ulnar artery aneurysm complicated by distal embolization: management with regional thrombolysis and...
TRANSCRIPT
Ulnar artery aneurysm complicated by distal embolization: Management with regional thrombolysis and resection Thomas W. Lawhorne , Jr., M.D., and Richard A. Sanders, M.D., Columbus, Ga.
We report the first use of preoperative regional thrombolysis followed by resection and primary anastomosis performed for distal embolization that compficated ulnar artery aneurysm. This treatment scheme may be applicable to other situations in which distal emboli complicate the management of arterial lesions. (J VAsc SuR~ 1986; 3:663-5.)
Ulnar artcry aneurysm associated with distal em- holi is an unusual cause of distal ischemia. Regional tnrombolytic therapy before standard microvascular reco'~truction can improve the distal vascular per- fusion. This procedure can enhance arterial runoff and improve the results o f subsequent vascular repair.
CASE REPORT
The patient was a 44-year-old right-handed white male laborer who presented with progressive pain and numbness in the long, ring, and small fingers of the right hand. He recalled striking his hand against a refrigerator 2 weeks earlier. There was no history of diabetes, cardiac, vascular, or collagen disease. At physical examination, the ulnar three fingers were cool and cyanotic and demonstrated poor cap- illary refill. The ring finger was especially ischemic. The ulnar and radial pulses were normal. The Allen test dem- onstrated sluggish filling from the ulnar artery. There was no tenderness or mass in the hypothenar eminence. An ECG yielded normal findings.
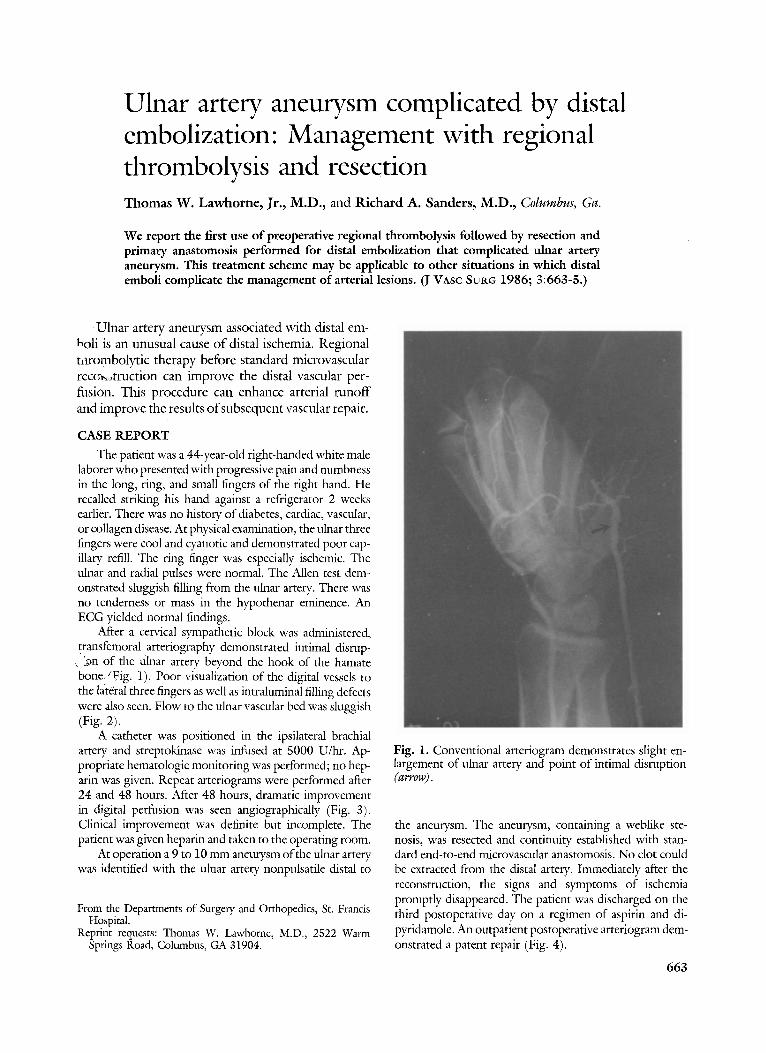
After a cervical sympathetic block was administered, transfemoral arteriography demonstrated intimal disrup- , ~n of the Ulnar artery beyond the hook of the hamate bone~JFig. 1). Poor visualization of the digital vessels to the lateral three fingers as well as intraluminal filling defects were also seen. Flow to the ulnar vascular bed was sluggish (Fig. 2).
A catheter was positioned in the ipsilateral brachial artery and streptokinase was infused at 5000 U/hr. Ap- propriate hematologic monitoring was pe4brmed; no hep- arin was given. Repeat arteriograms were performed after 24 and 48 hours. After 48 hours, dramatic improvement in digital perfusion was seen angiographically (Fig. 3). Clinical improvement was definite but incomplete. The patient was given heparin and taken to the operating room.
At operation a 9 to 10 mm aneurysm of the ulnar artery was identified with the ulnar artery nonpulsatile distal to
From the Departments of Surgery and Orthopedics, St. Francis Hospital.
Reprint requests: Thomas W. Lawhorne, M.D., 2522 Warm Springs Road, Columbus, GA 31904.
Fig. 1. Conventional arteriogram demonstrates slight en- largement of ulnar artery and point of intimal disruption (arrow).
the aneurysm. The aneurysm, containing a weblike ste- nosis, was resected and continuity established with stan- dard end-to-end microvascular anastomosis. No clot could be extracted from the distal artery. Immediately after the reconstruction, the signs and symptoms of ischemia promptly disappeared. The patient was discharged on the third postoperative day on a regimen of aspirin and di- pyridamole. An outpatient postoperative arteriogram dem- onstrated a patent repair (Fig. 4).
663
664 Lawhorne and Sanders
Journal of VASCULAR
SURGERY
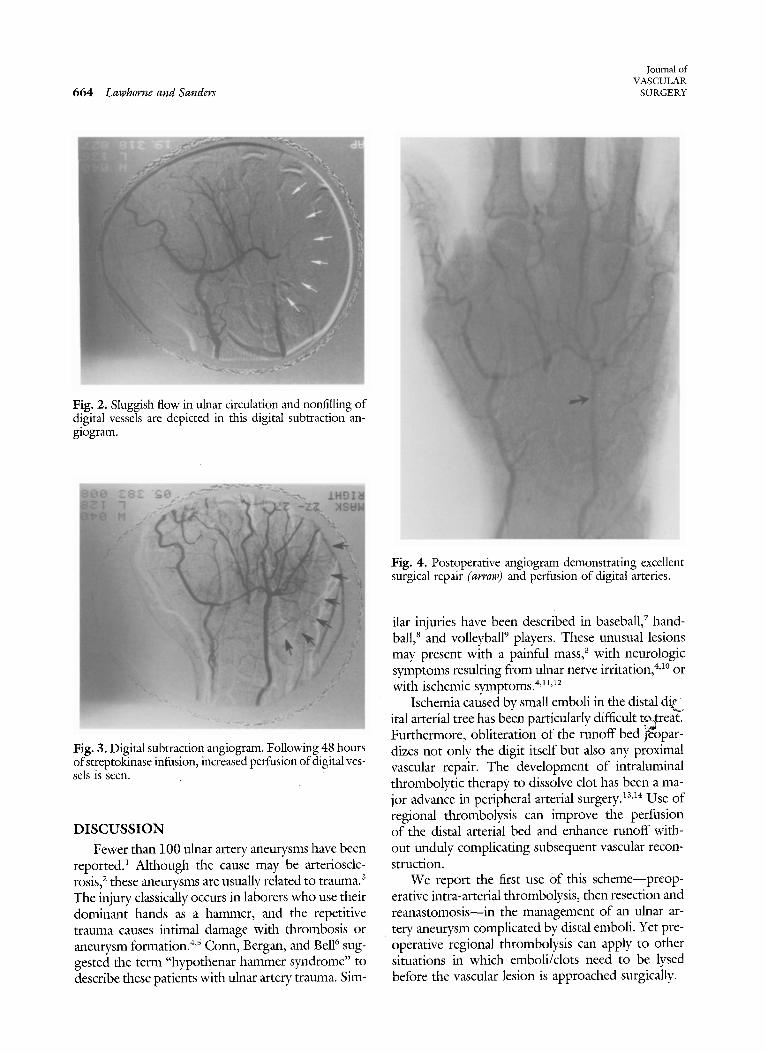
Fig. 2. Sluggish flow in ulnar circulation and nonfilling of digital vessels are depicted in this digital subtraction an- giogram.
Fig. 3. Digital subtraction angiogram. Following 48 hours ofstreptokinase infusion, increased perfusion of digital ves- sels is seen.
DISCUSSION
Fewer than 100 ulnar artery aneurysms have been reported) Although the cause may be artcrioscle- rosis, 2 these aneurysms are usually related to trauma. 3 The injury classically occurs in laborers who use their dominant hands as a hammer, and the repetitivc trauma causes intimal damage with thrombosis or aneurysm formation. 4's Conn, Bergan, and BeD sug- gested the term "hypothenar hammer syndrome" to describe these patients with ulnar artery trauma. Sim-
Fig. 4. Postoperative angiogram demonstrating excellent surgical repair (arrow) and perfusion of digital arteries.
ilar injuries have been described in baseball, 7 hand- ball, 8 and volleyball 9 players. These unusual lesions may present with a painful mass, 3 with neurologic symptoms resulting from ulnar nerve irritation, 4'1° or with ischemic symptoms. <n'12
Ischemia caused by small emboli in the distal di£~ ital arterial tree has been particularly difficult t.o~treat. Furthermore, obliteration of the runoff bed j~bpar- dizes not only the digit itself but also any proximal vascular repair. The development of intraluminal thrombolytic therapy to dissolve clot has been a ma- jor advance in peripheral arterial surgery) 3a4 Use of regional thrombolysis can improve the perfusion of the distal arterial bed and enhance runoff with- out unduly complicating subsequent vascular recon- struction.
We report the first use of this scheme--preop- erative intra-arterial thrombolysis, then resection and reanastomosis--in the management of an uhlar ar- tery aneurysm complicated by distal emboli. Yet pre- operative regional thrombolysis can apply to other situations in which emboli/clots need to be lysed before the vascular lesion is approached surgically.

Volume 3 Number 4 April 1986 Ulnar artery aneurysm 665
RE' 2RENCES 1. May Jr JW, Grossman JAI, Costas B. Cyanotic painful index
and long fingers associated with an asymptomatic ulnar artery aneurysm. Case report. J Hand Surg 1982; 7:622-5.
2. Thorrens S, Trippel OH, Bergan JJ. Arteriosclerotic aneu- rysms of the hand. Arch Surg 1966; 92:937-9.
3. Kleinert HE, Burget GC, Morgan JA, Kutz JE, Atasoy E. Aneurysms of the hand. Arch Surg 1973; 106:554-7.
4. Gaylis H. Occupational trauma to the ulnar artery. S A/'r Med J 1981; 59:746-8.
5. Koman LA, Urbaniak JR. Ulnar artery insufficiency: A guide to treatment. J Hand Surg 1981; 6:16-24.
6. Conn Jr J, Bergan JJ, Bell JL. Hypothenar hammer syndrome: Posttraumatic digital ischemia. Surgery 1970; 68:1122-8.
7. Lowry CW, Chadwick RO, Wattman EM. Digital vessel trauma from repetitive impacts in baseball catchers. J Hand Surg 1976; 1:236-8.
8. Buckhout BC, Warner MA. Digital perfusion of handball players. Am J Sports Med 1980; 8:206-7.
9. Kostianen S, Orava S. Blunt injury of the radial and ulnar arteries in volleyball players. Br J Sports Med 1983; 17: 172-6.
10. Kalisman M, Laborde K, WolffTW. Ulnar artery compres- sion secondary to ulnar artery false aneurysm at the Guyon's canal. J Hand Surg 1982; 7:137-9.
11. Millender LH, Nalebuff EA, Kasdon E. Aneurysms and thromboses of the ulnar artery in the hand. Arch Surg 1972; 105:686-90.
12. VonKuster L, Abt AB. Traumatic aneurysms of the ulnar artery. Arch Pathol Lab Med 1980; 104:75-8.
13. Bell WR. Thrombolytic therapy--a new realistic approach in treatment of thromboocclusive vascular disease. Surgery 1982; 92:913-4.
14. Sicard GA, Schier JJ, Totty WG, Gilula LA, Walker WB, Etheredge EE, Anderson CB. Thrombolytic therapy for acute arterial occlusion. J VASC SURG 1985; 2:65-78.