universidade federal de pelotas faculdade de...
TRANSCRIPT
1
UNIVERSIDADE FEDERAL DE PELOTAS
Faculdade de Odontologia
Programa de Pós-Graduação em Odontologia
Dissertação
Restauração de lesões cervicais não cariosas: fatores relacionados a sua
sobrevivência e impactos periodontais
Morgana Favetti
Pelotas, 2017
2
Morgana Favetti
Restauração de lesões cervicais não cariosas: fatores relacionados a sua
sobrevivência e impactos periodontais
Dissertação, apresentada ao Programa de Pós-Graduação em Odontologia da Faculdade de Odontologia da Universidade Federal de Pelotas, como requisito parcial à obtenção do título de Mestre em Odontologia, área de concentração em Dentística.
Orientador: Prof. Dr. Maximiliano Sérgio Cenci
Co-orientador: Prof. Dr. Thiago Marchi Martins
Co-orientadora: Profa. Dra. Anelise Fernandes Montagner
Pelotas, 2017
your
read
er’s
atte
ntio
n
with
a
grea
t
quot
e
from
the
doc
ume
nt or
use
this
spac
e to
emp
hasi
ze a
key
poin
t. To
plac
e
this
text
box
any
whe
re
on
the
Universidade Federal de Pelotas / Sistema de BibliotecasCatalogação na Publicação
F273r Favetti, MorganaFavRestauração de lesões cervicais não cariosas : fatoresrelacionados a sua sobrevivência e impactos periodontais /Morgana Favetti ; Maximiliano Sergio Cenci, orientador ;Thiago Marchi Martins, Anelise Fernandes Montagner,coorientadores. — Pelotas, 2017.Fav112 f. : il.
FavDissertação (Mestrado) — Programa de Pós-Graduaçãoem Dentística, Faculdade de Odontologia, UniversidadeFederal de Pelotas, 2017.
Fav1. Ensaio clinico controlado randomizado. 2. Lesõescervicais não cariosas. 3. Restauração dental permanente.4. Recessão gengival. 5. Sistema adesivo. I. Cenci,Maximiliano Sergio, orient. II. Martins, Thiago Marchi,coorient. III. Montagner, Anelise Fernandes, coorient. IV.Título.
Black : D2

Elaborada por Fabiano Domingues Malheiro CRB: 10/1955

3
Morgana Favetti
Restauração de lesões cervicais não cariosas: fatores relacionados a sua sobrevivência e impactos periodontais
Dissertação aprovada, como requisito parcial, para obtenção do grau de Mestre em Odontologia, Programa de Pós-Graduação em Odontologia, Faculdade de Odontologia de Pelotas, Universidade Federal de Pelotas. Data da defesa: 21/02/2017 Banca examinadora: Prof. Dr. Maximiliano Sérgio Cenci Doutor em Odontologia, área de concentração em Cariologia pela Universidade Estadual de Campinas. Prof. Dr. Mauro Elias Mesko Doutor em Odontologia, área de concentração em Dentística Restauradora, pela Universidade Federal de Pelotas. Prof. Dra. Patrícia Daniela Melchiors Angst Doutora em Clínica Odontológica, área de concentração em Periodontia pela Universidade Federal do Rio Grande do Sul. Prof. Dr. Fábio Herrmann Coelho de Souza (suplente) Doutor em Odontologia, área de concentração em Dentística pela Universidade Federal de Pelotas. Prof. Dra. Gabriela Romanini Basso (suplente) Doutora em Odontologia, área de concentração em Materiais Odontológicos pela Universidade Federal de Pelotas.
4
Agradecimentos
À Universidade Federal de Pelotas e à Faculdade de Odontologia, por
todo acolhimento e aprendizado desde a Graduação;
Ao Programa de Pós-Graduação em Odontologia, aos seus
professores, e seu coordenador Prof. Dr. Rafael Ratto Moraes, exemplos de
competência a serem seguidos;
Ao meu Orientador Prof. Dr. Maximiliano Sergio Cenci, pela
oportunidade que por ele me foi concedida de fazer parte do PPGO-UFPel
através de sua orientação atenta e competente, sempre incentivando meu
crescimento acadêmico e pessoal.
Ao meu Co-Orientador Prof. Dr. Thiago Marchi Martins, um grande
exemplo de docente e ser humano, pelos importantes conhecimentos
transmitidos.
À minha Co-Orientadora Prof. Dra. Anelise Fernandes Montagner, pelo
carinho e atenção, sempre disposta a ajudar e contribuir com o que fosse
preciso.
Ao Prof. Dr. Alexandre Severo Masotti, que através de sua colaboração
e disponibilidade no processo de avaliação dos pacientes, permitiu que este
trabalho pudesse ser executado com maestria.
À Prof. Dra. Silvia Terra Fontes, que gentilmente compartilhou conosco
os pacientes e sua tese de doutorado, para que pudéssemos dar continuidade à
coleta de dados e acompanhamento destes pacientes.
Àos meus colegas e amigos de Graduação e agora, de Pós-Graduação
Aryane, Andressa Spohr, Andressa Gastmann e Victório. Gratidão, por
fazerem parte dessa jornada, pelo apoio e pela amizade. Foi um grande prazer
compartilhar esse período da minha vida com vocês;
A todas os pacientes, participantes do estudo, pois sem eles este trabalho
não estaria acontecendo;
Aos meus pais, Ivete e Reini, que serão sempre um exemplo de força,
confiança, dedicação e amor. Por estarem sempre presentes e me fornecerem
o suporte necessário. Se eu cheguei até aqui, foi porque vocês estavam sempre

5
à frente abrindo meus caminhos e apoiando minha trajetória rumo ao
cumprimento de meus objetivos e sonhos;
Ao meu namorado e melhor amigo Lucas, obrigado pela compreensão,
companheirismo e apoio. Teu carinho e tua companhia foram essenciais para
tornar meus dias mais leves;
À todos que diretamente ou indiretamente participaram e contribuíram
com minha formação, o meu sincero muito obrigada!
6
Notas Preliminares
A presente dissertação foi redigida segundo o Manual de Normas para
Dissertações, Teses e Trabalhos Científicos da Universidade Federal de Pelotas
de 2013, adotando o Nível de Descrição 3 – estrutura em Capítulos não
convencionais, descrita no Apêndice do referido manual.
<http://sisbi.ufpel.edu.br/?p=documentos&i=7> Acesso em: 21/11/2016.
O projeto de pesquisa contido nesta dissertação é apresentado em sua
forma final após qualificação realizada em 3 de Setembro de 2015 e aprovado
pela Banca Examinadora composta pelos Professores Doutores Fábio Garcia
Lima, Natália Marcumini Pola e Mauro Elias Mesko (Suplente).
7
Resumo
FAVETTI, Morgana. Restauração de lesões cervicais não cariosas: fatores relacionados a sua sobrevivência e impactos periodontais. 2017. 112p. Dissertação Mestrado em Odontologia – Programa de Pós Graduação em Odontologia. Universidade Federal de Pelotas, Pelotas, 2017. O presente estudo teve como objetivo avaliar os aspectos de sobrevida de restaurações diante das intervenções propostas por dois ensaios clínicos randomizados com tempos de acompanhamento diferentes, um com 36 meses e outro com 60 meses. Adicionalmente, objetivou-se avaliar a condição periodontal de pacientes que receberam restaurações em lesões cervicais não cariosas (LCNC) nestes estudos. O estudo com 36 meses de acompanhamento (Número de pacientes - Np = 42; Número de restaurações -Nr= 182), foi realizado com 3 diferentes grupos, nos quais aplicavam-se diferentes soluções (controle - solução placebo, experimental 1 - solução de clorexidina 2%, e experimetal 2 - solução de hipoclorito de sódio 10%) durante 60 segundos após o condicionamento ácido e antes da aplicação do adesivo e da restauração das LCNC. Sendo assim, este primeiro estudo deu origem à 2 estudos (estudo 1 e 2), respectivamente sobre os efeitos do pré-tratamento com CHX 2% e NaOCl 10% na retenção de restaurações em LCNCs. O estudo com 60 meses de acompanhamento (Np = 36; Nr = 172) deu origem ao estudo 3, sendo que este foi desenvolvido para avaliar o efeito de diferentes formas de isolamento do campo operatório (isolamento absoluto - com dique de borracha e grampo, ou isolamento relativo - com fio retrator, afastador labial, e ambos com sugador de saliva) para a realização de restaurações de LCNC. Um avaliador experiente, treinado e calibrado em cada um dos dois grandes estudos, avaliou as restaurações após 6, 12, 24, 36 ou 60 meses utilizando os critérios da FDI. Para a avaliação periodontal, um mesmo avaliador, padrão ouro, para ambos os estudos, avaliou os casos seguindo critérios pré-estabelecidos. Outro pesquisador comparou as informações obtidas com as já existentes nas fichas clínicas dos pacientes com as que foram obtidas no exame clínico e na aplicação do questionário realizados nos últimos recalls de cada estudo, de 3 ou 5 anos. A união dos dados periodontais oriundos das duas amostras, deu origem à um quarto estudo, que representa a associação entre os aspectos relacionados às restaurações (nível da margem e tipo de isolamento) e os tecidos periodontais adjacentes. Os resultados demostraram que a utilização de diferentes soluções, como clorexidina 2% ou hipoclorito de sódio 10%, durante o processo restaurador, bem como o tipo de isolamento realizado durante a execução do tratamento restaurador, não influenciaram a taxa de sobrevida das restaurações de LCNC ao longo do tempo. Ainda, do ponto de vista periodontal, o tipo de isolamento e a presença das restaurações não demonstraram gerar dano aos critérios periodontais avaliados após acompanhamento de 36 ou 60 meses. Houve relevante associação de determinadas características das lesões e dos pacientes com as taxas de falhas das restaurações. Palavras-chave: Sistema adesivo, ensaio clínico controlado randomizado, restauração dentária permanente, lesões cervicais não cariosas, recessão genvival.

8
Abstract
FAVETTI, Morgana. Restoration of non-carious cervical lesions: factors related to their survival and periodontal impacts. 2017. 112p. Dissertation (Master degree in Dentistry). Graduate Program in Dentistry. Federal University of Pelotas, Pelotas, 2017.
The present study had as objective to evaluate the survival aspects of restorations before the interventions proposed by two randomized clinical trials with different times of follow-up, one with 36 months and another with 60 months. Additionally, the aim of this study was to evaluate the periodontal condition of patients who received non-carious cervical lesion restorations (NCCL) in these studies. The study with 36 months of follow-up (Number of patients - Np = 42; Number of restorations -Nr = 182) was performed with 3 different groups, in which different solutions were applied (control - placebo solution, experimental 1 - solution of Chlorhexidine 2%, and experimental 2 - 10% sodium hypochlorite solution) for 60 seconds after acid etching and before application of the adhesive and restoration of NCCL. Thus, this first study gave rise to two studies (study 1 and 2), respectively, on the effects of pretreatment with CHX 2% and NaOCl 10% on the retention of NCCL restorations. The study with 60 months of follow - up (Np = 36; Nr = 172) gave rise to study 3, which was designed to evaluate the effect of different forms of isolation of the operative field (absolute isolation - with rubber dam and clamp, Or relative insulation - with retractor wire, lip retractor, and both with saliva succion) for performing NCCL restorations. An experienced, trained and calibrated evaluator in each of the two large studies evaluated the restorations after 6, 12, 24, 36 or 60 months using the FDI criteria. For the periodontal evaluation, the same gold standard evaluator for both studies evaluated the cases according to pre-established criteria. Another researcher compared the information obtained with the already existing ones in the clinical records of the patients with those obtained in the clinical examination and in the application of the questionnaire carried out in the last recalls of each study, of 3 or 5 years. The union of the periodontal data from the two samples gave rise to a fourth study, which represents the association between aspects related to restorations (margin level and type of isolation) and adjacent periodontal tissues. The results demonstrated that the use of different solutions, such as 2% chlorhexidine or 10% sodium hypochlorite, during the restorative process, as well as the type of isolation performed during the restorative treatment, did not influence the survival rate of NCCL over time. Also, from the periodontal point of view, the type of insulation and the presence of the restorations did not show damage to the periodontal criteria evaluated after 36 or 60 months follow up. There was a relevant association between certain characteristics of the lesions and the patients with the failure rates of the restorations. Key-words: adhesive system, randomized controlled trial, dental restoration
permanent, noncarious cervical lesions, gingival recession.
9
LISTA DE ABREVIATURAS E SIGLAS
et al.
e outros
FO
Faculdade de Odontologia
IPV
Índice de Placa Visível
ISG
Índice de Sangramento Gengival
UFPel Universidade Federal de Pelotas
LCNC NG
Lesões Cervicais não cariosas Nível Gengival
mm Milímetro PS Profundidade de Sondagem CRX Clorexidina NaOCl
Hipoclorito de Sódio
NCCL
Non Carious Cervical Lesions
10
Sumário
Resumo.................................................................................................. 7
Abstract.................................................................................................. 8
1 Introdução ......................................................................................... 11
2 Capítulo 1: Effectiveness of pre-treatment with chlorhexidine in
restoration retention: a 36-month follow-up randomized clinical
trial…………………………………………………………………………….
15
3 Capítulo 2: Effect of sodium hypochlorite pre-treatment on the
retention of restorations for non-carious cervical lesions: a 3-year
randomized controlled trial…………………………………………….…
30
4 Capítulo 3: Retention of non-carious cervical restorations placed
under rubber dam or cotton rolls isolation: 60 months follow-up
of a randomized controlled clinical trial ………………………………..
5 Capítulo 4: Effects of cervical restorations on the periodontal
tissues……………………………………………………...……………...
50
69
6 Considerações finais........................................................................ 88
Referências .......................................................................................... 89
Apêndices ............................................................................................ 94
Anexos ................................................................................................. 110
11
1 Introdução
Restaurações de lesões cervicais não cariosas (LCNC) são tratamentos
desafiadores, tanto pela longevidade, quanto pelo íntimo contato que possuem
com os tecidos periodontais. A procura por este tipo de tratamento ocorre
principalmente por questões estéticas e de sensibilidade dentinária. Esse
mecanismo de dor, que impulsiona o paciente a procurar ajuda do cirurgião
dentista, é melhor explicado pela teoria hidrodinâmica, sendo que tanto o início
quanto a progressão da sensibidade dentinária são influenciados pelas
características dos dentes, do periodonto, do ambiente oral e de influências
externas (WEST et al., 2013).
O aparecimento de LCNC é tido como um evento multifatorial, onde
diversas características do meio influenciam. A perda de esmalte e dentina pode
ser devido a qualquer combinação dos processos de desgaste dos dentes, como
abrasão, erosão ou abfração. A interação entre erosão e abrasão parece ser o
maior responsável pelo desgaste na margem cervical e abertura de túbulos
dentinários (PIKDÖKEN et al., 2011; TOMASIK, 2006).
Além da prevenção e controle dos fatores que estejam causando danos,
existem opções de tratamentos que serão indicadas para cada caso de
sensibilidade em LCNC. Há opções não invasivas, e relativamente rentáveis, que
visam obstruir parcial ou completamente os túbulos dentinários abertos. Dentre
as abordagens nāo invasivas, pode-se citar a aplicação de uma camada adesiva,
dessensibilizadores ou verniz fluoretado, sendo que o paciente ainda pode fazer
uso doméstico de dentifricios dessensibilizantes contendo nitrato de potássio,
arginina ou nanoparticulas de hidroxiapatita (JENA; SHASHIREKHA, 2015;
PETERSSON, 2013; SHARIF; IRAM; BRUNTON, 2013). Ainda, a aplicação de
lasers também tem mostrado eficácia no combate à hipersensibilidade dentinária
(SGOLASTRA et al., 2013).
Quando opta-se pelo tratamento restaurador, existem diferentes
possibilidades de materiais a serem utilizados, como ionômero de vidro,
ionômero de vidro modificado por resina e resina composta. No caso das resinas
12
compostas, estas requerem o uso de sistemas adesivos, os quais demonstram
efetividade quando bem selecionados e aplicados (PEUMANS et al., 2014).
Porém, ao longo do tempo, falhas adesivas podem ocorrer, principalmente
quando da adesão em dentina, a qual oferece um substrato mais delicado para
o procedimento adesivo. A ação de metaloproteinases (MMPs) vem sendo
reportada como um dos causadores destas falhas, já que após realizado o
condicionamento ácido da dentina, estas enzimas presentes naturalmente na
estrutura do complexo dentinho pulpar, podem ser ativadas devido à queda do
pH. O sistema adesivo que deveria penetrar em toda a dentina descalcificada,
nem sempre consegue atingir toda a superfície, e assim, algumas fibras de
colágeno acabam ficando despotegidas e suscetíveis à açāo das MMPs
(GÖSTEMEYER; SCHWENDICKE, 2016).
Na tentativa de reduzir estas falhas, pode-se indicar o uso de substâncias
para aplicação durante o procedimento adesivo. A exemplo disso, nosso ensaio
clinico controlado randomizado, utilizou substâncias com o intuito de inibir as
MMPs, com a utilização de clorexidina 2%, e promover a remoção de fibras
colágenas da dentina, com o uso de hipoclorito de sódio 10%, após aplicação de
ácido fosfórico 37% e antes da aplicação do adesivo. Tais medidas tem o intuito
de diminuir a degradação da camada adesiva ao longo do tempo, e assim,
aumentar a longevidade adesiva das restaurações.
Porém, o sucesso das restaurações adesivas não dependem somente do
material utilizado, dependem muito dos aspectos operacionais da técnica
restauradora (DEMARCO et al., 2012). Fato este que vai desde o isolamento
eficaz do campo operatório, até o cumprimento dos passos exigidos pelo
fabricante do produto.
O tipo de isolamento do campo operatório (absoluto ou relativo) não é
consenso entre os cirurgiões dentistas, devido à isto, comparar as diferentes
técnicas é interessante. Isolamento dito absoluto com dique de borracha, grampo
e sugador de saliva, ou isolamento relativo, com rodetes de algodão, fio retrator,
afastador labial e igualmente, sugador de saliva, são técnicas disponíveis para
se obter um ambiente seco e limpo, livre de contaminações por sangue ou saliva
(ADA COUNCIL ON SCIENTIFIC AFFAIRS, 2003).
Mesmo quando as condições ideais para a execução da restauração são
atingidas, há outro fator que exige cuidado, a gengiva que estará em intimo
13
contato com esta restauração, principalmente no caso de restaurações de
LCNC. Deve-se procurar obter um acompanhamento efetivo do paciente,
garantindo seu estado de saúde. É importante adequada instrução de higiene
oral, para que o paciente consiga manter a saúde dos tecidos periodontais
adjacentes à restauração, e que, através de uma escovação correta e
atraumática, não cause aumento das lesões cervicais não cariosas antes
existentes, nem originem novas recessões gengivais.
Duas grandes investigações foram conduzidas, e contemplam os estudos
aqui apresentados. A primeira delas deu origem à 2 estudos (Capítulo 1 e 2),
respectivamente sobre os efeitos do pré-tratamento com CHX 2% e NaOCl 10%,
na retenção das restaurações de LCNCs, dados aqui reportados após 36 meses
de acompanhamento, e a segunda (Capítulo 3), refere-se ao impacto do tipo de
isolamento do campo operatório na taxa de falha das restaurações, também em
LCNCs, após 60 meses. Ademais, após a união dos dados oriundos das 2
grandes amostras, um quarto estudo (Capítulo 4), apresenta aqui a associação
entre os aspectos relacionados às restaurações (nível da margem e tipo de
isolamento) e os tecidos periodontais adjacentes.
Os estudos tiveram acompanhamento de 6 meses, 12 meses, 24 meses,
36 meses e em um deles, de até 60 meses. No último acompanhamento feito
em ambos, devido ao fato de se dar uma atenção especial aos critérios que
envolvem a saúde periodontal adjacente às restaurações, aliou-se ao exame
periodontal a aplicação de um breve questionário sobre hábitos possivelmente
nocivos dos pacientes, como ranger ou apertar os dentes à noite ou durante o
dia, se recebeu instruções de escovação e dieta quando fez as restaurações, se
cumpriu com as recomendações caso tenha recebido, qual o tipo de escova e o
tempo que ela costuma durar até a troca, qual o tipo de dentifrício utilizado, se é
muito abrasivo ou não, e por fim se havia sensibilidade antes e após as
restaurações terem sido feitas. Deste modo conseguimos obter uma ideia da
possível etiologia destas lesões. No entanto, sabe-se que LCNC são de origem
multifatorial (PEREZ et al., 2012), e devido à isso, devem ser tratadas com uma
visão holística do paciente e seus hábitos, para que o tratamento possa ser
realmente efetivo e não só paliativo.
A hipótese deste estudo, foi de que não haveria diferença significativa na
utilização dos diferentes métodos restauradores ou de isolamento, tanto na
14
sobrevida das restaurações quanto na saúde gengival dos pacientes, após
acompanhamento de 3 e 5 anos, respectivamente.
Sendo assim, o objetivo geral do presente estudo foi identificar a relação
entre restaurações em LCNC e sua sobrevida, bem como os impactos
periodontais em dois estudos clínicos randomizados com diferentes tempos de
acompanhamento.
Dentre os objetivos específicos executados, estão:
- Avaliar a efetividade do pré-tratamento da superfície dentinária com solução de
clorexidina 2% ou com hipoclorito de sódio 10%, na retenção das restaurações
de LCNC, com até 36 meses de acompanhamento.
- Verificar os efeitos do tipo de isolamento dental durante o tratamento
restaurador na sobrevivência de restaurações em LCNC, com até 60 meses de
acompanhamento.
- Identificar a resposta periodontal dos tecidos adjacentes às restaurações de
LCNC realizadas durante a execução de ambos os estudos acima, bem como, a
manutenção ou as modificações das características periodontais ao longo do
tempo.
15
Capítulo 1
Effectiveness of pre-treatment with chlorhexidine in restoration retention:
a 36-month follow-up randomized clinical trial
Abstract
Objectives: This study aimed to evaluate the effect of the pre-treatment with 2%
chlorhexidine as coadjutant in restoration retention of noncarious cervical lesions
(NCCL) after 36 months of follow-up.
Methods: A randomized controlled split-mouth and triple-blind (operators,
patients and evaluator) trial was carried out. Patients (n=42) with at least two non-
carious cervical lesions were included. The teeth with NCCL were randomly
assigned to two treatment groups: application of 2% CHX (experimental group)
or a placebo solution (control group) for 60 s after acid etching and before the
adhesive application. A trained and calibrated examiner evaluated the
restorations at baseline (1 week) and at each recall (6, 12, 24 and 36 months)
using the FDI criteria. A total of 225 restorations were evaluated after 36-month
follow-up. Data were subjected to survival analysis using the Kaplan-Meier
method, and the log-rank test was used to evaluate the existence of differences
between the survival curves (α=0.05).
Results: The restorations survival rate after 36 months of follow-up was 76.1%.
There was no difference in the retention and failure rates between the
experimental and the control group (p=0.968). There was an increased failure
trend when restorations were located subgingival compared to those at the
gingival level or supragingival.
Conclusion: The pre-treatment with 2% chlorhexidine digluconate did not
promote further restoration retention of noncarious cervical lesions.
16
Clinical Significance: Determine of the application of 2% chlorhexidine as
reducing MMP activity, improve the clinical performance of restorations over time
as they have high index of failure.
Keywords: chlorhexidine, MMP inhibitor, adhesive system, randomized
controlled trial, dental restoration, noncarious cervical lesions.
Introduction
The adhesion to dentin has been reported as a challenge to restorative dentistry
[1], especially in high stressful situations such as the restoration of noncarious
cervical lesions (NCCL), in which the retention of the restorative material relies
only on its adhesion to the non-retentive cavity. Despite all advances, the
micromechanical union between adhesive system and dentin substrate still
presents limitations that could jeopardize the longevity of adhesive restorations
in long term[2].
The loss of bond strength of resin to dentin occurs mainly by the degradation of
the hybrid layer, and has been a problem which directly influences the longevity
of the restoration. After etching, the adhesive system, should penetrate the entire
decalcified dentin, as it does not always occur, collagen fibers are unprotected
and susceptible to attack of metalloproteinases [3].
These enzymes are latently within the dentine and can be reactivated at the time
of etching with phosphoric acid for the mineral dissolution. Still, they can be
reactivated during the process of dental caries formation, or by the monomers
present in the acid etch systems. It has been suggested that the suspension of
the degrading activity of MMPs by protease inhibitors may modify the dentin
surface after acid etching [4,5], and this could increase the long-term stability of
resin-dentin interface.
The chlorhexidine digluconate (CRX) is an effective and non-specific MMP
inhibitor evidenced both in vivo and in vitro studies [6,7]. Many in vitro studies
have shown the chlorhexidine ability to prevent or at least retard the degradation
of the collagen fibrils of hybrid layer, which could extend the durability of the
adhesive bond between the tooth and restoration [8]. These results were recently
summarized in systematic reviews [9,10]
There are only few clinical trials [11–13] evaluating the applicability of
chlorhexidine in the longevity of restorations. Those studies showed no influence
of the application for chlorhexidine prior to the dentin adhesion on the clinical
durability of adhesive restorations. A recent systematic review concluded that
17
there is insufficient evidence to recommend or refute degradation inhibitory cavity
pre-treatment prior adhesively placing resin-based restorations [14]. However,
that conclusion was based mainly in studies presenting high risk of bias and with
shorter follow-ups. Only one study presented low risk of bias [13]. These results
may change if teeth are followed-up for longer.
Thus, the objective of this study was to evaluate the effect of the pre-treatment
with 2% chlorhexidine as coadjuvant in restoration retention of noncarious
cervical lesions, followed-up 36-month. The tested hypotheses were that the
reduction of MMP activity by chlorhexidine provides better clinical performance
of the restorations over time.
Materials and methods
Ethical Aspects
This study was approved by the Local Ethics Committee (protocol 210/2011). It
was registered in clinicaltrials.gov (NCT01947192), and followed the CONSORT
guidelines [15]. Prior to the participation in the study, all participants signed a
written informed consent.
Study Design
This study is a 36-month follow up of a prospective randomized clinical trial,
designed as split-mouth and triple-blind (operators, patients and evaluator) [13].
The teeth with noncarious cervical lesions (NCCL) were randomly divided into 2
treatment groups: test group (application of CHX 2%) or control group (application
of placebo solution), both applied after etching and before the adhesive system.
Ten operators (undergraduate students from the last year of the School of
Dentistry, Federal University of Pelotas) placed the restorations in 2011 and 2012
supervised by two researches (AFM and MSC).
Operators’ Training
The operators were previously trained according theoretical and practical aspects
to ensure the standardization of clinical procedures and minimize variations
inherent to different operators. During the theoretical phase, lectures were given
and pre-clinical activities were conducted. During the practical phase, each
operator performed the adhesive and restorative procedures in volunteers (10%
sample) not included in this study.
Sample Size
Taking into account a 92.3% retention percentage after 36 months to NCCLs
placed with the adhesive system Adper Single Bond 2 [16], the calculation of the
size of the sample was based on a 20% difference in retention rates between
18
groups at a significance level of 5%, with a power of 80%, resulting in a sample
of 35 patients in a split-mouth design. Considering the dropout rate throughout
the trial period, the need for 40 patients was considered.
Patient’s recruitment
Subjects were recruited by the examination of patients under treatment at the
School of Dentistry and by advertisements posters set in college. All those who
needed dental treatment of NCCL and fulfilled the inclusion and exclusion criteria
(Table 1) were invited to participate. Dental treatments were carried out in a
dental clinic specially organized for the treatment of NCCL at the School of
Dentistry, Federal University of Pelotas, to obtain the sample size required. All
dental needs of the subjects enrolled in this study, except for prosthetic
rehabilitation and orthodontic treatment, were provided.
NCCL screening
The selection of the NCCL was performed using a mouth mirror, an explorer and
periodontal millimetre probe by two researches. Reasons for treatment were
cervical tooth sensitivity, aesthetic complaints and/or prevention of further tooth
damage. The depth of NCCL was measured by placing the probe in its deepest
part, while the height was calculated by the distance between the most coronal
to the most apical point of the cavity margins. The degrees of dentinal sclerosis
were identified using a rating scale of 1 up to 4 [17]. The sensitivity test was
measured by compressed air for 3s at a distance of 2-3 cm, while the adjacent
teeth were protected with the fingers. Tooth vitality was tested using an Endo-
frost cold spray on the tooth. No attempt was made to determine the aetiology of
cervical lesions.
The teeth to be restored had a normal occlusal relationship with natural dentition
and at least one adjacent tooth contact, were vital and had a positive response
to cold. Cavosurface angleere not bevelled and no retentive grooves were placed.
Study Groups
All volunteers who met the eligibility criteria were randomly divided into test or
control groups, where the CHX 2% (test) or a placebo solution (control) were
applied to the dentin after acid etching procedure.
Randomization and Blinding Procedures
Randomization was performed using a computer program (Microsoft Excel, 2010)
by a person not directly involved in the study. A random table was used to allocate
NCCLs in each study group by random numbers, for a person not directly
involved in the clinical part of the study. The treatment was allocated regarding
the tooth dental group (incisors, canines and premolars), where the first tooth

19
restored was raffled for treatment, while the next tooth from the same tooth-group
was automatically assigned to the other treatment, according to the split-mouth
design. Thus, after being randomly assigned, each patient received the same
number of restorations of both groups, following the split-mouth design. Each
operator performed the same number of restorations for both groups.
Individual opaque sealed envelopes were used to conceal the randomization
sequence, which was coded as Treatment A or Treatment B. This condition
enabled blinding of operators and patients because the clinical procedure was
the same for both groups.
Clinical Procedures
The clinical protocol (the same for test and control groups) was printed and
posted in each dental unit so the operator was able to easily review the. There
was no making bevel or any cavity preparation before restorative procedures.
Prophylaxis was done and the tooth shade was selected using a shade guide
(VitaPan Classic, Vita Zahnfabrik, Bad Sackingen, Germany) before bonding
procedures. Where necessary, local anesthesia was taken. All procedures were
carried out using relative isolation method with labial retractors, cotton rolls, saliva
aspirator and gingival retraction cord (Cord # 000 Ultrapak, Ultradent, South
Jordan, UT, USA) into the gingival sulcus. The etching was performed with the
35% phosphoric acid (Adper Scotchbond Etchant, 3M ESPE) for 20 s in enamel
and 15 s in dentin, followed by rinsing with air/water spray for 30 s and removal
of excess moisture from cavity using absorbent paper. Afterwards, (1) for the test
group CHX 2% was applied (manipulated solution; Intended Use Pharmacy,
Pelotas, Brazil) under scrubbing action for 60 s using a disposable applicator and
the solution excess was removed. For the control group (2), a placebo solution
(solution similar to that used for test group, but without CHX) was applied on the
cavity at the same way as for test group. The application of a two-step etch-and-
rinse adhesive system (Single Bond 2 3M ESPE, St. Paul, MN, USA) was
performed according the manufacture’s instructions and light-cured for 10 s using
LED light-curing unit (Radii-Call; SDI, Bayswater, VI, Australia), intensity of 800
mW/cm2. The NCCLs were restored with a direct restorative nanocomposite resin
(Filtek Z350, 3M ESPE, Irvine, CA, USA) applied in at least two increments (no
more than 2 mm thick), using a selected instrument (Hu-Friedy , Chicago, IL,
USA). Each increment was light cured for 20 s.
Final contouring and polishing of the restorations were performed using a fine
diamond burs and ultra-thin (KG Sorensen, Barueri, SP, Brazil) under
refrigeration and low speed, floppy disks (Sof-Lex Pop-On, 3M ESPE), polishing
paste (Diamond Excel, Dental Products FGM, Joinville, Brazil) and rubber tips
(Enhance; Dentsply Caulk, Milford, dE, USA).
20
Clinical Assessment
Criteria approved by the FDI World Dental Federation were used for clinical
evaluation of restorations [18]. The primary clinical outcome was the retention of
the restoration, considering as failure, complete loss of restoration. Secondary
outcomes included the criteria as follows: 1) marginal adaptation, 2) marginal
staining, 3) the color of the surface, 4) post-operative sensitivity, 5) surface
brightness, 6) translucency and color, 7) fracture, 8) anatomical shape and 9)
preserving the vitality and integrity of teeth. Each criterion was expressed in five
scores, three for acceptable and two for non-acceptable (repair or replacement).
The evaluations were conducted by an experienced examiner previously trained
and calibrated examiner. The examiner was blind to the intervention and was not
involved in allocations or in restorative procedures. A Web-based tool
(www.ecalib.info) and clinical setting evaluation were used for training and
calibration of the examiner. The clinical intra-examiner calibration was carried out
with 30 NCCL restorations, which were re-examined 15 days later. A pre-
evaluation intra-agreement of at least 90% was obtained.
Recalls
Telephone contact was made with the patients to recall them for the periodic
assessment of the restorations. Those who were not touched by phone call; letter
was sent to the home address identified in the records. At each recall, the
examiner evaluated the restorations blindly. Revaluations were made for periods
of 6 months, 12 months, and 24 months after 36 months. Considering that some
patients took more time to attend to the recalls the time of follow up extended for
more than 36 months for some cases.
Statistical Analysis
Data were subjected to survival analysis using the Kaplan-Meier method. The
log-rank test was used to evaluate the existence of differences between the
survival curves. Crude Cox regression models with shared frailty were used to
verify the association between treatment and the risk of failure over time,
estimating the Hazard Ratios (HR) and 95% confidence intervals. Statistical
analysis was carried in October using Stata 11.0 Statistic Program (Stata Corp
LP, College Station, TX, USA).
Results
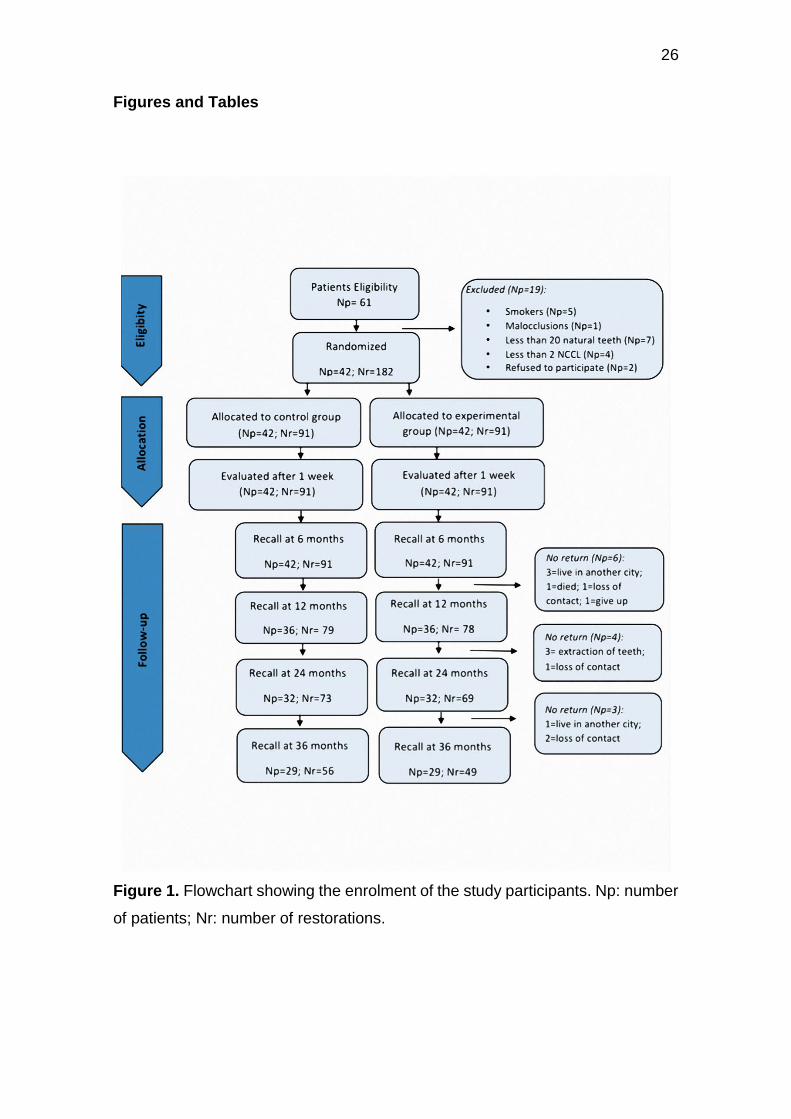
During the enrolment, from September 2011 to August 2012, 61 subjects were
assessed for eligibility. Forty-two patients (20 men and 22 women, mean age
49.7 years old) were enrolled in the study. After 36-month follow up, 29 patients
returned for re-evaluations. Details of the recruitment procedures, exclusion

21
characteristics of the patients, and the number of participants through each stage
of the trial are disclosed in the flow diagram (Figure 1).
A total of 105 restorations were evaluated at 36-month follow up. The restorations
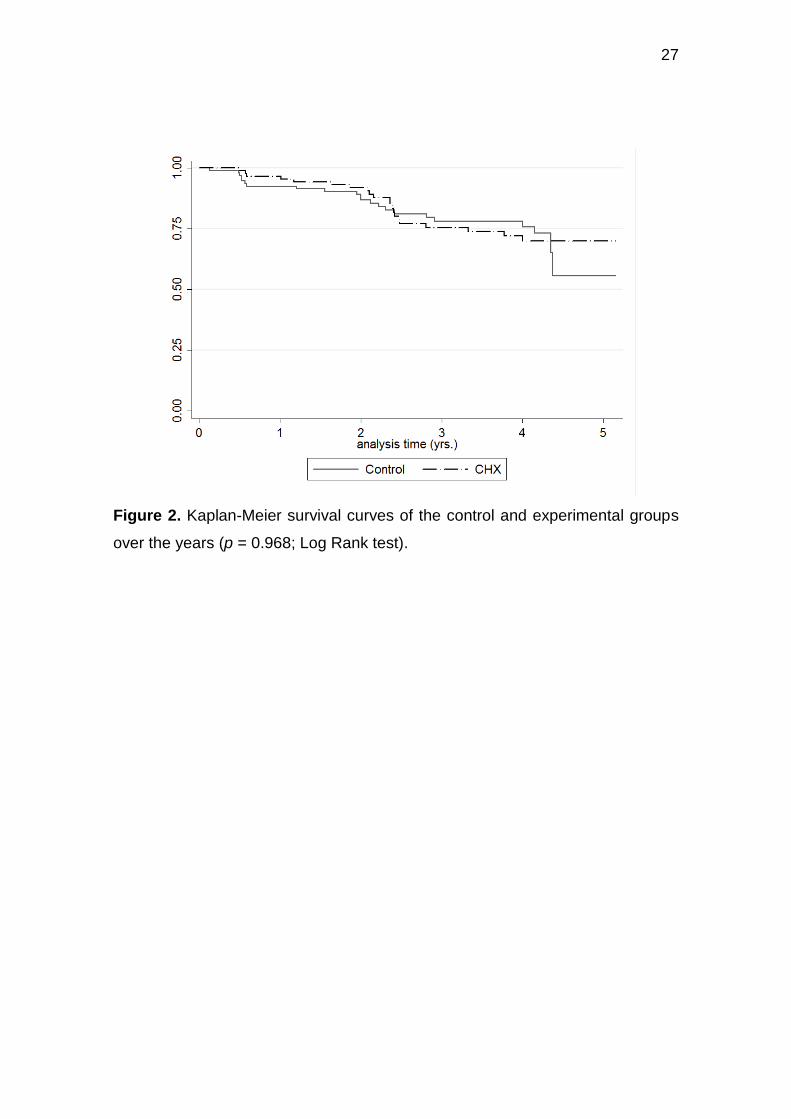
survival rate after 36 months of follow-up was 76.1%. The annual failure rate of
restorations was 8.4% at 3 years of follow up, and 5.5% at 2 years follow-up.
Figure 2 shows the Kaplan-Meier survival curves for both groups. It is possible to
observe that there is no difference between experimental and control groups
(p=0.968). The same result was found in cox regression model with shared frailty
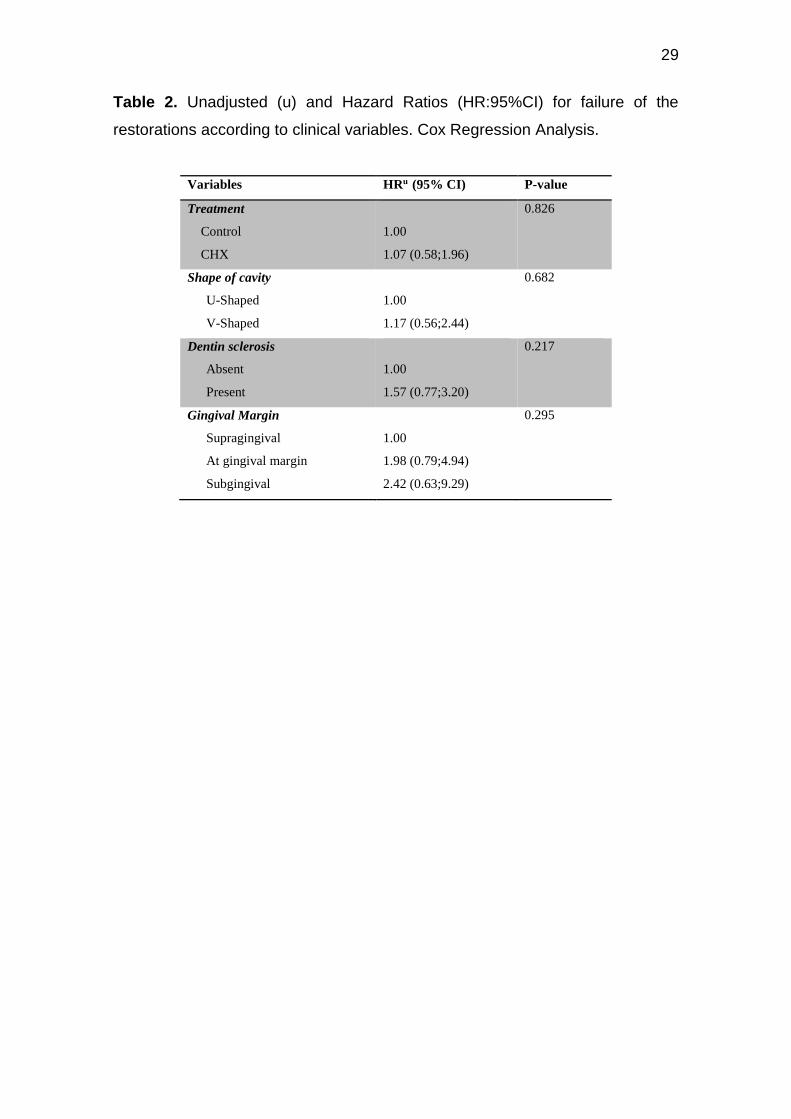
(Table 2). As is seen in Table 2, there is a tendency to failure increased when
restorations are located subgingival compared those to the level and
supragingival. On the data obtained, it can be inferred that the use of
chlorhexidine has not affected the risk for failure of restorations during the follow-
up.
Discussion
The findings of this study showed that there was no difference in the retention
and failure rates between the experimental and the control groups, up to 36
months follow-up. Although the chlorhexidine group presented a higher trend for
failure risk in restorations survival, there was no difference compared to the
control group. The hypothesis that the reduction and / or inhibition of MMPs by
chlorhexidine top clinical performance of restorations promotes' survival over time
was not confirmed.
Previous clinical trials studies [12,13] also showed no difference in survival of
non-carious cervical lesions using chlorhexidine as a coadjutant in the adhesive
procedure. Thus, so far, the increasing of an extra step of adhesive procedure
(the application of chlorhexidine solution) has not presented any advantage. At
present, there is only a single other trial that reported more than 24-month follow
up, and this study also concluded that etching with chlorhexidine digluconate
does not increase the durability of noncarious cervical restorations in 36-month
[11]. Maybe, even longer follow-ups are needed to show an evidence of the MMP
inhibition by chlorhexidine.
The laboratorial evidence does not convincingly support those findings showed
in clinical studies. Chlorhexidine has being used as a coadjuvant for dentin
adhesion and had showing a satisfactory effect on decreasing the resin-dentin
bond degradation long time [9], in in vitro and ex vivo studies, mainly in the first
months of function in the oral cavity [19]. Preserving the long-term integrity of the
resin-dentin hybrid layer in dental restoration by MMP inhibition is relevant, as it
could increase the longevity of restorations. However, the available clinical data
on effect of pre-treatment with chlorhexidine do not support such treatment for
reducing risk of retention loss or restoration failure [3]. Moreover, further
outcomes like safety (pulp irritation, allergy) should be assessed regarding

22
chlorhexidine application. So far, there is no indication that pre-treatment is
harmful.
Concerns still last regarding the use of chlorhexidine, studies exploring the
relationship between the concentration of chlorhexidine and bond strength values
have been performed and showed that the association between these aspects
does not occur linearly [10]. Chlorhexidine when applied to the dentin surface at
concentration equal to 0.1%, or greater, can Improve the bond strength values
long-term in vitro, by reducing the degradation mediated by endogenous
enzymes [20]. In a recent systematic review of this association, it was shown that
in most studies, pre-treatment with CHX presented smaller reduction in bond
strength than the control groups [21].
Nevertheless, it is important to note a relevant limitation of the clinical trials as the
patients accompaniments for long periods of time, since it can occurs the loss of
these patients, and consequently the loss of their data. Specially regarding the
subjects of this present study, the no return happens either by loss of contact with
them. Many patients changed the phone numbers or change the address. This
hinders the return and reduces the number of collected data.
In general, failure of restorations of NCCL might not have been solely related to
MMP inhibition treatment. Other factors such as caries risk or cavity size/shape
could influence restoration survival [22].The depth, height and cavity shape
(configuration) definitely play a role for failure-prognostic variables, as deeper
and wider lesions has presented more retention failure than the others [13].
However, the effect of cavity configuration or location in relation to the marginal
gingiva were not significant factors in the present study. The treatment of NCCLs
has a multifactorial character and presents clinical difficulties for restorative
procedures. Other parameters not only associated with restorative factors must
be observed, such as patient characteristics, diagnosis of harmful oral habits and
etiological factor removal [23]. In order to improve survival rate of restorations,
factors related to the patient and operator are of primary importance [24].
Therefore, treat the cause first can increase our restorations success rates.
Different approaches should be made to each specific situation. Considering the
effect of these patient individual characteristics on the survival of restorations, we
have carried out the present study with a split-mouth design to reduce the impact
of these variations on the research question.
Within the period of 36-month, noncarious cervical restorations placed with both
treatments performed equally with a survival rate of 76.1%, with acceptable
clinical performance. The application of CHX as a MMP inhibitor used as a pre-
treatment in dentin adhesion did not influence the retention of NCCL restorations
after 36-month of follow-up.
23
References
[1] A.L. Boskey, The role of extracellular matrix components in dentin mineralization., Crit. Rev. Oral Biol. Med. 2 (1991) 369–87. http://www.ncbi.nlm.nih.gov/pubmed/1654141 (accessed October 19, 2016).
[2] R.M. Carvalho, A.P. Manso, S. Geraldeli, F.R. Tay, D.H. Pashley, Durability of bonds and clinical success of adhesive restorations, Dent. Mater. 28 (2012) 72–86. doi:10.1016/j.dental.2011.09.011.
[3] G. Göstemeyer, F. Schwendicke, Inhibition of hybrid layer degradation by cavity pretreatment: Meta- and trial sequential analysis., J. Dent. 49 (2016) 14–21. doi:10.1016/j.jdent.2016.04.007.
[4] A. Mazzoni, D.H. Pashley, Y. Nishitani, L. Breschi, F. Mannello, L. Tjäderhane, M. Toledano, E.L. Pashley, F.R. Tay, Reactivation of inactivated endogenous proteolytic activities in phosphoric acid-etched dentine by etch-and-rinse adhesives, Biomaterials. 27 (2006) 4470–4476. doi:10.1016/j.biomaterials.2006.01.040.
[5] M.R.O. Carrilho, S. Geraldeli, F. Tay, M.F. de Goes, R.M. Carvalho, L. Tjäderhane, A.F. Reis, J. Hebling, A. Mazzoni, L. Breschi, D. Pashley, In vivo preservation of the hybrid layer by chlorhexidine., J. Dent. Res. 86 (2007) 529–33. http://www.ncbi.nlm.nih.gov/pubmed/17525352 (accessed October 19, 2016).
[6] W.W. Brackett, F.R. Tay, M.G. Brackett, A. Dib, R.J. Sword, D.H. Pashley, The effect of chlorhexidine on dentin hybrid layers in vivo., Oper. Dent. 32 (2007) 107–11. doi:10.2341/06-55.
[7] M.R.O. Carrilho, R.M. Carvalho, M.F. de Goes, V. di Hipólito, S. Geraldeli, F.R. Tay, D.H. Pashley, L. Tjäderhane, Chlorhexidine preserves dentin bond in vitro., J. Dent. Res. 86 (2007) 90–4. http://www.ncbi.nlm.nih.gov/pubmed/17189470 (accessed October 19, 2016).
[8] R. Gendron, D. Grenier, T. Sorsa, D. Mayrand, Inhibition of the activities of matrix metalloproteinases 2, 8, and 9 by chlorhexidine., Clin. Diagn. Lab. Immunol. 6 (1999) 437–9. http://www.ncbi.nlm.nih.gov/pubmed/10225852 (accessed October 19, 2016).
[9] A F. Montagner, R. Sarkis-Onofre, T. Pereira-Cenci, M.S. Cenci, MMP Inhibitors on Dentin Stability: A Systematic Review and Meta-analysis, J. Dent. Res. 93 (2014) 733–743. doi:10.1177/0022034514538046.
[10] F.M. Collares, S.B. Rodrigues, V.C. Leitune, R.K. Celeste, F. Borba de Araújo, S.M. Samuel, Chlorhexidine application in adhesive procedures: a meta-regression analysis., J. Adhes. Dent. 15 (2013) 11–8. doi:10.3290/j.jad.a28732.
[11] N. Sartori, S.C. Stolf, S.B. Silva, G.C. Lopes, M. Carrilho, Influence of chlorhexidine digluconate on the clinical performance of adhesive restorations: A 3-year follow-up, J. Dent. 41 (2013) 1188–1195. doi:10.1016/j.jdent.2013.09.004.
24
[12] M. Dutra-Correa, C.H. Saraceni, M.T. Ciaramicoli, V.H. Kiyan, C.S. Queiroz, Effect of chlorhexidine on the 18-month clinical performance of two adhesives., J. Adhes. Dent. 15 (2013) 287–92. doi:10.3290/j.jad.a29533.
[13] A.F. Montagner, A.P. Perroni, M.B. Correa, A.S. Masotti, T. Pereira-Cenci, M.S. Cenci, Effect of Pre-treatment with Chlorhexidine on the Retention of Restorations: A Randomized Controlled Trial., Braz. Dent. J. 26 (2015) 234–241. doi:10.1590/0103-6440201300009.
[14] G. Göstemeyer, F. Schwendicke, Inhibition of hybrid layer degradation by cavity pretreatment: Meta- and trial sequential analysis, J. Dent. (2016). doi:10.1016/j.jdent.2016.04.007.
[15] K.F. Schulz, D.G. Altman, D. Moher, WITHDRAWN: CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials, Int. J. Surg. 115 (2010) 1063–1070. doi:10.1016/j.ijsu.2010.09.006.
[16] A.D. Loguercio, D.D. Bittencourt, L.N. Baratieri, A. Reis, A 36-month evaluation of self-etch and etch-and-rinse adhesives in noncarious cervical lesions., J. Am. Dent. Assoc. 138 (2007) 507-14–7. http://www.ncbi.nlm.nih.gov/pubmed/17403742 (accessed October 19, 2016).
[17] A. V Ritter, H.O. Heymann, E.J. Swift, J.R. Sturdevant, A.D. Wilder, Clinical evaluation of an all-in-one adhesive in non-carious cervical lesions with different degrees of dentin sclerosis., Oper. Dent. 33 (2008) 370–378. doi:10.2341/07-128.
[18] R. Hickel, A. Peschke, M. Tyas, I. Mjör, S. Bayne, M. Peters, K.-A. Hiller, R. Randall, G. Vanherle, S.D. Heintze, FDI World Dental Federation - clinical criteria for the evaluation of direct and indirect restorations. Update and clinical examples., J. Adhes. Dent. 12 (2010) 259–72. doi:10.3290/j.jad.a19262.
[19] H.A. Ricci, M.E. Sanabe, C.A. de Souza Costa, D.H. Pashley, J. Hebling, Chlorhexidine increases the longevity of in vivo resin-dentin bonds, Eur. J. Oral Sci. 118 (2010) 411–416. doi:10.1111/j.1600-0722.2010.00754.x.
[20] J. De Munck, P.E. Van den Steen, A. Mine, K.L. Van Landuyt, A. Poitevin, G. Opdenakker, B. Van Meerbeek, Inhibition of enzymatic degradation of adhesive-dentin interfaces., J. Dent. Res. 88 (2009) 1101–6. doi:10.1177/0022034509346952.
[21] D. Dionysopoulos, Effect of digluconate chlorhexidine on bond strength between dental adhesive systems and dentin: A systematic review., J. Conserv. Dent. 19 (2016) 11–6. doi:10.4103/0972-0707.173185.
[22] N.J.M. Opdam, F.H. van de Sande, E. Bronkhorst, M.S. Cenci, P. Bottenberg, U. Pallesen, P. Gaengler, A. Lindberg, M.C.D.N.J.M. Huysmans, J.W. van Dijken, Longevity of posterior composite restorations: a systematic review and meta-analysis., J. Dent. Res. 93 (2014) 943–949. doi:10.1177/0022034514544217.
[23] C.D.R. Perez, M.R. Gonzalez, N.A.S. Prado, M.S.F. de Miranda, M. de A. Macêdo, B.M.P. Fernandes, C. dos R. Perez, M.R. Gonzalez, N.A.S. Prado, M.S.F. de
25
Miranda, M. de A. Macêdo, B.M.P. Fernandes, Restoration of noncarious cervical lesions: when, why, and how., Int. J. Dent. 2012 (2012) 687058. doi:10.1155/2012/687058.
[24] F.F. Demarco, M.B. Corrêa, M.S. Cenci, R.R. Moraes, N.J.M. Opdam, Longevity of posterior composite restorations: Not only a matter of materials, Dent. Mater. 28 (2012) 87–101. doi:10.1016/j.dental.2011.09.003.
26
Figures and Tables
Figure 1. Flowchart showing the enrolment of the study participants. Np: number
of patients; Nr: number of restorations.
27
Figure 2. Kaplan-Meier survival curves of the control and experimental groups
over the years (p = 0.968; Log Rank test).

28
Table 1 . Inclusion and exclusion Criteria used in this research
Inclusion criteria:
• Patients with at least 2 NCCLs in incisors, canines or pre molars;
• Patients with more than 20 teeth present in the mouth;
• Patients above 18 years of age;
• Patients able to understand the free and informed consent (IC);
• NCCLs with at least 1mm deep on the buccal teeth and may extend with a
small part for interproximal region;
• Individuals with good periodontal health.
Exclusion criteria:
• Patients smokers;
• Patients with bruxism;
• Patients with severe systemic diseases;
• Patients undergoing orthodontic treatment;
• Teeth with NCCL but without antagonists;
• Teeth wear facets with greater than 50% at the incisal and / or occlusal faces;
• Presence of decay or restoration in the area to be treated;
• Visible plaque index (VPI) and gingival bleeding index (GBI) greater than 20%;
• Probing depth and clinical attachment loss greater than 4 mm, with probing
bleeding;
• Lack of interest in return for follow-up or refusal to participate.
29
Table 2. Unadjusted (u) and Hazard Ratios (HR:95%CI) for failure of the
restorations according to clinical variables. Cox Regression Analysis.
Variables HRu (95% CI) P-value
Treatment
Control
CHX
1.00
1.07 (0.58;1.96)
0.826
Shape of cavity
U-Shaped
V-Shaped
1.00
1.17 (0.56;2.44)
0.682
Dentin sclerosis
Absent
Present
1.00
1.57 (0.77;3.20)
0.217
Gingival Margin
Supragingival
At gingival margin
Subgingival
1.00
1.98 (0.79;4.94)
2.42 (0.63;9.29)
0.295
30
Capítulo 2
Effect of sodium hypochlorite pre-treatment on the retention of restorations
for non-carious cervical lesions: a 3-year randomized controlled trial
Abstract
Objective: This study aimed to evaluate the failure rates of composite restorations
of non-carious cervical lesions (NCCL) performed with or without the pre-
treatment with 10% sodium hypochlorite (NaOCl) on etched dentin.
Materials and methods: A randomized controlled split-mouth and double blind
clinical trial was carried out. Patients (n=30) with at least two NCCL were included
and 100 NCCL were restored. Each patient received at least one pair of
composite restorations (Filtek Z350/3M ESPE), bonded either with 2 techniques:
control (acid etching + placebo solution for 60 seconds + Adper Single Bond 2/3M
ESPE) or experimental (acid etching + 10% NaOCl for 60 seconds + Adper Single
Bond 2). A calibrated examiner evaluated the restorations (baseline, 6-, 12-, 24-
and 36-month) using the FDI criteria. The primary outcome was retention of the
restoration. The data were submitted to the chi-square for the frequency of
failures according to the characteristics of the patients and the lesions. Survival
data were analyzed with the Kaplan-Meier method, log-rank test and Cox
regression (p<0.05).
Results: The average lifetime of the restorations in this study was 2.86 years. The
annual failure rate was 9% for the control group and 17.8% for the experiential
group. According to the Cox regression, the group that used NaClO failed 40%
more than the control group, but there was no statistically significant difference
compared to control (p = 0.075). A greater failure rate was observed in patients
with the presence of fewer teeth in the mouth (p=0.320), in teeth at the lower arch
(p=0.039), and mainly, in premolars (p=0.013).
Conclusion: The pre-treatment with 10% sodium hypochlorite as an adjuvant in
dentin adhesion did not improve the retention rate of NCCL restorations .
Clinical Significance: The use of 10% hypochlorite to remove collagen fibers from
the dentin does not have any benefit for the retention of NCCL restorations in a
36 months follow-up.
Keywords: randomized controlled trial, dental restoration, noncarious cervical
lesions, sodium hypochlorite.
31
1. Introduction
An effective and stable composite-dentin adhesion is fundamental for the
long-term durability of composite restorations, especially when little or no
marginal enamel is available for bonding [1]. In challenging situations, as the
restorative treatment of non-carious cervical lesions (NCCLs), the lost of
restoration’s retention is a common reported problem [2]. Clinical studies of
NCCLs restored with composite and without mechanical retentions constitute a
worthy model for evaluating the clinical performance of adhesive restorations,
since the retention of those restorations depends on the adhesive procedure [3].
Moreover, the prognosis of cervical restorations may be affected by several
factors, not only the adhesive procedure is defying, but also the clinical
characteristics of the cervical lesion and aspects related to the patient could play
a role in the retention rate of restorations [2].
It is known that phosphorical conditionated dentin is still a challenge, since
there are demineralized areas where the adhesive monomer does not have a
good infiltration, which leaves exposed collagen not impregnated by adhesive
[4,5]. These collagen fibrils can undergo hydrolysis, which directly interferes with
the degradation of the adhesive interface long-term. Based on this aspect and
taking into account the difficulties related to the presence of collagen in
hybridization, the attempt to remove dentin collagen by means of sodium
hypochlorite (NaOCl) application after phosphoric acid etching was considered.
NaOCl, a nonspecific proteolytic agent, has the ability to dissolve collagen
proportional to the time of application and to the concentration of active chlorine
and superoxide radicals [6,7]. At 10% NaOCl concentration applied after dentin
acid etching and before adhesive application, it promotes deproteinization of the
dentin surface. Further, the application of sodium hypochlorite aims to promote
the exposure and amplification of the dentin tubules, making the dentin reacts
similar to the enamel, which is a favorable surface for adhesion [8,9].
Some in vitro studies have demonstrated that collagen removal techniques
after dentin conditioning increase the dentin bond strength when compared to the
conventional etching – without collagen removal [10,11]. However, another in
vitro studies have shown that pre-treatment with sodium hypochlorite for dentin
deproteinization did not demonstrate any superior adhesive efficiency when
compared to the conventional adhesive technique long-term [8,12]. Because
positive (and sometimes controversial) results have been reported in laboratory
studies, the effectiveness of the collagen removal technique needs to be clinically
further evaluated.
Clinical studies evaluating the performance of the deproteinization
technique are scarce [13,14]. A previous pilot study concluded that the
preliminary evaluation of the sodium hypochlorite treatment in the restoration of
non-carious cervical lesions is encouraging [13]. Although no significant
differences were noted between the conventional (acid etch only) and
deproteinization (acid etch + collagen removal) techniques; additional, it was
suggested that the type of adhesive system might negatively affect the collagen
32
removal technique [14]. A similar trend has also been noted in laboratory studies
[8,15] although conflicting results have been reported.
By foregoing, there is still uncertainty as how this type of dentin pre-
treatment could clinically collaborate with the survival of the restorations. Thus,
the aim of this study was to evaluate the failure rates of composite restorations
of NCCL performed with or without the pre-treatment with 10% NaOCl on etched
dentin. The hypothesis of the present study was that the application of
deproteinization solution after acid etching does not influence the failure rate of
the restorations after a follow-up of 3 years.
2. Materials and methods
2.1. Ethical considerations
The present research was approved (protocol 210/2011) by the Ethics
Committee (CEP) of the School of Dentistry of the Federal University of Pelotas
(FO-UFPel). It was registered in clinicaltrials.gov and was reported according to
the guidelines of the Consolidated Standards of Reporting of Trials (CONSORT)
[16]. Prior to participating the study, all selected patients signed a free and
informed consent form.
2.2. Study Design
This study was a 3-year follow-up of a randomized clinical trial. The control
group used a placebo (water) solution, and the experimental group used 10%
sodium hypochlorite, both applied after dentin acid etching with 37% phosphoric
acid and before the adhesive system. It is a split-mouth and double blind (patients
and evaluator) study. It was not possible to blind the operators because of the
characteristic smell of sodium hypochlorite. The NCCL restorations were placed,
between 2011 up to 2012, by 10 operators (undergraduate students from the last
year of the Dental School) supervised by two researches (AFM and MSC).
2.3. Operators' Training
Theoretical and practical training of the operators was performed in order
to minimize variations among operators. The undergraduate students received a
manual containing materials’ instructions and the protocol of clinical procedures.
In addition, there were pre-clinical demonstratives training. For training, the
operators restored a number of teeth corresponding to 10% of the total NCCL
sample size in patients, following the same instructions received for clinical
execution, although those restorations/patients were not included on the sample
of the study.
33
2.4. Sample Size
Taking into account a 87% retention percentage after 36 months to NCCLs
placed with deproteinization technique [14] the calculation of the sample size was
based on a 20% difference in retention rates between groups at a significance
level of 5%, with a power of 80%,considering a sample loss during the follow up,
the sample size resulted in 30 patients in a split-mouth design.
2.5. Recruitment and selection of patients
The disclosure of the study was done through posters and pamphlets, and
patients who were interested in participating were clinically evaluated.
The inclusion criteria of the study were: a) patients with at least 2 NCCLs
in incisors, canines or pre molars, b) patients with more than 20 teeth present in
the mouth, c) patients above 18 years of age, d) patients able to understand the
free and informed consent and e) individuals with good periodontal health.
The exclusion criteria were as follows: a) smokers, b) patients with
bruxism, c) patients with severe systemic diseases, d) patients undergoing
orthodontic treatment, e) teeth with NCCL but without antagonists, f) teeth with
wear facets covering more than 50% at the incisal and / or occlusal surfaces, g)
presence of decay or restoration in the area to be treated, h) visible plaque index
(VPI) and gingival bleeding index (GBI) greater than 20%, probing depth and
clinical attachment loss greater than 4 mm, with probing bleeding, i) lack of
interest in return for follow-up or refusal to participate.
Patients who fulfilled the criteria received an informative letter about the
purpose of the study, as well as a free and informed consent form to be signed,
proving their voluntary interest in participate in the study. A detailed initial clinical
examination, including several criteria regarding the classification of NCCLs, was
met among the selected patients. The criteria for evaluation of NCCLs included
the following parameters: cervical lesion shape ("U" or "V"), length and height of
the lesion, relation of the cervical wall of the lesion with the gingival margin
(supragingival, gingival or subgingival margin), presence of wear facets,
presence and degree of dentin sclerosis when present, dentin sensitivity and pulp
vitality.
2.6. Randomization Blinding Procedures
Randomization was performed using a computer program (Microsoft
Excel, 2010), by a person (TPC) not directly involved in the study. A random table
was used to allocate the NCCLs in each study group. The treatment (control and
experimental) was allocated regarding the tooth-group (incisors, canines and
premolars), where the first tooth restored was raffled to one treatment, while the
next tooth from the same tooth-group was automatically assigned to the other
treatment, according to the split-mouth design. Thus, after being randomly
34
assigned, each patient received the same number of restorations of both groups.
Each operator performed the same number of restorations for both groups.
Individual opaque sealed envelopes were used to conceal the
randomization sequence, which was coded as Treatment A or Treatment B. The
same clinical sequence and identical bottles were used for both groups. However,
due to the characteristic odor of sodium hypochlorite, the operators could identify
the treatment solutions.
2.7. Clinical Protocol
Before the adhesive procedures, the prophylaxis of the tooth was
performed with rubber cup and paste based on pumice and water. No cavity
preparation or cavo-surface margin beveling was performed. Before the isolation
of the teeth, the color of the restoration was selected, following a color scale
(Vitapan Classical, Vita Zahnfabrik, Bad Sackingen, Germany). When necessary,
local anesthesia was taken.
After those preliminary steps, relative isolation of the operative field was
performed, using labial retractor, gingival retraction cord # 0000 (Ultrapak Cord,
Ultradent, South Jordam, UT, USA), cotton rollers and saliva aspirator. After
isolation, 37% phosphoric acid gel was applied to the surface for 15 sec, followed
by washing with air / water spray for 30 sec and drying with absorbent paper.
Then, for the experimental group, a manipulated solution of 10% sodium
hypochlorite (Uso Indicado Pharmacy, Pelotas, RS, Brazil) was applied with a
disposable pharmaceutical syringe, remaining 60 sec in contact with the dentin
surface. Subsequently, a thorough washing with air / water spray was performed
for 30 sec to remove as much residual NaOCl as possible. For the control group,
the same sequence was followed, however, using a placebo solution (similar to
the solution used for the experimental group but without NaOCl).
For both groups, the application of a two-step etch-and-rinse adhesive
system (Adper Single Bond, 3M ESPE, St. Paul, MN, USA) and restorative
technique using a nano-particulate composite resin (Filtek Z350, 3M ESPE, St.
Paul, MN, USA) were performed as recommended by the manufacture’s
instructions. Each increment was cured for 20 sec with a LED light-curing unit
(Radii-Call; SDI, Bayswater, VI, Australia), intensity of 800 mW/cm2.
All restorations were finished with # 12 scalpel blade, fine and ultra-fine
grained diamond burs (KG Sorensen, Barueri, SP, Brazil) under water-cooling in
order to remove excess material and / or improve the contour shape of the
restorations. Polishing was done with silicone tips, flexible discs of sandpaper
(Sof-Lex Pop-On, 3M ESPE, St. Paul, MN, USA), felt disks and polishing paste.
35
2.8. Clinical Assessment
A previously trained, calibrated and blinded examiner (MSC) who worked
as examiner in other clinical trials carried out the clinical evaluations at baseline
(1 week) and follow-up periods (6-, 12-, 24- and 36-month). A web-based training
and calibration tool (www.ecalib.info) and clinical setting evaluation were used for
training and calibration of the examiner. The clinical intra-examiner calibration
was carried out with 30 Class V restorations, which were re-examined 15 days
later. A pre-evaluation intra-agreement of at least 90% was obtained.
The examiner used the criteria approved by the FDI World Dental
Federation [18] for the clinical evaluation of the restorations. The primary clinical
outcome was the retention of the restoration, considering failure the complete
loss of restoration. Secondary endpoints included: marginal staining, the color of
the surface, post-operative sensitivity, surface brightness, translucency and
color, fracture, anatomical shape and preserving the vitality and integrity of teeth.
Each criterion was expressed in five scores, three for acceptable and two for non-
acceptable (repair or replacement).
2.9. Recalls
Patients were asked for re-evaluations in the 6-month, 12-month, 24-
month, and 36-month periods. Contact was made by telephone call (provided by
the patient during the last visit). In cases where there was no contact success,
letters were sent to the residential address informed in the clinical record.
Furthermore, in cases where the letters did not return, home visits were made by
the researchers and evaluators involved in the recalls (MSC and MF). In these
follow-ups, the restorations were evaluated according to FDI criteria and
photographic records were recorded.
2.10. Statistical Analysis
Statistical analysis was carried using Software Stata 14.2 (Stata Corp LP,
College Station, TX, USA). Descriptive analysis of interest variables was carried-
out. Differences between frequencies were assessed by Exact Fisher test.
Survival analysis was performed using Kaplan-Meier method. The log-rank test
was used to evaluate the existence of differences between the survival curves.
Unadjusted Cox regression models with shared frailty were used to verify the
association between treatment and the risk of failure over time, estimating the
Hazard Ratios (HR) and 95% confidence intervals. Annual failure rates were
calculated as described by Opdam et al., 2010 [19]. All analyses considered an
α=5%.

36
3. Results
During enrolment from September 2011 to August 2012, 62 patients were
assessed for eligibility, of whom 32 did not fulfilled the inclusion criteria or did not
want to participate. Thus, 30 patients (17 men and 13 women), mean age of 49-
year old (71.9% of the sample was between 41-60 years), with 100 restorations
in total, were enrolled in this study. Details of the recruitment procedures,
exclusion characteristics of the patients, lost and the number of participants
through each recall of the trial are disclosed in the flowchart (Figure 1).
The average lifetime of the restorations in this study was 2.86 years. At
36-month, the annual failure rate was 9% for the control group and 17.8% for the
experimental group.
In Table 1 it is possible to observe some characteristics of the subjects
evaluated at the last recall (36-month). Most patients had less than 24 teeth in
the mouth and 63.3% of the patients reported the consumption of acid foods and
/ or sour drinks, causing erosion. In addition, the presence of lesions in patients
with lower income and intermediate educational level was observed in our
patients on a larger scale (Table 1).
In Table 2 it is possible to observe the characteristics of the non-carious
cervical lesions. Regarding the characteristics of the restored lesions, it is
possible to emphasize that the most prevalent were "V" shaped cervical lesions,
with an average depth of less than 1mm and an average height of 1 to 3mm. The
most restored type of teeth were premolars (Table 2).
The Kaplan-Meier survival curves are presented in Figure 2. When
observed the failures and their distribution among the characteristics of the
patients and of the NCC lesions, there was a significant difference when
comparing the upper and lower jaw, with lower jaw showing more failures than
maxillary (p = 0.039). There was also a significant difference in failure rates
considering the tooth type, with premolars tooth-group presenting more failures
(p = 0.013). However, the type of dentin treatment (control and experimental) did
not influence on failure rates (p = 0.077) as well as the number of teeth in month
(p = 0.320 ). The data found in the Cox regression confirm these results regarding
their association significance (Table 5). Regarding the type of treatment, the
group that used NaOCl solution failed 40% more compared to the control group,
but the association was not significant (p = 0.075), this may be due to insufficient
sample size. The other evaluated criteria followed the same trend of Kaplan-
Meier survival curves.
When the data were submitted to the chi-square test (Table 3), in order to
measure the quantity and the percentage of the data according to the presence
or not of failure, it is observed that there was no significant difference in the failure
rates between the experimental and the control group (P = 0.054). Table 3
presents the variables influence on restoration’s retention. None studied variable
affected the restoration’s retention (all p > 0.05).

37
Regarding the sensitivity of the patients, obtained through a questionnaire,
before and after the restorations, it can be observed that 37.5% of patients never
had sensitivity, 56.3% had improvement in sensitivity after restoration, and only
6.3% of patients reported to remain sensitive even after restoring their lesions.
An interesting fact is that no patient in the experimental group (NaOCl) continued
with sensitivity after restoration, and 5 patients in the control group (placebo)
reported permanence of the sensitivity. However, there was no difference in
sensitivity reporting between the groups (p = 0.270).
After the 36-month follow up, most restorations for both treatment groups
(control and experimental) presented an FDI Score 1, which represents clinically
excellent (Table 4).
4. Discussion
This study evaluated the failure rates (based on restoration retention) and
clinical characteristics of restorations in non-carious cervical lesions, using 10%
sodium hypochlorite. It showed that the use of NaOCl as a dentin pre-treatment
did not affect directly the retention rates of the restorations placed in NCCLs,
however other factors as the tooth type and the position of the tooth in arch might
affect the failure rates of those restorations. Therefore, the hypothesis that the
use of 10% sodium hypochlorite after acid etching and before adhesive
application would not result in differences in restorative retention compared to the
conventional method was partially confirmed, because there was a greater loss
in the test group, even if influenced by other joint factors. Moreover, given the
loss of patients, it can not be said that there would be no difference.Also, due to
fewer resections in the test group at the end of the study, caution is required in
interpreting the results.
NaOCl is a deproteinizing agent that removes the collagen fibers from the
dentin and reduces the hydrolytic degradation of collagen not completely
infiltrated by the adhesive. The technique of collagen fibers removal is obtained
by applying NaOCl solution for 60 seconds, after phosphoric acid etching and
before the application of the adhesive, on the exposed dentin surface. At the
present study, noticeably more restorations bonded with deproteinization
technique were ‘lost’ when compared with conventional technique, however no
statistically significant differences were observed. In the literature, there is
information about the use of NaOCl in different situations and concentrations.
Among studies that reflect the execution of similar methodologies, concordant
results were observed. For instance, a similar clinical trial with a five-year follow-
up showed that the use of 10% NaOCl in dentin deproteinization does not affect
the clinical performance of class V restorations [14]. Further, another trial with a
lower follow-up period (two-years) obtained the same results [13]. Even if the
results for the retention of the restorations did not show a significant difference in
the different treatments used, interesting data can be drawn from studies
38
regarding the trend of greater failure due to the characteristics of the patient or
the restored teeth.
The failures in our study occurred more in patients with less than 24 teeth
in the mouth, probably because these teeth are compensating others during
mastication. Also, in vitro studies have shown that V-shaped lesions showed
higher stress concentration in comparison to the U-shaped [20,21]. In our
results, the failure rate was slightly higher in the U-shaped lesions. Many data
found help to confirm that non-carious cervical lesions are of multifactorial origin.
Our findings also showed more restoration failures in the lower arch, which can
be supposed to occur due to the fact that all restorations have been performed
with relative isolation, and the lower arch is more prone to difficulties in controlling
adequate moisture. Further, premolar teeth showed greater failure of
restorations, which may be attributed to the overload of these teeth due to the
loss of molars.
In most of the restorations evaluated, few changes were noted from
baseline to the 36-month evaluation recall for both groups. No significant
differences were observed between the two techniques in terms of retention or
any of the other evaluated criteria, including esthetic characteristics. According
to the evaluation of the restorations, performed by an experienced evaluator and
responsible for the other clinical trials evaluations, most of the esthetical,
functional, and biological criteria evaluated received an FDI score 1, which
represents clinically excellent. This demonstrates that the restorations have
remained satisfactory over time, irrespective of the treatment .
NCCL are generally chosen to verify retention of restorations because they
do not have macromechanical retention or cavity preparation. Moreover, they
also have other characteristics favorable to the preparation and evaluation of
restorations: they are usually present in anterior or premolar teeth, which allows
easy access to the lesion; when adhesive failure occurs, usually the loss of the
restoration occurs, and it is more objective to be evaluated; generally they do not
have preparation of the cavity, and this fact reduces the variation of the operator;
and they have a contact with large and accessible portions of dentin [22].
Another fact of extreme relevance in this study was that a minority of teeth
remained sensitive after restoration, which shows that the restorative treatment
has been shown to be effective in improving one of the patients' main complaints,
which is the dentin sensitivity.
A recent in vitro study reveals that the use a protocol of deproteinization
with 10% sodium hypochlorite may improve the adhesive longevity of the
restorations, but this study demonstrates one-year follow-up results [23].
Compared to our clinical study, the failures began to be more prevalent near to
the 2 years of follow-up. Although there was no significant association of failure
and type of treatment used, it can be inferred that there is a tendency to greater
failure of the restorations when using 10% NaOCl to treat the dentin surface
before bonding.

39
5. Conclusion
The application of 10% sodium hypochlorite to dentin, after acid etching, does not
improve the retention of class V restorations in non-carious cervical lesions and
the failure rates in a mean period of 36 months.
Acknowledgements
The authors would like to thank the participants and staff members, who were
fundamental in conducing this clinical trial. We also thank the Brazilian funding
agencies CNPq (Grants #486810/2012-7 and 306896/2011-7) and CAPES for
the financial support and scholarships.
40
References
[1] Chee B, Rickman LJ, Satterthwaite JD. Adhesives for the restoration of non-carious cervical lesions: A systematic review. J Dent 2012. doi:10.1016/j.jdent.2012.02.007.
[2] Namgung C, Rho YJ, Jin BH, Lim BS, Cho BH. A retrospective clinical study of cervical restorations: longevity and failure-prognostic variables. Oper Dent 2013. doi:10.2341/11-416-C.
[3] Heintze SD, Ruffieux C, Rousson V. Clinical performance of cervical restorations — A meta-analysis 2010;6:993–1000. doi:10.1016/j.dental.2010.06.003.
[4] Carvalho RM, Manso AP, Geraldeli S, Tay FR, Pashley DH. Durability of bonds and clinical success of adhesive restorations. Dent Mater 2012;28:72–86. doi:10.1016/j.dental.2011.09.011.
[5] Carvalho RM, Chersoni S, Frankenberger R, Pashley DH, Prati C, Tay FR. A challenge to the conventional wisdom that simultaneous etching and resin infiltration always occurs in self-etch adhesives. Biomaterials 2005. doi:10.1016/j.biomaterials.2004.04.003.
[6] Di Renzo M, Ellis TH, Sacher E, Stangel I. A photoacoustic FTIRS study of the chemical modifications of human dentin surfaces: II. Deproteination. Biomaterials 2001. doi:10.1016/S0142-9612(00)00239-8.
[7] Mannocci F, lecturer senior, Tay FR, professor associate, Pashley DH, Cook R. Deproteinization Effects of NaOCl on Acid-etched Dentin in Clinically-relevant vs Prolonged Periods of Application. A Confocal and Environmental Scanning Electron Microscopy Study. Oper Dent 2009:34–2. doi:10.2341/08-56.
[8] Uceda-gómez N, Dourado LOGUERCIO A, Kiss MOURA S, Helena Miranda GRANDE R, Oda M, Reis A, et al. Long-term bond strength of adhesive systems applied to etched and deproteinized dentin . J. Appl. Oral Sci 2007.
[9] Uceda- Gómez N, Reis A, Rocha De Oliveira M, Loguercio A, Rodrigues Filho LE, et al. Effect of sodium hypochlorite on the bond strength of an adhesive system to superficial and deep dentin. J. Appl. Oral Sci 2003.
[10] Arias VG, Bedran-de-Castro AKB, Pimenta LA. Effects of sodium hypochlorite gel and sodium hypochlorite solution on dentin bond strength. J Biomed Mater Res Part B Appl Biomater 2005;72B:339–44. doi:10.1002/jbm.b.30160.
[11] Pimenta L-AF, Amaral CM, Bedran de Castro AKB, Ritter AV. Stability of dentin bond strengths using different bonding techniques after 12 months: total-etch, deproteinization and self-etching. Oper Dent 2004.;29:592–8.
[12] Montagner AF, Perroni AP, Correa MB, Masotti AS, Pereira-Cenci T, Cenci MS. Effect of Pre-treatment with Chlorhexidine on the Retention of Restorations: A Randomized Controlled Trial. Braz Dent J 2015;26:234–41. doi:10.1590/0103-6440201300009.
[13] Almeida PC, André L, Pimenta F. 2-year Clinical Evaluation of Sodium
41
Hypochlorite Treatment in the Restoration of Non-carious Cervical Lesions: A Pilot Study .Operative Dentistry 2004. doi:10.2341/05-119.
[14] Torres CRG, Barcellos DC, Batista GR, Pucci CR, Antunes MJS, De La Cruz DB, et al. Five-year clinical performance of the dentine Deproteinization Technique in non-carious cervical lesions. J Dent 2014. doi:10.1016/j.jdent.2014.04.004.
[15] Shinohara MS, Ana /, Bedran-De-Castro KB, Cristiane /, Amaral M, Luiz /, et al. The Effect of Sodium Hypochlorite on Microleakage of Composite Resin Restorations Using Three Adhesive Systems 2004.
[16] Schulz KF, Altman DG, Moher D. WITHDRAWN: CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. Int J Surg 2010;115:1063–70. doi:10.1016/j.ijsu.2010.09.006.
[17] Loguercio AD, Bittencourt DD, Baratieri LN, Reis A. A 36-month evaluation of self-etch and etch-and-rinse adhesives in noncarious cervical lesions. J Am Dent Assoc 2007;138:507-14-7.
[18] Hickel R, Peschke A, Tyas M, Mjör I, Bayne S, Peters M, et al. FDI World Dental Federation - clinical criteria for the evaluation of direct and indirect restorations. Update and clinical examples. J Adhes Dent 2010;12:259–72. doi:10.3290/j.jad.a19262.
[19] Opdam NJM, Bronkhorst EM, Loomans B a C, Huysmans MCDNJM. 12-Year Survival of Composite Vs. Amalgam Restorations. J Dent Res 2010;89:1063–7. doi:10.1177/0022034510376071.
[20] Guimarães JC, Guimarães Soella G, Brandão Durand L, Horn F, Narciso Baratieri L, Monteiro S, et al. Stress amplifications in dental non-carious cervical lesions. J Biomech 2014;47:410–6. doi:10.1016/j.jbiomech.2013.11.012.
[21] Kuroe T, Caputo AA, Ohata N, Itoh H. Biomechanical effects of cervical lesions and restoration on periodontally compromised teeth. Quintessence Int 2001;32:111–8.
[22] Peumans M, Kanumilli P, Munck J De, Landuyt K Van, Lambrechts P, Meerbeek B Van. Clinical effectiveness of contemporary adhesives : A systematic review of current clinical trials 2005:864–81. doi:10.1016/j.dental.2005.02.003.
[23] Pucci CR, Barbosa NR, Bresciani E, Yui KC, Huhtala MFR, Barcellos DC, et al. Influence of Dentin Deproteinization on Bonding Degradation: 1-year Results. J Contemp Dent Pract 2016;17:985–9.
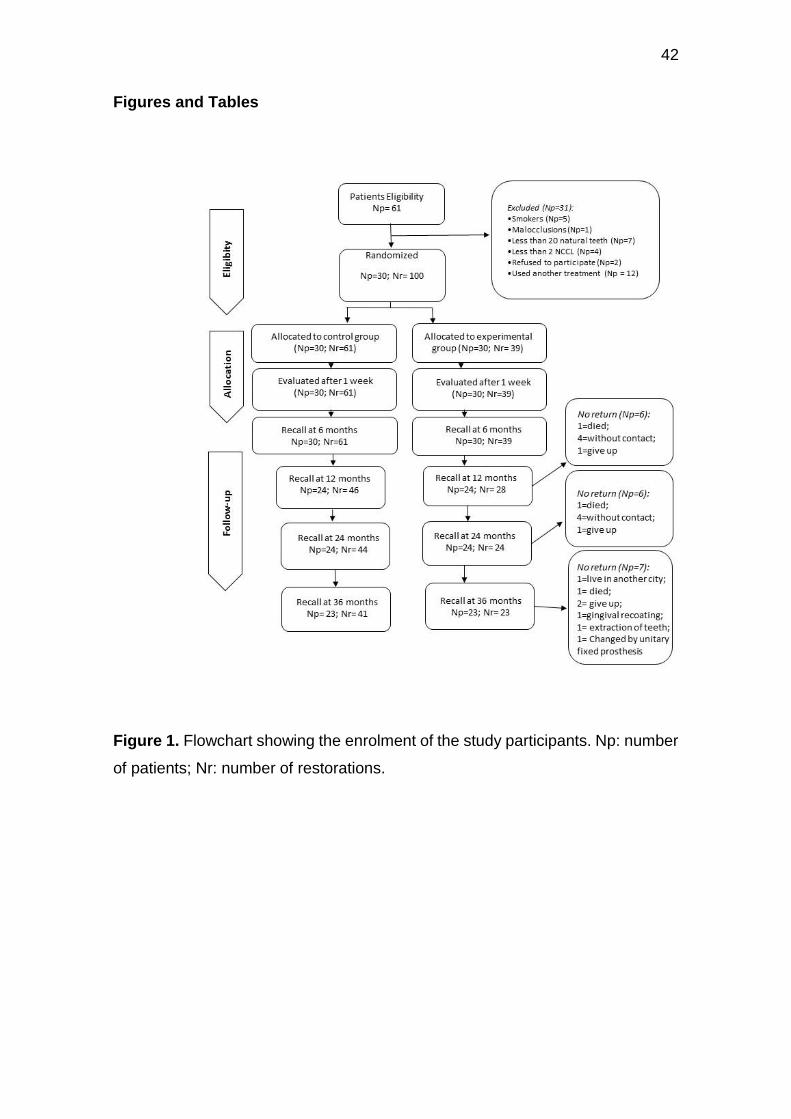
42
Figures and Tables
Figure 1. Flowchart showing the enrolment of the study participants. Np: number
of patients; Nr: number of restorations.
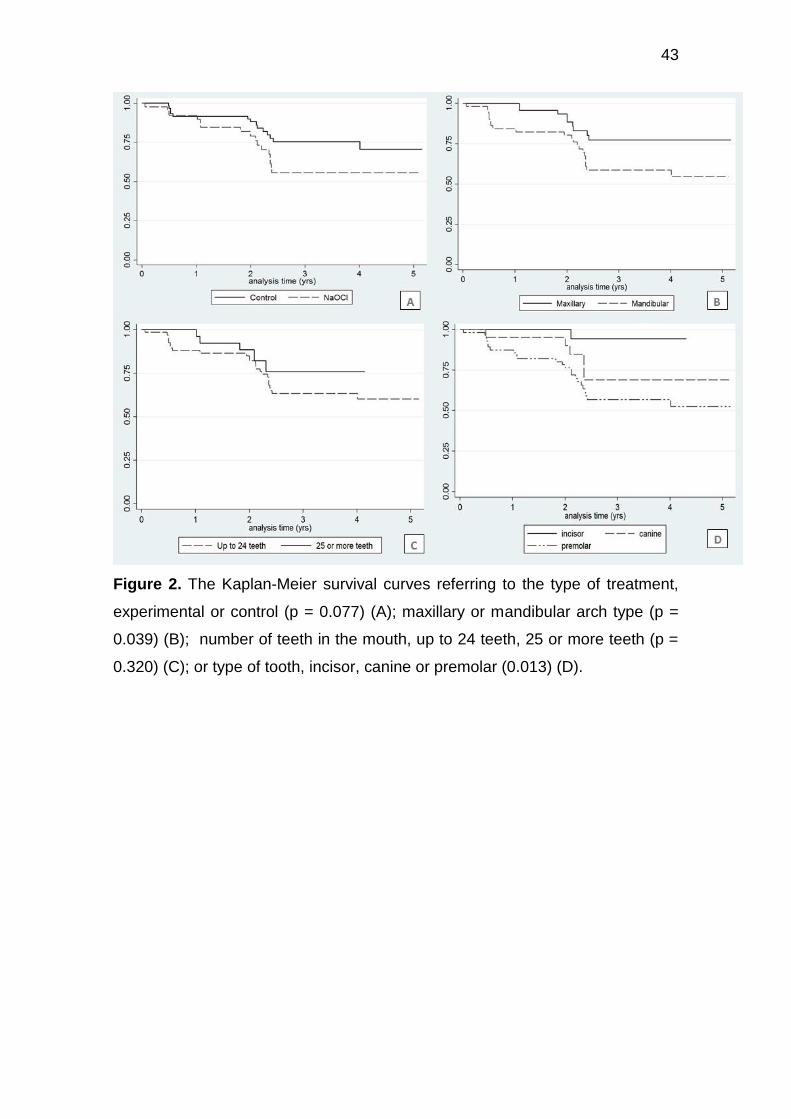
43
Figure 2. The Kaplan-Meier survival curves referring to the type of treatment,
experimental or control (p = 0.077) (A); maxillary or mandibular arch type (p =
0.039) (B); number of teeth in the mouth, up to 24 teeth, 25 or more teeth (p =
0.320) (C); or type of tooth, incisor, canine or premolar (0.013) (D).
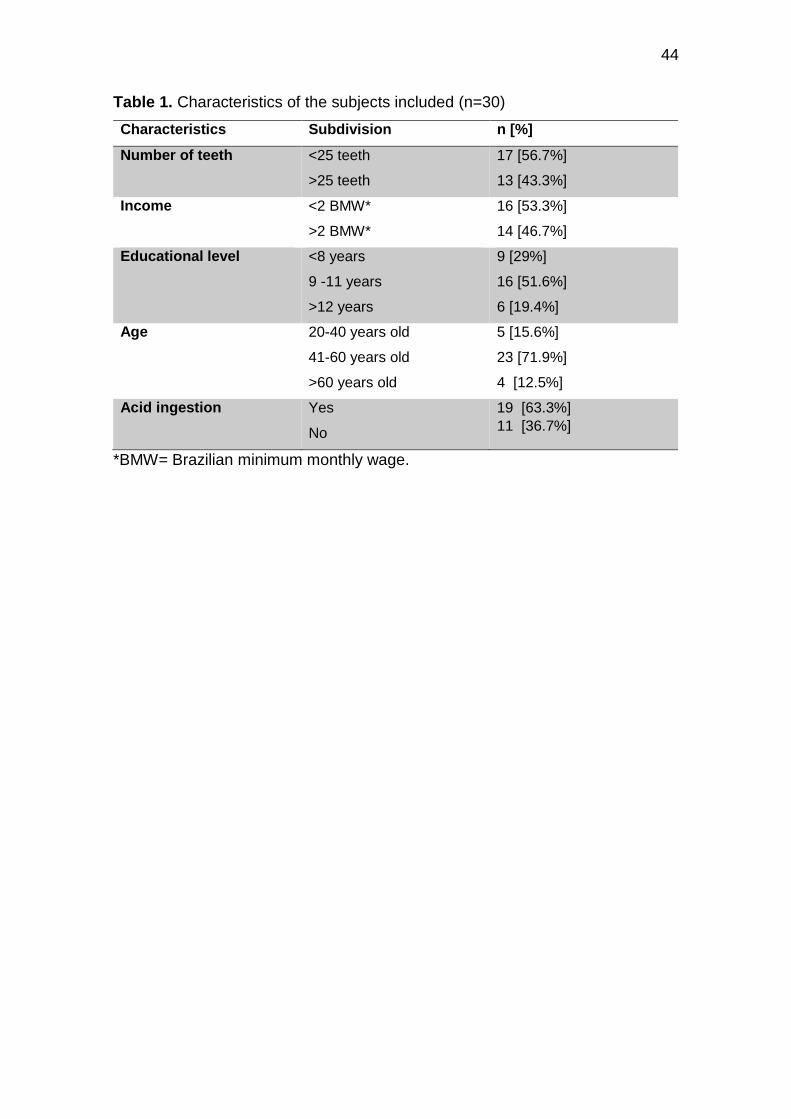
44
Table 1. Characteristics of the subjects included (n=30)
Characteristics Subdivision n [%]
Number of teeth <25 teeth
>25 teeth
17 [56.7%]
13 [43.3%]
Income <2 BMW*
>2 BMW*
16 [53.3%]
14 [46.7%]
Educational level <8 years
9 -11 years
>12 years
9 [29%]
16 [51.6%]
6 [19.4%]
Age 20-40 years old
41-60 years old
>60 years old
5 [15.6%]
23 [71.9%]
4 [12.5%]
Acid ingestion Yes
No
19 [63.3%]
11 [36.7%]
*BMW= Brazilian minimum monthly wage.

45
Table 2. Characteristics of the non-carious cervical lesions distributed in the
treatment groups (n=100)
Characteristics Subdivision Control group
N [%]
Test group
N [%]
Type of teeth Incisor
Canine
Premolar
15[71.4%]
15 [71.4%]
31 [53.5%]
6[28.6%]
6 [28.6%]
27 [46.6%]
Position Maxillary
Mandibular
34[69.4%]
27 [52.9%]
15 [30.6%]
24 [47%]
Depth <1 mm
1 up to 3 mm
3 up to 4 mm
>4 mm
28 [58.3%]
29 [63%]
1 [50%]
2 [100%]
20 [41.7%]
17 [37%]
1 [50%]
0 [0%]
Height <1 mm
1 up to 3 mm
3 up to 4 mm
>4mm
3 [42.9%]
30 [61.2%]
20 [62.5%]
4 [66.7%]
4 [57.1%]
19 [38.8%]
12 [37.5%]
2 [33.3%]
Cavity shape U saucer-shaped
V wedge-shaped
26 [65%]
35 [58.3%]
14 [35%]
25 [41.7%]
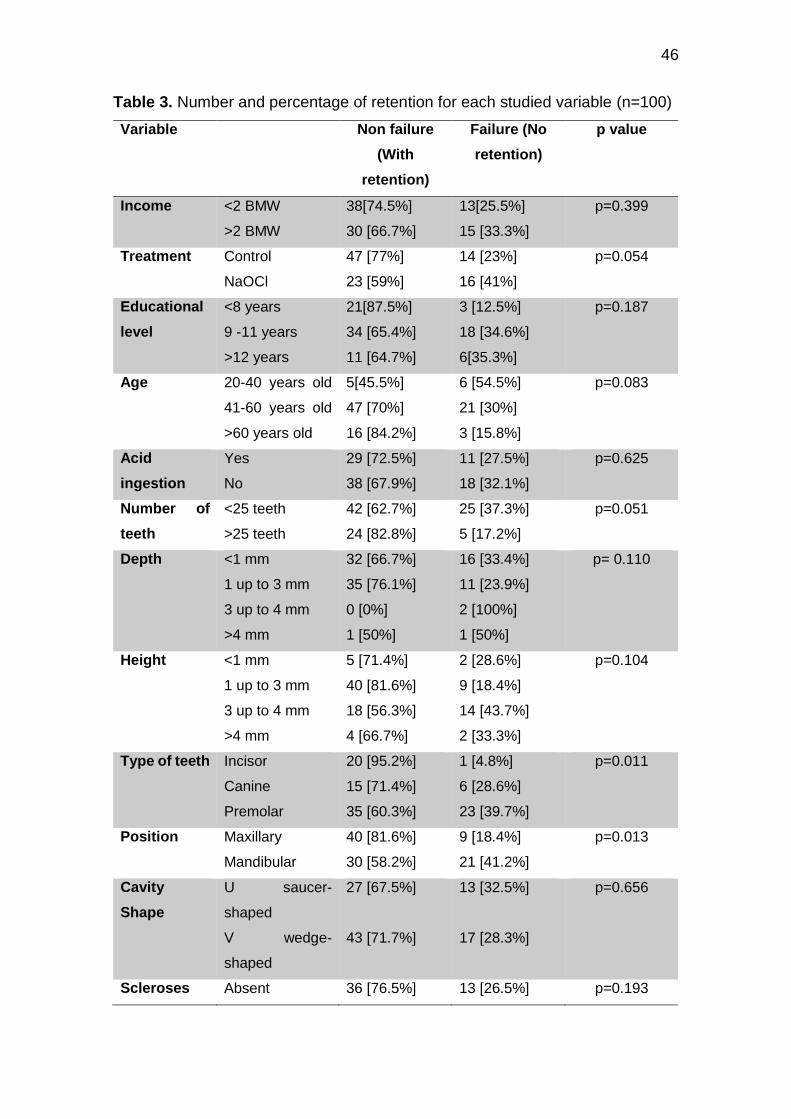
46
Table 3. Number and percentage of retention for each studied variable (n=100)
Variable Non failure
(With
retention)
Failure (No
retention)
p value
Income <2 BMW
>2 BMW
38[74.5%]
30 [66.7%]
13[25.5%]
15 [33.3%]
p=0.399
Treatment Control
NaOCl
47 [77%]
23 [59%]
14 [23%]
16 [41%]
p=0.054
Educational
level
<8 years
9 -11 years
>12 years
21[87.5%]
34 [65.4%]
11 [64.7%]
3 [12.5%]
18 [34.6%]
6[35.3%]
p=0.187
Age 20-40 years old
41-60 years old
>60 years old
5[45.5%]
47 [70%]
16 [84.2%]
6 [54.5%]
21 [30%]
3 [15.8%]
p=0.083
Acid
ingestion
Yes
No
29 [72.5%]
38 [67.9%]
11 [27.5%]
18 [32.1%]
p=0.625
Number of
teeth
<25 teeth
>25 teeth
42 [62.7%]
24 [82.8%]
25 [37.3%]
5 [17.2%]
p=0.051
Depth <1 mm
1 up to 3 mm
3 up to 4 mm
>4 mm
32 [66.7%]
35 [76.1%]
0 [0%]
1 [50%]
16 [33.4%]
11 [23.9%]
2 [100%]
1 [50%]
p= 0.110
Height <1 mm
1 up to 3 mm
3 up to 4 mm
>4 mm
5 [71.4%]
40 [81.6%]
18 [56.3%]
4 [66.7%]
2 [28.6%]
9 [18.4%]
14 [43.7%]
2 [33.3%]
p=0.104
Type of teeth Incisor
Canine
Premolar
20 [95.2%]
15 [71.4%]
35 [60.3%]
1 [4.8%]
6 [28.6%]
23 [39.7%]
p=0.011
Position Maxillary
Mandibular
40 [81.6%]
30 [58.2%]
9 [18.4%]
21 [41.2%]
p=0.013
Cavity
Shape
U saucer-
shaped
V wedge-
shaped
27 [67.5%]
43 [71.7%]
13 [32.5%]
17 [28.3%]
p=0.656
Scleroses Absent 36 [76.5%] 13 [26.5%] p=0.193
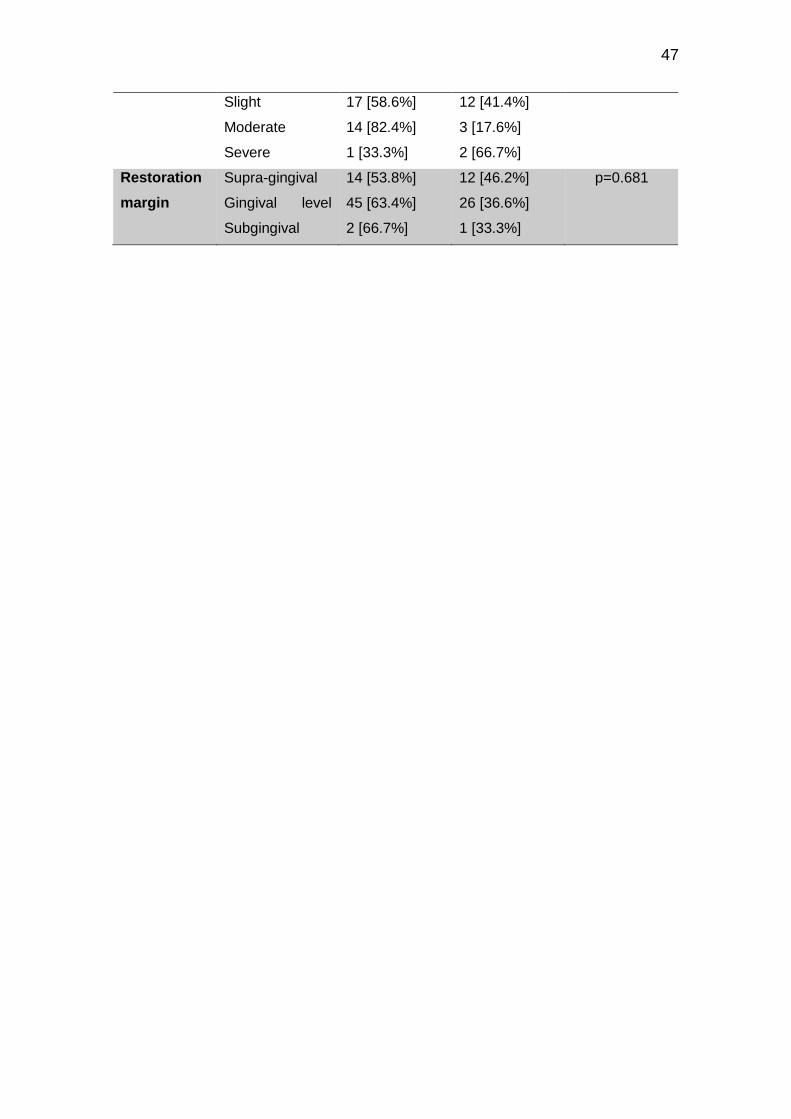
47
Slight
Moderate
Severe
17 [58.6%]
14 [82.4%]
1 [33.3%]
12 [41.4%]
3 [17.6%]
2 [66.7%]
Restoration
margin
Supra-gingival
Gingival level
Subgingival
14 [53.8%]
45 [63.4%]
2 [66.7%]
12 [46.2%]
26 [36.6%]
1 [33.3%]
p=0.681
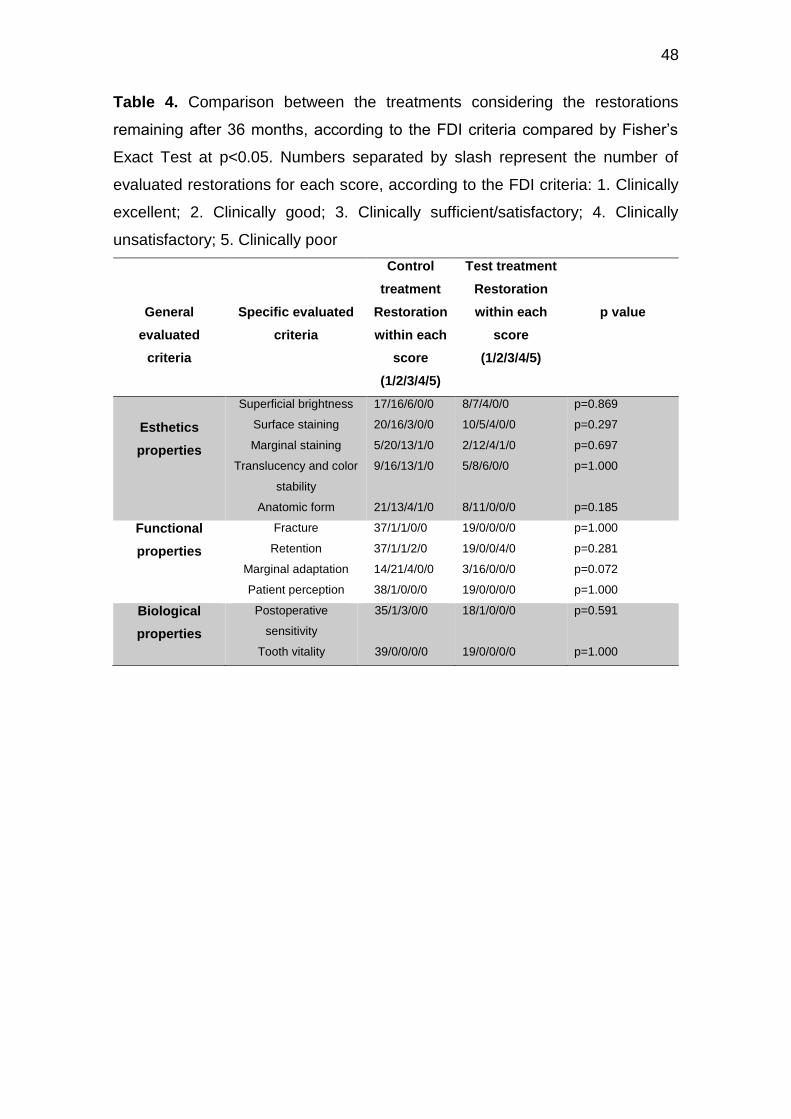
48
Table 4. Comparison between the treatments considering the restorations
remaining after 36 months, according to the FDI criteria compared by Fisher’s
Exact Test at p<0.05. Numbers separated by slash represent the number of
evaluated restorations for each score, according to the FDI criteria: 1. Clinically
excellent; 2. Clinically good; 3. Clinically sufficient/satisfactory; 4. Clinically
unsatisfactory; 5. Clinically poor
General
evaluated
criteria
Specific evaluated
criteria
Control
treatment
Restoration
within each
score
(1/2/3/4/5)
Test treatment
Restoration
within each
score
(1/2/3/4/5)
p value
Esthetics
properties
Superficial brightness
Surface staining
Marginal staining
Translucency and color
stability
Anatomic form
17/16/6/0/0
20/16/3/0/0
5/20/13/1/0
9/16/13/1/0
21/13/4/1/0
8/7/4/0/0
10/5/4/0/0
2/12/4/1/0
5/8/6/0/0
8/11/0/0/0
p=0.869
p=0.297
p=0.697
p=1.000
p=0.185
Functional
properties
Fracture
Retention
Marginal adaptation
Patient perception
37/1/1/0/0
37/1/1/2/0
14/21/4/0/0
38/1/0/0/0
19/0/0/0/0
19/0/0/4/0
3/16/0/0/0
19/0/0/0/0
p=1.000
p=0.281
p=0.072
p=1.000
Biological
properties
Postoperative
sensitivity
Tooth vitality
35/1/3/0/0
39/0/0/0/0
18/1/0/0/0
19/0/0/0/0
p=0.591
p=1.000
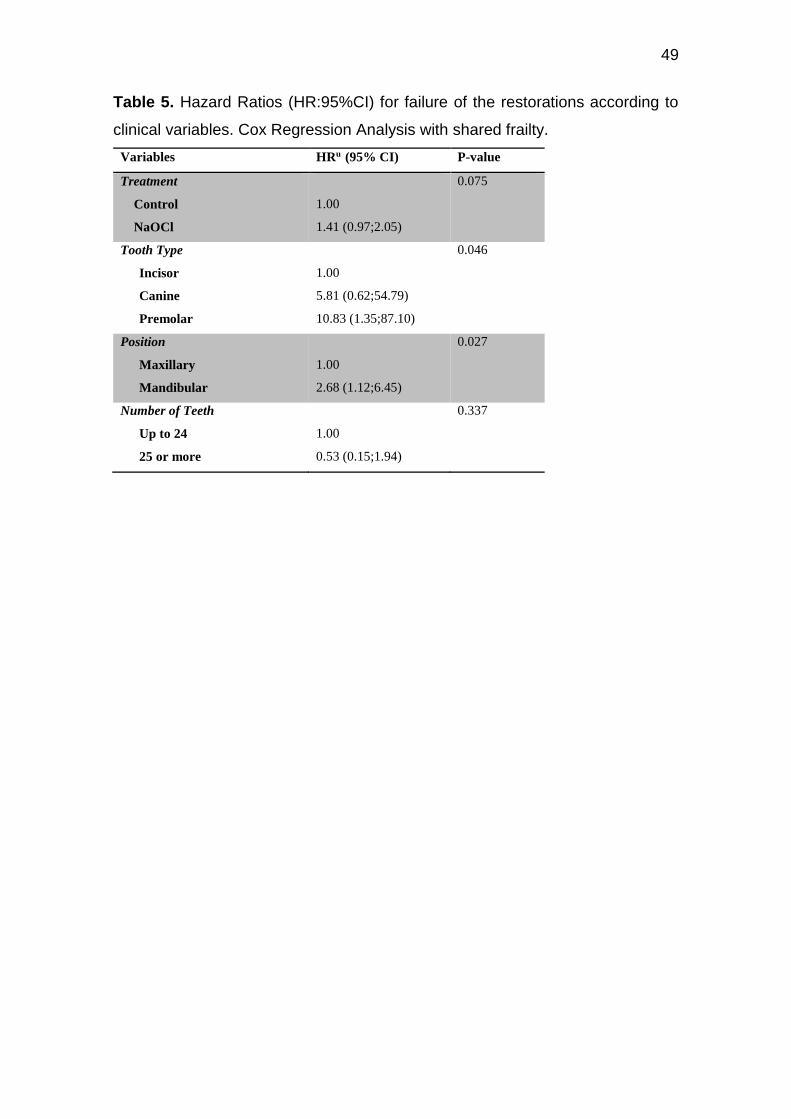
49
Table 5. Hazard Ratios (HR:95%CI) for failure of the restorations according to
clinical variables. Cox Regression Analysis with shared frailty.
Variables HRu (95% CI) P-value
Treatment
Control
NaOCl
1.00
1.41 (0.97;2.05)
0.075
Tooth Type
Incisor
Canine
Premolar
1.00
5.81 (0.62;54.79)
10.83 (1.35;87.10)
0.046
Position
Maxillary
Mandibular
1.00
2.68 (1.12;6.45)
0.027
Number of Teeth
Up to 24
25 or more
1.00
0.53 (0.15;1.94)
0.337
50
Capítulo 3
Retention of non-carious cervical restorations placed under rubber dam or
cotton rolls isolation: 60 months follow-up of a randomized controlled
clinical trial
Abstract
Objective: This randomized controlled clinical trial evaluated the effects of two
methods of isolating the operative field on the 60-months performances of
cervical restorations.
Methods: Thirty-six patients with at least two noncarious cervical lesions (NCCLs)
were enrolled in the study. A total of 174 NCCLs were randomized into the
following groups: (VAN MEERBEEK et al., 2010) isolation performed with rubber
dam and gingival retraction clamp, and (PEUMANS et al., 2005) isolation
provided with cotton rolls and gingival retraction cord. Both methods were used
with a saliva suction device. An all-in-one self-etching adhesive (Adper Easy One,
3M ESPE) and a nanofilled composite resin (Filtek Z350, 3M ESPE) were used
for both groups. The restorations were blindly assessed one week (baseline), 6,
12, 24 and 60 months after placement, using the FDI criteria. Clinical
performance was recorded in terms of material fracture and restoration retention,
marginal adaptation, marginal staining and postoperative hypersensitivity.
Results: The recall rate at 60 months was 89%. Fifteen restorations were lost
over this period, resulting in an overall annual failure rate after 5 years of 2.6%.
The Kaplan-Meier survival curves showed no statistically significant difference
between the type of isolation (p = 0.283).
Conclusion: Both methods of dental isolation do not directly influence the
retention and clinical success of restorations of non-carious cervical lesions.

51
Significance: Both methods of dental isolation work well for the retention and
clinical success of NCCL restorations when properly performed correctly by the
operator.
Keywords: adhesives; composite resins; controlled clinical trial; dental
restoration; rubber dam; self-etch.
Introduction
The outcomes of bonded restorations not only depend on the adhesive
category per se but also on operative aspects, such as the method used to isolate
the operative field from the rest of the oral cavity [3]. It is generally accepted that
adhesive restorations must be placed under well-controlled moisture conditions
[4] which suggests that the rubber dam is the ideal method to accomplish this in
routine restorative dentistry. Although a meta-analysis revealed no influence of
the isolation type on the clinical performance of cervical restorations [5], few
studies have addressed this important aspect. In a recent review, which sought
to evaluate the relationship between the type of dental isolation and the retention
of the restorations, included 4 articles, and only 1 of them were with restorations
in NCCL. This shows the lack of studies with good methodology and evidence of
quality regarding the subject [6].
Furthermore, no randomized clinical trial (RCT) has been designed
specifically to evaluate the role of isolation method in the longevity of restorations
bonded with the simplified self-etch adhesives (SEAs) in non carious cervical
lesions. These adhesives use non-rinse acidic monomers that demineralise and
infiltrate the dental substrate simultaneously to the same depth [1].
Thus, the aim of this randomized controlled trial was to evaluate the effects
of two isolation methods of the operative field on the clinical performance of
NCCL restorations. The null hypothesis to be tested was that no significant
differences on clinical performance between restorations placed under different
isolation methods will be detected after a 60- months follow-up.
Materials and Methods
Study design, sample size and ethics considerations
This study was designed as a split-mouth, single-blind (clinical evaluators
blinded), prospective and randomized controlled clinical trial. NCCLs were
randomly assigned to two different treatment groups, according to the method
used to isolate the operative field. The sample size was based on information
from a previous 6-month clinical trial [7]. The protocol and the consent form for
this study were approved by the Ethics Committee (CEP) of the School of

52
Dentistry of the Federal University of Pelotas (FO-UFPel), (PROTOCOL
093/2009). Before beginning the experiment, the participants signed a written
informed consent agreement to participate in the trial.
Patient and lesion selection
Recruitment of subjects was performed at the clinics of School of Dentistry
(Federal University of Pelotas, Pelotas, RS, Brazil) through advertisements,
considering patients who needed dental treatment of NCCLs. Reasons for
treatment were cervical tooth sensitivity, aesthetic complaints and/or prevention
of further tooth damage.
The eligibility criteria for volunteers were being at least 18 years old and
presenting more than one cervical lesion whose apical limit was not located below
the gingival margin, with at least 1 mm of depth in a vital permanent incisor,
canine, or premolar of the upper or the lower jaw. Typically, these defects were
situated at the facial surface of the teeth, sometimes with a small part extending
interproximally.
The patients were not admitted when any of the following criteria were
presented: (1) smoking habits; (2) severe systemic diseases; (3) active
orthodontic treatment; (4) malocclusion (Angle Class II or Class III); (5) less than
20 natural teeth in mouth; (6) absent of antagonist tooth; (7) wear facets over
more than 50% of the incisal/occlusion surface as a result of tooth attrition; (8)
caries or restorations in the area to be treated; (9) full-mouth visible plaque index
(VPI) or full-mouth gingival bleeding index (GBI) [8] more than 20%; (10) probing
depth (PD) and clinical attachment loss (CAL) values exceeding 4 mm with
bleeding on probing (BOP); and (11) unwillingness to return for follow-ups or (12)
refuse to participate.
The screening of lesions was performed using a mouth mirror, an explorer,
and a periodontal probe (University of North Carolina, Hu-Friedy, Chicago, IL,
USA). The NCCLs depths were measured by placing a probe into their deepest
part, and their heights were calculated by the distance of the most coronal and
apical points of the cavity margins. The degrees of dentin sclerosis were identified
using a scale ranked from 1 to 4 [9]. Sensitivity was measured by blowing a
stream of compressed air for 3 seconds at a distance of 2 to 3 cm, while shielding
the adjacent teeth with fingers. A visual analog scale was used with scores
ranging from 1 to 5, where 1 referred to no sensitivity, 2 to mild, 3 to moderate, 4
to considerable, and 5 to severe sensitivity. Tooth vitality was tested by the
application of an ice stick on the tooth and comparing the reaction with that of the
adjacent teeth. No attempt was made to determine the aetiology of the cervical
lesions.
Four weeks before the study began, the patients underwent a session of
dental scaling and polishing by a single operator using periodontal manual
curettes (Gracey and McCall, Trinity, São Paulo, SP, Brazil). They also received
detailed oral hygiene instructions, including a non-traumatic brushing technique

53
(coronally directed roll technique) with a soft toothbrush [10], and the use of the
dental floss.
Random assignment
A random table was used to generate the random allocation sequence of
the treatment groups among participants. This random table was assembled with
Microsoft Excel using the random number function, first generating a list with the
two possible treatments for the total number of restorations to be included in a
column, and then asking the program to make the ordination of these treatments
according to the random number generated in the next column. The random
sequence of treatments was concealed in opaque sealed envelopes by a
research (STF), not directly involved in the trial. This envelope was open only at
the time for each tooth intervention. While the first randomly selected treatment
was used for the lowest quadrant number, the second treatment was used for the
tooth with the second-lowest quadrant number (according to the FDI system).
This method was repeated for every other quadrant that required a cervical
restoration. In instances of an uneven number of NCCLs per patient, the unequal
number of lesions of one group was adjusted by restoring one more lesion in the
other group in the next patient presenting with an unequal number of cervical
lesions.
Interventions
The operative procedures were performed by two trained, skilled operators
(ANB and RLR), familiar with adhesive restorative dentistry, under the
supervision of an experienced clinician. They received thorough pre-clinical
training in the field isolation and adhesive procedures. Each operator placed an
equal number of restorations for each group.
Preoperatively, the teeth to be restored were cleaned with pumice and
water with a rubber prophylaxis cup. Subsequently, the colour of the restoration
was determined using a shade guide (Vitapan Classical, Vita, Zahnfabrik, Bad
Sackingen, Germany). No additional mechanical retention or enamel bevel was
prepared.
In order to secure moisture control of the operative field, two isolation
methods were standardized by a detailed protocol, which is briefly summarized
below.
(1) Rubber dam group: Moisture control was provided by a rubber dam and
a gingival retraction clamp placed in the cervical area of the tooth.
(2) Cotton roll group: Moisture control was provided using a labial retractor,
cotton rolls and gingival retraction cord placed into the gingival sulcus.
For both groups, a saliva suction device was held in position by an
assistant during the restorative procedure. If necessary, local anaesthesia was
given to prevent patient discomfort prior to treatment.
An all-in-one self-etch adhesive (Adper Easy One, 3M ESPE, Seefeld,
Germany) was used according to the manufacturer’s instructions (Table 1). The
54
NCLs were restored with a direct restorative nanocomposite (Filtek Z350, 3M
ESPE, Irvine, CA, USA) applied in at least two increments (not exceeding 2 mm
in thickness), using a composite hand-instrument (Hu-Friedy, Chicago, IL, USA).
Each increment was cured for 20 seconds with a LED light-curing unit (Radii-Call,
SDI, Bayswater, VI, Australia). All restorations were finished and polished with
fine- and ultra-fine-grain diamond burs (KG Sorensen, Barueri, SP, Brazil) under
water cooling, slow-speed flexible discs (Sof-Lex Pop-On, 3M ESPE, St Paul,
MN, USA), polishing paste (Prisma Gloss, Dentsply Caulk, Milford, DE, USA),
and rubber points (Enhance, Dentsply Caulk, Milford, DE, USA).
Clinical assessment
Criteria approved by the FDI World Dental Federation were used for
clinical assessment of restorations [11]. The primary clinical outcome was
material fracture and restoration retention. Secondary endpoints included the
following criteria: (1) marginal adaptation, (2) marginal staining, and (3)
postoperative hypersensitivity and preservation of tooth vitality. Each criterion
was expressed with five scores, 3 for acceptable and 2 for unacceptable (1 for
reparable and 1 for replacement). Restorations that needed repairs or
replacements were considered clinical failures, receiving scores of 4 or 5,
respectively (Table 2).
The evaluations were carried out by two independent examiners (PJ and
ASM) at 1 week (baseline), 6, 12, 24 and 60 months after the insertion of the
restoration. They were not the operators and were fully blinded to the assignment
of interventions. A Web-based training and calibration tool called e-calib
(www.ecalib.info) was used to train and calibrate the evaluators. After that, they
evaluated cervical restorations in clinical settings. A pre-evaluation agreement of
at least 80% was obtained among them. When disagreement in evaluation
occurred between the two examiners, consensus was reached by immediate re-
examination and discussion at chair side. Photo documentation was made pre-
operatively, at baseline and at recall.
Statistical analysis
Statistical analysis was performed using the Software Stata 14.2 (Stata
Corp LP, College Station, TX, USA). The same was performed by a researcher
not directly involved in the study. Frequencies of appearance of the
characteristics of both the patients and the restored lesions involved in the study
were verified through the chi-square test. The data regarding the scores received
for each criterion evaluated in the restorations according to the FDI criteria were
obtained and reported through the Fisher exact test. Survival analysis was
performed using Kaplan-Meier method. The log-rank test was used to evaluate
the existence of differences between the survival curves. Unadjusted Cox
regression models with shared frailty were used to verify the association between
treatment and the risk of failure over time, estimating the Hazard Ratios (HR) and
95% confidence intervals. All analyses considered an α=5%.
55
Results
During the recruiting period from March to December 2010, 86 subjects
were assessed for eligibility. 36 patients (12 men and 24 women) were enrolled
in the study, yielding a total of 172 restorations. The age of the included patients
varied from 19 to 69 years, and the most prevalent age group was 41-60 years
old (61.1%). The educational level of the participants had a balanced distribution
among the 3 levels of classification, and the highest concentration of individuals
was in the lowest income classification (Table 3). The flow diagram indicates the
number of participants through each stage of the trial (Figure 1).
The NCCLs included in the study were pre-operatively categorized in
terms of tooth distribution, shape, depth and height of the lesions, degree of
sclerosis, and sensitivity (Table 4). A rate of 95.3% of the restorations were made
at the gingival level. Most restorations (71.8%) were placed on pre-molars. The
most prevalent NCCL cavity form was U-shaped (68,4%). The type of isolation
for each restored tooth was randomized and therefore obtained a similar
distribution for the two groups studied.
The FDI criteria that were used to evaluate the quality of the restorations
in each of the revaluations were subjected to Fisher's exact test. (Table 5). When
evaluated at 60 months, most restorations obtained satisfactory scores. Due to
the fact that we are comparing types of isolation in the execution of these
restorations, two characteristics should be observed with caution, marginal
staining (p = 0.549) and marginal adaptation (p = 0.041). The scores obtained by
these two criteria were mostly satisfactory clinically.
The annual failure rate after 5 years for absolute isolation was 3.0%, and
the annual failure rate after 5 years for relative isolation was 1.9% . The Kaplan-
Meier survival curves show no statistically significant difference (p=0.283)
between the type of isolation, ruber dam or cottom roll (Table 2).
For failure of the restorations according to clinical variables, Cox
Regression Analysis with shared frailty (Table 6) was performed. None of the
evaluated criteria, characteristics of lesions and patients, had a statistically
significant association (p <0.05).
Discussion
The most common methods to isolate the operative field include rubber
dam and cotton rolls, both frequently combined with saliva suction device. The
literature emphasises that resin-composite restorations cannot be placed
successfully in a cavity surface that is contaminated by blood or saliva [4],
especially for restorations whose cervical margin is in direct contact with the
periodontal tissues, as is the case of class V restorations in non-carious cervical
lesions. Beyond moisture control, the protection of the patient from possible
aspiration and ingestion of dental foreign objects is an advantage only offered by
the use of the rubber dam in dental practise [12] . Meanwhile, most clinicians are
not sure which isolation method to choose and also show reluctance to use the
rubber dam during the operative dentistry procedures [13]. According to a 10-

56
year clinical study, similar performances were reported for posterior restorations
placed under cotton rolls and rubber dam isolation [14]. Additionally, a meta-
analysis showed that teeth restored with rubber dam presented statistically higher
retention rates than those without [15]. These results were somewhat confirmed
by a latter Cochrane review [6]. But the included studies were rated as low quality
with high risk of bias, and most of the included studies were evaluating ART
restorations [6]. However, there is still disagreement in the literature between the
results found in the studies regarding the influence of the type of dental isolation
and the longevity of the restorations, specially in situations such as the restoration
of NCCL is involved.
The studies showing results favouring the use of rubber dam were not
clear regarding the details of the technique adopted to isolate the operatory field
with cotton rolls. Usually, in order to achieve the best results of using cotton rolls,
other devices are used, such as especial suction apparatus, mouth openers, and
even retraction cords in the gingival sulcus. These combination of devices can
optimize the moisture control process. In fact, it seems reasonable to state that
regardless of the technique of choice, what really matters is to keep the operatory
field dry and free of contaminants during the adhesive procedures and during the
composite placement.
Several long term studies have confirmed that overall annual failure rates
(AFR) of restorations are not deeply affected by the type of isolation used. Taking
as an example, studies reporting on posterior composite restoration evaluated
after 17 and 22 years [16,17] using cotton rolls reported similar AFRs compared
to studies evaluating extensive restorations [18] placed without rubber dam over
more than a decade or studies that followed restorations for 30 years placed with
both, with or without rubber dam. It is worthy to emphasise that posterior
restorations are even more critical for operatory field isolation, especially in
molars in the lower arch. In more favourable situations, such as the buccal
surface of anterior teeth, keeping the moisture control with cotton rolls is expected
to be easier.
The sealing capacity of restorations has often been assessed by the
integrity and colour changes along part or all of the margins [11], however,
findings were considered clinically acceptable, which suggests that the isolation
method may have played an important role in the early deterioration of marginal
integrity. Additionally, these minor shortcomings could be attributed to the
superficial etching pattern of an ultra-mild self-etch adhesive. A similar
phenomenon of increased marginal defects and superficial discoloration was also
observed in a long-term clinical trial evaluation of a mild two-step self-etch
adhesive [19]. That is why the literature so far indicates selective phosphoric-acid
etching of the enamel cavity margins, followed by applying an ultra-mild Self-Etch
Adhesive (SEA). The purpose of this combined approach is to provide a better
self-etch interaction at enamel with favourable perspectives at dentin [1]. A recent
systematic review has shown that the selective enamel etching in non-carious
cervical lesions for self-adhesive adhesives can improve the performance of resin
57
composite cervical restorations and can produce restorations with higher
longevity [20]. Therefore restorations made with two-step self-etching and three-
step etch-and-rinse adhesive systems tend to have better clinical responses and
are therefore preferred to the use of one step self-etching adhesive systems
[15].Our study used the SEA system, and when the marginal adaptation of the
restorations after 5 years of follow-up was verified, there was a difference when
compared to the type of isolation, where the restorations that were made with
rubber dam had worse FDI evaluation criteria for marginal adaptation than the
restorations made with the relative isolation (p = 0.041).
Maybe the main challenge for dental adhesives is to provide an equally
effective bond to hard tissues of a different nature. Non carious class-V lesions
exhibit margins located in enamel, as well as in dentin, high degrees of sclerosis,
heterogeneous hyper-mineralized layer, and denatured collagen, seem to make
difficult the bonding in such clinically relevant substrates [21,22]. Nevertheless,
lesions were not excluded from the screening based on the proportion of margin
involving enamel and dentin, nor on the degree of dentin sclerosis. On the other
hand, the authors recognize that some specific habits of patients, such as poor
oral hygiene, smoking, or bruxism, may influence the clinical outcomes [11]. For
this reason, patients presenting severe wear facets were excluded from the
present study. It was assumed that wear facets indicate a higher concentration
of occlusal loads on the area, contributing to a higher detachment rate for
restorations. Then again, this exclusion criterion prevents us from extrapolating
our results to patients with parafunctional disorders.
Conclusion
The type of dental isolation does not directly influence the adaptation of
the restorations over time, making it no difference in the number of failures
between the groups studied.
Acknowledgements
This paper is based on a thesis submitted to the Graduate Program in
Dentistry, Federal University of Pelotas. Fontes ST held a PhD scholarship from
the National Council for Scientific and Technological Development (CNPq) during
this study. The authors also thank the staff members, who were fundamental in
the conduct of this clinical study, especially Ângelo Niemczewski Bobrowski and
Ronaldo Luiz Rossi for placing all the composite restorations.

58
References
[1] B. Van Meerbeek, K. Yoshihara, Y. Yoshida, A. Mine, D.M. J, V.L.K. L, State of the art of self-etch adhesives, Dent. Mater. 27 (2010) 17–28. doi:10.1016/j.dental.2010.10.023.
[2] M. Peumans, P. Kanumilli, J. De Munck, K. Van Landuyt, P. Lambrechts, B. Van Meerbeek, Clinical effectiveness of contemporary adhesives : A systematic review of current clinical trials, (2005) 864–881. doi:10.1016/j.dental.2005.02.003.
[3] F.F. Demarco, M.B. Corrêa, M.S. Cenci, R.R. Moraes, N.J.M. Opdam, Longevity of posterior composite restorations: Not only a matter of materials, Dent. Mater. 28 (2012) 87–101. doi:10.1016/j.dental.2011.09.003.
[4] ADA Council on Scientific Affairs, Direct and indirect restorative materials., J. Am. Dent. Assoc. 134 (2003) 463–72. http://www.ncbi.nlm.nih.gov/pubmed/12733780 (accessed December 1, 2016).
[5] S.D. Heintze, C. Ruffieux, V. Rousson, Clinical performance of cervical restorations — A meta-analysis, 6 (2010) 993–1000. doi:10.1016/j.dental.2010.06.003.
[6] Y. Wang, C. Li, H. Yuan, M.C.M. Wong, J. Zou, Z. Shi, X. Zhou, Rubber dam isolation for restorative treatment in dental patients, Cochrane Database Syst. Rev. 2016 (2016). doi:10.1002/14651858.CD009858.pub2.
[7] A.D. Loguercio, A. Costenaro, A.P. Silveira, N.R. Ribeiro, T.R. Rossi, A. Reis, A six-month clinical study of a self-etching and an etch-and-rinse adhesive applied as recommended and after doubling the number of adhesive coats., J. Adhes. Dent. 8 (2006) 255–61. http://www.ncbi.nlm.nih.gov/pubmed/16958291 (accessed December 1, 2016).
[8] J. Ainamo, I. Bay, Problems and proposals for recording gingivitis and plaque., Int. Dent. J. 25 (1975) 229–35. http://www.ncbi.nlm.nih.gov/pubmed/1058834 (accessed December 2, 2016).
[9] A. V Ritter, H.O. Heymann, E.J. Swift, J.R. Sturdevant, A.D. Wilder, Clinical evaluation of an all-in-one adhesive in non-carious cervical lesions with different degrees of dentin sclerosis., Oper. Dent. 33 (2008) 370–378. doi:10.2341/07-128.
[10] V.R. Santos, J.A. Lucchesi, S.C. Cortelli, C.M. Amaral, M. Feres, P.M. Duarte, Effects of Glass Ionomer and Microfilled Periodontal Tissue and Subgingival Biofilm : A 6-Month Evaluation, 78 (2007). doi:10.1902/jop.2007.070032.
[11] R. Hickel, A. Peschke, M. Tyas, I. Mjör, S. Bayne, M. Peters, K.-A. Hiller, R. Randall, G. Vanherle, S.D. Heintze, FDI World Dental Federation - clinical criteria for the evaluation of direct and indirect restorations. Update and clinical examples., J. Adhes. Dent. 12 (2010) 259–72. doi:10.3290/j.jad.a19262.
[12] K.K. Tiwana, T. Morton, P.S. Tiwana, Aspiration and ingestion in dental practice: a 10-year institutional review., J. Am. Dent. Assoc. 135 (2004) 1287–91. http://www.ncbi.nlm.nih.gov/pubmed/15493393 (accessed December 2, 2016).
[13] G.H. Gilbert, M.S. Litaker, D.J. Pihlstrom, F. Georgia, P. Dental, Operative Dentistry Procedures : Findings From The Dental PBRN, (2010) 491–499. doi:10.2341/09-287C.
[14] A. Raskin, J.C. Setcos, J. Vreven, N.H. Wilson, Influence of the isolation method on the 10-year clinical behaviour of posterior resin composite restorations., Clin.

59
Oral Investig. 4 (2016) 148–52. doi:10.1007/s007840000040148.784. [15] E. Mahn, V. Rousson, S. Heintze, Meta-Analysis of the Influence of Bonding
Parameters on the Clinical Outcome of Tooth-colored Cervical Restorations., J. Adhes. Dent. 17 (2015) 391–403. doi:10.3290/j.jad.a35008.
[16] P.A. da Rosa Rodolpho, M.S. Cenci, T.A. Donassollo, A.D. Loguércio, F.F. Demarco, A clinical evaluation of posterior composite restorations: 17-year findings, J. Dent. 34 (2006) 427–435. doi:10.1016/j.jdent.2005.09.006.
[17] P.A. Da Rosa Rodolpho, T.A. Donassollo, M.S. Cenci, A.D. Loguércio, R.R. Moraes, E.M. Bronkhorst, N.J.M. Opdam, F.F. Demarco, 22-Year clinical evaluation of the performance of two posterior composites with different filler characteristics, Dent. Mater. 27 (2011) 955–963. doi:10.1016/j.dental.2011.06.001.
[18] N.J.M. Opdam, E.M. Bronkhorst, B. a C. Loomans, M.C.D.N.J.M. Huysmans, 12-Year Survival of Composite Vs. Amalgam Restorations., J. Dent. Res. 89 (2010) 1063–1067. doi:10.1177/0022034510376071.
[19] M. Peumans, J. De Munck, K.L. Van Landuyt, A. Poitevin, P. Lambrechts, B. Van Meerbeek, Eight-year clinical evaluation of a 2-step self-etch adhesive with and without selective enamel etching, Dent. Mater. 26 (2010) 1176–1184. doi:10.1016/j.dental.2010.08.190.
[20] A. Szesz, S. Parreiras, A. Reis, A. Loguercio, Selective enamel etching in cervical lesions for self-etch adhesives: A systematic review and meta-analysis, J. Dent. 53 (2016) 1–11. doi:10.1016/j.jdent.2016.05.009.
[21] J. Perdigão, Dentin bonding — Variables related to the clinical situation and the substrate treatment, 6 (2009) 24–37. doi:10.1016/j.dental.2009.11.149.
[22] F.R. Tay, D.H. Pashley, Resin bonding to cervical sclerotic dentin : A review, (2004) 173–196. doi:10.1016/j.jdent.2003.10.009.
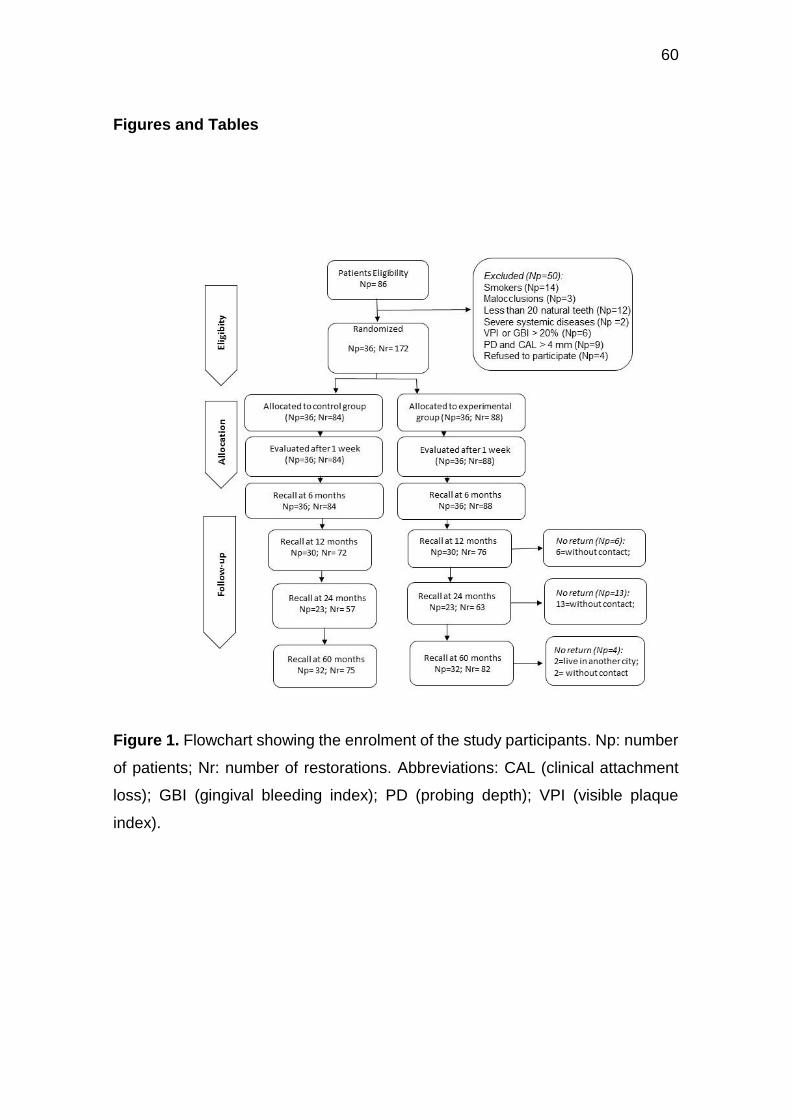
60
Figures and Tables
Figure 1. Flowchart showing the enrolment of the study participants. Np: number
of patients; Nr: number of restorations. Abbreviations: CAL (clinical attachment
loss); GBI (gingival bleeding index); PD (probing depth); VPI (visible plaque
index).

61
Figure 2. The Kaplan-Meier survival curves referring to the type of isolation, ruber
dam or cottom roll ( p= 0.283)
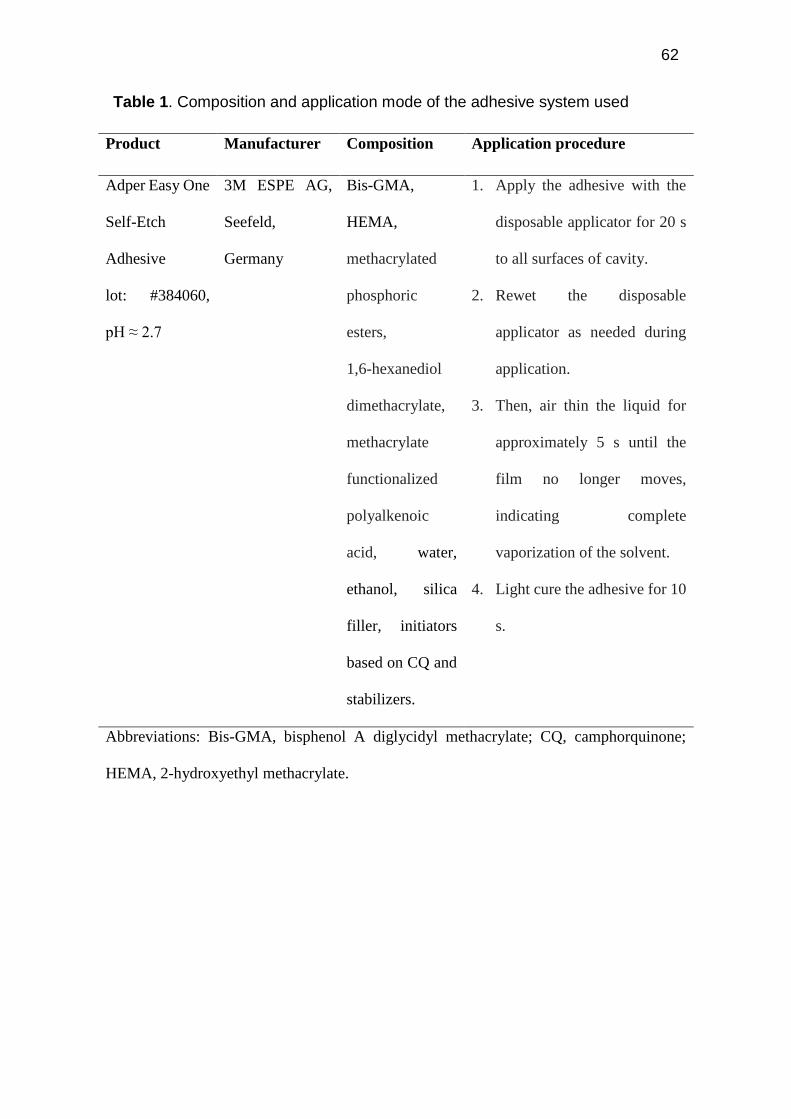
62
Table 1. Composition and application mode of the adhesive system used
Product Manufacturer Composition Application procedure
Adper Easy One
Self-Etch
Adhesive
lot: #384060,
pH ≈ 2.7
3M ESPE AG,
Seefeld,
Germany
Bis-GMA,
HEMA,
methacrylated
phosphoric
esters,
1,6-hexanediol
dimethacrylate,
methacrylate
functionalized
polyalkenoic
acid, water,
ethanol, silica
filler, initiators
based on CQ and
stabilizers.
1. Apply the adhesive with the
disposable applicator for 20 s
to all surfaces of cavity.
2. Rewet the disposable
applicator as needed during
application.
3. Then, air thin the liquid for
approximately 5 s until the
film no longer moves,
indicating complete
vaporization of the solvent.
4. Light cure the adhesive for 10
s.
Abbreviations: Bis-GMA, bisphenol A diglycidyl methacrylate; CQ, camphorquinone;
HEMA, 2-hydroxyethyl methacrylate.
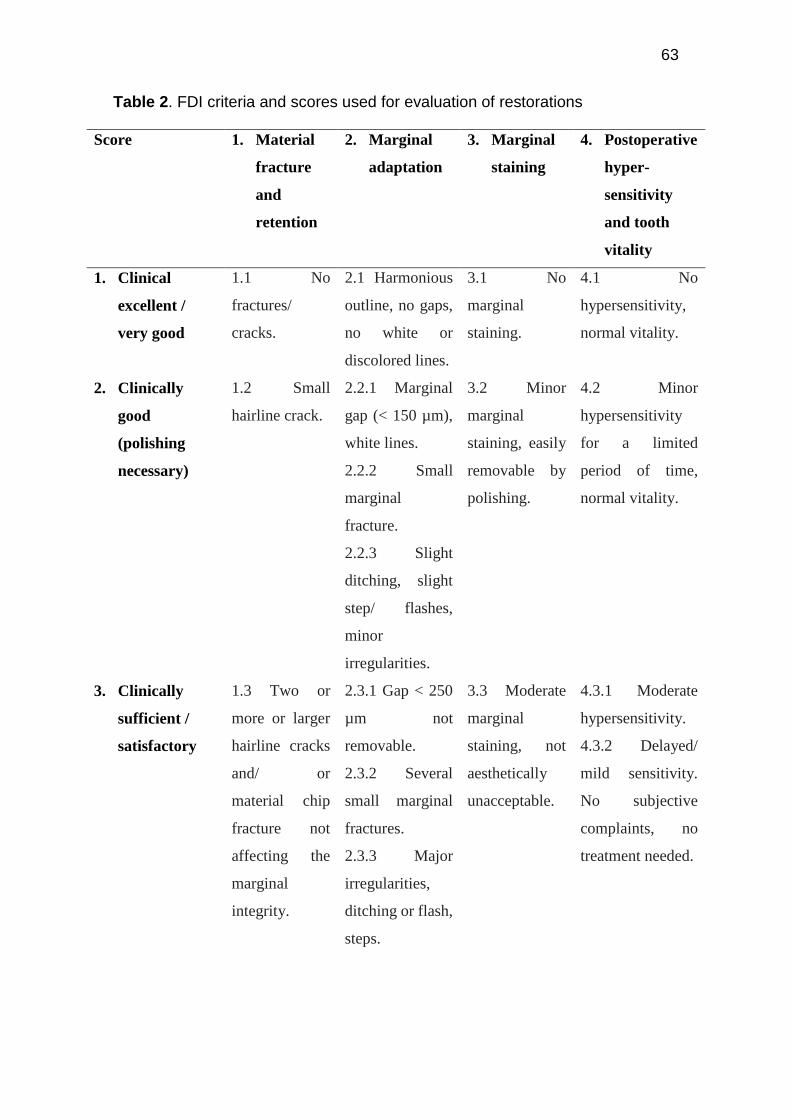
63
Table 2. FDI criteria and scores used for evaluation of restorations
Score 1. Material
fracture
and
retention
2. Marginal
adaptation
3. Marginal
staining
4. Postoperative
hyper-
sensitivity
and tooth
vitality
1. Clinical
excellent /
very good
1.1 No
fractures/
cracks.
2.1 Harmonious
outline, no gaps,
no white or
discolored lines.
3.1 No
marginal
staining.
4.1 No
hypersensitivity,
normal vitality.
2. Clinically
good
(polishing
necessary)
1.2 Small
hairline crack.
2.2.1 Marginal
gap (< 150 µm),
white lines.
2.2.2 Small
marginal
fracture.
2.2.3 Slight
ditching, slight
step/ flashes,
minor
irregularities.
3.2 Minor
marginal
staining, easily
removable by
polishing.
4.2 Minor
hypersensitivity
for a limited
period of time,
normal vitality.
3. Clinically
sufficient /
satisfactory
1.3 Two or
more or larger
hairline cracks
and/ or
material chip
fracture not
affecting the
marginal
integrity.
2.3.1 Gap < 250
µm not
removable.
2.3.2 Several
small marginal
fractures.
2.3.3 Major
irregularities,
ditching or flash,
steps.
3.3 Moderate
marginal
staining, not
aesthetically
unacceptable.
4.3.1 Moderate
hypersensitivity.
4.3.2 Delayed/
mild sensitivity.
No subjective
complaints, no
treatment needed.
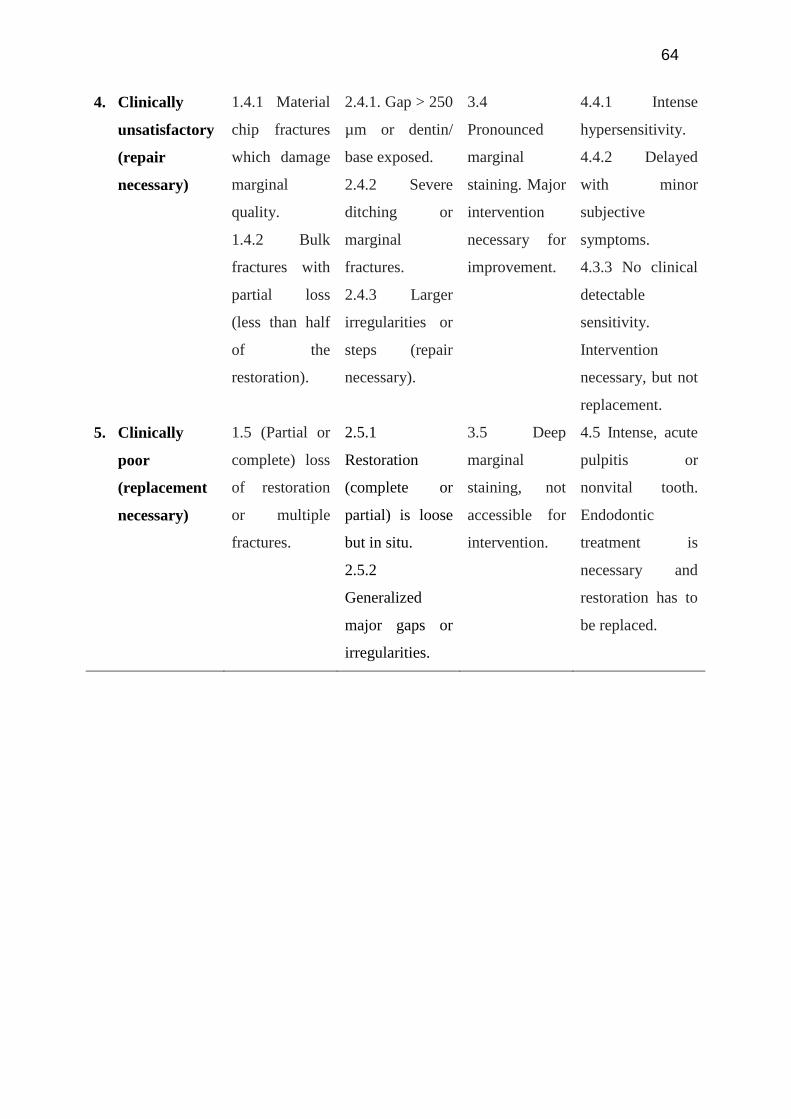
64
4. Clinically
unsatisfactory
(repair
necessary)
1.4.1 Material
chip fractures
which damage
marginal
quality.
1.4.2 Bulk
fractures with
partial loss
(less than half
of the
restoration).
2.4.1. Gap > 250
µm or dentin/
base exposed.
2.4.2 Severe
ditching or
marginal
fractures.
2.4.3 Larger
irregularities or
steps (repair
necessary).
3.4
Pronounced
marginal
staining. Major
intervention
necessary for
improvement.
4.4.1 Intense
hypersensitivity.
4.4.2 Delayed
with minor
subjective
symptoms.
4.3.3 No clinical
detectable
sensitivity.
Intervention
necessary, but not
replacement.
5. Clinically
poor
(replacement
necessary)
1.5 (Partial or
complete) loss
of restoration
or multiple
fractures.
2.5.1
Restoration
(complete or
partial) is loose
but in situ.
2.5.2
Generalized
major gaps or
irregularities.
3.5 Deep
marginal
staining, not
accessible for
intervention.
4.5 Intense, acute
pulpitis or
nonvital tooth.
Endodontic
treatment is
necessary and
restoration has to
be replaced.
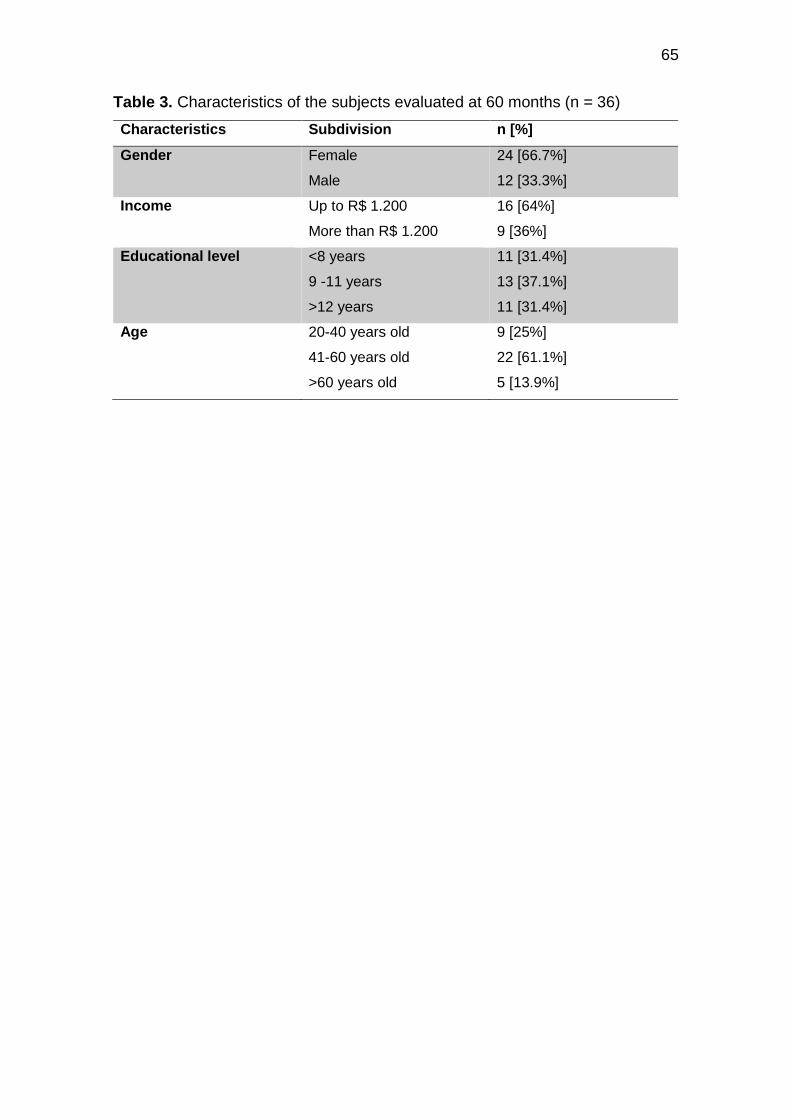
65
Table 3. Characteristics of the subjects evaluated at 60 months (n = 36)
Characteristics Subdivision n [%]
Gender Female
Male
24 [66.7%]
12 [33.3%]
Income Up to R$ 1.200
More than R$ 1.200
16 [64%]
9 [36%]
Educational level <8 years
9 -11 years
>12 years
11 [31.4%]
13 [37.1%]
11 [31.4%]
Age 20-40 years old
41-60 years old
>60 years old
9 [25%]
22 [61.1%]
5 [13.9%]
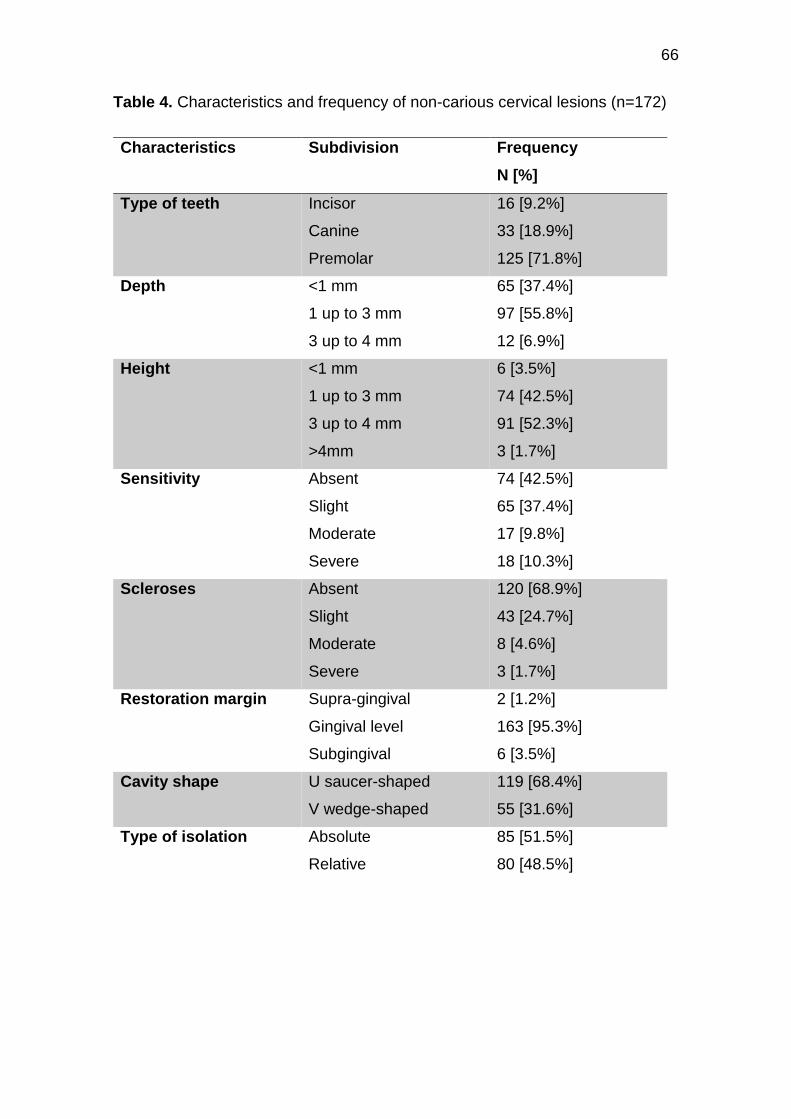
66
Table 4. Characteristics and frequency of non-carious cervical lesions (n=172)
Characteristics Subdivision Frequency
N [%]
Type of teeth Incisor
Canine
Premolar
16 [9.2%]
33 [18.9%]
125 [71.8%]
Depth <1 mm
1 up to 3 mm
3 up to 4 mm
65 [37.4%]
97 [55.8%]
12 [6.9%]
Height <1 mm
1 up to 3 mm
3 up to 4 mm
>4mm
6 [3.5%]
74 [42.5%]
91 [52.3%]
3 [1.7%]
Sensitivity Absent
Slight
Moderate
Severe
74 [42.5%]
65 [37.4%]
17 [9.8%]
18 [10.3%]
Scleroses Absent
Slight
Moderate
Severe
120 [68.9%]
43 [24.7%]
8 [4.6%]
3 [1.7%]
Restoration margin Supra-gingival
Gingival level
Subgingival
2 [1.2%]
163 [95.3%]
6 [3.5%]
Cavity shape U saucer-shaped
V wedge-shaped
119 [68.4%]
55 [31.6%]
Type of isolation Absolute
Relative
85 [51.5%]
80 [48.5%]
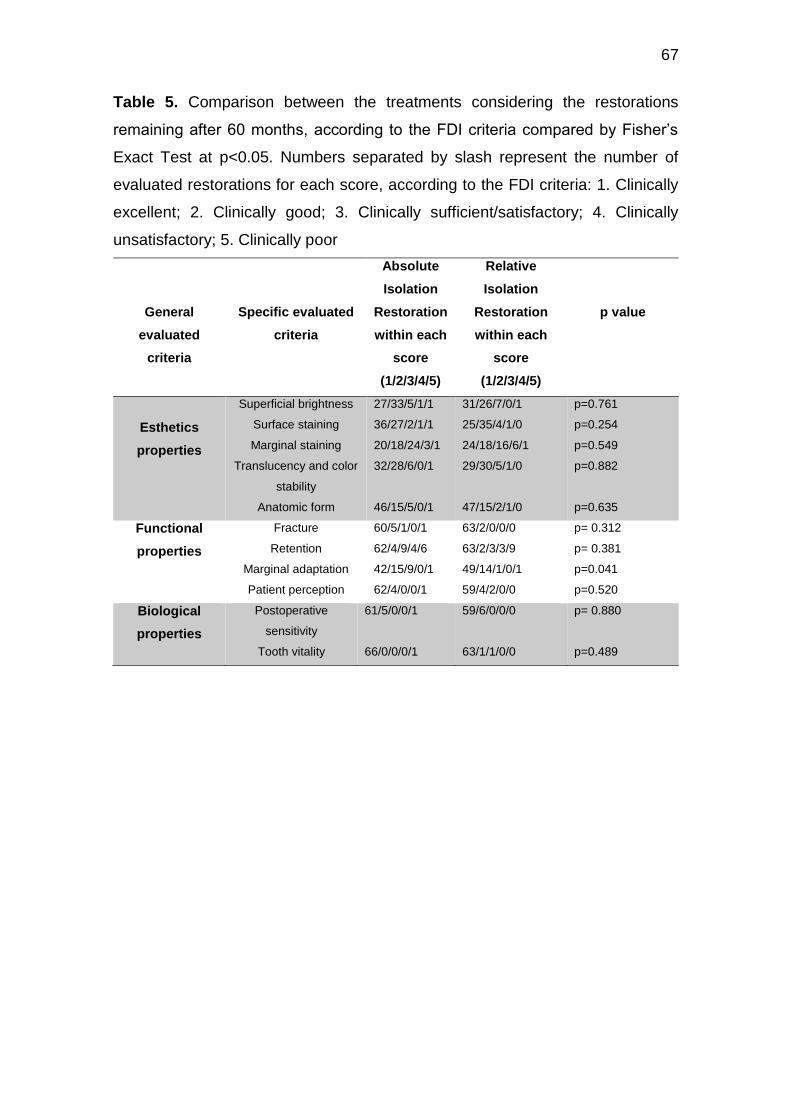
67
Table 5. Comparison between the treatments considering the restorations
remaining after 60 months, according to the FDI criteria compared by Fisher’s
Exact Test at p<0.05. Numbers separated by slash represent the number of
evaluated restorations for each score, according to the FDI criteria: 1. Clinically
excellent; 2. Clinically good; 3. Clinically sufficient/satisfactory; 4. Clinically
unsatisfactory; 5. Clinically poor
General
evaluated
criteria
Specific evaluated
criteria
Absolute
Isolation
Restoration
within each
score
(1/2/3/4/5)
Relative
Isolation
Restoration
within each
score
(1/2/3/4/5)
p value
Esthetics
properties
Superficial brightness
Surface staining
Marginal staining
Translucency and color
stability
Anatomic form
27/33/5/1/1
36/27/2/1/1
20/18/24/3/1
32/28/6/0/1
46/15/5/0/1
31/26/7/0/1
25/35/4/1/0
24/18/16/6/1
29/30/5/1/0
47/15/2/1/0
p=0.761
p=0.254
p=0.549
p=0.882
p=0.635
Functional
properties
Fracture
Retention
Marginal adaptation
Patient perception
60/5/1/0/1
62/4/9/4/6
42/15/9/0/1
62/4/0/0/1
63/2/0/0/0
63/2/3/3/9
49/14/1/0/1
59/4/2/0/0
p= 0.312
p= 0.381
p=0.041
p=0.520
Biological
properties
Postoperative
sensitivity
Tooth vitality
61/5/0/0/1
66/0/0/0/1
59/6/0/0/0
63/1/1/0/0
p= 0.880
p=0.489
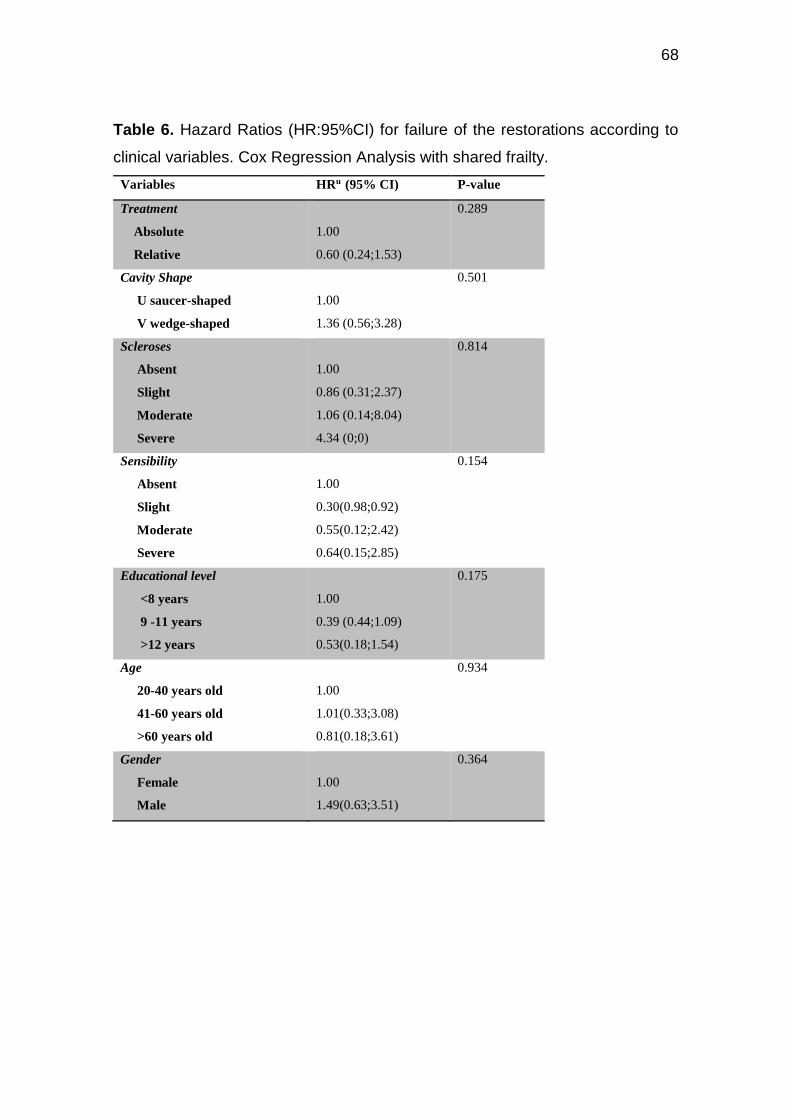
68
Table 6. Hazard Ratios (HR:95%CI) for failure of the restorations according to
clinical variables. Cox Regression Analysis with shared frailty.
Variables HRu (95% CI) P-value
Treatment
Absolute
Relative
1.00
0.60 (0.24;1.53)
0.289
Cavity Shape
U saucer-shaped
V wedge-shaped
1.00
1.36 (0.56;3.28)
0.501
Scleroses
Absent
Slight
Moderate
Severe
1.00
0.86 (0.31;2.37)
1.06 (0.14;8.04)
4.34 (0;0)
0.814
Sensibility
Absent
Slight
Moderate
Severe
1.00
0.30(0.98;0.92)
0.55(0.12;2.42)
0.64(0.15;2.85)
0.154
Educational level
<8 years
9 -11 years
>12 years
1.00
0.39 (0.44;1.09)
0.53(0.18;1.54)
0.175
Age
20-40 years old
41-60 years old
>60 years old
1.00
1.01(0.33;3.08)
0.81(0.18;3.61)
0.934
Gender
Female
Male
1.00
1.49(0.63;3.51)
0.364

69
Capítulo 4
Effects of cervical restorations on the periodontal tissues
Abstract
Background: This clinical study aimed to investigated the possible impact of the
placement of restorations at noncarious cervical lesions (NCCLs) on the adjacent
periodontal tissues health.
Methods: This study presents data from the follow-up of two randomized clinical
trials. In the study 1, with a 36-month follow-up study, the teeth with NCCLs were
restored according 3 groups: application of placebo solution (control group),
application of chlorhexidine 2% (CHX group) and application of sodium
hypochlorite 10% (NaOCl group). In the study 2, with a 60-month follow-up study,
the teeth with non-carious cervical lesions were restored according 2 groups: a)
relative insolation with cotton rolls and b) absolute insolation with rubber dam. An
experienced, trained and calibrated evaluator performed the restorations
evaluations at each study, using the FDI criteria. The periodontal evaluation was
done following criteria: 1) size of the keratinized tissue band, 2) size of gingival
range, 3) thickness of gingival tissue, 4) distance of restoration to gingival level,
5) classification of gingival recession, 6) presence of plaque 7) presence of
gingival retraction, 8) regular or irregular gingival margin 9) presence of
inflammatory signs: erythema, swelling, and bleeding, 10) presence of a new
recession 11) presence of new non-carious cervical lesion. The periodontal
criteria were evaluated using buccal mirror, periodontal probe (Millimeter Probe
PC N ° 15 – ICE), anaesthesia needle and rubber stop.Revaluations were made
for periods of 6, 12, 24 and 36 and 60 months. A total of 398 restorations (81
patients) were evaluated after 36-months and 60 months follow-up. Data were
subjected to survival analysis using the Kaplan-Meier method. The log-rank test
was used to evaluate the existence of differences between the survival curves.
The chi-square test was used to identify the frequency of occurrence of variables
involved with periodontal characteristics, as to verify association of variables with
alterations on the margin of the restoration in the baseline and the last follow-up.
Results: Any association between clinical restorations variables and changes in
baseline gingival margin until the last follow up were not statistically significant
(p>0.05). There was an improvement in the patients oral hygiene pattern,
confirmed by a decrease on visible plaque indexes after the restorations
placement and a reduction on gingival bleeding, specially on those patients who
reported having received and followed the hygiene instructions received from the
dentist when the restoration was done.

70
Conclusion: Neither the type of isolation used nor the presence of restorations
near the gingival margin caused damage according to the periodontal criteria
adapted in this study.
Clinical Significance: When correctly performed restorative treatment, with
good finishing, polishing and hygiene instructions to patients, NCCL restorations
have a healthy relationship with periodontal tissue.
Keywords: gingival recession, non carious cervical lesions, randomized clinical
trial, composite restoration, periodontal heath.
Introduction
Non-carious cervical lesions (NCCLs) are the result of a population with
controlled hygiene habits but not exactly adequate 1. These lesions may arise
due to several factors as the acidic diet exacerbated, manifesting as erosion, due
to a brushing performed with excessive force, called abrasion, or due to occlusal
problems, called abfraction. In general, these lesions are considered as
multifactorial origin 2,3.The appearance of NCCLs lesions leaves the exposed
dentin in the teeth cervical region, causing the patient aesthetic problems and
discomforts as to the dentin sensitivity. Faced with this, there are different
indications of treatments, according to the characteristics of the injury and the
need and expectation of the patient 4.
In cases where the lesions are shallow, fluoride varnish, desensitizers in
general, or gingival overlapping should be applied if the patient is suitable for the
surgical procedure. In cases where the lesions are deeper, it is possible to restore
them, and at this decision-making moment the greatest doubts arise from
dentists, as this type of restoration has adhesive challenges. Restorations of non-
carious cervical lesions are largely supported on the dentin, surface known for its
characteristic moisture. These have been tried to solve in several ways, either
through changes in materials used, or modifications in restorative techniques 5.
Another factor that causes concern among dentists is the effect of those
restorations, which are in such intimate contact with the periodontium, can
generate over time for the gingival margin tissues of the patient who will be
receiving restorative treatment as the solution to their complaint. However, there
are periodontal approaches that are able to provide an effective and complete
treatment, from the aesthetic and functional point of view for NCCLs associated
with gingival recessions 6.
Some features throughout the manufacture of NCCLs restorations require
careful attention to avoid damage on soft tissues. There is the idea, for example,
that after the use of the rubber-dam clamp there may be the development of
gingival recession. As well as, the location of the margin of the restoration can
interfere in the appearance of inflammation, gingival bleeding, gingival retraction
and periodontal pocket. Margins located at the level have the characteristic of
71
producing less inflammatory response than the subgingival restorations 7. Based
on these aspects, this clinical study aimed to elucidate the possible effects that
restorations of non-carious cervical lesions (NCCLs) and the type of tooth
isolation can generate in the adjacent periodontal tissues. Our hypothesis was
that neither the margin of the restorations nor the different isolation techniques
will result in significant impairs in the periodontal health of patients.
Materials and methods
Ethical Aspects
This study presents data from the follow-up period of two randomized
clinical trials. The Ethics Committee (CEP) of the School of Dentistry of the
Federal University of Pelotas (FO-UFPel) approved both (protocols 210/2011 and
093/2009). The studies were registered at clinicaltrials.gov (NCT01947192 and
NCT01506830), and followed the CONSORT guidelines 8. Prior to participating
the study, all selected patients signed a free and informed consent form.
Study Design
This clinical study was conducted through the follow-up of two different
split-month studies: 1) the results of a 36-month follow-up of a randomized, split-
mouth and triple- blind (patients,operator and evaluator) and, 2) the results of a
60-month follow-up from another randomized clinical trial, double-blind (patients
and examiner), where the gingival level of these restorations, the technique for
the isolation of these teeth, and the possible restoration failure rate were
analyzed.
At the 36-month follow-up study, the teeth with NCCLs were restored
according 3 different groups: application of placebo solution (control group),
application of chlorhexidine 2% (CHX group) and application of sodium
hypochlorite 10% (NaOCl group).
At the 60-month follow-up study, the teeth with non-carious cervical lesions
were restored according 2 different groups: relative insolation with cotton rolls or
absolute insolation with rubber dam, both groups complemented by saliva suction
device.
All restorations were performed by trained and calibrated undergraduate
students of the Dental School of the Federal University of Pelotas (UFPel,
Pelotas, RS, Brazil). Those responsible for the studies supervised the
undergraduate students during the entire period of care.
Operators’ Training
In both studies, the operators received theoretical and practical training.
The students went through pre-clinical activities, attending to the demonstration
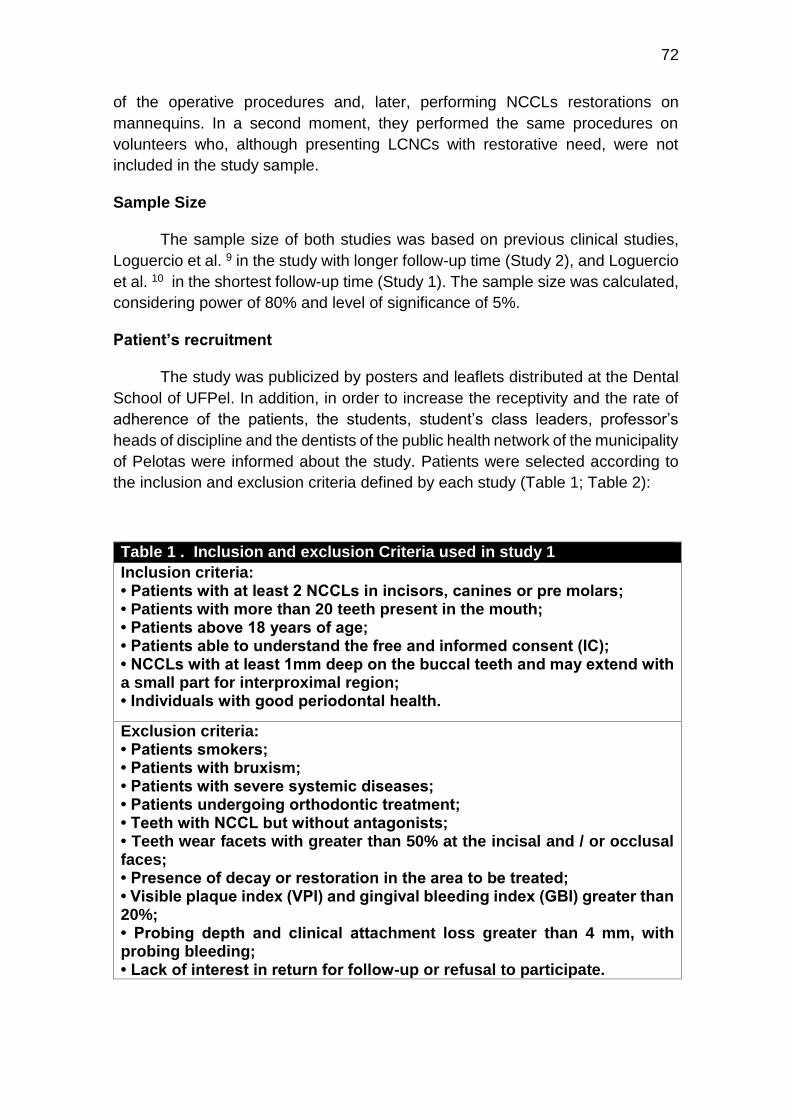
72
of the operative procedures and, later, performing NCCLs restorations on
mannequins. In a second moment, they performed the same procedures on
volunteers who, although presenting LCNCs with restorative need, were not
included in the study sample.
Sample Size
The sample size of both studies was based on previous clinical studies,
Loguercio et al. 9 in the study with longer follow-up time (Study 2), and Loguercio
et al. 10 in the shortest follow-up time (Study 1). The sample size was calculated,
considering power of 80% and level of significance of 5%.
Patient’s recruitment
The study was publicized by posters and leaflets distributed at the Dental
School of UFPel. In addition, in order to increase the receptivity and the rate of
adherence of the patients, the students, student’s class leaders, professor’s
heads of discipline and the dentists of the public health network of the municipality
of Pelotas were informed about the study. Patients were selected according to
the inclusion and exclusion criteria defined by each study (Table 1; Table 2):
Table 1 . Inclusion and exclusion Criteria used in study 1
Inclusion criteria: • Patients with at least 2 NCCLs in incisors, canines or pre molars; • Patients with more than 20 teeth present in the mouth; • Patients above 18 years of age; • Patients able to understand the free and informed consent (IC); • NCCLs with at least 1mm deep on the buccal teeth and may extend with a small part for interproximal region; • Individuals with good periodontal health.
Exclusion criteria: • Patients smokers; • Patients with bruxism; • Patients with severe systemic diseases; • Patients undergoing orthodontic treatment; • Teeth with NCCL but without antagonists; • Teeth wear facets with greater than 50% at the incisal and / or occlusal faces; • Presence of decay or restoration in the area to be treated; • Visible plaque index (VPI) and gingival bleeding index (GBI) greater than 20%; • Probing depth and clinical attachment loss greater than 4 mm, with probing bleeding; • Lack of interest in return for follow-up or refusal to participate.
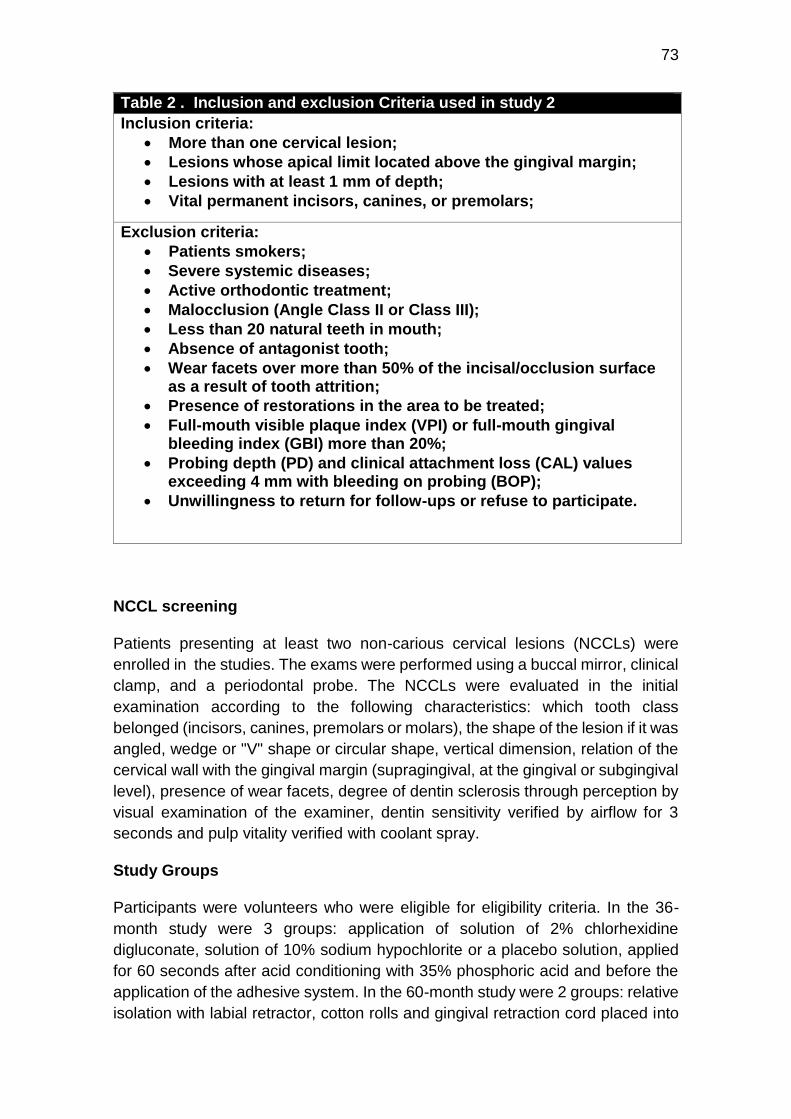
73
Table 2 . Inclusion and exclusion Criteria used in study 2
Inclusion criteria:
More than one cervical lesion;
Lesions whose apical limit located above the gingival margin;
Lesions with at least 1 mm of depth;
Vital permanent incisors, canines, or premolars;
Exclusion criteria:
Patients smokers;
Severe systemic diseases;
Active orthodontic treatment;
Malocclusion (Angle Class II or Class III);
Less than 20 natural teeth in mouth;
Absence of antagonist tooth;
Wear facets over more than 50% of the incisal/occlusion surface as a result of tooth attrition;
Presence of restorations in the area to be treated;
Full-mouth visible plaque index (VPI) or full-mouth gingival bleeding index (GBI) more than 20%;
Probing depth (PD) and clinical attachment loss (CAL) values exceeding 4 mm with bleeding on probing (BOP);
Unwillingness to return for follow-ups or refuse to participate.
NCCL screening
Patients presenting at least two non-carious cervical lesions (NCCLs) were
enrolled in the studies. The exams were performed using a buccal mirror, clinical
clamp, and a periodontal probe. The NCCLs were evaluated in the initial
examination according to the following characteristics: which tooth class
belonged (incisors, canines, premolars or molars), the shape of the lesion if it was
angled, wedge or "V" shape or circular shape, vertical dimension, relation of the
cervical wall with the gingival margin (supragingival, at the gingival or subgingival
level), presence of wear facets, degree of dentin sclerosis through perception by
visual examination of the examiner, dentin sensitivity verified by airflow for 3
seconds and pulp vitality verified with coolant spray.
Study Groups
Participants were volunteers who were eligible for eligibility criteria. In the 36-
month study were 3 groups: application of solution of 2% chlorhexidine
digluconate, solution of 10% sodium hypochlorite or a placebo solution, applied
for 60 seconds after acid conditioning with 35% phosphoric acid and before the
application of the adhesive system. In the 60-month study were 2 groups: relative
isolation with labial retractor, cotton rolls and gingival retraction cord placed into

74
the gingival sulcus and absolute insolation with rubber dam and retractor clamp
in the cervical area of the tooth.
Randomization and Blinding Procedures
The randomization process was performed using a computer program (Microsoft
Excel, 2010) by a team member not directly involved in the operative procedures,
nor in the clinical evaluation of the restorations in each of the studies. In study 1,
the person who performed the randomization (TPC) caused the randomization to
be performed according to the tooth-group (incisors, canines and premolars),
where the first restored tooth was raffed to one treatment, while the next tooth
from The same tooth-group was automatically assigned to the other treatment,
according to the split-mouth design. Thus, after randomization, each patient
received the same number of restorations in each group studied. In study 2, the
investigator (STF) performed quadrant randomization, where the type of isolation
of the first quadrant was drawn, and the remainder followed the split mouth
model. Each operator carried out the same number of interventions. The
treatments were placed in opaque envelopes and sealed to conceal the
randomization sequence.
Clinical Procedures
Initially, a prophylaxis of the element to be restored with rubber cup and paste
based on pumice and water was done. The color of the restoration was then
selected using a color scale (Vitapan Classical, Vita Zahnfabrik, Bad Sackingen,
Germany). In the study 1, NCCL restorations were performed following the same
protocol for all 3 groups (2% CRX, 10% sodium hypochlorite and control). All
restorations were performed with previous relative isolation. This type of isolation
consisted of the use of labial retractors, cotton rolls, saliva aspirator and gingival
retraction cord (Ultrapak Cord, Ultradent, South Jordan, UT, USA) in the gingival
sulcus. After this step, the teeth were conditioned with 35% phosphoric acid
(Adper Scotchbond Etchant, 3M ESPE) for 20 seconds in enamel and 15 seconds
in dentin, followed by rinsing with air / water spray for 30 seconds and removal of
excess moisture from cavity using absorbent paper. At this time, the substances
that were all in equal flasks to allow operator blinding were applied for 60 seconds
using a disposable applicator and the solution was removed. The application of
two-step etch-and-rinse adhesive system (Single Bond 2, 3M ESPE, St. Paul,
MN, USA) and restoration with a direct restorative nanocomposite resin (Filtek
Z350, 3M ESPE) following the manufacturer's standards.
In the study 2, the NCCLs was randomized into the following groups: (1) isolation
performed with rubber dam and gingival retraction clamp and (2) isolation
provided with cotton rolls and gingival retraction cord. Both techniques were used
with a saliva suction device. All restorative procedures were performed using a
self-etching adhesive system (Adper Scotchbond Multi-Use, 3M ESPE, St. Paul,
MN, USA) and nanoparticulate restorative composite (Filtek Z350, 3M ESPE, St.
75
Paul, MN, USA), strictly following the instructions of use provided by the
manufacturer.
At both studies, a LED device (Radii-Call, SDI, Bayswater, VI, Australia) was
used for photoactivation. The restorations were finished using fine-grained
diamond tips and multilaminate drills to remove excess material and improve the
contour shape of the restorations. Polishing was done using silicone tips, flexible
discs (Sof-Lex Pop-On, 3M ESPE, St. Paul, MN, USA), felt discs and specific
polishing pastes. The restorations were made on 3 different levels: supragingival,
at the gingival level and subgingival.
Clinical Assessment
For the clinical evaluation of restorations, the evaluation criteria approved by the
FDI World Dental Federation were used 11. Was evaluated the retention of the
restoration, where it was considered a failure, and as a secondary outcome, the
following criteria: 1) marginal adaptation, 2) marginal staining, 3) the color of the
surface, 4) post-operative Sensitivity, 5) surface brightness, 6) translucency and
color, 7) fracture, 8) anatomical shape and 9) preserving the vitality and integrity
of teeth. Each criterion was expressed in five scores, three for acceptable and
two for non-acceptable (repair or replacement).
For the periodontal evaluation, a clinical form was created formulated by the
researchers (Appendix E), following criteria: 1) size of the keratinized tissue band,
2) attached of gingival range, 3) thickness of gingival tissue, 4) distance of
restoration to gingival level, 5) classification of gingival recession, 6) visible
plaque index VPI 7) presence of gingival retraction, 8) regular or irregular gingival
margin 9) presence of inflammatory signs: erythema, swelling, and bleeding, 10)
presence of a new recession 11) presence of new non-carious cervical lesion.
The periodontal criteria were evaluated using buccal mirror, periodontal probe
(Millimeter Probe PC N ° 15 – ICE), anaesthesia needle and rubber stop. Also, a
periogram of the restored teeth was made for comparison with the periograms of
the previous appointments.
Examiners considered gold standard, both the periodontal part and the
restorative part, performed the evaluations. The periodontal examination was
performed in both studies by the same evaluator (TMM), and the evaluation of
the restoration was performed by a researcher (MSC) at the 36-month follow-up
and by another investigator (ASM) at the 60-month follow-up.
Recalls
Patients were followed up with the criteria established by the FDI to follow up the
restorations, by a trained and calibrated evaluator (MSC) in the baseline periods,
6 months, 12 months, 24 months, 36 months and in the case of the longer study,
up to 60 months. Regarding the periodontal criteria, for study 1, only a descriptive
76
analysis of how current periodontal health parameters was performed. In study
2, there is a complete periogram in all revaluations. Therefore, in the latter, a
comparison of the evolution of the characteristics of periodontal health of the
patients can be made. Also, periodontal information can be inferred from the
shorter study when the clinical file of initial examination is analysed.
The recalls were made through telephone connection. When no contact was
possible after several attempts, or the number on the clinical record was given as
non-existent, a letter was sent to the patient's residential address. In cases where
there was no return of the letters via telephone contact, letters or e-mail, a home
visit was chosen, where the researchers (MSC, TMM, ASM, MF) carried out the
examination of the patients in their own homes. Individuals, whose contact was
not possible even by this route, were considered losses.
Statistical Analysis
A researcher not directly involved in the study performed the statistical
analysis of the data. The analysis was carried using Stata 11.0 Statistic Program
(Stata Corp LP, College Station, TX, USA), considering 80% statistic power and
5% significance level. The data were tabulated and submitted to the Chi-square
Test to find the frequency of appearance of the variables involved with the
periodontal characteristics, as well as to make the association between data
referring to the patient and the lesions and some variables considered as an
outcome, as is the case of gingival margin alteration, the effect of the level of
restoration over the years on the location of the gingival margin, whether it
remained in the same position or has increased recession, and the effect that
guidelines received by patients on the day of restoration of NCCL, caused in the
periodontal health recalls. Also, some periodontal criteria that were measured
only in the second evaluation were synthesized in a descriptive way, presented
through the mean and standard deviation.
Results
This study is a result of the combination of two different samples of patients
with NCCL restorations made with different methodologies and follow-up times.
However, both samples had their data evaluated and collected by the same
evaluator, following the same evaluation criteria, present in the patient's clinical
record (Appendix E).
Of the total number of restorations (298) evaluated, 81.9% did not change
the level of the restoration margin and 18% worsened after the follow-up periods.
This means that most of the patients did not present an increase in gingival
recession, and of those that presented a difference in the position of the margin
of the restoration, only 2 teeth presented new NCCL. The criteria related to
gingival margin was crossed with type of isolation, toothbrush type and condition,
type of toothpaste used, receipt of hygiene instructions and type of toothbrush

77
and dentifrice to be used, as well as presence of harmful oral habits. However,
none of these associations were statically significant. (Table 1).
An improvement in patient hygiene pattern can be observed since the
visible plaque found in the baseline was 37% and in the last follow-up was present
in 24% of the evaluated teeth. We can divide this criteria in the following way:
those who never presented plaque were 50% of the cases, those that improved,
that is, presented before and not more now were 25%, those that worsened, since
they did not have before and now have 14% and those that already had visible
plaque and continue correspond to 9% (Table 2).
When it was associated visible plaque and bleeding presence data with
hygiene guidelines (which type of brush and dentifrice to use) it was found a
significant association (p<0.001) for gingival bleeding. Thus, who received the
guidelines, presented a decrease on marginal bleeding in comparison to those
who report not having received. However, the visible plaque factor was not
significant (p=0.116) but it is known that there may be a relationship between the
fact that the patient knows that they are evaluated by a dentist, they can perform
a different hygiene than the one performed daily. Therefore, even those who
reported not having received the guidelines may have made a better hygiene
because they knew that their teeth would be evaluated (Table 3).
Many of the periodontal data of this study could have their characteristics
tabulated in a descriptive way, as they did not have the same criteria of
periodontal evaluation previously in their clinical records, which would allow
comparing the current data with the past ones.
Discussion
Non-carious cervical lesions associated with gingival recession require
care in both the hard and soft tissues adjacent to the lesion. For this, when a
restorative treatment is performed, it is necessary a finishing and polishing of
excellence, after all, if a complementary surgical treatment is done, this will be a
critical factor to contribute with the clinical success of the case 12. Even if the
surgical treatment of root coverage is not performed, the finishing and polishing
must be performed very well, as the composite resins may present marginal
leakage, favoring the accumulation of subgingival plaque and development of a
microenvironment favorable to the development of a anaerobic flora 13.
When choosing the association of treatments, it is necessary to observe
some periodontal characteristics that allow the execution of the surgical
technique, and that allows to obtain the most favorable results possible. The
gingival recession cases that present as Class I, II or III characteristics may not
only be restored, but also are those with more predictable, results regarding root
coverage, that means the resolution of the lesion 14.
The majority of the evaluated cases presented classification of the gingival
recession was Class III (64.1%), a fact that is important from a periodontal point
of view (Table 2). In fact, in cases where there is Class I and II of Miller, it is

78
possible to obtain, after surgical procedure, total root coverage. In class III, there
is already loss of interdental bone and interdental papilla soft which allows us to
expect a partial root coverage of the NCCL 14.
Due to the trend of nonlinear progression of non-carious cervical lesions
with increasing patient age, deeper lesions, V-shaped lesions and signs of bone
loss appear to merit further attention, as these criteria show a proportional
amplification tendency of stress in these teeth 15.
Taking into account the aesthetic point of view and periodontal health, the
periodontal surgical treatment has more positive responses than only the
restorative treatment 16. However, not all cases will have a good surgical
response, for this, other periodontal factors should be verified, such as the
osseous level and the interproximal papilla. The majority of the cases evaluated
in our study had partial interproximal papilla (77.8%). This data may be derived
from some sequel of prior periodontal treatment or because of the effects of
traumatic tooth brushing on the periodontal tissues.
Moreover, in order to have a satisfactory surgical result, many others
characteristics of the patient should be analyzed. These encompasses the gingival
thickness, keratinized and attached gingiva, that herein were reported through their
mean and standard deviation (Table 4). Vandana et al. concluded in their study
that gingival thickness is a factor that varies according to dental arch, gender and
age. The upper jaws, men and the younger age group had thicker gingiva 17. In
the literature, there is a clinical study report that found that the lower the gingival
thickness, the greater the degree of recession, establishing an inversely
proportional relation 18. Another study reports a direct relationship between the
thickness of the flap and the reduction of the recession. In this study, the
thickness> 0.8 mm was associated with 100% of the root coverage 19. Always
taking into account the type of recession.Thus, in order to have a satisfactory
surgical result, several characteristics of the patient should be analyzed.
Another possible predisposing factors related to the patient for the
development of gingival recession is the amount of keratinized gingiva. However, the
literature shows controversial results, and the majority of studies have shown that
the mean amount of keratinized gingiva does not predispose gingival recession 20.
Besides the periodontal criteria, it was tried to evaluate the relation of these
with the type of isolation realized at the moment of the restoration and checked
that this did not was significantly influence with the distance between the gingival
margin and the margin of the restoration, that is, it did not increase the gingival
recession over time. The number of restorations performed with relative isolation
(78.2%) is much higher than that of absolute isolation (21.8%), due to the fact
that we used samples from two different studies, in which only one patient were
randomized as to the type of insulation, in the other where all restorations were
performed with relative insulation, with retractor wire, lip retractor, cotton swabs
and saliva suction unit. A study with a shorter follow-up period, by Daudt et al,
identified that the isolation technique with rubber dam, besides being identified
79
as more uncomfortable to the patient, resulted in the appearance of short-term
gingival recession 21.
A periodontal positive factor was that the gingival contour was mostly
regular, and some basic clinical signs of inflammation were not identified in the
vast majority of patients, such as edema and erythema. This shows that most
patients are achieving a good level of oral hygiene, and that the presence of the
restorations did not hinder proper plaque removal. Plaque accumulation can
result in caries and periodontal disease and cervical restorations may be a
contributing factor to this 4.
The majority of patients reported using soft toothbrush to make their daily
hygiene, and these were presented between good and regular state, prevailing
those that were in better state of conservation. The use of medium or hard
toothbrushes during tooth brushing may contribute to the development of new
non-carious cervical lesions, as well as the aggravation of existing ones 22. The
type of toothbrush, the type of toothpaste used and the strength of brushing are
factors that influence the etiology of NCCLs 23. The literature reveals that patients
with non-inflamatory gingival recession, may prevent the progression by doing a
correct tooth brushing 24. Young patients with multiple gingival recessions may
improve their aesthetic status with non-surgical and supportive periodontal
therapy including oral hygiene instruction, scaling and root planning 25. Therefore,
changing brushing habits can contribute to the stabilization of the margin.
Santamaria et al. proposes an adaptation of the medium with oral hygiene
instructions and suggests the use of soft toothbrushes prior to surgical
intervention 26. Participation in periodontal maintenance programs may aid in the
control of gingival recessions. Our patients, for the most part, reported having
received oral hygiene instructions and applied them in their routine, such as
brushing with the vertical technique, and use of soft toothbrush. Whitening
toothpastes can cause greater tooth wear through dentin abrasion than
conventional pastes 27. Regarding the type of dentifrice used, the majority
reported using conventional dentifrices. These data obtained through the
questionnaire applied, demonstrates that these patients were correctly instructed
and that above all are complying with these guidelines which are of paramount
importance mainly for patients who have non-carious cervical lesions.
80
References
1. Litonjua LA, Andreana S, Cohen RE. Toothbrush abrasions and noncarious cervical lesions: evolving concepts. Compend Contin Educ Dent [Internet]. 2005 Nov [cited 2016 Dec 6];26(11):767–8, 770–4, 776 passim. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16300231
2. Bartlett DW, Shah P. A critical review of non-carious cervical (wear) lesions and the role of abfraction, erosion, and abrasion. J Dent Res [Internet]. 2006 Apr [cited 2016 Dec 6];85(4):306–12. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16567549
3. Grippo JO, Simring M, Schreiner S. Attrition, abrasion, corrosion and abfraction revisited: a new perspective on tooth surface lesions. J Am Dent Assoc [Internet]. 2004 Aug [cited 2016 Dec 6];135(8):1109-18-5. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15387049
4. Perez CDR, Gonzalez MR, Prado NAS, de Miranda MSF, Macêdo M de A, Fernandes BMP, et al. Restoration of noncarious cervical lesions: when, why, and how. Int J Dent [Internet]. 2012 [cited 2016 Oct 19];2012:687058. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22216032
5. Peumans M, De Munck J, Mine A, Van Meerbeek B. Clinical effectiveness of contemporary adhesives for the restoration of non-carious cervical lesions. A systematic review. Dent Mater. 2014;
6. Zucchelli G, Gori G, Mele M, Stefanini M, Mazzotti C, Marzadori M, et al. Non-Carious Cervical Lesions Associated With Gingival Recessions: A Decision-Making Process. J Periodontol. 2011;82:1713–24.
7. Elias MG, Carvalho W, Barboza EP. Location of the final preparation in aesthetic restorations: a discussion related to periodontal health. RGO -Revista Gaúcha Odontol. 2013;61:441–5.
8. Schulz KF, Altman DG, Moher D. WITHDRAWN: CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. Int J Surg [Internet]. 2010;115(5):1063–70. Available from: http://dx.doi.org/10.1016/j.jclinepi.2010.02.005
9. Loguercio AD, Costenaro A, Silveira AP, Ribeiro NR, Rossi TR, Reis A. A six-month clinical study of a self-etching and an etch-and-rinse adhesive applied as recommended and after doubling the number of adhesive coats. J Adhes Dent [Internet]. 2006 Aug [cited 2016 Dec 1];8(4):255–61. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16958291
10. Loguercio AD, Bittencourt DD, Baratieri LN, Reis A. A 36-month evaluation of self-etch and etch-and-rinse adhesives in noncarious cervical lesions. J Am Dent Assoc [Internet]. 2007 Apr [cited 2016 Dec 6];138(4):507-14-7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17403742
81
11. Hickel R, Peschke A, Tyas M, Mjör I, Bayne S, Peters M, et al. FDI World Dental Federation - clinical criteria for the evaluation of direct and indirect restorations. Update and clinical examples. J Adhes Dent [Internet]. 2010 Aug [cited 2016 Dec 6];12(4):259–72. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20847997
12. Yang S, Lee H, Jin S-H. A combined approach to non-carious cervical lesions associated with gingival recession. Restor Dent Endod [Internet]. 2016 Aug [cited 2017 Jan 13];41(3):218–24. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27508164
13. Paolantonio M, D'Ercole S, Perinetti G, Tripodi D, Catamo G, Serra E, et al. Clinical and microbiological effects of different restorative materials on the periodontal tissues adjacent to subgingival class V restorations. 1-Year results. J Clin Periodontol. 2004;31(3):200–7.
14. Miller PD. A classification of marginal tissue recession. Int J Periodontics Restorative Dent [Internet]. 1985 [cited 2016 Dec 6];5(2):8–13. Available from: http://www.ncbi.nlm.nih.gov/pubmed/3858267
15. Guimarães JC, Guimarães Soella G, Brandão Durand L, Horn F, Narciso Baratieri L, Monteiro S, et al. Stress amplifications in dental non-carious cervical lesions. J Biomech [Internet]. 2014;47(2):410–6. Available from: http://dx.doi.org/10.1016/j.jbiomech.2013.11.012
16. Leybovich M, Bissada NF, Teich S, Demko CA, Ricchetti PA. Treatment of noncarious cervical lesions by a subepithelial connective tissue graft versus a composite resin restoration. Int J Periodontics Restorative Dent [Internet]. [cited 2017 Jan 9];34(5):649–54. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25171035
17. Vandana KL, Savitha B. Thickness of gingiva in association with age, gender and dental arch location. J Clin Periodontol. 2005;32(7):828–30.
18. Maroso FB, Gaio EJ, Rösing CK, Fernandes MI. Correlation between gingival thickness and gingival recession in humans. Acta Odontol Latinoam [Internet]. 2015 [cited 2017 Jan 9];28(2):162–6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26355887
19. Baldi C, Pini-Prato G, Pagliaro U, Nieri M, Saletta D, Muzzi L, et al. Coronally Advanced Flap Procedure for Root Coverage. Is Flap Thickness a Relevant Predictor to Achieve Root Coverage? A 19-Case Series. J Periodontol [Internet]. 1999;70(9):1077–84. Available from: http://www.joponline.org/doi/abs/10.1902/jop.1999.70.9.1077
20. Closs LQ, Branco P, Rizzatto SD, Raveli DB, Rösing CK. Gingival margin alterations and the pre-orthodontic treatment amount of keratinized gingiva. Braz Oral Res. 2007;21(1):58–63.
82
21. Daudt E, Lopes GC, Vieira LC. Does operatory field isolation influence the performance of direct adhesive restorations? J Adhes Dent [Internet]. 2013;15(1):27–32. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23534003
22. Brandini D, de Sousa A, Trevisan C, Pinelli L, Santos S do C, Pedrini D, et al. Noncarious Cervical Lesions and Their Association With Toothbrushing Practices: In Vivo Evaluation. Oper Dent [Internet]. 2011;36(6):581–9. Available from: http://www.jopdentonline.org/doi/10.2341/10-152-S
23. Wiegand A e., Schlueter N. The Role of oral hygiene: Does toothbrushing harm? Erosive Tooth Wear From Diagnosis to Ther. 2012;25:215–9.
24. Heasman PA, Holliday R, Bryant A, Preshaw PM. Evidence for the occurrence of gingival recession and non-carious cervical lesions as a consequence of traumatic toothbrushing. J Clin Periodontol. 2015;42(S16):S237–55.
25. Ando K. Case Report Improvement of Multiple Facial Gingival Recession by Non-Surgical and Supportive Periodontal Therapy : J Periodontol. 1999;70(August):909–13.
26. Santamaría MP, Ambrosano GMB, Casati MZ, Nociti FH, Sallum AW, Sallum EA. Connective tissue graft and resin glass ionomer for the treatment of gingival recession associated with noncarious cervical lesions: a case series. Int J Periodontics Restorative Dent [Internet]. 2011;31(5):e57-63. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21845238
27. Vieira GHA, Nogueira MB, Gaio EJ, Rosing CK, Santiago SL, Rego RO. Effect of Whitening Toothpastes on Dentin Abrasion: An In Vitro Study. Oral Health Prev Dent [Internet]. 2016 [cited 2017 Jan 16];14(6):547–53. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27351730
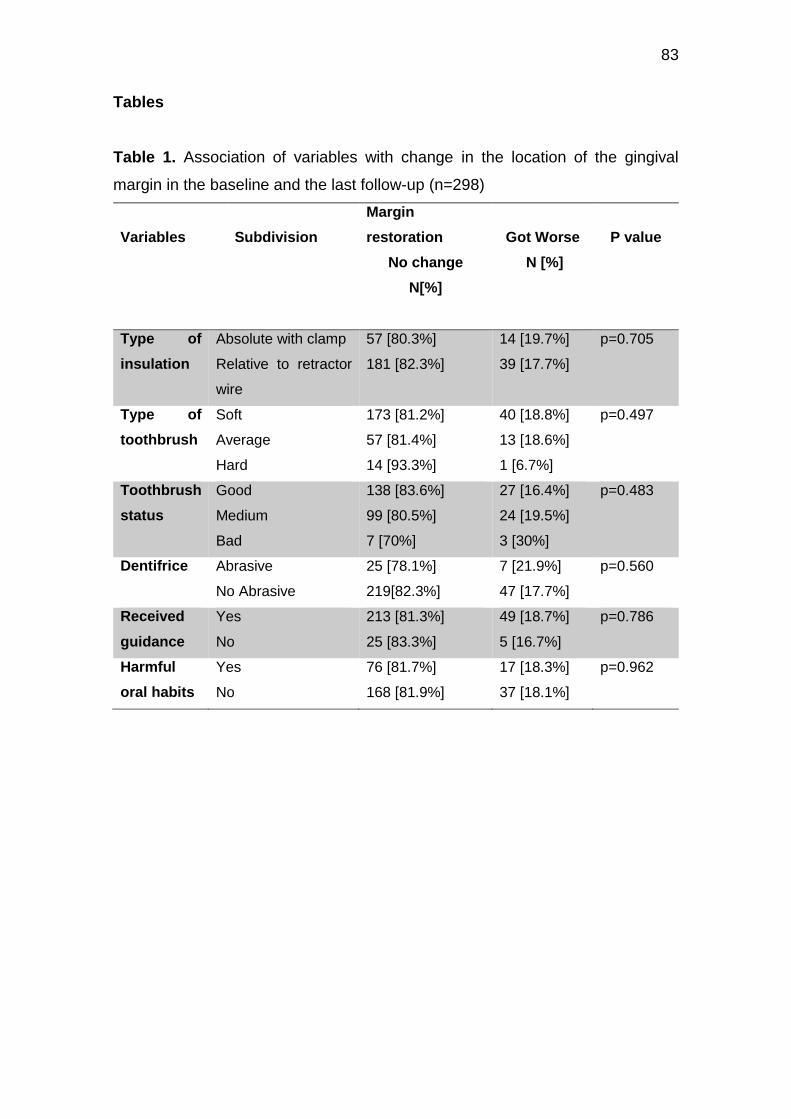
83
Tables
Table 1. Association of variables with change in the location of the gingival
margin in the baseline and the last follow-up (n=298)
Variables
Subdivision
Margin
restoration
No change
N[%]
Got Worse
N [%]
P value
Type of
insulation
Absolute with clamp
Relative to retractor
wire
57 [80.3%]
181 [82.3%]
14 [19.7%]
39 [17.7%]
p=0.705
Type of
toothbrush
Soft
Average
Hard
173 [81.2%]
57 [81.4%]
14 [93.3%]
40 [18.8%]
13 [18.6%]
1 [6.7%]
p=0.497
Toothbrush
status
Good
Medium
Bad
138 [83.6%]
99 [80.5%]
7 [70%]
27 [16.4%]
24 [19.5%]
3 [30%]
p=0.483
Dentifrice Abrasive
No Abrasive
25 [78.1%]
219[82.3%]
7 [21.9%]
47 [17.7%]
p=0.560
Received
guidance
Yes
No
213 [81.3%]
25 [83.3%]
49 [18.7%]
5 [16.7%]
p=0.786
Harmful
oral habits
Yes
No
76 [81.7%]
168 [81.9%]
17 [18.3%]
37 [18.1%]
p=0.962

84
Table 2. Frequency of variables involved with periodontal characteristics
Characteristics Subdivision Frequency
N [%]
Visible plate after
restoration
Without plaque
improved
Got worse
Always had plaque
141 [50.2%]
72 [25.6%]
41 [14.6%]
27 [9.6%]
Gingival bleeding
after restoration
Without bleeding
improved
Got worse
Always had bleeding
162 [56.5%]
72 [25%]
35 [12.2%]
18 [6.3%]
Type of insulation Absolute with clamp
Relative to retractor
wire
85 [21.8%]
305 [78.2%]
Margin restoration No change
Got worse
275 [81.9%]
54 [18%]
Class recession
(miller)
Without recession
Class I
Class II
Class III
Class IV
76 [26.2%]
25 [8.6%]
2 [0.7%]
186 [64.1%]
1 [0.3%]
Erythema Yes
No
37 [11.8%]
276 [88.2%]
Edema Yes
No
29 [9.3%]
284 [90.7%]
Gingival retraction Yes
No
10 [3.2%]
303 [96.8%]
Gingival margin
outline
Regular
Irregular
290 [92.7%]
23 [7.3%]
Harmful oral habits Yes
No
231 [66.9%]
114 [33.1%]
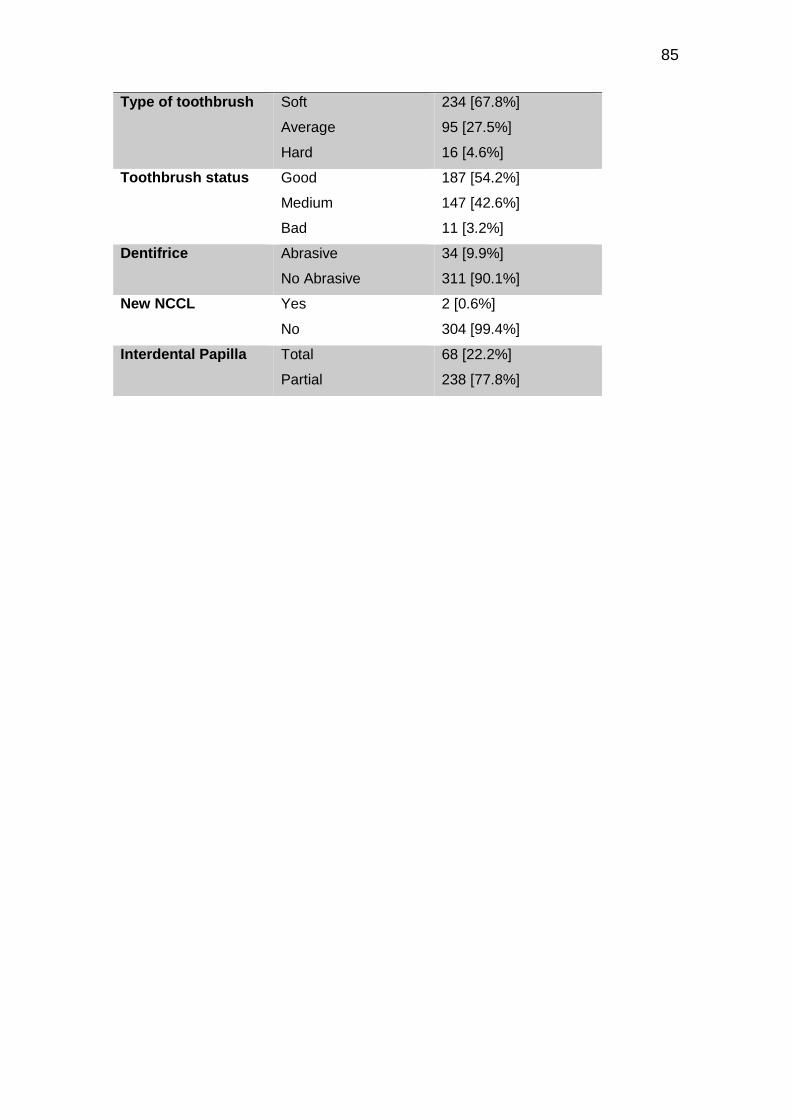
85
Type of toothbrush Soft
Average
Hard
234 [67.8%]
95 [27.5%]
16 [4.6%]
Toothbrush status Good
Medium
Bad
187 [54.2%]
147 [42.6%]
11 [3.2%]
Dentifrice Abrasive
No Abrasive
34 [9.9%]
311 [90.1%]
New NCCL Yes
No
2 [0.6%]
304 [99.4%]
Interdental Papilla Total
Partial
68 [22.2%]
238 [77.8%]
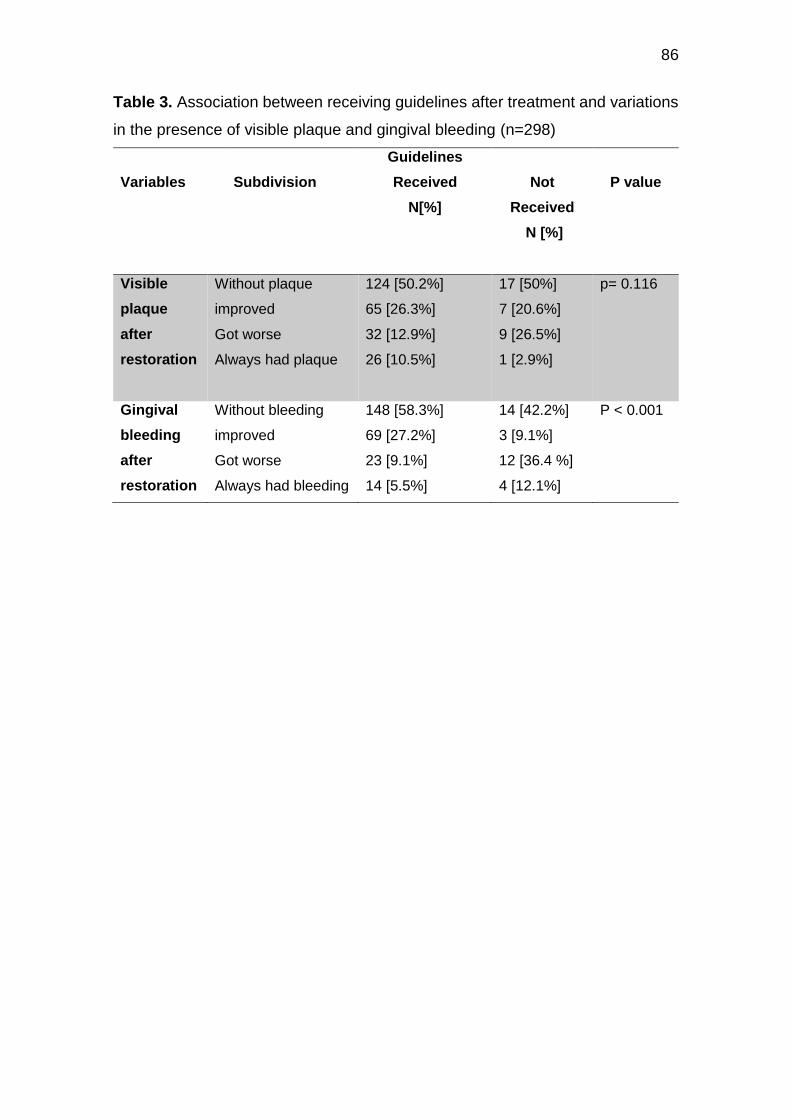
86
Table 3. Association between receiving guidelines after treatment and variations
in the presence of visible plaque and gingival bleeding (n=298)
Variables
Subdivision
Guidelines
Received
N[%]
Not
Received
N [%]
P value
Visible
plaque
after
restoration
Without plaque
improved
Got worse
Always had plaque
124 [50.2%]
65 [26.3%]
32 [12.9%]
26 [10.5%]
17 [50%]
7 [20.6%]
9 [26.5%]
1 [2.9%]
p= 0.116
Gingival
bleeding
after
restoration
Without bleeding
improved
Got worse
Always had bleeding
148 [58.3%]
69 [27.2%]
23 [9.1%]
14 [5.5%]
14 [42.2%]
3 [9.1%]
12 [36.4 %]
4 [12.1%]
P < 0.001
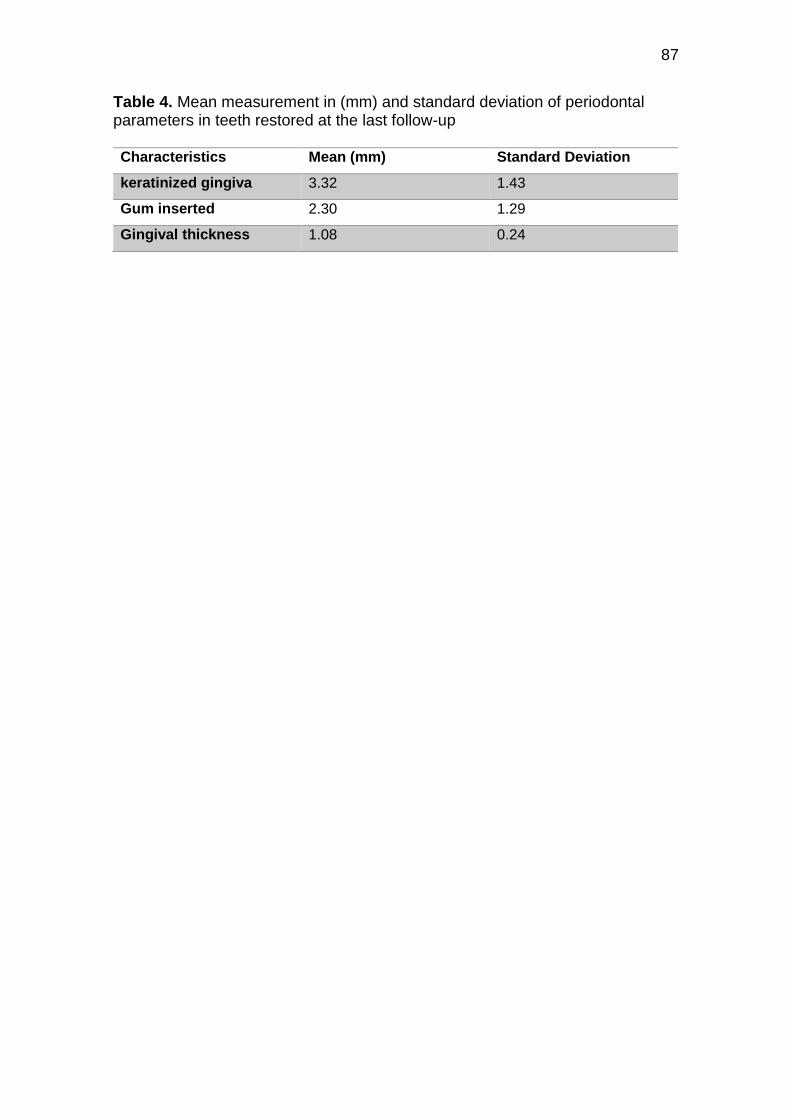
87
Table 4. Mean measurement in (mm) and standard deviation of periodontal parameters in teeth restored at the last follow-up Characteristics Mean (mm) Standard Deviation
keratinized gingiva 3.32 1.43
Gum inserted 2.30 1.29
Gingival thickness 1.08 0.24
88
6 Considerações finais
Os resultados obtidos pelos estudos desenvolvidos confirmaram nossas
hipóteses de que não haveria associação significativa entre os pontos
estudados.
- O pré-tratamento com solução de clorexidina a 2% não promoveu uma maior
retenção das restaurações de lesões cervicais não cáriosas, após
acompanhamento de 36 meses. Porém, observou-se uma tendência à falha
aumentada quando as restaurações estão localizadas subgengivalmente
comparadas às que estão ao nível e supragengival.
- O pré-tratamento com hipoclorito de sódio a 10% embora tenha levado a uma
maior taxa de falha em restaurações de LCNC, não diferiu estatisticamente do
grupo controle, ao longo de 36 meses. Outros fatores, tais como arco dentário
(mandíbula), tipo dentário (pré-molares) e pacientes com menos de 24 dentes
presentes em boca foram significativamente associados com maior número de
falhas das restaurações nessas lesões.
- Ambos os métodos de isolamento dental funcionam bem para a retenção e
sucesso clínico de restaurações de lesões cervicais não cariosas, quando
realizadas corretamente pelo operador. Houve associação significativa entre tipo
de isolamento e adaptação marginal, sendo que os scores obtidos por esta
propriedade, segundo os critérios da FDI avaliados, foram na sua grande
maioria, clinicamente satisfatórios.
- Os critérios avaliados em ambas as amostras destes estudos, não
influenciaram diretamente em respostas gengivais relevantes. Portanto, nem o
tipo de isolamento utilizado, nem a presença de restaurações perto da margem
genvival, causaram danos ao periodonto de acordo com os critérios utilizados.
Houve uma melhora por parte da higiene dos pacientes, quando obervados os
índices de placa visível antes e após as restaurações, e diminuição do
sangramento gengival por parte dos pacientes que relataram ter recebido e
seguido as instruções de higiene recebidas pelo dentista após a confecção da
restauração.
89
Referências
ADA COUNCIL ON SCIENTIFIC AFFAIRS. Direct and indirect restorative materials. Journal of the American Dental Association (1939), v. 134, n. 4, p. 463–72, abr. 2003. AINAMO, J.; BAY, I. Problems and proposals for recording gingivitis and plaque. International dental journal, v. 25, n. 4, p. 229–35, dez. 1975. ALMEIDA, P. C.; ANDRÉ, L.; PIMENTA, F. 2-year Clinical Evaluation of Sodium Hypochlorite Treatment in the Restoration of Non-carious Cervical Lesions: A Pilot Study. Operative Dentistry,v.29, n.5, p.592-598, 2004. ANDO, K. Case Report Improvement of Multiple Facial Gingival Recession by Non-Surgical and Supportive Periodontal Therapy : Journal of Periodontololy, v. 70, n. August, p. 909–913, 1999. ARIAS, V. G.; BEDRAN-DE-CASTRO, A. K. B.; PIMENTA, L. A. Effects of sodium hypochlorite gel and sodium hypochlorite solution on dentin bond strength. Journal of Biomedical Materials Research Part B: Applied Biomaterials, v. 72B, n. 2, p. 339–344, 15 fev. 2005. BALDI, C. et al. Coronally Advanced Flap Procedure for Root Coverage. Is Flap Thickness a Relevant Predictor to Achieve Root Coverage? A 19-Case Series. Journal of Periodontology, v. 70, n. 9, p. 1077–1084, 1999. BARTLETT, D. W.; SHAH, P. A critical review of non-carious cervical (wear) lesions and the role of abfraction, erosion, and abrasion. Journal of dental research, v. 85, n. 4, p. 306–12, abr. 2006. BOSKEY, A. L. The role of extracellular matrix components in dentin mineralization. Critical reviews in oral biology and medicine : an official publication of the American Association of Oral Biologists, v. 2, n. 3, p. 369–87, 1991. BRACKETT, W. W. et al. The effect of chlorhexidine on dentin hybrid layers in vivo. Operative dentistry, v. 32, n. 2, p. 107–11, 2007. BRANDINI, D. et al. Noncarious Cervical Lesions and Their Association With Toothbrushing Practices: In Vivo Evaluation. Operative Dentistry, v. 36, n. 6, p. 581–589, 2011. CARRILHO, M. R. O. et al. Chlorhexidine preserves dentin bond in vitro. Journal of dental research, v. 86, n. 1, p. 90–4, jan. 2007a. CARRILHO, M. R. O. et al. In vivo preservation of the hybrid layer by chlorhexidine. Journal of dental research, v. 86, n. 6, p. 529–33, jun. 2007b. CARVALHO, R. M. et al. A challenge to the conventional wisdom that simultaneous etching and resin infiltration always occurs in self-etch adhesives. Biomaterials, 2005. CARVALHO, R. M. et al. Durability of bonds and clinical success of adhesive restorations. Dental Materials, v. 28, n. 1, p. 72–86, 2012. CHEE, B.; RICKMAN, L. J.; SATTERTHWAITE, J. D. Adhesives for the restoration of non-carious cervical lesions: A systematic reviewJournal of Dentistry, 2012. CLOSS, L. Q. et al. Gingival margin alterations and the pre-orthodontic treatment amount of keratinized gingiva. Brazilian oral research, v. 21, n. 1, p. 58–63, 2007. COLLARES, F. M. et al. Chlorhexidine application in adhesive procedures: a meta-regression analysis. The journal of adhesive dentistry, v. 15, n. 1, p. 11–
90
8, 2013. DA ROSA RODOLPHO, P. A. et al. A clinical evaluation of posterior composite restorations: 17-year findings. Journal of Dentistry, v. 34, n. 7, p. 427–435, 2006. DA ROSA RODOLPHO, P. A. et al. 22-Year clinical evaluation of the performance of two posterior composites with different filler characteristics. Dental Materials, v. 27, n. 10, p. 955–963, 2011. DAUDT, E.; LOPES, G. C.; VIEIRA, L. C. Does operatory field isolation influence the performance of direct adhesive restorations? The journal of adhesive dentistry, v. 15, n. 1, p. 27–32, 2013. DE MUNCK, J. et al. Inhibition of enzymatic degradation of adhesive-dentin interfaces. Journal of dental research, v. 88, n. 12, p. 1101–6, 2009. DEMARCO, F. F. et al. Longevity of posterior composite restorations: Not only a matter of materials. Dental Materials, v. 28, n. 1, p. 87–101, 2012. DI RENZO, M. et al. A photoacoustic FTIRS study of the chemical modifications of human dentin surfaces: II. Deproteination. Biomaterials, v.22, n.8, p. 793-7, 2001. DIONYSOPOULOS, D. Effect of digluconate chlorhexidine on bond strength between dental adhesive systems and dentin: A systematic review. Journal of conservative dentistry : JCD, v. 19, n. 1, p. 11–6, 2016. DUTRA-CORREA, M. et al. Effect of chlorhexidine on the 18-month clinical performance of two adhesives. The journal of adhesive dentistry, v. 15, n. 3, p. 287–92, jun. 2013. ELIAS, M. G.; CARVALHO, W.; BARBOZA, E. P. Location of the final preparation in aesthetic restorations: a discussion related to periodontal health. RGO -Revista Gaúcha de Odontologia, v. 61, p. 441–445, 2013. GENDRON, R. et al. Inhibition of the activities of matrix metalloproteinases 2, 8, and 9 by chlorhexidine. Clinical and diagnostic laboratory immunology, v. 6, n. 3, p. 437–9, maio 1999. GILBERT, G. H. et al. Operative Dentistry Procedures : Findings From The Dental PBRN.Operative Dentistry, v.35, n.5 p. 491–499, 2010. GÖSTEMEYER, G.; SCHWENDICKE, F. Inhibition of hybrid layer degradation by cavity pretreatment: Meta- and trial sequential analysis. Journal of dentistry, v. 49, p. 14–21, jun. 2016. GRIPPO, J. O.; SIMRING, M.; SCHREINER, S. Attrition, abrasion, corrosion and abfraction revisited: a new perspective on tooth surface lesions. Journal of the American Dental Association (1939), v. 135, n. 8, p. 1109-18–5, ago. 2004. GUIMARÃES, J. C. et al. Stress amplifications in dental non-carious cervical lesions. Journal of Biomechanics, v. 47, n. 2, p. 410–416, 2014. HEASMAN, P. A. et al. Evidence for the occurrence of gingival recession and non-carious cervical lesions as a consequence of traumatic toothbrushing. Journal of Clinical Periodontology, v. 42, n. S16, p. S237–S255, 2015. HEINTZE, S. D.; RUFFIEUX, C.; ROUSSON, V. Clinical performance of cervical restorations — A meta-analysis.Dental Materials, v. 6, p. 993–1000, 2010. HICKEL, R. et al. FDI World Dental Federation - clinical criteria for the evaluation of direct and indirect restorations. Update and clinical examples. The journal of adhesive dentistry, v. 12, n. 4, p. 259–72, ago. 2010. JENA, A.; SHASHIREKHA, G. Comparison of efficacy of three different desensitizing agents for in-office relief of dentin hypersensitivity: A 4 weeks clinical study. Journal of Conservative Dentistry, v. 18, n. 5, p. 389, 2015.
91
KUROE, T. et al. Biomechanical effects of cervical lesions and restoration on periodontally compromised teeth. Quintessence international (Berlin, Germany : 1985), v. 32, n. 2, p. 111–8, fev. 2001. LEYBOVICH, M. et al. Treatment of noncarious cervical lesions by a subepithelial connective tissue graft versus a composite resin restoration. The International journal of periodontics & restorative dentistry, v. 34, n. 5, p. 649–54, 2014. LITONJUA, L. A.; ANDREANA, S.; COHEN, R. E. Toothbrush abrasions and noncarious cervical lesions: evolving concepts. Compendium of continuing education in dentistry (Jamesburg, N.J. : 1995), v. 26, n. 11, p. 767–8, 770–4, 776 passim, nov. 2005. LOGUERCIO, A. D. et al. A six-month clinical study of a self-etching and an etch-and-rinse adhesive applied as recommended and after doubling the number of adhesive coats. The journal of adhesive dentistry, v. 8, n. 4, p. 255–61, ago. 2006. LOGUERCIO, A. D. et al. A 36-month evaluation of self-etch and etch-and-rinse adhesives in noncarious cervical lesions. Journal of the American Dental Association (1939), v. 138, n. 4, p. 507-14–7, abr. 2007. MAHN, E.; ROUSSON, V.; HEINTZE, S. Meta-Analysis of the Influence of Bonding Parameters on the Clinical Outcome of Tooth-colored Cervical Restorations. The journal of adhesive dentistry, v. 17, n. 5, p. 391–403, ago. 2015. MANNOCCI, F. et al. Deproteinization Effects of NaOCl on Acid-etched Dentin in Clinically-relevant vs Prolonged Periods of Application. A Confocal and Environmental Scanning Electron Microscopy Study. Operative Dentistry, p. 34–2, 2009. MAROSO, F. B. et al. Correlation between gingival thickness and gingival recession in humans. Acta odontologica latinoamericana : AOL, v. 28, n. 2, p. 162–6, 2015. MAZZONI, A. et al. Reactivation of inactivated endogenous proteolytic activities in phosphoric acid-etched dentine by etch-and-rinse adhesives. Biomaterials, v. 27, n. 25, p. 4470–4476, 2006. MILLER, P. D. A classification of marginal tissue recession. The International journal of periodontics & restorative dentistry, v. 5, n. 2, p. 8–13, 1985. MONTAGNER, A. F. et al. Effect of Pre-treatment with Chlorhexidine on the Retention of Restorations: A Randomized Controlled Trial. Brazilian dental journal, v. 26, n. 3, p. 234–241, 2015. MONTAGNER, A F. et al. MMP Inhibitors on Dentin Stability: A Systematic Review and Meta-analysis. Journal of Dental Research, v. 93, n. 8, p. 733–743, 2014. NAMGUNG, C. et al. A retrospective clinical study of cervical restorations: longevity and failure-prognostic variables. Operative dentistry, 2013. OPDAM, N. J. M. et al. 12-Year Survival of Composite Vs. Amalgam Restorations. Journal of dental research, v. 89, n. 10, p. 1063–1067, 2010. OPDAM, N. J. M. et al. Longevity of posterior composite restorations: a systematic review and meta-analysis. Journal of dental research, v. 93, n. 10, p. 943–949, 2014. PAOLANTONIO, M. et al. Clinical and microbiological effects of different restorative materials on the periodontal tissues adjacent to subgingival class V restorations. 1-Year results. Journal of Clinical Periodontology, v. 31, n. 3, p. 200–207, 2004.
92
PERDIGÃO, J. Dentin bonding — Variables related to the clinical situation and the substrate treatment. Dental Materials, v. 6, n. 1996, p. 24–37, 2009. PEREZ, C. D. R. et al. Restoration of noncarious cervical lesions: when, why, and how. International Journal of Dentistry, v. 2012, p. 687058, 2012. PETERSSON, L. G. The role of fluoride in the preventive management of dentin hypersensitivity and root caries. Clinical Oral Investigations, v. 17, n. SUPPL.1, p. 63–71, 2013. PEUMANS, M. et al. Clinical effectiveness of contemporary adhesives : A systematic review of current clinical trials.Dental Materials, v.21, n.9 p. 864–881, 2005. PEUMANS, M. et al. Eight-year clinical evaluation of a 2-step self-etch adhesive with and without selective enamel etching. Dental Materials, v. 26, n. 12, p. 1176–1184, 2010. PEUMANS, M. et al. Clinical effectiveness of contemporary adhesives for the restoration of non-carious cervical lesions. A systematic review. Dental Materials, 2014. PIKDÖKEN, L. et al. Cervical wear and occlusal wear from a periodontal perspective. Journal of Oral Rehabilitation, v. 38, n. 2, p. 95–100, 2011. PIMENTA, L.-A. F. et al. Stability of dentin bond strengths using different bonding techniques after 12 months: total-etch, deproteinization and self-etching. Operative dentistry, v. 29, n. 5, p. 592–8, 2004. PUCCI, C. R. et al. Influence of Dentin Deproteinization on Bonding Degradation: 1-year Results. The journal of contemporary dental practice, v. 17, n. 12, p. 985–989, 2016. RASKIN, A. et al. Influence of the isolation method on the 10-year clinical behaviour of posterior resin composite restorations. Clinical oral investigations, v. 4, n. 3, p. 148–52, 2016. REIS , A. et al. Effect of sodium hypochlorite on the bond strength of an adhesive system to superficial and deep dentin. Journal of Applied Oral Science, v.11, n.3, 2003. RICCI, H. A. et al. Chlorhexidine increases the longevity of in vivo resin-dentin bonds. European Journal of Oral Sciences, v. 118, n. 4, p. 411–416, 2010. RITTER, A. V et al. Clinical evaluation of an all-in-one adhesive in non-carious cervical lesions with different degrees of dentin sclerosis. Operative dentistry, v. 33, p. 370–378, 2008. SANTAMARÍA, M. P. et al. Connective tissue graft and resin glass ionomer for the treatment of gingival recession associated with noncarious cervical lesions: a case series. The International journal of periodontics & restorative dentistry, v. 31, n. 5, p. e57-63, 2011. SANTOS, V. R. et al. Effects of Glass Ionomer and Microfilled Periodontal Tissue and Subgingival Biofilm : A 6-Month Evaluation. Journal of Periodontology, v. 78, n. 8, 2007. SARTORI, N. et al. Influence of chlorhexidine digluconate on the clinical performance of adhesive restorations: A 3-year follow-up. Journal of Dentistry, v. 41, n. 12, p. 1188–1195, 2013. SCHULZ, K. F.; ALTMAN, D. G.; MOHER, D. WITHDRAWN: CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. International Journal of Surgery, v. 115, n. 5, p. 1063–1070, 2010. SGOLASTRA, F. et al. Lasers for the treatment of dentin hypersensitivity: a meta-analysis. Journal of dental research, v. 92, n. 6, p. 492–9, 2013.

93
SHARIF, M. O.; IRAM, S.; BRUNTON, P. A. Effectiveness of arginine-containing toothpastes in treating dentine hypersensitivity: A systematic review. Journal of Dentistry, v. 41, n. 6, p. 483–492, 2013. SHINOHARA, M. S. et al. The Effect of Sodium Hypochlorite on Microleakage of Composite Resin Restorations Using Three Adhesive Systems. v. 6, n. 2, 2004. SZESZ, A. et al. Selective enamel etching in cervical lesions for self-etch adhesives: A systematic review and meta-analysis. Journal of Dentistry, v. 53, p. 1–11, 2016. TAY, F. R.; PASHLEY, D. H. Resin bonding to cervical sclerotic dentin : A review.Journal of Dentistry , v.32, p. 173–196, 2004. TIWANA, K. K.; MORTON, T.; TIWANA, P. S. Aspiration and ingestion in dental practice: a 10-year institutional review. Journal of the American Dental Association (1939), v. 135, n. 9, p. 1287–91, 2004. TOMASIK, M. [Analysis of etiological factors involved in noncarious cervical lesions]. Annales Academiae Medicae Stetinensis, v. 52, n. 3, p. 125–36, 2006. TORRES, C. R. G. et al. Five-year clinical performance of the dentine Deproteinization Technique in non-carious cervical lesions. Journal of Dentistry, 2014. UCEDA-GÓMEZ, N. et al. Long-term bond strength of adhesive systems applied to etched and deproteinized dentin. Journal of Applied Oral Science,v.15, n.6, 2007. VAN MEERBEEK, B. et al. State of the art of self-etch adhesives. Dental Materials, v. 27, n. 1, p. 17–28, 2010. VANDANA, K. L.; SAVITHA, B. Thickness of gingiva in association with age, gender and dental arch location. Journal of Clinical Periodontology, v. 32, n. 7, p. 828–830, 2005. VIEIRA, G. H. A. et al. Effect of Whitening Toothpastes on Dentin Abrasion: An In Vitro Study. Oral health & preventive dentistry, v. 14, n. 6, p. 547–553, 2016. WANG, Y. et al. Rubber dam isolation for restorative treatment in dental patients. Cochrane Database of Systematic Reviews, v. 2016, n. 9, 2016. WEST, N. X. et al. Dentin hypersensitivity: Pain mechanisms and aetiology of exposed cervical dentin. Clinical Oral Investigations, v. 17, n. SUPPL.1, p. 9–19, 2013. WIEGAND, A. E.; SCHLUETER, N. The Role of oral hygiene: Does toothbrushing harm? Erosive Tooth Wear: From Diagnosis to Therapy, v. 25, p. 215–219, 2012. YANG, S.; LEE, H.; JIN, S.-H. A combined approach to non-carious cervical lesions associated with gingival recession. Restorative dentistry & endodontics, v. 41, n. 3, p. 218–24, ago. 2016. ZUCCHELLI, G. et al. Non-Carious Cervical Lesions Associated With Gingival Recessions: A Decision-Making Process. Journal of Periodontology, v. 82, p. 1713–1724, 2011.

94
Apêndices
95
APÊNDICE A – Carta de informação ao paciente (Follow-up 60 meses)
Universidade Federal de Pelotas
Faculdade de Odontologia
Programa de Pós-Graduação em Odontologia
CARTA DE INFORMAÇÃO AO PACIENTE
O objetivo deste estudo será verificar a influência da técnica de isolamento
utilizada para controle de umidade do campo operatório através da avaliação do
desempenho clínico longitudinal de restaurações em lesões cervicais não-
cariosas.
As técnicas de isolamento constituem métodos empregados
rotineiramente para controle de umidade na prática clínica. Os materiais
utilizados estão disponíveis no mercado odontológico e foram previamente
avaliados quanto as suas propriedades físicas e biológicas, sem demonstrar
nenhum risco à integridade do ser humano.
Sendo assim, dou pleno consentimento para a Faculdade de
Odontologia da Universidade Federal de Pelotas (FOUFPEL), por intermédio de
aluno(s) de graduação, aluno(s) de pós-graduação e professor(es) devidamente
autorizados e envolvidos neste estudo, realizar diagnóstico, planejamento,
tratamento, fotografias, moldagens, além de consultas de avaliação, de acordo
com os conhecimentos enquadrados no campo desta especialidade.
Concordo, ainda, que a documentação referente aos exames efetuados
e quaisquer outras informações concernentes ao estudo constituem propriedade
exclusiva da FOUFPEL, à qual concedo pleno direito de uso para fins de ensino
e divulgação, respeitando os respectivos códigos de ética. Também me disponho
a participar das reavaliações clínicas para controle do tratamento.
Pelotas, _____ de _________________ de 2010.
_________________________ Documento no: _______________________
Assinatura do paciente
96
APÊNDICE B – Termo de consentimento livre e esclarecido (Follow-up 60 meses)
Universidade Federal de Pelotas
Faculdade de Odontologia
Programa de Pós-Graduação em Odontologia
TERMO DE CONSENTIMENTO LIVRE E ESCLARECIDO
Título do projeto: Influência do isolamento do campo operatório em
restaurações Classe V: Ensaio clínico randomizado.
Pesquisador responsável pelo estudo: Silvia Terra Fontes
Nome do paciente: ___________________________________ Ficha no:
_______Por este instrumento que atende às exigências legais, o(a)
senhor(a)________________________________________________________
_, portador(a) da cédula de identidade nº________________________
SSP/___, após leitura minuciosa da CARTA DE INFORMAÇÃO AO PACIENTE,
detalhadamente explicada pelos pesquisadores envolvidos neste estudo, ciente
dos procedimentos aos quais será submetido(a), não restando dúvidas a
respeito do lido e do explicado, firma CONSENTIMENTO LIVRE E
ESCLARECIDO em concordância a participar da pesquisa proposta no que lhe
é cabível, conforme a carta de informação ao paciente.
Fica claro que o paciente ou seu representante legal pode, a qualquer
momento, retirar seu consentimento livre e esclarecido, sem ser prejudicado no
tratamento, deixando de participar do estudo alvo da pesquisa e estando ciente
que todo trabalho realizado torna-se informação confidencial guardada por força
do sigilo profissional (Art. 9º do Código de Ética Odontológica).
Por estarem entendidos e conformados, assinam o presente termo.
Pelotas, _____ de _________________ de 2010.
____________________________ _________________________
Assinatura do paciente Assinatura do pesquisador
97
APÊNDICE C – Carta de informação ao paciente (Follow-up 36 meses)
Universidade Federal de Pelotas Faculdade de Odontologia
Programa de Pós-Graduação em Odontologia
CARTA DE INFORMAÇÃO AO PACIENTE
O objetivo deste estudo será avaliar a influência da aplicação de digluconato de clorexidina 2 % (solução antibacteriana utilizada para diversos fins em Odontologia), em dentina na resistência de união (força entre o dente/restauração), e na estabilidade de união proporcionada por diferentes sistemas adesivos.
Os materiais utilizados estão disponíveis no mercado odontológico e foram previamente avaliados quanto as suas propriedades físicas e biológicas, sem demonstrar nenhum risco a integridade do ser humano.
Caso aceite participar desta pesquisa, serão confeccionadas janelas (espaços) na parte que simula a gengiva de sua prótese, com necessidade de troca, e colocados no interior fatias de dente humano, extraído de outro paciente e autoclavado, que será restaurado com resina composta, permanecendo por 6 meses. Essas janelas serão protegidas com telas plásticas para evitar que as fatias se desloquem quando o paciente se alimenta ou realiza higiene bucal.
Quanto aos riscos, eles são mínimos e referem-se, principalmente, ao acúmulo de placa dentária em função das janelas (espaços) abertas nas próteses. Porém é importante ressaltar que poderá continuar a limpeza normal de sua prótese. E todos os voluntários receberão tratamento necessário e serão encaminhados às clínicas da Faculdade para realização de tratamento.
Caso não aceite participar desta pesquisa, você será atendido com a
mesma agilidade e rapidez como aqueles que optarem pela sua participação no
estudo.
Sendo assim, dou pleno consentimento para a Faculdade de Odontologia da Universidade Federal de Pelotas (FOUFPel), por intermédio de aluno(s) de Graduação, aluno(s) de pós-graduação e professor(es) devidamente autorizados e envolvidos neste estudo, realizar diagnóstico, planejamento, tratamento, fotografias, além de consultas de avaliação, de acordo com os conhecimentos enquadrados no campo desta especialidade.
Concordo, ainda, que a documentação referente aos exames efetuados e quaisquer outras informações concernentes ao estudo constituem propriedade exclusiva da FOUFPel, a qual concedo pleno direito de uso para fins de ensino e divulgação, respeitando os respectivos códigos de ética.
Qualquer dúvida, pode-se entrar em contato com o pesquisador responsável pelo fone 53-81257290.
Pelotas, _____ de _________________ de 2011. _________________________ Documento no: _______________________ Assinatura do paciente
98
APÊNDICE D – Termo de consentimento livre e esclarecido (Follow-up 36 meses)
Universidade Federal de Pelotas Faculdade de Odontologia
Programa de Pós-Graduação em Odontologia
TERMO DE CONSENTIMENTO LIVRE E ESCLARECIDO
Titulo do projeto: ESTUDO IN SITU: RESISTÊNCIA DE UNIÃO DE SISTEMA ADESIVOS EM DENTINA PRÉ-TRATADA COM CLOREXIDINA E SUBMETIDA A ENVELHECIMENTO IN VIVO. Pesquisadora responsável pelo estudo: Anelise Fernandes Montagner
Nome do paciente: ___________________________________ Ficha no: _______________. Por este instrumento que atende as exigências legais, o(a) senhor(a)_______________________________________________________, portador(a) da cédula de identidade no________________________ SSP/___, após leitura minuciosa da CARTA DE INFORMAÇÃO AO PACIENTE, detalhadamente explicada pelos pesquisadores envolvidos neste estudo, ciente dos procedimentos aos quais será submetido(a), não restando dúvidas a respeito do lido e do explicado, firma CONSENTIMENTO LIVRE E ESCLARECIDO em concordância a participar da pesquisa proposta no que lhe é cabível, conforme a carta de informação ao paciente.
Fica claro que o paciente ou seu representante legal pode, a qualquer momento, retirar seu consentimento livre e esclarecido, sem ser prejudicado no tratamento, deixando de participar do estudo alvo da pesquisa e estando ciente que todo trabalho realizado torna-se informação confidencial guardada por força do sigilo profissional (Art. 9o do Código de Ética Odontológica).
Por estarem entendidos e conformados, assinam o presente termo.
Pelotas, _____ de _________________ de 2011.
_________________________ __________________________ Assinatura do paciente Assinatura do pesquisador Fone: 53 81257290

99
APÊNDICE E - Ficha Clinica
DADOS DE IDENTIFICAÇÃO
Nome completo: ___________________________________________________________________ Data: ____/___ /__________ Ficha no: _________
Data de nascimento: ____/_____ /__________ Idade: ______ anos Prontuário no: __________ (Faculdade de Odontologia)
Sexo: ( ) F ( ) M Cor da pele: _________ Estado civil: ____________________________ Indicado por: _________________________________
Escolaridade: _______________________________ Renda familiar: __________________________ Naturalidade: _________________________________
Endereço (res.): _____________________________ Número: ________ Complemento: _______ Nacionalidade: ________________________________
Bairro: _____________________________________ Cidade: ________________________________ Estado: ______________________________________
CEP: _____________________-_________________ R.G.: __________________________________ Email: _______________________________________
Endereço (prof.): ____________________________ Número: ________ Complemento: _______ Profissão: ____________________________________
Telefones: 1) _____________ (residencial) 2) _____________ (profissional) 3) _____________ (celular) 4) _____________ (outro )
ANAMNESE GERAL
Não Sim Observações
Fumante (CE) No de cigarros/dia: ________
Gestante ou lactante
Alergias (medicamentos, anestesias, etc.)
Doenças infecciosas (hepatite, tuberculose, herpes, etc.)
Doenças crônicas (diabete, hipertensão, d. cardíacas, respiratórias, endócrinas, etc.)
Medicamentos em uso (analgésico, antibiótico, contraceptivo oral, etc.)
Procedimentos cirúrgicos recentes (± 1 ano)
ANAMNESE ODONTOLÓGICA
Não Sim Observações
Queixa principal (problema odontológico)
Percepção de sangramento gengival ao escovar os dentes
Higiene bucal ( ) escova de dentes ( )Macia/ ( ) Média /( )Dura ( ) fio ou fita dental ( ) dentifrício Tipo_______________ ( ) enxaguatório bucal Escovação : ( ) traumática/ ( ) atraumática
Freqüência diária: ________ Sentido da escovação: ________________ ( ) Destro ( ) Canhoto
Flúor ( ) água de abastecimento ( ) água mineral ( ) dentifrício ( ) bochecho ( ) profissional
Sacarose Freqüência diária: ________
Alimentos e bebidas ácidas Freqüência diária: ________
Sensação de boca seca Freqüência diária: ________
Problemas para abrir a boca ( ) dor ( ) ruído ( ) limitação de movimento ( ) dificuldade ao mastigar ( ) outra ______________
100
Hábitos nocivos ( ) rói unhas ( ) masca chiclete ( ) morde palito, grampo, caneta, cachimbo, etc.
Alterações Oclusais ( ) dores de cabeça região temporal ( ) dores em região de ATM ( ) estalos ao abrir e/ou fechar a boca ( ) apertamento dentário ( ) range dentes ( ) desgaste de cúspides dentárias
Aparelho ortodôntico, placa ou prótese (CE)
Tratamentos dentários recentes (± 1 ano)
ODONTOGRAMA
18 17 16 15 14 13 12 11 21 22 23 24 25 26 27
28
48 47 46 45 44 43 42 41 31 32 33 34 35 36 37 38
LEGENDA
* Cálculo / Ausente Lesão cervical
FD - Faceta de desgaste
RA – Restauração de amálgama
RR - Restauração de resina
RP - Restauração provisória
RG – Recessão gengival
C - Cavidade
EXAME CLÍNICO
Características
No de dentes em boca: _____ (CE) Elementos ausentes:
Classificação das oclusopatias (Angle)
( ) Oclusão normal – Relação ântero-posterior normal.
( ) Classe I – Oclusopatia na região anterior.
( ) Classe II – Retrognatismo mandibular.
( ) Classe III – Prognatismo mandibular.
Movimentos mandibulares Lado direito ( ) Guia canina ( ) Função de grupo
Lado esquerdo ( ) Guia canina ( ) Função de grupo
Lesões cervicais não cariosas Atenção: As lesões selecionadas para a amostra deverão ser circuladas, as demais deverão ser anotadas apenas.
( ) Dentes anteriores Incisivos:
Caninos:
( ) Dentes posteriores Pré-molares:
Molares:
Forma ( ) Forma angulada, em cunha ou “V”
( ) Forma circular, em pires ou “U”
Profundidade (dimensão horizontal)
( ) < 1 mm
( ) 1 a 2 mm
( ) 3 a 4 mm
( ) > 4 mm
Altura (dimensão vertical) ( ) < 1 mm
( ) 1 a 2 mm
( ) 3 a 4 mm
( ) > 4 mm
Relação da parede cervical da lesão com a margem gengival
( ) Supragengival
( ) Ao nível da gengiva
( ) Subgengival
101
Facetas de desgaste (CE) ( ) Perda estrutural ≤ 50 % ( ) Perda estrutural > 50 %
Esclerose dentinária ( ) Ausente
( ) Leve
( ) Moderada
( ) Severa
Sensibilidade dentinária Atenção: Deve ser utilizado jato de ar por 3s junto da ESCALA ANALÓGICA VISUAL.
( ) Ausente
( ) Leve
( ) Moderada
( ) Considerável
( ) Severa
Vitalidade pulpar (CE) Atenção: Deve ser utilizado spray refrigerante.
( ) Sim.
( ) Não.
Motivo da necessidade de intervenção
( ) insatisfação estética ( ) hipersensibilidade dentinária
( ) limitação da progressão da lesão
EXAME PERIODONTAL
Examinador: _______________________ Estado atual de higiene bucal: Bom (ISG ≤ 20%) Deficiente (ISG > 20%)
102
Examinador: _______________________ Estado atual de higiene bucal: Bom (ISG ≤ 20%) Deficiente (ISG > 20%)
PLANO DE TRATAMENTO OBSERVAÇOES
( ) CE = Critério de Exclusão
CRONOGRAMA DE ATENDIMENTO
Data Operador Materiais utilizados e procedimentos efetuados

103
PACIENTE: Avaliador 1:
Avaliador 2:
DATA DO
EXAME
DENT
E
CRITÉRIOS DE AVALIAÇÃO
Propriedades
Estéticas
Propriedades
Funcionais
Propriedades
Biológicas
1. B
rilh
o s
uper
fici
al
2.a
. M
anch
amen
to s
uper
fici
al
2.b
. M
anch
amen
to m
argin
al
3. E
stab
ilid
ade
de
cor
e tr
ansl
uci
dez
4. F
orm
a an
atôm
ica
5.a
. F
ratu
ra
5.b
. R
eten
ção
6. A
dap
taçã
o m
argin
al
7. P
erce
pçã
o d
o p
acie
nte
8. R
ecorr
ênci
a da
pat
olo
gia
9. In
tegri
dad
e d
enta
l
10.a
. S
ensi
bil
idad
e pós-
oper
atóri
a
10.b
. V
ital
idad
e pulp
ar
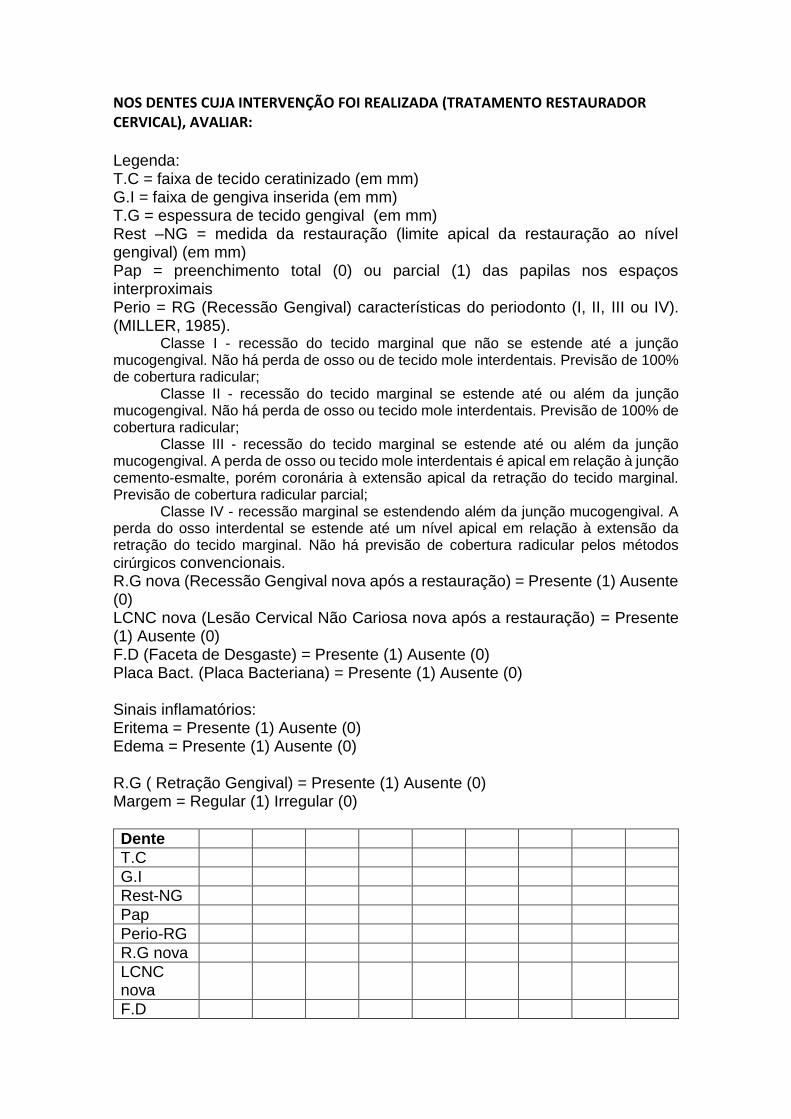
104
NOS DENTES CUJA INTERVENÇÃO FOI REALIZADA (TRATAMENTO RESTAURADOR CERVICAL), AVALIAR: Legenda: T.C = faixa de tecido ceratinizado (em mm) G.I = faixa de gengiva inserida (em mm) T.G = espessura de tecido gengival (em mm) Rest –NG = medida da restauração (limite apical da restauração ao nível gengival) (em mm) Pap = preenchimento total (0) ou parcial (1) das papilas nos espaços interproximais Perio = RG (Recessão Gengival) características do periodonto (I, II, III ou IV). (MILLER, 1985).
Classe I - recessão do tecido marginal que não se estende até a junção mucogengival. Não há perda de osso ou de tecido mole interdentais. Previsão de 100% de cobertura radicular;
Classe II - recessão do tecido marginal se estende até ou além da junção mucogengival. Não há perda de osso ou tecido mole interdentais. Previsão de 100% de cobertura radicular;
Classe III - recessão do tecido marginal se estende até ou além da junção mucogengival. A perda de osso ou tecido mole interdentais é apical em relação à junção cemento-esmalte, porém coronária à extensão apical da retração do tecido marginal. Previsão de cobertura radicular parcial;
Classe IV - recessão marginal se estendendo além da junção mucogengival. A perda do osso interdental se estende até um nível apical em relação à extensão da retração do tecido marginal. Não há previsão de cobertura radicular pelos métodos
cirúrgicos convencionais. R.G nova (Recessão Gengival nova após a restauração) = Presente (1) Ausente (0) LCNC nova (Lesão Cervical Não Cariosa nova após a restauração) = Presente (1) Ausente (0) F.D (Faceta de Desgaste) = Presente (1) Ausente (0) Placa Bact. (Placa Bacteriana) = Presente (1) Ausente (0) Sinais inflamatórios: Eritema = Presente (1) Ausente (0) Edema = Presente (1) Ausente (0) R.G ( Retração Gengival) = Presente (1) Ausente (0) Margem = Regular (1) Irregular (0)
Dente
T.C
G.I
Rest-NG
Pap
Perio-RG
R.G nova
LCNC nova
F.D
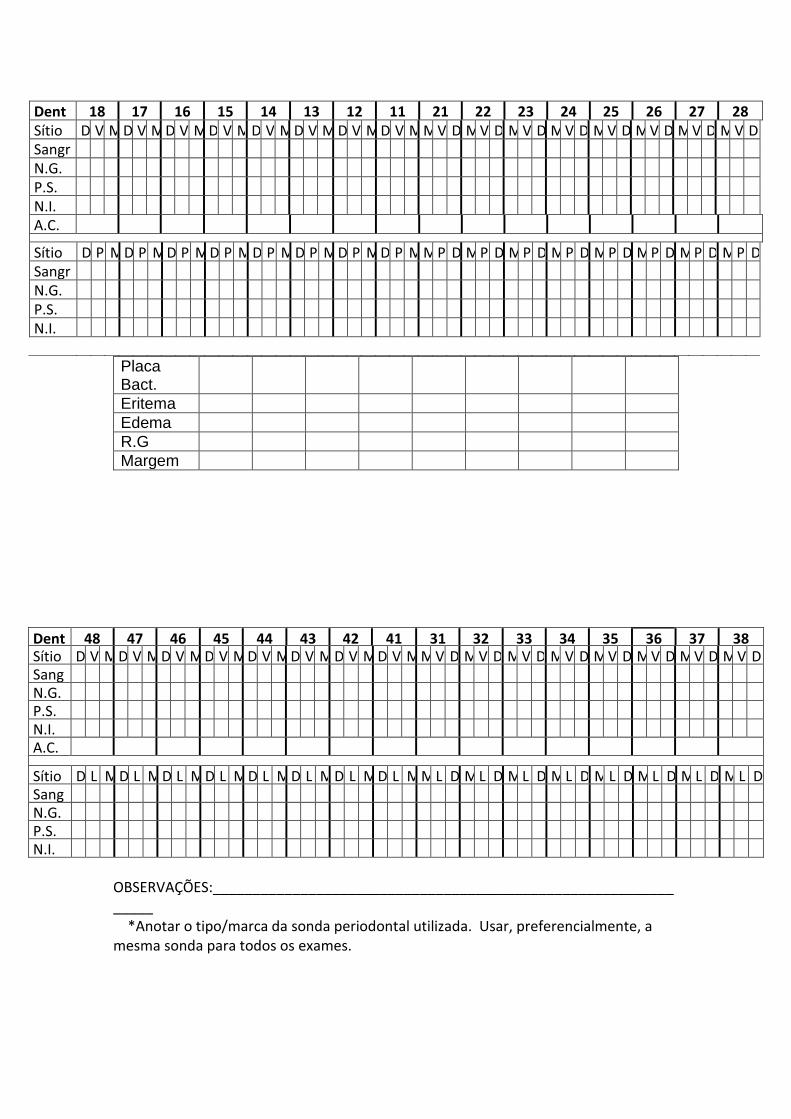
105
Placa Bact.
Eritema
Edema
R.G
Margem
Dente
48 47 46 45 44 43 42 41 31 32 33 34 35 36 37 38 Sítio D V M D V M D V M D V M D V M D V M D V M D V M M V D M V D M V D M V D M V D M V D M V D M V D Sangr.
N.G. P.S. N.I. A.C. Sítio D L M D L M D L M D L M D L M D L M D L M D L M M L D M L D M L D M L D M L D M L D M L D M L D Sangr.
N.G. P.S. N.I.
OBSERVAÇÕES:_______________________________________________________________ *Anotar o tipo/marca da sonda periodontal utilizada. Usar, preferencialmente, a mesma sonda para todos os exames.
Dente
18 17 16 15 14 13 12 11 21 22 23 24 25 26 27 28 Sítio D V M D V M D V M D V M D V M D V M D V M D V M M V D M V D M V D M V D M V D M V D M V D M V D Sangr.
N.G. P.S. N.I. A.C. Sítio D P M D P M D P M D P M D P M D P M D P M D P M M P D M P D M P D M P D M P D M P D M P D M P D Sangr.
N.G. P.S. N.I.
106
ENTREVISTA: Presença de hábitos bucais nocivos ( )não ( ) sim . Quais? __________ Paciente lembra de ter recebido alguma orientação após tratamento? (escovação e/ou dieta) ( )não ( ) sim Paciente abandonou algum hábito nocivo desde o inicio do tratamento? ( )não ( )sim Tipo de escova do paciente ( )macia ( )média ( )dura Qual o estado da escova de dentes do paciente ( )bom ( )regular ( ) ruim Paciente utiliza dentifrício com abrasivo? ( )não ( )sim . Qual? ________ Paciete possuía sensibilidade antes da restauração? ( )não ( )sim Se sim, diminuiu após a restauração? ( )não ( )sim

107
Apêndice F – Nota da Dissertação
A multidisciplinariedade envolvida na confecção e manutenção de
restaurações em lesões cervicais não cariosas
The multidisciplinarity involved in the confection and maintenance of restorations in non-carious cervical lesions
A presente dissertação de mestrado incluiu pacientes que possuíssem lesões
cervicais, cuja localização é perto da genviva, e que não fossem causadas por
cárie, mas sim por uma associação de fatores, como a abrasão (geralmente
resultante de uma escovação traumática), erosão (na maioria dos casos por
fatores relacionados à dieta ácida ou doenças gástricas como refluxo) e
abfração (comumente evidenciada por trauma oclusal). Sendo assim, o estudo
objetivou verificar como restaurações de lesões cervicais não cariosas se
comportam ao longo do tempo, tanto do ponto de vista restaurador (qualidade
da restauração), quanto periodontal (saúde dos tecidos moles adjacentes). Os
resultados obtidos neste estudo nos fazem refletir sobre a importância da
correta execução das etapas clínicas envolvidas no tratamento restaurador,
não se fazendo necessário o uso de substâncias que aumentem a retenção
das restaurações, afinal elas se mostraram satisfatórias quando bem
executadas. Ainda, é de suma relevância, uma atenta instrução de higiene aos
pacientes, para que estes possam realizar uma escovação atraumática e
eficiente no controle de placa, e assim, possam manter a saúde gengival. Por
fim, esta dissertação mostrou a importância do fornecimento de instruções aos
pacientes, bem como ver o paciente de maneira holística e procurar tratar a
doença, que é multifatorial, da maneira mais adequada para cada tipo de
paciente, tratando as lesões já existentes e procurando prevenir o avanço e/ou
surgimento de novas.
Campo da pesquisa: Clínica Odontológica, Materiais Odontológicos, Periodontia. Candidato: Morgana Favetti, Cirurgiã-dentista pela Universidade Federal de Pelotas (2014) Data da defesa e horário: 21/02/2017 às 9h
108
Local: Auditório do Programa de Pós-graduação em Odontologia da Universidade Federal de Pelotas. 5º andar da Faculdade de Odontologia de Pelotas. Rua Gonçalves Chaves, 457. Membros da banca: Prof. Dr. Mauro Elias Mesko, Universidade Federal de Pelotas, Doutor em Odontologia, área de concentração em Dentística Restauradora. Prof. Dra. Patrícia Daniela Melchiors Angst, Universidade Federal do Rio Grande do Sul, Doutora em Clínica Odontológica, área de concentração em Periodontia. Prof. Dr. Fábio Herrmann Coelho de Souza, Universidade Federal de Pelotas, Doutor em Odontologia, área de concentração em Dentística. (suplente) Prof. Dra. Gabriela Romanini Basso, Universidade Federal de Pelotas, Doutora em Odontologia, área de concentração em Materiais Odontológicos. (suplente) Orientador: Prof. Dr. Maximiliano Sérgio Cenci, Universidade Estadual de Campinas, Doutor em Odontologia, Área de concentração em Cariologia. Co-orientadores: Prof. Dr. Thiago Marchi Martins, Universidade Estadual Paulista Júlio de Mesquita Filho, Doutor em Odontologia, Área de concentração em Periodontia e Prof. Dra. Anelise Fernandes Montagner, Universidade Federal de Pelotas, Doutora em Odontologia, Área de concentração em Dentística. Informação de contato: Morgana Favetti, [email protected], Rua Alvaro Chaves, 2015, apto.203.

109
Apêndice G – Súmula do currículo do candidato
Súmula do currículo
Morgana Favetti nasceu em 17 de Janeiro de 1990, em Joaçaba, Santa Catarina.
Completou o ensino fundamental em Escola Estadual em Luzerna, e médio em
Escola privada em Joaçaba. No ano de 2009 ingressou na Faculdade de
Odontologia da Universidade Federal de Pelotas (UFPel), tendo sido graduada
cirugiã-dentista em 2014. No ano seguinte ingressou no Mestrado do Programa
de Pós-graduação em Odontologia da Universidade Federal de Pelotas (UFPel),
área de concentração Dentística, sob orientação do Prof. Dr. Maximiliano Sérgio
Cenci. Durante o período de graduação foi bolsista do Programa PET- Saúde.
Durante o período de mestrado foi bolsista da CAPES e desenvolvou trabalhos
na interface dentística-periodontia.
Publicações:
Prevalência de Fluorose Dentária em Adolescentes de Escolas Municipais da
Área Urbana do Município de Pelotas/RS, 2010. Spohr, RA, Menegaz, AM,
Favetti M, Flores RZ, Horn T, Benetti T, Bighetti TI. Revista da Faculdade de
Odontologia de Porto Alegre. 2010.
Custo das hospitalizações por infecções focais dentárias em um município do sul
do Brasil. Favetti M, Spohr AR, Flores RZ, Horn T, Benetti T, Bighetti TI, de
Castilhos ED, Torriani MA. Revista de Cirurgia e Traumatologia Buco-Marxilo-
Facial. 2015.
Efetividade de mantedores de espaço em odontopediatria: revisão sistemática.
Menegaz AM, Favetti M, Michelon D, Azevedo MS, da Costa CT. Revista da
Faculdade de Odontologia de Passo Fundo. 2015.
Effectiveness of pre-treatment with chlorhexidine in restoration retention: a 36-
month follow-up randomized clinical trial. Favetti M, Schroeder T, Montagner
AF,
Correa MB, Pereira-Cenci T, Cenci MS. Journal of Dentistry. (Aceito com
modificações em 20/01/2017).

110
Anexos
111
ANEXO A – Parecer do Comitê de Ética em Pesquisa (Follow-up 36 meses)
112
ANEXO B– Parecer do Comitê de Ética em Pesquisa (Follow-up 60 meses)