understanding death with dignity legislation: a necessity for the palliative care provider - frances...
TRANSCRIPT
Understanding Death with Dignity Legislation: A Necessity for the
Palliative Care Provider
The Washington and Oregon Experiences
Frances DeRook, MD, FACC,Fellow in Palliative Medicine
University of Washington, Seattle, WA

Sources of information:
• Health Department Web Sites– Oregon Public Health Authority– Washington State Department of Health
• Compassion & Choices (Washington and Oregon)– Monthly meetings of volunteers– Client visits– Survey of volunteers
• Personal experience • Colleagues and experts in the field• The literature
Pre-test1. Death with Dignity is also correctly known as
a.Assisted Suicideb.Physician aid in dying c.Euthanasiad.Voluntary Euthanasia
2. Death with Dignity is legal ina.Oregon and Washington onlyb.Oregon, Washington and Californiac.Oregon, Washington, California and Coloradod.Oregon, Washington, Montana and Vermont
3. In the 17 years since it has been legal, DWD has been used by about how many people?e.1,000f. 10,000g.100,000
Pre-test4. In some states DWD is legal in children
a.TRUEb.FALSE
5. Under some DWD laws, someone can use the law if unconscious or demented
c.TRUEd.FALSE
6. Under DWD laws, patients must have the following prognosis:
a. Less than 3 monthsb. Less than 6 monthsc. Less than one year
7. Which of the following patients can use a DWD law:a. Recurrent cancer with a prognosis of 1 yearb. Severe end stage dementiac. Comatose with a severe traumatic brain injuryd. ALS with inability to swallow and bilateral arm paralysis e. None of the above

Pre-test8. If a patient has a terminal diagnosis,
decisional capacity and wishes to use DWD in a state where it is legal, s/he could get a prescription for life-ending medication 7 days after seeing an attending physician.a. TRUEb. FALSE
9. Most of the patients who use DWD do so due to intractable pain.a. TRUEb. FALSE
10.What percent of patients who use DWD are on hospice?a. 10%b. 50%c. 75%d. 90%
ObjectivesAfter this presentation:
1.You will be able to describe why Death with Dignity (DWD) should not be called assisted suicide.
2.You will be able to describe the steps involved with the legal end-of-life choice known as DWD in OR and WA.
3.You will be able to describe the patients in WA and OR who have used the law thus far.
4.You will be able to describe how the legal option of DWD has affected the field of Palliative Care.
Case 1: B
• 47 year old man with high grade primary brain cancer diagnosed 3 months earlier
• Daily chemo and 5X/week XRT– Describes experience as “torture” – Constant HA, restlessness, insomnia, seizures; getting worse with
treatment– Not on hospice; no palliative care consult
• MRI results “pleasing to my docs”• Mother came from Florida to help care for him• Asked for C&C help with DWD process
– Concerns: that he would lose ability to take lethal medication and that his MDs would not help him

Pt. B
• His mother: “Finding out WA was one of the states where he could do this was a huge relief.”
• Admitted with pneumonia • Sent home on hospice, treated with morphine
and died three days later

Case 2: A
• 63 yo man with ALS– Diagnosed 1 yr earlier, rapidly progressive– Communicates via tablet computer with headmouse– Starting to have trouble swallowing
• Does not want a feeding tube
– Arm weakness• “I want peace.”• Worried about “window of opportunity” closing• Wife: Not ready to “let him go” but does not “want
him to suffer”
Pt. A
• A’s neurologist served as the AP.• The patient and his family wanted to keep his
death private.• They gathered at his home at the time that he
took the lethal dose of medication.
Case 3: Pt. C
• 61 yo woman with ALS followed at the UW. Lived in remote small town 150 miles from Seattle
• Disease progressing rapidly. No LE fcn. Only one arm functional
• Tremendous hardship for her to come to clinic• AP made house call, CP met pt at a clinic ½ way• Pt completed process in 16 days. • Died peacefully at her home on day 17 surrounded by
close friends who had helped her through her illness.
Case 4: Mr. E
• 77 yo man with end stage pulmonary fibrosis on continuous HFO, hospice
• SOB with talking, home bound• Does not want to die gasping for air• Trouble finding docs willing to be participating
physicians• Process took about 2 months• Pt plans to hold on to his prescription

Case 5: RG
• 53 yo man with multiple system atrophy, on hospice
• Visited pt at home with his adult dau; confused about process, timeline, how long it will take
• No MDs at his hospital had previously participated• With assistance of motivated MSW, education of
MDs about DWD initiated• About 2 weeks later pt died suddenly while sitting
in his wheelchair at home

Case 6: F
• 53 yo man with Pompe’s Disease; diagnosed at 22, very symptomatic since 35
• Profound muscle weakness, deposition of glycogen in GI tract
• Failed experimental enzyme infusions• On hospice, G and J tubes• Describes himself as “miserable”• “I don’t want to be just a living breathing body that someone
else has to take care of.”• Wife and 16 yo dau present for interview• Some difficulty identifying MDs willing to participate
Words Matter
• Euthanasia: Literally “peaceful dying,” but in practice an act taken by another that ends the life of the patient. Can be voluntary (at the patient’s request) or involuntary (capital punishment). ILLEGAL in healthcare setting.
• Assisted Suicide: The act of assisting someone who is not terminally ill and/or not mentally competent in ending his/her own life. ILLEGAL throughout the U.S..
Legal DefinitionsRCW 70.245.180Nothing in this chapter authorizes a physician or any other person to end a patient's life by lethal injection, mercy killing, or active euthanasia. Actions taken in accordance with this chapter do not, for any purpose, constitute suicide, assisted suicide, mercy killing, or homicide, under the law.
2011c336 § 360; 1975 1st ex.s. c260 § 9A.36.060A person is guilty of promoting a suicide attempt when he or she knowingly causes or aids another person to attempt suicide. Promoting a suicide attempt is a class C felony.So, Assisted Suicide is still Illegal in Washington and Oregon.
04/15/2023 16

“Assisted Suicide” rejected by:
• American Academy of Hospice and Palliative Medicine
• American Public Health Association• American Medical Women’s Association• American College of Legal Medicine• American Medical Student Association• Washington State Psychological
Association
04/15/2023 17

Words Matter: Correct Terminology
• Physician Aid in Dying: The act whereby a qualified terminally ill patient self-administers life-ending medication provided by a physician. Unlike suicide, the person is going to die and curative treatment is not available. (American Public Health Association terminology)
• Physician-Assisted Death: AAHPM terminology
• Death with Dignity: Term used in OR, WA and VT to indicate legislation that codifies the practice04/15/2023 18

Legal Definition
• The law allows a mentally competent, terminally ill adult with a prognosis of 6 months or less to self administer a lethal dose of medication obtained from a medical or osteopathic physician.
• Must complete the requirements of the process as outlined in the law
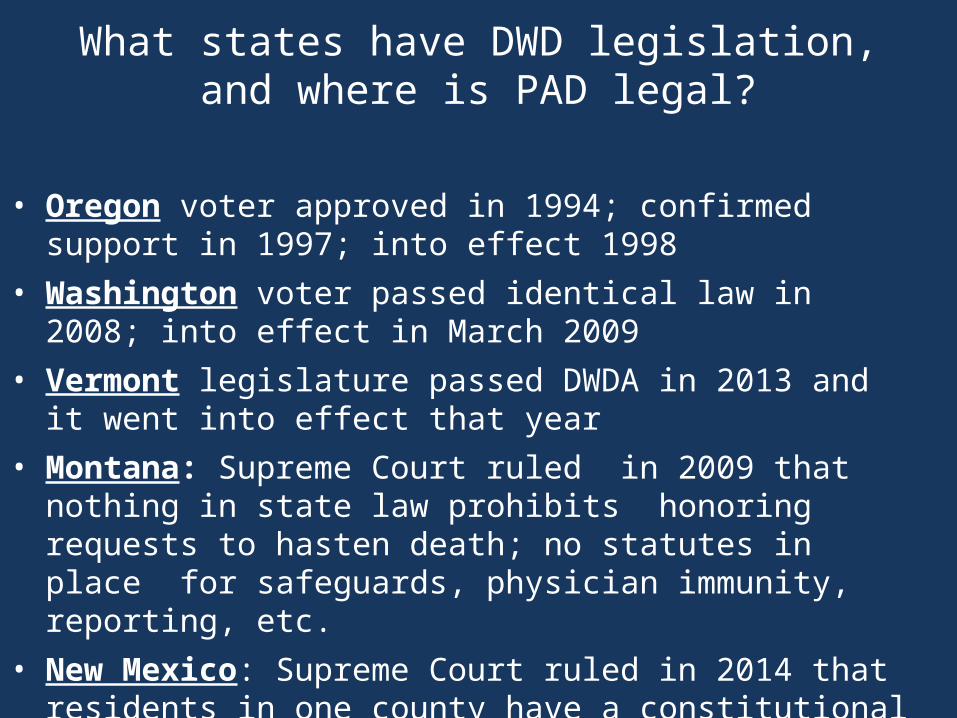
What states have DWD legislation,and where is PAD legal?
• Oregon voter approved in 1994; confirmed support in 1997; into effect 1998
• Washington voter passed identical law in 2008; into effect in March 2009
• Vermont legislature passed DWDA in 2013 and it went into effect that year
• Montana: Supreme Court ruled in 2009 that nothing in state law prohibits honoring requests to hasten death; no statutes in place for safeguards, physician immunity, reporting, etc.
• New Mexico: Supreme Court ruled in 2014 that residents in one county have a constitutional right to hastened death and that doctors who prescribe prescriptions can’t be prosecuted.

I-1000 (WA Death with Dignity Act) passed in all but 9 counties with 58% of the vote
04/15/2023 21

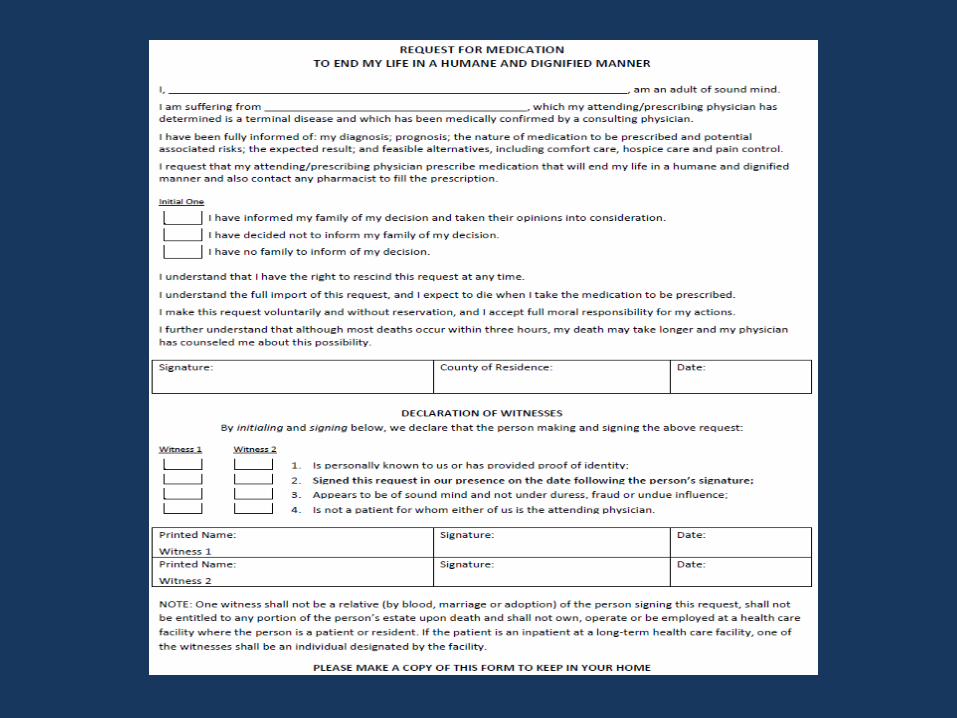
Who is eligible to use DWD?
• The law applies to:– Adults: 18 years of age or older– State residents– Have decisional capacity– Have a terminal illness– Able to self-administer– Able to make two oral requests at least 15
days apart for life-ending medication– Written request can only be made by a patient
who has been informed of the effects of the DWD medications and of the alternatives to DWD.
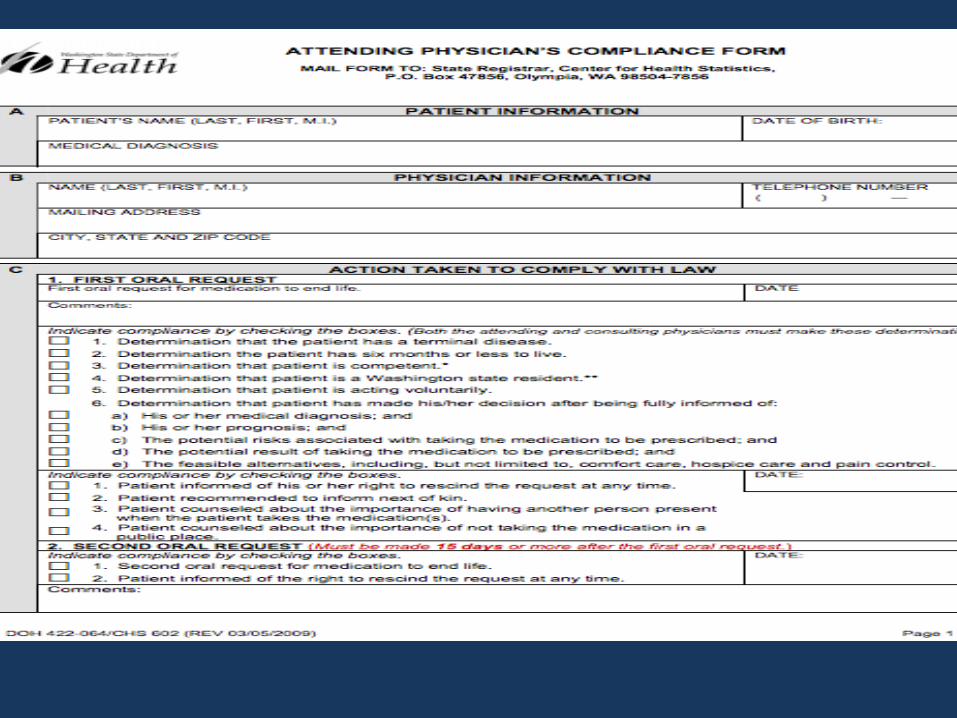
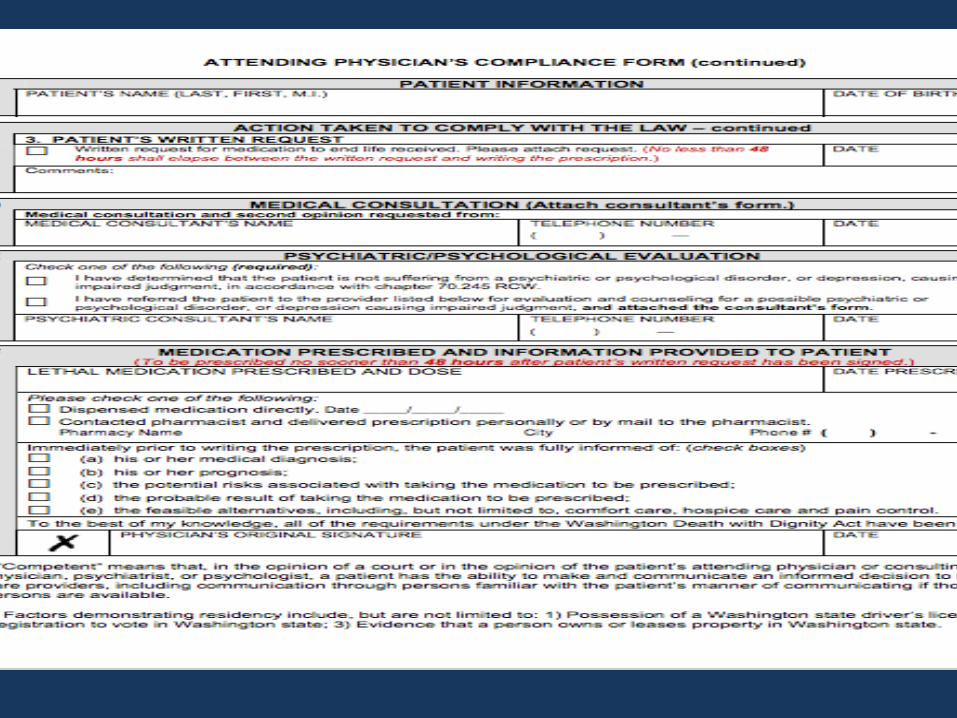
Physician Roles
• Attending Physician (AP)– Counsels the patient, ensures
compliance with the law, and submits physician documents to the Department of Health
–Writes prescriptions for DWD medications
• Consulting Physician (CP) – Confirms patient’s diagnosis, prognosis,
ability to make an informed voluntary decision

Timetable for Completing the Eligibility Process

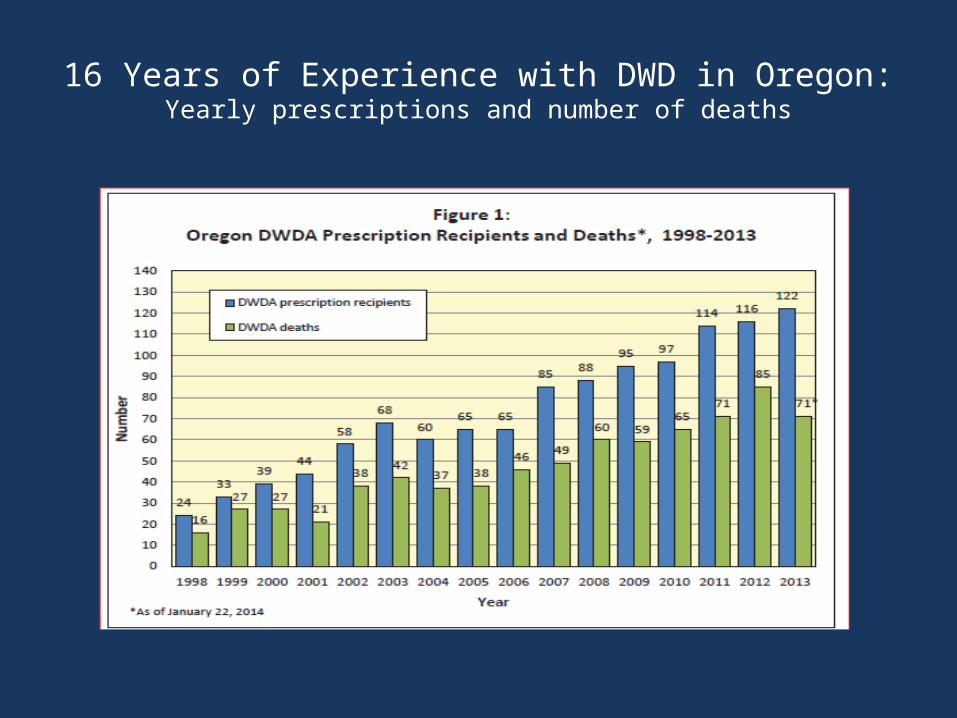
16 Years of Experience with DWD in Oregon:Yearly prescriptions and number of deaths

OR & WA Data 1998 - 2013
04/15/2023 30
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 20130
20
40
60
80
100
120
140
160
180
200
# OR Rxs # OR Died OR DWD Deaths/10,000 # WA Rxs # WA Died WA DWD Deaths/10,000
Num
ber o
f Per
sons
WA Prescriptions
WA Deaths
OR Prescriptions
OR Deaths
OR Rate WA Rate0.2%
OR Prescriptions
OR Deaths
WA prescriptions
WA deaths
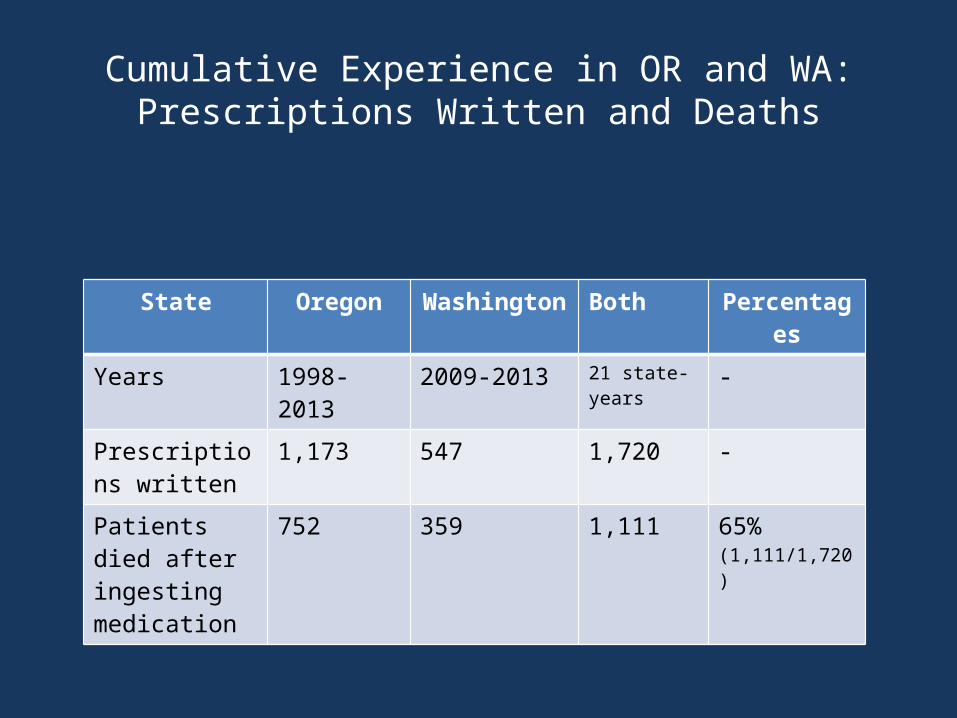
Cumulative Experience in OR and WA:Prescriptions Written and Deaths
State Oregon Washington Both Percentages
Years 1998-2013
2009-2013 21 state-years
-
Prescriptions written
1,173 547 1,720 -
Patients died after ingesting medication
752 359 1,111 65%(1,111/1,720)
How many people have used the law?
• In Oregon as of 2013– 1173 prescriptions/752 ingestions– 22 DWD deaths per 10,000 total deaths
• 0.2% of deaths • 2 out of every 1,000 deaths in the
state
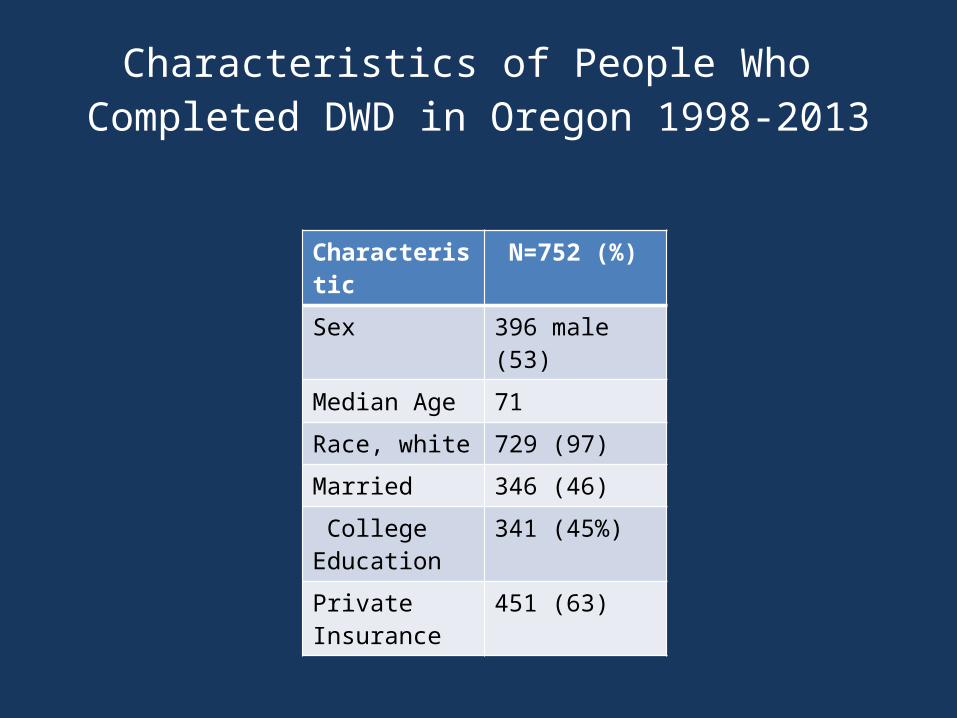
Characteristics of People Who Completed DWD in Oregon 1998-2013
Characteristic N=752 (%)
Sex 396 male (53)
Median Age 71
Race, white 729 (97)
Married 346 (46)
College Education
341 (45%)
Private Insurance
451 (63)
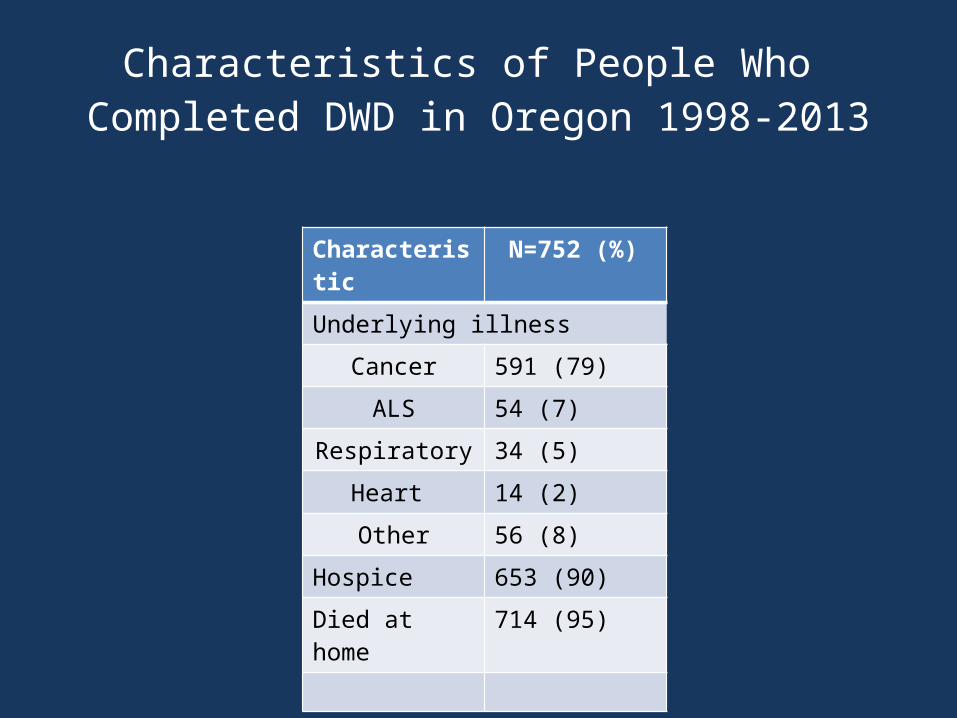
Characteristics of People Who Completed DWD in Oregon 1998-2013
Characteristic N=752 (%)
Underlying illness
Cancer 591 (79)
ALS 54 (7)
Respiratory 34 (5)
Heart 14 (2)
Other 56 (8)
Hospice 653 (90)
Died at home 714 (95)

Most Frequently cited reasons for Using DWD Law (1998-2013)
04/15/2023 35
Patients’ Fear of- Oregon Washington
loss of autonomy 91% 91%
loss of dignity 81% 80%
loss of quality 89% 87%

How often was inadequate pain control
or concern about it in the future cited as a factor?
Oregon: 24%Washington: 35%

Motivation of those who seek physician-assisted death
• Desire to control circumstances of death• Die at home• Maintain independence• Avoid future physical symptoms• Seekers tend to be:– Active, independent/anti-dependent types– Long-time believers in self-determination– Pragmatic, take-charge people – Less interested in quantity of life than in quality
of life• Seekers seem greatly palliated by knowing that
the option is accessible on demand.
Ganzini L et al. Oregonians’ reasons for requesting PAD Arch Intern Med 2009;169:489-492Ganzini L et al.Physicians experiences with the ODWDA NEJM 2000;342-557-563

Timing of Medication Use
• Timing of medication use varies:–Some use meds quickly–Some leave the prescription
on file at the pharmacy for months –1/3 never take the meds

N Engl J Med 2013;368:1417-24.

Seattle Cancer Care Alliance Experience
• DWD policy written and approved by the Med Exec committee
• Information packets created for patients and physicians
• Patients were not accepted solely to access the law
• Information regarding DWD was NOT posted
• Participants signed an agreement not to take the medication in a public area or manner
Seattle Cancer Care Alliance Experience
• Licensed social workers act as patient advocates in the process– Assisted patients, family, physicians, and pharmacists
throughout the process– Tracked required documentation– Assesses patient’s rationale for and interest in
participation– Preliminary chart review– Identify prescribing physician– Formally documents request, verifies state residency,
completes a psychosocial assessment (PHQ 9 and GAD 7)
Seattle Cancer Care Alliance Experience
• Additional Social Worker Functions:– Arrange for clinician to be present at time of ingestion if
desired– Provide advice on securing and disposal of unused medication– Provide grief and legacy support through periodic calls and
visits– Request family notify SCCA when patient ingests the
medication– Bereavement support– Aid physician in completing reporting forms
• Random audits by director of supportive care: nearly 100% compliance with completion of mandated forms and processes
Seattle Cancer Care Alliance Experience
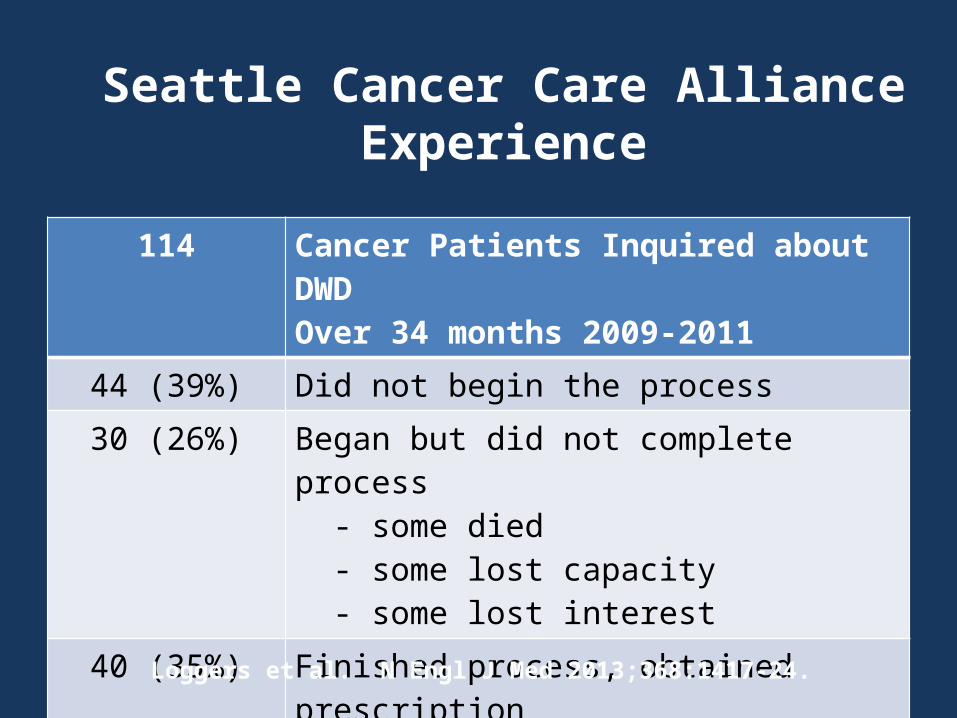
114 Cancer Patients Inquired about DWDOver 34 months 2009-2011
44 (39%) Did not begin the process
30 (26%) Began but did not complete process - some died - some lost capacity - some lost interest
40 (35%) Finished process, obtained prescription
24 (21%) Ingested lethal medication
Loggers et al. N Engl J Med 2013;368:1417-24.

Arguments Against Physician Assisted Death
• Sanctity of life• Harmful consequences
• Vulnerable populations would be adversely affected
• The “Slippery Slope” or broadening of application of the law
• Improper regulation with patient coercion
• Quality of Palliative Care would suffer

Arguments Against: Harmful Consequence #1Vulnerable Populations
• It was predicted that there would be improper overuse in vulnerable populations.
• Those who have used the law are disproportionately:
• Financially secure• Educated• Non-minority

Arguments Against: Harmful Consequence #2The “Slippery Slope”
• Many predicted that the law would be broadened to include anyone who wanted to die for any reason.
• The same classes of patients are eligible in Oregon and Washington.
• No serious efforts to extend the law to other populations or other practices (such as euthanasia) have occurred.

Arguments Against: Harmful Consequence #3
Improper Regulation• Predicted that patients would receive
aid in dying when not competent, that there would be abuse (patient coercion)
• Multiple requirements: – two physicians with face to face evaluation– psychological evaluation if physician
believes judgment may be impaired– patient maintains control: may rescind
request, not fill prescription, not take medication and must self administer
• No convincing evidence for abuse

Arguments Against: Harmful Consequence #4Palliative Care Would Suffer
• Predicted that efforts to relieve symptoms of the terminally ill would decrease.
• Quality of Palliative Care in Oregon has increased since law’s passage– Physicians have made deliberate effort to improve
knowledge of PC (Ganzini et al 2000)– Forced a discussion of treatment options at end of
life– 90% of patients who use the law are on hospice
(Ganzini 2006, Oregon Health Authority and Washington Dept of Health)
– Inadequate palliative care is not a significant motivation for requesting aid in dying.

CAPC State Report Card on Access to Palliative Care
On the Day of a Death With Dignity
• Most have family and/or friends present– Sometimes a planned celebration– Often final words of love and appreciation– Rarely, only the patient and C&C
volunteers• Timing (median)• Ingestion to unconsciousness: 5 minutes• Ingestion to death: 25 minutes
• SCCA experience: families described deaths as “peaceful”
Journal of Palliative Medicine Volume 14, No 4, 2011

What Constitutes a Good Death?
• Symptom management• Treatment in accord with patient wishes• Psychological health• Spiritual and existential well-being• Social support• Experience of Death

Quality of Death and Dying (QODD) Questionnaire
• 31 Item questionnaire developed at the University of Washington
• Attempts to match patient preferences to reports from family members after death
• 4 domains: – symptom control– social connectedness– preparation for death– transcendence
• Highly validated
Curtis JR et al. Journal of Pain and Symptom Management Vol. 24 No.1 July 2002 p 17-31

What is the dying experience when patients use physician aid in dying?
• Interested in whether access to a lethal prescription helped patients meet their goals
• QODD given to 147 family members of Oregonians who died of a terminal illness between 2004 and 2007: – 52 patients who received lethal
prescriptions • 32 died as a result
– 32 patients who requested but did not receive prescriptions
– 63 non participants in the law (comparison group)
What is the dying experience when patients use physician aid in dying?
• Conclusions:– Connectedness & Transcendence: No significant
differences between groups– Symptom control: Better symptom control – Preparedness: More prepared
• Study limitations: – Retrospective assessment by family members– Sample size and possible selection bias

Mental Health Outcomes of Family Members of Those who use PAD
Journal of Pain and Symptom Management, December 2009
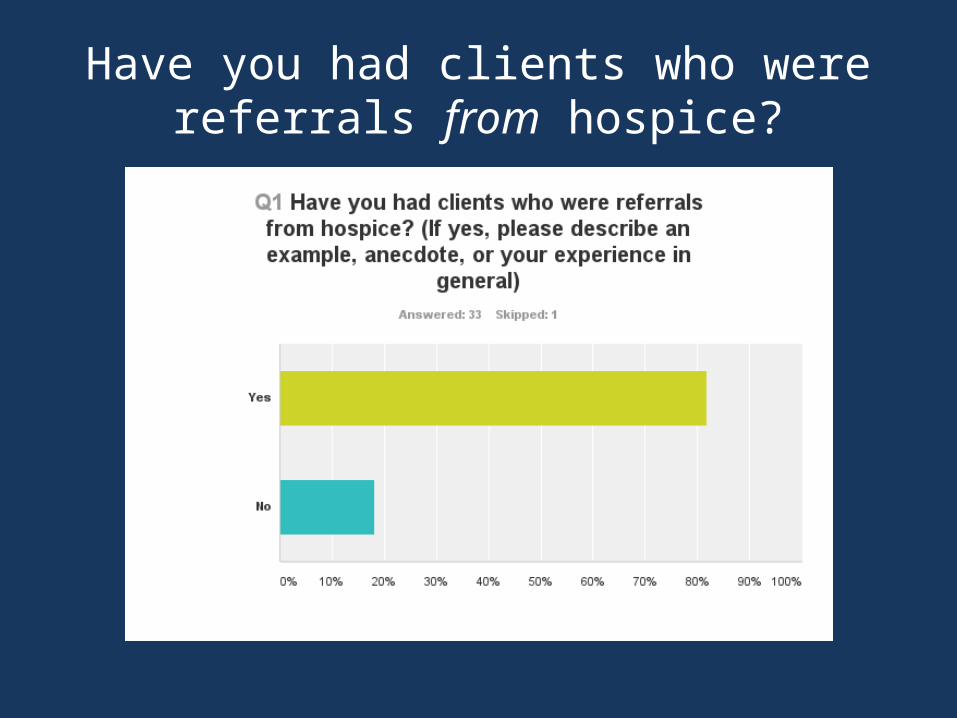
Have you had clients who were referrals from hospice?

Have you had clients who were referrals from hospice?
“We at Compassion and Choices of Oregon have had an exceptional relationship with many hospices in our State who referred their clients to us. WE appreciate the opportunity to collaborate with Hospice for it gives far more holistic care to our clients. “
“Most of our clients are either in hospice already or are referred to us by hospice. “
“Several referrals from hospice nurses and social workers with many different levels of involvement by hospice providers, from rather arms-length, to very intimate participation.”
“I've had patients referred by hospice social workers and hospice nurses. When we work as part of a care team, patients feel much more supported and receive better end of life care. “
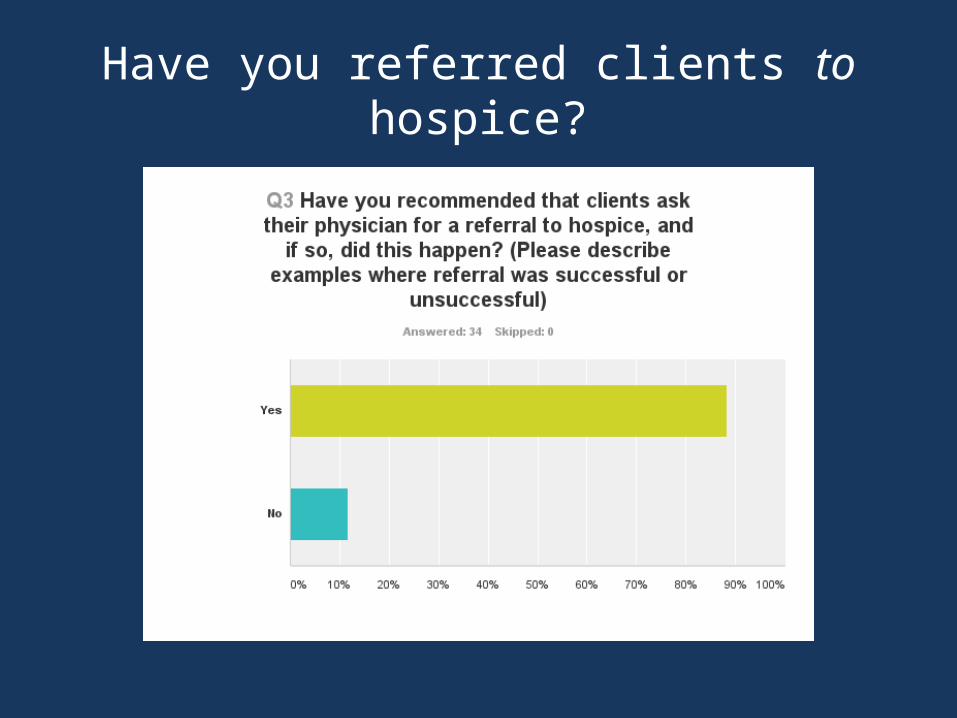
Have you referred clients to hospice?
Have you recommended that clients ask their physicians for a referral to hospice?
“All of our team members automatically talk with their clients about hospice on the first phone call (as does the intake person in Portland). It’s imperative that our clients make their EOL choice from a place of comfort vs. desperation. Most clients don’t realize the extent of services offered by hospice and thank us after experiencing the support they get.”
Have you recommended that clients ask their physicians for a referral to hospice?
“Every client I have been assigned I have done my best to get into hospice. As a former hospice nurse I know the benefits of being cared for by the hospice team. Unfortunately, not all clients understand or want to understand the gifts of hospice. I do my best to explain and tell them I was a hospice nurse.”

Have you perceived any barriers to getting your clients onto hospice?
Have you perceived any barriers to getting your clients onto hospice?
“Sometimes docs especially oncologists have a hard time acknowledging the deterioration and profound disability massive medical interventions cause for their clients and their loved ones. I have witnessed this for at least 30 years. It makes me so very sad to see this abuse and feel powerless to change it.”

Barriers to clients getting needed pain medications from hospice?

Barriers to clients getting needed pain medications from hospice?
“I'm a volunteer with Cascade Hospice in addition to volunteering with CCO. During my 12 years of hospice volunteering with 47 patients, I haven't encountered a case where a patient felt that they were being under-medicated for pain. “
“But there is the occasional patient who is intolerant of the "usually-prescribed" medications that hospice has to offer.”
“I've certainly worked with clients with horrible, unremitting, breakthrough pain. I've seen the frustration of hospice staff.”



Post-test1. Death with Dignity is also correctly known as
a.Assisted Suicideb.Physician-Assisted Deathc.Euthanasiad.Voluntary Euthanasia
2. Death with Dignity is legal ina.Oregon and Washington onlyb.Oregon, Washington and Californiac.Oregon, Washington, California and Coloradod.Oregon, Washington, Montana and Vermont
3. In the 17 years since it has been legal, DWD has been used by about how many people?e.1,000f. 10,000g.100,000
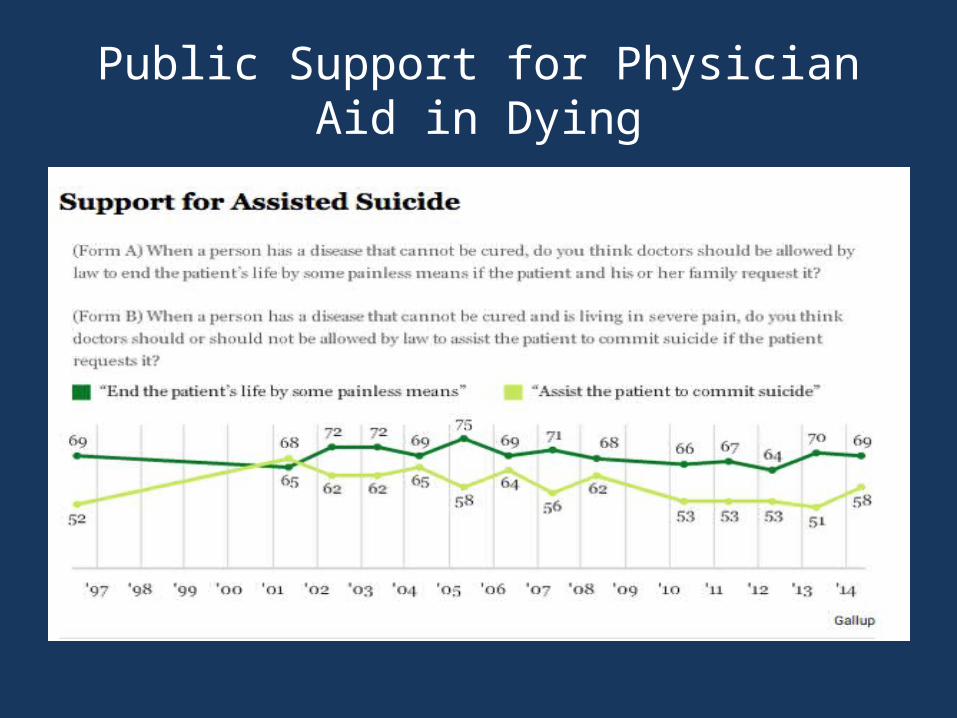
Public Support for Physician Aid in Dying
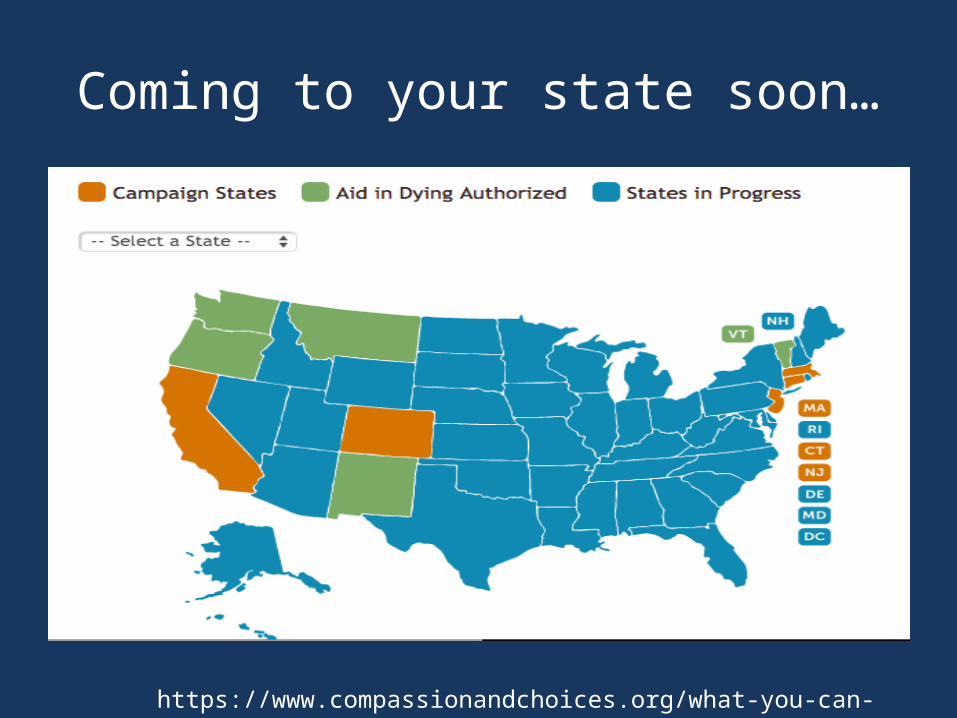
Coming to your state soon…
https://www.compassionandchoices.org/what-you-can-do/in-your-state/
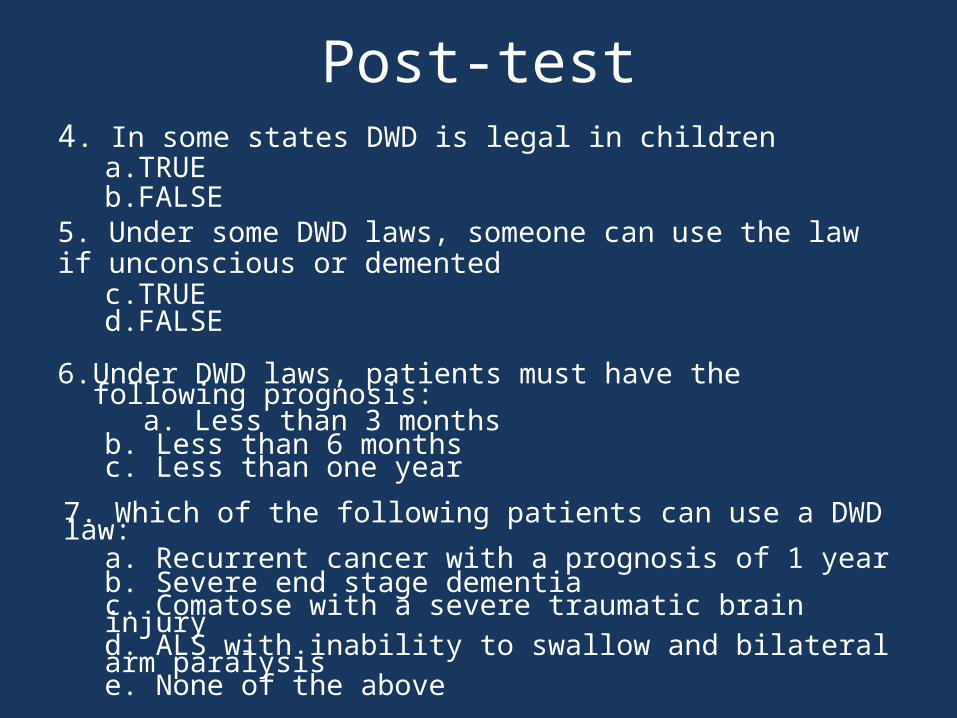
Post-test4. In some states DWD is legal in children
a.TRUEb.FALSE
5. Under some DWD laws, someone can use the law if unconscious or demented
c.TRUEd.FALSE
6. Under DWD laws, patients must have the following prognosis:
a. Less than 3 monthsb. Less than 6 monthsc. Less than one year
7. Which of the following patients can use a DWD law:a. Recurrent cancer with a prognosis of 1 yearb. Severe end stage dementiac. Comatose with a severe traumatic brain injuryd. ALS with inability to swallow and bilateral arm paralysis e. None of the above
Post-test8. If a patient has a terminal diagnosis,
decisional capacity and wishes to use DWD in a state where it is legal, s/he could get a prescription for life-ending medication 7 days after seeing an attending physician.a. TRUEb. FALSE
9. Most of the patients who use DWD do so due to intractable pain.a. TRUEb. FALSE
10.What percent of patients who use DWD are on hospice?a. 10%b. 50%c. 75%d. 90%
Resources• www.public.health.oregon.gov/ProviderPartnerResources/
EvaluationResearch/DeathwithDignityAct• http://www.doh.wa.gov/YouandYourFamily/IllnessandDisease/
DeathwithDignityAct• www.deathwithdignity.org• www.compassionandchoices.org• www.compassionwa.org• www.CAPC.org• Documentary film: How to Die in Oregon• Loggers,ET et al. N Engl J Med 2013;368:1417-24.• Stutsman, Eli, Political Strategy and Legal Change in Physician-Assisted Dying:
The Case for Palliative Care and Patient Choice.Johns Hopkins University Press. 2004.
• Smith, KA et al. The Quality of Death and Dying in Patients who Request Physician-Assisted Death. Journal of Palliative Medicine Volume 14, No 4, 2011.
Resources• Ganzini L et al. Oregonians’ reasons for requesting physician aid in dying, Arch
Intern Med 2009;169:489-492.• Ganzini L et al.Physicians experiences with the Oregon Death with Dignity Act,
NEJM 2000;342-557-563.• Ganzini L et al: Why Oregon patients request assisted death: Family members’
views. J Gen Intern Med 2007;23:154-157.• Ganzini L et al: Experiences of Oregon nurses and social workers with hospice
patients who requested assistance with suicide. NEJM 2002;347:582-588.• Ganzini L et al. Mental Health Outcomes of Family Members of Oregonians
Who Request Physician Aid in Dying. J Pain Symptom Manage 2009;38:807- 815.
• http://www.theatlantic.com/international/archive/2015/02/canada-supreme-court-revokes-ban-on-assisted-suicide/385247/
• Emanuel, E and Battin, M. What are the potential cost savings from legalizing physician-assisted suicide, NEJM 1998;339(3):167-171.
• Campbell C and Black M. Dignity, death, and dilemmas: a study of Washington hospices and physician-assisted death, J Pain & Symptom Management 2013

Valuable assistance by
Robb Miller, Patrick Long, Bob Wood and all of the client support volunteers of Compassion and Choices of WA
Matt Whitaker, Wendy Haile, David Grube and the client support volunteers of Compassion and Choices of OR
Jeff Beck of the University of Washington
The End
• Thank you for your attention• Please leave text answer sheets on your seat
or drop at the door• Questions?

The “All suffering can be relieved with good palliative care” argument
“Good palliative care can alleviate most suffering, but not all. Pain is usually easier to relieve than many other kinds of suffering, such as weakness, loss of bodily functions, shortness of breath and nausea. Moreover, sometimes the side effects of drugs used to palliate suffering are not acceptable to the patient…”Marcia Angell, How to Die in Massachusetts, New York Review of Books Feb.21,
2013

Cumulative Experience in OR and WA:Prescriptions Written and Deaths
State Oregon Washington Both Percentages
Years 1998-2013
2009-2013 21 state-years
-
Prescriptions written
1,173 547 1,720 -
Patients died after ingesting medication
752 359 1,111 65%(1,111/1,720)
Awoke 6 2 8 0.7%(8/1,111)
