universidade federal do cearÁ - repositorio.ufc.br · “porque deus amou o mundo de tal forma,...
TRANSCRIPT

1
UNIVERSIDADE FEDERAL DO CEARÁ
CAMPUS DE SOBRAL
SHIRLEY MOREIRA ALVES
LECTINA DE ABELMOSCHUS ESCULENTUS REDUZ HIPERNOCICEPÇÃO
INFLAMATÓRIA NA ARTICULAÇÃO TEMPOROMANDIBULAR DE RATOS
DEPENDENTE DE RECEPTORES OPIOIDES CENTRAIS
SOBRAL-CE
2016

2
SHIRLEY MOREIRA ALVES
LECTINA DE ABELMOSCHUS ESCULENTUS REDUZ HIPERNOCICEPÇÃO
INFLAMATÓRIA NA ARTICULAÇÃO TEMPOROMANDIBULAR DE RATOS
DEPENDENTE DE RECEPTORES OPIOIDES CENTRAIS
Dissertação de Mestrado apresentada ao Programa de Pós-Graduação – Curso Ciências da Saúde, da Universidade Federal do Ceará – Campus Sobral, como requisito parcial para obtenção do Título de Mestre em Ciências da Saúde. Área de concentração: Farmacologia.
Orientadora: Profª. Drª. Hellíada Vasconcelos Chaves
SOBRAL-CE
2016

3
Dados Internacionais de Catalogação na Publicação Universidade Federal do Ceará
Biblioteca Universitária Gerada automaticamente pelo módulo Catalog, mediante os dados fornecidos pelo(a) autor(a)
M839l Moreira Alves, Shirley.
LECTINA DE ABELMOSCHUS ESCULENTUS REDUZ HIPERNOCICEPÇÃO
INFLAMATÓRIA NA ARTICULAÇÃO TEMPOROMANDIBULAR DE RATOS DEPENDENTE DE RECEPTORES OPIOIDES CENTRAIS / Shirley Moreira Alves. – 2017. 65 f. : il. color.
Dissertação (mestrado) – Universidade Federal do Ceará, Campus de Sobral, Programa de Pós-Graduação em Ciências da Saúde, Sobral, 2017. Orientação: Profa. Dra. Hellíada Vasconcelos Chaves.
1. Abelmoschus esculentus. 2. Articulação temporomandibular. 3. TNF-alfa. 4. Hipernocicepção. 5. Lectina. I. Título.
CDD 61

4
SHIRLEY MOREIRA ALVES
LECTINA DE ABELMOSCHUS ESCULENTUS REDUZ HIPERNOCICEPÇÃO
INFLAMATÓRIA NA ARTICULAÇÃO TEMPOROMANDIBULAR DE RATOS
DEPENDENTE DE RECEPTORES OPIOIDES CENTRAIS
Dissertação de Mestrado apresentada ao Programa de Pós-Graduação – Curso Ciências da Saúde, da Universidade Federal do Ceará – Campus Sobral, como requisito parcial para obtenção do Título de Mestre em Ciências da Saúde. Área de concentração: Farmacologia.
Orientadora: Profª. Drª. Hellíada Vasconcelos Chaves
Aprovado em:13/12/2016.
BANCA EXAMINADORA
__________________________________________________ Profª. Drª. Hellíada Vasconcelos Chaves (Orientadora)
Universidade Federal do Ceará (UFC) – Campus Sobral
_____________________________________________ Prof. Dr. Vicente de Paulo Teixeira Pinto
Universidade Federal do Ceará (UFC) – Campus Sobral
____________________________________________ Profª. Drª. Theodora Thaís Arruda Cavalcante
Instituto Superior de Tecnologia Aplicada (INTA) – Campus Sobral

5
A Deus, por todo zelo e cuidado para
comigo. À minha família, alicerce firme
e norteador: Ana Lúcia Moreira, José
Alves da Costa, Sheila Moreira Alves,
Ernando Rodrigues Batista, Antônio
Dias Lima Filho.

6
AGRADECIMENTOS
Ao Senhor Jesus, que é bom em todo o tempo. Tem coração manso e nos
reserva sempre o melhor. Obrigada Senhor!!!
À minha mãe, Ana Lúcia Moreira, por ter escolhido a família muitas vezes
em detrimento de si própria. Mãe, sem você jamais seria quem sou hoje.
Obrigada por você existir, te amo!
Ao meu pai José Alves da Costa, por ter me dado vida e discernimento.
À minha “contraparte clara”: minha irmã Sheila Moreira Alves que nas mais
diversas situações sempre esteve ao meu lado. Essa vitória também é sua.
Ao meu cunhado-irmão Ernando Rodrigues Batista, por se fazer porto
seguro sempre que necessário. Você é presente do Senhor.
Ao meu esposo Antônio Dias Lima Filho, pela paciência e serenidade nos
momentos mais turbulentos. Obrigada pelo apoio e carinho.
A todos os meus professores, desde os primeiros anos de ensino aos dias
de hoje. Sem eles essa conquista não seria possível.
Ao Prof. Dr. Paulo Roberto Santos, pela extrema humildade e sabedoria.
Exemplo a ser seguido.
A Todos que compõem o Laboratório de Farmacologia da UFC – Campus
Sobral na pessoa da Profª Ms. Danielle Rocha do Val. Agradeço cada dia de
dedicação, envolvimento e conhecimento empenhados. Aprendi muito com vocês.
À Profª. Drª. Mirna Marques Bezerra, por deixar transparecer amor em seu
trabalho. Deus é seu escudo e nos presenteia com sua presença.
À minha orientadora, Profª. Drª. Hellíada Vasconcelos Chaves, por toda a
compreensão, paciência e parceria nesse tempo de formação. Sua competência é
inquestionável.

7
À Universidade Federal do Ceará (UFC); ao Laboratório de Farmacologia
de Sobral (LAFS – UFC); ao Programa de Pós-Graduação em Bioquímica; à
Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES); ao
Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq); à
Fundação Cearense de Amparo à Pesquisa (FUNCAP), e ao Instituto de
Biomedicina do Semi-Árido Brasileiro (INCT-IBISAB), pelo apoio e custeio do
presente projeto.
E a todos que de alguma forma contribuíram para a realização deste
trabalho.

8
“Porque Deus amou o mundo de tal
forma, que deu seu único filho, para
todo aquele que nele crê não pereça,
mas tenha vida eterna.” (João, 3:16)

9
RESUMO
Relevância etnofarmacológica: Abelmoschus esculentus é amplamente
cultivada no Nordeste do Brasil para fins medicinais, no tratamento de pneumonia,
bronquite e tuberculose pulmonar, apresentando também atividade anti-
inflamatória. Objetivo do estudo: Avaliar a atividade antinociceptiva e anti-
inflamatória da lectina de Abelmoschus esculentus (AEL) no modelo inflamatório
de hiperalgesia induzida por formalina na articulação temporomandibular (ATM)
de ratos. Materiais e métodos: Os experimentos comportamentais (CEUA nº
02/15) foram realizados em ratos Wistar machos (180-240 g). Os ratos foram pré-
tratados (i.v.) com salina ou AEL (0,001, 0,01 ou 0,1 mg/kg). Depois de 30 min.
receberam uma injeção intra-articular (i.art) de formalina (1,5 %/50 µl) ou solução
salina (controle) na ATM esquerda e foram monitorados durante 45 min. para
observar a resposta comportamental nociceptiva quantificada, em segundos,
pelos atos de coçar da região injetada e erguer a cabeça reflexivamente. Em
seguida, os animais foram anestesiados e submetidos a eutanásia e os tecidos
periarticulares, gânglio trigeminal e subnúcleo caudal foram removidos e
processados para dosagem de TNF-α pelo método ELISA. Para investigar a
permeabilidade vascular, os animais receberam 50 mg/kg (i.v) de corante azul de
Evans 30 min. antes da administração de AEL e, após 30 min., receberam uma
injeção intra-articular de formalina (1,5 %/50 uL). Após 45 min., os animais foram
eutanasiados e as ATMs removidas para análise. Ademais, foi estudada a
participação da via opioide na resposta antinociceptiva de AEL, utilizando o
antagonista opioide Naloxona (15 µg/10 µl) ou os antagonistas dos receptores
opióides Kappa (ҡ), Nor-Binaltorfimina (15 ou 45 µg/10 µl), ou Delta (δ),
Naltrindole (10 ou 30 µg/10 µl), ou mu (µ), CTOP (10 µg/10 µl) por via intra-tecal
15 min. antes da aplicação de AEL. Resultados: AEL (0,01 mg/kg) foi eficaz na
redução da nocicepção induzida por formalina (p<0,05) e extravasamento de azul
de Evans. Houve uma redução dos níveis de TNF-α (p<0,05) no tecido
periarticular, gânglio trigeminal e subnúcleo caudal de ratos pré-tratados com
AEL. Além disso, o efeito antinociceptivo de AEL é dependente dos receptores
opioides ҡ e δ, porém não de µ. Conclusão: AEL apresenta efeitos anti-
inflamatório e antinociceptivo, que podem resultar da inibição de citocinas, da
diminuição do extravasamento plasmático e da ativação de receptores opioides ҡ

10
e δ.Palavras-chave: Abelmoschus esculentus, articulação temporomandibular,
TNF-alfa, hipernocicepção, lectina
Abstract:
Ethnopharmacological relevance: Abelmoschus esculentus is largely cultivated
in Northeastern Brazil for medicinal purposes, like in cases of pneumonia,
bronchitis, pulmonary tuberculosis and inflammation. Aim of the study: To
evaluate the Abelmoschus esculentus (AEL) in reducing formalin-induced
temporomandibular joint inflammatory hypernociception in rats. Materials and
Methods: The behavioral experiments (CEUA nº 02\15) were performed on male
Wistar rats (180–240 g). Rats were pre-treated (i.v.) with AEL (0.001, 0.01 or 0.1
mg/kg) thirty minutes before 1.5% formalin injection in the TMJ. Further, to analyze
the possible effect of opioid pathways on AEL efficacy, animals were pre-treated
via intrathecal injection of naloxone or CTOP (the antagonist of Mu (µ) opioid
receptor), naltrindole (antagonist of Delta (δ) opioid receptor) or Nor-
Binaltorphimine (antagonist of Kappa () opioid receptor) 15 minutes before AEL
followed by intra-TMJ injection of 1.5% formalin. Behavioral analysis were
perfomed, animals were monitored for a 45 min observation period to quantify the
nociceptive response. TMJ tissue, trigeminal ganglion and caudal subnucleus
collection was performed for TNF-α dosage (ELISA). In addition, vascular
permeability was evaluated by Evans Blue extravasation. Results: AEL
significantly reduced formalin-induced TMJ inflammatory hypernociception and
decreased Evans blue extravasation. It also decreased TNF-α levels in TMJ
tissue, trigeminal ganglion and caudal subnucleus. AEL antinociceptive effects,
however, were not observed in the presence of naltrindole or Nor-Binaltorphimine.
Conclusions: These findings suggest that AEL efficacy depends on TNF-α
inhibition and the activation of δ and opioid receptors.
Keywords: Abelmoschus esculentus; temporomandibular joint, TNF-α,
hypernociception, lectin

11
LISTA DE ILUSTRAÇÕES
Quadro 1 - Classificação das Disfunções Temporomandibulares…………….. 19
Figura 1A - Anatomia do Complexo Trigeminal do Tronco Encefálico………… 17
Figura 1 - Eficácia da AEL na hipernocicepção inflamatória induzida por
formalina na ATM de ratos……………………………………………
37
Figura 2 - Efeito de AEL sobre a permeabilidade vascular na
hipernocicepção inflamatória induzida por formalina na ATM de
ratos…………………………………….............................................
37
Figura 3 - Efeito de AEL sobre os níveis de TNF-α na hipernocicepção
inflamatória induzida por formalina na ATM de
ratos…………..…………………………………………………………
38
Figura 4 - Efeito do antagonista não seletivo (naloxona) e seletivos (µ,
eδ) na atividade antinociceptiva de AEL na hipernocicepção
inflamatória induzida por formalina na ATM de
ratos……………………………….…………………………………….
40

12
LISTA DE SIGLAS E ABREVIATURAS
AEL: Lectina de Abelmoschus esculentus
ANOVA: Análise de Variância
ATM: Articulação Temporomandibular
ATP: Adenosina Trifosfato
BioGeR: Laboratório de Genética Bioquímica e Radiobiologia
b2-AR: Adrenoreceptor β2
CAPES: Coordenação de Aperfeiçoamento de Pessoal de Nível Superior
CEUA: Comissão de Ética no Uso de Animais
COMT: catecol-O-metiltransferase
CNPq: Conselho Nacional de Pesquisa
CTOP: antagonista do receptor opióide µ
DAINES: Drogas anti-inflamatórias não-esteroidas
DEAE – Sephacel: permutador iônico
DTM: Disfunção temporomandibular
DBCA: Diretriz Brasileira para o Cuidado e a Utilização de Animais Para Fins
Científicos E Didáticos
δ: Receptor opioide delta
ELISA: Enzyme-Linked Immunosorbent Assay
FITC: fluorescein isothiocyanate
FUNCAP: Fundação Cearense de Apoio ao Desenvolvimento Científico e
Tecnológico
g: Grama
GRK: Cinase do receptor acoplado à Proteína-G
H2SO4: Solução de ácido sulfúrico
HO-1: Hemeoxigenase-1
i.art.: Intra articular
IL-1β: Interleucina-1beta
INCT- IBSAB: Instituto de Biomedicina do Semi -Árido Brasileiro
i.t.: Intra tecal
i.v.: Intra venoso
ҡ: Receptor opioide kappa

13
LAFS: Laboratório de Farmacologia de Sobral
mg: Miligrama
mg/kg: Miligrama por quilo
µ: Receptor opioide mu
µg: Micrograma
µl: Microlitro
n: Número de animais
NaCl: Cloreto de Sódio
nm: Namômetro
TNF-α: Fator de necrose tumoral alfa
NT: Neuralgia do trigêmio
PGE2: Prostaglandina E2
pg/ml: picograma por mililitro
PZM21: Agonista seletivo do receptor opioide µ
p<0,05: Probabilidade de erro estatístico 5%
s: Segundos
SBCAL: Sociedade Brasileira de Ciência em Animais de Laboratório
s.c: Subcutânea
TJM: Temporomandibular Joint
º C: Grau Celsius
± EPM: Mais ou menos o erro padrão da média
5HTT: Recepor serotoninérgico
UFPB: Universidade Federal da Paraíba
Zy: Zymosam

14
SUMÁRIO
1 INTRODUÇÃO……………………………….……………………...……….……. 15
1.1 Dor Orofacial......…………………………….………….………………………… 15
1.2 Processo inflamatório na região da articulação temporomandibular... 17
1.3 Disfunção temporomandibular………………….………….……...…………. 18
1.4 Lectinas …………………………….………….……………............................... 21
1.5 Propriedades biológicas de lectinas ………....……………..….………..…. 23
2 JUSTIFICATIVA…………………………….………….……………...………….. 25
3 OBJETIVOS…………………………….………….….…………………………... 26
3.1 Objetivo Geral…………………………….………….….……………………...… 26
3.2 Objetivos Específicos…………………………….………………….....……… 26
4 CAPÍTULO 1: LECTIN FROM ABELMOSCHUS ESCULENTUS
REDUCES RAT TEMPOROMANDIBULAR JOINT INFLAMMATORY
HYPERNOCICEPTION DEPENDENT FROM CENTRAL OPIOID
RECEPTORS…...............................................................................................
27
REFERÊNCIAS…………………………….………….….……………………..… 51
APÊNDICE: Graphical Abstract Exigido pelo Periódico Journal of
Ethnopharmacology…………………………………………………………..….
58
ANEXO A: Declaração de Aceite do Comitê de Ética…………………….... 59
ANEXO B: Normas da Revista Journal of Ethnopharmacology………..... 60

15
1 INTRODUÇÃO
1.1 Dor orofacial
A dor exerce papel fisiológico importante nos organimos no sentido de
alertar os sistemas biológicos para possíveis danos, o que torna a capacidade de
sentir dor um importante mecanismo de sobrevivência (SBED, 2010), e de
acorodo com a Associação Internacional para o Estudo da Dor (IASP, 2008) é
compreendida como uma experiência sensorial e emocional desagradável,
associada a um dano tecidual real ou potencial, ou ainda descrita nesses termos.
Os componentes da dor diferem da nocicepção, uma vez que a percepção
da dor envolve diversos fatores como estímulo dos nociceptores primários,
percepção emocional e cognitiva (componente subjetivo da dor) (Julius; Basbaum,
2001). Em contrapartida, a nocicepção (do latim nocere: nocivo; capere: captar,
receber) pode ser definida como a captação do nocivo, envolvendo apenas os
mecanismos de transmissão desse estímulo ao sistema nervoso central (SNC)
(Oliveira, 2001). Dessa forma, o termo dor deve ser aplicado aos estudos
envolvendo humanos, por possuírem a capacidade de identificar seu caráter
subjetivo, e nocicepção quando as pesquisas utilizarem animais, por estes serem
desprovidos da capacidade de captar o estímulo emocional da dor.
A dor orofacial tem se revelado como um grande problema de saúde
pública nas últimas décadas, comprometendo a funcionalidade articular e a
qualidade de vida dos indivíduos atingidos (Okeson, 1998; Hargreaves, 2011;
Monteiro et al., 2011). Adicionalmente, estudos tem demonstrado que os
processos dolorosos representam um custo financeiro elevado por conta do
grande número de horas disperdissadas durante o processo produtivo
(Macfarlane, 2002). Ademais, apesar de acometer indivíduos jovens, pesquisas
têm revelado que a dor orofacial possui alto grau de prevalência na população
mundial como um todo (Hargreaves, 2011). Obermann (2010) afirma que pelo
menos 10% da população adulta é acometida por dor orofacial, e que esse índice
aumenta em idosos em mais de 50%, com tendência de as mulheres serem mais
propensas às formas crônicas de dor orofacial, incluindo neuralgia do trigêmio e
as disfunções temporomandibulares (DTM).
Região comumente referida como dolorosa, a face abriga a mandíbula,
único osso móvel dessa região, que interage através de duas articulações

16
temporomandibulares (ATM) reconhecidas como articulações especializadas que
realizam diversos tipos de movimentos a fim de cumprir suas funções fisiológicas.
Além disso, fazem parte do sistema estomatognático a ATM, os músculos faciais,
dentes, língua, glândulas, nervos, dentre outras estruturas (Okeson, 2008;
Barretto et al., 2013) que juntas permitem o desempenho harmônico de funções
como a respiração, mastigação, deglutição e fala. Estas estruturas estão sujeitas
a variações de pH (potencial de hidrogênio), temperatura, concentrações
moleculares e estímulos mecânicos que podem levar a lesões e inflamação,
provocando dor (Kitsoulis et al., 2011; Rando; Waldron, 2012; SBED, 2013).
Nesse contexto, a dor orofacial pode ser compreendida como qualquer dor
associada aos tecidos não mineralizados/moles (pele, vasos sanguineos,
glandulas ou musculos) e mineralizados (ossos e dentes) da cavidade oral e face,
estando normalmente relacionada aos eventos dolorosos que atingem a cabeça
e/ou região do pescoço, ou ainda à cervicalgia, odinofagia, cefaleias primárias e
doenças reumáticas tais como fibromialgia e artrite reumatoide (Leeuw, 2010).
Porreca et al. (2002) e Verri-Junior et al. (2006) relatam em seus estudos
que a dor, comum em diversas desordens clínicas, incluindo as que acometem a
região orofacial, se apresenta como um dos sinais clássicos da inflamação, sendo
iniciada pela sensibilização dos nociceptores aferentes primários. Assim, a
capacidade de reconhecer os possíveis agentes lesivos habilita a liberação de
mediadores da resposta inflamatória através do sistema imune (Robbins; Cotran,
2005). A percepção dolorosa da região orofacial está diretamente ligada ao
estímulo polongado de nociceptores periféricos (Reyes; Uyanik, 2014) que, por
sua vez, transmitem a informação nociva ao sistema nervoso central (SNC) e aos
centros superiores do tronco encefálico, comunicando-se com o complexo
trigeminal do tronco encefálico (tálamo e córtex somatosensorial) (Sessle, 2000).
Este possui, em sua maioria, os corpos celulares dos neurônios sensoriais
localizados no gânglio trigeminal, que mante´m de forma geral relação estreita
com o sistema límbico, responsável pelo processamento subjetivo da dor
(Matthews; Sessle, 2002).
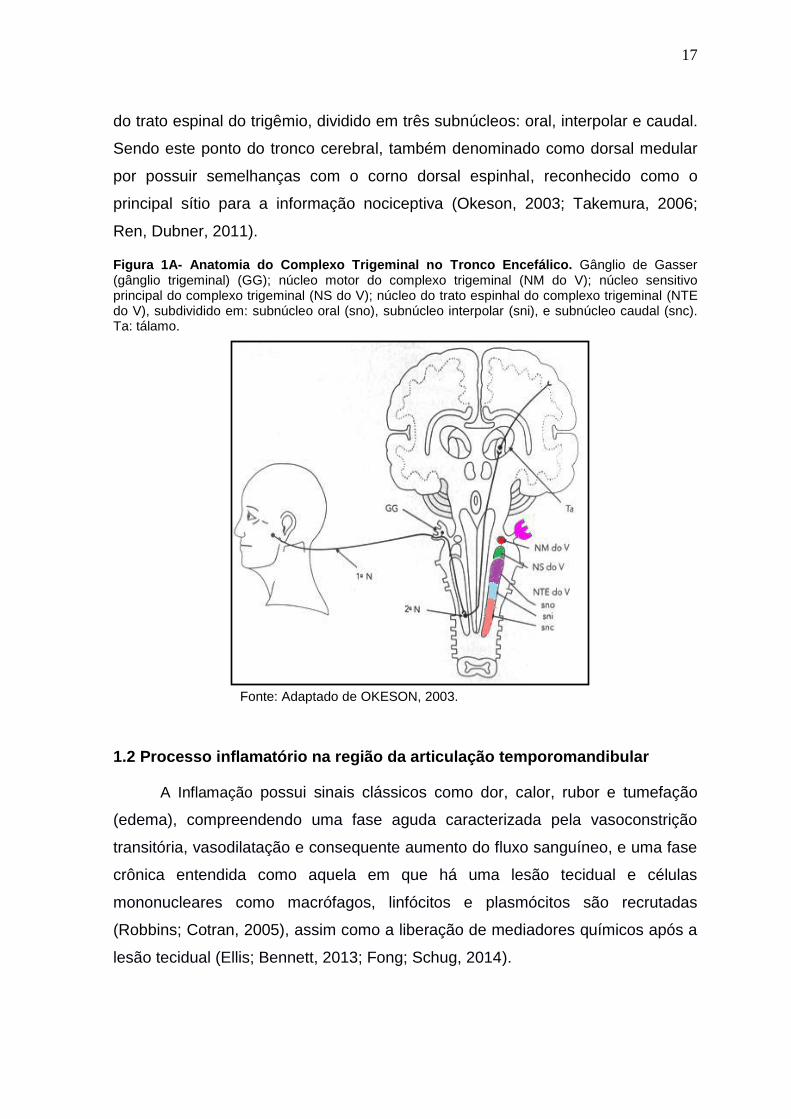
É importante destacar que o complexo trigeminal (Figura 1A) compreende
o núcleo sensorial principal, responsável pela transmissão das sensações de
propriocecpção e tato; o núcleo motor, envolvido nas respostas motoras, e núcleo
17
do trato espinal do trigêmio, dividido em três subnúcleos: oral, interpolar e caudal.
Sendo este ponto do tronco cerebral, também denominado como dorsal medular
por possuir semelhanças com o corno dorsal espinhal, reconhecido como o
principal sítio para a informação nociceptiva (Okeson, 2003; Takemura, 2006;
Ren, Dubner, 2011).
Figura 1A- Anatomia do Complexo Trigeminal no Tronco Encefálico. Gânglio de Gasser (gânglio trigeminal) (GG); núcleo motor do complexo trigeminal (NM do V); núcleo sensitivo principal do complexo trigeminal (NS do V); núcleo do trato espinhal do complexo trigeminal (NTE do V), subdividido em: subnúcleo oral (sno), subnúcleo interpolar (sni), e subnúcleo caudal (snc). Ta: tálamo.
Fonte: Adaptado de OKESON, 2003.
1.2 Processo inflamatório na região da articulação temporomandibular
A Inflamação possui sinais clássicos como dor, calor, rubor e tumefação
(edema), compreendendo uma fase aguda caracterizada pela vasoconstrição
transitória, vasodilatação e consequente aumento do fluxo sanguíneo, e uma fase
crônica entendida como aquela em que há uma lesão tecidual e células
mononucleares como macrófagos, linfócitos e plasmócitos são recrutadas
(Robbins; Cotran, 2005), assim como a liberação de mediadores químicos após a
lesão tecidual (Ellis; Bennett, 2013; Fong; Schug, 2014).
18
Durante a resposta inflamatória mediadores lipídicos (prostaglandinas),
protéicos (citocinas), histamina, óxido nítrico, bradicinina e neuropeptídios são
responsáveis pela manutenção e amplificação do processo inflamatório.
Delineamentos de pesquisa envolvendo animais para a investigação do processo
inflamatório articular apontam os neutrófilos como sendo os primeiros a migrarem
para a artiulação afetada, além disso, a inflamação estimula a liberação de
mediadores pró-inflamatórios denominados citocinas, como as interleucinas IL-1β,
IL-6 e IL-8 e o fator de necrose tumoral alfa (TNF-α) (Venkatesha et al., 2011),
promovendo, dessa forma, a degradação da ATM (cartilagem articular, membrana
sinovial e parte óssea). Tais superfícies danificadas podem acarretar em dor,
inflamação e limitação da mobilidade local (Kostrzewa-Janicka et al., 2012).
Além disso, o TNF-α, produzido principalmente por macrofagos, é apontado
em diversos estudos como uma importante citocina mediadora do processo
inflamatório crônico e agudo observado durante o desenvolvimento de doenças
articulares degenerativas (Kostrzewa-Janicka et al., 2012). Outro mediador
inflamatório identificado em níveis elevados na sinóvia da ATM de pessoas que
apresentam dor inflamatória é a serotonina (5-HTT), encontrada no SNC e em
todos os tecidos periféricos (Oliveira-Fusaro et al., 2012). Contudo, mediadores
químicos que compõem a inflamação podem ser estimulados por células gliais
satélite que permeiam corpos neuronais, funcionando como um efetores da
resposta inflamatória, o que evidencia que a inflamação não é somente resultado
de mecanismos periféricos, mas também centrais (Ellis; Bennett, 2013).
1.3 Disfunção temporomandibular
As disfunções temporomandibulares (DTM) englobam um grupo de
condições musculoesqueléticas e neuromusculares envolvendo a ATM, os
músculos mastigatórios e todos os tecidos associados (Greene, 2010). Quanto
aos fatores etiológicos, hábitos parafuncionais podem desencadear DTM, como
bruxismo, onicofagia, ou mastigação não-funcional, assim como hábitos
ocupacionais, frouxidão ligamentar, traumatismos, iatrogenia (intubação) e
disfunção hormonal também fazem parte dos fatores predisponentes para as DTM
(Milam et al., 1987; Scrivani et al., 2008; Sharma et al., 2011; De Rossi et al.,

19
2014). As DTM são classificadas em seis grandes grupos, e estes se ramificam
em outras disfunções, que podem ser observadas no Quadro 1.
Quadro 1: Classificação das Dinfunções Temporomandibulares
Disfunções Temporomandibulares
* Disfunções Articulares
* Dor articular - Artralgia - Artrite
* Disfunçoes articulares
- do complexo côndilo-disco - de hipomo-bilidade e hipermobilidade
* Doenças articulares
- Condilose - Osteocondrose dissecante - Osteonecrose - Condromatose sinovial - Articulares degenerativas
- Osteoartrite - Osteoartrose
* Disfunções congênitas ou de desenvolvimento
- artrite sistêmica - neoplasia
* Fraturas
Fonte: Adaptado de Leeuw; Klasser (2013).
Em um estudo realizado com 578 adolescentes chineses, a fim de
investigar a prevalência de sintomas de DTM e sua relação com a qualidade do
sono e distúrbios psíquicos, indicou que 61,4% da população estudada
apresentou pelo menos um sintoma de DTM, e que 1/3 dos indivíduos
experimentaram alteração do sono (não-reparador), depressão e estresse, e
ainda que 65,2% sofriam de ansiedade, dando robustez aos estudos que afirmam
a íntima relação entre distúrbios do sono e sofrimento de ordem psíquica com as
DTM (Lei et al., 2016). Sabe-se que condições dolorosas relacionadas à região
orofacial (principalmente a dor crônica) refletem negativamente na qualidade de
vida dos indivíduos afetados, gerando consequências graves como incapacidade
funcional e para o trabalho, prejuízos de ordem social, econômica e afetiva
(SBED, 2012; Greene, 2010).
Preditores sociodemográficos da incidência de DTM foram analisados em
um estudo de coorte prospectivo realizado com a população adulta dos Estados
Unidos (2.737 pessoas), sendo avaliados clinicamente os pacientes que relataram
sintomas. Foi constatado que 3,9% dos participantes desenvolveram DTM, e que

20
persistiram em 61% dos brancos contra 35% dos afro-americanos. Essas
variações podem estar relacionadas ao viés de incidência-prevalência, viés de
seleção que pode ocorrer em desenhos de pesquisas transversais (Slade et al.,
2016). Apesar das divergências encontradas na literatura acerca da prevalência
de DTM, com variações que giram em torno de 5-6% a 12% (De Rossi et al.,
2014), a dor associada à DTM foi relatada em 9-13% da população em geral (com
relação homem:mulher de 2:1), entretanto apenas 4-7% buscam tratamento (4
vezes mais mulheres). Já investigações realizadas por Steven; Kraus (2014) com
um grupo de 511 pessoas (8 hispânicos, 63 afro-americanos, 401 brancos e 39 de
outras etnias) que apresentavam quadro de DTM, com média de idade de 43,9
anos (44,9 entre as mulheres e 43,7 entre os homens), a proporção
homem:mulher foi de 5:1. Ademais, os sinais e sintomas atingem seu pico entre
20-40 anos de idade (Manfredini et al., 2011).
A DTM, portanto, é uma doença complexa que resulta da interação de
causas de domínios genéticos e ambientais (estresse, má qualidade no sono,
tabagismo, hábitos parafuncionais, doenças sistêmicas e etc.) (Slade et al., 2016).
No âmbito genético, pesquisas clínicas realizadas com genes da COMT (catecol-
O-metiltransferase), b2-AR (adrenoreceptor β2) e 5HTT (receptor serotoninérgico)
indicam que polimorfismos são relacionados com o processamento da dor e risco
de desenvolvimento de DTM (Maixner et al., 2011). Adicionalmente, estudos
realizados por Slade et al., 2015 e Slade et. al., 2016 demonstraram que a COMT,
participante da regulação do catabolismo de neurotransmissores de catecol,
possui papel importante na modificação da resposta ao estresse psicológico sobre
a dor, sendo aumentado em pessoas com DTM.
Os mecanismos periféricos envolvidos na dor relacionada às DTM
envolvem estimulação química e mecânica de nociceptores, liberação aumentada
de neuropeptídeos e mediadores inflamatórios como o óxido nítrico (NO),
citocinas, histamina, bradicinina, serotonina (5-hidroxitriptamina), adenosina
trifosfato (ATP), substância p, e eicosanoides, que por sua vez, possuem papel
relevante na artrite da ATM (Cairns, 2010; Chaves et al., 2011; Fusaro et al.,
2010). Já a via central da dor envolve células gliais (microglia e astrocitos),
neurônios nociceptivos do sistema trigeminal e vias aferentes que parecem estar

21
envolvidas na patogenia aguda e crônica de dor orofacial (Chiang et al., 2011;
Chiang et al., 2012).
O caráter multifatorial da DTM dificulta não só o diagnóstico como também
o seu tratamento. Neste sentido, intervenções terapêuticas farmacológicas, com
drogas anti-inflamatórias não-esteroidas (DAINES) tem sido a abordagem, muitas
vezes, de primeira escolha, para o alívio das dores e demais sintomas
associados. Contudo, o tratamento deve priorizar intervenções conservadoras
diante de quadros não-cirúrgicos e que não apresentem degeneração das partes
moles e nem óssea da ATM (Cairns, 2010). Outras modalidades terapêuticas
incluem placas oclusais, fisioterapia, exercícios madibulares, acupuntura,
laserterapia, toxina botulínica, dentre outros (Okeson, 2008; Fernandes et al.,
2009).
Nesse contexto, tem-se revelado promissora a pesquisa com recursos
naturais (como lectinas e polissacarídeos) na descoberta de ferramentas
farmacológicas que possam ser utilizadas para testes de novas substâncias a fim
de reduzir os efeitos pró-inflamatórios das DTM (do Val et al., 2014; Rivanor et al.,
2014; Rodrigues et al., 2014; Freitas et al., 2016).
1.4 Lectinas
A capacidade de se combinar específica e reversivelmente com várias
substâncias é uma característica da maioria das proteínas. Enzimas que se ligam
a seus substratos e inibidores ou anticorpos que se ligam ao antígeno, são
exemplos bem conhecidos (Sharon; Lis, 1989). Lectinas, entretanto, são
proteínas definidas inicialmente como moléculas que se ligam reversivelmente a
carboidratos, aglutinam células e/ou precipitam polissacarídeos e glicoproteínas.
A primeira definição de lectinas foi proposta por Boyd; Shapleigh (1954) que
utilizaram o termo “lectina”, oriundo da palavra latina legere, que significa
selecionar ou escolher, para definir uma classe de aglutininas de plantas
superiores, algumas das quais mostraram especificidade para grupos sangüíneos
humanos.

22
Goldstein et al. (1980) propuseram uma nova definição de lectinas, na qual
estas eram descritas como “proteinas de origem não imune, que se ligam a
carboidratos ou glicoproteínas, aglutinam células e/ou precipitam
glicoconjugados” definição modificada posteriormente por Kocourek; Horejsi
(1981), que sugeriram que lectinas “são proteinas ou glicoproteinas de natureza
não imune que se ligam a carboidratos, sem apresentar atividade enzimática
frente a esses açúcares e não requerem grupos hidroxilas livres para sua
ligação”.
Atualmente, a definição mais aceita para lectinas é a proposta por
Peumans; Van Damme (1995), que definem lectinas como proteínas de origem
não imune contendo pelo menos um domínio não-catalítico capaz de ligar-se
reversivelmente a mono ou oligossacarídeos específicos. Fundamentados no
conhecimento da estrutura das lectinas, Peumans; Van Damme (1995)
classificaram as lectinas em três grupos: merolectinas, hololectinas e
quimerolectinas. As merolectinas possuem um único sítio de ligação a
carboidratos sendo desprovidas de atividade hemaglutinante. As hololectinas são
semelhantes as merolectinas, entretanto, possuem dois ou mais sítios de ligação
a carboidratos podendo, desta forma aglutinar células ou precipitar
glicoconjugados. As quimerolectinas se diferenciam das duas outras classes por
possuírem além do sítio de ligação a carboidratos, um outro domínio não
relacionado que apresenta atividade biológica distinta e independente, podendo
ou não apresentar atividade hemaglutinante, dependendo do número de sítios de
ligação a açúcares.
As sequências de aminoácidos de uma grande quantidade de lectinas já
foram estabelecidas, e em geral as estruturas terciárias e quaternárias
encontradas são extremamente variáveis (Sharon; Lis, 2007), e podem ser
inativadas ou desnaturadas por processos como aumento de temperatura, pH
alterado (em relação ao seu pH ótimo) e tratamento com enzimas proteolíticas
tais como papaína ou tripsina (Gorakshakar; Ghosh, 2016).
A capacidade de reconhecimento entre proteinas e hidratos de carbono se
mostra fundamental em diversos processos biologicos como infecções virais,
bacterianas, a micoplasma e a parasitas e, ainda, na marcação de células e
componentes soluveis, fertilização, metástases cancerigenas e no crescimento e

23
ron, diferenciação celular (Pneumans; Van Damme, 1995; Beuth et al., 1995;
Sharon; Lis, 2004).
As Lectinas são empregadas em estudos diversos, sobretudo nos em que
há a necessidade de detectar, identificar e avaliar a funcionalidade de
carboidratos. Além disso, as lectinas podem ser utilizadas como ferramentas
para detecção antigenos nas células com base na sua estrutura superficial, e
suas interações com células e substâncias solúveis podem ser revertidas por
açúcares simples, sendo essa interação comumente utilizada como indicativo da
existência de hidratos de carbono (Sharon; Lis, 2007; Gorakshakar; Ghosh,
2016).
1.5 Propriedades biológicas de lectinas
Nas últimas décadas, pesquisadores têm voltado sua atenção à utilização
de moléculas de origem vegetal - proteínas e metabólitos secundários - na
perspectiva de avaliar a eficácia e segurança como agentes farmacológicos
(Cairns, 2010). A utilização de lectinas e polissacarídeos isolados de algas
marinhas no tratamento das condições inflamatórias das DTM já foi demonstrada
em estudos pré-clínicos (do Val et al.,Rivanor et al., 2014; Rodrigues et. al.,
2014). Ademais, atividade inflamatória, anti-inflamatória, anti-hipernociceptiva
(Alencar et al., 2007; Assreuy et al., 2009; Rangel et al., 2011; Figueiredo et al.,
2009), e ausência de citoxicidade aguda e crônica na utilização de lectinas
(Sabitha et al., 2011; Kumar et al., 2009) foram constatadas.
Diversas pesquisas têm descrito as atividades biológicas das lectinas,
aumentando o interesse e demonstrando segurança na utilização dessas
proteínas para fins terapêuticos como, por exemplo, na modulação da ligação de
insulina ao receptor de fator de crescimento 1, na síntese de óxido nítrico e até
mesmo na inibição do sistema nervoso central, através do mecanismo
dependente de GABA (Gadelha et al., 2005; Maniskosa et al., 2008; Vasconcelos
et al., 2009). Napimoga et al. (2007) em seus estudos apontaram a diminuição da
migração de leucócitos e da hipernocicepção mecânica por inibição na produção
de citocinas e quimiocinas. Em modelo de edema de pata induzido por

24
carragenina, também foi observada atividade anti-inflamatória de lectinas (Soares
et al., 2012).
Nesse contexto, destaca-se o potencial biológico da lectina de sementes de
Abelmoschus esculentus (AEL), planta originária da África, popularmente
conhecida como quiabeiro, e considerada de alto valor nutritivo (rico em cálcio,
vitaminas A, C e B1) (Panero et al., 2009). A AEL tem sido empregada no
controle glicêmico em pessoas com diabetes mellitus, além de inibir a absorção
de colesterol e reduzir o nível de lipídios e ácidos graxos no sangue (Khosrozadeh
et al., 2016), além de possuir efeito protetor gástrico e antioxidante (Ribeiro et al.,
2016). Adicionalmente, estudos envolvendo a AEL no tratamento da DTM tem
revelado seu potencial como agente anti-inflamatórios (Chaves et al., 2011;
Freitas et al., 2016).

25
2 JUSTIFICATIVA
É inegável que inúmeras conquistas ocorreram no âmbito da saúde bucal,
porém um número muito grande de pessoas sofrem com dor orofacial, e as DTM
estão entre as condições de maior queixa clínica (SBED, 2012). Uma abordagem
terapêutica eficaz pode fazer diferença no tratamento de sintomas como dor
crônica e incapacitante, contudo, o caráter multifatorial que envolve as DTM
dificulta essa escolha.
Portanto, esse cenário de alta prevalência, incidência e dificuldades na
identificação e tratamento que envolvem as DTM têm encorajado a comunidade
científica para o estudo de novas alternativas terapêuticas para o alívio de tais
condições através da utilização de recursos naturais como a AEL, dentre outras
(do Val et al., 2014; Rivanor et al., 2014; Rodrigues et al., 2014; Freitas et al.,
2016). O único registro de estudos utilizando a AEL em modelos de indução de
artrite na ATM de ratos por agentes pro-inflamatórios como zymosam foi
desenvolvido por nosso grupo de pesquisa, trazendo evidências da eficácia dessa
lectina na redução de eventos inflamatórios. Contudo, ainda não foi estudado o
papel anti-inflamatório e antinociceptivo da AEL produzidos na via central da dor
orofacial, tornando importante tal investigação. Ademais, o uso de substâncias
naturais pode se configurar como única forma de tratamento das DTM em muitas
comunidades em todo o mundo.

26
3 OBJETIVOS
3.1 Objetivo Geral
Avaliar o uso da AEL como alternativa terapêutica para DTM verificando
sua ação antinociceptiva, anti-inflamatória e sobre receptores opioides em modelo
animal.
3.2 Objetivos Específicos
- Investigar o efeito antinociceptivo e anti-inflamatório promovido pela lectina de
Abelmoschus esculentus no modelo de hipernocicepção induzida por formalina na
ATM de ratos;
- Estudar o papel dos receptores opioides em seu mecanismos de ação no
modelo hipernocicepção inflamatória induzida pela formalina na ATM de ratos;
- Averiguar o envolvimento dos receptores opioides na resposta antinociceptiva
promovido pela lectina de Abelmoschus esculentus no modelo hipernocicepção
inflamatória induzida pela formalina na ATM de ratos.

27
4 CAPÍTULO 1: LECTIN FROM ABELMOSCHUS ESCULENTUS REDUCES
RAT TEMPOROMANDIBULAR JOINT INFLAMMATORY HYPERNOCICEPTION
DEPENDENT FROM CENTRAL OPIOID RECEPTORS
Shirley Moreira Alves1, Raul Sousa Freitas2, Danielle Rocha do Val3, Lorena
Vasconcelos Vieira4, Ellen Lima de Assis4, Carlos Alberto de Almeida Gadelha5,
Tatiane Santi Gadelha5, José Thalles Jocelino Gomes de Lacerda5, Juliana
Trindade Clemente-Napimoga6, Vicente de Paulo Teixeira Pinto7, Mirna Marques
Bezerra1,7 and Hellíada Vasconcelos Chaves1,7.
1Master of Healthy Sciences Degree Program, Federal University of Ceará,
Avenida Comandante Maurocélio Rocha Pontes, 100 Derby - CEP: 62.042-280
Sobral, Ceará, Brazil. [email protected]
2Department of Morphology Federal University of Ceará - UFC, Rua Delmiro de
Farias, s/n - Rodolfo Teófilo, CEP: 60.430-170, Fortaleza, Ceará, Brazil.
3Northeast Biotechnology Network (Renorbio), Federal University of Pernambuco -
UFPE, Avenida Prof. Moraes Rego, 1235 Cidade Universitária CEP: 50670-901,
Recife, Pernambuco, Brazil. [email protected]
4Faculty of Dentistry, Federal University of Ceará - UFC, Avenida Comandante
Maurocélio Rocha Pontes, 100 Derby - CEP: 62.042-280 Sobral, Ceará, Brazil.
[email protected]; [email protected]
5Department of Molecular Biology, Federal University of Paraíba - UFPB, Cidade
Universitária, CEP: 58059-900 João Pessoa, Paraíba, Brazil.
[email protected]; [email protected];
6Faculty of Dentistry, University of Campinas - UNICAMP, Avenida Limeira, 901,
Vila Rezende,CEP 13414-903, Piracicaba, São Paulo, Brazil.
7Faculty of Medicine, Federal University of Ceará - UFC, Avenida Comandante
Maurocélio Rocha Pontes, 100 -Derby - CEP: 62.042-280 Sobral, Ceará, Brazil.

28
*Corresponding author:
Profa. Dra. Hellíada V. Chaves
Faculty of Dentistry of Sobral - Federal University of Ceará
Avenida Comandante Maurocélio Rocha Pontes, 100
Derby - CEP: 62.042-280
Phone: 55 88-3611-2202 - Fax: 55 88-3611- 8000
Sobral - Ceará - Brazil
E-mail: [email protected]
Conflicts of Interest: The authors declare that there is no conflict of interests
regarding the publication of this paper.
Abstract:
Ethnopharmacological relevance: Abelmoschus esculentus is largely cultivated
in Northeastern Brazil for medicinal purposes, like in cases of pneumonia,
bronchitis, pulmonary tuberculosis and inflammation. Aim of the study: To
evaluate the Abelmoschus esculentus (AEL) in reducing formalin-induced
temporomandibular joint inflammatory hypernociception in rats. Materials and
Methods: The behavioral experiments (CEUA nº 02\15) were performed on male
Wistar rats (180–240 g). Rats were pre-treated (i.v.) with AEL (0.001, 0.01 or 0.1
mg/kg) thirty minutes before 1.5% formalin injection in the TMJ. Further, to analyze
the possible effect of opioid pathways on AEL efficacy, animals were pre-treated
via intrathecal injection of naloxone or CTOP (the antagonist of Mu (µ) opioid
receptor), naltrindole (antagonist of Delta (δ) opioid receptor) or Nor-
Binaltorphimine (antagonist of Kappa () opioid receptor) 15 minutes before AEL
followed by intra-TMJ injection of 1.5% formalin. Behavioral analysis were
perfomed, animals were monitored for a 45 min observation period to quantify the
nociceptive response. TMJ tissue, trigeminal ganglion and caudal subnucleus
collection was performed for TNF-α dosage (ELISA). In addition, vascular
permeability was evaluated by Evans Blue extravasation. Results: AEL
significantly reduced formalin-induced TMJ inflammatory hypernociception and
decreased Evans blue extravasation. It also decreased TNF-α levels in TMJ
tissue, trigeminal ganglion and caudal subnucleus. AEL antinociceptive effects,

29
however, were not observed in the presence of naltrindole or Nor-Binaltorphimine.
Conclusions: These findings suggest that AEL efficacy depends on TNF-α
inhibition and the activation of δ and opioid receptors.
Keywords: Abelmoschus esculentus; temporomandibular joint, TNFα,
hypernociception, lectin
1. Introduction
Temporomandibular joint (TMJ) arthritis presents as one of the differential
diagnoses in temporomandibular disorders (TMD), which, in turn, encompasses a
group of musculoskeletal and neuromuscular conditions involving the TMJ,
masticatory muscles and all associated tissues. TMDs are often associated to
acute or persistent pain, and the patients may suffer from other painful disorders.
Chronic forms of TMD may lead to withdrawal or disability at work or to social
activities, resulting to a impairment in the quality of life (Greene, 2010).
A study evaluating the prevalence of TMD symptoms and its relation to
sleep quality and psychic disorders, has shown that 61.4% of the studied
population showed less than one TMD symptom, and that 1/3 of the subjects
experienced altered sleep, depression and stress, and 65.2% had anxiety (Lei et
al., 2016). Socio-demographic predictors indicate a 3.9% incidence of TMD per
year with moderate or disabling pain (Slade et al., 2013). Despite the divergences
found in the literature about the prevalence of TMD (variations between 5%-6%
and 12%) (De Rossi et al., 2014), the pain related to TMD was reported in 9-13%
of the general population on proportion man: woman of 2:1). In addition, signs and
symptoms peaked around 20-40 years old (Manfredini et al., 2011).
TMD is, therefore, a complex disease that results from an interaction of
causes of genetic and environmental domains (Slade et al., 2016). The
multifactorial nature of TMD hinders not only the diagnosis but also its treatment.
In this way, pharmacological therapeutic interventions with non-steroidal anti-
inflammatory drugs (NSAIDs) have been an approach, often the first choice, for
the relief of the pain and associated symptoms.

30
In the recent decades, researchers have been growing interest in
alternative therapies and use of natural products to assessing their efficiency and
safety (Cairns, 2010; Rivanor et al., 2014; Freitas et al., 2016) in order to develop
potential tools for new therapies to ameliorate inflammatory pain, which have
encouraged scientific studies to search for new substances with therapeutic action
and to confirm the efficacy of medicines derived from plants.
Due to the high prevalence, incidence and difficulties in identifying and
treating the inflammatory conditions related to TMD, our group has demonstrated,
through preclinical studies, the use of natural products in the treatment of
inflammatory conditions of TMDs, especially those derived from plants such as
Abelmoschus esculentus lectin (AEL) (Freitas et al., 2016) and Tephrosia toxicaria
(Do Val et al., 2014), as well as lectins and polysaccharides derivated from marine
algae (Rivanor et al., 2014; Rodrigues et al., 2014) Abelmoschus esculentus
(Malvaceae) (popularly called okra) is originated from Africa and has spread
across a number of tropic countries, including northeastern Brazil. This species is
considered of high nutritional value (rich source of calcium and vitamins A, C and
B1), easy cultivation (tropical regions, temperatures between 18 and 35 °C), and
its commercialization has been used for medicinal purposes (treatment of
pneumonia, bronchitis, pulmonary tuberculosis, still acting as a laxative, and
inflammation) (Castro et al., 2008; Panero et al., 2009).
Monte et al. (2014) showed selective anti-tumor effects on human breast
cancer cells, and Soares et al. (2012) showed anti-inflammatory, antinociceptive
and hemagglutinating AEL activities. To our knowledge, the only study which
demonstrates that AEL, a plant-derived lectin, is able to exert antinociceptive and
anti-inflammatory effects on the TMJ pain, especially in the rat TMJ arthritis
models was developed by our group, bringing evidence of the efficacy of this lectin
in the reduction of inflammatory events in TMDs (Freitas et al., 2016). However,
there is still no study about the anti-inflammatory and antinociceptive role played
by AEL on the central and peripheral pathways of orofacial pain. Therefore, the
present study aimed to investigate the unexplored anti-nociceptive and anti-
inflammatory efficacy of AEL in the rat model of formalin-induced
temporomandibular joint inflammatory hypernociception. Additionally, we

31
investigated the role of opiod receptors and the putative involviment of TNF-α in
AEL efficacy.
2. MATERIALS AND METHODS
2.1. Animals
Male Wistar rats (160–220 g) (n=6) were housed in standard plastic cages
with food and water available ad libitum. They were maintained in a temperature
controlled room (23 ± 2 °C) with a 12/12- hour light-dark cycle. All experiments
were designed to minimise animal suffering and to use the minimum number of
animals required to achieve a valid statistical evaluation. The animal supplier for
this study was the Central Animal House of the Federal University of Ceará and
the experimental protocol was conducted in accordance with the Institutional
Animal Care and with the approval of the Ethics Committee of the Federal
University of Ceará, Fortaleza, Brazil (CEUA nº 02\15).
2.2. Source Material
A. esculentus seeds were collected in the municipality of Conde, Paraíba,
Brazil (geographical coordinates: S-7°17'629 "W-34°48'085") for botanical
identification. Professor Rita Balthazar de Lima (Department of Botany, Federal
University of Paraiba - UFPB, Brazil) identified species of the Malvaceae family to
which A. esculentus species belong. The specimen was deposited in the UFPB
herbarium under the identification number of 41,386. Lectin purification was
performed in BioGeR (Laboratory of Biochemical Genetics and Radiobiology).
2.3. Extraction of Lectin
Seeds were grounded to powder and its lipids removed with n-hexane. To
obtain the protein extract, the powder was placed in added in Tris-HCl buffer pH
7.4 with 0.1 M NaCl 0.15 M for 3 h and then centrifuged at 5.000 rpm at 4 °C for
20 min. The resulting precipitate was discarded, and the supernatant was
subjected to ammonium sulfate precipitation, obtaining a lectin fractionwithin the
range of 30–60% saturation. The lectin fraction was dialyzed exhaustively against
water, lyophilized, and then isolated by ion exchange chromatography on DEAE –
Sephacel (Ion exchanger) equilibrated with bibasic sodium phosphate 0.025 M pH

32
7.4. Lectin elution was prepared using the gradient of bibasic sodium phosphate
0.025 M and NaCl pH 7.4 1 M. Elution wasmonitored by spectrophotometer at a
wave length of 280 nm, being it dialyzed against water, frozen and lyophilized.
Furthermore, this lectin under study is endotoxin free which ultimately mean it
does not exert toxic effects on animals under investigation.
2.4. Efficacy of lectin from Abelmoschus esculentus on formalin-induced
temporomandibular joint inflammatory hypernociception in rats
2.4.1. TMJ injection
The animals were briefly anesthetized by inhalation of isoflurane and the
posteroinferior border of the zygomatic arch was palpated. Rats received an intra-
articular injection of 1.5% formalin (Roveroni et al., 2001). The needle was
inserted immediately inferior to this point and was advanced in an anterior
direction until reaching the posterolateral aspect of the condyle. TMJ injections
were performed via a 30-gauge needle introduced to the left TMJ at the moment of
the injection. A cannula consisting of a polyethylene tube was connected to the
needle and also to a 50 μL syringe (Hamilton, Reno, NV). Volume per injection
was 50 μL. Each animal regained consciousness approximately 30s after
discontinuing the anesthetic and was returned to the test chamber.
2.4.2. Experimental design
Thirty minutes before formalin injection rats were pre-treated (0.1 mL/100g
body weight) with AEL 0.001, 0.01 or 0.1 mg/kg) by intravenous (i.v.) injection or
0.9% sterile (sham group) fallowed by intra-TMJ injection of 1.5% formalin in a
final volume of 50 µl as above described. Immediately after the behavioral
analyzes, the animals were anesthetized and euthanized by decapitation, and the
periarticular tissues, trigeminal ganglion and caudal subnucleus were removed
and processed for biochemical analysis.
2.4.3. Behavioral tests for evaluation of nociceptive responses
Each animal was placed in a test chamber (30 X 30 X 30 cm mirrored-wood
chamber with a glass at the front side) for a 15-min habituation period to minimize
stress (Abbott et al., 1986). Each animal was used in only one experiment and

33
was sacrificed at the end of the experiment. Testing sessions took place during the
light phase (between 9:00 AM and 5:00 PM) in a quiet room maintained at 25 °C
and all animals were manipulated for 7 days before the experiment to be
habituated to the experimental manipulation. (Tjolsein, 1992). Each animal
immediately recovered from anesthesia after TMJ injection and was returned to
the test chamber for counting nociceptive responses during the following 45 min
observation period. The nociceptive response score was defined as the cumulative
total number of seconds that the animal spent rubbing the orofacial region
asymmetrically with the ipsilateral fore or hind paw plus the number of head
flinches counted during the observation period as described previously (Roveroni
et al., 2001). Results are expressed as the duration time of nociceptive behavior.
Rats did not have access to food or water during the test.
2.4.4. Collection of biological materials
2.4.4.1. TMJ tissue
The superficial tissues were dissected until reaching the left TMJ then the
TMJ soft tissues were collected. The samples were stored in a freezer -80º C.
2.4.4.2. Trigeminal ganglion
In order to access to the trigeminal ganglion, which is lodged at the base of
the skull in the trigeminal cavus region in the temporal bone, the skullcap and the
brain were removed, and the trigeminal ganglion was carefully identified and
collected. The samples were stored in a freezer -80 ºC.
2.4.4.3. Caudal subnucleus of the spinal tract of the trigeminal nerve
In order to have access to the caudal subnucleus, which is located in the
brainstem, the brain was removed, which was positioned in a specific matrix for
the neural structures of rats. The removal of the caudal subnucleus was performed
by cutting with a scalpel blade positioned 2 mm in the caudal direction to obex.
2.5. Evaluation of anti-inflammatory parameters
2.5.1. Evans blue extravasation measurement

34
In another sequence of experiments, AEL (0.01 mg/kg) was administered to
rats 30 min prior to formalin. Immediately after formalin injection (1.5% i.art) Evans
Blue dye 1% (5mg/kg, i.v.) was administered administered systemically to assess
plasma extravasation (Torres-Chavéz et al., 2012). After 45 minutes, the animals
were euthanized and the ATMs removed for analysis. Immediately after the
extraction, the periarticular tissue was weighed and placed in 1mL of formamide
overnight at 60 ºC (Fiorentino et al., 1999). The supernatant (100 μL) was
extracted, and the absorbance at 620 nm was determined in spectrophotometer.
The concentration was determined by comparison to a standard curve of known
amounts of Evans blue dye in the extraction solution, which was assessed within
the same assay. The amount of Evans blue dye (μg) was then calculated per mg
of exudates.
2.5.2. TMJ periarticular tissue, trigeminal ganglion and caudal subnucleus
TNF-α assay
TNF-α concentrations were determined in the TMJ periarticular tissue,
trigeminal ganglion and caudal subnucleus 45 min after formalin injection in rats
that received 0.01mg/kg AEL or vehicle (0.9% sterile saline). TMJ periarticular
tissue, trigeminal ganglion and caudal subnucleus were removed and stored at
−80 °C. The material was homogenized in a solution of RIPA Lysis Buffer System
(Santa Cruz Biotechnology, USA), and the supernatant was used to determine the
cytokine levels were quantified by the following kit: TNF-α–Rat TNF-
alpha/TNFSF1A Quantikine ELISA Kit (R&D Systems, catalog number RTA00) by
enzyme-linked immunosorbent assay (ELISA). All assays were carried out
according to the manufacturer's instructions. Briefly, microtiter plates were coated
overnight at room temperature (20–23 °C) with an antibody capture against rat
TNF-α (4.0 μg/mL). The plate was blocked by adding of Reagent Diluent to each
well, incubated at room temperature for a minimum of 1 h. After blocking the plate,
the samples and standard at various dilutions were added and incubated at room
temperature for 2 h. The plate was washed three times with buffer and of the
Detection Antibody, was added (100 μL/well). After further incubation at room
temperature for 2 h, the plate was washed and Streptavidin-HRP was added. The
colour reagent (H2O2 and Tetramethylbenzidine; 100 μL/well) was added 15 min

35
later and the plate was incubated in the dark at room temperature for 15–20 min.
The enzyme reaction was stopped with H2SO4 and absorbance was measured at
450 nm. TNF-α concentrations were expressed as pg/ml.
2.6. Evaluation of the involvement of the opioid pathway in the
antinociceptive AEL effect on formalin-induced temporomandibular joint
inflammatory hypernociception
2.6.1. Intrathecal drug administration
Rats were briefly anesthetized by the inhalation of isoflurane, and a small
area of the skin that covers a cervical region was trichotomized with an electric
appliance. The animals were positioned in the ventral decubitus position, in order
to the suboccipital space was easily found. A 30 gauge needle, connected to a 50
μL Hamilton syringe, by a polyethylene cannula, was used for the injection. First
the needle was inserted just below the occipital bone penetrating the skin over the
suboccipital space up to 4 mm deep and then to slightly inclined towards the
cranial. The needle was advanced plus 2 mm to puncture the atlanto-occipital
membrane and reach the bulbar subarachidoid space. This technique allows direct
administration of the drug in the cerebrospinal fluid in the proximity to the
trigeminal caudal subnucleus. The total volume of intrathecal injections was 10 μL
and administered in a rate of 1 μL/s, as previously standardized (Fischer et al.,
2009). Immediately after behavioral analysis, the animals were anesthetized and
euthanized by decapitation. The administered drugs were diluted in sterile saline
solution (0.9%).
2.6.2. Effect of the nonselective opioid receptor antagonist naloxone on AEL-
induced antinociception
Rats were pretreated (15 min) with an intrathecal injection of naloxone (Nlx;
15 µg/10 µl/intrathecal / n= 5; Eisenberg et al., 1996) followed by AEL (0.01
mg/kg/i.v.) 30 min prior 1.5 % formalin intra-TMJ injection (50 µl /TMJ). Behavioral
nociception response was evaluated for 45 min observation period. All animals
received a final volume of 50 µl of solutions into TMJ.

36
2.6.3. Effect of µ, δ and -opioid receptors on AEL-induced antinociception
Rats were divided in groups of five animals, and each group was pretreated (15 min) with
an intrathecal injection of a specific inhibitor of µ-opioid receptor CTOP (10 µg/10 µl
/intrathecal) the inhibitor of δ -opioid receptor Naltrindole (10 or 30 µg/10 µl/intrathecal)
or the selective -opioid receptor antagonist Nor-BNI (15 or 45 µg/10 µl/intrathecal);
followed by AEL (0.01 mg/kg /i.v.) 30 min prior 1.5% formalin intra-TMJ injection (50 µl
/TMJ). Behavioral nociception response was evaluated for 45 min period observation. All
animals received a final volume of 50 µl of solutions into TMJ (Picolo; Cury, 2004;
Clemente et al., 2004).
2.7. Statistical analysis
The data are presented in figures and text as the means±SEM. The number
(n) of animals per experimental group was at least 5. Differences between means
were compared using a one-way ANOVA followed by the Bonferroni test. A
probability level of less than 0.05 (P<0.05) was considered to indicate statistical
significance.
3. Results
3.1. AEL reduces formalin-induced temporomandibular joint inflammatory
hypernociception in rats
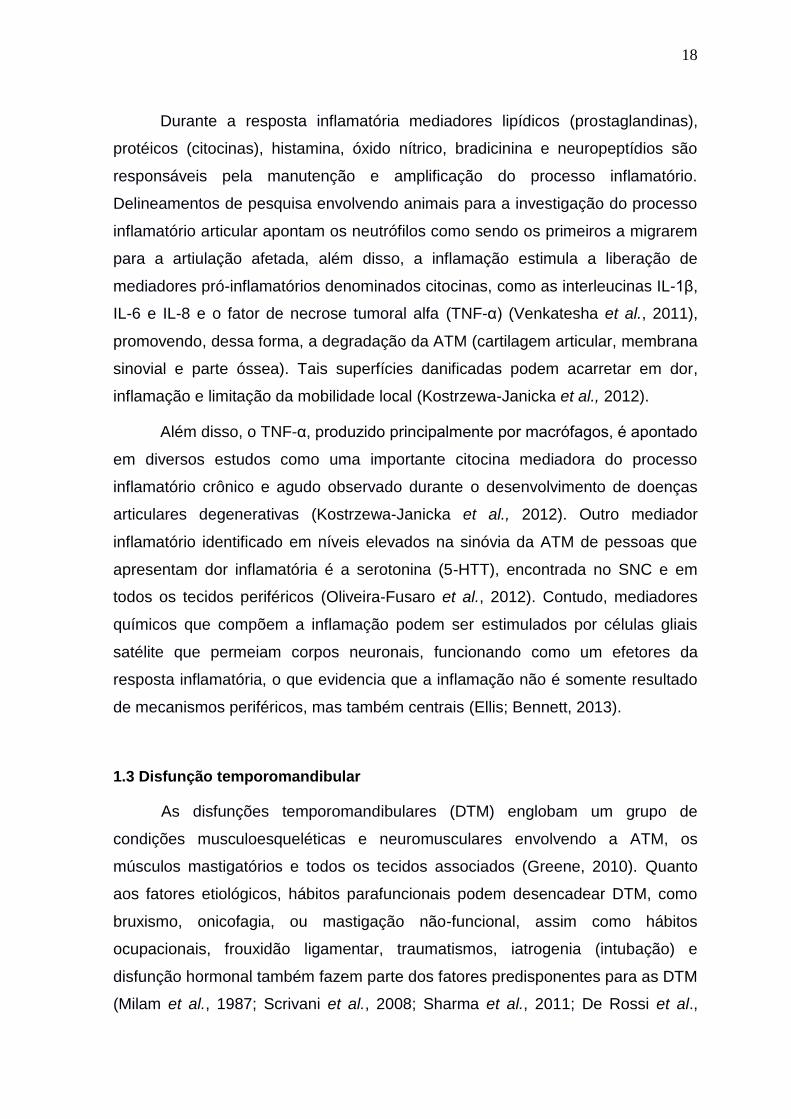
The formalin 1.5% injection (i.art.) resulted in a significant increase in the
behavioral nociceptive response compared to the saline group. Treatment with
AEL (0.001, 0.01 and 0.1 mg/kg; i.v.) significantly (p<0.05) reduced the behavioral
nociceptive response induced by the injection of formalin 1.5% into the TMJ when
compared to the formalin group (Fig. 1). Considering this result, the followed
experiments, in order to elucidate the mechanisms of action of this substance,
were performed using AEL 0.01 mg/kg.
37
Saline _ Mor 0.001 0.01 0.10
100
200
300
*
#
# #
Formalin 1.5% (50 L/art.)
AEL (mg/kg)
#
**
No
cice
pti
ve b
ehav
ior
(s)
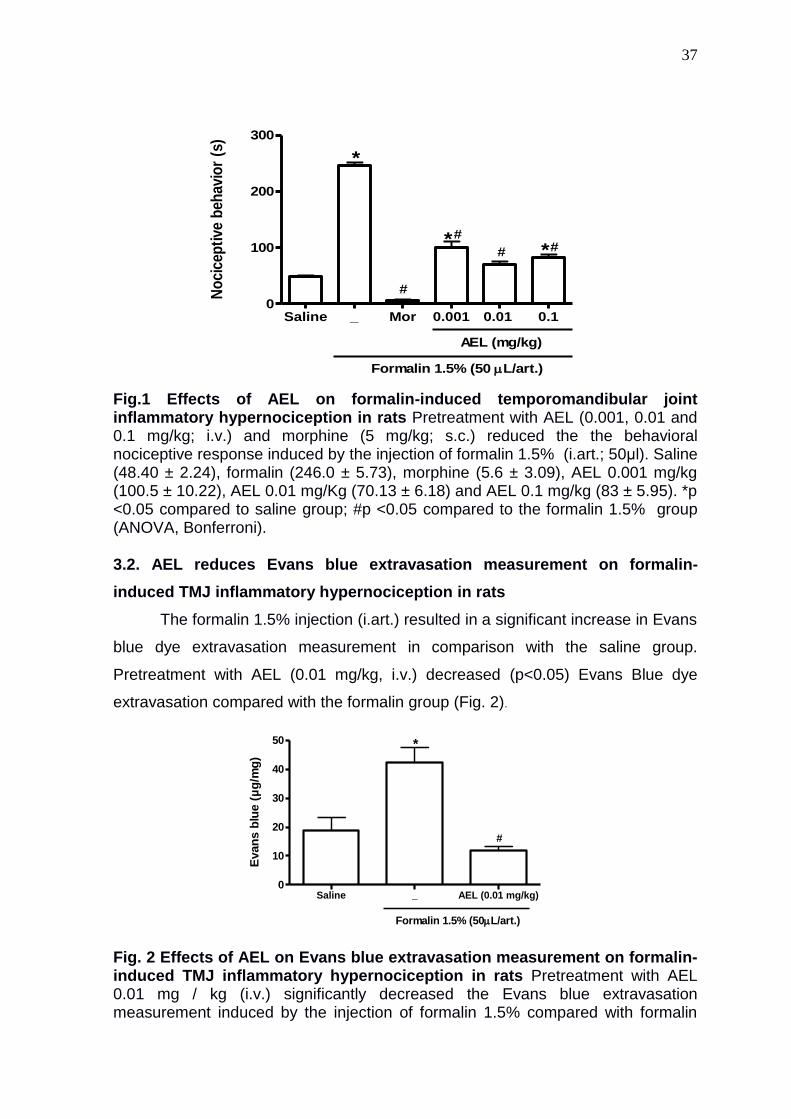
Fig.1 Effects of AEL on formalin-induced temporomandibular joint inflammatory hypernociception in rats Pretreatment with AEL (0.001, 0.01 and 0.1 mg/kg; i.v.) and morphine (5 mg/kg; s.c.) reduced the the behavioral nociceptive response induced by the injection of formalin 1.5% (i.art.; 50μl). Saline (48.40 ± 2.24), formalin (246.0 ± 5.73), morphine (5.6 ± 3.09), AEL 0.001 mg/kg (100.5 ± 10.22), AEL 0.01 mg/Kg (70.13 ± 6.18) and AEL 0.1 mg/kg (83 ± 5.95). *p <0.05 compared to saline group; #p <0.05 compared to the formalin 1.5% group (ANOVA, Bonferroni). 3.2. AEL reduces Evans blue extravasation measurement on formalin-
induced TMJ inflammatory hypernociception in rats
The formalin 1.5% injection (i.art.) resulted in a significant increase in Evans
blue dye extravasation measurement in comparison with the saline group.
Pretreatment with AEL (0.01 mg/kg, i.v.) decreased (p<0.05) Evans Blue dye
extravasation compared with the formalin group (Fig. 2).
Saline _ AEL (0.01 mg/kg)0
10
20
30
40
50
Formalin 1.5% (50L/art.)
*
#
Evan
s b
lue (
µg
/mg
)
Fig. 2 Effects of AEL on Evans blue extravasation measurement on formalin-induced TMJ inflammatory hypernociception in rats Pretreatment with AEL 0.01 mg / kg (i.v.) significantly decreased the Evans blue extravasation measurement induced by the injection of formalin 1.5% compared with formalin

38
group. Saline (18.88 ± 4, 29), formalin (42.33 ± 5.13) and AEL 0.01 mg/kg (12.01 ± 1.14). *p <0.05 compared to saline group; #p <0.05 compared to the formalin group 1.5% (ANOVA, Bonferroni). 3.3. AEL decreases TNF-α levels in TMJ tissue, trigeminal ganglion and caudal subnucleus on formalin-induced TMJ inflammatory hypernociception in rats The formalin 1.5% injection (i.art.) resulted in a significant increase in TNF-α
levels in TMJ tissue, trigeminal ganglion and caudal subnucleus compared with
saline group. AEL 0.01 mg/kg (i.v.) also reduced TNF-α in TMJ tissue, trigeminal
ganglion and caudal subnucleus in comparison with formalin group.
Fig. 3 Effects of AEL on TNF-α levels in the TMJ periarticular tissue (A), trigeminal ganglion (B) and caudal subnucleus (C) on formalin-induced TMJ inflammatory hypernociception Pretreatment with AEL (0.01 mg/kg, i.v.)
Saline _ AEL 0.01 mg/kg0
50
100
150
200
250
300
Formalin 1.5% (50L/art.)
*
#
A
TN
F-
(p
g/m
L T
MJ t
issu
e)
Saline _ AEL 0.01 mg/kg0
50
100
150
*
#
B
Formalin 1.5% (50L/art.)
TN
F-
(p
g/m
L t
rig
em
inal
gan
gli
on
)
Saline _ AEL 0.01 mg/kg
0
50
100
150
200
250
*
#
C
Formalin 1.5% (50L/art.)
TN
F-
(p
g/m
L c
au
dal
su
bn
ucle
us)

39
reduced levels of TNF-α in the TMJ tissue (Figure A), saline (61.29 ± 7.19), formalin (227.5 ± 15.5), and AEL 0.01 mg/Kg (131.8 ± 7.70); In the trigeminal ganglion (Figure B), saline (81 ± 4,16), formalin (113.8 ± 2.62), and AEL 0.01 mg/kg (84. 67 ± 0.88), and in the caudal subnucleus (Figure C), saline (97 ± 21.01), formalin (188.5 ± 27.18) and AEL 0.01 mg/kg (109.4 ± 10.51). * P <0.05 compared to saline group; #p <0.05 compared to the formalin group 1.5% (ANOVA, Bonferroni). 3.4 AEL inhibits formalin-induced temporomandibular joint inflammatory hypernociception through central opioids receptor activation In order to investigate whether the antinociceptive effect of AEL depends on
the central opioid activation, was tested the effect of the pretreatment with
naloxone, a non selective opioid receptor antagonist or the selective µ-opioid
receptor CTOP, δ-opioid receptor Naltrindole or the selective -opioid receptor
antagonist Nor-BNI 15 min before AEL treatment. The intrathecal administration of
naloxone (15 μl/10μl) significantly reversed (p <0.05) the antinociceptive effect of
AEL (0.01 mg/kg). This result suggests that the antinociceptive effect of AEL
depends on the central opioid receptors activation (Fig. 4A).
The Intrathecal administration of naltridole, a selective opioid receptor
antagonist delta (δ) (10 or 30 ug/10 uL), significantly reversed (p<0.05) the
antinociceptive effect of AEL (0.01 mg/kg). This result suggests that the
antinociceptive effect of AEL depends on the activation of the δ opioid receptor
(Figure 4B). The intrathecal administration of nor-binaltorfimine, a selective opioid
receptor antagonist kappa (ĸ) (15 or 45ug/10uL) 15 minutes prior AEL treatment
significantly abolishes (p<0.05) the antinociceptive effect of AEL 0.01 mg/Kg. This
fiding may suggests that the antinociceptive effect of AEL also depends on the
activation of the opioid receptor ĸ (Figure 4C). The intrathecal administration of
CTOP, a selective opioid receptor antagonist mu (μ) (10ug/10uL) 15 minutes
before intravenous injection of AEL does not reverse the antinociceptive effect of
AEL 0.01 mg/Kg what may suggests that the antinociceptive effect of AEL does
not depend on mu opioid receptor activation (μ) (Figure 4D).

40
Fig.4 Effect of the non selective (naloxone) and selective (μ, ĸ and δ) opioid receptor antagonists on the AEL antinociceptive efficacy on formalin-induced TMJ inflammatory hypernociception Naloxone (15ug/10uL/intrathecal) reversed the antinociceptive effect of AEL (0.01 mg/kg) (Figure A); Saline (48.4 ± 2.24), formalin (211.7 ± 7.82), morphine + naloxone (147.2 ± 4.60), AEL (0.01 mg/kg) (92.8 ± 15.66) and AEL (0.01 mg/kg) + naloxone (160 ± 8.51). Naltrindole (10 or 30ug/10uL) the delta (δ) opioid receptor antagonist reversed the antinociceptive effect of AEL (0.01 mg/kg) (Figure B); Saline (48.4 ± 2.24), formalin (211.7 ± 7.82), AEL (0.01 mg/kg) (82 ± 14.63), naltrindole 10 ug/10 uL + AEL (0.01 mg/Kg) (109.2 ± 5.59), naltrindole 30 ug/10 uL + AEL (0.01 mg/kg) (139.8 ± 7.34) and naltrindole 30 μg/10μl (203.8 ± 5,92). Nor-binaltorfimine (15 or 45μg/10μl) the opioid receptor antagonist kappa (ĸ) reversed the antinociceptive effect of AEL (0.01 mg/kg) (Figure C); Saline (47.57 ± 1.73), formalin (211.2 ± 8.36), AEL (0.01 mg/kg) (88.4 ± 8.88), nor-binaltorfimine 15μg/10μl + 1 mg/kg) (159.9 ± 12.34), nor-binaltorfimine 45μg/10μl + AEL (0.01 mg/kg) (174.5 ± 7.98) and nor-binaltorfimine (45μg/10μl) (235.2 ± 21.31). CTOP 10 (μg/10μl) the Opioid receptor antagonist mu (μ) did not reverse the antinociceptive effect of AEL (0.01 mg/kg) (Figure D); Saline (48.40 ± 2.24), formalin (165 ± 25.09), AEL (0.01 mg/kg) (71.4 ± 9.75), CTOP 10 μg/10μl + AEL (0.01 mg/Kg) (51.5 ± 14.82), CTOP 10μg/10μl (203.8 ± 5.92). * P <0.05 compared to saline group; #P <0.05 compared
Salina Nal Nal 0
100
200
300
Formalin 1.5% (50 L/art.)
*
#
+
AEL (0,01mg/kg)Morphine
#
&
A
No
cic
ep
tive b
eh
avio
r (s
)
Saline 10 30 300
100
200
300
AEL (0,01 mg/kg)
Naltrindole (µg/10 µL)
Formalin 1.5% (50 L/art.)
*
#
+
B
+
No
cic
ep
tive b
eh
avio
r (s
)
Salina 15 45 450
100
200
300
AEL (0,01 mg/kg)
Binaltorphirmine (µg/10 µL)
Formalin 1.5% (50 L/art.)
*
#
++
C
No
cic
ep
tive b
eh
avio
r (s
)
Saline 10 100
100
200
300
AEL (0,01 mg/kg)
CTOP (µg/10 µL)
Formalin 1.5% (50 L/art.)
*
#
D
No
cic
ep
tive b
eh
avio
r (s
)

41
to the formalin group 1.5%; P<0.05 compared to the morphine group and +P<0.05 compared to the AEL 0.01 mg/kg group (ANOVA, Bonferroni).
4. Discussion
We demonstrated the antinociceptive and anti-inflammatory effect of lectin
of Abelmoschus esculentus on formalin-induced temporomandibular joint
inflammatory hypernociception in rats and that its effects are mediated via central,
through opioid receptors activation. AEL effects depended in part on reduction of
inflammatory parameters, such as TNF-α levels, as there was a reduction of these
cytokines concentration in the TMJ tissue, trigeminal ganglion and caudal
subnucleus. Regarding inflammatory parameters, AEL administration also
decreased plasma extravasation in synovial exudates compared with formalin
group, being this parameter determined by Evans blue dye extravasation.
Alencar et al. (2007) demonstrated the effect of Vatairea macrocarpa lectin
on macrocytic activation and chemotaxis of inflammatory mediators. Assreuy et al.
(2009) demonstrated the relevance of vasodilation caused by diocletian lectin
(Canavalia genus) in the inflammatory process. The antinociceptive effect of
dioclenáceas lectins in the contortion model caused by acetic acid, in turn, was
demonstrated by Rangel et al. (2011). The Bolivian Canavalia lectin and its
antinociceptive effect, besides its toxicity, were studied by Figueiredo et al. (2009).
Additionally, our group demonstrated the anti-inflammatory and anti-nociceptive
effect of Caulerpa cupressóides lectin (CcL) on zymosam-induced TMJ arthritis in
rats (Rivanor et al., 2014). However, not only anti-inflammatory effects, are
demonstrated in plant lectins. Bauhinia bauhinioides and Dioclea wilsonii lectins
present proinflammatory effects by activation of proteolytic enzymes and induction
of neutrophil migration, respectively (Silva et al., 2011; Rangel et al., 2011).
The study of the properties of the lectin of Abelmoschus esculentus has
great relevance, since this species has been used to treat a variety of disorders,
such as microbial infection, hypoglycemia, constipation, urinary retention and
inflammation (Gürbüz et al., 2002; Kumar et al., 2009). Regarding the anti-
inflammatory effects, AEL was investigated in an experimental model of acute
inflammation, in which it showed an inhibitory effect on carrageenan-induced paw
edema but not on dextran-induced edema. This data suggests that the anti-

42
inflammatory effect of AEL occurs only in edema involving cell infiltrate, since
edema caused by carrageenin is due to intense neutrophil infiltration and it is
associated with the release of inflammatory mediators whereas dextran-induced
edema involves histamine, Serotonin and bradykinin (Masnikosa et al., 2008).
Similar results were found in other leguminous lectins (Assreuy et al., 2007).
Soares et al. 2012, in turn, demonstrated the anti-nociceptive effect of AEL, in the
same three doses tested in this work, on the model of the contortions induced by
acetic acid.
Recently, our group demonstrated the antinociceptive and anti-inflammatory
effect of AEL on zymosan-induced TMJ hypernociception in rats, we found
evidences that, at least in part, the antinociceptive and anti-inflammatory effects of
the AEL depend on the integrity of the HO-1 pathway, corroborating with other
works that show that the inhibition of the HO-1 pathway is associated with the
worsening of the inflammatory response (Freitas et al., 2016; Vicente et al., 2003).
The experimental use of formalin as a pro-inflammatory agent in rats, a
model used in this study, is considered quite representative of the pain clinically
observed in humans, and the similarity between clinical and experimental results
suggests that the formalin test in rat TMJ is an effective model for assessing the
mechanisms involved in TMD dysfunctions (Tjolsein et al., 1992; Roveroni et al.,
2001; Clemente et al., 2004). In addition to the nociceptive effects caused by
formalin, this substance also causes a local edema and plasma extravasation
induced directly and indirectly. Formalin promotes vascular effects by different
mechanisms that in common cause the stimulation of non-neuronal and neuronal
cells. In response to stimulation, both cells release inflammatory substances
causing intense edema and local plasma extravasation (Torres-Chávez et al.,
2012).
TNF-α, the cytokine investigated in this work, has a detrimental effect on
bone and cartilage (Gunson et al., 2012). In addition, a positive correlation was
found between cytokines in the synovial fluid and osteoarthritis. It has been
suggested that the presence of IL-1β and TNF-α in the synovial fluid of the TMJ
may affect the treatment outcome in patients with osteoarthritis (Hamada et al.,
2008). High TNF-α levels were found in symptomatic TMJs when compared to
normal joints (Shafer et al., 1994; Nordahl et al., 2000; Emshoff et al., 2000). The

43
anti-inflammatory effect of AEL was also observed by decreasing the plasma
extravasation and reducing of TNF-α levels in periarticular tissue, trigeminal
ganglion and caudal subnucleus.
We also demonstrated that the central antinociceptive response mediated
by AEL in the TMJ hypernociception results from the activation of the δ and
receptors, but not of μ opioid receptor. In addition, its anti-inflammatory effects
may also be related to opioid receptors. Nũnéz et al. (2007) provided the genetic,
proteomic and behavioral evidence for the involvement of peripheral opioid
receptors in relieving inflammatory pain from craniofacial muscle tissues and
suggested that all three subtypes of opioid receptors are involved in inflammatory
responses. Napimoga et al. (2007) demonstrated that the antinociceptive effects in
peripheral hypernociception of 15d-PGJ2, peroxisome proliferator-activated
endogenous protein (PPAR-ᵧ), recognized as a potent anti-inflammatory mediator,
promotes peripheral analgesia by endogenous opioid stimulation, suggesting that
this protein Can directly activate opioid receptors present in primary sensory
neurons. In addition, PPAR-ᵧ may stimulate the release of opioids that act to
control inflammatory pain by resident macrophages, supporting the understanding
that opioid receptors may be involved in the inflammatory response of orofacial
pain.
Pena-dos-Santos et al. (2009) showed that δ/ opioid receptors mediate
antinociception at the temporomandibular joint in rats, as also we demonstrated in
this study. Chicre-Alcântara et al. (2012) have provided evidence that the
activation of kappa opioid receptors located in the TMJ region reduces two
important parameters of inflammation, such as plasma extravasation and
neutrophil migration. Intra-articular administration of the selective kappa agonist
blocks plasma protein extravasation and neutrophil migration induced by formalin
in a dose-dependent way. Additionally, studies performed by Cunha et al. (2012)
evidenced that the peripheral activation of the kappa opioid receptor directly
blocks the inflammatory hyperalgesia induced by PGE2. The non-participation of
the μ opioid receptor in the induction of central antinociceptive response mediated
by AEL in the TMJ hypernociception can be explained by the fact that the opioid
receptors are sensitized in different ways.

44
The activation of μ receptor is related to the increasement of GRK
expression, a kinase coupled to a G-protein receptor, and the activation of beta-
arrestin, the protein responsible for the desensitization of receptors coupled to a
G-protein (Zang et al., 1998; Raehal et al., 2005). In other words, it is required a
higher phosphorylation GRK-mediated to activate the μ receptor than what is
required for δ and receptors, which suggests that the expression of this protein
in different cells and tissues may lead to distinct antinociceptive responses. In
addition, the action of morphine on the μ receptor, the opioid agent used in this
study, differs from other opioid agonists such as etorphine. It is noteworthy that
both morphine and etorphine effectively activate the μ receptor, but morphine is
not able to stimulate μ receptor phosphorylation by GRK in certain cell types,
indicating substantial differences in the agonist sites binding of this receptor (Zang
et al., 1998). Several studies have been carried out in order to elucidate the
molecular bases of the μ opioid receptor and to discover new ligands with
chemotypes for coupling of this receptor, such as the compound PZM21, a
selective and potent agonist of μ, However, it promotes analgesia only to the
affective component of the pain, what means it is more specific for reflexive spinal
responses (Manglik et al., 2016).
5. Conclusion
In conclusion, we demosntrated the antinociceptive and anti-inflammatory
activity of AEL in a model of formalin-induced TMJ inflammatory hypernociception
in rats. Additionally, our results strongly suggest that AEL efficacy involves TNF-α
inhibition and the activation of the δ and , but not of μ opioid receptor. Given the
well-demonstrated anti-nociceptive and anti-inflammatory efficacy of AEL, the
design of novel compounds is highly encouraged with the hope of defining new
pharmacological targets for the treatment of inflammatory TMJ pain.
6. Acknowledgments
This work was supported by Brazilian grants from Fundação Cearense de
Apoio ao Desenvolvimento Científico e Tecnológico (FUNCAP), Conselho
Nacional de Pesquisa (CNPq), Coordenação de Aperfeiçoamento de Pessoal de

45
Nível Superior (CAPES) and Instituto de Biomedicina do Semi-Árido Brasileiro
(INCT-IBSAB).
7. References
Abbott, F. V., Franklin, K. B., Connell, B., 1986. The stress of a novel environment
reduces formalin pain: possible role of serotonin. European journal of
pharmacology, 126(1), 141-144.
Alencar, N. M., Assreuy, A. M., Havt, A., Benevides, R. G., de Moura, T. R., de
Sousa, R. B., Cavada, B. S., 2007. Vatairea macrocarpa (Leguminosae) lectin
activates cultured macrophages to release chemotactic mediators. Naunyn-
Schmiedeberg's archives of pharmacology, 374(4), 275-282.
Assreuy, A. M. S., Fontenele, S. R., de Freitas Pires, A., Fernandes, D. C.,
Rodrigues, N. V. F. C., Bezerra, E. H. S., Cavada, B. S., 2009. Vasodilator effects
of Diocleinae lectins from the Canavalia genus. Naunyn-Schmiedeberg's archives
of pharmacology, 380(6), 509-521.
Cairns, B. E., 2010. Pathophysiology of TMD pain–basic mechanisms and their
implications for pharmacotherapy. Journal of oral rehabilitation, 37(6), 391-410.
Castro, M. M., Godoy, A. R., Cardoso, A. I. I., 2008. Qualidade de sementes de
quiabeiro em função da idade e do repouso pós-colheita dos frutos. Ciênc.
agrotec., 32(5), 1491-1495.
Chicre-Alcântara, T. C., Torres-Chávez, K. E., Fischer, L., Clemente-Napimoga, J.
T., Melo, V., Parada, C. A., Tambeli, C. H., 2012. Local kappa opioid receptor
activation decreases temporomandibular joint inflammation. Inflammation, 35(1),
371-376.
Clemente, J.T., Parada, C.A., Veiga, M.C.A., Gear, R.W., Tambeli, C.H., 2004.
Sexual dimorphism in the antinociception mediated by kappa opioid. Neuroscience
Letters, 372: 250–255.
Cunha, T.M., Souza, G.R., Domingues, A.C., Carreira, E.U., Lotufo, C.M., Funez,
M.I., Verri Jr, W.A., Cunha, F.Q., Ferreira, S.H., 2012. Stimulation of peripheral
Kappa opioid receptors inhibits inflammatory hyperalgesia via activation of the
PI3Kg/AKT/nNOS/NO signaling pathway. Molecular Pain, 8:10.

46
De Rossi, S.S., Greenberg, M.S., Lui, F., Steinkeler, A., 2014. Temporomandibular
Disorders: Evaluation and Management. The Medical Clinics of North America, 98
(6): 1353-1384.
Do Val, D.R., Bezerra, M.M., Silva, A.A.R., Pereira, K.M.A., Rios, L.C., Lemos,
J.C., Arriaga, N.C., Vasconcelos, J.N., Benevides, N.M.B., Pinto, V.T.P., Cristino-
Filho, G., Brito, G.A.C., Silva, F.R.L., Santiago, G.M.P., Arriaga, A.M.C., Chaves,
H.V., 2014. Tephrosia toxicaria Pers. Reduces temporomandibular joint
inflammatory hypernociception: the involvement of the HO-1 pathway. Eur. J. Pain,
18: 1280–1289.
Emshoff, R., Puffer, P., Rudisch, A., & Gaßner, R., 2000. Temporomandibular joint
pain: Relationship to internal derangement type, osteoarthrosis, and synovial fluid
mediator level of tumor necrosis factor-α.Oral Surgery, Oral Medicine, Oral
Pathology, Oral Radiology, and Endodontology, 90(4): 442-449.
Figueiredo, J. G., da Silveira Bitencourt, F., Beserra, I. G., Teixeira, C. S., Luz, P.
B., Bezerra, E. H. S., de Alencar, N. M. N., 2009. Antinociceptive activity and
toxicology of the lectin from Canavalia boliviana seeds in mice. Naunyn-
Schmiedeberg's archives of pharmacology, 380(5): 407-414.
Fiorentino, P. M., Cairns, B. E., Hu, J. W., 1999. Development of inflammation
after application of mustard oil or glutamate to the rat temporomandibular joint.
Archives of oral biology, 44(1): 27-32.
Fischer, L., Arthuri, M.T., Torres-Chavez, K. E., Tambeli, C.H., 2009. Contribution
of endogenous opioids to gonadal hormones-induced temporomandibular joint
antinociception. Behavioral neuroscience (5): 1129.
Freitas, R.S, do Val, D.R., Fernandes, M.E.F., Gomes, F.I.F., Lacerda, J.T.J.G.
de, Gadelha, T.S., Gadelha, C.A.A., Pinto, V.P.T., Cristino-Filho, G., Pereira,
K.M.P., Brito, G.A.C., Bezerra, M.M., Chaves, H.V., 2016. Lectin from
Abelmoschus esculentus reduces zymosan-induced temporomandibular joint
inflammatory hypernociception in rats via heme oxygenase-1 pathway integrity
and tnf-α and il-1β suppression. Iternational Immunopharmacology, 38: 313-23.
Greene, C.S., 2010. Managing the care of patients with temporomandibular
disorders. The Journal of the American Dental Association, 141(9), 1086-1088.

47
Gunson, M.J., Arnett, G.W., Milam, S.B., 2012. Pathophysiology and
pharmacologic control of osseous mandibular condylar resorption. Journal of Oral
and Maxillofacial Surgery, 70(8): 1918-1934.
Gürbüz, I., Üstün, O., Yeşilada, E., Sezik, E., Akyürek, N., 2002. In vivo
gastroprotective effects of five Turkish folk remedies against ethanol-induced
lesions. Journal of ethnopharmacology, 83(3): 241-244.
Hamada, Y., Kondoh, T., Holmlund, A. B., Sakota, K., Nomura, Y., Seto, K., 2008.
Cytokine and clinical predictors for treatment outcome of visually guided
temporomandibular joint irrigation in patients with chronic closed lock. Journal of
Oral and Maxillofacial Surgery, 66(1): 29-34.
Kumar, R., Patil, M. B., Patil, S. R., & Paschapur, M. S., 2009. Evaluation of
Abelmoschus esculentus mucilage as suspending agent in paracetamol
suspension. Int J. Pharm.Tech. Res.,1(3): 658-665.
Lei, J., Fu, J., Yap, A.U., Fu, K.Y., 2016. Temporomandibular disorders symptoms
in Asian adolescents and their association with sleep quality and psychological
distress. Cranio: the journal of craniomandibular practice, 34(4), 242-9.
Manfredini, D., Guarda-Nardini, L., Winocur, E., Piccotti, F., Ahlberg, J., Lobbezoo,
F., 2011. Research diagnostic criteria for temporomandibular disorders: a
systematic review of axis I epidemiologic findings. Oral Surgery, Oral Medicine,
Oral Pathology, Oral Radiology, and Endodontology, 112(4): 453-462.
Manglik, A., Lin, H., Aryal, D.K., McCorvy, J.D., Dengler, D., Corder, G., Levit, A.,
Kling, R.C., Bernat, V., Hübner, H., Huang, X-P., Sassano, M.F., Giguère, P.M.,
Löber, S., Duan, D., Scherrer, G., Kobilka, B.K., Gmeiner, P., Roth, B.L., Shoichet,
B.K., 2016. Structure-based discovery of opioid analgesics with reduced side
effects. Nature, 537: 185-190.
Masnikosa, R., Nikolić, A. J., & Nedić, O., 2008. Lectin-induced alterations of the
interaction of insulin and insulin-like growth factor 1 receptors with their ligands.
Journal of the Serbian Chemical Society, 73(8-9): 793-804.
Monte, L.G., Santi-Gadelha, T., Reis, L.B., Barganhol, E., PrietschR.F.,
Dellagostin, O.A., Rodrigues e Lacerda, R., Gadelha, C.A.A., Conceição, F.R.,

48
Pinto, L.S., 2014. Lectin of Abelmoschus esculentus (okra) promotes selective
antitumor effects in human breast cancer cells. Biotechnology Latters, 36(3):461-9.
Napimoga, M.H., Cavada, B.S., Alencar, N.M.N., Mota, M.L., Bittencourt, F.S.,
Alves-Filho, J.C., Grespan, R., Gonçalves, R.B., Clemente-Napimoga, J.T., de
Freitas, A., Parada, C.A., Ferreira, S.H., Cunha, F.Q., 2007. Lonchocarpus
sericeus lectin decreases leukocyte migration and mechanical hypernociception by
inhibiting cytokine and chemokines production. International
Immunopharmacology, 7: 824–835.
Nũnéz, S., Lee, J. S., Zhang, Y., Bai, G., & Ro, J. Y., 2007. Role of peripheral μ-
opioid receptors in inflammatory orofacial muscle pain. Neuroscience, 146(3):
1346-1354.
Nordahl, S., Alstergren, P., & Kopp, S., 2000. Tumor necrosis factor-alpha in
synovial fluid and plasma from patients with chronic connective tissue disease and
its relation to temporomandibular joint pain. Journal of oral and maxillofacial
surgery, 58(5): 525-530.
Panero, F. S., Vieira, M. F. P., Cruz, Â. M., Moura, M. F. V., da Silva, H. E. B.,
2009. Aplicação da análise exploratória de dados na discriminação geográfica do
quiabo do Rio Grande do Norte e Pernambuco. Eclética Química, 34(3): 33-40.
Pena-dos-Santos, D. R., Severino, F. P., Pereira, S. A. L., Rodrigues, D. B. R.,
Cunha, F. Q., Vieira, S. M., ... & Clemente-Napimoga, J. T., 2009. Activation of
peripheral κ/δ opioid receptors mediates 15-deoxy-Δ12, 14-prostaglandin J 2
induced-antinociception in rat temporomandibular joint. Neuroscience, 163(4):
1211-1219.
Picolo, G., Cury, Y., 2004. Peripheral neuronal nitric oxide synthase activity
mediates the antinociceptive effect of Crotalus durissus terrificus snake venom, a
delta- and kappa-opioid receptor agonist. Life Sciences 75: 559–573.
Rangel, T. B. A., Assreuy, A. M. S., Pires, A. D. F., Carvalho, A. U. D., Benevides,
R. G., Simões, R. D. C., Nagano, C. S., 2011. Crystallization and characterization
of an inflammatory lectin purified from the seeds of Dioclea wilsonii. Molecules,
16(6): 5087-5103.

49
Raehal, K.M., Walker, J.K.L., Bohn, L.M., 2005. Morphine Side Effects in β-
Arrestin 2 Knockout Mice. Journal of Pharmacology and Experimental
Therapeutics, 314(3): 1195-1201.
Rivanor, R.L.C., Chaves, H.V., do Val., D.R., Freitas, A.R., Lemos, J.C.,
Rodrigues, J.A.G., Pereira, K.M.A., Araújo, I.W.F., Bezerra, M.M., Benevides,
N.M.B.A., 2014. A Lectin from the gren seaweed Caulerpa cupressoides reduces
mechanical typernociception and inflamation in the rat temporomandibular joint
during zymosam-induced arthrits, Int. Immunopharmacol, 21: 34-43.
Rodrigues, J.A.G., Chaves, H.V., Alves, K.S., Filgueira, A.A., Bezerra, M.M.,
Benevides, N.M., 2014. Structural features and assessment of zymosan-induced
arthritis in rat temporomandibular joint model using sulfated polysaccharide. Acta
Scientiarum. Biological Sciences Maringá, 36(2): 127-135.
Roveroni, R.C., Parada, C.A., Cecília, M., Veiga, F.A., Tambeli, C.H., 2001.
Development of a behavioral model of TMJ pain in rats: the TMJ formalin test.
Pain, (94):185-191.
Shafer, D. M., Assael, L., White, L. B., & Rossomando, E. F., 1994. Tumor
necrosis factor-α as a biochemical marker of pain and outcome in
temporomandibular joints with internal derangements. Journal of oral and
maxillofacial surgery, 52(8): 786-791.
Silva, H.C., Alfa, U.B., Pereira-Junior, F.N., Simões, R.C., Barroso-Neto, I.L.,
Nobre, C.B., Pereira, G.M., Nascimento, K.S., Rocha, B.A.M., Delatorre, P.,
Nagano, C.S, Assreuy, A.M.S., Cavada, B.S., 2011. Purification and Partial
Characterization of a New Pro-Inflammatory Lectin from Bauhinia bauhinioides
Mart (Caesalpinoideae) Seeds. Protein and Peptide letters, 18(4): 396-402.
Slade G.D., Bair, E., Greenspan, J.D., Dubner, R., Fillingim, R.B., Diatchenko, L.,
Maixner, W., Knott, C., Ohrbach, R., 2013. Signs and symptoms of first-onset TMD
and sociodemographic predictors of its development: the OPPERA prospective
cohort study. Journal Pain, 14(12):T20–T32.e1–e3.
Slade, G.D., Ohrbach, R., Greenspan, J.D., Fillingim, R.B., Bair, E., Sanders, A.E.,
Dubner, R., Diatchenko, L., Meloto, C.B., Smith, S., Maixner, W., 2016. Painful

50
temporomandibular disorder: decade of discovery from oppera studies. Journal of
Dental Research, 95(10): 1084-1092.
Soares, G. D. S. F., Assreuy, A. M. S., de Almeida Gadelha, C. A., de Morais
Gomes, V., Delatorre, P., da Conceiçao Simoes, R., Pessoa, H. D. L. F., 2012.
Purification and biological activities of Abelmoschus esculentus seed lectin. The
protein journal, 31(8): 674-680.
Tjolsein, A., Berge, O. G., Hunskaar, S., Rosland, J. H., Hole, K., 1992. The
formalin test: an evaluation of the method. Pain, 51(1): 5-17.
Torres-Chavéz, K.E., Sanfins, J.M., Clemente-Napimoga, J.T., Pelegrini-Da-Silva,
A., Parada, C.A., Fischer, L., Tambeli, C.H., 2012. Effect oh gonadal sterroid
hormones on formalin-induced temporomandibular joint inflammation.
EuropeanJournal of Pain, 16(2): 204-216.
Vicente, A. M., Guillén, M. I., Habib, A., & Alcaraz, M. J., 2003. Beneficial effects
of heme oxygenase-1 up-regulation in the development of experimental
inflammation induced by zymosan. Journal of Pharmacology and Experimental
Therapeutics, 307(3): 1030-1037.
Zang, J., Ferguson, S.S.G., Barak, L.S., Bodduluri, S.R., Laporte, E.A., Law, P-Y.,
Caron, M.G., 1998. Role for G protein-coupled receptor kinase in agonist-specific
regulation of m-opioid receptor responsiveness. Neurobiology, 95: 7157-7162.

51
REFERÊNCIAS
ALENCAR, N.M. et al. Vatairea macrocarpa (Leguminosae) lectin activates cultured macrophages to release chemotactic mediators. Naunyn-Schmiedeberg's archives of pharmacology, v. 374 (4), p. 275-282, 2007. ASSREUY, A.M.S. et al. Vasodilator effects of Diocleinae lectins from the Canavalia genus. Naunyn-Schmiedeberg's archives of pharmacology, v. 380 (6), p. 509-521, 2009. BARRETTO, S.R. et al. Evaluation of anti-nociceptive and anti-inflammatory activity of low-level laser therapy on temporomandibular joint inflammation in rodents. Journal of Photochem. and Photobio. B: Bio., v. 129, p. 135–142, 2013. BEUTH, J. et al. Importance of lectins for the prevention of bacterial infections and cancer metastases. Glycoconjugate Journal, v. 12, p. 1-6, 1995. BOYD, W.C.; SHAPLEIGH, E. Specific precipitating activity of plant agglutinins (Lectins). Science, v. 119 (3091), p 419, 1954. CAIRNS, B.E. Pathophysiology of TMD pain–basic mechanisms and their implications for pharmacotherapy. Journal of Oral Rehabilitation, v. 37 (6), p. 391-410, 2010. CASTRO, M.M.; GODOY, A.R.; CARDOSO, A. I.I. Qualidade de sementes de quiabeiro em função da idade e do repouso pós-colheita dos frutos. Ciênc. Agrotec., v. 32 (50), p. 1491-1495, 2008. CHAVES, H. V. et al. Experimental model of zymosan-induced arthritis in the rat temporomandibular joint: role of nitric oxide and neutrophils. Journal of Biomedicine & Biotechnology. V. 2011, p. 1-11, 2011. CHIANG, C.Y. et al. Role of glia in orofacial pain. The Neurocisntist, v. 17 (3), p. 303-320, 2011.
CHIANG, C.Y.; SESSLE, B.J.; DOSTROVSKY, J.O. Role of astrocytes in pain. Springer Science, v. 37, p. 2419-2431, 2012.
De ROSSI, S.S. et al. Temporomandibular Disorders: Evaluation and Management. The Medical Clinics of North America, v. 98 (6), p. 1353-1384, 2014.
Do VAL, D.R. et al. Tephrosia toxicaria Pers. Reduces temporomandibular joint inflammatory hypernociception: the involvement of the HO-1 pathway. European Journal Pain, v. 18, p. 1280-1289, 2014. ELLIS, A.; BENNETT, D.L. Neuroinflammation and the generation of neuropathic pain. British Journal of Anaesthesia, v. 111 (1), p. 26–37, 2013.

52
FERNANDES, W.V.B.; MICHELOTTO, A.B.; KIMURA, S. Comparação entre Técnicas Osteopáticas e Fisioterapia Convencional para o Tratamento das Desordens Temporomandibulares. Revista Inspirar. Curitiba, v. 1 (1), p. 29-33, 2009.
FIGUEIREDO, J.G. et al. Antinociceptive activity and toxicology of the lectin from Canavalia boliviana seeds in mice. Naunyn-Schmiedeberg's archives of pharmacology, v. 380 (5), p. 407-414, 2009. FONG, A.; SCHUG, S.A. Pathophysiology of pain: a pratical primer. Plast. Reconstr. Surg., v. 134 (4-2), p. 8S-14S, 2013.
FREITAS, R.S. Lectin from Abelmoschus esculentus reduces zymosan-induced temporomandibular joint inflammatory hypernociception in rats via heme oxygenase-1 pathway integrity and tnf-α and il-1β suppression. Iternational Immunopharmacology, v. 38, p. 313-23, 2016.
FUSARO, M. C. G. O. et al. P2X3 and P2X2/3 receptors mediate mechanical hyperalgesia induced by bradykinin, but not by pro-inflammatory cytokines, PGE2 or dopamine. European Journal of Pharmacology, v. 649, p. 177-182, 2010.
GADELHA, C.A. et al. Native crystal structure of a nitric oxide-releasing lectin from the seeds of Canavalia maritima. Journal of Structural Biology, v. 152, p. 185–194, 2005.
GOLDEINSTEIN, I.J. et al. What should be caled a lectin? Nature, v. 285, p. 66, 1980.
GORAKSHAKAR, A.C.; GHOSH, A. Use of lectins in immunohematology. Asian J Transfus Sci., v. 10 (1), p. 12–21, 2016. GREENE, C. S. Managing the care of patients with temporomandibular disorders. The Journal of the American Dental Association, 141(9): 1086-1088, 2010.
HARGREAVES, K.M. Review - Orofacial pain. Pain, 152: S25-S32, 2011.
JULIUS, D., BASBAUM, A.I. Molecular mechanisms of nociception. Nature, v. 413 (6852), p. 203-210, 2001.
KITSOULIS, P. et al. Signs and Symptoms of Temporomandibular Joint Disorders Related to the Degree of Mouth Opening and Hearing Loss. BMC Ear. Nose and Throat Disorders, v. 11 (5), p. 1-8, 2011.

53
KHOSROZADEH, M., HEYDARI, N., ABOOTALEBI, M. The Effect of Abelmoschus Esculentus on Blood Levels of Glucose in Diabetes Mellitus. Iran. J. Med. Sci., v. 41 (3), p. S63, 2016. KOCOUREK, J.; HOREJSI, V. Nature, News & Views, v. 290, p.188, 1981.
KOSTRZEWA-JANICKA, J. et al. Inflammatory markers in temporomandibular joint disorders. Centr Eur J Immunol., v. 37 (3), p. 290-293, 2012.
KUMAR, R. et al. Evaluation of Abelmoschus esculentus mucilage as suspending agent in paracetamol suspension. Int J. Pharm.Tech. Res., v. 1 (3), p. 658-665, 2009.
LEEUW, R. Dor orofacial: guia de avaliação, diagnóstico e tratamento. 4ª ed. Quintessence, 2010.
LEEUW, R., KLASSER, G.D. Orofacial Pain-Guildeness for assessement, diagnosis, and management. 5th edition, Quintessence, 2013.
LEI, J. et al. Temporomandibular disorders symptoms in Asian adolescents and their association with sleep quality and psychological distress. Cranio: the journal of craniomandibular practice, v. 34 (4), p. 242-9, 2016.
LI, Y.X. et al. Antifatigue Effects of Ethanol Extracts and Polysaccharides Isolated from Abelmoschus esculentus. Pharmacogn Mag., v. 12 (47), p. 219–224, 2016.
CHRISPEELS, M.J., RAIKHELB, N.V. Lectins, Lectin Genes, and Their Role in Plant Defense. The Plant Cell, v. 3, p. 1-9, 1991.
MACFARLANE, T.V. Orofacial pain in the community: prevalence and associated impact. Community Dentistry Oral Epidemiology, Copenhagen, v. 30 (1), p. 56-60, 2002.
MAIXNER, W. et al. Orofacial Pain Prospective Evaluation and Risk Assessment Study – The oppera study. The Journal of Pain, v. 12 (11), p. T4-T11, 2011.
MANFREDINI, D. et al. Research diagnostic criteria for temporomandibular disorders: a systematic review of axis I epidemiologic findings. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, v. 112 (4), p. 453-462, 2011.
MATTHEWS, B., SESSLE, B.J. Mecanismos periféricos da dor orofacial. In: Dor orofacial – Da ciência Básica à Conduta Clínica. Quintessence, v. 1, p. 37-46, 2002.

54
MANISKOSA, R., NIKOLIĆ, A.J., NEDIĆ, O. Lectin-induced alterations of the interaction of insulin and insulin-like growth factor 1 receptors with their ligands. Journal of the Serbian Chemical Society, v. 73 (8-9), p. 793-804, 2008.
MILAM, S.B., AUFDEMORTE, T.B., SHERIDAN, P.J. Sexual dimorphism in the distribution of estrogen receptors in the temporomandibular joint complex of the baboon.Oral Surg; Oral Med; Oral Pathol, v. 64, p. 527–32, 1987.
MONTE, L.G. et al. Lectin of Abelmoschus esculentus (okra) promotes selective antitumor effects in human breast cancer cells. Biotechnology Latters, v. 36 (3), p. 461-9, 2014.
MONTEIRO, D.R. et al. Relationship between anxiety and chronic orofacial pain of temporomandibular disorder in a group of university students. J. of Prost. Res., v. 55, p. 154–158, 2011.
OBERMANN, M. Treatment options in trigeminal neuralgia. Therap. Adv. in neur. Disor., v. 3, p. 107-115, 2010.
OKESON, J. P. Dor orofacial: guia para avaliação, diagnóstico e tratamento. São Paulo (SP): Santos Livraria, 1998.
OKESON, J. P. Dores Bucofaciais de Bell. São Paulo (SP): Quintessence, 2003.
OKESON, J. P.; Tratamento das desordens temporomandibulares e oclusão. Rio de Janeiro (RJ): Elsevier, 2008.
OLIVEIRA-FUSARO, M.C.G. et al. 5-HT induces temporomandibular joint nociception in rats through the local release of inflammatory mediators and activation of local β adrenoceptors. Pharm., Bioch. and Beh., v. 102, p. 458–464, 2012.
OLIVEIRA, L.F. Atualização em mecanismos e fisiopatologia da dor. In: Primer Simposio Virtual De Dolor. Medicina Paliativa y Avances en Farmacologia Del Dolor, nov./ dez. Anais… [S. l.]: [S. n.], 2011.
PANERO, F.S. et al. Aplicação da análise exploratória de dados na discriminação geográfica do quiabo do Rio Grande do Norte e Pernambuco. Eclética Química, v. 34 (3), p. 33-40, 2009.
PNEUMANS, W.J., VAN DAMME, E.J.M. Lectins as plant defense proteins. Plant Physiology, v. 109, p. 347–352, 1995.
55
PORRECA, F., OSSIPOV, M.H., GEBHART, G.F. Chronic pain and medullary descending facilitation. Tre. Neurosci., v. 25, p. 319-124, 2012.
RANDO, C., WALDRON, T. TMJ osteoarthritis: A new approach to diagnosis. Amer. J. of Physical Anthr., v. 148 (1), p. 45-53, 2012.
RANGEL, T.B.A. et al. Crystallization and characterization of an inflammatory lectin purified from the seeds of Dioclea wilsonii. Molecules, v. 16 (6), p. 5087-5103, 2011.
REN, K.; DUBNER, R. The role of trigeminal interpolaris-caudalis transition zone in persistent orofacial pain. Int. Rev. Neurobiol., v. 97, p. 207-25, 2011.
REYES, M.R., UYANIK, J.M. Orofacial pain management: current perspectives.
Dove Press Journal: Journal of Pain Research, v. 7, p. 99-115, 2014.
RIBEIRO, K.A. et al. Αlpha-2 Adrenergic and Opioids Receptors Participation in Mice Gastroprotection of Abelmoschus esculentus Lectin. Curr. Pharm. Des., v. 22 (30), p. 4736-4742, 2016.
RINNI, J.M. Lectin Structure. Annu. Rev. Biophys. Biomol. Struct., v. 24, p. 551-577, 1995.
RIVANOR, R.L.C. et al. A Lectin from the gren seaweed Caulerpa cupressoides reduces mechanical typernociception and inflamation in the rat temporomandibular joint during zymosam-induced arthritis. Int. Immunopharmacol, v. 21, p. 34-43, 2014.
ROBBINS; COTRAN. Patologia: Bases Patológicas das Doenças. 4ª ed. Elsevier, 2005.
RODRIGUES, J.A.G. et al. Structural features and assessment of zymosan-induced arthritis in rat temporomandibular joint model using sulfated polysaccharide. Acta Scientiarum. Biological Sciences Maringá, v. 36 (2), p. 127-135, 2014.
SABITHA, S.R.; NAVEEN, K.R.; PANNEERSELVAM, K. Antidiabetic and antihyperlipidemic potential of Abelmoschus esculentus (L.) Moench. In streptozotocin induced diabetic rats. J. Pharm. Bioallied Sci., v. 3, p. 397-402, 2011.
SCRIVANI, S.J.; KEITH, D.A.; KABAN, L.B. Temporomandibular disorders. N Engl J Med., v. 359, p. 2693–705, 2008.

56
SESSLE, B.J. Acute and chronic craniofacial pain: brainstem mechanisms of nociceptive transmission and neuroplasticity, and their clinical correlates. Crit. Rev. Oral Biol. Med., v. 11 (1), p. 57-91, 2000.
SHARMA, S. et al. Etiological factors of temporomandibular joint disorders. Nat. J. Maxillofac. Surg., v. 2 (2), p. 116-119, 2011.
SHARON, N.; LIS, H. lectins as cell recognition molecules. Science, v. 246 (4927), p. 227-34, 1989.
SHARON, N.; LIS, H. History of lectins: from hemagglutinins to biological recognition molecules. Glycobiology, v. 14 (11), p. 53R-62R, 2004.
SHARON, N.; LIS, H. Lectins. Springer Science & Business Media, 2007. SLADE, G.D. et al. Painful temporomandibular disorder: decade of discovery from oppera studies. Journal of Dental Research, v. 95 (10), p. 1084-1092, 2016.
SLADE, G.D. et al. COMT Diplotype Amplifies Effect of Stress on Risk of Temporomandibular Pain. Journal of Dental Research, v. 94 (9), p. 1187-1195, 2015.
SOARES, G.D.S.F. et al. Purification and biological activities of Abelmoschus esculentus seed lectin. The protein journal, v. 31 (8) p. 674-680, 2012.
SOCIEDADE BRASILEIRA PARA O ESTUDO DA DOR (SBED). Salve seu cérebro. Jornal da Dor, v. 36, p. 4, 2010.
SOCIEDADE BRASILEIRA PARA O ESTUDO DA DOR (SBED). Dor Orofacial: desafios e perspectivas. Jornal da Dor, v. 43, p. 3, 2012.
SOCIEDADE BRASILEIRA PARA O ESTUDO DA DOR (SBED). Ano internacional de combate à dor orofacial. Jornal da Dor, v. 48, p. 03, 2013.
STEVEN, L.; KRAUS, P.T. Characteristics of 511 patients with temporomandibular disorders referred for physical therapy. Oral Medicine, v. 118 (4), p. 432-439, 2014.
TAKEMURA, M. et al. Mechanisms of orofacial pain control in the central nervous system. Arch. Histol. Cytol., v. 69, p. 79-100, 2006.
VASCONCELOS, S.M.M. at al. Central action of Araucaria angustifolia seed lectin in mice. Epilepsy & Behavior, v. 15 (3), p. 291-293, 2009.

57
VENKATESHA, S.H.; BERMAN, B.M.; MOUDGIL, K.D. Review- Herbal medicinal products target defined biochemical and molecular mediators of inflammatory autoimmune arthritis. Bioorg. & Med. Chem., v. 19, p. 21-29, 2011.
VERRI-JUNIOR, W.A. et al. Hypernociceptive role of cytokines and chemokines: Targets for analgesic drug development? Pharm. & Ther., v. 112 (116), p. 138, 2006.

58
APÊNDICE
Resumo Gráfico Exigido pelo Periódico Journal of Ethnopharmacology

59
ANEXO A
Declaração de Aceite do Comitê de Ética

60
ANEXO B
Normas da Revista Journal of Ethnopharmacology
Article structure
Subdivision - numbered sections
Divide your article into clearly defined and numbered sections. Subsections should
be numbered 1.1 (then 1.1.1, 1.1.2,), 1.2, etc. (the abstract is not included in
section numbering). Use this numbering also for internal cross-referencing: do not
just refer to 'the text'. Any subsection may be given a brief heading. Each heading
should appear on its own separate line.
Introduction
State the objectives of the work and provide an adequate background, avoiding a
detailed literature survey or a summary of the results.
Material and methods
Provide sufficient detail to allow the work to be reproduced. Methods already
published should be indicated by a reference: only relevant modifications should
be described.
Theory/calculation
A Theory section should extend, not repeat, the background to the article already
dealt with in the Introduction and lay the foundation for further work. In contrast, a
Calculation section represents a practical development from a theoretical basis.
Results
Results should be clear and concise.
Discussion
This should explore the significance of the results of the work, not repeat them. A
combined Results and Discussion section is often appropriate. Avoid extensive
citations and discussion of published literature.

61
Conclusions
The main conclusions of the study may be presented in a short Conclusions
section, which may stand alone or form a subsection of a Discussion or Results
and Discussion section.
Glossary
Please supply, as a separate list, the definitions of field-specific terms used in your
article.
Appendices
If there is more than one appendix, they should be identified as A, B, etc.
Formulae and equations in appendices should be given separate numbering: Eq.
(A.1), Eq. (A.2), etc.; in a subsequent appendix, Eq. (B.1) and so on. Similarly for
tables and figures: Table A.1; Fig. A.1, etc.
Essential title page information Title
Concise and informative. Titles are often used in information-retrieval systems.
Avoid abbreviations and formulae where possible. • Author names and
affiliations. Please clearly indicate the given name(s) and family name(s) of each
author and check that all names are accurately spelled. Present the authors'
affiliation addresses (where the actual work was done) below the names. Indicate
all affiliations with a lower-case superscript letter immediately after the author's
name and in front of the appropriate address. Provide the full postal address of
each affiliation, including the country name and, if available, the e-mail address of
each author. • Corresponding author. Clearly indicate who will handle
correspondence at all stages of refereeing and publication, also post-publication.
Ensure that the e-mail address is given and that contact details are kept up
to date by the corresponding author. • Present/permanent address. If an
author has moved since the work described in the article was done, or was visiting
at the time, a 'Present address' (or 'Permanent address') may be indicated as a
footnote to that author's name. The address at which the author actually did the
work must be retained as the main, affiliation address. Superscript Arabic
numerals are used for such footnotes.

62
Abstract
A concise and factual abstract is required. The abstract should state briefly the
purpose of the research, the principal results and major conclusions. An abstract is
often presented separately from the article, so it must be able to stand alone. For
this reason, References should be avoided, but if essential, then cite the author(s)
and year(s). Also, non-standard or uncommon abbreviations should be avoided,
but if essential they must be defined at their first mention in the abstract itself. The
author should divide the abstract with the headings Ethnopharmacological
relevance, Aim of the study, Materials and Methods, Results, and
Conclusions.
Graphical abstract
A Graphical abstract is mandatory for this journal. It should summarize the
contents of the article in a concise, pictorial form designed to capture the attention
of a wide readership online. Authors must provide images that clearly represent
the work described in the article. Graphical abstracts should be submitted as a
separate file in the online submission system. Image size: please provide an
image with a minimum of 531 × 1328 pixels (h × w) or proportionally more. The
image should be readable at a size of 5 × 13 cm using a regular screen resolution
of 96 dpi. Preferred file types: TIFF, EPS, PDF or MS Office files. You can view on
our information site. Authors can make use of Elsevier's Illustration and
Enhancement service to ensure the best presentation of their images also in
accordance with all technical requirements:
Keywords
After having selected a classification in the submission system, authors must in
the same step select 5 keywords. These keywords will help the Editors to
categorize your article accurately and process it more quickly. A list of the
classifications and set keywords can be found. In addition, you can provide a
maximum of 6 specific keywords, using American spelling and avoiding general
and plural terms and multiple concepts (avoid, for example, "and", "of"). Be sparing
with abbreviations: only abbreviations firmly established in the field may be
eligible. These keywords will be used for indexing purposes.

63
Chemical compounds
You can enrich your article by providing a list of chemical compounds studied in
the article. The list of compounds will be used to extract relevant information from
the NCBI PubChem Compound database and display it next to the online version
of the article on ScienceDirect. You can include up to 10 names of chemical
compounds in the article. For each compound, please provide the of the most
relevant record as in the following example: Glutamic acid (PubChem CID:611).
Please position the list of compounds immediately below the 'Keywords' section. It
is strongly recommended to follow the exact text formatting as in the example
below: Chemical compounds studied in this article Ethylene glycol (PubChem CID:
174); Plitidepsin (PubChem CID: 44152164); Benzalkonium chloride (PubChem
CID: 15865).
Plant names
In the Materials and Methods section there must be a separate heading for
describing the material used. That includes official name, local name, English
name (if known), GPS position in case of collection in the wild or cultivation, a
voucher specimen must be deposited in an official herbarium for possible future
comparison. In the text it should be stated that the plant name has been checked
with mentioning the data of accessing that website. In case of commercially
procured material should mention the source, batch number, quality control data.
Data on chemical characterization (metabolomics, chromatographic methods)
should also be presented, in case of known active compounds their quantitative
analysis should be presented.
Acknowledgements
Collate acknowledgements in a separate section at the end of the article before
the references and do not, therefore, include them on the title page, as a footnote
to the title or otherwise. List here those individuals who provided help during the
research (e.g., providing language help, writing assistance or proof reading the
article, etc.).
Formatting of funding sources
List funding sources in this standard way to facilitate compliance to funder's

64
requirements: Funding: This work was supported by the National Institutes of
Health [grant numbers xxxx, yyyy]; the Bill & Melinda Gates Foundation, Seattle,
WA [grant number zzzz]; and the United States Institutes of Peace [grant number
aaaa].
It is not necessary to include detailed descriptions on the program or type of grants
and awards. When funding is from a block grant or other resources available to a
university, college, or other research institution, submit the name of the institute or
organization that provided the funding.
If no funding has been provided for the research, please include the following
sentence: This research did not receive any specific grant from funding agencies
in the public, commercial, or not-for-profit sectors.
Math formulae
Please submit math equations as editable text and not as images. Present simple
formulae in line with normal text where possible and use the solidus (/) instead of a
horizontal line for small fractional terms, e.g., X/Y. In principle, variables are to be
presented in italics. Powers of e are often more conveniently denoted by exp.
Number consecutively any equations that have to be displayed separately from the
text (if referred to explicitly in the text).
Footnotes
Footnotes should be used sparingly. Number them consecutively throughout the
article. Many word processors can build footnotes into the text, and this feature
may be used. Otherwise, please indicate the position of footnotes in the text and
list the footnotes themselves separately at the end of the article. Do not include
footnotes in the Reference list.
References Citation in text
Please ensure that every reference cited in the text is also present in the reference
list (and vice versa). Any references cited in the abstract must be given in full.
Unpublished results and personal communications are not recommended in the
reference list, but may be mentioned in the text. If these references are included in
the reference list they should follow the standard reference style of the journal and

65
should include a substitution of the publication date with "Unpublished results".
"Personal communication" will not be accepted as a reference. Citation of a
reference as "in press" implies that the item has been accepted for publication.
Reference style
Text: All citations in the text should refer to:
1. Single author: the author's name (without initials, unless there is ambiguity) and
the year of publication;
2. Two authors: both authors' names and the year of publication;
3. Three or more authors: first author's name followed by 'et al.' and the year of
publication.
Citations may be made directly (or parenthetically). Groups of references should
be listed first alphabetically, then chronologically.
Examples: 'as demonstrated (Allan, 2000a, 2000b, 1999; Allan and Jones, 1999).
Kramer et al. (2010) have recently shown .…' List: References should be arranged
first alphabetically and then further sorted chronologically if necessary. More than
one reference from the same author(s) in the same year must be identified by the
letters 'a', 'b', 'c', etc., placed after the year of publication.
Examples:
Reference to a journal publication: Van der Geer, J., Hanraads, J.A.J., Lupton,
R.A., 2010. The art of writing a scientific article. J. Sci. Commun. 163, 51–59.
Reference to a book: Strunk Jr., W., White, E.B., 2000. The Elements of Style,
fourth ed. Longman, New York.
Reference to a chapter in an edited book: Mettam, G.R., Adams, L.B., 2009. How
to prepare an electronic version of your article, in: Jones, B.S., Smith, R.Z. (Eds.),
Introduction to the Electronic Age. E-Publishing Inc., New York, pp. 281–304.
Reference to a website:Cancer Research UK, 1975. Cancer statistics reports for
the UK. (accessed 11.11.16).