update in women’s health 2014 martina jelley, md, msph, facp university of oklahoma school of...
TRANSCRIPT
Update in Women’s Health 2014
Martina Jelley, MD, MSPH, FACPUniversity of Oklahoma School of
Community Medicine

Get ready!
• Whirlwind tour of important studies published in 2013 and first part of 2014
• Pay attention – this may change your practice!• Summarized from presentations at national
ACP and SGIM meetings earlier this year, with a couple of my additions

Henrietta P Vee
• Ms. Henrietta P. Vee is a 36 year old woman who had her last cervical cancer screening test about 2 years ago. As far as she knows, her tests have always been normal. She has heard that maybe she can be screened less often but is a little nervous about it. What do you tell her about when she should have her next test?
Cervical Cancer Screening
• Dramatic reduction in mortality withroutine cervical cancer screening
• HPV is the causative agent in the majority of cases of cervical cancer
– HPV testing incorporated into new guidelines
• Long latency period for development ofcervical cancer
• Many lesions will regress on their own
Cervical Cancer ScreeningGuidelines
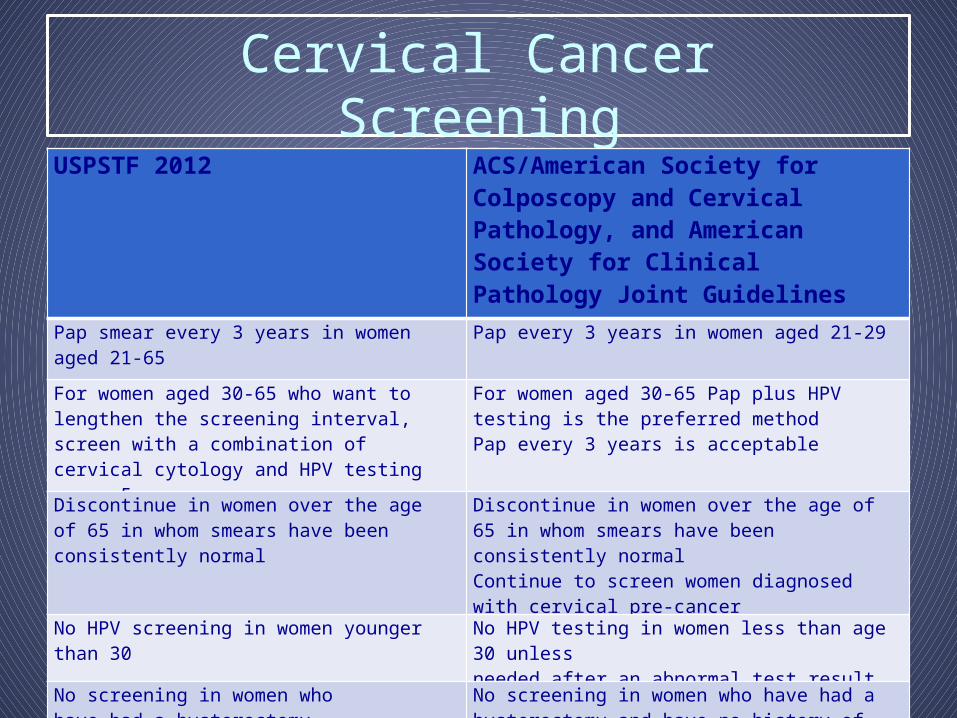
USPSTF 2012 ACS/American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology Joint Guidelines 2012
Pap smear every 3 years in women aged 21-65 Pap every 3 years in women aged 21-29
For women aged 30-65 who want to lengthen the screening interval, screen with a combination of cervical cytology and HPV testing every 5 years
For women aged 30-65 Pap plus HPV testing is the preferred methodPap every 3 years is acceptable
Discontinue in women over the age of 65 in whom smears have been consistently normal
Discontinue in women over the age of 65 in whom smears have been consistently normalContinue to screen women diagnosed with cervical pre-cancer
No HPV screening in women younger than 30 No HPV testing in women less than age 30 unlessneeded after an abnormal test result
No screening in women who have had a hysterectomy
No screening in women who have had a hysterectomy and have no history of cervical cancer or pre-cancer

HPV based screening
• Four RCTs have compared HPV based screening with cytology based screening– Precursors of cancer were the endpoints in all the
trials– Lower CIN3 incidence with HPV testing in all
studies• HPV based screening detects persistent high grade
CIN before cytology, increasing probability of treatment before invasion
• Relative efficacy of HPV based screening vs cytology for prevention of invasive cancer is not known

The News• Efficacy of HPV-based screening for
prevention of invasive cervical cancer: follow- up of four European randomised controlled trials.– Ronco et al. Lancet 2014
• Aim: To evaluate the relative efficacy of HPV- based vs cytology based screening for prevention of invasive cancer in women who undergo regular screening, of modifiers of the relative efficacy and of the duration of protection.
Methods• 176,464 women aged 20-64 assigned to HPV or
cytology based screening in 4 RCTS in 4 countries: Swedescreen, POBASCAM, ARTISTIC and NTCC
• Mean follow-up 6.5 years• – (1,214,415 person-years)
• 107 invasive cervical cancers identified

Results: Rate Ratios• Overall for invasive cervical cancer (HPV vs cytology)
– 0.60 (0.40-0.89)
• Detection of cervical cancer similar in first 2.5 years but lower after that
– 0.79 (0.46-1.36) first 2.5 years
– 0.45 (0.25-0.81) after 2.5 years
• Low rate ratio with negative test at entry
– 0.30 (0.15-0.60)
• Rate ratio lowest in women aged 30-34
– 0.36 (0.14-0.94)

Conclusions
• HPV-based screening provides 60-70% greater protection against invasive cervical carcinomas compared with cytology based screening

Take Home Message
• Evidence from these large RCTs supports initiation of HPV based screening at the age of 30 and extension of screening intervals to at least 5 years
Back to Henrietta
• Her last normal Pap was two years ago• If it included HPV testing, she could be
screened again in 3 years (5 year interval)
• If it did not include HPV testing, sheshould have her next Pap next year.

Screening Pelvic Exam?
• New clinical practice guideline from ACP• ACP recommends against performing
screening pelvic exam in asymptomatic, nonpregnant, adult women (strong recommendation, moderate-quality evidence)
Qaseem, et al. Ann Intern Med. 2014;161:67-72

Rationale for ACP rec
• Diagnostic accuracy of ovarian cancer is poor– PPV 0-3.6%
• No reduction in ovarian cancer mortality rates• Many false positives with possible harms • Psychological harms do exist

ACOG statement (2014)
• The College guidelines recommend that a pelvic examination be performed on an annual basis in all patients aged 21 years and older (2). No evidence supports or refutes the annual pelvic examination or speculum and bimanual examination for the asymptomatic, low-risk patient. An annual pelvic examination seems logical, but also lacks data to support a specific time frame or frequency of such examinations. The decision whether or not to perform a complete pelvic examination at the time of the periodic health examination for the asymptomatic patient should be a shared decision after a discussion between the patient and her health care provider.

Kimberly• Kimberly is 43 year old healthy female who has been
getting annual mammograms since the age of 40. She is a non-smoker, drinks alcohol occasionally, and exercises regularly. She has no family history of cancer.
• She notes that her mammograms are quite painful and fairly inconvenient. She has been called back twice for “minor abnormalities” which necessitated additional images (all of which were negative).
• She recently read an article in The New York Times which stated that mammograms may be less beneficial than previously thought. She wonders if she needs her mammogram this year.

Background
• Several trials have shown that mammography reduces breast cancer mortality, although their results may be affected by the adequacy of randomization.
• Mammography may also be associated with significant harms, including false-positives and over-diagnosis.
Cochrane Database Syst Rev 2013; Jun 4:6.

The News• Twenty five year follow-up for breast cancer
incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial.– Miller AB et al. BMJ 2014.
• Aims:– 1. To evaluate the benefit of annual breast
physical exam and screening mammography among women aged 40-49 compared with usual care.
– 2. To evaluate the risk/benefit of adding mammography to breast physical examination among women aged 50-59.

Women aged 40-59 who were non-pregnant, had no diagnosis of breast cancerand no mammography in prior 12 months
N= 89,835
Screening period: 5 yrs
Outcome: Breast cancer mortality
Randomization by study coordinator
Mammography+
breast exam N= 19, 694
Breast exam Alone
N = 19, 694
Randomization by study coordinator
Mammography+
breast exam N= 25, 214
Usual care N = 25, 216
Breast examination byexaminer
Women aged 40-49 N= 50,430 Women aged 50-59 N= 39, 405

Results: Years 1-5(screening phase)
*p = 0.01**p = 0.53
Variable Control Arm (usual care, annual
breast exam) N = 524
Mammogram Arm
N = 666
Mean age at diagnosis (years) 52.6 52.5
Died from breast cancer (%) 171 (32.6) 180 (27.0)
Tumor size (cm)* 2.1 (0.2-7.0) 1.9 (0.2-9.0)
Lymph node status positive(%)**
170 (32.4) 204 (30.6)
Estrogen receptor status (%)
Negative 85 (16.2) 102 (15.3)
Equivocal 41 (7.8) 41 (6.2)
Positive 261 (49.8) 312 (46.9)
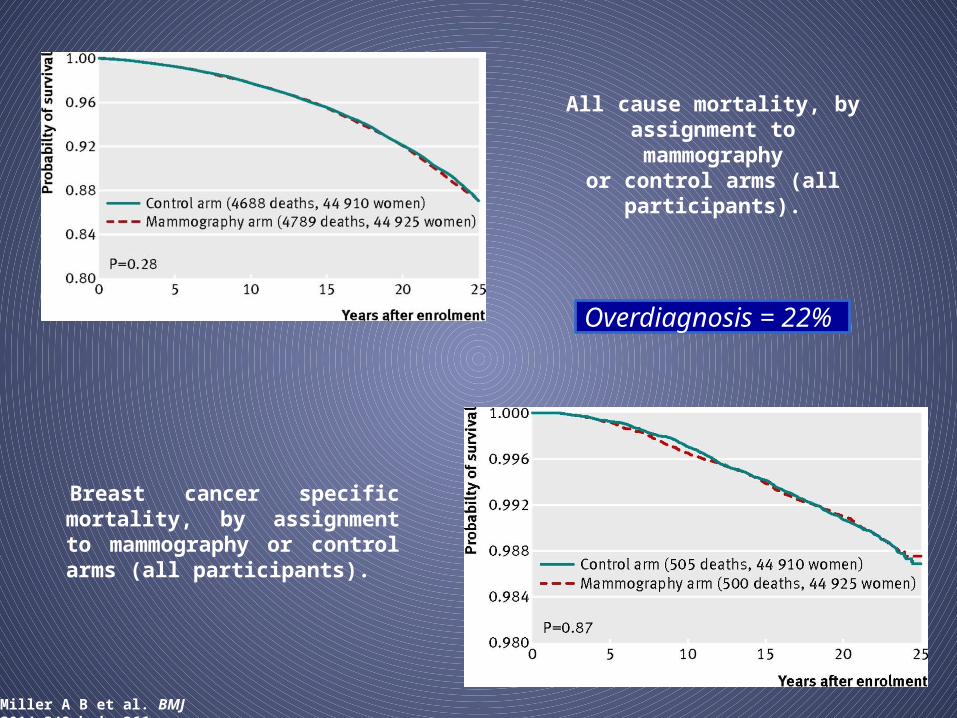
Breast cancer specific mortality, by assignment to mammography or control arms (all participants).
Miller A B et al. BMJ 2014;348:bmj.g366
Overdiagnosis = 22%
All cause mortality, by assignment tomammography
or control arms (all participants).

Potential limitations– Selection bias
• Exclusion of prevalent breast cancers did not change results• Equal proportions of women in both groups were
diagnosed with breast cancer after screening was complete (mammogram arm: 5.8%, control arm: 5.9%)
– Contamination• 26% of usual care group received mammograms• Adjustment for outside mammography did not change
results
– Mammography after end of screening phase• Unlikely that screening after the study was differential
between study arm participants or masked a benefit from screening during the study

Comparison with Other Trials• Swedish Two-County Trial
– 30% breast cancer mortality reduction– Randomization was by county
• Possible selection bias?– Analysis was based on invitation to screen
• Possible selection bias?
• Review of data from SEER– 31% overdiagnosis rate
• Wider age range included
Radiology 2011; Sept 260(3): 658-3.N Engl J Med 2012; 367:1998-2005.

Conclusions
• In this randomized study, mammography did not reduce breast cancer mortality; moreover, 22% of cancers were over- diagnosed
• Taken in context…– Prior trials may not have had
adequate randomization– Benefit may be related to
improvements intreatment rather than screening

How Should I CounselKimberly?

Key Article• Quantifying the Benefits and Harms of
Screening Mammography– Welch HG and Passow HJ. JAMA 2013.
• Aim: To use all available data to quantify the benefit- risk trade-off for screening mammography among women ages 40-69
• Outcomes assessed:– Reduction in breast cancer deaths– False-positive results– Over-diagnosis

How do I counsel Kimberly?
*Range of benefits include data from the Canadian National Breast Cancer Screening Studies and Swedish Two-County trials
Outcome Among 1000 40-year old women screened with annual mammography for 10
years
Benefits 0.1-1.6 will avoid dying from breast cancer*
Harms 510-690 women will have a false-positive result
60-80 will have a false-positive biopsyrecommendation
Up to 11 women will be over-diagnosed andpotentially receive unnecessary treatment

Take-Home Message
• Decisions regarding mammographic screening should be highly individualized and take into account the range of possible benefits and risks.
But what if Kimberly has dense breasts?
• Outcomes of screening mammography by frequency, breast density, and postmenopausal hormone therapy.– Kerlikowske et al., JAMA Intern Med 2013
• High breast density is associated with an increase risk of breast cancer
• USPSTF rec – biennial screening for women aged 40-49 is individualized decision

Dense breasts
• Prospective cohort study – 11000 women with breast cancer– 922000 women without
• Compared with annual mammo, biennial for women 40-49 with extremely dense breasts was associated with increased risk for advanced-stage breast cancer (OR 1.89)
• False positives high (65% 10 year risk)
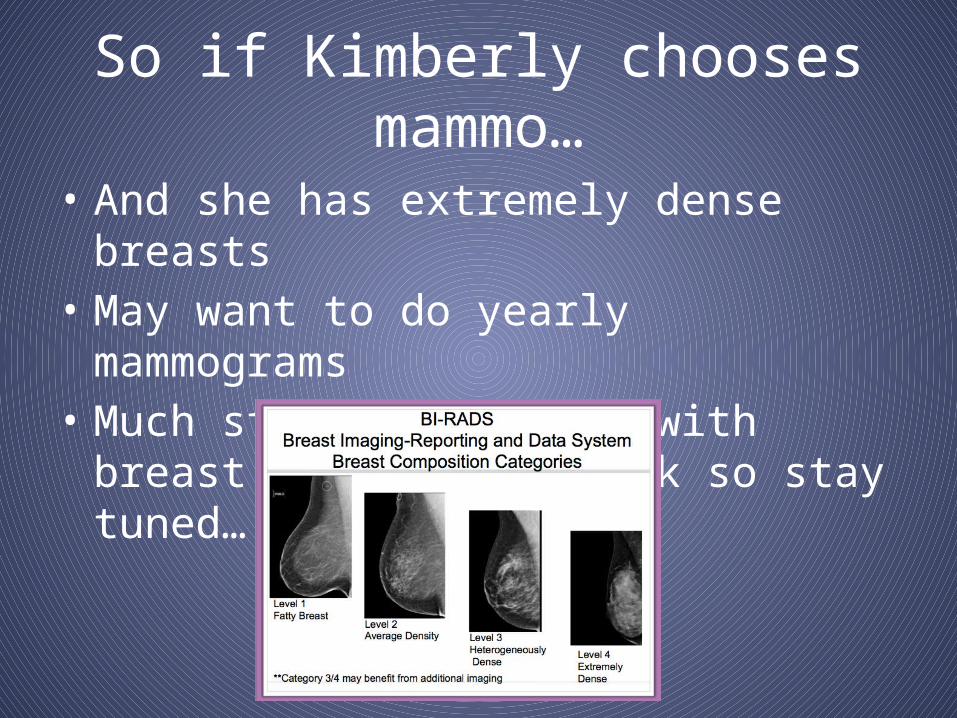
So if Kimberly chooses mammo…
• And she has extremely dense breasts • May want to do yearly mammograms• Much study being done with breast density
and risk so stay tuned….

Debbie• Debbie is a 53 year old female who was
diagnosed with estrogen and progesterone-receptor positive breast cancer 5 years ago.
• She underwent a right breast lumpectomy and sentinel-node biopsy and was subsequently treated with chemotherapy, radiation, and tamoxifen.
• Debbie was excited about the possibility of discontinuing her tamoxifen this year, until her oncologist brought up the results of a new study…

The News
• Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor- positive breast cancer: ATLAS, a randomised trial.– Davies C et al. The Lancet 2013
• Aim: To assess the relative benefits and risks of continuing tamoxifen therapy for 10 years after diagnosis of invasive breast cancer

Background
• Among women with ER+ breast cancer, treatment with 5 years of tamoxifen significantly reduces the risk of breast cancer recurrence and mortality over 10-15 years of follow-up.
• It is unclear what additional benefit, if any, might accrue with longer durations of tamoxifen therapy.
Lancet 2011; 378:771-784.

Methods15,244 women with early stage breast
cancer, randomized to:• Continue tamoxifen for another 5 years , n=7629
• Stop tamoxifen immediately, n = 7615
2350 excluded because prior treatment with tamoxifen was less than 4 years
12,894 included in analysis of side effects (median prior tamoxifen duration: 5 years
6846 with ER+ breast cancer included inefficacy analysis
•3428 continued tamoxifen for another 5 years•3418 stopped tamoxifen immediately
Outcomes:All cause mortalityBreast cancer recurrence
Breast cancer mortality
36 countries, trial years 1996-2005
6048 excluded because ER status was unknown or negative
Responsible clinicians provided information on outcomes; “death certificates were also sought.” Outcome assessor was not blinded to treatment assignment.

Source: The Lancet 2013; 381:805-816 (DOI:10.1016/S0140-6736(12)61963-1)
Breast cancer recurrence Breast cancer mortality
Absolute recurrence reduction 3.7%
Absolute mortality reduction 2.8%

ResultsER-Positive
Patients Who Experienced…
Continued tamoxifen to
10 yearsN= 3428
Stopped tamoxifen at 5
yearsN= 3418
Event rate ratio(95% CI)
P-value
Any death 639 722 0.87 (0.78-0.97) 0.01
Death with recurrence
331 397 0.83 (0.72 –0.96) 0.01
Death without recurrence
308 325 0.91 (0.78-1.06) 0.24
Stroke 130 119 1.06 (0.83-1.36) 0.63
Pulmonaryembolus
41 21 1.87 (1.13-3.07) 0.01
Ischemic heart dz 127 163 0.76 (0.60-0.95) 0.02
Endometrial CA 116 63 1.74 (1.30-2.34) 0.0002
Cataract 72 63 1.11 (0.79-1.56) 0.54

Conclusions
• Among women with ER+ breast cancer, continuing tamoxifen for a total of 10 years, as compared to 5 years, further reduces the risk of breast cancer recurrence and mortality during 10-15 years of follow-up.
• These benefits must be weighed against potential harms, including a 2-5% risk of endometrial cancer at year 15.

Back to Debbie…
• She had experienced multiple episodes of vaginal bleeding while on tamoxifen and had undergone 2 endometrial biopsies. She was very concerned about her risk for endometrial cancer and wanted to avoid further procedures. She elected not to continue on tamoxifen.

Take Home Message
• While continuing treatment with tamoxifen to 10 years after diagnosis is associated with clear benefits, the decision to do so must be highly individualized, and take into account the potential harms of therapy.
Bonnie Bony
• Bonnie Bony is a 72 year old woman who wants to know when she should have her next bone mineral density test. Her last BMD was 2 years ago and showed osteopenia with a t score of -1.8. What do you tell her?

USPSTF Recommendations
• Screen all women age 65 and older– Evidence for screening is indirect
• Screen younger women whose fracture risk is equal to or greater than a 65 year old white woman who has no additional risk factors
• “Evidence is lacking about optimal intervals for repeated screening”– A minimum of 2 years may be needed to reliably
measure a change in BMD– Longer intervals may be needed to improve
fracture risk prediction» USPSTF 2011
BMD testing
• Medicare pays for BMD every two years regardless of baseline BMD
• Is repeat BMD useful?• Does change in BMD provide additional
information about fracture risk?

Monitoring Guidelines• All recommend follow-up monitoring but no
consensus on site and frequency• What is “treatment failure?”• ISCD: DEXA spine and hip when expected
change in BMD exceeds LSC expected on bone densitometer– Typically every 1-2 years– Less often once stable
• AACE: DEXA spine and hip every 1-2 years untilstability
• NAMS: DXA hip every 2 years• Question: What are you going to do?

The News
• Repeat bone mineral density screening and prediction of hip and major osteoporotic fracture.– Berry et al. JAMA 2013;310:1256-62.
• Aim: To determine whether BMD changes after 4 years provide additional information on fracture risk and to quantify the change in fracture risk classification after a second BMD measure

Methods
• Framingham Osteoporosis Study population basedcohort of 310 men and 492 women– Two BMD measures from 1987 to 1999
• Outcome: risk of hip or major osteoporotic fracture through 2009 or 12 years after second BMD measure
• Net Reclassification Index (NRI):– Quantifies change in risk classification after a
second BMD measure
– High risk: Risk of hip fracture 3% or greater or major
osteoporotic fracture 20% or greater (vs low risk)

Results• Mean age 74.8 years• Mean BMD change -0.6% per year• Median follow up 9.6 years• NRI increased proportion classified as high
risk by 3.9% and decreased the proportion defined as low risk by 2.2%
• Adding BMD change to a model that included baseline BMD did not improve performance of the ROC curve– AUC baseline 0.71 (0.65-0.67) vs 0.72 (0.66-0.79)

Figure Legend:
Receiver Operating Characteristic Curves for Models Investigating Fracture in Older Adults From the Framingham Osteoporosis StudyBMD indicates bone mineral density. All models are adjusted for age, sex, body mass index, weight loss (per pound), and history of fracture measured at the time of the second BMD test. Models are defined in the Methods section.
Copyright © 2014 American Medical Association.
ROC Curves for Hip and Major Osteoporotic Fractures
Take home message
• Repeating a BMD after 4 years to improve fracture risk prediction may not be necessary in adults of this age untreated for osteoporosis
What might be the right interval?
• Study of Osteoporotic Fractures in women 67 years and older
• Intervals capturing 90% of women developing osteoporosis (T -2.5)– 15 years for baseline normal or T -1 to -1.49– 5 years for T -1.5 to -1.99– 1 years for T -2.0 to -2.49





New recommendation 2013!
• The U.S. Preventive Services Task Force (USPSTF) recommends that clinicians screen women of childbearing age for intimate partner violence (IPV), such as domestic violence, and provide or refer women who screen positive to intervention services.
• This is a B recommendation. This recommendation applies to women who do not have signs or symptoms of abuse.

