and other causes of abdominal symptoms
with fever, in Principles Practices of Infectious Diseases, Mandell, GL, Bennet, JE, Dolin, R
editors, Churchill Livingstone, New York, London. pp. 998-1012.
Pegues, DA, Hantman, MJ, Behlau, I, Miller, SI 1995, PhoP/PhoQ transcriptional repression
of Salmonella typhimurium invasion genes: evidence for a role in protein secretion,
Molecular Microbiology, vol. 17, no. 1, pp. 169-181.
Popoff, MY, Bockemüh, J and Brenner, FW 2000, Supplement 1998 (no. 42) to the
Kauffmann-White scheme, Research in Microbiology, vol. 151, pp. 63-65.
Prakash, P, Mishra, OP, Singh, AK, Gulati, AK and Nath, G 2005, Evaluation of nested PCR
in diagnosis of typhoid fever, Journal of Clinical Microbiology, vol. 43, pp. 431-432.
Rahman, M, Ahmad, A, Shoma, S 2002, Decline in epidemic of Multidrug resistant
Salmonella typhi is not associated with increased incidence of antibiotic-susceptible strain in
Bangladesh, Epidemiology and Infection, vol. 129, pp. 29-34.
Rahman, M, Siddique, AK, Shoma, S, Rashid, H, Salam, MA, Ahmed, QS, Nair, GB,
Brieman, RF, 2006, Emergence of multidrug-resistant Salmonella enterica serotype typhi
with decreased ciprofloxacin susceptibility in Bangladesh, Epidemiology and Infection, vol.
134, no. 2, pp. 433�438.
Rahman, M, Siddique, AK, Tam, FC, Sharmin, S, Rashid, H, Iqbal, A et al. 2007, Rapid
detection of early typhoid fever in endemic children by TUBEXR 09-antibody test,
Diagnostic Microbiology and Infectious Disease, vol. 58, pp. 275-281.
Rajagopalan, P, Kumar, R and Malaviya, AN 1982, Immunological studies in typhoid fever,
II. Cell-mediated immune responses and lymphocyte Subpopulations in patients with typhoid
fever, Clinical and experimental Immunology, vol. 47, pp. 269-274.
Rao, PS, Prasad, SV, Arunkumar, G, S,hiva-nanda, PG 1999, Salmonella typhi Vi antigen
coagglutination test for the rapid diagnosis of typhoid fever, Indian Journal of Medical
Science, vol, 53, pp. 7-9.
Rechard and Thompson 2007, Specimen collection, transport and processing chapter �
Bacteriology, in Manual of Clinical Microbiology, Murray, PP, Baron, EJ, Jorgensen, JH,
Landry, ML, Pfaller, MA, editors, 9th edition ,Washington DC, vol. 1, p. 310.
Reeves, PR 1993, Evolution of Salmonella O antigen variation by interspecific gene transfer
on a large scale, Trends in Genetics, vol. 9, pp. 17-22.
Rithidech, KN, Dunn, JJ, Gordon, CR 1997, Combining multiplex and touchdown PCR to
screen murine microsatellite polymorphisms, Bio Techniques, vol. 23, pp. 36�45.
Rodrigues, C 2003, The Widal test more than 100 years old: abused but still used, Indian
Journal Association of Physicians, vol. 51, pp. 7-8.
Rotger, R and Casadesús, J 1999, the virulence plasmids of Salmonella. International
Microbiology, vol. 2, pp. 177�184.
Rubin, FA, Mcwhirter, PD, Burr, D, Punjabi, NH, Lane, E, Kumala, SY et al. 1990, Rapid
Diagnosis of typhoid Fever through Identification of Salmonella typhi within 18 Hours of
Specimen Acquisition by Culture of the Mononuclear Cell-Platelet Fraction of Blood,
Journal of Clinical Microbiology, vol. 28, pp. 825-827.
Saha, MR, Dutta, P, Palit, A, Dutta D, Bhattacharya, MK, Mittra, U et al. 2003, A Note on
Incidence of Typhoid Fever in Diverse Age Groups in Kolkata, India, Japanese Journal of
Infectious Disease, vol. 56, pp. 121-122.
Saha, SK and Saha, SK 1994, Antibiotic resistance of Salomonella typhi in Bangladesh,
Journal of Antimicrobial and Chemotherapy, vol. 33, pp. 190-191.
Saha, SK, Baqui, AH, Hanif, M, Darmstadt, GL, Ruhulamin, M, Nagatake, T et al. 2001,
Typhoid fever in Bangladesh: implications for vaccination policy, Pediatric Infectious
Disease Journal, vol. 20, pp. 521-524.
Saha, SK, Ruhulamin, M, Hanif, M, Islam, M, Khan, WA 1996, Interpretation of the Widal
test in the diagnosis of typhoid fever in Bangladeshi children, Annals of Tropical Paediatrics,
vol, 16, pp. 75�78.
Saha, SK, Talukder, SY, Islam, M, Saha, S 1999, A highly ceftriaxone-resistant in
Bangladesh, The Pediatric Infectious Disease Journal, vol. 18, pp. 297-303.
Sarma, VNB, Malviya, AN, Kumar, R, Ghai, OP and Bakhtary, MM 1977, Development of
immune response during typhoid fever in man, Clinical and experimental Immunology, vol.
28, pp. 35-39.
Saxena, V, Basu, S, Sharma, CL 2007, Perforation of the gall bladder following typhoid
fever-induced ileal perforation, HongKong Medical journal, vol. 13, pp. 475-477.
Schoeder, SA 1968, Interpretation of serologic tests for typhoid fever, Journal of American
Medical Association, vol. 206, pp. 839-840.

Schwalbe, RS, Hoge, CW, Morris, JG, O�Hanlon, PN, Crawford, RA, Gilligan, PH et al.
1990, In vivo selection for transmissible drug resistance in Salmonella typhi during
antimicrobial therapy, Antimicrobial Agents and Chemotherapy, vol. 34, pp. 161-163.
Seoud, M, Saade, G, Uwaydah, M, Azoury, R 1988, Typhoid fever in pregnancy, Obstetrics
and gynecology, vol. 71, pp. 711-714.
Shanahan, PM, Karamat, KA, Thomson, CJ, Amyes, SGB 2000, Characterization of multi-
drug resistant Salmonella typhi from Pakistan, Epidemiology and Infection, vol. 124, pp. 9-
16.
Sharma, KB, Bhat BM, Paricha, A, Vaze, S 1979, Multiple antibiotic resistance among
Salmonellae in India, Journal of Antimicrobial and Chemotherapy, vol. 5, pp.15-21.
Shukla, S, Patel, B, Chitinnis, DS 1997, 100 years of widal test and its reapparisial in an
endemic area, Indian Journal of Medical Research, vol. 105, pp. 53-57.
Siddiqui, FJ, Rabbani, F, Hasan, R, Nizami, SQ, Bhutta, ZA 2006, Typhoid fever in children:
some epidemiological considerations from Karachi, Pakistan, International Journal of
Infectious Diseases, vol. 10, no. 3, pp. 215-222.
Singh, B 2001, Typhoid fever: epidemiology, Journal of Indian Academy of Clinical
Medicine, vol. 2, pp. 17-20.

Sinha, A, Sazwal, S, Kumar, R, Sood, S, Reddaiah, VP, Singh, B et al. 1999, Typhoid fever
in children aged less than 5 years, Lancet, vol. 354, pp. 734-737.
Song, JH, Cho, H, Park, MY, Na, DS, Moon, HB, Pai, CH et al. 1993, Detection of
Salmonella typhi in the blood of patients with typhoid fever by polymerase chain reaction,
Journal of Clinical Microbiology, vol. 31, pp. 1439�1443.
Sood, S, Rishi, P, Vohra, H, Sharma, S, Ganguly, NK 2005, Cellular immune response
induced by Salmonella enterica serotype typhi iron-regulated outer-membrane proteins at
peripheral and mucosal levels, Journal of Medical Microbiology, vol. 54, pp. 815�821.
Sulaiman, K and Sarwari, AR 2007, Culture-confirmed typhoid fever and pregnancy,
International Journal of Infectious Diseases, vol. 11, pp. 337�341.
Sur, D, Ali, M, Seidlein, LV, Manna, B, Jacqueline, L, Deen, BL et al. 2007, Comparisons of
predictors for typhoid and paratyphoid fever in Kolkata, India, BMC Public Health, vol. 7, p.
289.
Sztein, MB 2007, Cell-Mediated Immunity and Antibody Responses Elicited by Attenuated
Salmonella enterica Serovar Typhi Strains Used as Live Oral Vaccines in Humans, Clinical
Infectious Diseases, vol. 45, pp. 15�19.

Tang, SS, Tan, WS, Devi, S, Wang, LF, Pang,T, Thong, KL et al. 2003, Mimotopes of the
Vi Antigen of Salmonella enterica Serovar Typhi Identified from Phage Display Peptide
Library, Clinical and Vaccine Immunology, vol. 10, no. 6, pp. 1078-1084.
Threlfall, EJ and Ward, LR 2001a, Decreased susceptibility to ciprofloxacin in Salmonella
enterica serotype Typhi, United Kingdom, Emerge Infectious Disease, vol. 7, pp. 448�450.
Threlfall, EJ, Skinner, JA, Ward, LR 2001b Detection of decreased in vitro susceptibility to
ciprofloxacin in Salmonella enterica serotypes typhi and paratyphi A, Journal of
Antimicrobial and Chemotherapy, vol. 48, pp. 740-741.
Threlfall, EJ, Ward, LR, Rowe, Raghupathi, BS, Chandrasekaran, V, Vandepitte, J et al.
1992, widespread occurrence of multiple drug-resistant Salmonella typhi in India, European
Journal of Clinical Microbiology and Infectious Disease, vol. 11, pp. 990-993.
Threlfall, EJ, Ward, LR, Skinner, JA, Smith, HR, Lacey, S 1999, Ciprofloxacin resistant
Salmonella typhi and treatment failure, Lancet, vol. 353, pp. 1590-1591.
Topley and Wilson 1990, Salmonella, in Principles of Bacteriology, Virology and
Immunology, 8th edition, London, vol. 2, pp. 482-489.
Tran, HH, Bjune, G, Nguyen, BM, Rottingen, JA, Grais, RF, Guerin, PJ et al. 2005, Risk
factors associated with typhoid fever in Son La province, northern Vietnam, Transactions of
the Royal Society of Tropical Medicine & Hygiene, vol. 99, no. 11, pp. 819-826.
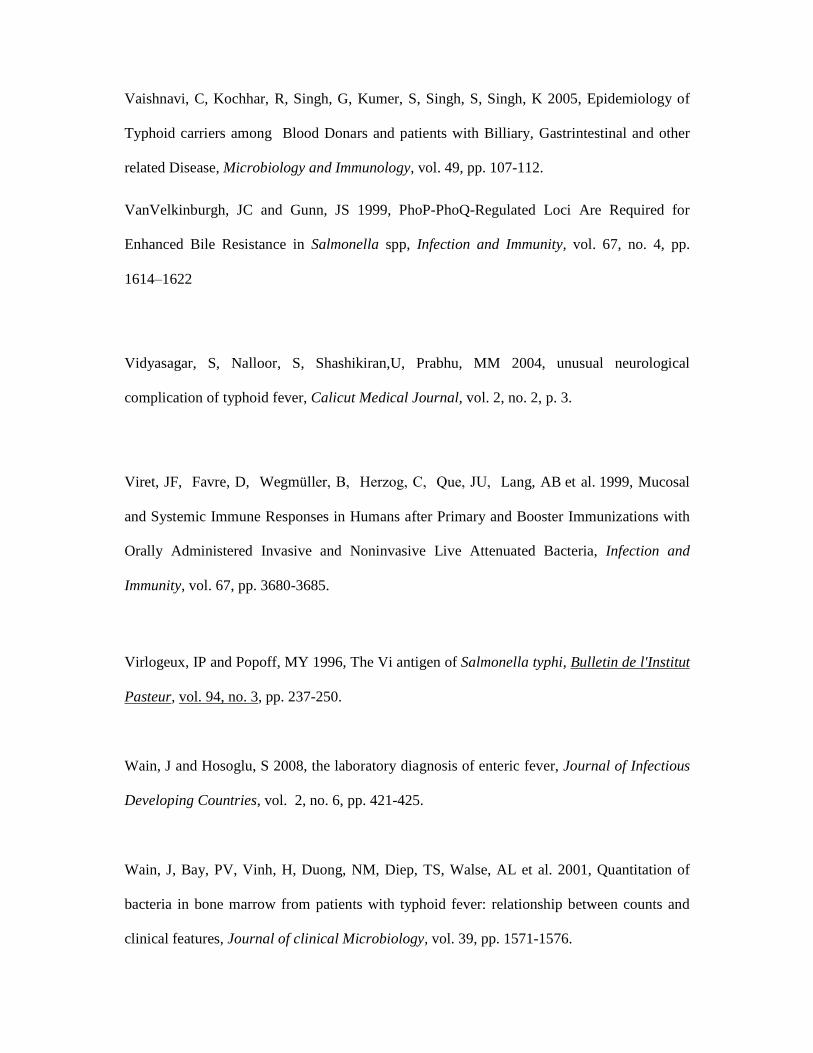
Vaishnavi, C, Kochhar, R, Singh, G, Kumer, S, Singh, S, Singh, K 2005, Epidemiology of
Typhoid carriers among Blood Donars and patients with Billiary, Gastrintestinal and other
related Disease, Microbiology and Immunology, vol. 49, pp. 107-112.
VanVelkinburgh, JC and Gunn, JS 1999, PhoP-PhoQ-Regulated Loci Are Required for
Enhanced Bile Resistance in Salmonella spp, Infection and Immunity, vol. 67, no. 4, pp.
1614�1622
Vidyasagar, S, Nalloor, S, Shashikiran,U, Prabhu, MM 2004, unusual neurological
complication of typhoid fever, Calicut Medical Journal, vol. 2, no. 2, p. 3.
Viret, JF, Favre, D, Wegmüller, B, Herzog, C, Que, JU, Lang, AB et al. 1999, Mucosal
and Systemic Immune Responses in Humans after Primary and Booster Immunizations with
Orally Administered Invasive and Noninvasive Live Attenuated Bacteria, Infection and
Immunity, vol. 67, pp. 3680-3685.
Virlogeux, IP and Popoff, MY 1996, The Vi antigen of Salmonella typhi, Bulletin de l'Institut
Pasteur, vol. 94, no. 3, pp. 237-250.
Wain, J and Hosoglu, S 2008, the laboratory diagnosis of enteric fever, Journal of Infectious
Developing Countries, vol. 2, no. 6, pp. 421-425.
Wain, J, Bay, PV, Vinh, H, Duong, NM, Diep, TS, Walse, AL et al. 2001, Quantitation of
bacteria in bone marrow from patients with typhoid fever: relationship between counts and
clinical features, Journal of clinical Microbiology, vol. 39, pp. 1571-1576.

Wain, J, Hien, TT, Connerton, P, Ali, T, Parry, CM, Chinh, NTT et al. 1999, Molecular
typing of multiple antibiotic- resistant Salmonella enterica serovar typhi from Vietnam:
application to acute and relapse cases of typhoid fever, Journal of clinical Microbiology, vol.
37, pp. 2466-2472.
Wain, J, Hoa,, NT, Chinh NT, Vinh, H, Everett, MJ, Diep, TS et al. 1997, Quinolone-
resistant Salmonella typhi in Viet Nam: molecular basis of resistance and clinical response to
treatment, Clinical Infectious Disease, vol. 25, pp. 1404-1410.
Watson, KC 1956, A Method for the Isolation of Salmonella Typhi from Blood Clot,
American Journal of Tropical Medicine and Hygiene, vol. 5, pp. 131-132.
Watson, KC 1978, Laboratory and Clinical Investigation of Recovery of Salmonella typhi
from Blood, Journal of Clinical Microbiology, vol. 7, no. 2, pp. 122-126.
West, B, Richens, JE, Howard, PF 1989, Evaluation in Papua New Guinea of a urine
coagglutination test and a Widal slide agglutination test for rapid diagnosis of typhoid fever,
Transaction of Royal Society of Tropical Medicine and Hygiene, vol. 83, pp. 715-717.
Wikipedia 2011, Salmonella, Webpage available at �http//en.wikipedia.org/wiki/
Salmonella.� (Accessed on February 24. 2011).
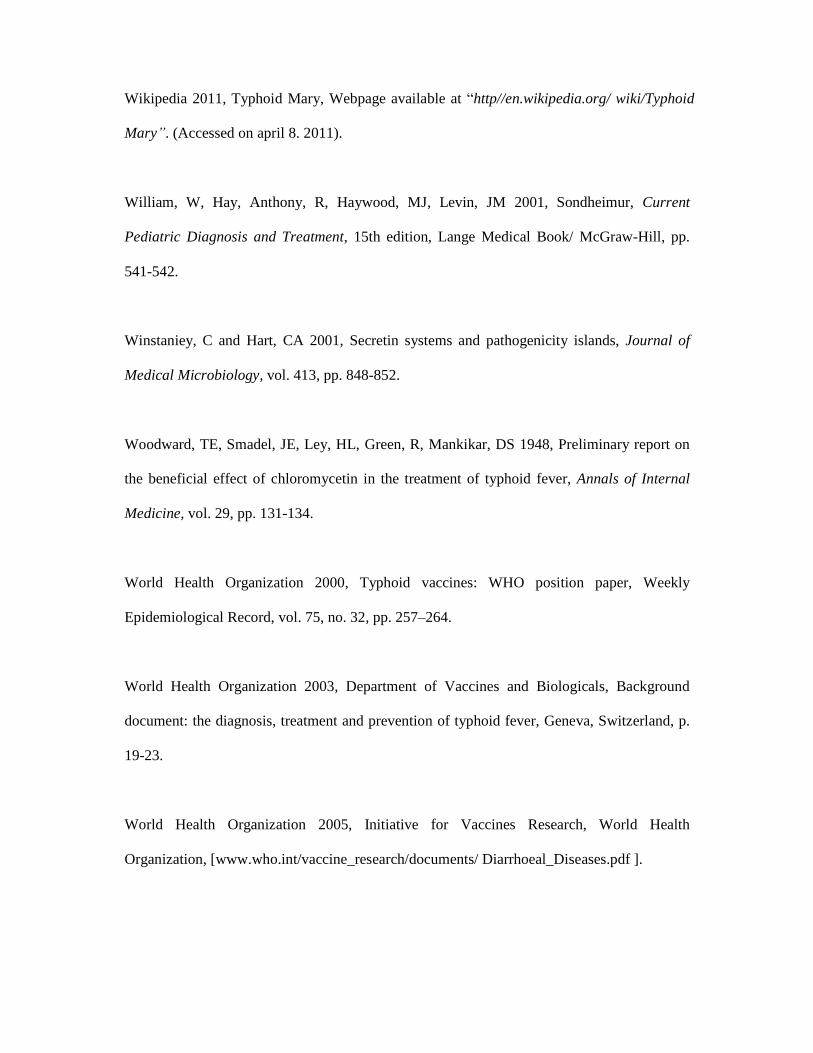
Wikipedia 2011, Typhoid Mary, Webpage available at �http//en.wikipedia.org/ wiki/Typhoid
Mary�. (Accessed on april 8. 2011).
William, W, Hay, Anthony, R, Haywood, MJ, Levin, JM 2001, Sondheimur, Current
Pediatric Diagnosis and Treatment, 15th edition, Lange Medical Book/ McGraw-Hill, pp.
541-542.
Winstaniey, C and Hart, CA 2001, Secretin systems and pathogenicity islands, Journal of
Medical Microbiology, vol. 413, pp. 848-852.
Woodward, TE, Smadel, JE, Ley, HL, Green, R, Mankikar, DS 1948, Preliminary report on
the beneficial effect of chloromycetin in the treatment of typhoid fever, Annals of Internal
Medicine, vol. 29, pp. 131-134.
World Health Organization 2000, Typhoid vaccines: WHO position paper, Weekly
Epidemiological Record, vol. 75, no. 32, pp. 257�264.
World Health Organization 2003, Department of Vaccines and Biologicals, Background
document: the diagnosis, treatment and prevention of typhoid fever, Geneva, Switzerland, p.
19-23.
World Health Organization 2005, Initiative for Vaccines Research, World Health
Organization, [www.who.int/vaccine_research/documents/ Diarrhoeal_Diseases.pdf ].

Yang, HH, Kilgore, PE, Yang, LH, Park, JK, Pan, YF, Kim, Y et al. 1999, An outbreak of
typhoid fever, Xing-An County, People�s Republic of China, Estimation of the field
effectiveness of Vi polysaccharide typhoid vaccine, The Journal of Infectious Disease, vol.
183, pp. 1775-1780.
Yang, HH, Wu, CG, Xie, GZ, Ding, TS, Yang, YO, Tang, WS et al. 2001, Efficacy trial of Vi
polysaccharide vaccine against typhoid fever in southwestern China, Bulletin of the World
Health Organization, vol. 79, no. 7, pp. 625-631.
Yashavanth, R and Vidyalakshmi, K 2010, The Re-Emergence Of Chloramphenicol
Sensitivity Among Enteric Fever Pathogens In Mangalore, Journal of Clinical and
Diagnostic Research, vol. 4, pp. 3106-3108.
Zhang, XL, Tsui, ISM, Yip, CC, Fung, AWY, Wong, DKH, Dai, X et al. 2000, Salmonella
enterica Serovar Typhi Uses Type IVB Pili To Enter Human Intestinal Epithelial Cells,
Infection and immunity, vol. 68, pp. 3067�3073.
Zwadyk, P 1992, Enterobacteriaceae: Salmonella and Shigella, Intestinal pathogens, in
Joklik, WK, Willet, HP, Amos, B and Wilfert, CM editors, Zinsser Microbiology, 20th editon,
USA, Appleton and Lange, pp. 556-565.

Photograph-1: Steps of preparing and processing of sample for Nested PCR
One ml EDTA containing blood
in a appendorf tube
Centrifuge at 13000 rpm for 5
minutes.
Supernatant
discarded
One ml 0.2%
triton X-100
was added to
the pellete
Boiled at 990C for 10 minutes
Preparation of master mixture in PCR tubes
Placing the PCR tube in thermal cycler
Gel electrophoresis of amplified
products
Visualization of the amplified products by UV light trans-
illuminator.
The mixture was vortexed.
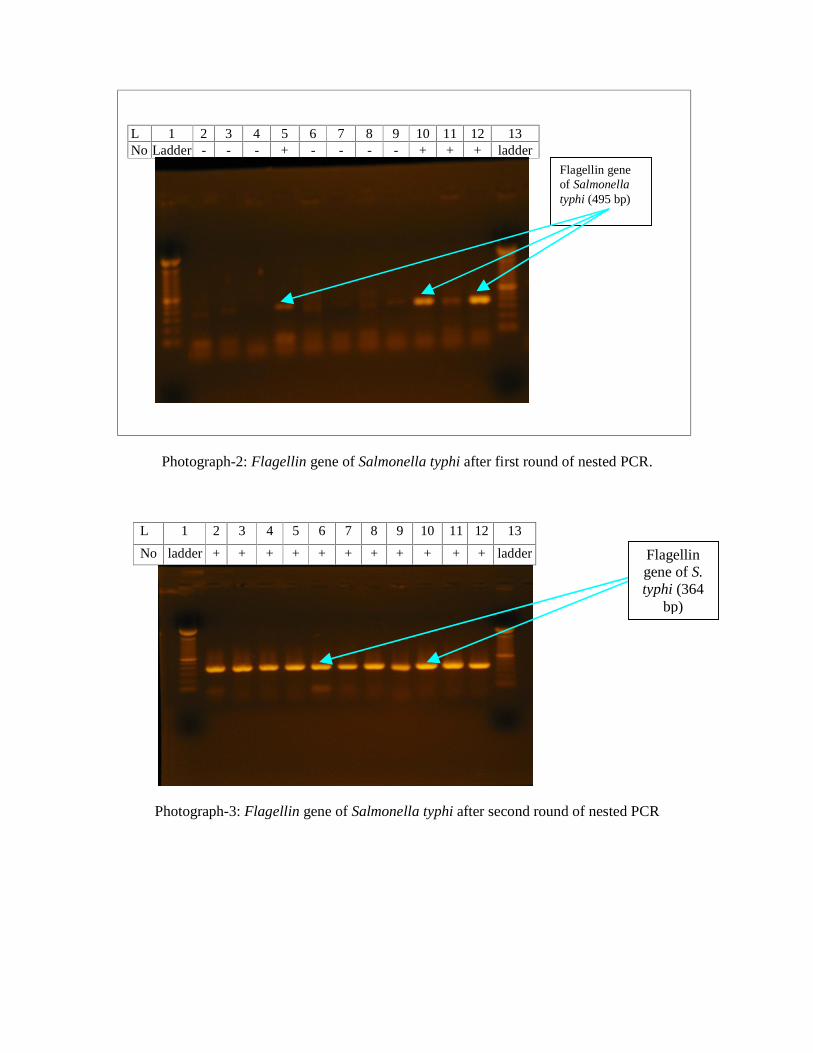
Flagellin gene of Salmonella typhi (495 bp)
L 1 2 3 4 5 6 7 8 9 10 11 12 13 No Ladder - - - + - - - - + + + ladder
Photograph-2: Flagellin gene of Salmonella typhi after first round of nested PCR.
L 1 2 3 4 5 6 7 8 9 10 11 12 13
No ladder + + + + + + + + + + + ladder
Photograph-3: Flagellin gene of Salmonella typhi after second round of nested PCR
Flagellin gene of S. typhi (364
bp)

Photograph-4: Heparinized tube containing lytic solution
Photograph-5: Initial processing of blood for culture by lytic centrifugation method

.
Photograph-6: Growth of S. typhi after 24 hours of incubation by lytic centrifugation method. Photograph-7: Growth of non lactose fermenting colony Salmonella typhi on Mac conkey�s
agar media.
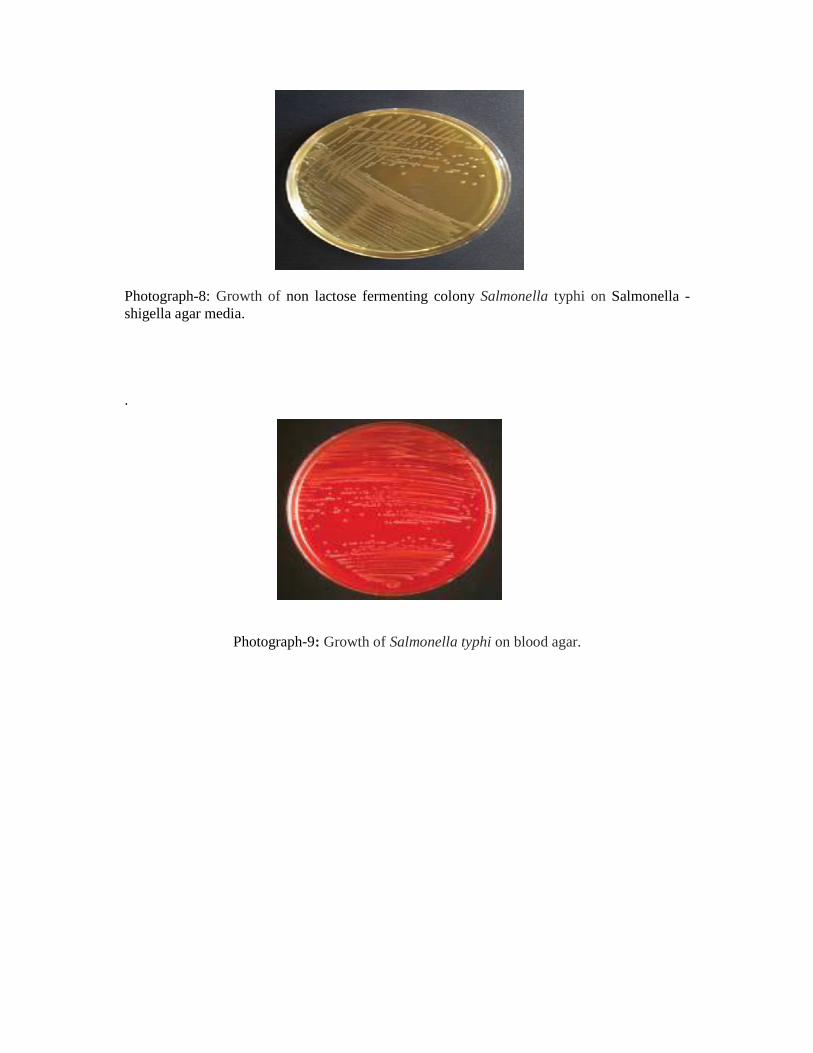
Photograph-8: Growth of non lactose fermenting colony Salmonella typhi on Salmonella - shigella agar media. .
Photograph-9: Growth of Salmonella typhi on blood agar.
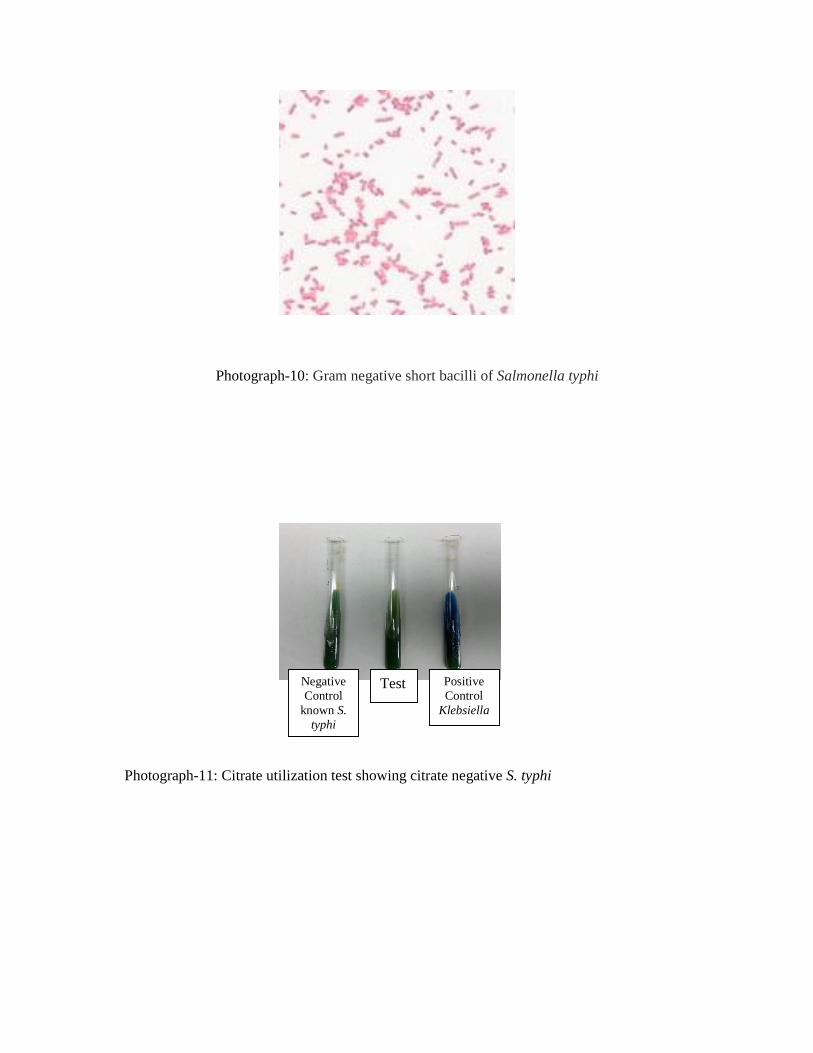
Photograph-10: Gram negative short bacilli of Salmonella typhi
Photograph-11: Citrate utilization test showing citrate negative S. typhi
Negative Control
known S. typhi
Test Positive Control
Klebsiella
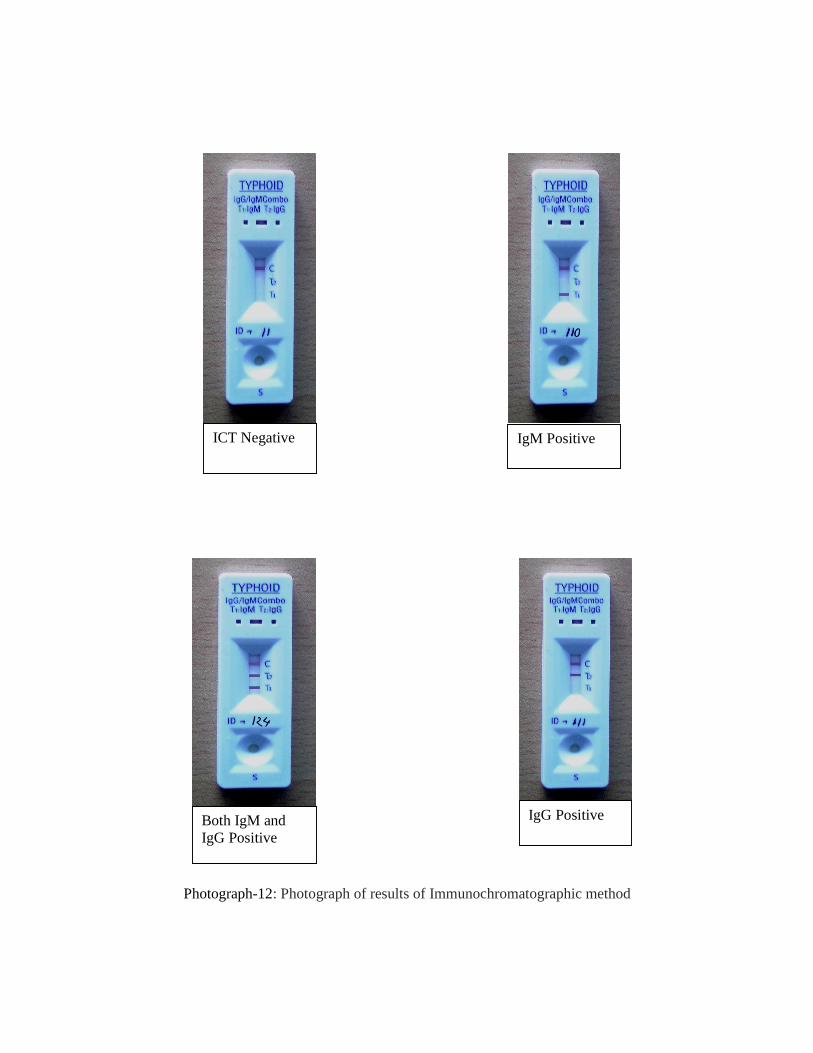
Photograph-12: Photograph of results of Immunochromatographic method
ICT Negative
IgG Positive
IgM Positive
Both IgM and IgG Positive

Photograph-13: Photograph of micro centrifuge

Photograph-14: Photograph of Thermal cycler

Photograph-15: Photograph of Documentation chamber with digital camera.
Photograph-16: Photograph of Horizontal Electrophoresis.
Appendix-I
DATA COLLECTION SHEET
Title of the thesis: Comparison of different test methods including polymerase chain reaction
for early and reliable diagnosis of typhoid fever.
ID no. �������..
Date of enrollment: ����/����./������
Particulars of the patient
1. Name: �������������.Age: ����. Sex: ����
2. Address: Vill: ���������. PO: ����..
Thana: �������. District: ���
5. Education: Yes/ No If Yes, level of education:������
6. Income per month of the patient/ guardian: Tk��������./-
7. Living conditions:
a. Living area : Rural/ City/ Slum
b. Housing condition : Kancha (mud house)/ Tinshed/ Tinshed Building/
Buiding
c. Type of latrine using : Sanitary / Open
d. Source of drinking water : Municipal supply/ Tube well/ Pond/ River
8. Presenting complaints:
a) Fever for ����days; Temperature at maximum rise: ��.. 0C
b) ��������c)������������d)��������

9. On examination
a) Physical condition: alert/ toxic b) Temperature: ���..0C
b) Pulse: ����. / min c) Coated tongue
d) Rose spot e) Abdominal tenderness
f) Caecal gurgling g) Liver
h) Spleen
10. Previous history
a) Antibiotic intake: Yes/ No
If Yes, name of antibiotic���������
Dose & route of administration����� Duration: for���..days
b) History of contact from similar illness in last 1 moth: Yes/ No
c) History of vaccination: Yes/ No If Yes, date of vaccination: ���
Laboratory findings:
1) ICT: Positive/ Negative If Positive: IgG/ IgM/ both
2) PCR: Flagellin gene positive/ negative
3) Blood culture (lytic centrifugation method) result:
Shows growth of �����������������after 24/48 hrs

Identification tests done:
Date Test name Findings comments
Motility by Hanging
drop
MIU
TSI
Citrate Utilization test
Sensitivity test result
Antibiotic IZD
(mm)
Result Antibiotic IZD
(mm)
Result
Appendix - II For Patients
AeMwZµ�g m¤§wZcÎ
GB m¤§wZc�Îi D�Ïk¨ Avcbv�K cÖ�qvRbxq Z_¨ cÖ̀ vb Kiv, �h Z_¨¸�jv Avcbv�K wm×v�� wb�Z mvnvh¨ Ki�e,
Avcbvi m��vb/�ivMx GB M�elYvq AskMÖnb Ki�e wKbv bv?
D�Ïk¨ I c×wZ
UvBd�qW �ivM evsjv�`�k GKwU mvaviY mgm¨v| Avgvi M�elYvi D�×k¨ n�jv UvBd�qW �ivM wbY©q Kiv Ges �ivM
wbY�©qi mnRZg c×wZ �ei Kiv| G�Z cieZx©�Z mwVK, mjc mg�q Ges mnRZg c×wZ�Z UvBd�qW �ivM wbY©q K�i
gvbz�li UvBd�qWRwbZ RwVjZv Kg�e|
Avcwb hw` Avcbvi m��vb/�ivMx�K GB M�elYvq AskMÖnY Kiv�Z m¤§Z _v�Kb Zvn�j Avcbvi/Avcbvi �ivMxi
Amy¯�Zv Ges wPwKrmv m¤úwK©Z wKQz cÖk � Kiv n�e Ges Zv bw_�Z msi¶Y Kiv n�e| M�elbvi Rb¨ 6 wgwj i³ �bqv
n�e|
M�elYvi SzuwK
GB M�elYvq AskMÖn�Y �Kvb kvixwiK SzuwKi m¤¢vebv �bB|
LiP
M�elYvq AskMÖn�Yi Rb¨ Avcbvi m��vb/�ivMxi �ivM wbY� ©qi �Kvb LiP bvB ev Avcbv�K Avw_©K mn�hvMxZv Kivi
Rb¨ e¨e �̄v bvB|
�MvcbxqZv
M�elYv PjvKvjxb I cieZx©�Z cÖk � �_�K cÖvß Z_¨ I j¨ve�iUix �_�K cÖvß Z_¨ K�Vvifv�e �Mvcb ivLv n�e|
M�elYvq AskMÖnY
GB M�elYvq AskMÖnY m¤ú~Y© �¯^�Qvg~jK| Avcwb M�elYvq AskMÖn�Y A¯x̂K �wZ Rvbv�Z cv�ib A_ev M�elYv PjvKxb
�h�Kvb mg�q M�elYv �_�K Avcbvi m��vb/�ivMx�K cªZ¨vnvi K�i wb�Z cv�ib| GB di�g ¯v̂¶i Ki�j Avcbvi
AvBbMZ �Kvb AwaKvi Le© n�e bv| Avcbvi m��vb/�ivMxi wPwKrmv h_vh_fv�e Pj�e| hw` Avcbvi �Kvb cÖk � _v�K,
Avcwb wRÁvmv Ki�Z cv�ib, Avgiv Zvi DËi cÖ̀ vb Kivi h_vmva¨ �Póv Kie|
m¤§wZ ¯x̂Kv�ivw³
Avwg M�elYvq wb�qvwRZ wPwKrm�Ki mv�_ GB M�elYv wb�q Av�jvPbvq m��wó cÖKvk KiwQ| Avwg m¤§wZc�Îi kZ©̧ �jv
c�owQ/Avi m¤§y�L cwVZ n�q�Q Ges �¯^�Qvq Avgvi m��vb�K M�elYvq AskMÖnY Ki�Z m¤§wZ Ávcb KiwQ|
mv¶vrMÖnYKvixi ¯v̂¶i
ZvwiL t
Awffve�Ki ¯v̂¶i/e �×v½yjxi Qvc
ZvwiL t
For Control Group : AeMwZµ�g m¤§wZcÎ
GB m¤§wZc�Îi D�Ïk¨ Avcbv�K cÖ�qvRbxq Z_¨ cÖ̀ vb Kiv, �h Z_¨¸�jv Avcbv�K wm×v�� wb�Z mvnvh¨ Ki�e,
Avcbvi m��vb/�ivMx GB M�elYvq AskMÖnb Ki�e wKbv bv?
D�Ïk¨ I c×wZ
Avcbvi/Avcbvi m��v�bi �ivM cÖwZ�iva ¶gZv ¯v̂fvweK Av�Q wKbv Zv i�³i K�qKwU cwi¶vi gva¨�g wbY©q Kiv
m¤¢e| GB M�elbvi Rb¨ K�qKRb my¯ �̈ ev�Pv/cÖvß eq¯��K A��f©~³ Kiv n�e| i�³i cwi¶v¸�jv gqgbwmsn �gwW�Kj
K�j�R gvB�µvev�qvjRx wefv�M Kiv n�e| UvBd�qW �ivM evsjv�`�k GKwU mvaviY mgm¨v| Avgvi M�elYvi D�×k¨
n�jv UvBd�qW �ivM wbY©q Kiv Ges �ivM wbY�©qi mnRZg c×wZ �ei Kiv |
Avcwb hw` Avcbvi m��vb/�ivMx�K GB M�elYvq AskMÖnY Kiv�Z m¤§Z _v�Kb Zvn�j Avcbvi/Avcbvi �ivMxi
Amy¯�Zv Ges wPwKrmv m¤úwK©Z wKQz cÖk � Kiv n�e Ges Zv bw_�Z msi¶Y Kiv n�e| M�elbvi Rb¨ 6 wgwj i³ �bqv
n�e|
M�elYvi SzuwK
GB M�elYvq AskMÖn�Y �Kvb kvixwiK SzuwKi m¤¢vebv �bB|
LiP
M�elYvq AskMÖn�Yi Rb¨ Avcbvi m��vb/�ivMxi �ivM wbY� ©qi �Kvb LiP bvB ev Avcbv�K Avw_©K mn�hvMxZv Kivi
Rb¨ e¨e �̄v bvB|
�MvcbxqZv
M�elYv PjvKvjxb I cieZx©�Z cÖk � �_�K cÖvß Z_¨ I j¨ve�iUix �_�K cÖvß Z_¨ K�Vvifv�e �Mvcb ivLv n�e|
M�elYvq AskMÖnY
GB M�elYvq AskMÖnY m¤ú~Y© �¯^�Qvg~jK| Avcwb M�elYvq AskMÖn�Y A¯x̂K �wZ Rvbv�Z cv�ib A_ev M�elYv PjvKxb
�h�Kvb mg�q M�elYv �_�K Avcbvi m��vb/�ivMx�K cªZ¨vnvi K�i wb�Z cv�ib| GB di�g ¯v̂¶I Ki�j Avcbvi
AvBbMZ �Kvb AwaKvi Le© n�e bv| Avcbvi m��vb/�ivMxi wPwKrmv h_vh_fv�e Pj�e| hw` Avcbvi �Kvb cÖk � _v�K,
Avcwb wRÁvmv Ki�Z cv�ib, Avgiv Zvi DËi cÖ̀ vb Kivi h_vmva¨ �Póv Kie|
m¤§wZ ¯x̂Kv�ivw³
Avwg M�elYvq wb�qvwRZ wPwKrm�Ki mv�_ GB M�elYv wb�q Av�jvPbvq m��wó cÖKvk KiwQ| Avwg m¤§wZc�Îi kZ©̧ �jv
c�owQ/Avi m¤§y�L cwVZ n�q�Q Ges �¯^�Qvq Avgvi m��vb�K M�elYvq AskMÖnY Ki�Z m¤§wZ Ávcb KiwQ|
mv¶vrMÖnYKvixi ¯v̂¶i
ZvwiL t
Awffve�Ki ¯v̂¶i/e �×v½yjxi Qvc
ZvwiL t
Appendix III

Preparation of lytic solution
Composition of lytic solution:
For adult:
Sodium polyanethol sulfonate (SPS) ----1.53 gram
Saponin ----- 2.80 gram
Distilled water -----100ml
For Infant:
Sodium polyanethol sulfonate (SPS) ---- 0.19 gram
Saponin ---- 0.80 gram
Distilled water ----- 20ml
Sterilization of lytic solution:
By autoclaving at a temparature of 121ºc, pressure of 15ib for 15 minutes.
With all aseptic precaution by the help of sterile pipette and sterile tips lytic solution
dispensed into Heparinized tubes within a biosafety cabinet.
For adult 1 ml and for infant 125µå of lytic solution in each heparinized tube.
Appendix IV
The composition and methods of preparation of different media used in this study are given
bellow:
Blood agar media:
Dehydrated blood agar base : 40 grams.
Distilled water : 1000.0ml
PH : 6.8
Autoclave at 1210 C for 15 minutes under 15 Ibs. Pressure, cooled down at 500 C, 7% sheep
blood (defibrinated, aseptically colleted) was added, mixed well and poured into sterile Petri
dishes.
MacCokey�s agar media:
Dehydrated MacConkey�s agar base : 51.5 gm
Distilled water : 1000.0ml
Media was dissolved and PH was adjusted to 7.2 to 7.6 at 250 C and autoclave at 1210 C for
15 minutes. When it was cooled to 550 C, poured into sterile Petri dish.
Nutrient agar media:
Dehydrated blood agar base : 40 gm
Distilled water : 1000.0ml
PH 7.3 ± 0.2
Autoclave at 1210 C for 15 minutes. When it was cooled to 550 C, poured into sterile Petri
dish.
Triple sugar iron (TSI) agar media:
Dehydrated TSI agar base : 65.0 gm.
Distilled water : 1000.0 ml
PH : 7.2-7.6
The ingredients were dissolved by boiling and the PH was checked, distributed into test tube
in 5 ml amounts and sterilized by autoclaving at 121oC for 15 minutes under 15 Ibs. Pressure.
Allow the medium to solidify in a sloped position to give a butt 25-30 mm and a slope 20-25
mm long. Store in a cool dark place or at 2- 80 C.
Simmon�s citrate media:
Dehydrated media : 24.2 gm.
Distilled water : 1000.0 ml
PH : 6.8
Ingredient dissolved, dispensed into test tubes and autoclave at 1210 C for 15 minutes and
allowed to set as slopes.
Appendix - V

Gram staining technique (Cheesbrough 2010)
Required
Crystal violet stain, Lugol�s iodine, Acetone-alcohol decolourizer, Neutral red, 1 g/l (0.1%
w/v).
Before Gram staining smear of positive control of known S. typhi in one side of a slide, a
negative control of gram positive cocci in another side of slide and test in the middle of slide
were prepared.
Method:
1. Fix the dried smear by gentle heat.
2. Cover the fixed smear with crystal violet stain for 30-60 seconds.
3. Rapidly wash off the stain with clean water.
4. Tip of all the water, and cover the smear with Lugol�s iodine for 30-60 seconds.
5. Wash of the iodine with clean water.
6. Decolourize rapidly (few seconds) with acetone-alcohol. Wash immediately with clean
water.
7. Cover the smear with neutral red stain for 2 minutes.
8. Wash off the stain with clean water.
9. Wipe the back of the slideclean, and place it in a draining rack for the smear to air dry.
10. Examine the smear microscopically, first with the 40X objectives to check the staining
and to see the distribution of material, and then with the oil immersion objectives to report
the bacteria and cells.
Appendix - VI

Muller Hinton agar medium
Composition
Ingredients gram/liter
Beef dehytrated infusion 300
Casein hydrolysate 17.50
Starch agar 1.5
Agar 17.00
Thirty-eight grams of dehydrated Mueller Hinton agar medium was suspended in 1000 ml
cold distilled water and boiled to dissolve the medium completely. The solution was then
sterilized by autoclaving at 1210C and 15 lbs pressure for 15 minutes. The autoclaved media
was stored at 40C
Appendix �VII
McFarland Turbidity Standard No. 0.5 (Cheesbrough 2010)
McFarland Standard 0.5 are used as a reference to adjust the turbidity of bacterial
suspensions so that the number of bacteria will be within a given range. A 0.5 McFarland
standard is equivalent to a bacterial suspension containing between 1 x 108 and 2 x
108 CFU/ml of E. coli.
Original McFarland standards were mixing specified amounts of barium chloride and sulfuric
acid together. Mixing the two compounds forms a barium sulfate precipitate, which causes
turbidity in the solution. A 0.5 McFarland standard is prepared by mixing 0.05 mL of 1.175%
barium chloride dihydrate (BaCl2�2H2O), with 9.95 mL of 1% sulfuric acid (H2SO4).
Reagents:
McFarland Turbidity Standard No. 0.5
Approximate Formula Per 100 mL Purified Water
Sulfuric Acid, 0.18 M 99.5 mL
Barium Chloride, 0.048 M 0.5 mL
Preparation of 1 % (V/V) solution of Sulphuric acid by adding 1 ml of concentrated sulphuric
acid to 99 ml of water and 1% (W/V) solution of barium chloride was prepared by dissolving
0.5g of dehydrated barium chloride (BaCl2�2H2O) in 50 ml of distilled water in two separate
sterile flasks. Then 99.5 ml of sulphuric acid and o.5 ml of barium chloride were added to the
clean screw capped test tube, mixed well and 5- 10 ml was distributed in sterile capped test
tubes and sealed.
Appendix �VIII Interpretation of ICT
Positive result:
Both presence of C band and T1 band were indicate for presence of anti S. typhi IgM, The
result was positive.
Both presence of C band and T2 band were indicate for presence of anti S. typhi IgG, The
result was positive.
Presence of C band both T1and T2 band were indicate for presence of anti S. typhi IgG and
IgM, The result was also positive.
Negative results:
If only presence of the C band and absence of any color in the both T (T1 and T2) bands
indicate the result was negative.
Invalid result:
If no C band was developed indicate the assay was invalid.
Appendix �IX
Preparation of 0.2% Triton X 100
To make 100 ml 0.2% Triton X 100 required:
Distilled water���������.100ml.
Concentrated Triton X������0.2ml.
Triton X 100 was mixed well with distilled water by inverting the tube 3-5 times and then
stored at room temperature.
Appendix �X
Maintenance and preservation of culture strains
Organisms grown in appropriate medium for 24 hours were preserved in a nutrient agar slant
at 2-80C in a refrigerator and this culture was used for three month. For long-term
preservation selected and identified strains were stored in brain heart infusion broth with 20%
glycerol and stored frozen without significant loss of viability at �200C until further study
(Cheesbrough 2010).
Appendix �XI
Formula for sensitivity
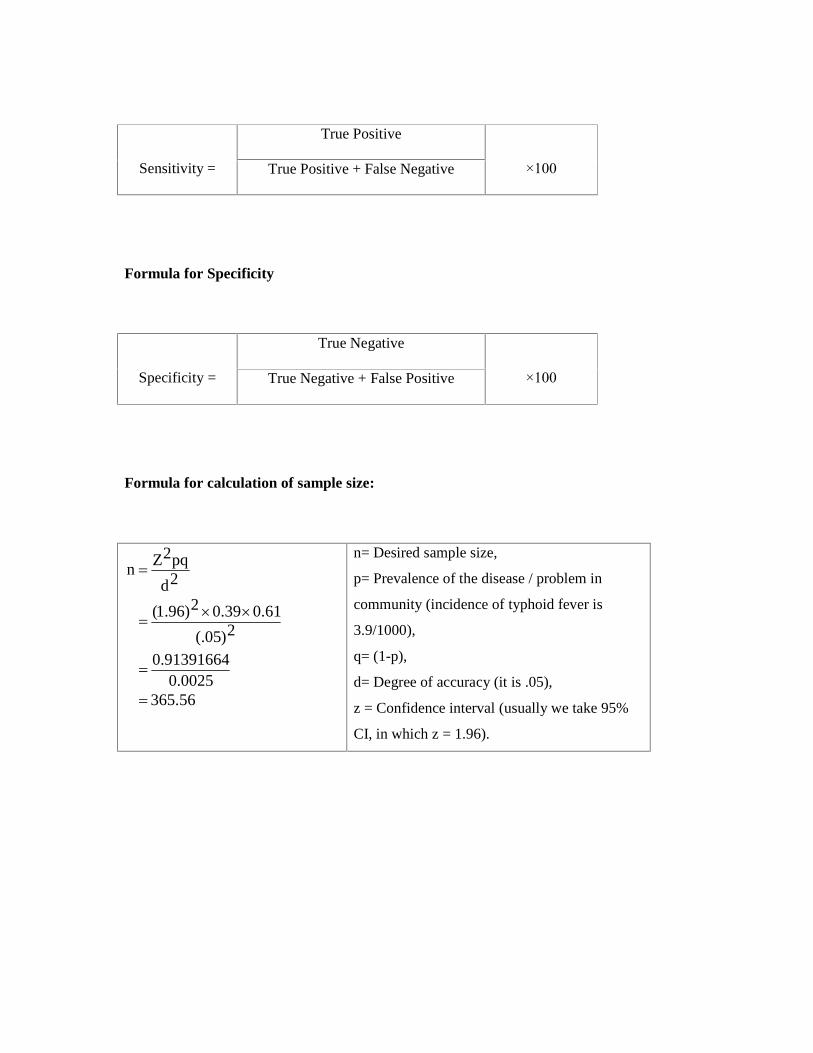
True Positive
Sensitivity = True Positive + False Negative
×100
Formula for Specificity
True Negative
Specificity = True Negative + False Positive
×100
Formula for calculation of sample size:
56.365 0025.0
91391664.0
2)05(.
61.039.02)96.1(
2d
pq2Zn
n= Desired sample size,
p= Prevalence of the disease / problem in
community (incidence of typhoid fever is
3.9/1000),
q= (1-p),
d= Degree of accuracy (it is .05),
z = Confidence interval (usually we take 95%
CI, in which z = 1.96).