unusual presentation of a cervical pseudomeningocele: a case report and review of the literature
TRANSCRIPT

3
3
3
3
3
4
4
4
J6
Ocflrmpcvnpcifepct
R
t
S
S
p
p
6
©
0
d
556 UNUSUAL CERVICAL PSEUDOMENINGOCELE PRESENTATION
5. Hedner T, Samuelsson O, Lunde H, et al: Angio-oedema inrelation to treatment with angiotensin converting enzyme in-hibitors. BMJ 304:941, 1992
6. Sadeghi N, Panje WR: Life-threatening perioperative angio-edema related to angiotensin-converting enzyme inhibitor ther-apy. J Otolaryngol 28:354, 1999
7. Kyrmizakis DE, Papadakis CE, Fountoulakis EJ, et al: Tongueangioedema after long-term use of ACE inhibitors. Am J Oto-laryngol 19:394, 1998
8. Mchaourab A, Sarantopoulos C, Stowe DF: Airway obstructiondue to late-onset angioneurotic edema from angiotensin-con-
verting enzyme inhibition. Can J Anaesth 46:975, 1999Scott Tate, DDS, MS,* Richard A. Rak, MD,
R
wcoHiatpmcrrcu
lqwdonTd
siTsdu
wistpoi:10.1016/j.joms.2004.07.024
9. Guo X, Dick L: Late onset angiotensin-converting enzyme in-duced angioedema: Case report and review of the literature. JOkla State Med Assoc 92:71, 1999
0. Carr AA, Prisant LM: Losartan: First of a new class of angio-tensin antagonists for the management of hypertension.J Clin Pharmacol 36:3, 1996
1. Chiu AG, Krowiak EJ, Deeb ZE: Angioedema associated withangiotensin II receptor antagonists: Challenging our knowledge ofangioedema and its etiology. Laryngoscope 111:1729, 2001
2. Abdi R, Dong VM, Lee CJ, et al: Angiotensin II receptorblocker-associated angioedema: On the heels of ACE inhib-
itor angioedema. Pharmacotherapy 22:1173, 2002Oral Maxillofac Surg3:556–559, 2005
Unusual Presentation of a CervicalPseudomeningocele: A Case Report
and Review of the Literature
† and Jonathan S. Bailey, DMD, MD‡ral and maxillofacial surgeons are commonlyalled on to manage patients with cerebrospinaluid (CSF) leaks, which present as otorrhea orhinorrhea, secondary to craniomaxillofacial trau-a.1,2 We present an unusual case of a CSF leakresenting as an anterior cervical pseudomeningo-ele. Review of the literature revealed only 1 pre-ious case report of an anterior cervical pseudome-ingocele.3 Eight additional cases with leaksresenting in the retropharyngeal space, posteriorervical subgaleal space, and spinal canal weredentified. Previously reported treatment optionsor cervical pseudomeningocele include surgicalxcision or repair, lumboperitoneal or ventriculo-eritoneal shunting, and lumbar drainage. Identifi-ation and treatment of this problem are imperativeo prevent associated neurologic decline.
eceived from the Carle Foundation Hospital and Clinic Associa-
ion, Urbana, IL.
*Formerly, Chief Resident, Division of Oral and Maxillofacial
urgery.
†Assistant Clinical Professor, Division of Neurosurgery.
‡Assistant Clinical Professor, Division of Oral and Maxillofacial
urgery.
Address correspondence and reprint requests to Dr Bailey: De-
artment of Oral and Maxillofacial Surgery, Carle Foundation Hos-
ital and Clinic Association, 602 W University Ave, Urbana, IL
1801; e-mail: [email protected]
2005 American Association of Oral and Maxillofacial Surgeons
278-2391/05/6304-0021$30.00/0
eport of a Case
The patient was a 26-year-old morbidly obese womanho was the unrestrained driver involved in a motor vehi-
le accident on April 3, 2002. She had been stabilized at anutside hospital and was transferred to Carle Foundationospital (CFH) for further evaluation and treatment. Her
njuries included C6-7 fracture dislocation with quadriplegiand bilateral pulmonary contusions. Her past medical his-ory was significant for morbid obesity and asthma. Theatient was admitted to the intensive care unit and initiallyaintained on biphasic positive airway pressure but hyper-
arbia and hypoxia developed. She was intubated for respi-atory failure. On April 5, 2002, she underwent C6-7 ante-ior cervical discectomy and anterior arthrodesis with iliacrest allograft. On exposure of the anterior vertebral col-mn, a CSF collection and leak was noted.Postoperatively, the patient was weaned from the venti-
ator and extubated on April 15, 2002. The patient subse-uently became bradycardic and progressed to asystole. Sheas emergently reintubated. The resuscitative efforts wereifficult secondary to her morbid obesity and the presencef the cervical collar. After stabilization, a firm swelling wasoted in the right neck underlying the cervical fusion site.he neurosurgery service was notified, and the clinicaliagnosis of a postoperative hematoma was made.The Division of Oral and Maxillofacial Surgery was con-
ulted for tracheostomy due to respiratory failure. On phys-cal examination, the patient’s neck was short and obese.he previous surgical site was firm to palpation but hemo-tatic. In consultation with the neurosurgery service, theecision was made to proceed with tracheostomy and evac-ation of the hematoma.In the operating room, a horizontal suprasternal incisionas marked out 2 fingerbreadths above the sternal notch,
nferior to the previous cervical fusion incision. The inci-ion was made through the skin and subcutaneous tissue. Ashe platysma was incised, a significant leak of clear fluid,
resumably CSF, was expressed through the wound. The
wiwd
flc1pAdoewaprdoppctfcrwti
D
c
rCtosot
ivrEgsor
dfCmatichpeC
Fccu
FaLip
Ts
TATE, RAK, AND BAILEY 557
ound was packed. The neurosurgeon was notified andnspected the wound. The decision was made to close the
ound and plan to observe for reaccumulation and possibleecompression if indicated.Magnetic resonance imaging shows a 4.5 � 3.0 � 3.0-cm
uid collection, consistent with a pseudomeningocele, lo-ated anterior to the lower cervical spine C6-7 region (Figs-3). Despite several attempts at percutaneous aspiration,erformed under sterile conditions, the CSF reaccumulated.n attempt to place a lumbar drain was unsuccessful due toifficulty positioning the patient secondary to her morbidbesity, cervical spine injury, and the presence of the oralndotracheal tube. A second attempt at lumbar punctureas performed but was again unsuccessful. On the third
ttempt, with fluoroscopic guidance, a lumbar drain waslaced. In addition, 20 mL of CSF accumulation was aspi-ated from her anterior cervical pseudomeningocele. Therain output was 25 mL on day 1, 12 mL on day 2, and 5 mLn day 3. The lumbar drain was removed 3 days afterlacement. Five days after lumbar drain placement, theatient underwent tracheostomy by the oral and maxillofa-ial surgery service without complication. One week afterhe tracheostomy, the tracheostomy tube was changed to aenestrated style and no CSF leakage was noted. Repeatomputed tomography scan of the cervical spine showedesolution of the pseudomeningocele. During the next 3eeks, the tracheostomy tube was downsized and the pa-
ient was transferred to an out-of-house rehabilitation facil-ty for the remainder of her care and recovery.
iscussion
Oral and maxillofacial surgeons are commonly
IGURE 1. Sagittal magnetic resonance image of the cervical spinefter cervical spine fusion. Numbers indicate cervical spine vertebrae.arge white arrow shows pseudomeningocele, with small white arrowndicating upper aerodigestive tract. Spinal cord edema is also notedosterior to traumatized segments.
ate, Rak, and Bailey. Unusual Cervical Pseudomeningocele Pre-entation. J Oral Maxillofac Surg 2005.
alled on to manage patients with CSF otorrhea orTs
hinorrhea as a result of craniomaxillofacial trauma.1,2
SF otorrhea and rhinorrhea are most commonlyreated with a multidisciplinary approach. Treatmentptions include observation and conservative mea-ures, lumbar drain placement, and reduction of crani-maxillofacial fractures including extracranial or in-racranial dural repair when indicated.1-9
We present an unusual case of a CSF leak present-ng as an anterior cervical pseudomeningocele. Re-iew of the literature revealed only 1 previous caseeport of an anterior cervical pseudomeningocele.3
ight additional cases presenting in the retropharyn-eal space, posterior cervical subgaleal space, andpinal canal were identified4,10-16 (Table 1). All previ-us cases were reported in the otolaryngology, neu-osurgery, or anesthesia literature.
As in the more typical presentation of a CSF leak,evelopment of cervical pseudomeningocele resultsrom a disruption in the integrity of the dura allowingSF to leak into low-pressure regions. The most com-on etiology is atlanto-occipital dislocation second-
ry to trauma.10,12,13,15 This injury results in a tear ofhe dura at the craniocervical junction.15,16 Thesenjuries have been described after motor vehicle ac-idents and may occur in combination with a closedead injury, hydrocephalus, and elevated intracranialressure.10,13,15 The presence of hydrocephalus andlevated intracranial pressure may lead to diversion ofSF through the traumatic defect.15
IGURE 2. Sagittal magnetic resonance image of cervical spine afterervical spine fusion. Large white arrow shows pseudomeningoceleommunicating with spinal canal. Small white arrow indicates thepper aerodigestive tract.
ate, Rak, and Bailey. Unusual Cervical Pseudomeningocele Pre-entation. J Oral Maxillofac Surg 2005.
prsfhtapagTr
ig1spwp
ctgcotmdlcsd
ppircwHrpmrrdvor
fiS
Fccap
Ts
CSLWHN
NG
T
558 UNUSUAL CERVICAL PSEUDOMENINGOCELE PRESENTATION
Cervical pseudomeningocele has also been re-orted after cervical spine surgery.3,4,14 Nair et al3
eported the case of a 51-year-old woman who pre-ented 2 months after anterior cervical fusion per-ormed for cervical myelopathy and radiculopathy. Ater initial surgery, a small tear in the dura was iden-ified and managed with bovine pericardium andcrylic glue. One day after discharge, the patient re-resented with pain and swelling at the operative sitend dysphagia. A clinical diagnosis of pseudomenin-ocele was made and managed with a lumbar drain.he swelling promptly resolved and the drain wasemoved. Two months later, she again presented with
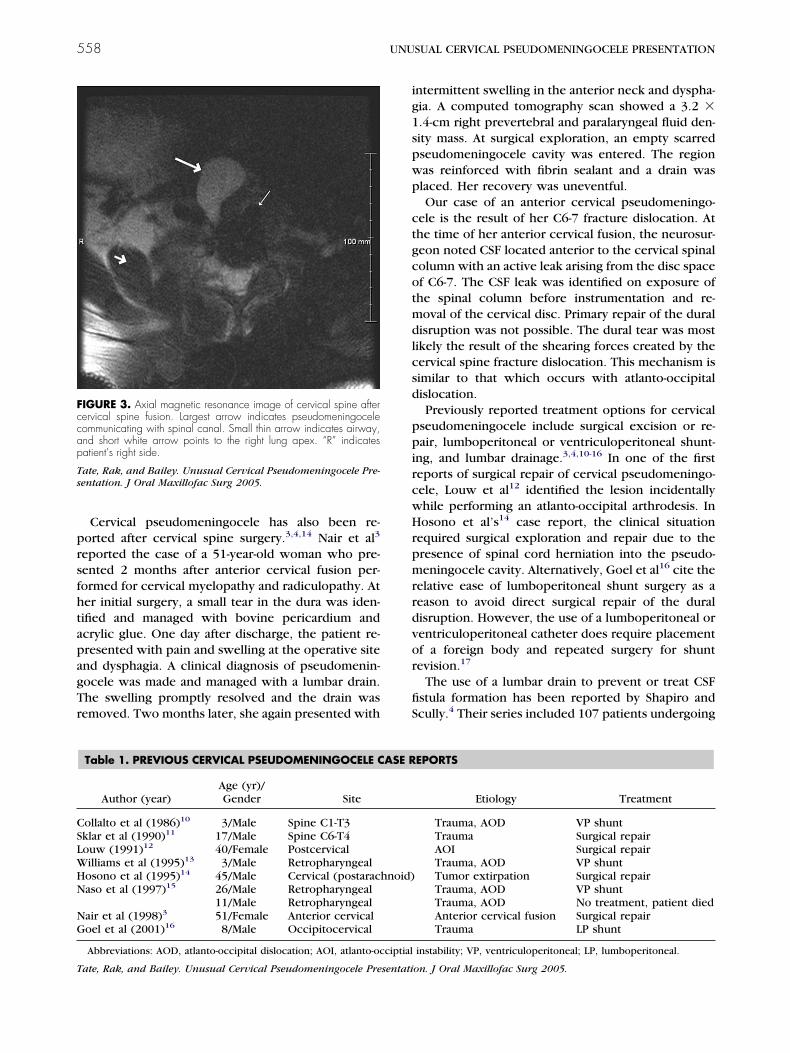
IGURE 3. Axial magnetic resonance image of cervical spine afterervical spine fusion. Largest arrow indicates pseudomeningoceleommunicating with spinal canal. Small thin arrow indicates airway,nd short white arrow points to the right lung apex. “R” indicatesatient’s right side.
ate, Rak, and Bailey. Unusual Cervical Pseudomeningocele Pre-entation. J Oral Maxillofac Surg 2005.
Table 1. PREVIOUS CERVICAL PSEUDOMENINGOCELE C
Author (year)Age (yr)/Gender Site
ollalto et al (1986)10 3/Male Spine C1-T3klar et al (1990)11 17/Male Spine C6-T4ouw (1991)12 40/Female Postcervicalilliams et al (1995)13 3/Male Retropharyngealosono et al (1995)14 45/Male Cervical (postaracaso et al (1997)15 26/Male Retropharyngeal
11/Male Retropharyngealair et al (1998)3 51/Female Anterior cervicaloel et al (2001)16 8/Male Occipitocervical
Abbreviations: AOD, atlanto-occipital dislocation; AOI, atlanto-oc
ate, Rak, and Bailey. Unusual Cervical Pseudomeningocele Presentati
ntermittent swelling in the anterior neck and dyspha-ia. A computed tomography scan showed a 3.2 �.4-cm right prevertebral and paralaryngeal fluid den-ity mass. At surgical exploration, an empty scarredseudomeningocele cavity was entered. The regionas reinforced with fibrin sealant and a drain waslaced. Her recovery was uneventful.Our case of an anterior cervical pseudomeningo-
ele is the result of her C6-7 fracture dislocation. Athe time of her anterior cervical fusion, the neurosur-eon noted CSF located anterior to the cervical spinalolumn with an active leak arising from the disc spacef C6-7. The CSF leak was identified on exposure ofhe spinal column before instrumentation and re-oval of the cervical disc. Primary repair of the dural
isruption was not possible. The dural tear was mostikely the result of the shearing forces created by theervical spine fracture dislocation. This mechanism isimilar to that which occurs with atlanto-occipitalislocation.Previously reported treatment options for cervical
seudomeningocele include surgical excision or re-air, lumboperitoneal or ventriculoperitoneal shunt-
ng, and lumbar drainage.3,4,10-16 In one of the firsteports of surgical repair of cervical pseudomeningo-ele, Louw et al12 identified the lesion incidentallyhile performing an atlanto-occipital arthrodesis. Inosono et al’s14 case report, the clinical situation
equired surgical exploration and repair due to theresence of spinal cord herniation into the pseudo-eningocele cavity. Alternatively, Goel et al16 cite the
elative ease of lumboperitoneal shunt surgery as aeason to avoid direct surgical repair of the duralisruption. However, the use of a lumboperitoneal orentriculoperitoneal catheter does require placementf a foreign body and repeated surgery for shuntevision.17
The use of a lumbar drain to prevent or treat CSFstula formation has been reported by Shapiro andcully.4 Their series included 107 patients undergoing
EPORTS
Etiology Treatment
Trauma, AOD VP shuntTrauma Surgical repairAOI Surgical repairTrauma, AOD VP shuntTumor extirpation Surgical repairTrauma, AOD VP shuntTrauma, AOD No treatment, patient diedAnterior cervical fusion Surgical repairTrauma LP shunt
instability; VP, ventriculoperitoneal; LP, lumboperitoneal.
ASE R
hnoid)
ciptial
on. J Oral Maxillofac Surg 2005.

ctotetp(
scoTmNwvronpmrwTatpl
mbduvaieti
qTtlwpwtiapdpd
ccvetct
tmecfaprw
R
1
1
1
1
1
1
1
TATE, RAK, AND BAILEY 559
ranial surgery or spinal surgery or who experiencedraumatic CSF rhinorrhea or otorrhea. One hundredne patients (94%) were successfully managed withhis technique. Specifically, the authors make refer-nce to 4 patients with cervical pseudomeningoceleshat were treated successfully in this manner. Com-lications included transient nerve root irritation14%), overdrainage (5%), and spinal headache (1%).
The surgeon who treats patients with cranial andpinal injuries should be familiar with this unusuallinical problem. Prompt identification and treatmentf a cervical pseudomeningocele are mandatory.hese lesions often present in a delayed manner anday be associated with significant neurologic decline.aso et al15 reported the case of a 26-year-old manith atlanto-occipital dislocation following a motor
ehicle accident. At 3.5 months into the patient’secovery, he developed significant neurologic deteri-ration that included headache, nausea, emesis, cog-itive decline, and progressive dysphagia requiringercutaneous endoscopic gastrostomy tube place-ent and tracheostomy. Magnetic resonance imaging
evealed the retropharyngeal pseudomeningocele,hich was treated by ventriculoperitoneal shunting.he patient’s neurologic function improved immedi-tely. The patient was decannulated and the gastros-omy tube was removed. At the time of discharge, theatient was able to perform the activities of daily
iving and was able to ambulate with a walker.Hosono et al14 reported a case of a cervical pseudo-eningocele occurring 14 years after removal of a
enign spinal cord tumor. In this instance, the patienteveloped gait disturbance and spasticity of his rightpper extremity. Magnetic resonance imaging re-ealed a pseudomeningocele posterior to the sub-rachnoid space with herniation of the spinal cordnto the cyst cavity. Following surgical exploration,xcision of the pseudomeningocele, and reduction ofhe herniated spinal cord, the patient’s neurologicmpairments resolved.
In our case, the patient was morbidly obese anduadriplegic and had bilateral pulmonary contusions.racheostomy was required to improve pulmonary
oilet and allow for a slow ventilatory wean. Pro-onged oral intubation would not allow for ventilatory
eaning due to her body habitus and high airwayressures required to ventilate the patient. However,ith the cervical pseudomeningocele located anterior
o the trachea, tracheostomy carried the risk of seed-ng a sterile CSF collection with respiratory flora. Inddition, surgical repair of the dural leak was notossible due to the inaccessible location of the duralisruption. Therefore, the need to decompress theseudomeningocele and allow for healing of the dural
isruption was imperative.1
It was the opinion of the treating services to pro-eed with lumbar drain placement. This was techni-ally difficult due to the patient’s body habitus, cer-ical spine injury, and the presence of thendotracheal tube. The lumbar drain was placed onhe third attempt using fluoroscopic guidance. Theervical pseudomeningocele was decompressed andracheostomy was performed without complication.
No series exists that prospectively or retrospec-ively compares treatment options for the manage-ent of a cervical pseudomeningocele. We offer our
xperience to increase the awareness of this uniquelinical problem. Treatment guidelines cannot be of-ered based on our limited experience. The etiologynd surgical accessibility of the dural disruption, theresence or absence of hydrocephalus, and the neu-ologic status of the patient should be consideredhen deciding on a treatment course.
eferences1. Brandt MT, Jenkins WS, Fattahi TT, et al: Cerebrospinal fluid:
Implications in oral and maxillofacial surgery. J Oral MaxillofacSurg 60:1049, 2002
2. Clemenza JW, Kaltman SI, Diamond DL: Craniofacial traumaand cerebrospinal leakage: A retrospective clinical study. J OralMaxillofac Surg 53:1004, 1995
3. Nair SB, Flood LM, Nath F: An unusual complication of Clo-ward’s procedure presenting to the otolaryngologist. J LaryngolOtol 112:1087, 1998
4. Shapiro SA, Scully T: Closed continuous drainage of cerebro-spinal fluid via a lumbar subarachnoid catheter for treatment orprevention of cranial/spinal cerebrospinal fluid fistula. Neuro-surgery 30:241, 1992
5. McCallum J, Maroon JC, Jannetta PJ: Treatment of postopera-tive cerebrospinal fluid fistulas by subarachnoid drainage.J Neurosurg 42:434, 1975
6. Findler G, Sahar A, Beller AJ: Continuous lumbar drainage ofcerebrospinal fluid in neurosurgical patients. Surg Neurol8:455, 1977
7. Wax MK, Ramadan HH, Ortiz O, et al: Contemporary manage-ment of cerebrospinal fluid rhinorrhea. Otolaryngol Head NeckSurg 116:442, 1997
8. Schmidek HH, Sweet WH, Dagi TF: Operative NeurosurgicalTechniques: Indications, Methods, and Results (4th ed, vol 1).Philadelphia, PA, Saunders, 1998, pp 164-177
9. McCormack B, Cooper PR, Persky M, et al: Extracranial repairof cerebrospinal fluid fistulas: Technique and results in 37patients. Neurosurgery 27:412, 1990
0. Collalto PM, Demuth WW, Schwentker EP, et al: Traumaticatlanto-occipital dislocation. J Bone Joint Surg 68:1106, 1986
1. Sklar EML, Quencer RM, Green BA: Posttraumatic spinalpseudomeningocele: MR and clinical features. AJNR Am J Neu-roradiol 11:1184, 1990
2. Louw JA: Traumatic atlanto-axial pseudomeningocele. S AfrJ Surg 29:26, 1991
3. Williams MJ, Elliot JL, Nichols J: Atlanto-occipital dislocation: Acase report. J Clin Anesth 7:156, 1995
4. Hosono N, Yonenobu K, Ono K: Postoperative cervicalpseudomeningocele with herniation of the spinal cord. Spine20:2147, 1995
5. Naso WB, Cure J, Cuddy BG: Retropharyngeal pseudomenin-gocele after atlanto-occipital dislocation: Report of two cases.Neurosurgery 40:1288, 1997
6. Goel A, Desai KI, Nadkarni TD, et al: An unusual post-traumaticoccipitocervical pseudomeningocele. Surg Neurol 56:62, 2001
7. Hahn YS: Commentary: An unusual post-traumatic occipitocer-vical pseudomeningocele. Surg Neurol 56:65, 2001