university of science and technology beijing
DESCRIPTION
Modern Tools to Understand the Epidemiology of Infectious Diseases. Lequan Min. University of Science and Technology Beijing. Outline. 1. Introduction. 2. Viral Infection/ Anti-Viral Infection Therapy/ Epidemic Spreading. 3. Modeling Viral Infection /Anti-Viral - PowerPoint PPT PresentationTRANSCRIPT

University of Science and Technology Beijing
Lequan Min
Modern Tools to Understand the Epidemiology of Infectious Diseases
1
1. Introduction 1. Introduction 1. Introduction 1. Introduction
3. Modeling Viral 3. Modeling Viral InfectionInfection /Anti-Viral /Anti-Viral Infection Therapy/ Infection Therapy/ Epidemic Spreading3. Modeling Viral 3. Modeling Viral InfectionInfection /Anti-Viral /Anti-Viral Infection Therapy/ Infection Therapy/ Epidemic Spreading
4. Concluding Remarks 4. Concluding Remarks 4. Concluding Remarks 4. Concluding Remarks
2. Viral Infection/ 2. Viral Infection/ Anti-Viral Infection Anti-Viral Infection Therapy/ Epidemic Therapy/ Epidemic Spreading2. Viral Infection/ 2. Viral Infection/ Anti-Viral Infection Anti-Viral Infection Therapy/ Epidemic Therapy/ Epidemic Spreading
Outline
2

Acknowledgements:
This work is jointly supported by the 11TH 5- Year Plan Key Research Project of China (No.2008ZX10005-006) , and the NNSF of China (Nos. 61074192).
Many thanks my colleagues Asoci. Prof. Yongmei Su at USTB, Pro. Yang Kuang at the Arizona State Univ., and my students Dr. Yu Zheng, Dr. Xiao Chen, Dr. Qun Zhang, Qilin Su, Quian Huang, Yao Hu and Pengfei Zhang for their very valuable co-operations, and Dr. Stefan F. Wieland at the Scripps Research Institute US for kindly providing the data for seven chimpanzees.
3

1. Introduction1. Introduction 1. Introduction1. Introduction
4

●Two major viruses infected people in the world: ● 1966, B. S. Blumberg: Hepatitis B virus (HBV).● 1983, F. Barré-Sinoussi and L. MontagnierHuman immunodeficiency virus (HIV).
1. Introduction1. Introduction 1. Introduction1. Introduction
5
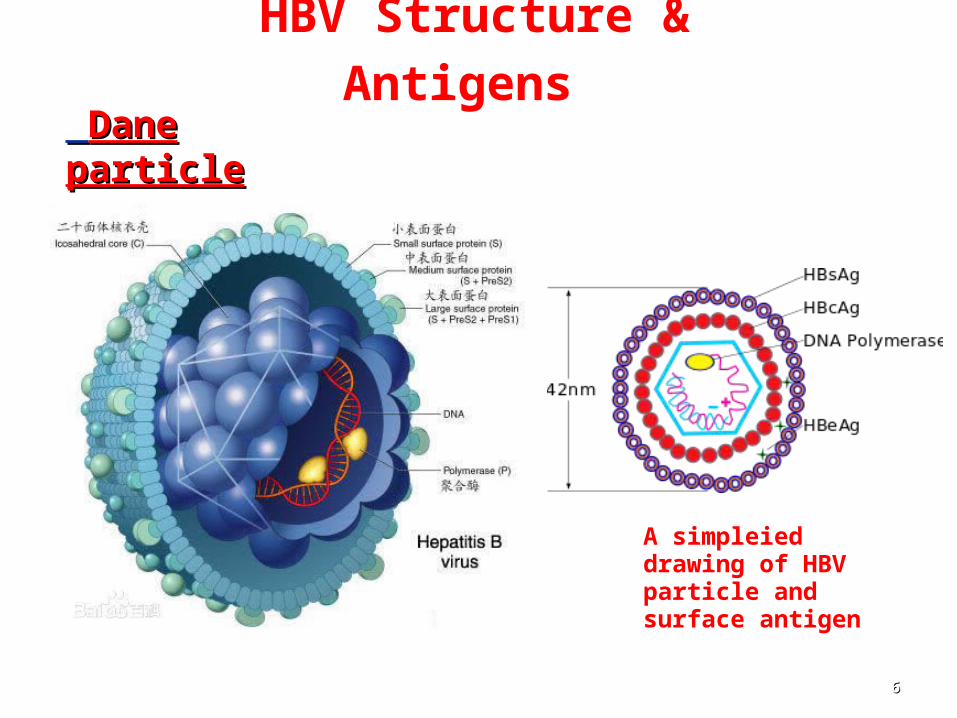
HBV Structure & Antigens Dane Dane particleparticle
66
A simpleied drawing of HBV particle and surface antigen
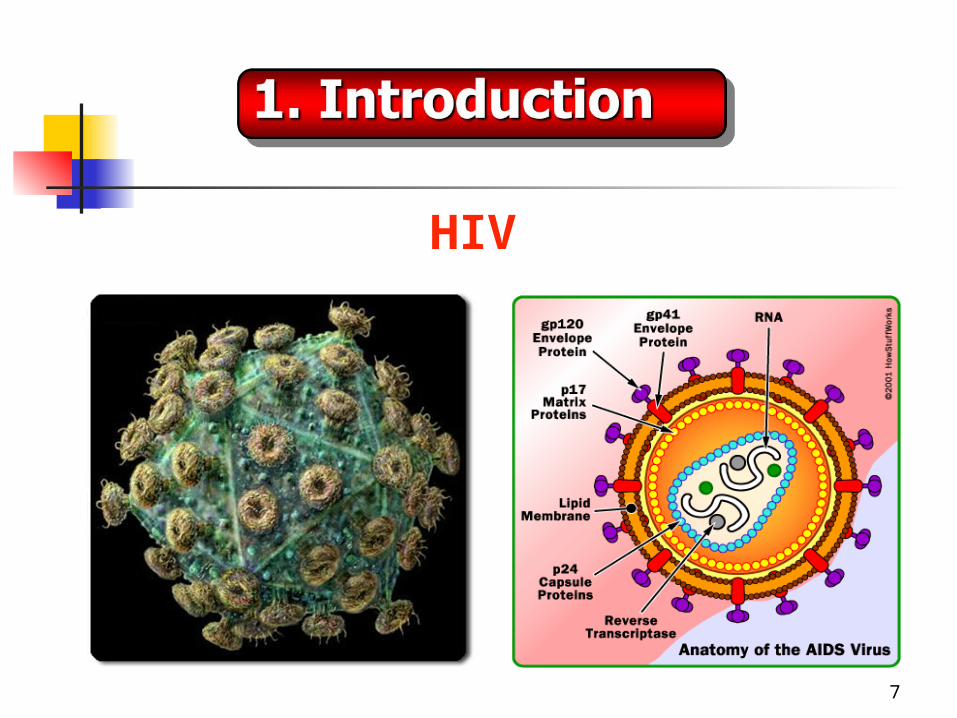
HIV
7

1. Introduction1. Introduction 1. Introduction1. Introduction
Against SARS
herpes zoster virus infection
chest-wall virus infectionVaricella zoster Virus infection
Over 5 hundred kind viruses are able to infect Human Beings .
8
Why are there unknown reason infections? Why do some virus infected people have
recovered without therapy? Why do some people appear very sensitive
to viruses and become persistent infections? Why do some anti-HBV/HIV infection therapy
patients’ serum viruses have relapsed , and become worse after stopping treatments ?
9

Why do wild animals without any prevention have hardly become extinct by attacks of various infectious diseases?
Why do domestic animals more easily die by attacks of infectious diseases?
Why did Influenza during 1918-1919 killed nearly 50 million people, and no similar cases appear now day?
This talk will give some interpretations with some clinic/experimental evidences by modelling dynamics of viral infection and anti-viral infection therapy/epidemic spreading, and not going to address conclusive statements.
10

Black Death resulted in the deaths of an estimated 75 to 200 million people during 1346-1353, killed 30–60% of Europe's total population.
Influenza pandemic during 1918-1919 killed nearly 50 million people worldwide.
SARS pandemic in 2003. WHO: cumulative SARS cases worldwide total of 8,422 . Death total
of 919.
2.1 Epidemic Spreads
11

Hepatitisweb studySource: CDC and Prevention. MMWR 2008;57(RR-8):1-20.
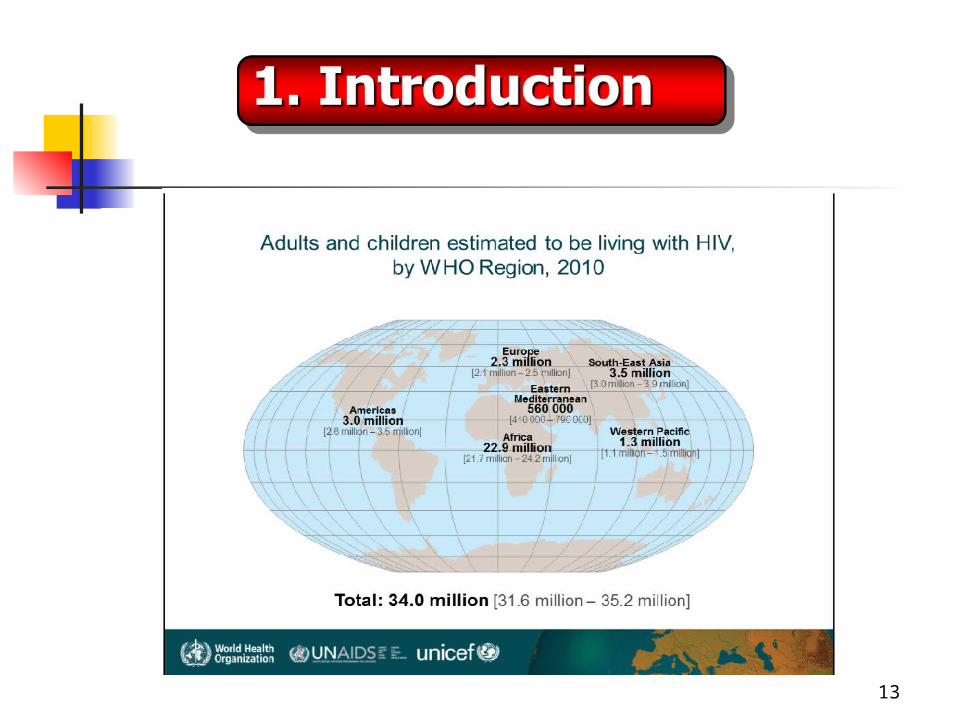
Prevalence of Chronic HBV Infection, Worldwide
HEPATITIS B : EPIDEMIOLOGY
More
Over 400 million people have chronic HBV infections
13

Source: WHO, Hepatitis B , 2014, (http://www.who.int)
全球超过 20 亿的人曾感染过乙肝病毒。 2 billion people have been infected with the hepatitis B virus (HBV) .
每年有超过 78 万的人死于急慢性乙型肝炎。 More than 780 000 people die every year due to the acute or chronic consequences of hepatitis B.
超过 2.4 亿的人为慢性 ( 终生 ) 乙肝感染者。 More than 240 million have chronic (lifelong) HBV infections.
慢性乙肝患者可以通过有效的治疗避免死亡。 Effective treatment of chronic HBV infection patient can aim to prevent the death from HBV disease.
2.2 HBV Infection and Anti-HBV Infection Therapy
14

Approved HBV treatments
Interferon:Interferon alfa-2b – 1991 Peginterferon alfa-2a (Peg-INF)– 2005Nucleoside Analogues (NA):Lamivudine (LAM)– 1998Adefovir (ADV)– 2002Entecavir – 2005Telbivudine (LTD)– 2006Tenofovir (TDF) – 2008
15
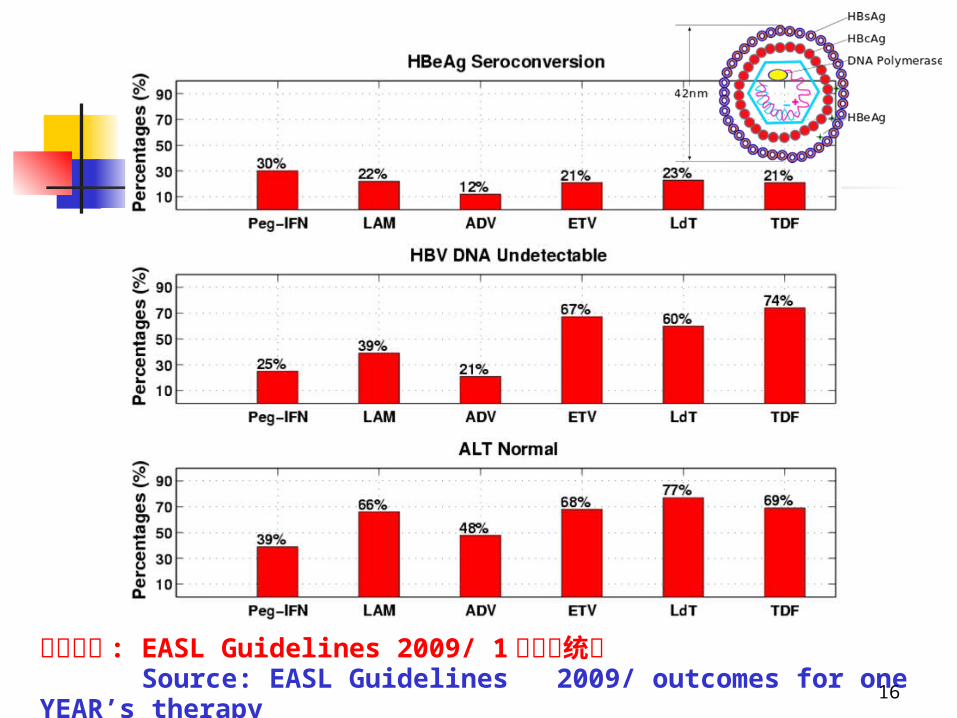
资料来源 : EASL Guidelines 2009/ 1 年疗效统计 Source: EASL Guidelines 2009/ outcomes for one YEAR’s therapy
16

Slide 25
0
20
40
60
80
Incid
enc
e of resistan
ce (%
)
0% 2%
11%
18%
5%
24%
0.3% 0.4%0.1% 0.8%
12%
25%
40%
Resistance to NAs…is it just a matter of time??
Lai, Clin Infect Dis, 2003, Westand, Hepatology 2003, Colonno, EASL 2007, Gane, EASL, 2008
Antiviral resistance increases over time

Source: Nowak M. J. et. al. Proc. Natl. Acad .Sci. USA 93, 1996: 4398-4402.
Serum HBV Relapsed immediately after stopping 168 days’ treatment with drug lamivudine.
An HBV infected patient with almost normal ALT treated by LVD
106 copies/ml was the lowest limit of detection
18

An Int. Anti-HBV Infection Therapy Trail.
19
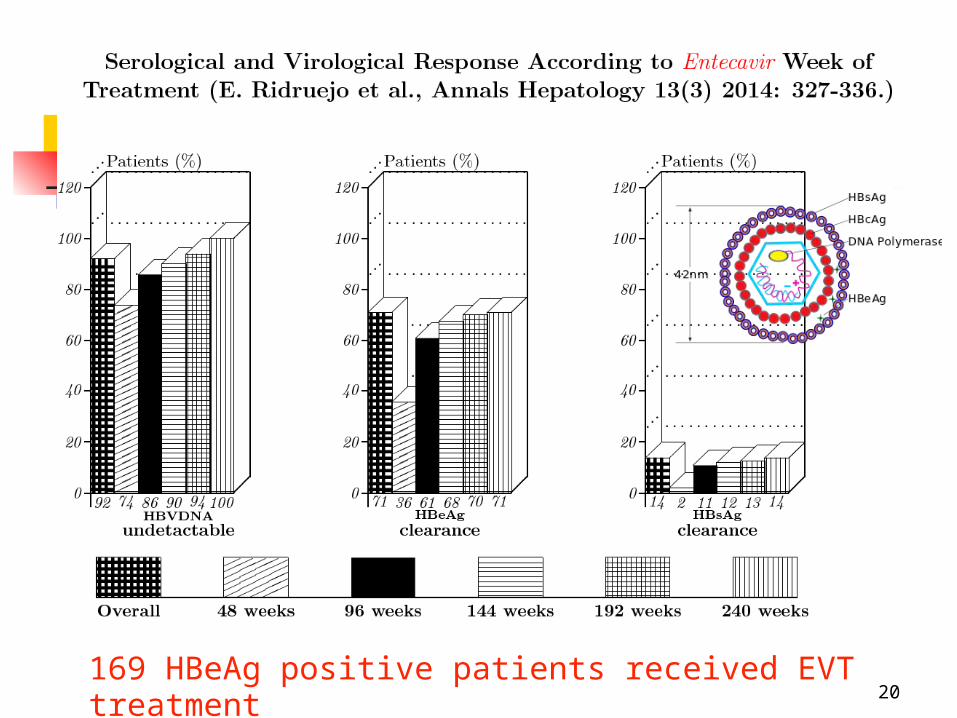
169 HBeAg positive patients received EVT treatment 20

PEG-IFN alpha, tenofovir (TDF), entecavir (ETN) had been selected as the first-line therapy to initial treatment in naive Chronic HBV infected patients.
In China, some Traditional Chinese Medicine (TCM) have also accepted as one choice to HBV infection therapy.
In particular to the patients who failed for NA treatments.
Source: EASL Clinical Practice Guidelines: management of chronic HBV infection, J. Hepatal 2012: 57: 167-185
21

Monotone Traditional Chinese Medicine (TCM) treatment.
TCM + NA combination treatment.
22

L. Min, Y. Ye, Proc. of The 3rd Int. Conf. On Bioinformatics and Biomedical Engineering (iCBBE 2009)
Long-term personalized TCM treatment to suppress HBV
1000 copies/ml was the lowest limit of detection
23
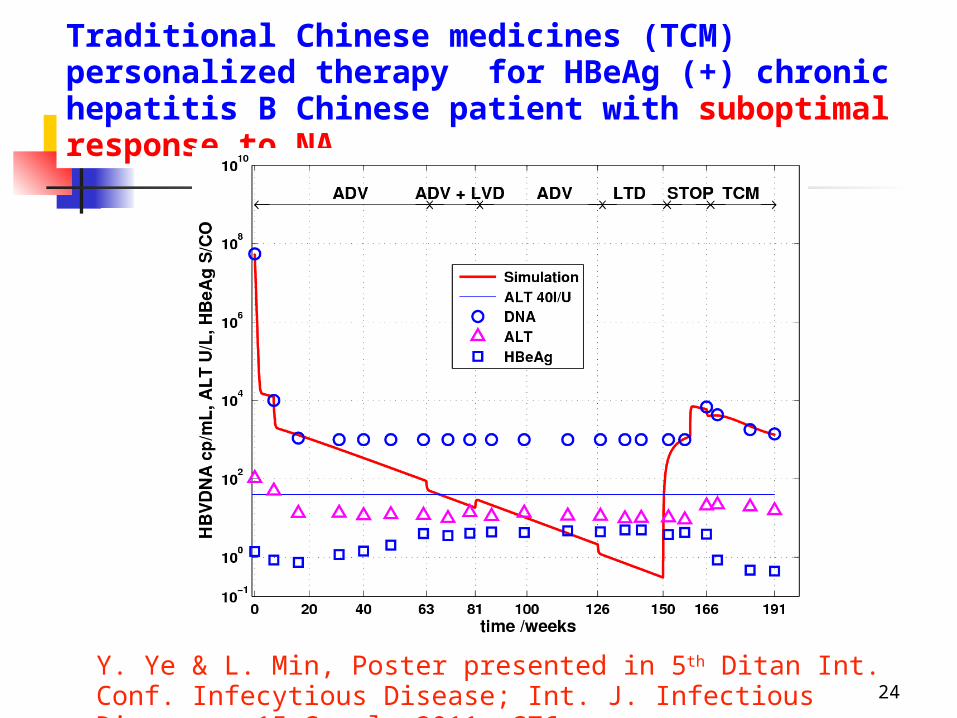
Traditional Chinese medicines (TCM) personalized therapy for HBeAg (+) chronic hepatitis B Chinese patient with suboptimal response to NA.
Y. Ye & L. Min, Poster presented in 5th Ditan Int. Conf. Infecytious Disease; Int. J. Infectious Diseases, 15 Suppl. 2011, S76.
24

X. Chen, L. Min, Y. Ye, Q. Zhang, Oral presentation addressed in 5th Ditan Int. Conf. Infecytious Disease; Int. J. Infectious Diseases, 15 Suppl. 2011, S28; Computer Eng. & Appl. (in Chinese), 48(24), 2012:20-27.
TCM + NA anti-HBV infection personalized combination therapy for a chronic HBV patient with almost normal ALT
25

TCM Treatments
Evidences show that traditional Chinese medicine (TCM) may regulate chronic hepatitis B (CHB) patients’ immune functions.
ChiCTR-TRC-10001263 was a double-bind randomized placebo-controlled trial.
Two kinds of TCMs were used in the trial: Tiaoganjianpihuoxue grain (TCM1) and Tiaoganjieduhuashi grain (TCM2).
26
A total of 560 CHB Chinese patients with HBeAg-positive were randomly assigned, in 1:1 ratio, two groups: experimental group (EXG) and controlled group (CTG), and each group are further divided into 3 subgroups.
CTG received 10 mg of ADV + placebo for TCM orally daily for 48 weeks.
Roughly speaking, EXG received TCM1 or TCM2 +placebo for ADV orally daily for the first 24 weeks, and then switched to TCM2 + ADV for additional 24 weeks.
27

The TCMs + AD therapy resulted significantly in increased proportion of patients achieving HBeAg loss in EXG two subgroups than the two CTG subgroups.
The other virologic and biochemical responses of CG and EG had not significant differences at week 48.
28
Results:
●28 / 31 patients in EXG / CTG achieved complete response.
● 42 /55 in EXG / CTG responded poorly.

29

Outcomes of the complete-response patients’ therapy efficacy in experimental group (EXG) and control (CTG) group.
Source: L. Min, X. Chen, Y. Ye et al., Evidence-Based Complementary and Alternative Medicine Volume 2013, http://dx.doi.org/10.1155/2013/767290 30
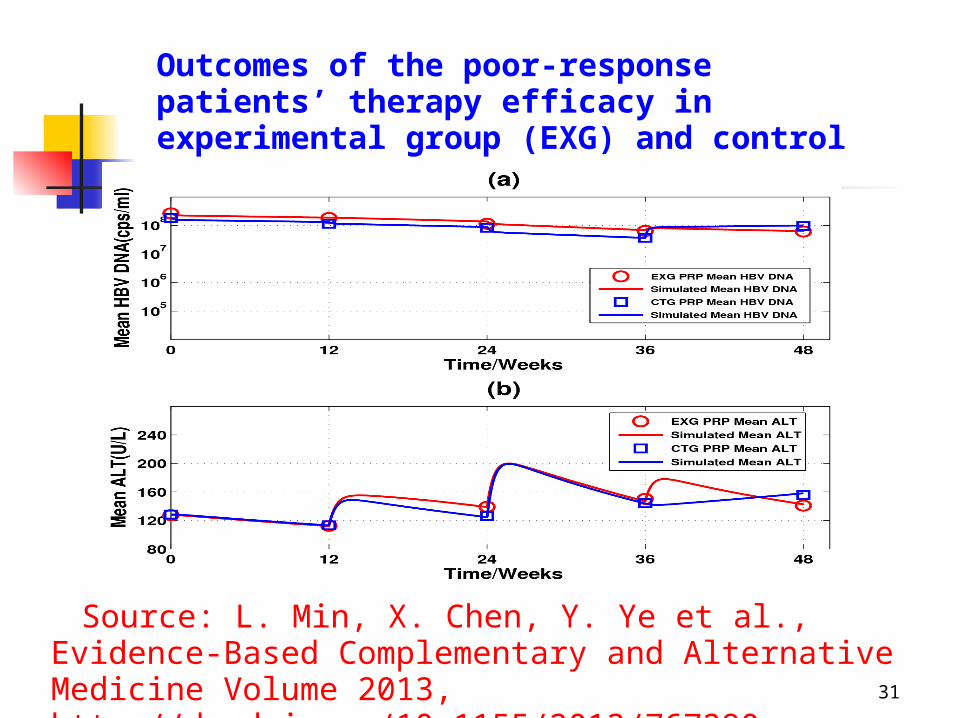
Source: L. Min, X. Chen, Y. Ye et al., Evidence-Based Complementary and Alternative Medicine Volume 2013, http://dx.doi.org/10.1155/2013/767290
Outcomes of the poor-response patients’ therapy efficacy in experimental group (EXG) and control (CTG) group
31
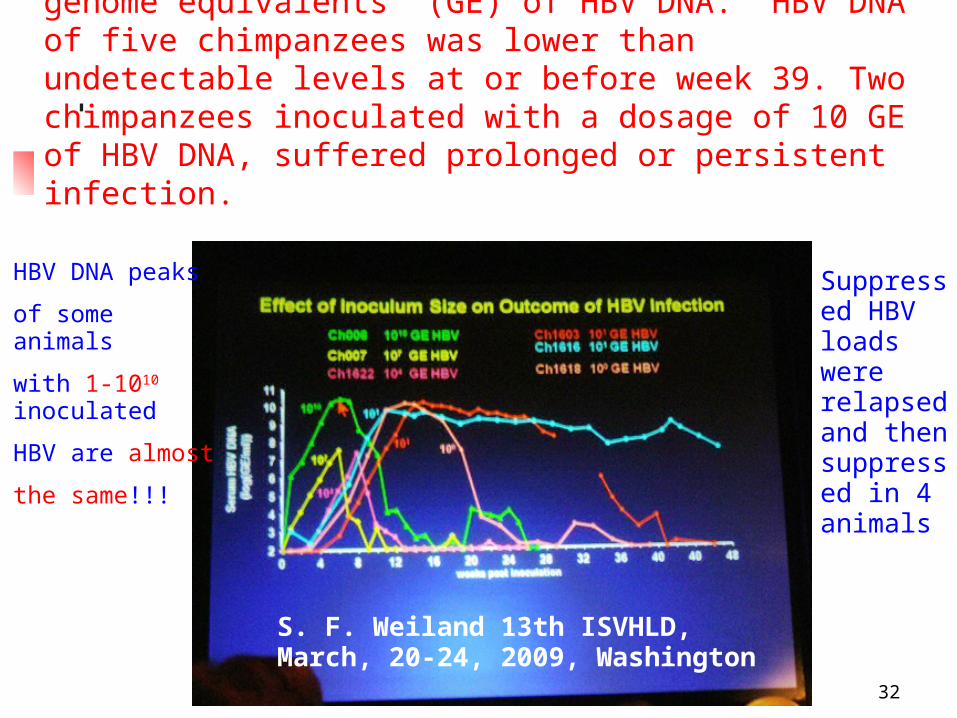
Seven chimpanzees were inoculated 1 to 1010 genome equivalents (GE) of HBV DNA. HBV DNA of five chimpanzees was lower than undetectable levels at or before week 39. Two chimpanzees inoculated with a dosage of 10 GE of HBV DNA, suffered prolonged or persistent infection.
S. F. Weiland 13th ISVHLD, March, 20-24, 2009, Washington
HBV DNA peaks
of some animals
with 1-1010 inoculated
HBV are almost
the same!!!
Suppressed HBV loads were relapsed and then suppressed in 4 animals
32

Source: WHO, Progress Report 2011 (http://www.who.int)
2010 全球新增 HIV 感染者人数约 2.7 百万 .
About 2.7 million people have been infected newly with HIV in 2010 .
2010 全球约有 1.8 百万人死于 HIV.
About 1.87 million people deaths from HIV in 2010 . 2010 全球约有 0.8% - 3 千 4 百万人感染 HIV.
About 0.8% --34 million people have been infected by HIV estimated in 2010 .
33
Antiretroviral (ART) medicines
Abacavir (ABC) Didanosine (DDI) Emtricitabine (FTC)
Lamivudine (3TC) Stavudine (D4T) Zidovudine (AZT)
Tenofovir (TDF) Efavirenz (EFV) Nevirapine (NVP) Tripranvir (TPV) Atazanavir (ATV) Durunavir (DRV) Fosamprenavir (f-APV) Indinavir (IDV) Lopinavir (LPV) Nelfinavir (NFV) Ritonavir (RTV) Saquinavir (SQV)
34

● *ART 治疗可使 10-30% 的初治患者在治疗前 4-8 周内伴有免疫恢复
● ART treatments may make 10–30% of the people be associated with immune recovery usually within the first 4–8 weeks.
● ART 治疗可显著地延长 HIV 感染者的寿命 ● ART treatments can significantly
prolong the life of HIV infected patients.
Antiretroviral (ART) medicines
*Source: WHO : Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection Progress 35
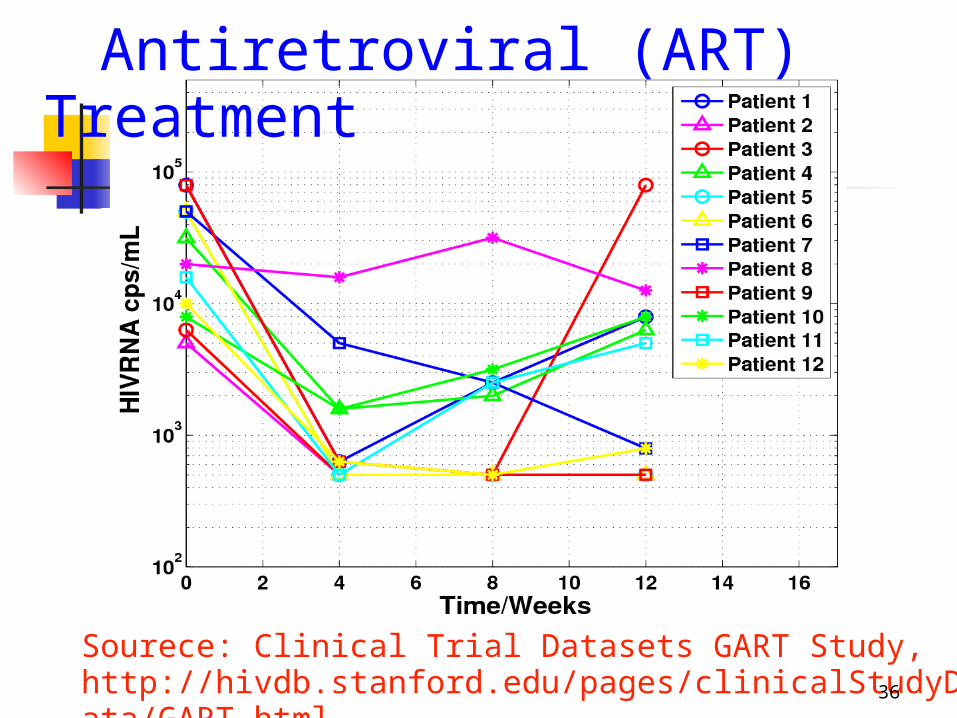
Antiretroviral (ART) Treatment
Sourece: Clinical Trial Datasets GART Study, http://hivdb.stanford.edu/pages/clinicalStudyData/GART.html.
36

The first and only man to be cured of HIV infection is Timothy Ray Brown treated for his HIV infection with a normal anti-HIV drug regimen.
When he developed leukemia, he underwent twice bone marrow transplants.
His HIV became imeidately undetectable after the first bone marrow transplants.
Five years later, Brown remains HIV free. Source http://www.webmd.com/hiv-aids/features/hiv-cure-
in-reach
37
It is a long way to against HIV
An HIV infected baby from Mississippi received treatment medications just 30 hours after birth.
Another HIV infected baby from California was treated when she was only 4 hours old.
The California baby is still HIV-negative almost a year after birth.
The Mississippi baby tested HIV-free for more than 2 years, but is now HIV-positive again.
http://www.webmd.com/hiv-aids/features/hiv-cure-in-reach
38

3.1. 乙肝病毒 (HBV) 感染 / 抗 HBV 感 染治疗动力学模型
3.1.1 Modelling anti-HBV Infection Therapy without Immune Response
39

Source: Nowak M. J. et. al. Proc. Natl. Acad . Sci. USA 93, 1996: 4398-4402
Basic virus infection model ( 基本病毒感染模型 ) Virus infection model Anti-virus infection therapy
model
(1)
40

x, y, v 分别表示未感染的细胞个数, 感染的细胞个数,游离病毒 (HBV) 个数 .
λ — 未感染细胞的产生速率。dx — 未感染细胞的死亡速率。βvx — 未感染细胞被游离病毒感染的速率。ay — 感染细胞的死亡速率。ky — 感染细胞产生病毒的速率。uv — 游离病毒被清除的速率。
● Without immune responds.
● Describe non-symptom
infections♂41

模型有两个常数解(平衡点):Two constant solution (equilibrium points)
Q1 ----- 康复平衡点(代表宿主痊愈)host's disease-free (virus free steady-
state) .
Q2 ----- 带毒平衡点(代表宿主持续感染)host's persistent infection (endemic
steady-state). 42
Source: P. D. Leenheer, H. L. Smith, SIAM J. Appl. Math. 63, 2003, 1313-1327.
基本病毒复制数 : Basic reproduce number:
如果
I. R 0< 1 ,则 Q1 是大范围吸引的 . If R 0 < 1 , then Q1 is globally attractive.
II. R 0 >1, 则 Q2 是大范围吸引的 . If R 0 > 1 , then Q2 is globally attractive.
43

基本病毒复制数 :Basic reproduce number:
Theoretical suggestions I. 具有 R 0< 1 的无症状病毒感染者,即使感染大量病毒也能自愈 ● Non-symptom infected individual with R 0< 1 will recover eventually even infected a large amount virus. II. 具有 R 0 >1 的无症状病毒感染者,即使感染 1 个病毒也成为持续带毒者 . ● Non-symptom infected individual with R 0> 1 will become persistent infection even infected one virus. 44
● R0 中的 λ/d 项表示患者肝细胞的总数量。
Term λ/d in R0 represents the total number of cells of the patients liver.
● 这意味着肝脏大的患者比肝脏小的感染者更容易持续带毒。 This implies that an individual with larger liver will more easily become persistent infection than the one with smaller liver.
● R0 的实际意义有异议的 .
The practical meaning of R0 is questionable .Source: L Min, Y Su , Y Kuang, Rocky Mountain J. Math. 8, 2008, 1573-1585. 45

An amended Basic Virus Indection Model
(4)(4)
Virus basic reproductive number R0= βk/au R0= (1 – m)(1 – n) βk/au
Independent on the total number of liver cells.
Source: L. Min, Y. Su, Kuang Y, Rocky Mountain J. Math. 8, 2008, 1573-1585.
3.1.1 3.1.1 Modelling anti-HBV Infection Therapy Modelling anti-HBV Infection Therapy without Immune Responsewithout Immune Response3.1.1 3.1.1 Modelling anti-HBV Infection Therapy Modelling anti-HBV Infection Therapy without Immune Responsewithout Immune Response
(4)
46
Source: L Min, Y Su, Y Kuang, Rocky Mountain J. Math. 8(5):1573-1585, 2008.
Y Zheng, L Min, Y. Ji, et al., J. Systems Science and Complexity. 23: 1221–1230,
Theorem 1 (L. Min, Y. Su & Y. Kuang 2008, Y. Zheng, L. Min, Y. Ji & Y. Kuang 2010)
If R0= βk/au ≤ 1. Then Q1 is globally attractive.
Non-symptom infected individual with R0= βk/au < 1 will recover eventually even infected a large amount virus. Since R0 is independent on λ/d, our model gives a more reasonable description than that of Nowak et al’s basic virus infection Model. Source: Y Zheng, L Min, Y. Ji, et al., J. Systems Science and Complexity. 23: 1221–1230, 2010.47

Source: L Min, Y Su, Y Kuang, Rocky Mountain J. Math. 8(5):1573-1585, 2008.
Y Zheng, L Min, Y. Ji, et al., J. Systems Science and Complexity. 23: 1221–1230,
Theorem 2 (Y. Zheng, L. Min, Y. Ji & Y. Theorem 2 (Y. Zheng, L. Min, Y. Ji & Y. Kuang 2010)Kuang 2010)
If If RR00= = ββk/auk/au > 1. Then > 1. Then QQ22 is globally is globally attractive. attractive.
Non-symptom infected individual withNon-symptom infected individual with RR0 0 = = ββk/auk/au > 1 will become persistent > 1 will become persistent
infection even infection even infected one virusinfected one virus..
Since Since RR00 is independent on is independent on λ/dλ/d, our model , our model gives a more reasonable description than that gives a more reasonable description than that of Nowak et al.’s basic virus infection Model. of Nowak et al.’s basic virus infection Model.
Source: Y Zheng, L Min, Y. Ji, et al., J. Systems Science and Complexity. 23: 1221–1230, 2010.48

Source: L Min, Y Su, Y Kuang, Rocky Mountain J. Math. 8(5):1573-1585, 2008.
Y Zheng, L Min, Y. Ji, et al., J. Systems Science and Complexity. 23: 1221–1230, 2010.
● ● 对于 R0= βk/au ≤ 1 的无症状感染者
即使感染大量病毒,也将最终痊愈。 ● 对于 R0= βk/au > 1 的无症状感染
者 即使感染微量( 1 个)病毒,也会成为 持续带毒者 .
49
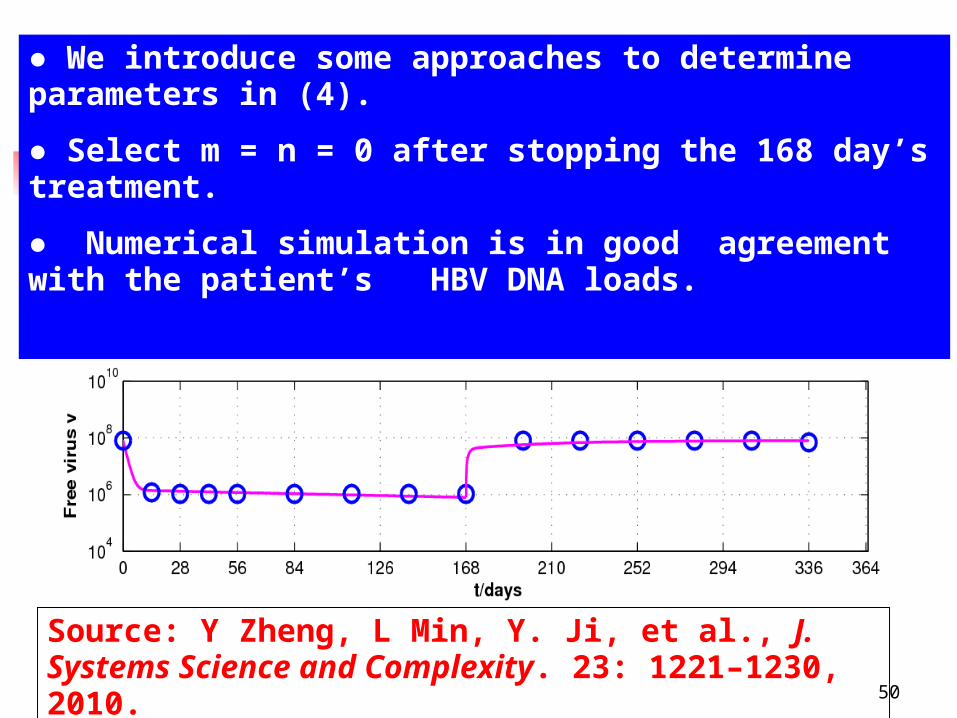
Fig. Modeling (solid line) LVD anti-HBV infection therapy and virus rebounded after stopping treatment at 168th day (circles) reported by Nowak et al. 1996. 模拟 Nowak et al. 等 1966 报道的 一个肝功ALT 正常患者拉米夫定抗 HBV 感染治疗( 1-168天)和停药 (168 天后 ) 反弹 .
Source: Y Zheng, L Min, Y. Ji, et al., J. Systems Science and Complexity. 23: 1221–1230, 2010.
● We introduce some approaches to determine parameters in (4).
● Select m = n = 0 after stopping the 168 day’s treatment.
● Numerical simulation is in good agreement with the patient’s HBV DNA loads.
50

Source: [1] Y Zheng, L Min, X Chen, et al., The 21st Conf. APASL, 2011 (poster: A-315-0046-01657).
[2] Y Zheng, L Min, X Chen, et al., Proc. of the 2011 IEEE International conference on Intelligent Computation and Bio-Medical Instrumentation, 291-295.
3.1.2 Modelling Anti-HBV Infection Therapy with Immune Response Term
(5)
51
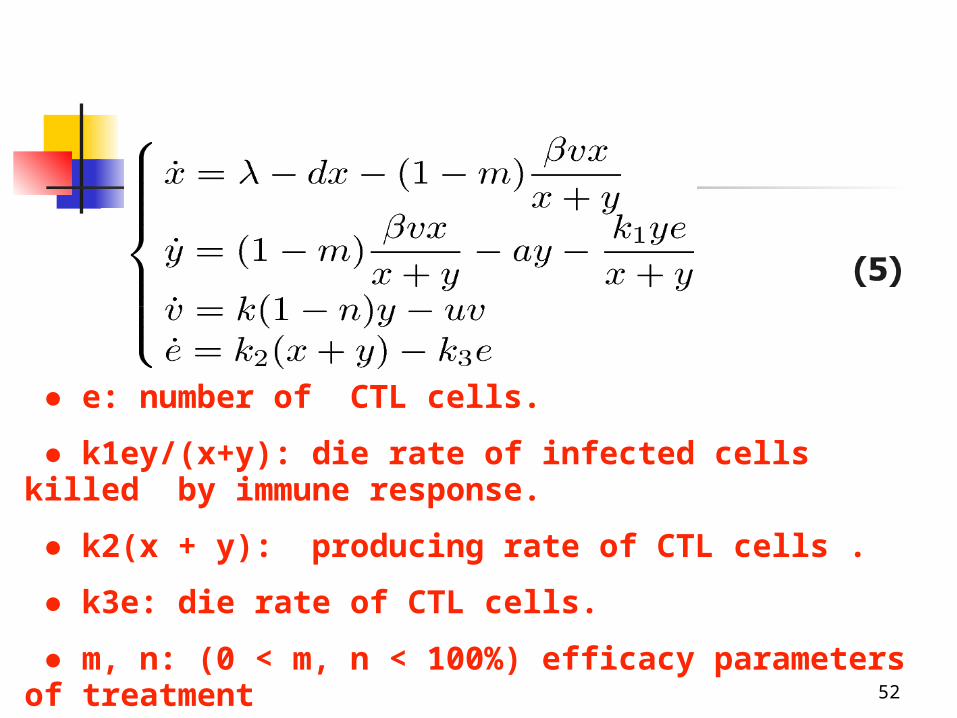
● e: number of CTL cells.
● k1ey/(x+y): die rate of infected cells killed by immune response.
● k2(x + y): producing rate of CTL cells .
● k3e: die rate of CTL cells.
● m, n: (0 < m, n < 100%) efficacy parameters of treatment 52

Theorem
● ● If R0 < 1 , then Q1 is locally
attractive.
●●
R0 patients with normal ALT without therapy
Efficacy of treatment
0 < m, n< 100%
Treatment make immune parameter k2 and Immune killing parameter k1 increase.
virus free steady-state
Source: Y Zheng, L Min, X Chen, et al., Proc. of the 2011 IEEE Int. conference on Intelligent Computation and Bio-Medical Instrumentation, 291-295.
●● Since R0 is independent on λ/d, and includes immune parameters ki’s and efficacy of treatment parameters m, n, our model gives a reasonable description for anti-HBV infection therapy.
53
Modelling Anti-HBV Infection Therapy
Background:
●● An Int. co-operation study on anti-HBV infection treatment reported by G. K. Lau et al.
●● OOne group of chronic HBV patients were assigned to receive peginterferon alfa-2a once weekly plus 100 mg of lamivudine once daily.
●● The study was comprised of 48 weeks of treatment and 24 weeks of treatment-free follow-up.
54
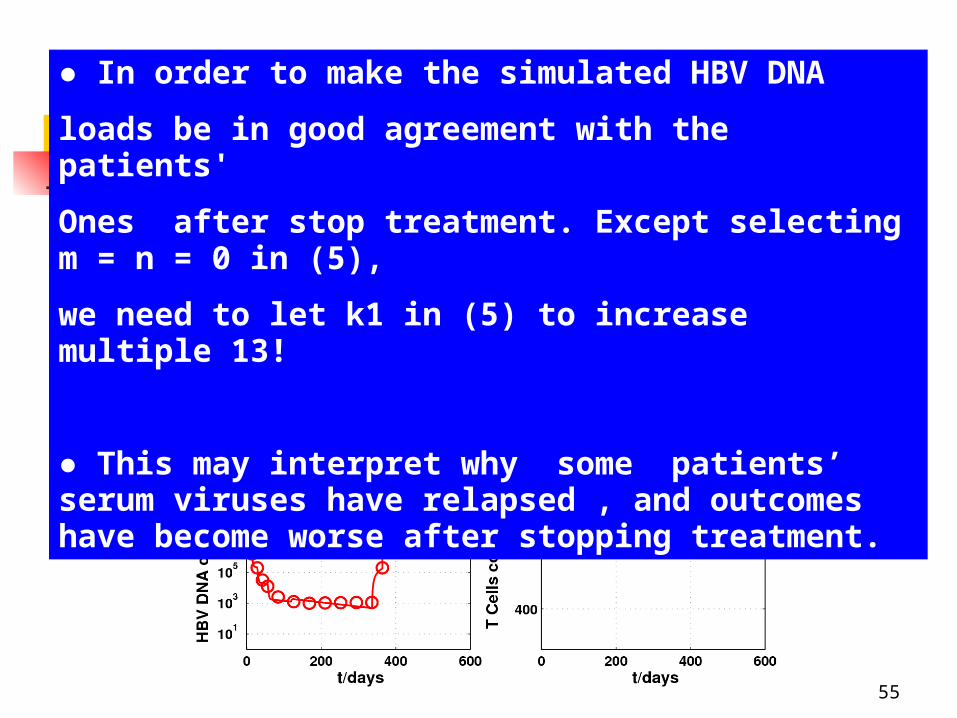
Fig. Solid lines: the dynamic routes of models. Circles: patient clinic data. (a) Uninfected cells. (b) Infected cells. (c) Virus decline in response to drug treatment and relapse after stopping the treatment. (d) T cells.
● In order to make the simulated HBV DNA
loads be in good agreement with the patients'
Ones after stop treatment. Except selecting m = n = 0 in (5),
we need to let k1 in (5) to increase multiple 13!
● This may interpret why some patients’ serum viruses have relapsed , and outcomes have become worse after stopping treatment.
55

Fig. 2.3 Simulations of five years of continuous treatment. Solid lines: the dynamic routes of models and. Circles: patient clinic data. (a) Uninfected cells. (b) Infected cells. (c) Virus decline in response to drug treatment and relapse after stopping the treatment. (d) T cells.
56

● Our Theorem and the representation of R0 suggest that long term therapy will clear all infected virus if no virus mutation or drug resistance exists. ● The numerical simulation of 5 years of continuous treatment and half year's follow up showed rapid reduction and relapse of patients’ mean HBV DNA levels. ● ● This suggests that many patients’ immune abilities cannot strong enough such that R0 < 1 after cease treatment. ● Numerical simulation result shows that 11 years of treatment is required to clear the hepatitis B virus from all hepatocytes.
57
3.1.3 Modelling Traditional Chinese Medicine (TCM) & ADEFOVIR (ADV) Combination Anti-HBV Infection Therapy
Background:
● ● Some TCM anti-CHB infection medicines have the advantages of rare viral mutation, rare side, and cheap price.
● Evidences show that TCM can regulate chronic hepatitis B (CHB) patients' immune functions.● ● Nucleoside analogues (NA) +TCM therapy have better efficacy than monotone treatment.Source: L. Min, X. Chen & Y. Ye et al., Poster BP-23,
The 22st Conference of the Asian Pacific Association for the Study of the Liver, 16-19 February, 2012, Taipei. Hepatology Intenational, 6(1) 2012.
58

● Study ChiCTR-TRC-10001263 : double-bind randomized placebo-controlled trial.● EXG TCM1/TCM2 + placebo AD for 24 weeks and switched TCM2 + AD for following 24 weeks.Results: ●28 / 31 patients in EXG / CTG achieved complete response.● 42 /55 in EXG / CTG responded poorly.● The TCMs + AD therapy resulted significantly in increased proportion of patients achieving HBeAg loss in EXG two subgroups than the two CTG subgroups.
59

The aim:● Model and simulate the dynamics of complete and poor response HBeAg positive CHB Chinese patients for ADV and TCM plus ADV therapy.
● Interpret the specific role of the TCM in the anti-HBV infection study ChiCTR-TRC-10001263
60

Two ModelsModel I: Modelling controlled group (CTG)
Model II: Modelling Experiemental group (EXG)
61
Kill virus
directly
w
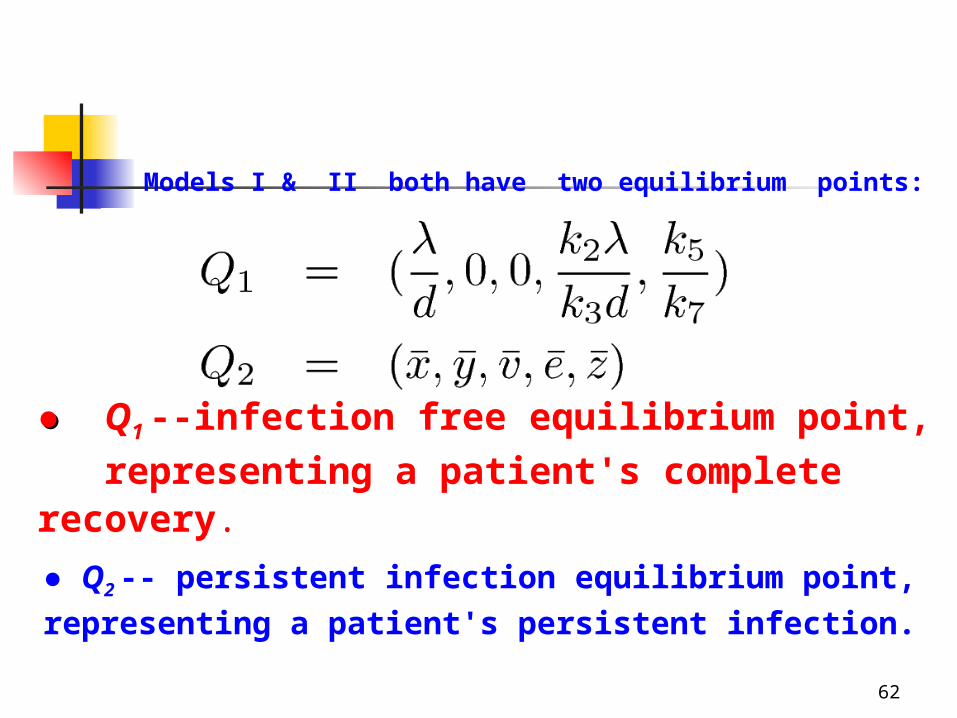
●● Q1 --infection free equilibrium point, representing a patient's complete recovery.
x
● Q2 -- persistent infection equilibrium point, representing a patient's persistent infection.
Models I & II both have two equilibrium points:
62

Model I: Modelling controlled group
Model II: Modelling expeeriement group
Treatment makes immune parameter k2, k4 increase
Theorem
● ● If R0 < 1 , then Q1 is locally
attractive.
●●
63
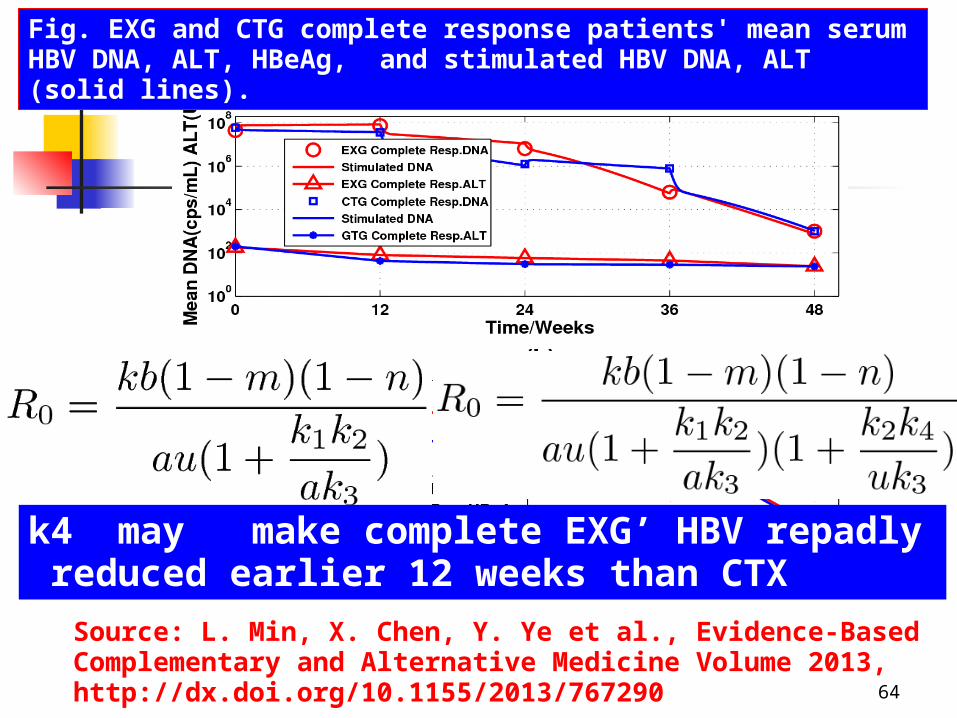
Fig. EXG and CTG complete response patients' mean serum HBV DNA, ALT, HBeAg, and stimulated HBV DNA, ALT (solid lines).
Source: L. Min, X. Chen, Y. Ye et al., Evidence-Based Complementary and Alternative Medicine Volume 2013, http://dx.doi.org/10.1155/2013/767290 64
k4 may make complete EXG’ HBV repadly reduced earlier 12 weeks than CTX

Fig. EXG and CTG poor response patients' mean serum HBV DNA, ALT, HBeAg, and stimulated HBV DNA, ALT (solid lines).
65
Additional TCM drug did not make EXG poor response patients' mean serum HBV DNA, ALT, HBeAg,Become worse

● The additional kinging parameter k4 made the EXG complete response patients' mean HBV DNA levels have reduced rapidly 12 weeks early than the ones in CTG.
● Long time treatment scheme may be benefit for the EXG patients if their activated immune abilities can be kept. 66
● Our model assumes: both TCMs and ADV have the function that prevents complete-response patients’ infected hepatocytes from being injured by CTLs; that is, the killing parameter 𝑘1 becomes smaller than its baseline values.● This hypothesis may interpret why the complete-response patients’ ALT loads decreased quickly while their HBV DNA levels decreased slowly or increased during the first 12-weektherapy
67

3.1.4 Modeling TCM + ADV + Entecovior (ENT) Combination Anti-HBV Infection Therapy
Background: A 57 years old male chronic HBeAg positive Patient (nucleosides-native) With mild cirrhosis and near normal ALT did not got any anti-HBV infection therapy in near 36 months before the combination treatment.
During February 2009 .2~ July 2011, the patient had received personalized TCM and
NA combination therapy. The results are shown in following Figs .
68

Fig. 2. 5. Outcomes of the treatment of the patient. (a) HBV DNA levels, Triangles: ALT levels, (b) Circles: HBeAg levels, Triangles: HBeAb levels.
69

Modeling TCM+ ADV + ENT against HBV Infection
k4ev/(x+y): clearing rate of virus generated by some specific immune abilities activated via anti-virus infection treatmentk8 is used to describe the liver injuiry caused by some drugs or unkwon reasons.
70

k4ev/(x+y) : clearing rate of virus generated by some specific Immune abilities activated via anti-virus infection treatment without killing liver cells
Model
Specific immuneability
Source: X. Chen, L. Min, et. Al, Leture Notes in Elctrical Engineering 123; Advance in Automation and Robotics, Vol. 2, (2011), 557-566.
The basic virus reproductive The basic virus reproductive numbernumber
71

The model has two equilibrium The model has two equilibrium points:points:
●● QQ1 1 is the infection free equilibrium point, is the infection free equilibrium point,
x
●● QQ2 2 is the persistent infection equilibrium is the persistent infection equilibrium
pointpoint
ModelModel
Theorem If the basic virus reproductive number R0 < 1, then the infection free equilibrium point Q1 is locally stable.
72

下午 09:25:40 73
Fig. 6. Outcomes of the treatment efficacy of the patient. (a) Fig. 6. Outcomes of the treatment efficacy of the patient. (a) Circles: the clinic HBV DNA levels. Solid line: numerical simulation. Circles: the clinic HBV DNA levels. Solid line: numerical simulation. (b) Triangles: the clinic ALT levels. Solid line: numerical simulation. (b) Triangles: the clinic ALT levels. Solid line: numerical simulation.
Numeric SimulationNumeric Simulation
73

3.2 Modelling acute hepatitis B virus infection in chimpanzees
● In a conference presentation,S. F. Wieland report the course of acute HBV infection in seven chimpanzees.
● Doses of the experimental inoculation were 1 to 1010 genome equivalents (GE) of HBV DNA.
● After HBV DNA reached its peaks, the HBV DNA of five chimpanzees was lower than undetectable levels at or before week 39.
● The other two chimpanzees , inoculated with a dosage of 10 GE of HBV DNA, suffered prolonged or persistent infection.
74

Seven chimpanzees were inoculated 1 to 1010 genome equivalents (GE) of HBV DNA. HBV DNA of five chimpanzees was lower than undetectable levels at or before week 39. Two chimpanzees inoculated with a dosage of 10 GE of HBV DNA, suffered prolonged or persistent infection.
S. F. Weiland 13th ISVHLD, March, 20-24, 2009, Washington
HBV DNA peaks
of some animals
with 1-1010 inoculated
HBV are almost
the same!!!
Suppressed HBV loads were relapsed and then suppressed in 4 animals
75

At week 15/11, the HBV DNA/ HBV DNA reached peak. Before week 15/11, the dynamic model is described by (1), After that by (2). The basic virus reproductive number R0’s in (1) and (2) are
Before week 15/11 After week 15/11
Modelling the dynamics of Acute HBV infection in Chimpanzee Ch1603/Chi1616
77
Here λ ≈ 4 ×1010, d = a ≈ 6.3 ×10-3 u = 4.1489.
Other parameters can be determined by R0 . k(t) is changeable exponent function.
Before its’ immune activated, the calculated R0 for Chimpanzees Ch 1603/1616 is 58/77 via minimization --maximum relative error square criterion.
At the ends of observation, R0 = 0.62/1.2346Source X. Chen, L. Min, Y. Zheng, Y. Yang, Y. Ye, Math. And Computers in Simulation, 96 2014: 57-170.
78

79
k1 CTL killing
k2 CTL generating

Outcome of HBV DNA infection in chimpanzee: (a) Ch1603, (b) Ch 1616. Circles: the experimental data, 100 GE/ml is the lower limit of detection; solid line: simulation of the model.
(a)
(b)
80

Ch1603's HBV DNA level has a relapse during weeks 38∼40. In this period k1 = 0. This results guess that some irregular living habits and/or other sudden events (for example catching a cold) made the chimpanzee’s immune ability have disappeared temporarily (k1 = 0) .
Theorem If ≤ 1 then the virus free equilibrium is globally attractive otherwise the virus persistent equilibrium is globally attractive. If R0 < 1 the virus free equilibrium is locally stable, otherwise is unstable.
Chimpanzee Ch 1603’ s = 58. Only 10 Virus GM infection made HBV DNA reach (attract) the peak: virus persistent equilibrium point. After that R 0 < 1, such that HBV DNA attract to virus free equilibrium point.
81
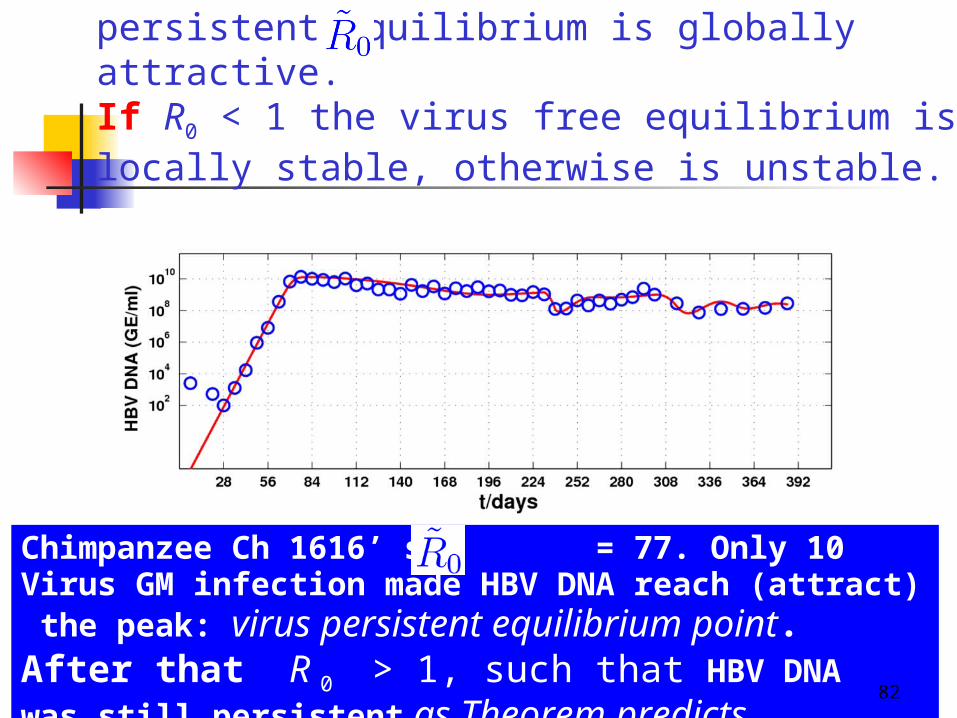
Theorem If ≤ 1 then the virus free equilibrium is globally attractive otherwise the virus persistent equilibrium is globally attractive. If R0 < 1 the virus free equilibrium is locally stable, otherwise is unstable.
Chimpanzee Ch 1616’ s = 77. Only 10 Virus GM infection made HBV DNA reach (attract) the peak: virus persistent equilibrium point. After that R 0 > 1, such that HBV DNA was still persistent as Theorem predicts.
82

An An HIV Indection Model
basic reproductive number R0= λak1/d1d3(d2+p) Dependent on the total number of CD4+ T cells.Source: P.K. Srivastava and P.Chandra, Nonlinear Analysis:
RealWorld Applications, vol. 11, no. 2, pp. 612–618,2010.
3.3 Modeling HIV Infection and Anti-Virus 3.3 Modeling HIV Infection and Anti-Virus Infection TherapyInfection Therapy3.3 Modeling HIV Infection and Anti-Virus 3.3 Modeling HIV Infection and Anti-Virus Infection TherapyInfection Therapy
(4.1)
83
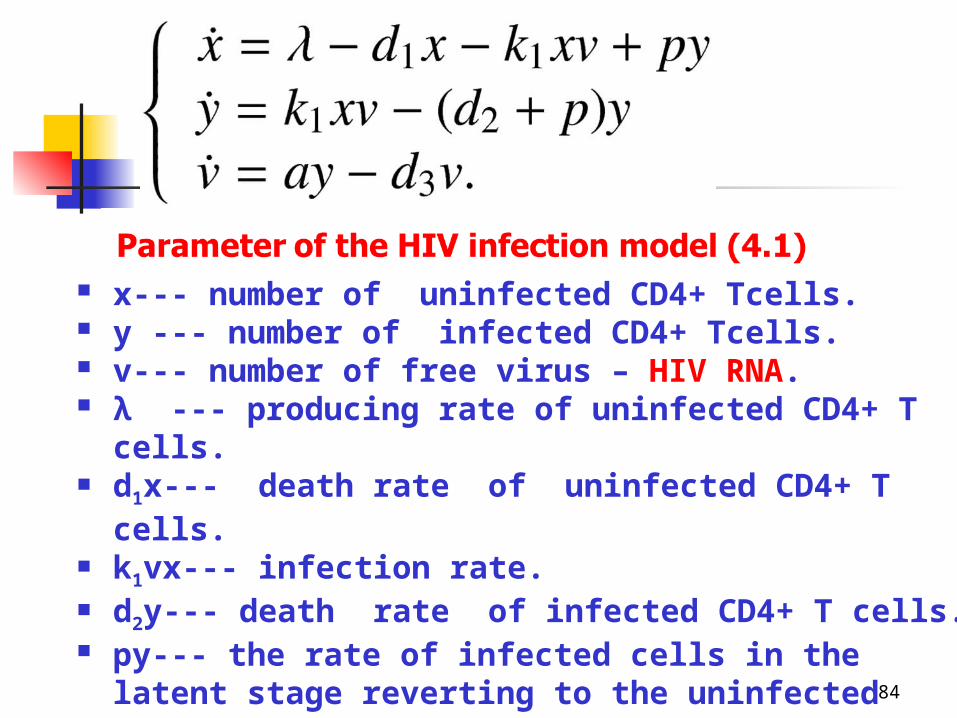
x--- number of uninfected CD4+ Tcells. y --- number of infected CD4+ Tcells. v--- number of free virus – HIV RNA. λ --- producing rate of uninfected CD4+ T
cells. d1x--- death rate of uninfected CD4+ T cells. k1vx--- infection rate. d2y--- death rate of infected CD4+ T cells. py--- the rate of infected cells in the latent
stage reverting to the uninfected class ay--- producing rate of free virus. d3v--- death rate of free virus.
84
virus free steady-state
Persistent virus infection steady-state
They have proved that if R0<1, the infection-
free steady state of (4.1) is globally
attractive; if R0>1, the endemic steady state
of (4.1) is globally attractive.85
● Similar to the case in Nowak et al.’ s basic virus
infection Model. The basic reproductive number
R0= λak1/d1d3(d2+p)
implies
● More CD4+T cells an individual has , more easily
he is infected.
● We introduce an amended model as follows86

Amended
HIV Infection Model/Anti-HIV Infection Therapy
basic reproductive number R0= ak1/d3(d2+p) R0= (1 – m)(1 – n) ak1/d3(d2+p)
Independent on the total number of CD4+ T cells.
Source: Q. Sun, L. Min, Computational and Mathematical Methods in Medicine, vol.2014.
(4.2)
87

virus free steady-state
Persistent virus infection steady-state
88

Source: L Min, Y Su, Y Kuang, Rocky Mountain J. Math. 8(5):1573-1585, 2008.
Y Zheng, L Min, Y. Ji, et al., J. Systems Science and Complexity. 23: 1221–1230,
Theorem 1 If R0 < 1. Then Q1 is globally attractive.
This means: an infected individual with R0< 1 will recover eventually even infected a large amount of HIV.
Theorem 2 If R0 > 1. Then Q2 is globally attractive.
This means: an infected individual with R0> 1 will be persistent infection even infected only one HIV.
89

●Two group (Nos. 15/13) HIV patients’ data selected from Clinical Trial Datasets GART Study are used for simulations.
●Both group patients received the same protease inhibitors: ritonavir and saquinavir. Additionally, Group I received nucleoside reverse transcriptase inhibitors (NRTI): strvudine. Group II received NRTI: strvudine and dideoxyinosine.
Numeric Simulation
Source: Clinical Trial Datasets GART Study, http://hivdb.stanford.edu/pages/clinicalStudyData/GART.html. 90
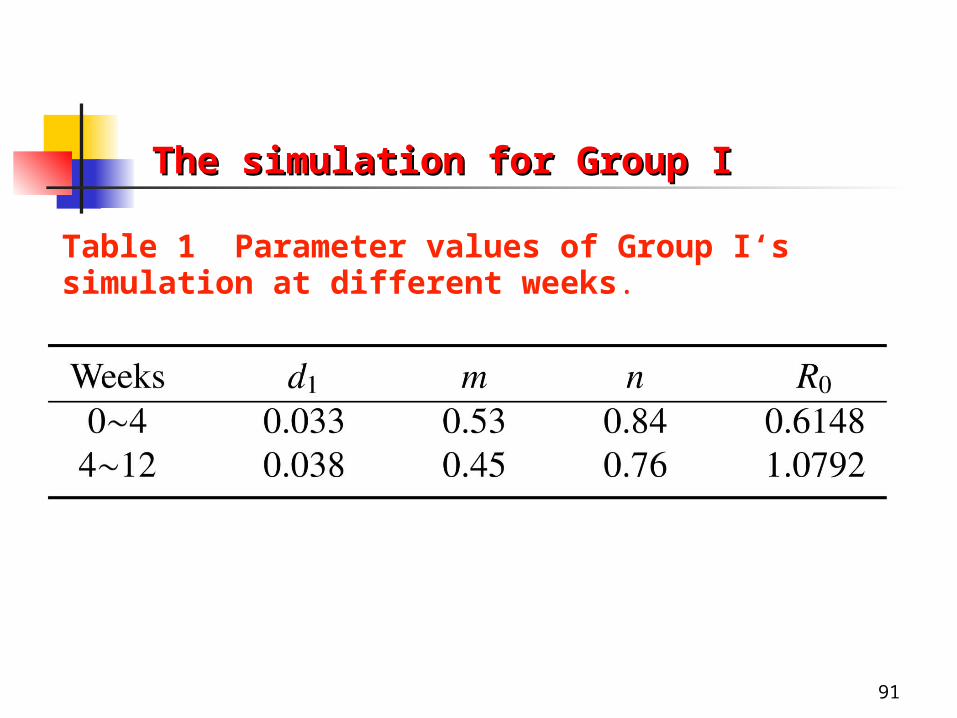
The simulation for Group IThe simulation for Group I
Table 1 Parameter values of Group I‘s simulation at different weeks.
91

Fig. 4.1: Solid lines: the dynamic simulations of the model (4.2). Circles: the clinical data. (a) Mean uninfected CD4+ T cell counts, (b) mean HIV RNA levels
92

Fig. 4.2: The long-term prediction for the treatment efficacy of Group I.
93
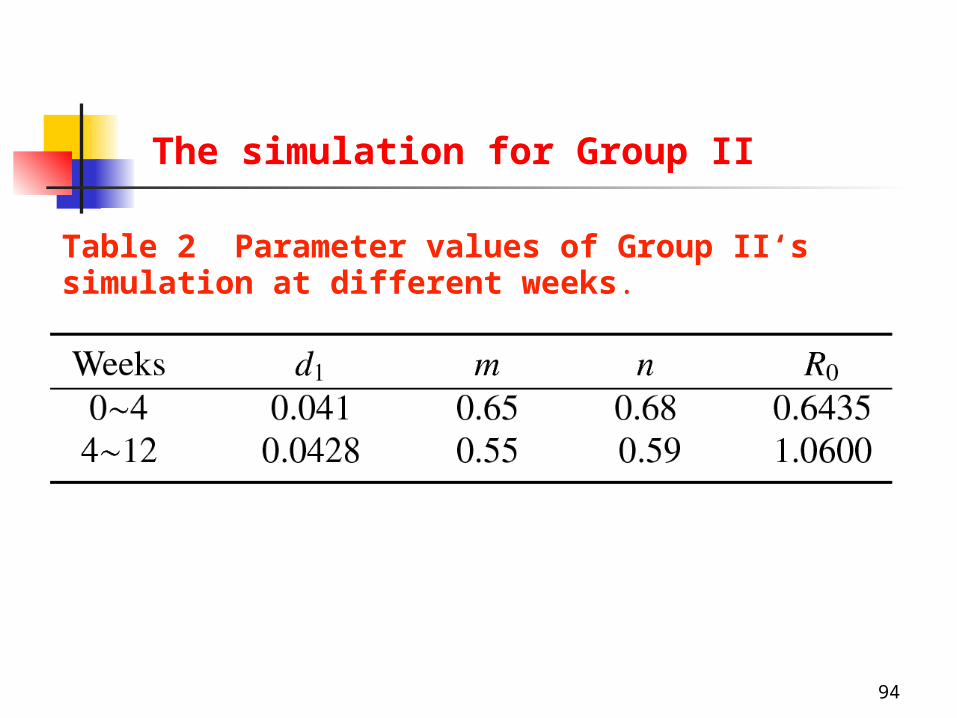
The simulation for Group II
Table 2 Parameter values of Group II‘s simulation at different weeks.
94

Fig. 4.3: Solid lines: the dynamic simulations of the model (4.2). Circles: the clinical data. (a) Mean uninfected CD4+ T cell counts, (b) mean HIV RNA levels.
95

Fig. 4.4: The long-term prediction for the treatment efficacy of Group I.
96
Simulation Results & Discussion
● The numerical simulation results have shown that the first 4 weeks' treatments made the two group patients’ R0’s reduced to be less than one as those shown in Tables 1 and 2.
● After the two periods, drug resistance made the two groups’ R0’s be larger than one as those shown in Tables 1 and 2. As a result, two group patients' mean HIV RNA levels both raised slowly.
● The results interpret why patients' mean CD4+ T cell counts raised and mean HIV RNA levels declined rapidly in the first two periods, but contrary in the following weeks.
97

● Three HIV infected patients (a Berlin Man and two Kenya Men) may be cured via bone marrow transplants.
● Hence we can postulate that most individuals who are similar to the three bone marrow donators will not be infected by HIV.
● They either have R0 < 1 or can produce specific HIV CTL to kill all infected CD4+ T cells like the case of HBV infection. So that they can recover automatically
● The fact has not been recognized since AIDS has been discovered in 1983.http://articles.latimes.com/2012/jul/27/news/la-heb-hiv-cure-aids-meeting-20120727.http://www.africareview.com/Special-Reports/After-Berlin-Man–two-reported-cured-of-HIV-in-Kenya/-/979182/1843388/-/3saq6o/-/index.html.n[
98
Simulation Results & Discussion

99
3.4 Modelling Epidemic Spreading
● Dynamic behavior of the susceptible-infected-susceptible (SIS) model and the susceptible-infected-recovered (SIR) model have been widely studied on epidemic spreading.
● A recent paper introduces a SIRS homogenous network model with vaccinated population, considering different death rates for susceptible individuals and infected individuals.Source: Q. Huang, L. Min, X. Chen, Mathematical Methods in the Applied Science, DOI:10.1002/mma.3048, Dec. 2013 on line.
100
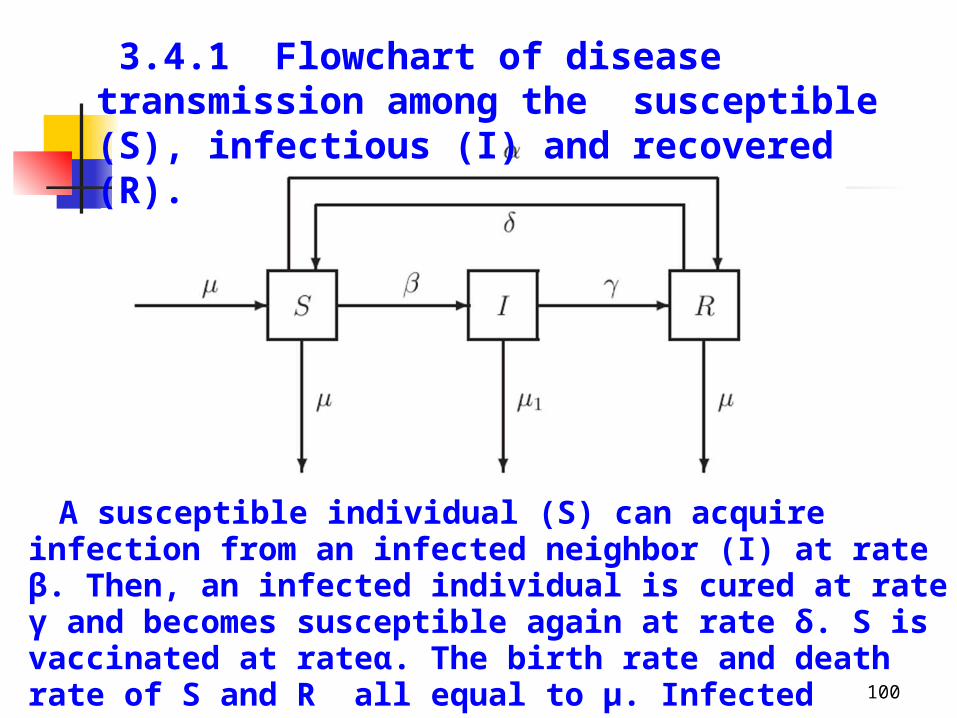
3.4.1 Flowchart of disease transmission among the susceptible (S), infectious (I) and recovered (R).
A susceptible individual (S) can acquire infection from an infected neighbor (I) at rate β. Then, an infected individual is cured at rate γ and becomes susceptible again at rate δ. S is vaccinated at rateα. The birth rate and death rate of S and R all equal to μ. Infected individual die a rate μ1˛

3.4.2 SIRS model on homogenous networks
1
(t)(t) (t) (t) ( ) (t)
(t)(t) (t) ( ) (t)
(t)(t) ( ) (t) (t)
dSk S I R S
dtdI
k S I Idt
dRI R S
dt
1(t) (t) (t) 1S I R
Here <k> is the average value of ki ’s , ki is the edge numbers of the nods in the networks.
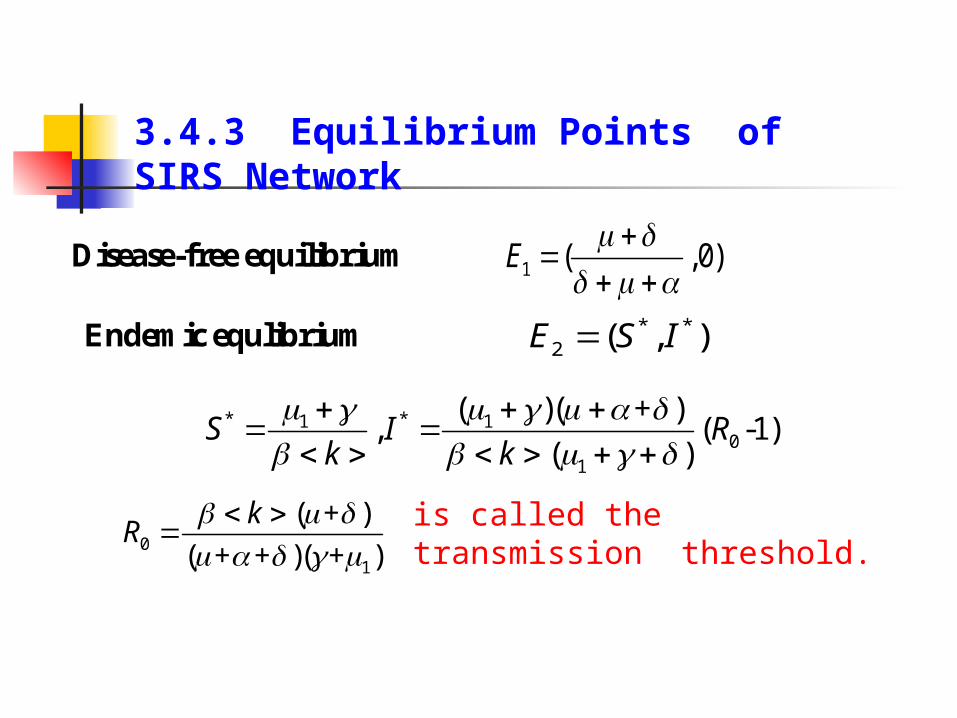
3.4.3 Equilibrium Points of SIRS Network
is called the transmission threshold.
1 ( ,0)E
Disease-free equilibrium
* *2 ( , )E S IEndemic equlibrium
* *1 10
1
( )( + ), ( -1)
( )S I R
k k
01
( + )
( + + )( + )
kR

3.4.4 Global asymptomatically stability of equilibria
Theorem 1. If , then the disease-free equilibrium is globally asymptotically stable.
0 1R 1E
Theorem 2. If , then the endemic equilibrium is globally asymptotically stable.
0 1R 2E
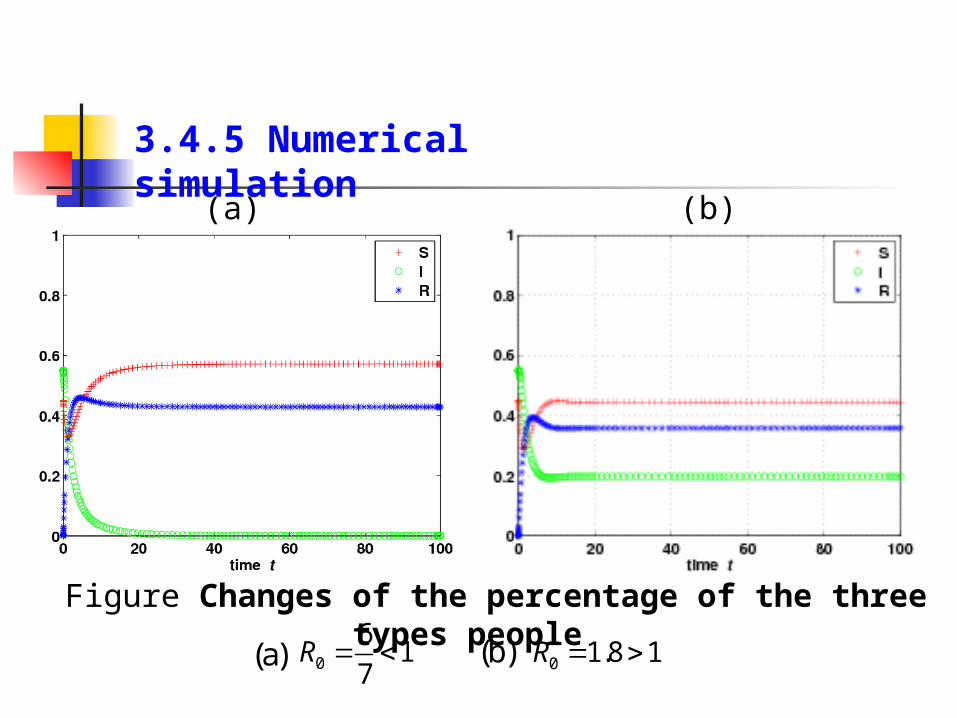
Figure Changes of the percentage of the three types people
3.4.5 Numerical simulation
(a) (b)
0
61
7R 0 1.8 1R (a) (b)

3.4.5. Discussions
01
R1 /
k
An equivalent representation of the transmission threshold R0 of this model is
Theorems 1 and 2 suggest that reducing contact rate <k>, high percentage (large α) of vaccinated population and high death rate (large μ1) of infected population are important factors to make epidemic diseases disappear (R0 < 1).Hence we provide theoretical interpretations for the rationality of the current strategy for epidemic spreading.

4. Conclusions4. Conclusions4. Conclusions4. Conclusions
I Individuals have no any symptoms and can recover automatically even if infected with a large amount of virus if their virus reproductive numbers R0 < 1.
II.Individuals have no any symptoms and become persistent infections even if infected with micro scale (may just one) virus if their virus reproductive numbers R0 > 1
III. Individuals have acute infection symptoms and can recover automatically even if infected with a large amount of virus if their virus reproductive numbers R0 < 1.
IV. Individuals have acute infection symptoms and become persistent infections even if infected with micro scale (may just one) virus if thei virus reproductive numbers R0 > 1.
Human infected with virus can be divided into four groups:
106
4. Conclusions4. Conclusions4. Conclusions4. Conclusions
综上所述我们提出假说(陈晓 , 闵乐泉 , 郑宇等 , 计算机工程与应用 , 48(24) (2012): 20-27 ):群体受病毒感染后可以分为 4 类:
(1) 基本感染系数 R0<1 的群体, 即使受大量病毒感染也不会发病且能自愈;
(2) R0>1 的群体,受微量病毒感染也会持续带毒但不会发病 .
(3) 具有免疫响应 R0<1 的群体, 受大量病毒感染会发病但能自愈 .
(4) 具有免疫响应 R0>1 的群体,受微量病毒感染也会持续带毒且发病 ( 包括死亡 ).
107
Why are there unknown reasons infections?
Why do some virus infected people have recovered without therapy?
Why do some people appear very sensitive to some viruses?
Why do some anti-HBV/HIV infection therapy patients’ serum viruses have relapsed , and become worse after stopping treatment ?
The I & II kind individuals infect secretly the III & IV kind individuals
Because they belong to the I & III kind individuals.
Because they belong to the II & IV kind individuals.
108
Because treatment cannot activate or make patient keep activated immune abilities. So that one virus hided in vivo may make patients’ virus load rebound. Particularly, some activated function preventing infected cells to be killed by CTL do not disappear immediately after stopping treatment, which may make patients’ virus levels higher and outcomes worse.

Why do wild animals without any prevention have hardly become extinct by attacks of various infectious diseases?
Why do domestic animals more easily die by attacks of infectious diseases?
Why did Influenza during 1918-1919 killed nearly 50 million people, and no similar cases appear now day?
109
Because million years biological evolutions may make wild animal populations’ basic reproduction number R0 < 1 or transmission threshold R0 less than one or slightly larger than one.
Because dense living circumstances and no natural living ways may make domestic animal populations have larger <k> and β than wild animals
Because many people lived in that period had basic influenza virus reproductive number R0's which were larger than one. However, most modern people's various basic virus reproductive R0's are less than one because much better living conditions and/or biological evolution. So that over 5 hundred human infected viruses have only infected small part of human beings.

When an epidemic disease is coming, decreasing contact opportunities (reducing <k>) and preventing old people and children (they may have large β’s) may be the most effective approaches to against epidemics.
Consequently, human beings do not need to fear spreadings of new epidemics.

该假说可以对 HBV 感染、禽流感、传染性非典型肺炎 (SARS) 感染等流行病中出现的无明显传染源的病毒感染现象作出解释:(1) 受病毒感染后无症状的人群造了对易感人群的隐性感染 . 野生动物群体在毫无防护的情况下很少被病毒灭绝,是因为经过千百万年的生物进化使得各类群体中大部分成员对各类病毒的基本病毒复制数R0均小于 1.
(2) 家养动物群体比野动物群体更容易遭受病毒的侵袭是人为的饲养环境破坏了动物自身的生长规律 .
(3) 对于人类情况也是类似的 . 我们应该尽力地使人类的生存、生活和工作环境符合人类生存的自然规律,就可做到百毒不侵、延年益寿, (4) 新病毒对人类的威胁也是有限的 . Weiland 关于黑猩猩乙肝病毒急性感染的实验报道,可看成是对我们假说的 有力支持 . 111
Our research suggest:
(1) Current anti-HBV/HIV infection treatments should be very efficient if no virus mutation or/and drug resistance appear.
(2) Suddenly stopping anti-virus therapy may be dangerous for some patients.
(3) Medicines which are able to activate efficiently patients’ specific virus immune functions are needed.
(4) The tests for patients’ specific CTL are needed both for clinic practice and theoretical researches.
(5) More clinic and experimental data are needed in aim to set up more reasonable models.
112
Thank You For Attentions
113