update on accelerated update on accelerated … on accelerated update on accelerated whole &...
TRANSCRIPT

10/15/2012
1
Update on Accelerated Update on Accelerated Whole & Whole & Partial Breast IrradiationPartial Breast Irradiation
Frank Vicini, MD, FACRFrank Vicini, MD, FACR
Michigan Healthcare Professionals/21Michigan Healthcare Professionals/21stst Century OncologyCentury Oncology
Farmington Hills, MichiganFarmington Hills, Michigan
1010thth Annual Adjuvant & Annual Adjuvant & NeoadjuvantNeoadjuvant TherapyTherapy
New York, New YorkNew York, New York
October 13, 2012October 13, 2012
OutlineOutline
•• Definition/Rationale for Accelerated Whole & Definition/Rationale for Accelerated Whole & Partial Breast Radiation (PBI) Partial Breast Radiation (PBI) –– Discuss scientific basis for altered fractionation Discuss scientific basis for altered fractionation
schemesschemes
•• Review Whole Breast & PBI DataReview Whole Breast & PBI Data
•• FutureFuture::–– Discuss future trendsDiscuss future trends
BackgroundBackground
•• Breast Conserving TherapyBreast Conserving Therapy::–– Equivalence to mastectomy proven in Equivalence to mastectomy proven in
lti l h III t i llti l h III t i lmultiple phase III trialsmultiple phase III trials•• 2020--30 year survival data (NSABP B06/Milan)30 year survival data (NSABP B06/Milan)
•• Excellent cosmetic resultsExcellent cosmetic results
•• Minimal longMinimal long--term toxicityterm toxicity
•• “Standard of care” “Standard of care”
10/15/2012
2
BackgroundBackground
•• Trends in the Local Treatment of Early Stage Trends in the Local Treatment of Early Stage Breast Cancer Managed With BCT:Breast Cancer Managed With BCT:–– Improvement in Local ControlImprovement in Local Control
O ti i i l t h iO ti i i l t h i•• Optimize surgical techniquesOptimize surgical techniques•• Define factors associated with local recurrenceDefine factors associated with local recurrence•• Define the optimal RT dose (e.g., boost)Define the optimal RT dose (e.g., boost)•• Optimal integration with systemic therapiesOptimal integration with systemic therapies
–– Improvements in Cosmetic ResultsImprovements in Cosmetic Results•• Optimize surgical techniquesOptimize surgical techniques•• Optimize radiotherapy techniques (e.g., homogeneity)Optimize radiotherapy techniques (e.g., homogeneity)•• Optimize combination of local/systemic therapiesOptimize combination of local/systemic therapies
BackgroundBackground
•• Trends in the Local Treatment of Early Stage Trends in the Local Treatment of Early Stage Breast Cancer Managed With BCT:Breast Cancer Managed With BCT:–– Reduction in acute/chronic toxicity from RTReduction in acute/chronic toxicity from RT
•• Use of IMRTUse of IMRT•• Gated therapy/Breath HoldGated therapy/Breath Hold•• Improved treatment of regional lymphaticsImproved treatment of regional lymphatics
–– Improvement in Quality of LifeImprovement in Quality of Life•• Elimination of RT in selected patients Elimination of RT in selected patients •• Reduction in overall treatment timeReduction in overall treatment time
–– Accelerated therapyAccelerated therapy»» Whole breast RTWhole breast RT»» Partial breast RTPartial breast RT
Areas of InvestigationAreas of Investigation
Breast Conservation TherapyBreast Conservation Therapy
LumpectomyLumpectomyLumpectomyLumpectomyLumpectomyLumpectomy
plus WBIplus WBI
LumpectomyLumpectomy++
Hypofx WBIHypofx WBI
LumpectomyLumpectomyAloneAlone
LumpectomyLumpectomy++
APBIAPBI
10/15/2012
3
Focus of Today’s DiscussionFocus of Today’s Discussion
Breast Conservation TherapyBreast Conservation Therapy
LumpectomyLumpectomyLumpectomyLumpectomyLumpectomyLumpectomy
plus WBIplus WBI
LumpectomyLumpectomy++
Hypofx WBIHypofx WBI
LumpectomyLumpectomyAloneAlone
LumpectomyLumpectomy++
APBIAPBI
≤ ≤ 1 week 1 week 22--4 weeks4 weeks
Modifications of the Modifications of the Radiotherapy ScheduleRadiotherapy Schedule
1)1) HyperfractionationHyperfractionation –– delivery of a low delivery of a low dose/fractiondose/fraction (for radio sensitive tumours)(for radio sensitive tumours)dose/fraction dose/fraction (for radio sensitive tumours)(for radio sensitive tumours)
2)2) HypofractionationHypofractionation –– delivery of a higher delivery of a higher dose/fraction dose/fraction (for less radio sensitive tumours)(for less radio sensitive tumours)
3)3) AcceleratedAccelerated -- treatment in a shorter time treatment in a shorter time (for (for moderatemoderate--fast growing tumours)fast growing tumours)
Background
•• Biological effect of radiation is related to total Biological effect of radiation is related to total dose, fraction size and time of treatmentdose, fraction size and time of treatment
•• Suggests that an increase in the fraction sizeSuggests that an increase in the fraction sizeSuggests that an increase in the fraction size, Suggests that an increase in the fraction size, will increase the treatment effectwill increase the treatment effect
•• BED = Total Dose (1 + BED = Total Dose (1 + fraction sizefraction size) ) –– f(T)f(T)•• Treatment times can be shortened and still Treatment times can be shortened and still
produce equivalent local control & toxicityproduce equivalent local control & toxicity
//

10/15/2012
4
Accelerated Whole Breast Accelerated Whole Breast IrradiationIrradiation
•• Can the length of treatment for BCT with Can the length of treatment for BCT with radiation be reduced by increasing the radiation be reduced by increasing the dose/fraction?dose/fraction?dose/fraction?dose/fraction?–– Improve quality of lifeImprove quality of life
–– Allow greater utilization of BCT resourcesAllow greater utilization of BCT resources
•• Will local control, cosmesis & toxicities be Will local control, cosmesis & toxicities be equivalent? equivalent?
1,234 patientsT1-2, N0 ®
50 Gy/25 frac/5 wks [2 Gy]50 Gy/25 frac/5 wks [2 Gy]
Ontario Clinical Oncology Group (OCOG) Ontario Clinical Oncology Group (OCOG) Trial of Accelerated Hypofractionated Trial of Accelerated Hypofractionated
Whole Breast IrradiationWhole Breast Irradiation
with clear margins
®42.5 Gy/16 frac/3 wks [2.7 Gy]42.5 Gy/16 frac/3 wks [2.7 Gy]
Median follow-up 10 years
Tim WhelanTim Whelan
97
98
99
100
Percent
Event-free
Short(42.5 Gy/16)
Long(50 Gy/25)
97.2%
96 8%
Local RecurrenceLocal Recurrence--Free SurvivalFree Survival
0 1 2 3 4 5
95
96
Years Since Randomization
At Risk:
96.8%
Long 612 597 575 554 460 266
Short 622 609 591 565 466 246

10/15/2012
5
ConclusionConclusion
The shorter radiation fractionation schedule The shorter radiation fractionation schedule 42.5 Gy/1642.5 Gy/16
was was as good asas good as a more traditional schedule a more traditional schedule 50 Gy/2550 Gy/25 in in
terms of local breast cancer recurrence (6.2 vs 6.7%) terms of local breast cancer recurrence (6.2 vs 6.7%)
and cosmesis @ 10 yearsand cosmesis @ 10 years
N Engl J Med. 2010 Feb 11;362(6):513N Engl J Med. 2010 Feb 11;362(6):513--20 20
2,236 patientsT1-3, N0-1 ®
50 Gy/25 frac/5 wks [2 Gy]
41.6 Gy/13 frac/5 wks [3.2 Gy]*
START Trial A (Hypofractionated)START Trial A (Hypofractionated)
Mo ® y [ y]
* Boost radiation permitted Dewer, Yarnold et al., ASCO 2006
39 Gy/13 frac/5 wks [3.3 Gy]39 Gy/13 frac/5 wks [3.3 Gy]
Median follow-up 5.1 years
2,215 patientsT1-3, N0-1 ®
50 Gy/25 frac/5 wks [250 Gy/25 frac/5 wks [2 Gy]*
START Trial BSTART Trial B(Accelerated and Hypofractionated)(Accelerated and Hypofractionated)
Mo ®
* Boost radiation permitted Dewer, Yarnold et al., ASCO 2006
40 Gy/15 frac/3 wks [2.7 Gy]40 Gy/15 frac/3 wks [2.7 Gy]
Median follow-up 6.0 years

10/15/2012
6
Study Radiation Treatment No. of Pts.
Median F/U (yrs)
Local Rec. (%)
Toxicity Br (%)
OCOG, 2002*
50 Gy/25 frac/5 wks
42.5 Gy/16 frac/3 wks
612
622
5.8 3.2
2.8
40
34
ICR, 2006**
50 Gy/25 frac/5 wks
42 9 Gy/13 frac/5 wks
470
466
9.7 12.1
9 6
40
46
RCT’s of Hypofractionated Whole Breast RCT’s of Hypofractionated Whole Breast IrradiationIrradiation
*Whelan et al., JNCI 94:1143-1150, 2002. **Owen, Yarnold et al., Lancet Oncol 7:467-71, 2006. Dewer, Yarnold et al., ASCO 2006
42.9 Gy/13 frac/5 wks
39 Gy/13 frac/5 wks
466
474
9.6
14.8
46
30
Start A*** 50 Gy/25 frac/5 wks
41.6 Gy/13 frac/5 wks
39 Gy/13 frac/5 wks
749
737
750
5.1 3.7
3.5
5.3
42
42
31
Start B*** 50 Gy/25 frac/5 wks
40 Gy/15 frac/3 wks
1105
1110
6.0 3.7
3.2
40
33
Short Whole Breast Schedules Can Be Short Whole Breast Schedules Can Be Considered a Standard Option In Considered a Standard Option In
Selected PatientsSelected Patients
-- ASTRO Consensus Panel Guideline ASTRO Consensus Panel Guideline Recommendations Developed Recommendations Developed --
Short Whole Breast Schedules Short Whole Breast Schedules Not Widely Used in the United Not Widely Used in the United
StatesStates
•• Boost irradiation commonly used Boost irradiation commonly used
•• Concerns re: longConcerns re: long--term toxicityterm toxicity
•• Concerns re: interactions with systemic Concerns re: interactions with systemic chemotherapy chemotherapy
•• Longer schedules used for larger breast size Longer schedules used for larger breast size
10/15/2012
7
R ARM 1: Standard fractionationA Wh l B 50 G / 25 f i / 2 0 G d il
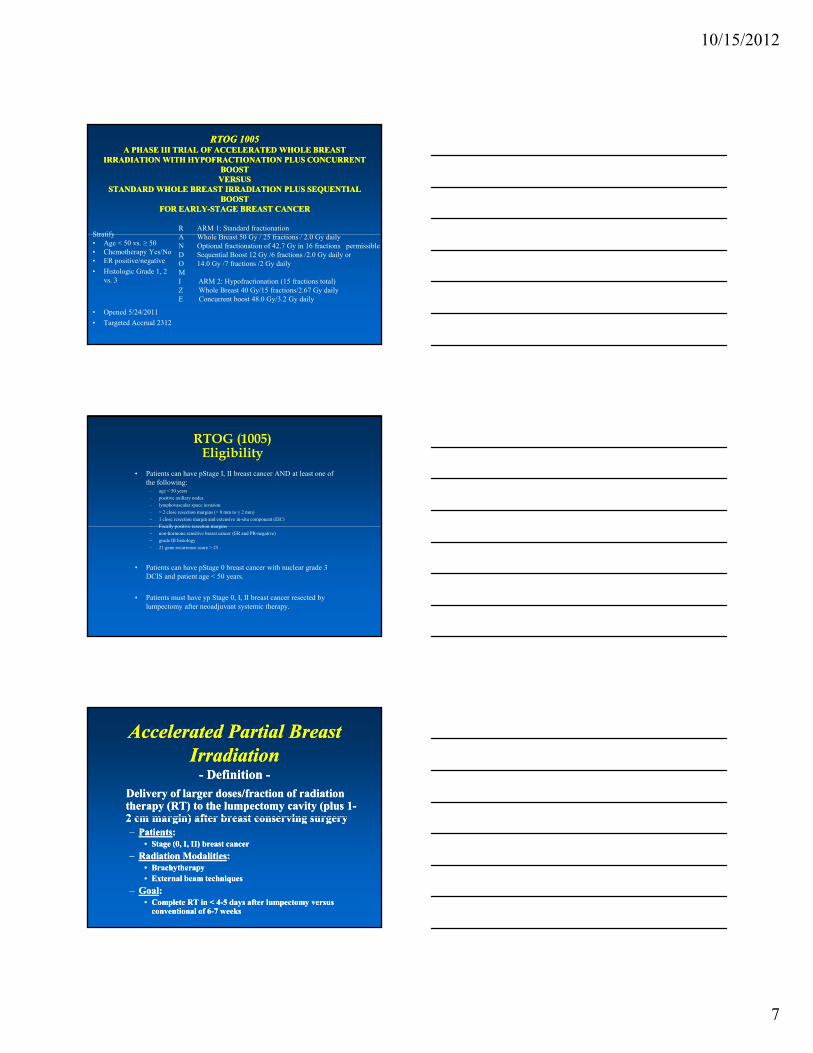
RTOG 1005RTOG 1005A PHASE III TRIAL OF ACCELERATED WHOLE BREAST A PHASE III TRIAL OF ACCELERATED WHOLE BREAST
IRRADIATION WITH HYPOFRACTIONATION PLUS CONCURRENT IRRADIATION WITH HYPOFRACTIONATION PLUS CONCURRENT BOOST BOOST VERSUS VERSUS
STANDARD WHOLE BREAST IRRADIATION PLUS SEQUENTIAL STANDARD WHOLE BREAST IRRADIATION PLUS SEQUENTIAL BOOST BOOST
FOR EARLYFOR EARLY--STAGE BREAST CANCERSTAGE BREAST CANCER
Stratify A Whole Breast 50 Gy / 25 fractions / 2.0 Gy daily N Optional fractionation of 42.7 Gy in 16 fractions permissibleD Sequential Boost 12 Gy /6 fractions /2.0 Gy daily orO 14.0 Gy /7 fractions /2 Gy dailyMI ARM 2: Hypofractionation (15 fractions total) Z Whole Breast 40 Gy/15 fractions/2.67 Gy dailyE Concurrent boost 48.0 Gy/3.2 Gy daily
Stratify• Age < 50 vs. ≥ 50• Chemotherapy Yes/No• ER positive/negative
• Histologic Grade 1, 2 vs. 3
• Opened 5/24/2011
• Targeted Accrual 2312
• Patients can have pStage I, II breast cancer AND at least one of the following:
– age < 50 years
– positive axillary nodes
– lymphovascular space invasion
– > 2 close resection margins (> 0 mm to ≤ 2 mm)
– 1 close resection margin and extensive in-situ component (EIC)
Focally positive resection margins
RTOG (1005)Eligibility
– Focally positive resection margins
– non-hormone sensitive breast cancer (ER and PR-negative)
– grade III histology
– 21 gene recurrence score > 25
• Patients can have pStage 0 breast cancer with nuclear grade 3 DCIS and patient age < 50 years.
• Patients must have yp Stage 0, I, II breast cancer resected by lumpectomy after neoadjuvant systemic therapy.
Accelerated Partial Breast Accelerated Partial Breast IrradiationIrradiation
-- Definition Definition --
Delivery of larger doses/fraction of radiation Delivery of larger doses/fraction of radiation therapy (RT) to the lumpectomy cavity (plus 1therapy (RT) to the lumpectomy cavity (plus 1--2 cm margin) after breast conserving surgery2 cm margin) after breast conserving surgery2 cm margin) after breast conserving surgery2 cm margin) after breast conserving surgery–– PatientsPatients: :
•• Stage (0, I, II) breast cancerStage (0, I, II) breast cancer
–– Radiation ModalitiesRadiation Modalities: : •• BrachytherapyBrachytherapy•• External beam techniquesExternal beam techniques
–– GoalGoal: : •• Complete RT in < 4Complete RT in < 4--5 days after lumpectomy versus 5 days after lumpectomy versus
conventional of 6conventional of 6--7 weeks7 weeks

10/15/2012
8
Rationale For APBIRationale For APBI
•• Time and Inconvenience of BCTTime and Inconvenience of BCT
•• Improve Documented Underutilization of BCTImprove Documented Underutilization of BCTImprove Documented Underutilization of BCTImprove Documented Underutilization of BCT
•• Potentially Reduce Acute and Chronic ToxicityPotentially Reduce Acute and Chronic Toxicity
•• Improve Quality of Life of PatientsImprove Quality of Life of Patients
•• Eliminate Scheduling Problems With Systemic Eliminate Scheduling Problems With Systemic ChemotherapyChemotherapy
APBIAPBI-- Available Techniques Available Techniques --
•• Catheter based brachytherapyCatheter based brachytherapy
•• MammoSite Balloon DeviceMammoSite Balloon Device
•• 3D Conformal external beam radiation 3D Conformal external beam radiation therapytherapy
•• SingleSingle--fraction, intrafraction, intra--operative PBIoperative PBI
Catheter Based BrachytherapyCatheter Based BrachytherapyTraditional FreeTraditional Free--HandHand
MultiMulti--cathetercatheterTechniqueTechnique
Kuske templateKuske template

10/15/2012
9
Published APBI ResultsPublished APBI Results-- Catheter Based Brachytherapy Catheter Based Brachytherapy --
Institution # Patients
Follow-Up (Months)
% Local Recurrence
NIO-Hungary (phase II) 45 136 9.3* WBH 199 113 5*
Orebro University 50 86 4+ MGH 48 84 2
Tufts/Brown University 33 84 9 NIO-Hungary (phase III) 128 81 4.7
O h Cli i 51 75 2 0Oschner Clinic 51 75 2.0 RTOG 95-17 99 74 4.0
Joe Arrington Cancer Center 214 72 4.2 German-Austrian MC Trial 171 71 -- University of Wisconsin*** 136 60 4.8
Tufts-Brown University 33 58 6 Washington University 192 55 2.1
VCU 59 50 5.1 University of Wisconsin 247 48 3**
Joe Arrington Cancer Center 136 48 3.7 German-Austrian MC Trial 274 38 0.4
University Kansas 24 37 0 University of Perugia, Italy 80 30 0
Florence Italy 90 27 4.4 Totals 2309 27-136 0-9%
*12-year rate, += 7-year rate ** High-risk patients, ***ASTRO Cautionary Group
< 5 years< 5 years
Published APBI ResultsPublished APBI Results-- Catheter Based Brachytherapy Catheter Based Brachytherapy --
Institution # Patients
Follow-Up (Months)
% Local Recurrence
NIO-Hungary (phase II) 45 136 9.3* WBH 199 113 5*
Orebro University 50 86 4+ MGH 48 84 2
Tufts/Brown University 33 84 9 NIO-Hungary (phase III) 128 81 4.7
O h Cli i 51 75 2 0 55--yearsyearsOschner Clinic 51 75 2.0 RTOG 95-17 99 74 4.0
Joe Arrington Cancer Center 214 72 4.2 German-Austrian MC Trial 171 71 -- University of Wisconsin*** 136 60 4.8
Tufts-Brown University 33 58 6 Washington University 192 55 2.1
VCU 59 50 5.1 University of Wisconsin 247 48 3**
Joe Arrington Cancer Center 136 48 3.7 German-Austrian MC Trial 274 38 0.4
University Kansas 24 37 0 University of Perugia, Italy 80 30 0
Florence Italy 90 27 4.4 Totals 2309 27-136 0-9%
*12-year rate, += 7-year rate ** High-risk patients, ***ASTRO Cautionary Group
55 yearsyears
Published APBI ResultsPublished APBI Results-- Catheter Based Brachytherapy Catheter Based Brachytherapy --
Institution # Patients
Follow-Up (Months)
% Local Recurrence
NIO-Hungary (phase II) 45 136 9.3*
RTOG 95-17 Hungary Phase III
99 129
146 144
6.2 6
WBH 199 113 5* Orebro University 50 86 4+
MGH 48 84 2 T ft /B U i it 33 84 9
> 10 years> 10 years
Tufts/Brown University 33 84 9 NIO-Hungary (phase III) 128 81 4.7
Oschner Clinic 51 75 2.0 RTOG 95-17 99 74 4.0
Joe Arrington Cancer Center 214 72 4.2 German-Austrian MC Trial 171 71 -- University of Wisconsin*** 136 60 4.8
Tufts-Brown University 33 58 6 Washington University 192 55 2.1
VCU 59 50 5.1 University of Wisconsin 247 48 3**
Joe Arrington Cancer Center 136 48 3.7 German-Austrian MC Trial 274 38 0.4
University Kansas 24 37 0 University of Perugia, Italy 80 30 0
Florence Italy 90 27 4.4 Totals 2309 27-136 0-9%
*12-year rate, += 7-year rate ** High-risk patients, ***ASTRO Cautionary Group

10/15/2012
10
Balloon Catheter‘MammoSite’
• MammoSite device (Proxima, Cytyc, Hologic)
• Inflatable Balloon Placed In Lumpectomy Cavity At Surgery
• HDR brachytherapy• 34 Gy in 10 fractions • FDA clearance May 2002• Since 2002, > 75,000
cases treated
Published APBI ResultsPublished APBI Results-- MammoSite MammoSite --
Institution # Cases
Follow-Up (Months)
% Local Recurrence
FDA Trial ASBS Registry
43 400
66 60
0% 3.2%ASBS Registry
NY Hospital/Cornell (DCIS) 400 48
60 60
3.2% 6.3%
University of Wisconsin 26 48.5 3%* ASBS Registry Trial 1449 51 2.6%
MUSC 99 46 3.1% Texas Cancer Center 573 31 1.0%
Rush 70 26 6% WBH 80 24 2.9% VCU 483 24 1.2%
Tufts/VCU/NEMC 28 19 0% Single Institution Experiences 1000 2-12 0-3%
Totals 3899 2-66 0-6.3% *High-risk patients
Published APBI ResultsPublished APBI Results-- MammoSite MammoSite --
Institution # Cases
Follow-Up (Months)
% Local Recurrence
FDA Trial ASBS Registry
43 400
66 60
0% 3.2%ASBS Registry
NY Hospital/Cornell (DCIS) 400 48
60 60
3.2% 6.3%
University of Wisconsin 26 48.5 3%* ASBS Registry Trial 1449 51 2.6%
MUSC 99 46 3.1% Texas Cancer Center 573 31 1.0%
Rush 70 26 6% WBH 80 24 2.9% VCU 483 24 1.2%
Tufts/VCU/NEMC 28 19 0% Single Institution Experiences 1000 2-12 0-3%
Totals 3899 2-66 0-6.3% *High-risk patients
< 5 years< 5 years

10/15/2012
11
Published APBI ResultsPublished APBI Results-- MammoSite MammoSite --
Institution # Cases
Follow-Up (Months)
% Local Recurrence
FDA Trial ASBS Registry
43 400
66 60
0% 3.2% 55--yearsyearsASBS Registry
NY Hospital/Cornell (DCIS) 400 48
60 60
3.2% 6.3%
University of Wisconsin 26 48.5 3%* ASBS Registry Trial 1449 51 2.6%
MUSC 99 46 3.1% Texas Cancer Center 573 31 1.0%
Rush 70 26 6% WBH 80 24 2.9% VCU 483 24 1.2%
Tufts/VCU/NEMC 28 19 0% Single Institution Experiences 1000 2-12 0-3%
Totals 3899 2-66 0-6.3% *High-risk patients
55 yearsyears
3D Conformal External Beam Radiotherapy3D Conformal External Beam Radiotherapy-- APBI APBI --
Published APBI ResultsPublished APBI Results-- 3D Conformal External Beam RT 3D Conformal External Beam RT --
Institution # Patients
Follow-Up (Months)
% Local Recurrence
Grade III Toxicity
NYU (prone) 98 60 1% 3% WBH 96 47 1% 4%
RTOG 0319 52 42 6% 4% Canadian Multi-Center 127 36 <1% <1% Loma Linda (Protons) 50 36 0% 0%( )
NYU/Keck School Medicine 10 36 0% -- MGH 99 36 2% --
Rocky Mountain Cancer Center 105 36 0% -- NIO-Hungary 40 34 2% --
NSABP B39/RTOG 0413 338 32 -- <2% Stanford 62 29 0% 1.6%
NYU 78 28 0% -- University of Michigan 34 24 -- --
California Pacific Med Center 51 22 0% 0% Virginia Commonwealth Univ 61 18 0% 7%
Tufts 64 15 -- 8.3% Baptist 24 13 0% -- Totals 1289 13-47 0-6% 1-8%

10/15/2012
12
Published APBI ResultsPublished APBI Results-- 3D Conformal External Beam RT 3D Conformal External Beam RT --
Institution # Patients
Follow-Up (Months)
% Local Recurrence
Grade III Toxicity
NYU (prone) 98 60 1% 3% WBH 96 47 1% 4%
RTOG 0319 52 42 6% 4% Canadian Multi-Center 127 36 <1% <1% Loma Linda (Protons) 50 36 0% 0%( )
NYU/Keck School Medicine 10 36 0% -- MGH 99 36 2% --
Rocky Mountain Cancer Center 105 36 0% -- NIO-Hungary 40 34 2% --
NSABP B39/RTOG 0413 338 32 -- <2% Stanford 62 29 0% 1.6%
NYU 78 28 0% -- University of Michigan 34 24 -- --
California Pacific Med Center 51 22 0% 0% Virginia Commonwealth Univ 61 18 0% 7%
Tufts 64 15 -- 8.3% Baptist 24 13 0% -- Totals 1289 13-47 0-6% 1-8%
< 5< 5--yearsyears
Published APBI ResultsPublished APBI Results-- 3D Conformal External Beam RT 3D Conformal External Beam RT --
Institution # Patients
Follow-Up (Months)
% Local Recurrence
Grade III Toxicity
NYU (prone) 98 60 1% 3% WBH 96 47 1% 4%
RTOG 0319 52 42 6% 4% Canadian Multi-Center 127 36 <1% <1% Loma Linda (Protons) 50 36 0% 0%
55--yearsyears
( )NYU/Keck School Medicine 10 36 0% --
MGH 99 36 2% -- Rocky Mountain Cancer Center 105 36 0% --
NIO-Hungary 40 34 2% -- NSABP B39/RTOG 0413 338 32 -- <2%
Stanford 62 29 0% 1.6% NYU 78 28 0% --
University of Michigan 34 24 -- -- California Pacific Med Center 51 22 0% 0% Virginia Commonwealth Univ 61 18 0% 7%
Tufts 64 15 -- 8.3% Baptist 24 13 0% -- Totals 1289 13-47 0-6% 1-8%
APBIAPBI-- Phase III Trials Phase III Trials --
•• Nine Phase III TrialsNine Phase III Trials•• Four PBI TechniquesFour PBI Techniques::
–– BrachytherapyBrachytherapy RT (Interstitial/RT (Interstitial/MammoSiteMammoSite))•• NSABP BNSABP B--39/RTOG 041339/RTOG 0413•• GECGEC--ESTRO Working GroupESTRO Working GroupGECGEC ESTRO Working GroupESTRO Working Group•• National Institute of HungaryNational Institute of Hungary
–– SingleSingle--Fraction IntraFraction Intra--Operative RTOperative RT•• European Institute of OncologyEuropean Institute of Oncology•• University College of LondonUniversity College of London
–– Fractionated External Beam RTFractionated External Beam RT•• NSABP BNSABP B--39/RTOG 041339/RTOG 0413•• National Institute of HungaryNational Institute of Hungary•• Canadian Phase III trialCanadian Phase III trial•• Medical Research CouncilMedical Research Council--UKUK•• BarcelonaBarcelona•• FlorenceFlorence

10/15/2012
13
National Institute of OncologyNational Institute of Oncology-- Budapest, Hungary Budapest, Hungary --
•• SchemaSchema::–– Arm IArm I: External Beam Whole Breast RT: External Beam Whole Breast RT
•• 5050 GyGy in 25 fractionsin 25 fractions50 50 GyGy in 25 fractionsin 25 fractions
–– Arm IIArm II: Partial Breast Irradiation: Partial Breast Irradiation•• Brachytherapy: 5.2 Brachytherapy: 5.2 GyGy x 7x 7
–– 258 enrolled (Trial Closed)258 enrolled (Trial Closed)–– Trial closed to support GECTrial closed to support GEC--ESTRO Phase III trialESTRO Phase III trial
National Institute of OncologyNational Institute of Oncology-- Budapest, Hungary Budapest, Hungary --
•• Results/New Data:Results/New Data:•• Presented at ESTRO 2012Presented at ESTRO 2012•• 1010 year update (median f/u 120 months)year update (median f/u 120 months)•• 1010--year update (median f/u 120 months)year update (median f/u 120 months)•• No differences noted in local failureNo differences noted in local failure
–– 5.9 5.9 vsvs 5.1%5.1%
•• 81% E/G 81% E/G cosmesiscosmesis with APBI with APBI vsvs 63% with WBI63% with WBI
European Institute of OncologyEuropean Institute of Oncology-- Milan, Italy (Veronesi) Milan, Italy (Veronesi) --
•• SchemaSchema::–– Arm IArm I: External Beam Whole Breast RT: External Beam Whole Breast RT
•• 5050 GyGy in 25 fractions plus 10in 25 fractions plus 10 GyGy boostboost•• 50 50 GyGy in 25 fractions plus 10 in 25 fractions plus 10 GyGy boostboost
–– Arm IIArm II: Partial Breast IORT: Partial Breast IORT•• 21 21 GyGy intraintra--operative single fraction after operative single fraction after quadrentectomyquadrentectomy
–– Accrual: 1303 patientsAccrual: 1303 patients–– ClosedClosed: Summer 2007: Summer 2007

10/15/2012
14
European Institute of OncologyEuropean Institute of Oncology-- Milan, Italy (Veronesi) Milan, Italy (Veronesi) --
•• Results/New Data:Results/New Data:–– Presented at ESTRO 2012Presented at ESTRO 2012–– Overall, higher IBTR in 21Gy arm (5% Overall, higher IBTR in 21Gy arm (5% vsvs 1%)1%), g y (, g y ( ))–– No difference in the Suitable ASTRO CP Group No difference in the Suitable ASTRO CP Group
(1% (1% vsvs 1%)1%)
University College of LondonUniversity College of London-- London, England London, England --
•• Randomized TrialRandomized Trial –– 17 Centers Participated17 Centers Participated•• Accrual GoalAccrual Goal: 1116 patients/arm: 1116 patients/arm•• StatisticsStatistics::StatisticsStatistics::
–– Arm IArm I: External Beam Whole Breast RT: External Beam Whole Breast RT•• Conventional RT (doses per center)Conventional RT (doses per center)
–– Arm IIArm II: Partial Breast Irradiation: Partial Breast Irradiation•• Single, intraSingle, intra--operative fraction of 5 operative fraction of 5 GyGy @ 1.0 c@ 1.0 c
University College of LondonUniversity College of London-- London, England London, England --
•• Presented at ASCO 2010Presented at ASCO 2010•• Equivalence @ 4 years demonstrated (ASCOEquivalence @ 4 years demonstrated (ASCOEquivalence @ 4 years demonstrated (ASCO Equivalence @ 4 years demonstrated (ASCO
’10)’10)--Median followMedian follow--up only 2yearsup only 2years•• Lancet 2010 Jul 10;376(9735):91Lancet 2010 Jul 10;376(9735):91--102.102.

10/15/2012
15
GECGEC--ESTROESTRO-- MultiMulti--Center Phase III Trial Center Phase III Trial --
50 Gy whole breast E B I 7 x 4 3 Gy H D R-BT
B C S(n = 1170)
50 G y whole breast E B I+ 10 G y E L E boost
7 x 4.3 G y H D R-BTor 8 x 4 G y H D R-BTor 50 G y P D R-BT
StatusStatus: : Activated May 2004Activated May 2004
AccrualAccrual::1195 enrolled, 2009 (closed),1195 enrolled, 2009 (closed),
GECGEC--ESTROESTRO-- MultiMulti--Center Phase III Trial Center Phase III Trial --
Presented at ESTRO 2012Presented at ESTRO 2012No differences in toxicity at 5 years!No differences in toxicity at 5 years!Outcome data not yet reportedOutcome data not yet reported
Canadian Phase III TrialCanadian Phase III Trial-- Rapid OCOG Trial Rapid OCOG Trial --
•• Arm IArm I: : –– 3D Conformal PBI Only3D Conformal PBI Only
•• Arm IIArm II::C ti l Wh l B t RTC ti l Wh l B t RT–– Conventional Whole Breast RTConventional Whole Breast RT
•• Low risk patientsLow risk patients
•• 2128 Accrual goal2128 Accrual goal
•• 2135 accrued (closed 72135 accrued (closed 7--2011)2011)–– Verbal communication: Tim Whelan, M.D.Verbal communication: Tim Whelan, M.D.

10/15/2012
16
Canadian Phase III TrialCanadian Phase III Trial-- Rapid OCOG Trial Rapid OCOG Trial --
•• 33--year year toxicity, toxicity, cosmesiscosmesis, and , and efficacyefficacy::–– MMulticenter ulticenter study of external beam, accelerated study of external beam, accelerated
partial breast irradiation (APBI) for earlypartial breast irradiation (APBI) for early--stage stage bb i f i i hi f i i hbreast breast cancer using same fractionation scheme as cancer using same fractionation scheme as their phase III trialtheir phase III trial
–– 127 patients127 patients
–– One grade III toxicityOne grade III toxicity
–– 82% good/82% good/excellentcosmesisexcellentcosmesis
-- Interim Analysis on Interim Analysis on CosmesisCosmesis--ASTRO (Oct 2012)ASTRO (Oct 2012)
IntInt J J RadiatRadiat OncolOncol BiolBiol Phys. 2011 Dec 1;81(5):Phys. 2011 Dec 1;81(5):12201220--77
Medical Research CouncilMedical Research Council--UKUK
•• IMPORT Low TrialIMPORT Low Trial
•• Arm IArm I: WBI : WBI -- 2.67 Gy x 15 2.67 Gy x 15 –– Accelerated whole breast RTAccelerated whole breast RTAccelerated whole breast RTAccelerated whole breast RT
•• Arm IIArm II: : –– (1): WBI (1): WBI -- 2.4 Gy x 15 plus 2.4 Gy x 15 plus
–– Concurrent PBI: 2.67 Gy x 15Concurrent PBI: 2.67 Gy x 15
–– (2): PBI: 2.67 Gy x 15(2): PBI: 2.67 Gy x 15
•• Enrolment goals: 1935 casesEnrolment goals: 1935 cases
NSABP BNSABP B--39/RTOG 041339/RTOG 0413Phase III APBI TrialPhase III APBI Trial
Wh l B t I di ti ft P ti l B t I di ti i
Eligible Patients with Lumpectomy
RANDOMIZED
Whole Breast Irradiation after Adjuvant Chemotherapy
50 Gy (2.0 Gy/fraction) or50.4 Gy (1.8 Gy/fraction) to whole
breast, followed by optional boost to > 60 Gy
Partial Breast Irradiation prior to Adjuvant Chemotherapy
For a total of 10 treatments given on 5 days over 5 to 10 days:
34 Gy in 3.4 Gy fractionsInterstitial Brachytherapy or
Mammosite Balloon Catheter or
38.5 Gy in 3.85 Gy fractions3D Conformal External Beam

10/15/2012
17
NSABP BNSABP B--39/RTOG 041339/RTOG 0413
•• OpenOpen: : –– March 21, 2005March 21, 2005
•• AccrualAccrual::
–– October 12, 2012: October 12, 2012: 4171 (4300 total)4171 (4300 total) 97%97%•• Participating SitesParticipating Sites::Participating SitesParticipating Sites: :
–– 78 78 –– NSABPNSABP–– 142 142 –– RTOG/CTSURTOG/CTSU
•• PBI TechniquePBI Technique–– 71.0%: 3D Conformal71.0%: 3D Conformal–– 23.3 %: 23.3 %: MammoSiteMammoSite–– 5.7%: Interstitial5.7%: Interstitial
•• Anticipated closure: 7/2013Anticipated closure: 7/2013
NSABP BNSABP B--39/RTOG 041339/RTOG 0413-- Current Status Current Status --
•• EfficacyEfficacy: : –– Interim analyses performed annually after 44 IBTRsInterim analyses performed annually after 44 IBTRs–– Estimated to be 3.5 years after the trial opensEstimated to be 3.5 years after the trial opensy py p–– Fall 2010Fall 2010
NSABP BNSABP B--39/RTOG 041339/RTOG 0413-- Current Status Current Status --
• Toxicity: –– Adverse events, including toxicities, second primary Adverse events, including toxicities, second primary
cancers and deaths monitored continuously (q/month)cancers and deaths monitored continuously (q/month)y (q )y (q )–– Progress reports presented to Data Monitoring Progress reports presented to Data Monitoring
Committee (DMC) at 6 month intervals (reviewed Committee (DMC) at 6 month intervals (reviewed internally monthly)internally monthly)
•• To date, DMC has found no reason for concernTo date, DMC has found no reason for concern•• Majority of dermatologic toxicities, pain, fibrosisMajority of dermatologic toxicities, pain, fibrosis--cosmesiscosmesis, ,
infection, etc., have been Grade 1 and 2 (<2% grade III)infection, etc., have been Grade 1 and 2 (<2% grade III)
•• Applies to all forms of APBIApplies to all forms of APBI
•• IntInt J J RadiatRadiat OncolOncol BiolBiol Phys. 2010 May 1;77(1):317Phys. 2010 May 1;77(1):317;;
10/15/2012
18
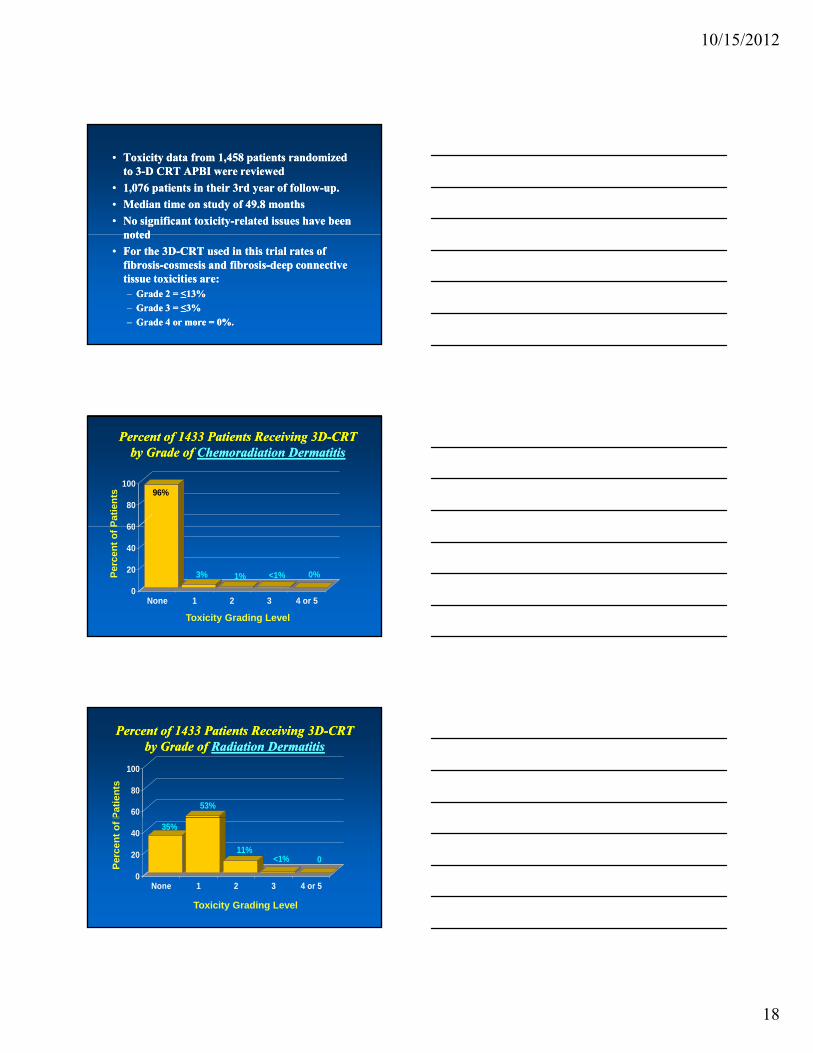
•• Toxicity data from 1,458 patients randomized Toxicity data from 1,458 patients randomized to 3to 3--D CRT APBI were reviewedD CRT APBI were reviewed
•• 1,076 patients in their 3rd year of follow1,076 patients in their 3rd year of follow--up. up.
•• Median time on study of 49.8 monthsMedian time on study of 49.8 months
•• No significant toxicityNo significant toxicity--related issues have been related issues have been notednotednotednoted
•• For the 3DFor the 3D--CRT used in this trial rates of CRT used in this trial rates of fibrosisfibrosis--cosmesiscosmesis and fibrosisand fibrosis--deep connective deep connective tissue toxicities are: tissue toxicities are: –– Grade 2 = ≤13%Grade 2 = ≤13%
–– Grade 3 = ≤3%Grade 3 = ≤3%
–– Grade 4 or more = 0%. Grade 4 or more = 0%.
Percent of 1433 Patients Receiving 3DPercent of 1433 Patients Receiving 3D--CRTCRTby Grade of by Grade of ChemoradiationChemoradiation DermatitisDermatitis
96%
60
80
100
Pat
ien
ts
3% 1% <1% 0%
0
20
40
60
None 1 2 3 4 or 5
Toxicity Grading Level
Per
cen
t o
f P
Percent of 1433 Patients Receiving 3DPercent of 1433 Patients Receiving 3D--CRTCRTby Grade of by Grade of Radiation DermatitisRadiation Dermatitis
53%60
80
100
Pat
ien
ts
35%
11%<1% 0
0
20
40
None 1 2 3 4 or 5
Toxicity Grading Level
Per
cen
t o
f P

10/15/2012
19
Percent of 1433 Patients Receiving 3DPercent of 1433 Patients Receiving 3D--CRTCRTby Grade of by Grade of HyperpigmentationHyperpigmentation
50%44%60
80
100
Pat
ien
ts
44%
7% 0 0
0
20
40
60
None 1 2 3 4 or 5
Toxicity Grading Level
Per
cen
t o
f P
Percent of 1433 Patients Receiving 3DPercent of 1433 Patients Receiving 3D--CRTCRTby Grade of by Grade of IndurationInduration
63%
60
80
100
Pat
ien
ts
27%
8% 2% 0
0
20
40
60
None 1 2 3 4 or 5
Toxicity Grading Level
Per
cen
t o
f P
Percent of 1433 Patients Receiving 3DPercent of 1433 Patients Receiving 3D--CRTCRTby Grade of by Grade of TelangiectasiaTelangiectasia
86%
60
80
100
Pat
ien
ts
11%3% <1% 0
0
20
40
60
None 1 2 3 4 or 5
Toxicity Grading Level
Per
cen
t o
f P

10/15/2012
20
Percent of 1433 Patients Receiving 3DPercent of 1433 Patients Receiving 3D--CRTCRTby Grade of by Grade of UlcerationUlceration
99%
60
80
100
Pat
ien
ts
0 <1% <1% 0
0
20
40
60
None 1 2 3 4 or 5
Toxicity Grading Level
Per
cen
t o
f P
Percent of 1433 Patients Receiving 3DPercent of 1433 Patients Receiving 3D--CRTCRTby Grade of by Grade of FibrosisFibrosis--CosmesisCosmesis
67%
60
80
100
Pat
ien
ts
18%11%
3% 0
0
20
40
60
None 1 2 3 4 or 5
Toxicity Grading Level
Per
cen
t o
f P
Percent of 1433 Patients Receiving 3DPercent of 1433 Patients Receiving 3D--CRTCRTby Grade of by Grade of FibrosisFibrosis--Deep Connective TissueDeep Connective Tissue
68%
60
80
100
Pat
ien
ts
17% 13%2% 0
0
20
40
None 1 2 3 4 or 5
Toxicity Grading Level
Per
cen
t o
f P

10/15/2012
21
APBI ConclusionsAPBI Conclusions
•• Majority of interstitial APBI data in low risk patients Majority of interstitial APBI data in low risk patients are excellentare excellent–– Some 10Some 10--year results availableyear results available
•• Preliminary Preliminary MammoSiteMammoSite data look gooddata look good–– Some 5 Some 5 ––year data availableyear data available–– Monitor for new toxicities/efficacy Monitor for new toxicities/efficacy
•• Insufficient 3D Conformal PBI data available to draw Insufficient 3D Conformal PBI data available to draw any conclusions (any conclusions (proceed cautiouslyproceed cautiously--conflicting dataconflicting data))
•• First completed/published contemporary phase III PBI First completed/published contemporary phase III PBI trial using interstitial APBI shows equivalent results to trial using interstitial APBI shows equivalent results to WBI at 7WBI at 7--years (very small study, however)years (very small study, however)
•• First completed/published contemporary phase III PBI First completed/published contemporary phase III PBI trial using singletrial using single--fraction IORT shows equivalent fraction IORT shows equivalent results to WBI at 4results to WBI at 4--years years
APBI ConclusionsAPBI Conclusions
•• Remaining QuestionsRemaining Questions::–– Mature phase III data will not be available for several Mature phase III data will not be available for several
years (2015years (2015--2020)2020)–– What should we do until additional phase III data are What should we do until additional phase III data are pp
available?available?–– ASBS, ABS, & several European groups provide guidelines ASBS, ABS, & several European groups provide guidelines
for the use of APBI offfor the use of APBI off--protocol in selected patients protocol in selected patients –– ASTRO consensus panel formed with published guidelines ASTRO consensus panel formed with published guidelines
now availablenow available•• J Am Coll Surg. 2009 Aug; 209(2):269J Am Coll Surg. 2009 Aug; 209(2):269--7777•• Int J Radiat Oncol Biol Phys. 2009 Jul 15;74(4):987Int J Radiat Oncol Biol Phys. 2009 Jul 15;74(4):987--1001.1001.
Prospective Randomized TrialsProspective Randomized TrialsConservative Surgery PlusConservative Surgery Plus
RT vs Mastectomy for Early Stage Breast CancerRT vs Mastectomy for Early Stage Breast Cancer
Trial # Pts Time Period
Stage Surgery Systemic Therapy
NSABP 1219 76-84 I-II WE, MRM Melphalan, 5FU
Milan 701 73-80 I Q, RM CMF
Q,
NCI
237 79-87 I-II LE, MRM AC
EORTC
868 80-86 I-II LE, MRM CMF
IGR
179 72-80 I WE, MRM None
DBCG 904 83-89 I-III WE, Q, MRM
CMF, T

10/15/2012
22
Prospective Randomized TrialsProspective Randomized Trials
TechniqueTechnique # Phase III # Phase III TrialsTrials
# of Patients # of Patients EnrolledEnrolled
BCT vs MastectomyBCT vs Mastectomy 66 4,1084,108
AWBI vs WBIAWBI vs WBI 33 3,4493,449
APBI vs WBIAPBI vs WBI 99 14, 20014, 200
APBI ConclusionsAPBI Conclusions
•• Please support enrollment highPlease support enrollment high--risk patients risk patients on the NSABP B39/RTOG 0413 phase III on the NSABP B39/RTOG 0413 phase III APBI t i l!APBI t i l!APBI trial!APBI trial!
•• Proceed conservatively until additional data Proceed conservatively until additional data are available (conflicting 3D data)are available (conflicting 3D data)