understanding fatigue and an introduction to the facets programme
TRANSCRIPT

Dorset MS Service
Understanding fatigue and an introduction
to
the FACETS programmeAlison Nock, Vicky Slingsby, Occupational Therapists,
Dorset MS Service, Poole Hospital NHS Foundation Trust

Fatigue in multiple sclerosis
Most common symptom in MS
Up to 86% report current fatigue
Over 75% experience severe fatigue
50-60% consider fatigue to be one of three most troubling symptoms
Main cause of unemployment
Findings equivocal r.e. relationship to neurological impairment, neuropsychological performance, disease duration, disability, gender or age
Invisible nature can lead to misinterpretation/difficulties in personal and work relationships

Fatigue - invisible

Fatigue - challenges
Well, my family forget….I think they genuinely forget coz I just walk into the house as I
am. I haven’t got a label on my head they just forget all the
time & I just sit there & think “oh I’m so tired”
If you say you’ve got fatigue they
say “oh yeah I get tired”

I think I speak for everybody & say that we fight the problem every day. There is always a problem every day, isn’t
there?
I don’t think you can…..you can’t describe fatigue. It’s different every day, it’s
different for every part of your body.
I feel tired when I wake up every morning

you start a sentence and when you’re very
fatigued you can’t even remember how
you were going to end it and then you can’t remember how you
started it
when it really kicks in you just want to sit and do absolutely nothing. You don’t want to think, you don’t want to look at the television you don’t want to read, you just want to
stare into space

Definition of fatigue
“A subjective lack of physical and/or mental energy that is perceived by the individual or caregiver to interfere with usual or desired
activities”
(Clinical Practice Guidelines, 1998)

….it is much more than just being overly tired …It causes me to feel weak, light headed and nauseous, it affects my eyesight and causes my speech to slur and I find it impossible to concentrate on whatever I was doing. This can happen to me many times in a day and it is a lot worse if I become warm.
Anonymous, MS Society chat rooms

Fatigue is
identified as
a significant
problem
Multiple SclerosisPrimary Fatigue
Secondary Fatigue
Normal fatigue
EnvironmentPhysical
Social
Institutional
Cultural
Psychological
healthAnxiety
Stress
Depression
Other
Sleep
disordersPrimary
Secondary
Physical
healthComorbid
conditions
Drug side
effects
From MSC 1998

Primary fatigue

Secondary fatigue

Fatigue management
A means of facilitating coping behaviours via:
Education regarding both fatigue management principles as well as practical problem solving which aims to address fatigue
Requires a co-ordinated approach
Involves active participation of pwMS and by those in contact with the individual

Fatigue management
“a process by which the individual increases understanding of the factors which
contribute to & exacerbate his/her fatigue. Then through education & adaptation,
he/she learns to optimise function within the context of fatigue through goal setting
& the use of energy conservation strategies”
(Harrison 2007)

The ‘boom-and-bust’ pattern
‘Bad’ day
Activity
Time
‘Good’ day

Energy effectiveness techniques
Take frequent rests
Prioritise activities
Plan Ahead
Organise tools, materials and work areas
Adopt a good posture
Lead a healthy lifestyle and exercise

Putting it into practice
Common sense principles but need to put theory into practice
Daily/weekly record along with fatigue level
Identify baseline to work from
Build in routines
Adopt the right attitude for change, positive self talk and acceptance important to make changes
Support and communication

Self-management
How a chronic condition impacts upon daily life and the ways in which people can take greater control over their condition on a day-to-day basis
Self-management programmes can be specifically designed to reduce the severity of symptoms and improve confidence, resourcefulness and self-efficacy.
Source: Department of Health. The expert patient: a new approach to chronic disease management for the 21st century. London: DoH; 2001
Energy effectiveness
Energy effectiveness is a therapeutic
approach to planning daily activities and
finding more efficient ways of doing them.
Achieving a balance between activity and
rest is a central feature
It also can involve modifying the
environment

Over to you…….sharing experiences
What interventions are carried out in your practice?
Group vs. individual?
Resources used?
Evaluation/outcomes?

Introducing FACETS…..
Fatigue: Applying Cognitive
behavioural
and Energy effectiveness Techniques
to
lifeStyle

The research team
Professor Peter Thomas (Chief Investigator)Professor of HealthCare Statistics & Epidemiology School of Health and Social Care, Bournemouth University, UK
Dr Sarah ThomasSenior Research FellowSchool of Health and Social Care, Bournemouth University, UK
Dr Paula Kersten, Dr Rosie Jones (Principal Investigators)
Dr Charles Hillier, Mrs Alison Nock, Mrs Vicky SlingsbyDorset MS Service, Poole Hospital NHS Foundation Trust
Mrs Angela Davies Smith
Dr Colin Green, Professor Roger Baker, Professor Kate Galvin
Tim Worner, Geoff Linder (Service users)

Contributors
Ms Felicity Burgess - Recruitment
Dr Sara Demain - Delivered intervention
Mrs Caroline Birch - Delivered intervention
Ms Charlie Ewer-Smith - Delivered intervention
Dr Jo Kileff - Delivered intervention
Ms Jen Gash - Delivered intervention
Mrs Sheila Chartres - Delivered intervention
And all the participants in the trial.

Fatigue treatments - evidence
Drug treatments work for some but not all
(Sheng et al., 2013)
Energy effectiveness approaches of
moderate benefit in shorter term (Blikman et
al., 2013)
Cognitive behavioural therapy (CBT)
shown to be helpful in other conditions
(Chronic Fatigue Syndrome, Rheumatoid
arthritis)
Guiding principles
Blends cognitive behavioural (CB) & energy effectiveness approaches
Self-management
Delivered in groups
Manualised
Delivered by OTs, physiotherapists, nurses etc.
Easy to roll out in current health services

Phase 1
Developing FACETS
Phase 2
Trying out locally
locally Phase 3
3 centre pilot
Phase 4
RCT
Rolling out
FACETS

Theoretical underpinnings

Self-management
How a chronic condition impacts upon daily life and the ways in which people can take greater control over their condition on a day-to-day basis
Self-management programmes can be specifically designed to reduce the severity of symptoms and improve confidence, resourcefulness and self-efficacy.
Source: Department of Health. The expert patient: a new approach to chronic disease management for the 21st century. London: DoH; 2001

Self-efficacy
A person’s confidence in their ability to
accomplish a task or cope with a
challenging situation
Before I used to battle with it [fatigue],convinced that I could beat it . . . but since
taking this course I’ve realised that perhaps Ican’t beat it, I can manage it

Energy effectiveness approach
Energy effectiveness is a therapeutic
approach to planning daily activities and
finding more efficient ways of doing them.
Achieving a balance between activity and
rest is a central feature
It also can involve modifying the
environment

Cognitive behavioural approach
Is concerned with:
Individuals’ attitudes & ways of thinking (that’s the ‘cognitive’ part)
what they do (that’s the ‘behavioural’’ bit).
based on the theory that cognitions, emotions & behaviour interact and
that sometimes changing how we think about a situation influences what we feel and what we do.

Adapted from Padesky & Greenberger,
1995

Cognitive behavioural approach
Structured
Working in partnership
Uses problem solving
Helps people to gain insights into how they think, feel and behave
Can help people to explore other ways of thinking and behaving that might be more
helpful for managing fatigue

Objectives of FACETS
Normalise experience of fatigue
Use available energy more effectively
Develop “helpful thinking styles” about
fatigue

Structure of FACETS
Six sessions held weekly, 2 facilitators experience of MS and MS-fatigue, group work, CB
approaches
Closed group (8-10 participants)
Sessions build upon each other
1¾ hrs with refreshment break (*1st session =
2 hrs)

FACETS resources
Facilitator manual
PowerPoint slides
Participant workbook for each session
Handouts/signposts to relevant resources

− Describe the different types of fatigue
− Normalise the experience of fatigue
Homework: Activity diary & energy measure
− Introduce idea of budgeting energy− Describe how to establish rest/sleep/
activity routines
Homework: Rest/activity/sleep planner
− Describe components of activity− Introduce toolbox approach to activity
management
Homework: Setting realistic goals
− Explain fight/flight response− Ways of coping with stress− Introduce CB approach via example
Homework: Thought diary
− Describe unhelpful thinking styles− How to challenge unhelpful thoughts− Introduce concept of core beliefs
Homework: Thought challenge sheet
− Pull together programme components− Plan for setbacks, reframing them as a
learning experience
Homework: ‘Keeping on track’ planner

Reflections
Morning session
Timing
Venue important
Closed group, sessions build upon each
other
Maximum 10 people, first session involves
significant other
Funding

Our experiences
“It was good to hear real issues face-to-face
and have time/permission to talk about the
whole complex business of MS in a safe and
caring environment. The group helped me
feel relaxed and confident to speak about
anything. I have steered away from “groups”
and found online forums rather depressing -
this was a really positive experience!”

FACETS trial - design
–Pragmatic parallel arm multi-centre
randomised controlled trial
–FACETS plus current local practice
–versus
–Current Local Practice (CLP)

FACETS trial - aims
PRIMARY Does FACETS improve fatigue severity, self-efficacy, and MS-
specific quality of life?
SECONDARY Does FACETS improve fatigue impact, mood, general quality of
life, and activity patterns?
Is it cost-effective?
What are participants’ experiences? What changes have they
made? What barriers to change were encountered?
Helpful/unhelpful aspects?
FACETS trial - eligibility
Inclusion criteria Diagnosis of MS
Significant fatigue (impacting on daily life)
Ambulatory
Exclusion criteria Non-English speaking
Relapse within past 3 months
Recently started disease modifying drug or anti-depressants
Cognitive deficits ruling out group participation
Under the care of psychiatrist or addiction services
FACETS trial - outcomes
FATIGUEFatigue Assessment Instrument FAI]Fatigue Symptom Inventory [FSI]
SELF-EFFICACYFatigue Self-Efficacy Scale [FSE](control subscale)
QUALITY OF LIFEMS Impact Scale [MSIS-29]MO Short-Form 36 [SF-36]EuroQol 5-Dimensions [EQ-5D-3L]
MOODHospital Anxiety & Depression Scale [HADS]
Fatigue Management Strategies
Questionnaire (FMSQ)ActivPAL™ tri-axial accelerometer

1 month follow-up (n=75) 94%
Given information pack
FACETS + UC (n=84)Received ≥4 sessions (n=72)
USUAL CARE (n=80)
1 month follow-up (n=71) 85%
4 month follow-up (n=70) 83% 4 month follow-up (n=74) 93%
ExcludedIneligible (n=112)Declined (n=142)
Waiting list (n=34)
12 month follow-up (n=62) 74% 12 month follow-up (n=69) 86%
Randomised (n=164)stratified by centre
INCLUSION CRITERIA:
Diagnosis of MS; significant fatigue; ambulatory
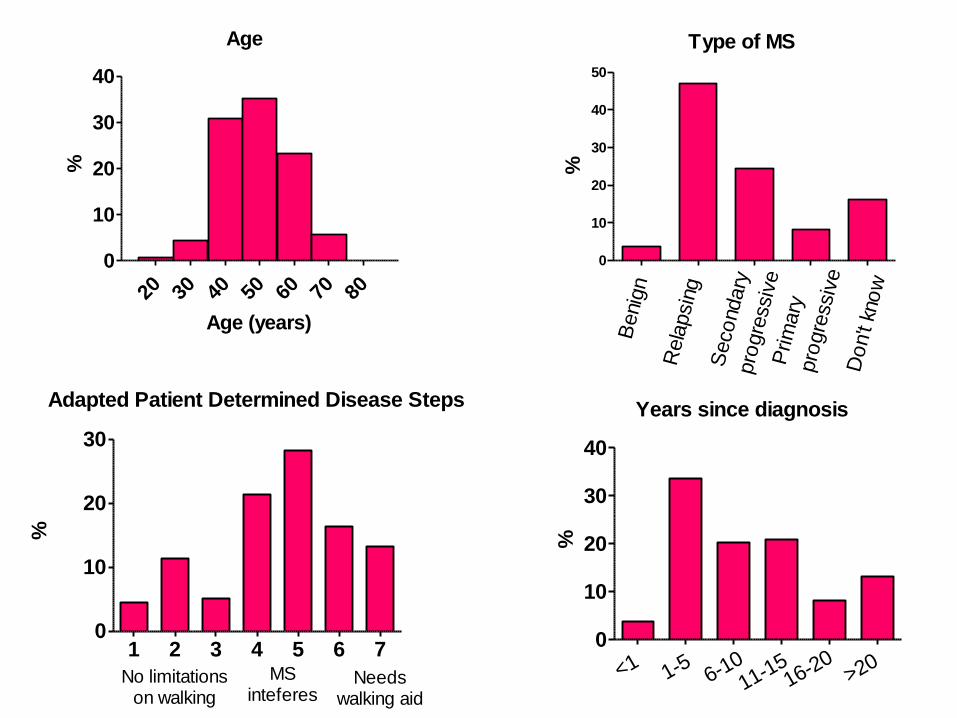
Age
20 30 40 50 60 70 80
0
10
20
30
40
Age (years)
%
Type of MS
0
10
20
30
40
50
Benig
n
Rela
psin
g
Seco
ndary
pro
gre
ssiv
e
Do
n't
kno
w
Prim
ary
pro
gre
ssiv
e
%
Adapted Patient Determined Disease Steps
1 2 3 4 5 6 70
10
20
30
No limitationson walking
MSinteferes
Needswalking aid
%
Years since diagnosis
0
10
20
30
40
<1 1-5 6-1011-15
16-20>20
%
-15
-10
-5
0
5
10
15
1 mth 4 mths 12 mths
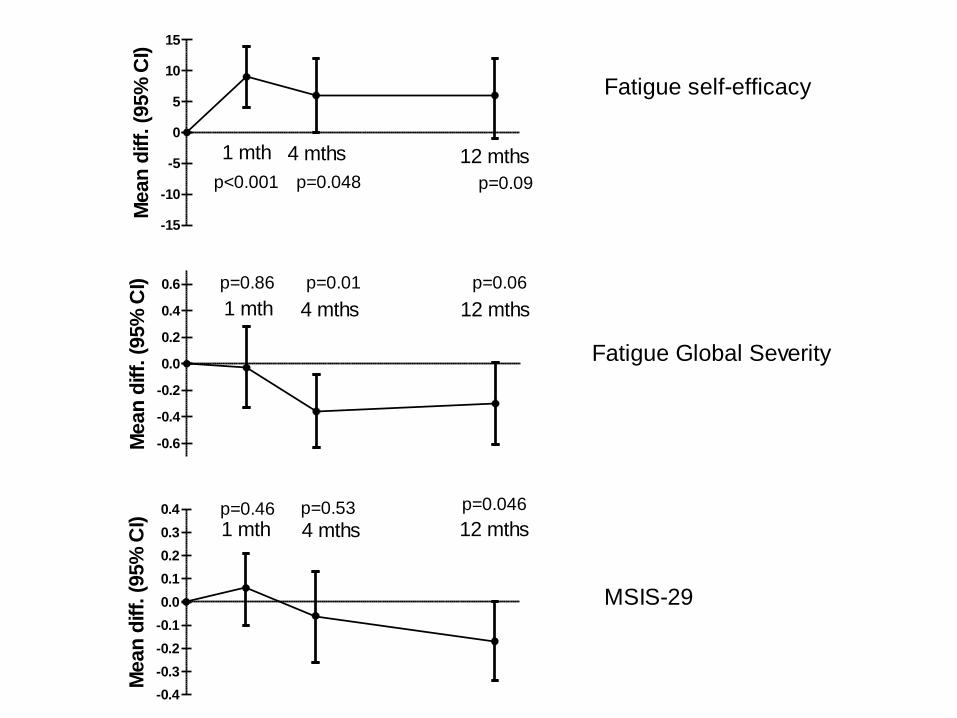
Fatigue self-efficacy
p<0.001 p=0.048 p=0.09
Mean
diff.
(95%
CI)
-0.6
-0.4
-0.2
0.0
0.2
0.4
0.6
1 mth 4 mths 12 mths
Fatigue Global Severity
p=0.86 p=0.01 p=0.06
Mean
diff.
(95%
CI)
-0.4
-0.3
-0.2
-0.1
0.0
0.1
0.2
0.3
0.4
1 mth 4 mths 12 mths
MSIS-29
p=0.46 p=0.53 p=0.046
Mean
diff.
(95%
CI)

Secondary outcomes
Significant Not Significant
SF-36 Vitality (4 mths) Other SF-36 subscales
Fatigue Symptom Inventory- average fatigue (1 & 4 mths)- current fatigue (1 mth)
Fatigue Symptom Inventory- most fatigued- least fatigued- interference with activities
Hospital Anxiety and Depression Scale
ActivPAL™ - energy expenditure

80 78 78 7571
66 6359 58 55
49
0
10
20
30
40
50
60
70
80
90
%Fatigue management strategies
used at 4 months

Economic evaluation
Cost of FACETS £453 per patient (~50% facilitation)
No significant difference in Quality Adjusted Life Years (QALYs): FACETS 0.26 v CLP 0.31 (p=0.31)
Cost of £1,259 per unit reduction in fatigue severity(or in a more policy-relevant context £2,157 per additional person with a clinically significant improvement in fatigue (GFS)).
No significant difference in health and social care costs over 3 months: [FACETS £218 v CLP £265]
Uncertainty around cost-effectiveness

Conclusions
FACETS has small-to-medium effect sizes
By 1 month follow-up, improved self-efficacy (MS-FSE)
By 4 months follow-up, reduced fatigue severity (FSS)
By 12 months follow-up, improved quality of life (MSIS-29)
Inexpensive
Designed to be easily incorporated into practice
Update
FACETS has been translated into French,
Norwegian, and German
One year follow-up paper published (BMC
Neurology)

Phase 1
Developing FACETS
Phase 2
Trying out locally
locally Phase 3
3 centre pilot
Phase 4
RCT
Rolling out
FACETS

Roll out - the manual
MS Society has supported design and production of facilitator manual and participant materials

Roll out - training courses
MS Society supporting/organising one day FACETS training courses for health professionals (HPs)– Delivered by Alison Nock and Vicky Slingsby– To date, 123 HPs trained (London, Glasgow,
Manchester, Belfast, Bristol and Bradford)

ReferencesThomas S, Kersten P, Thomas PW. The Multiple Sclerosis-Fatigue Self-Efficacy (MS-FSE) Scale: initial validation. Clin Rehabil. 2014 Aug 26. DOI: 10.1177/0269215514543702 [Epub ahead of print]
Thomas PW, Thomas S, Kersten P, Jones R, Slingsby V, Nock A,Davies Smith A, Baker R, Galvin KT, Hillier C.Oneyear follow-up of a pragmatic multi-centre randomised controlled trial of a group-based fatigue managementprogramme (FACETS) for people with multiple sclerosis. BMC Neurol 2014; 14:109
Thomas S, Kersten P. Fatigue, FACETS and future directions for fatigue management. Int J Ther Rehabil 2014; 21,57.
Thomas S, Thomas PW, Kersten P et al., A pragmatic parallel arm multi-centre randomised controlled trial toassess the effectiveness and cost-effectiveness of a group-based fatigue management programme (FACETS) forpeople with multiple sclerosis. J Neurol Neurosurg Psychiatry Published Online First: [10 July 2013]doi:10.1136/jnnp-2012-303816
Thomas PW, Thomas S, Kersten P, et al. Trial Protocol: Multi-centre parallel arm Randomised controlled trial to assess the
effectiveness and cost-effectiveness of a group-based cognitive behavioural approach to managing fatigue in people with
multiple sclerosis BMC Neurol 2010;10:43. Doi:10.1186/1471-2377-10-43.
Thomas S, Thomas PW, Nock A, et al. Development and preliminary evaluation of a cognitive behavioural approach to
fatigue management in people with multiple sclerosis. Patient Educ Couns 2010;78;204-210.
Thomas S, Thomas P, Nock V, Slingsby V, Galvin K, Baker R, Moffat N, Hillier C. Development and preliminary evaluation of a
fatigue management programme for People with multiple sclerosis. Mult Scler 007;13: S7-S273.
Thomas PW, Thomas S, Hillier C, Galvin K, Baker R. Psychological interventions for multiple sclerosis. Cochrane