ultrasound advanced image optimization provided by inland imaging llc. presented by scott cutler bs,...
TRANSCRIPT

UltrasoundAdvanced Image Optimization
Provided By
Inland Imaging LLC.Presented By
Scott Cutler BS, RDMS, RVT, RDCS

Answering the clinical question…
• 42 year old female who is a marathon runner • Complains of severe abdominal pain and
bloating with exercise• Pain developed over a few months• Has had CT’s and Ultrasounds locally and at
very reputable institutions showing negative results to explain pain
• I scanned and we had the patient and her husband, her doctor, my manager, a nurse and the GI sonographer that scanned her originally.

Think Outside The Box…Way Outside!
• This woman’s physician, who was retired, demonstrated the “Fred Factor” in this patient’s care.
• He brought her into our facility in Colorado Springs which was set up for cardiac and vascular ultrasound.
• I was selected to scan her• Her doctor wanted to do an excursive
abdominal scan (???) to reproduce the symptoms

Game Plan
• It was a little intimidating scanning after facilities like Mayo Clinic and UC Davis
• We had to come up with a game plan• The first diagnosis that made sense was
Arcuate Ligament Syndrome. This was quickly ruled out
• Healthy individual with pain and bloating (didn’t look like bloating) after excursive???
• What looked abnormal? Hepatic Veins and the IVC were aliasing. That was it!
Think Tank
• We reviewed the symptoms and the history• The only thing I could think of that would
cause these symptoms was Portal Hypertension.
• But, I already scanned her liver and it was homogeneous with normal echogenicity and it measured within normal limits.
• All we knew was that the hepatic vein confluence and the IVC were aliasing.

Re-Scan
• I looked closer at the aliasing. • I determined that the IVC was aliasing due to
weight of the liver. This was determined normal after rolling her on her side relieving the pressure.
• But the Hepatic vein aliasing was still there.• Doppler sampling revealed a continuous
hepatofugal flow of 200 cm/sec.• I Doppler sampled the other hepatic vessels
and they were relatively normal.

Treadmill…
• Next step, the treadmill.• She lasted 3 minutes and was in severe pain
so we pushed her to 5 minutes (had to make sure it was real).
• It took 2 doses of fentanyl to calm her down enough to Doppler. (can’t fake that pain)
• The post stress Doppler gave velocities over 320 cm/sec.

Diagnosis???
• The only thing that made sense was Budd-Chiari Syndrome.
• The text books only show advanced stages of this disease where the diagnostic criteria are occlusion of the hepatic veins by external compression.
• The veins were dilated.• I figured there had to be early stages of the
disease progression so we went with this theory.

Back to California’s UC Davis
• This patient’s doctor sent her back to a major institution where they did a CT and immediately ruled out Budd-Chiari by standard diagnosis. They did confirm our ultrasound findings.
• Her doctor convinced the specialist to check the pressure and they found very high pressures in the hepatic vein. (By Doppler that we obtained 40 mmHg, normal 6 mmHg)
• They performed a TIPS which relieved her pain and bloating for the first time in months.

Back home
• For two weeks she was symptom free• Then she thrombosed the TIPS• Then I found that she was on hormone replacement
therapy due to hysterectomy• This contributed to the Budd-Chiari diagnosis• Mid forties female on hormone replacement therapy.• I suggested she went off the hormones but she
refused• She was dethrombosed twice before I moved and
lost contact.

What’s the point???
• Think outside the box
• Answer the clinical question
• Think like a physiologist
• Have passion for ultrasound
• Passion can’t be taught!

How Does this relate to Image Optimization?
• To get the proper diagnosis and answer the clinical question you need to have the right tools for the job and know how to use them.

Basic Rules of 2D Imaging
Preset – Generally speaking the presets are optimized to the exam type. There are some presets such as OB that have internal changes that are set by the engineers for FDA power regulations and filtering specific to types of exams.

Basic Rules of 2D Imaging
Transducer – Select the appropriate transducer for the application. Think outside the box and try other transducers you may not have considered.
Frequency (speckle size) – We often think of frequency only when we need penetration. Do you consider increasing frequency for smaller speckle size?

Basic Rules of 2D Imaging
• Window!!! – Your image can only be as good as your window. Be aware of what is in front of your target.
• When you watch someone scan see if you can instruct them how to move the transducer for a better image.

Basic Rules of 2D Imaging
Proper Depth – Not only is there irrelevant information and wasted frame rate the detail is degraded and small, then once zoomed the pixel size is large and bloomed.
Number of focal zones (more or less) – Is more always better? What does it do? It focuses the beam throughout and KILLS the frame rate.

Basic Rules of 2D Imaging
Sector size (Same # of lines, more densely packed) – It is fine to take one image showing surrounding structures and the general environment. However, typically you must decrease the sector size taking in just a little more than the structure of interest such as ovaries, transverse aorta, transverse kidneys, gallbladder and over the color Doppler region of interest

Basic Rules of 2D Imaging
Gain – Be very careful not to over or under gain
TGC’s / Auto Optimize – Balanced gain. Have the same from front to back. Don’t have dark in near field and bright in far field.
Zoom – When you zoom, the lines of sight and line density have not changed. You must always change depth and sector size before you zoom. Don’t waste your precious lines of sight. Post processing zoom only magnifies pixels.

Basic Rules of 2D Imaging
Virtual Convex/Beam Steering – Use virtual convex only when you need to see beyond the linear margins. However, when you change to transverse on a structure and it fits in the linear parameters you should use linear rather than virtual convex. Note that most color ROI’s don’t extend to the virtual convex margins. Beam Steering should be used to angle in one direction. This is useful with needle visualization during biopsies.

Basic Rules of 2D Imaging
Frame Rates!!! – Time is an important factor in imaging. You can have all of the technology on for best detail but you will miss the frame you need because you missed the time component. And when you freeze the image it will be blurry.
It is like putting on high definition glasses and using a strobe light. You only see flashes of your target.

Frame Rate Video
http://www.youtube.com/watch?v=aC-d2VckqUw&feature=related

Advanced Imaging:
I’m not saying it’s easy, I am saying it’s worth it.

Advanced Imaging
From Blah To WOW!!!

Advanced Imaging – Get the Money Shot
Dynamic Range – Dynamic range specifies how many shades of gray are available.
Post processing Maps/Colorize Maps – Arrange the given shades of gray into different patterns of gray. Some maps emphasize greater differences between the shades making a higher contrast and others have a more subtle difference making a softer image. Colorized maps give a different perception of the information forcing your eyes to use the cones rather than the rods.

Advanced Imaging – Get the Money Shot
Spatial Compounding (Cross Beam, ASC, ApliPure, Sono CT.) – Multiple lines of sight on each frame. Incredible detail with improved border detection. Be aware of the limitations. Compounding will let you see behind some structures but will also minimize clinical marker such as shadowing and posterior enhancement. It will hit your processing speed so you must slow down. There are changes you will make to your image to improve the frame rates. What structures would you use it on and which would you not. Are there moving structures adjacent to your structure of interest like the heart or a pulsatile artery or even a patient who has significant breathing motion? Don’t think of this as a simple increase and decrease. There are other things you need to consider.

Advanced Imaging – Get the Money Shot
Real Time Adaptive Filters or RTAF’s (SRI, DTCE, Precision, X-Res) – This is not just a smoothing technique. This is a speckle reduction. Our image is made of speckle and each technology is designed to filter the speckle to see what we see as real versus not real. Think of the speckle seen in a bladder, gallbladder or vessels. Is it sludge, plaque, thrombus or just noise?
Pixels in borders are smoothed laterally and pixels within parenchyma are smoothed in all directions.

Standard Definition

Advanced Imaging
From Blah To WOW!!!

Advanced Imaging – Get the Money Shot
Frame Averaging – Think of an old CRT TV (television, not transvaginal). When you turn the TV off you see the image fade away. Frame averaging or Persistence is similar in function. The frame lags on the screen while new frames are added to the image. This fills in gaps in the image. It will give a visual perception of low frame rates. This is good for course images that are not moving fast and are not using compounding. If the image is dynamic like a fetal heart you should use a low frame average.

Advanced Imaging – Get the Money Shot
Edge – Edge is used for better border definition or edge definition. Higher edge is isolates the individual pixels while a lower edge smoothes them together. This is technology does not affect the frame rate and is useful with high end technology like compounding.
Edge affects all pixels the same way. This is different from RTAF’s

Advanced Imaging – Get the Money Shot
Rejection – Rejects low amplitude echoes. Think of this as a filter. Be careful when changing this that you change it back when you move to a different structure.
Suppression – Eliminates low-level echoes associated with acoustic/electrical noise.

Advanced Imaging – Get the Money Shot
• Line density – Optimizes B Mode frame rate or spatial resolution for better detail. This strongly affects frame rate.
• Power – ALARA, as low as reasonably achievable. Not many sonographers use this. The power output will directly affect the MI. This changes the intensity of the beam. You cannot go higher than FDA regulated allowances like on OB. If we could we would penetrate every patient.

Bio Break

How Much Difference Does it Really Make?
• “I believe that every sonographer will miss something in their career…I just hope I don’t miss something significant.”
- Scott Cutler
• You have to have a healthy amount of fear to keep yourself sharp.

Case In Point
• 66 year old male• Ordered for abdominal pain and elevated
alkaline level• Lower back pain• Pylonidal cyst (spelled wrong)• Taking Synthroid• Abnormal liver lab work• History of kidney stones

Pilonidal Cyst ???
• A pilonidal cyst is a cyst that develops along the tailbone (coccyx) near the cleft of the buttocks. These cysts usually contain hair and skin debris. The term pilonidalis derived from the Latin words pilus (hair) and nidus (nest). Individuals with a pilonidal cyst may not have any symptoms at all (termed asymptomatic), whereas others may develop an infection of the cyst with associated pain and inflammation. The treatment and management of pilonidal cysts depends on many factors, including the presence of symptoms and the extent of the disease. Recurrence of pilonidal cysts is common.
• Pilonidal cysts occur more frequently in men than in women, and they are more common in Caucasians than in other racial groups. Pilonidal cysts usually occur between the ages of 15 to 24, and their development is uncommon after the age of 40.

What is the clinical question?
• What else do you want to know?• What else would the radiologist want to
know?

Images

Images

Images
Images

Images

Images

Images

Images

Impressions
Sonographer Impressions:• Inhomogeneous Liver .• Pancreas tail obscured by gas.
Radiologist Impressions:1. Mild heterogeneity of the liver likely due to geographic fatty infiltration.2. CBD diameter is 6.5 mm and no intrahepatic ductal dilatation is seen. No CBD stone is noted.3. Incomplete visualization of the pancreas.
CT

CT

CT

IMPRESSION:
Findings consistent with rectosigmoid carcinoma with probableassociated fistulous communication with a loop of distal ileum.Abnormal adjacent lymph node is noted in addition to numerous liverlesions compatible with metastases.

IMPRESSION:
• Specifically:• Too numerous to count low attenuation
lesions scattered throughout allsegments of the liver compatible with metastases. Representativemeasurements are as follows:1. Segment II, 14 mm.2. Segment VII, 15 mm.3. Segment VIII, 14 mm.4. Segment III, 13 mm.5. Segment VI, 15 mm.

Are your eyes open???

What’s wrong with this picture?

How do I fix this?

How do I fix this?

How do I fix this?

How do I fix this?

How do I fix this?

How do I fix this?

How do I fix this?

How do I fix this?

How do I fix this?

Measurements and Annotation

Measurements and Annotation

Measurements and Annotation

Measurements and Annotation

Sonographer gave wrong diagnosis

What Would You Do Next?

Imaginomas?

Imaginomas?

Best image from transplant study

Next day with linear transducer

From this to…

That.

What Would You Change?

Femoral Vein Mid Original
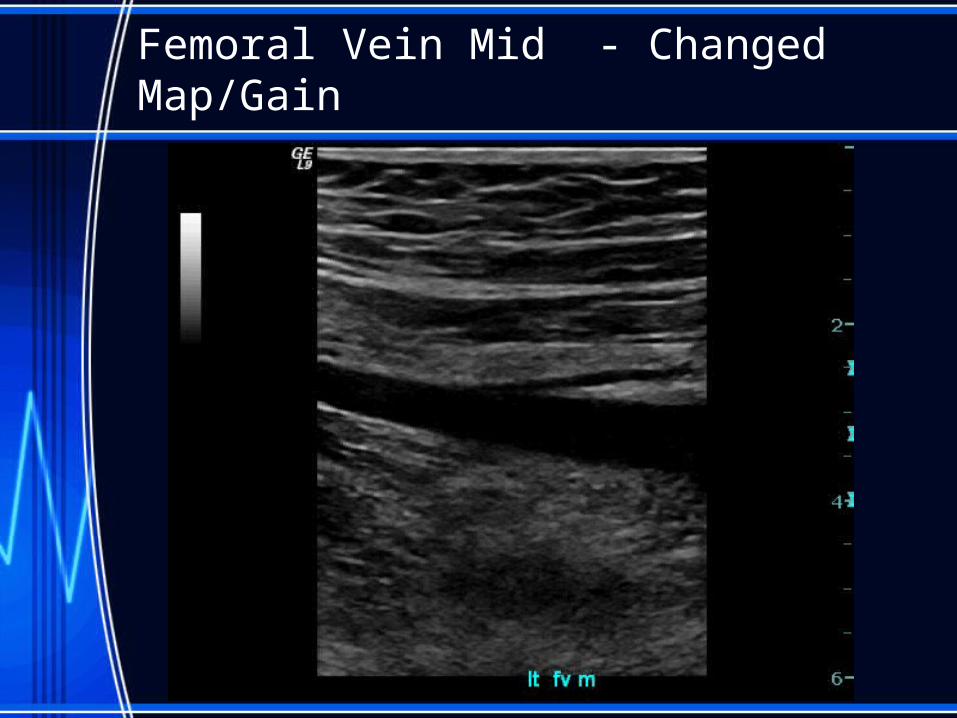
Femoral Vein Mid - Changed Map/Gain

Femoral Vein Mid - SRI

Peroneal Veins with Compression

Popliteal Artery

Another Popliteal Vein

PTV / Peroneal Veins

Another PTV/PER V Clip

Same one with some post processing