update on acute kidney injury - rcp london
TRANSCRIPT

Royal Derby Hospital
Dr Nick Selby
Associate Professor of Nephrology
Centre for Kidney Research and Innovation
Division of Health Sciences and Graduate Entry Medicine
University of Nottingham
Royal Derby Hospital
Update on Acute Kidney Injury

Royal Derby Hospital

Royal Derby Hospital
5-15% of hospital admissions, mortality ~25% and >35% in AKI3
High incidence, poor outcomes
No specific therapies
Silent presentation, variation in
care

Royal Derby Hospital
AKI is distributed across all specialties
Only 7.5% of patients under nephrology
Selby NM et al CJASN 2012; 7(4): 533

Royal Derby Hospital
https://www.thinkkidneys.nhs.uk

Royal Derby Hospital
AKI detection
Intranet Guidelines
Streamlined nephrology
referral Care bundles
Education programme

Royal Derby Hospital
Better outcomes in patients with AKI care bundle
Kolhe NV, Staples D, Reilly T, Merrison D, Selby NM, et al. (2015) Impact of Compliance with a Care Bundle on Acute Kidney Injury Outcomes: A Prospective Observational Study. PLoS ONE 10(7): e0132279. doi:10.1371/journal.pone.0132279

Royal Derby Hospital What is AKI?
AKI stage Serum creatinine criteria Urine output criteria
1 An increase of more than 26mol/l above baseline (within 48hrs) OR An increase of more than or equal to 1.5 to 2 fold from baseline
<0.5mg/kg/hr for at least 6hours
2 An increase of more than or equal to 2 to 3 fold from baseline
<0.5mg/kg/hr for at least 12hours
3 An increase of more than 3 fold from baseline OR AKI with creatinine 355mol/l OR Initiation of RRT
<0.3mg/kg/hr for at least 24hours OR Anuria for >12hours
2727
782
636
Number of patients per annum sustaining each stage of AKI in 1000-bedded hospital
total: 4145
1. No mention of cause 2. What to do when no
baseline available? 3. Interpreting small
changes in creatinine in clinical practice

Royal Derby Hospital Why such small changes in creatinine?
• Even small changes in renal function are significant
• Multiple studies with same findings
• Findings persist after adjustment for co-morbidities
©2005 by American Society of Nephrology
Chertow G M et al. JASN 2005;16:3365-3370
26-35mol/l 88-167mol/l 44-80mol/l >176mol/l
>44µmol/l increase in s.creat – 6 fold increase in odds of death

Royal Derby Hospital
Small changes in creatinine can reflect larger changes in GFR
CV
CV CV
20% drop in GFR
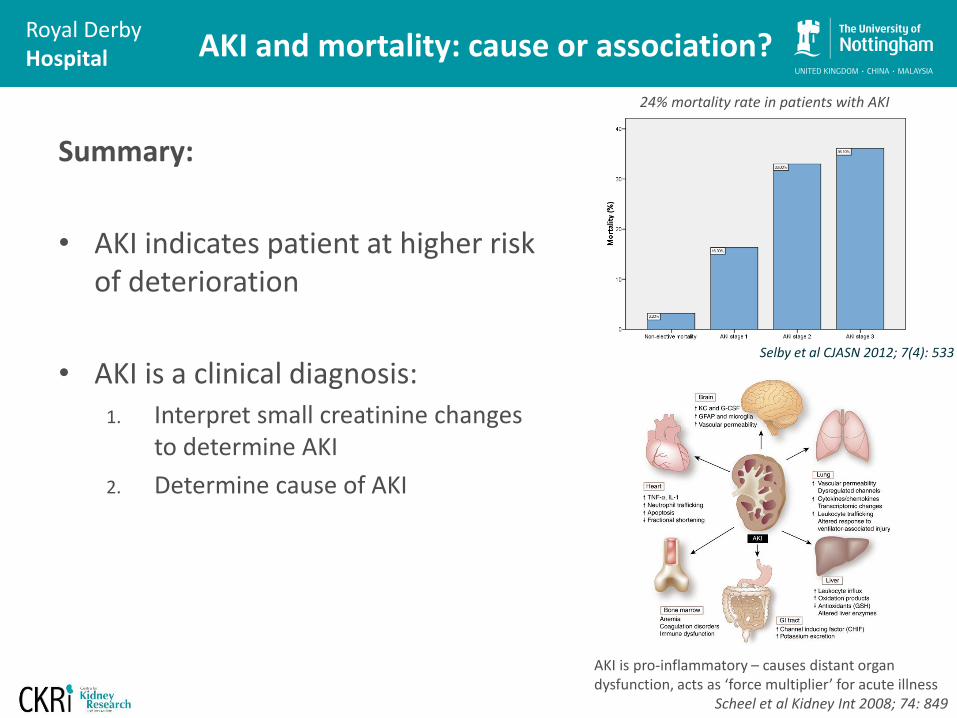
Royal Derby Hospital AKI and mortality: cause or association?
Summary:
• AKI indicates patient at higher risk of deterioration
• AKI is a clinical diagnosis: 1. Interpret small creatinine changes
to determine AKI
2. Determine cause of AKI
Selby et al CJASN 2012; 7(4): 533
24% mortality rate in patients with AKI
AKI is pro-inflammatory – causes distant organ dysfunction, acts as ‘force multiplier’ for acute illness
Scheel et al Kidney Int 2008; 74: 849

Royal Derby Hospital Causes of AKI
Pre-renal
• Hypotension
• Sepsis
• Volume depletion
• Bleeding
• CCF
• Hepato-renal syndrome
Intrinsic renal disease
• Tubular
Ischaemic ATN
Drugs/toxins/Contrast
Rhabdomyolysis
Tumour lysis
Tubulo-interstitial nephritis
Myeloma
• Vascular – large vessels
Renal artery thrombosis
Athero/Cholesterol emboli
Small vessels and glomeruli
GN or Vasculitis
HUS/TTP
Malignant BP
Post renal
• Bladder outflow
(including blocked catheter)
• Retroperitoneal disease
• Stones (rare)
OVERLAP

Royal Derby Hospital
Relative proportions of causes of AKI
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pre-renal Obstruction GN/vasculitis TIN Atheroemboli
Perc
enta
ge
ATN Pre-existing CKD
Liano F; Pascual J. Kidney Int 1996 Sep;50(3):811-8.
*
* Includes toxic and ischaemic ATN
80-90% of AKI due to pre-renal, toxic or post-renal
causes

Royal Derby Hospital
Efferent arteriole
Filtrate (urine)
Afferent arteriole
Pre-renal factors: response to renal hypoperfusion
Renin Angiotensin 1
Angiotensin 2
Aldosterone
Angiotensin 2 will cause vasoconstriction efferent > afferent; GFR maintained over range of arterial pressures Prostaglandins prevents afferent vasocontriction

Royal Derby Hospital
Effect of ACEI and ARB
• Effect on angiotensin 2 on efferent vessels is lost
• Glomerular pressure decreases
• Filtration fraction falls
• GFR falls
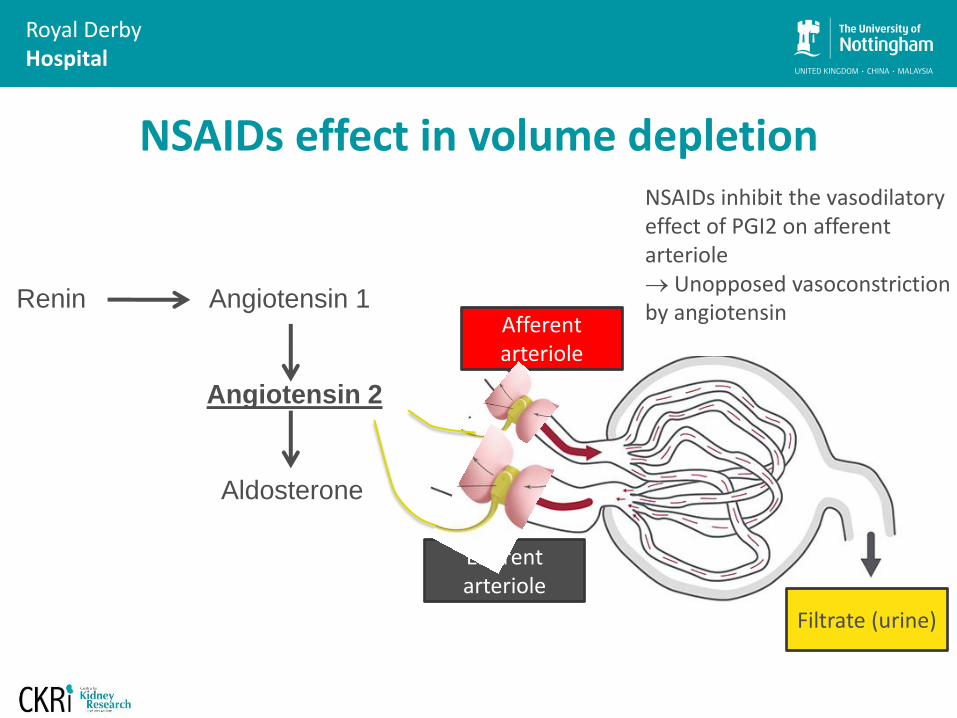
Royal Derby Hospital
Efferent arteriole
Filtrate (urine)
Afferent arteriole
Renin Angiotensin 1
Angiotensin 2
Aldosterone
NSAIDs inhibit the vasodilatory effect of PGI2 on afferent arteriole Unopposed vasoconstriction by angiotensin
NSAIDs effect in volume depletion

Royal Derby Hospital
Case • 74yr old lady
• Admitted by GP: abnormal renal
function on routine bloods
• Felt well • No systemic or urinary symptoms • Good oral intake
• PMH:
Hyperlipidaemia Hypertension Recent Ix for weight loss, NAD
• DH: Amlodipine 5mg od Simvastatin 20mg od Omeprazole 20mg od
• Urine dip:
1+ protein only
• Other blood tests unremarkable
• Ultrasound kidneys: normal
6m ago
5wks ago
Now
Creatinine 82 87 246
What are the possible causes of AKI? Which is most likely?

Royal Derby Hospital
ALWAYS DIP THE URINE
NAD
Pre-renal Post-renal Myeloma
Tubulo-interstitial dis (Renovascular)
Blood and protein
Still can be ATN, but raises the possibility of
inflammatory renal disease
e.g. vasculitis
Proteinuria (PCR>3)
(=Protein loss>3g per day)
Definitely glomerular
Urine dip is not to look for infection, it’s to help with diagnosis

Royal Derby Hospital
Drug induced Tubulointerstitial nephritis
• Often occurs without classic symptoms • Sometimes – only clue is lack of other causes
plus temporal relationship with drug
• Urine dip: 1+ leuk, blood, protein Can be NAD
• Antibiotics, PPI, NSAIDs, diuretics, allopurinol, ++
• Diagnosis: usually needs renal biopsy prior to
steroid therapy

Royal Derby Hospital
Mechanisms whereby a drug (or one of its metabolites) can induce acute interstitial nephritis
(A) The drug can bind to a normal component of the tubular basement membrane (TBM) and act as an allergen.
(B) The drug can mimic an antigen normally present within the TBM or the interstitium and induce an immune response that will also be directed against this antigen.
Allergen

Royal Derby Hospital Case
• 65yr old male • Undergoes primary PCI
for STEMI
• Contrast volume: 138ml
• BP 142/74, maintained
• Day 3 develops AKI: creatinine 294µmol/l (previously 116)
Other features: • Urine dip: NAD • Discomfort in toes: on
examination appear dusky
• Notable blood tests: • Eosinophils: 0.83x109/l () • C3 low
What are the possible causes of AKI? Which is most likely?

Royal Derby Hospital
AKI and eosinophilia
• Acute TIN
• Cholesterol emboli
• Churg-Strauss syndrome
• DRESS syndrome
• Lymphoma
• Hypereosinophilic syndrome
• Schistosomiasis
• Vascular risk factors, AAA, vascular intervention (?anti-coagulation)
• Skin, AKI; sometimes abdominal symptoms, Hollenhorst plaque
• Treatment is largely risk factor modification
Cholesterol emboli

Royal Derby Hospital Case
• 67 year old man
• Brought to A+E
• Found at home on the floor
• House unkempt, empty whiskey bottles
• What would you expect to find in his urine?
Previous
Hb 14.1
WBC 18
Plt 163
Na 141
K 6.1 4.2
Ur 29 7
Creat 301 78
CCa 2.11
PO4 2.2
ALT 250
CK 24,670

Royal Derby Hospital
Rhabdomyolysis
• +ve urinalysis blood, few RBC on microscopy
• Myoglobinuria absent in 25% patients with rhabdo
• Mx Recognise and treat fluid and
electrolyte disturbances Identify cause
Some less obvious causes e.g.: • Statins, precipitated by drug interactions • Viral infection • Hypothyoidism
Look out for compartment syndrome

Royal Derby Hospital
Recreational drugs, poisoning and AKI
• Heroin, cocaine etc. Cocaine cut with levamisole – can induce ANCA assoc. vasculitis variant (MPO
and PR3 positivity)
• Ecstasy Rhabdo, circulatory collapse (seratonin syn), hyponatraemia (ADH release)
Fahal IH. BMJ 305: 29, 1992
• Legal highs Reports of Mephadrone (MCAT) causing AKI requiring dialysis
Rhidian BMJ Case Rep 2013
Bath salts (methylenedioxypyrovalerone, MDPV) - rhabdo Adebamiro Am J Kidney Dis. 2012 Feb;59(2):273
SPICE (synthetic cannabanoid) causing ATN Bhanushali Clin J Am Soc Nephrol 8: 523–526, 2013
• Poisoning:
Ethylene glycol: raised anion gap acidosis, raised osmolar gap, high lactate on ABG
Paracetamol (delayed presentation)

Royal Derby Hospital
Indicators of ‘inflammatory’ AKI
ACTIVE URINE More than 2+ of blood and protein
VASCULITIC RASH
SYSTEMIC SYMPTOMS
Often present for months – myalgias, arthralgias, malaise
EPISTAXIS, SINUSITIS, HAEMOPTYSIS
Low platelets, high calcium, eosinophilia

Royal Derby Hospital
IV Fluids and AKI
Which type?
How much?
How fast?

Royal Derby Hospital
The SAFE Study Investigators. N Engl J Med 2004;350:2247-2256.
No benefit of colloids over crystalloids
Perel. Cochrane review 2013
No benefit with colloids Possible suggestions of harm Less of a difference in fluid volume than would have been anticipated
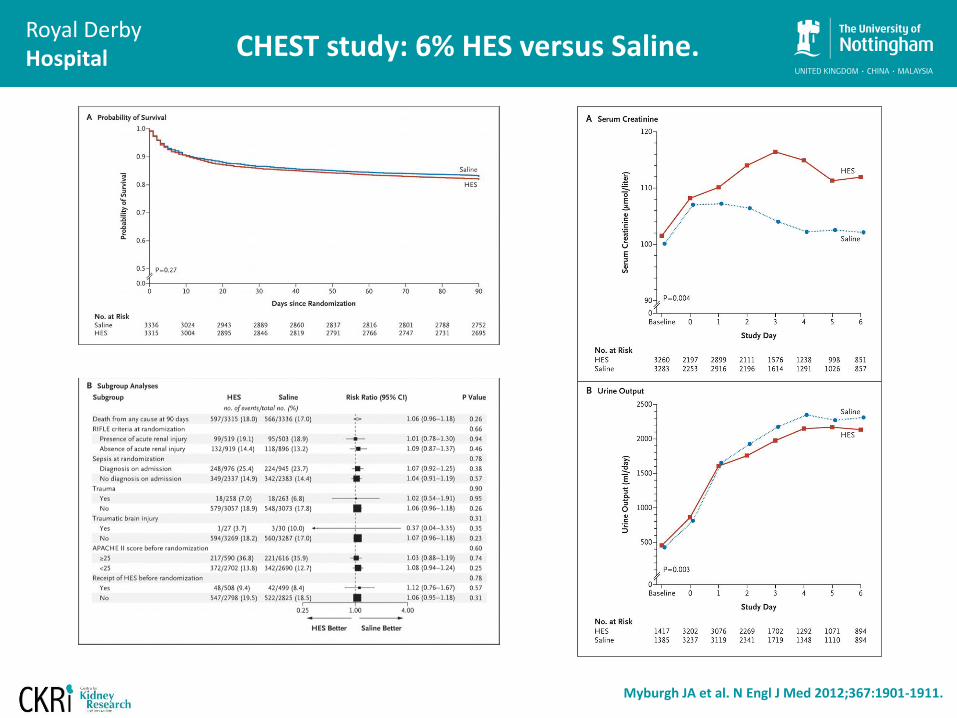
Royal Derby Hospital
Myburgh JA et al. N Engl J Med 2012;367:1901-1911.
CHEST study: 6% HES versus Saline.

Royal Derby Hospital
Perner A et al. N Engl J Med 2012;367:124-134.
Worse outcomes with 6% HES versus Ringers lactate – 6S trial

Royal Derby Hospital
From ~1million patients, only 10% received one type of fluid only
• Retrospective database study
• Patients: SIRS needing >0.5L iv fluids
• Patients receiving saline were propensity matched to those receiving Ringers lactate or Plasmalyte
In-hospital mortality higher with saline 3.27 % vs. 1.03 %, p<0.001 No difference in AKI rates Similar study in post-surgical patients did report increased RRT
‘Toxicity’ of saline?

Royal Derby Hospital
Chloride liberal versus restrictive approach
• Single ICU
• Switched from chloride liberal to chloride restrictive regime
• Less AKI, less RRT after the switch
• Number of limitations with this study
Yunos JAMA 2012; 308(15):1566-1572

Royal Derby Hospital
Saline and renal perfusion
• 12 healthy males
• Randomised cross-over study 2L of IV fluid in 1hr
• MR with ASL used to measure perfusion that reduced with saline but not with Plasmalyte
Chowdhury Annals Surg 2012; 256 (1): 18–24
Perfusion Map

Royal Derby Hospital
• Blinded cluster randomised controlled trial
• Saline versus Plasmalyte-148
• 4 ICUs in New Zealand
• Primary outcome: incidence of AKI
• Number of secondary endpoints and pre-planned subgroup analyses
• RRT was an exclusion criterion
• 2278 patients randomised
• 1162 versus 1116
• No differences between groups, generally low co-morbidity
• ~70% were post-operative
JAMA 2015;314(16):1701-1710

Royal Derby Hospital
Results Median fluid volumes 2000 mL Mortality 7.6% versus 8.6%, p=0.4 No differences in any subgroups No difference in acidosis
Blinding failed No sample size calculation
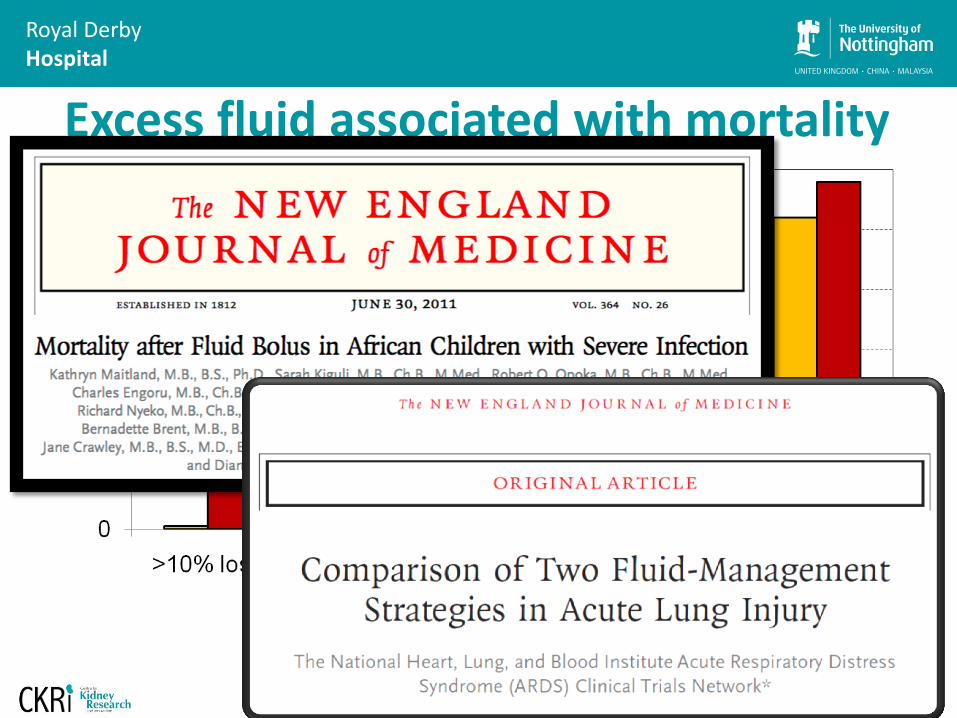
Royal Derby Hospital
Excess fluid associated with mortality
Adapted from Bouchard et al, Kidney Int 2009.
Adjusted odds ratio for death associated with fluid
overload at dialysis initiation = 2.07
Royal Derby Hospital Conclusions
• AKI is a major challenge; evidence emerging to support efforts to reduce variation in quality of AKI care
• AKI identifies patients at higher risk of adverse outcomes; need a holistic approach
• Clinical interpretation remains key and guides subsequent management: Is this AKI? What is the cause of AKI?
• The composition of fluid may affect the risk of AKI
No benefit of colloids Starch harmful Convincing evidence for saline avoidance remains elusive
• Fluid resuscitation should be weighed against potential for volume overload
[email protected] www.nottingham.ac.uk/research/groups/renal