uog journal club: poor neonatal acid–base status in term fetuses with low cerebroplacental ratio...
Upload: international-society-of-ultrasound-in-obstetrics-and-gynecology-isuog
Post on 15-Jul-2015
718 views
TRANSCRIPT

UOG Journal Club: February 2015
Poor neonatal acid–base status in term fetuses with low
cerebroplacental ratio
J. Morales-Roselló, A. Khalil, M. Morlando, A. Bhide, A. Papageorghiou
and B. Thilaganathan
Volume 45, Issue 2, Date: February (pages 156–161)
Human fetal growth is constrained below optimal for perinatal
survival
B. Vasak, S.V. Koenen, M.P.H. Koster, C.W.P.M. Hukkelhoven, A. Franx,
M.A. Hanson and G.H.A. Visser
Volume 45, Issue 2, Date: February (pages 162–167)
Journal Club slides prepared by Dr Aly Youssef
(UOG Editor for Trainees)

UOG Journal Club: February 2015
Poor neonatal acid–base status in term fetuses with low
cerebroplacental ratio
J. Morales-Roselló, A. Khalil, M. Morlando, A. Bhide, A. Papageorghiou
and B. Thilaganathan
Volume 45, Issue 2, Date: February (pages 156–161)

Introduction
• Term fetuses with birth weight above the 10th centile are labeled
appropriate for gestational age (AGA)
• Although AGA fetuses are considered to be healthy, it is
accepted that some of them may suffer from placental
insufficiency and fail to reach their genetic growth potential
• A potentially useful approach to detect AGA fetuses at increased
risk of adverse pregnancy outcome is the use of the
cerebroplacental ratio (CPR) to suggest placental insufficiency
and failure to reach their growth potential (FRGP), regardless of
their absolute birth-weight centile
Poor neonatal acid–base status in term fetuses with low cerebroplacental ratioMorales-Roselló et al., UOG 2015

To evaluate to what extent arterial and venous umbilical
blood pH at birth are associated with birth weight
and fetal CPR
Aim of the study
Poor neonatal acid–base status in term fetuses with low cerebroplacental ratioMorales-Roselló et al., UOG 2015
• This was a retrospective cohort study in two tertiary centers, including
singleton term fetuses that underwent an ultrasound scan within 14 days of
delivery.
Methods
• The umbilical (UA) and fetal middle cerebral (MCA) arteries were examined
using color Doppler ultrasound
• CPR was calculated as the ratio between the MCA and UA pulsatility
indices (PI)
• Birth weights were converted into centiles, and CPR values were converted
into multiples of the median (MoM), correcting for gestational age
Poor neonatal acid–base status in term fetuses with low cerebroplacental ratioMorales-Roselló et al., UOG 2015
• A pregnancy with a fetal CPR below 0.6765 MoM was considered more
likely to have placental insufficiency (also labeled as failure to reach growth
potential; FRGP)

• The acid–base status represented by the arterial and venous
umbilical cord pH obtained at birth was correlated with CPR and
birth weight using scattergrams, calculating the correlation
coefficient r² and P-value.
Subsequently, arterial and venous pH were compared between the
subgroups with and without low CPR
• Large for gestational age (LGA) was defined as birth weight > 90th
percentile, small for gestational age (SGA) was defined as birth
weight < 10th percentile and AGA was defined as birth weight
between the 10th and 90th percentiles
Poor neonatal acid–base status in term fetuses with low cerebroplacental ratioMorales-Roselló et al., UOG 2015
Methods

Results: correlation between birth weight and neonatal blood pH
There was a significant
correlation between birth
weight and venous-blood pH
(r2 = 0.005, P < 0.001),
but not between birth weight
and arterial-blood pH
(Figure; r2 = 0.001,
P = 0.180)
Poor neonatal acid–base status in term fetuses with low cerebroplacental ratioMorales-Roselló et al., UOG 2015
Solid lines represent best fit with linear regression; dashed lines are 95% confidence intervals

Results: correlation between CPR and neonatal blood pH
CPR was significantly
correlated with both arterial-
blood and venous-blood
pH (r2 = 0.008, P < 0.0001 and
r2 = 0.01, P < 0.0001,
respectively)
Poor neonatal acid–base status in term fetuses with low cerebroplacental ratioMorales-Roselló et al., UOG 2015
Solid lines represent best fit with linear regression; dashed lines are 95% confidence intervals
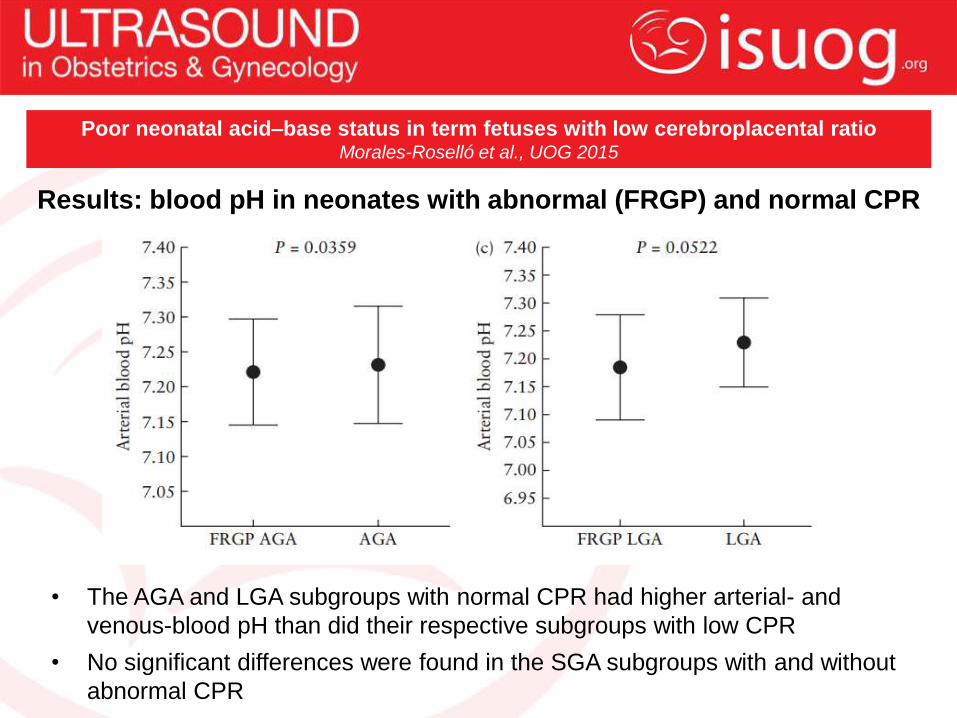
Results: blood pH in neonates with abnormal (FRGP) and normal CPR
• The AGA and LGA subgroups with normal CPR had higher arterial- and
venous-blood pH than did their respective subgroups with low CPR
• No significant differences were found in the SGA subgroups with and without
abnormal CPR
Poor neonatal acid–base status in term fetuses with low cerebroplacental ratioMorales-Roselló et al., UOG 2015

• This study demonstrates that at term, fetal CPR is better correlated with
umbilical cord blood pH than it is with birth weight
• AGA fetuses with low CPR presented with significantly lower neonatal
pH than AGA fetuses with normal CPR
• Identifying fetuses with placental insufficiency near term is challenging,
as the baby has usually already attained a good weight.
• The data of this study support the assertion that CPR may be just as
good at predicting AGA fetuses at risk of compromise as it is at
predicting SGA fetuses at risk
• This finding may be of value in risk assessment for stillbirth at term and
long-term neurodevelopmental disability
Discussion
Poor neonatal acid–base status in term fetuses with low cerebroplacental ratioMorales-Roselló et al., UOG 2015
Weaknesses
• Retrospective design; however this limitation is mitigated to a
certain extent by the size of the population studied and the
prospective data collection of fetal Doppler indices and
umbilical cord blood pH
• Umbilical cord blood pH at birth is likely to be influenced by
multiple maternal characteristics and intrapartum confounders
Poor neonatal acid–base status in term fetuses with low cerebroplacental ratioMorales-Roselló et al., UOG 2015

Discussion points
• How should women at term with AGA fetuses and low CPR be
managed?
• Which cut-off value for CPR should be used to define fetal blood flow
redistribution?
• Should middle cerebral artery and umbilical artery measurements be
performed routinely in women with AGA fetuses?
Future studies are needed to evaluate the performance of the CPR in
AGA fetuses in the prediction of perinatal mortality and neonatal
neurodevelopmental impairment, with the aim of optimizing the timing
of delivery and reducing perinatal complications and long-term
neonatal handicap
Future perspectives
Poor neonatal acid–base status in term fetuses with low cerebroplacental ratioMorales-Roselló et al., UOG 2015

UOG Journal Club: February 2015
Human fetal growth is constrained below optimal
for perinatal survival
B. Vasak, S.V. Koenen, M.P.H. Koster, C.W.P.M. Hukkelhoven,
A. Franx, M.A. Hanson and G.H.A. Visser
Volume 45, Issue 2, Date: February (pages 162–167)
• Use of fetal growth charts assumes that optimal size at birth is at
the 50th birth-weight centile
• However, the interaction between maternal constraints and risks
associated with small and large fetal size at birth may indicate that
this assumption is not valid for perinatal mortality rates
• Indeed, it is believed that human fetal growth is constrained
below its genetic potential in all pregnancies, to a greater or lesser
degree, to match size at birth to maternal physical characteristics
• However, this optimal size assumption has not been examined in
a sufficiently large contemporary population in a high-income setting
to describe this aspect of human biology.
Background
Human fetal growth is constrained below optimal for perinatal survival Vasak et al., UOG 2015

To investigate the distribution and timing of perinatal
mortality and morbidity in relation to birth weight and
gestational age at delivery
Objective
Human fetal growth is constrained below optimal for perinatal survival Vasak et al., UOG 2015
• This was a retrospective population-based cohort study including data
collected from the Netherlands Perinatal Registry on 1 170 127 births that
delivered between 28–43 weeks’ gestation from singleton pregnancies
between 2002–2008
• Children with congenital abnormalities were excluded
• Birth weight was displayed in centile groups
Data analysis
Human fetal growth is constrained below optimal for perinatal survival Vasak et al., UOG 2015
• Distribution of perinatal mortality according to birth weight was studied
• Mortality rates were subdivided in to antepartum, intrapartum and neonatal
death to assess these relationships separately for the different time periods
of occurrence of death
• The relationship between perinatal mortality, birth weight and gestational
age at delivery was studied
Methods

Results
• Among 1 170 534 singleton fetuses included in the study period,
there were 5075 (0.43%) perinatal deaths
• 54% of all perinatal deaths occurred ≥ 37 weeks’ gestation
• 29% of the perniatal deaths occurred in infants with birth weight
< 10th centile, but 64% in infants with a weight between the 10th
and 90th centiles, with a similar distribution at all gestational ages
Human fetal growth is constrained below optimal for perinatal survival Vasak et al., UOG 2015
Human fetal growth is constrained below optimal for perinatal survival Vasak et al., UOG 2015
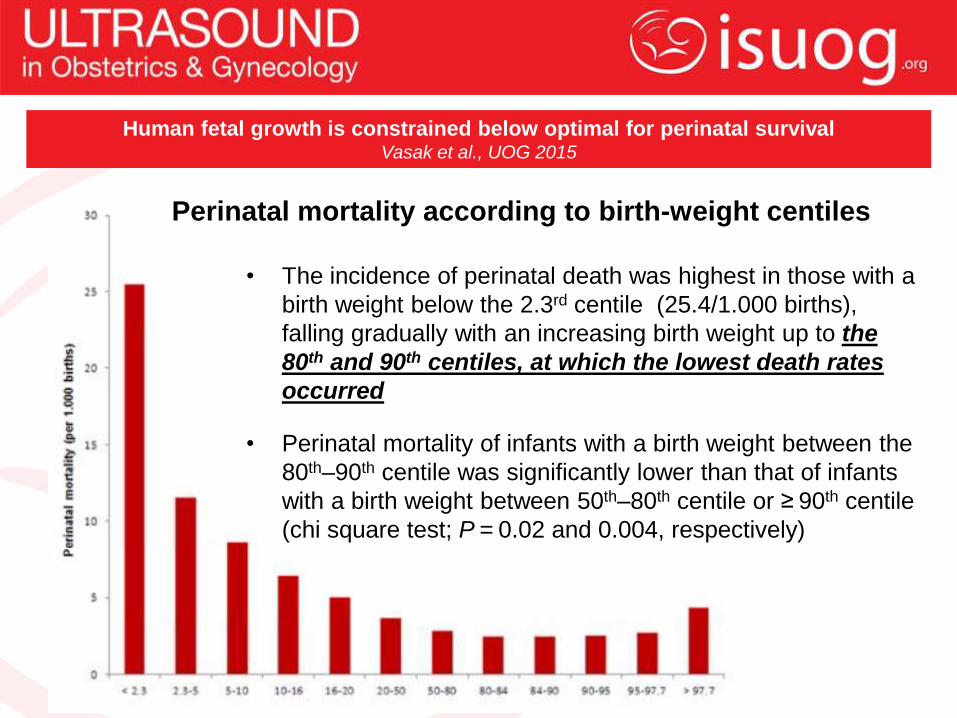
Perinatal mortality according to birth-weight centiles
• The incidence of perinatal death was highest in those with a
birth weight below the 2.3rd centile (25.4/1.000 births),
falling gradually with an increasing birth weight up to the
80th and 90th centiles, at which the lowest death rates
occurred
• Perinatal mortality of infants with a birth weight between the
80th–90th centile was significantly lower than that of infants
with a birth weight between 50th–80th centile or ≥ 90th centile
(chi square test; P = 0.02 and 0.004, respectively)

Results: antepartum, intrapartum and neonatal deaths
• Antepartum deaths accounted for 72% of all perinatal
deaths and were lowest in infants of birth weight
between the 90th and 95th centiles
• Intrapartum and neonatal deaths were lowest between
the 80th and 84th centiles
• The same patterns were found when data were
restricted to infants born ≥ 37 weeks of gestation, or to
those born between 39 and 40 weeks
Human fetal growth is constrained below optimal for perinatal survival Vasak et al., UOG 2015
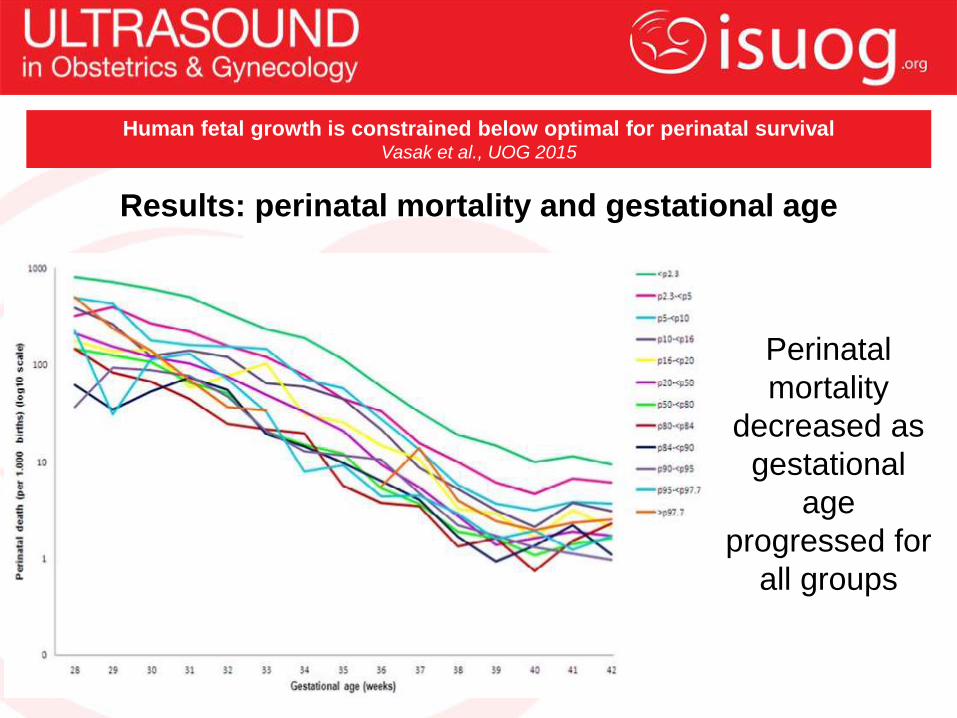
Results: perinatal mortality and gestational age
Perinatal
mortality
decreased as
gestational
age
progressed for
all groups
Human fetal growth is constrained below optimal for perinatal survival Vasak et al., UOG 2015

• This study shows that, from an immediate survival perspective,
optimal fetal growth requires a live birth weight between the 80th to
90th centile
• Median birth weight in the population is by definition substantially
lower, implying that the majority of fetuses exhibit some form of
maternal constraint of growth
• The finding that lowest perinatal mortality and morbidity is not
present in infants with a birth weight around the 50th centile, but at a
much higher centile, raises important issues about human
development
• These findings may represent the adaptations evolved in humans,
in conjunction with large head size and bipedalism, to reduce the
risk of obstructed delivery
Discussion
Human fetal growth is constrained below optimal for perinatal survival Vasak et al., UOG 2015

Limitations
• Lack of information on the cause of death
• Possible inaccuracies in discriminating between antepartum and
intrapartum deaths
• The use of customized growth charts might have refined the data,
but such information is not present in The Netherlands Perinatal
Registry
• Large population size, with data from The Netherlands Perinatal
Registry containing approximately 95% of all births in The
Netherlands
Strengths
Human fetal growth is constrained below optimal for perinatal survival Vasak et al., UOG 2015

Discussion points
• Are the present definitions and centiles accurate for
identifying fetuses with inadequate intrauterine growth?
• Should other instruments (e.g. cerebroplacental ratio)
be integrated routinely in to the assessment of fetal
growth at or near term?
Human fetal growth is constrained below optimal for perinatal survival Vasak et al., UOG 2015