understanding how we are wired and explaining why ... - appd · disclosure •none of the...
TRANSCRIPT
Understanding How We Are Wired and Explaining Why We Short Circuit:
A Workshop in Medical Decision Making and Error
Emily Ruedinger, MD University of Washington
Andrew Olson, MD
University of Minnesota
Maren Olson, MD, MPH University of Minnesota
Emily Borman-Shoap, MD University of Minnesota

Disclosure
• None of the presenters have any relevant conflicts of interest
• But we do all have experience making errors.
• This work is supported by a Clinical Innovations Award from the AAMC

Schedule
• 2:00-2:30: Introduction
• 2:30-3:00: Small Group Case Discussion
• 3:00-3:30: Large Group Debrief
• 3:30-4:00: Implementation/Q&A

All men make mistakes…
- Winston Churchill
It is the nature of medicine that you are
gonna screw up.
- Dr. House
creativecommons.org/licenses/by-nc-sa/2.0/
All men make mistakes…
…but only wise men learn from their mistakes.
-Winston Churchill
Objectives
By the end of the workshops, attendees will: • Gain the knowledge needed to help trainees reflect
on their own decision making and identify cognitive errors
• Practice reviewing clinical experiences in which diagnostic errors occurred and trial techniques to help trainees collaboratively identify strategies to avoid these errors.
• Develop the skills to promote trainees’ involvement in constructive, non-judgmental feedback when an error occurs.

Curriculum Overview
• Series of 5 modules focused on teaching concepts of medical decision making and diagnostic error to residents
• We conducted sessions during 3 block education sessions.
• Modules adaptable to 60-90 minutes and single or contiguous sessions.

Modules
Module 1: Introduction to Medical Decision-Making and Diagnostic Error Module 2: Faculty Panel Discussion about Diagnostic Error Module 3: Case Studies in Diagnostic Error Module 4: Personal and Small Group Reflection on Diagnostic Error Module 5: Feedback Training- How to Discuss Diagnostic Error with Colleagues
Let’s start with an example
A I3 C 12 I3 14 Ann
approached the bank.

You made a choice
but didn’t know it

Image retrived on 31Oct2014 from: https://www.flickr.com/photos/frosch50/14918770014/in/photolist-oJjAyE-eWuKqB-fF3USJ-nojk2G-frnrgV-9jUgw7-hSotFA-azQDSa-fbuCv9-h6yodi-nDmXPb-fvyxkm-ntPSq1-6SHqu1-gSNm9a-9pbx2i-nwXBch-eS7wQV-mTSDjr-f3LvGM-cHqmeo-nxixzv-514qBV-fBf1RX-fG117a-bn6xge-n42iez-bDTQAB-kB8TCg-ahRkyL-fF3WxE-fSfM5c-88ZggE-62aLHE-jACgcQ-J7y6F-fA2Mia-k2Nuaa-mRNisn-hAPAMT-9v7FUg-eTz1hS-jDXD6F-8ZMjnZ-atmnDa-iPwU34-FgLJd-fZ59PV-9mAAqx-f6d6FqCreative Commons License associated: https://creativecommons.org/licenses/by/2.0/

Heuristics
Automatic shortcuts we use in response to familiar scenarios
(Think about the last time you went to work)
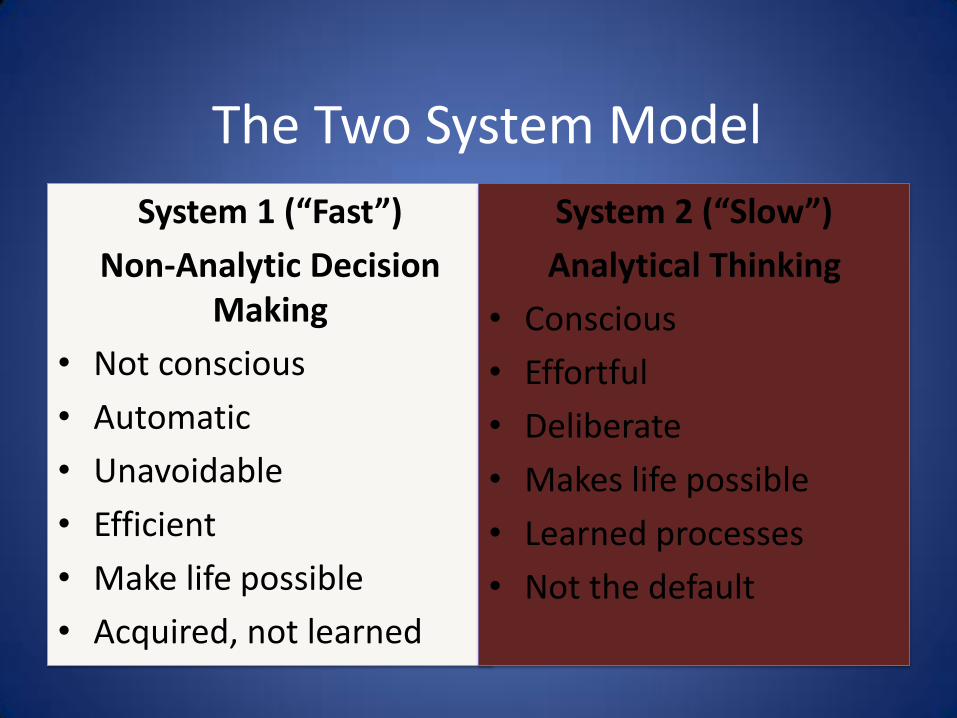
The Two System Model
System 1 (“Fast”)
Non-Analytic Decision Making
• Not conscious
• Automatic
• Unavoidable
• Efficient
• Make life possible
• Acquired, not learned
System 2 (“Slow”)
Analytical Thinking
• Conscious
• Effortful
• Deliberate
• Makes life possible
• Learned processes
• Not the default
Pneumonia

Bronchiolitis

Kartagener Syndrome
Reflect on the ways you see your learners practicing diagnostic reasoning: When to they practice System 1 (non-analytic, fast) decision making? When do they practice System 2 (analytic, slow) thinking? When is this appropriate or inappropriate?
Cognitive Biases
When the diagnosis is made, the thinking stops Premature Closure
Locking into salient features of a patients’ initial presentation and failing to adjust your impression in light of later information
Anchoring Bias

Judging things as more likely if they readily come to mind Availability

How we see things is strongly influenced by the way a problem is framed.
Framing Effect
Statistics presented about surgical treatment for lung cancer
“1 month survival rate = 90%”
“10% mortality in the first month”
84% chose surgery
50% chose surgery
Once a diagnostic label is attached to a patient, it becomes stickier and sticker.
Diagnostic Momentum

Emotional responses, stereotypes, assumptions
Visceral Biases

Deferring to an “authority” and following along without
thinking for oneself or challenging the authority
Blind Obedience
Think about a case that didn’t go well. What biases were at play?
• Premature Closure
• Anchoring Bias
• Availability
• Framing
• Diagnostic momentum
• Visceral Bias
• Blind obedience

HTTPS://WWW.YOUTUBE.COM/WATCH?V=YNSJAF8NON0

Diagnostic errors: “any mistake or failure in the diagnostic process leading to an incorrect diagnosis, a missed diagnosis or delayed diagnosis.” Overdiagnosis in an asymptomatic patient
Reilly JB, Ogdie AR, Von Feldt JM, Myers JS. Teaching about how doctors think: a longitudinal curriculum in cognitive bias and diagnostic error for residents. BMJ Qual. Saf. 2013.

31
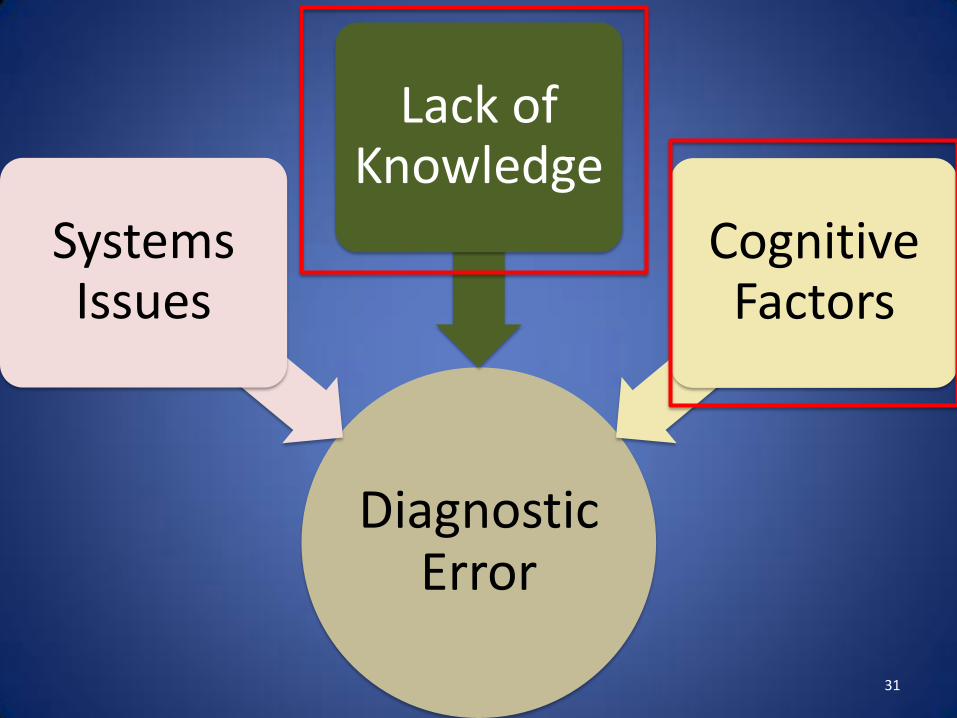
Diagnostic Error
Systems Issues
Lack of Knowledge
Cognitive Factors
32
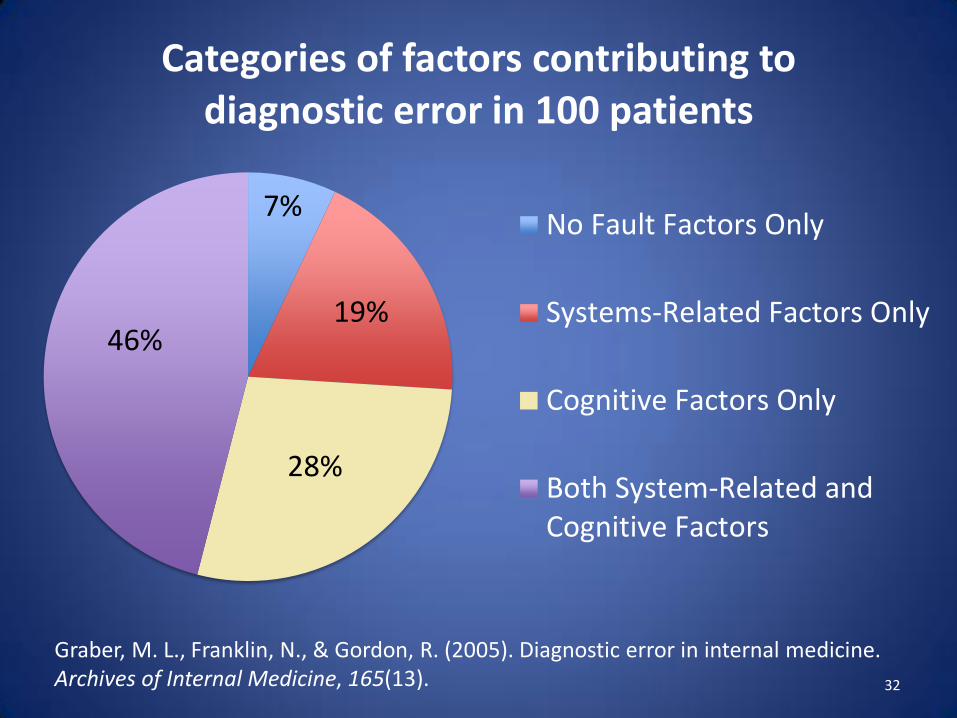
7%
19%
28%
46%
Categories of factors contributing to diagnostic error in 100 patients
No Fault Factors Only
Systems-Related Factors Only
Cognitive Factors Only
Both System-Related andCognitive Factors
Graber, M. L., Franklin, N., & Gordon, R. (2005). Diagnostic error in internal medicine. Archives of Internal Medicine, 165(13).

83%
14%
3%
Cognitive Contributions to Error
Faulty Synthesis of Informationor Flawed Processing
Faulty Data Gathering
Inadequate or FaultyKnowledge
Graber, M. L., Franklin, N., & Gordon, R. (2005). Diagnostic error in internal medicine. Archives of Internal Medicine, 165(13).
Cognitive errors are defined as errors related to the way we think
and make diagnostic and treatment decisions.
Reilly JB, Ogdie AR, Von Feldt JM, Myers JS. Teaching about how doctors think: a longitudinal curriculum in cognitive bias and diagnostic error for residents. BMJ Qual. Saf. 2013.
Residents need this.
Survey conducted of our residents in 2013: • 75% think it is important to disclose cognitive errors to patients and
families • 90% think it is important to discuss cognitive errors with attendings • 98% believe that reducing cognitive errors will improve patient
safety. • Only 54% had seen discussion of cognitive error modeled by their
attendings.
• Only 31% felt encouraged by their supervisors to discuss cognitive errors
• Residents who were encouraged by their attendings to discuss cognitive errors were more likely to be aware of error reduction strategies (42 vs 18%, p<0.05)
Yee, Ruedinger and Olson
Group Exercise
• Divide into groups
• Read the case and then answer the questions that follow
• Put yourself in the team’s shoes
Choosing a New Curriculum
• Why now?
• How will it fit?
• Sustainability?
• Downstream and upstream support?
• Synergies?
Diagnostic Error Curriculum at Your Institution
• Take a few minutes at your table to discuss how this content could fit in
– Key faculty and institutional champions
– Likely settings
– Opportunities/Threats
– Outcomes you might track
Cognitive Bias Curriculum at University of Minnesota
• Key Faculty—Andrew Olson, Emily Ruedinger, Maren Olson
• Block education and morning reports
• Outcomes
Thank you for coming today!
z.umn.edu/diagnosticerror