update on food allergy and asthma jason friesen md oregon allergy associates oak street medical
TRANSCRIPT
Update on Food Allergyand Asthma
JASON FRIESEN MDOREGON ALLERGY ASSOCIATESOAK STREET MEDICAL
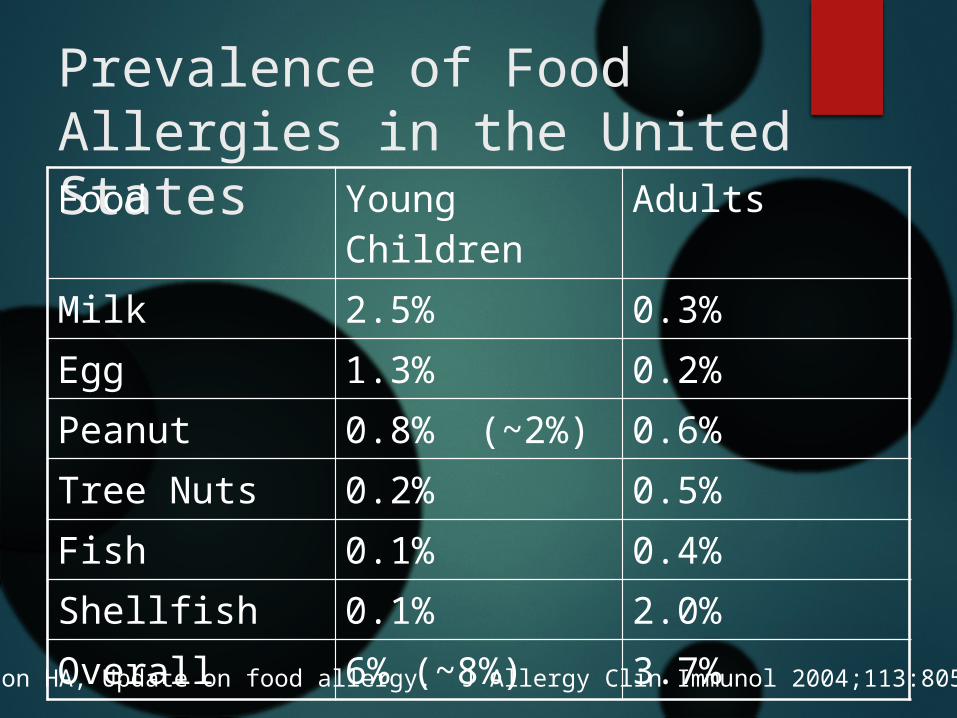
Prevalence of Food Allergies in the United StatesFood Young Children Adults
Milk 2.5% 0.3%
Egg 1.3% 0.2%
Peanut 0.8% (~2%) 0.6%
Tree Nuts 0.2% 0.5%
Fish 0.1% 0.4%
Shellfish 0.1% 2.0%
Overall 6% (~8%) 3.7%
Sampson HA, Update on food allergy. J Allergy Clin Immunol 2004;113:805-19

Perceived prevalence of Food Allergy
A whole population birth cohort was established on the Isle of Wight.
Parents reported food hypersensitivity in 25.8% of their children.
The actual incidence of food hypersensitivity confirmed by open food challenge or DBPCFC at one year was 4.0%.
Venter C, Pereira B, Grundy J, Clayton CB, Roberts G, Higgins B, et al. Incidence of parentally reported and clinically diagnosed food hypersensitivity in the first year of life. J Allergy Clin Immunol 2006;117:1118-24.
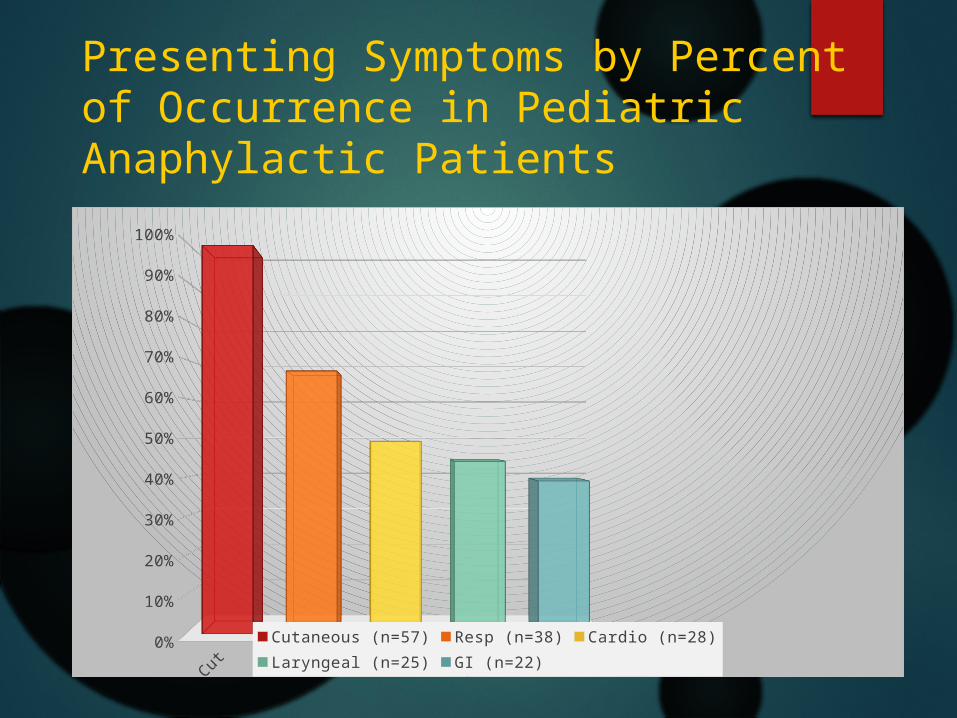
Presenting Symptoms by Percent of Occurrence in Pediatric Anaphylactic Patients
Cuta-neous (n=57)
Resp (n=38)
Cardio (n=28)
Laryngeal (n=25)
GI (n=22)0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Cutaneous (n=57) Resp (n=38) Cardio (n=28)Laryngeal (n=25) GI (n=22)
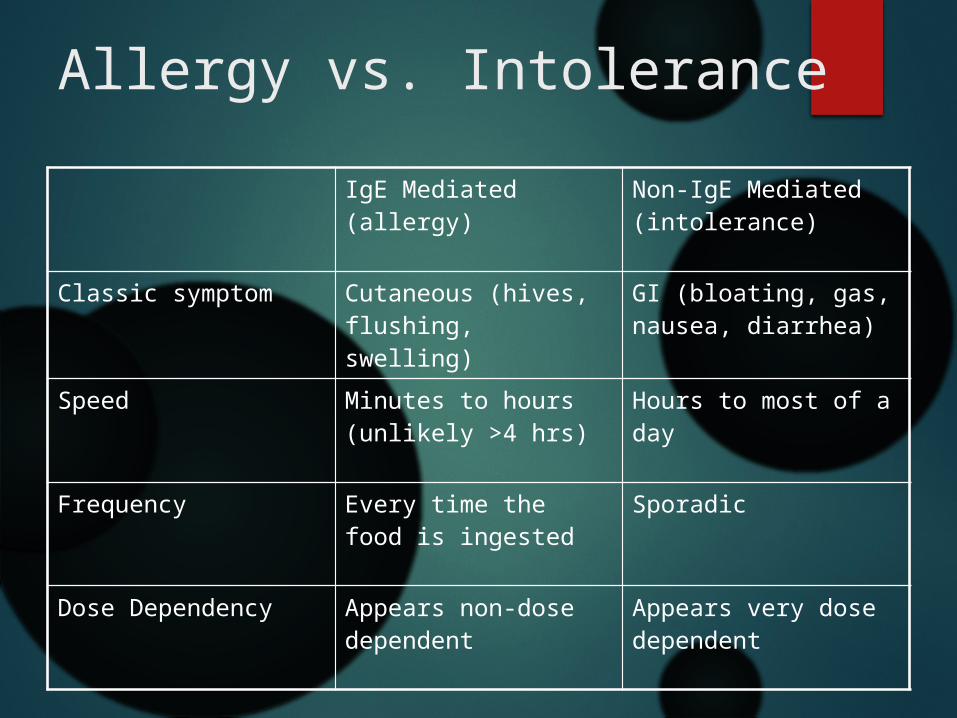
Allergy vs. Intolerance
IgE Mediated (allergy) Non-IgE Mediated (intolerance)
Classic symptom Cutaneous (hives, flushing, swelling)
GI (bloating, gas, nausea, diarrhea)
Speed Minutes to hours (unlikely >4 hrs)
Hours to most of a day
Frequency Every time the food is ingested
Sporadic
Dose Dependency Appears non-dose dependent
Appears very dose dependent
Casual contact with peanut
Thirty highly allergic children underwent the challenges.
None experienced a systemic or respiratory reaction. Erythema (3 subjects), pruritus without erythema (5 subjects), and wheal-and-flare reactions (2 subjects) developed only at the site of skin contact with peanut butter.
“From this number of participants, it can stated with 96% confidence that at least 90% of highly sensitive children with peanut allergy would not experience a systemic-respiratory reaction from casual exposure to peanut butter.”
J Allergy Clin Immunol. 2003 Jul;112(1):180-2.
Airborne peanut exposure
Participants consumed peanuts in various forms to simulate situations that might create airborne peanut allergen. To simulate a school cafeteria setting,
participants consumed peanut butter sandwiches.
For environments similar to sporting events, participants shelled and consumed roasted peanuts. Participants were encouraged to discard peanut shells on the floor and were also allowed to walk on the shells during many of the sessions.
To simulate the environment on commercial airliners, each participant opened 15 bags of unshelled peanuts in small, ½-oz packages and consumed the nuts.
J Allergy Clin Immunol 2004;113:973-6.
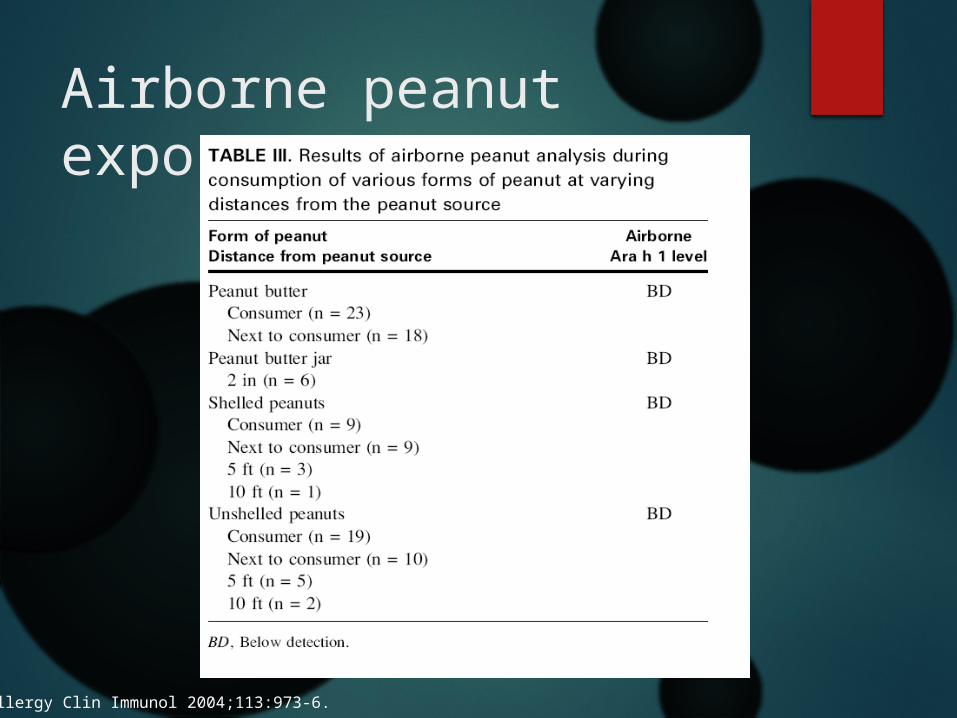
Airborne peanut exposure
J Allergy Clin Immunol 2004;113:973-6.
Severe and fatal reactionsFear vs. dread “Social scientists have known for a long time
that there are dangers whose risks we underestimate, and there are dangers whose risks we overestimate. They talk about the difference between things that we fear and things that we dread.
“We fear cancer and heart disease and traffic crashes, but psychopaths and serial killers and airplane crashes are things that we dread. So when a danger seems like it's inexplicable, when we have absolutely no control over it, when suddenly, out of the blue, it causes mass casualties, this causes not fear, but dread. And when it comes to dread, that's when we tend to overestimate the risks.”

Incidence of fatal food reactions
In food-allergic people, fatal food anaphylaxis has an incidence rate of 1.81 per million person-years (95%CI 0.94, 3.45; range 0.63, 6.68). In sensitivity analysis with different estimated food allergy prevalence, the incidence varied from 1.35 to 2.71 per million person-years. At age 0–19, the incidence rate is 3.25 (1.73, 6.10; range 0.94, 15.75; sensitivity analysis 1.18–6.13).
Putting it in perspective
Shark attack: 0.1 per million person years
Death by lightning: 0.22 per million person years
Fatal anaphylaxis: 1-3 per million person years (in allergic persons)
Fatal influenza: 100 per million person years (in the US)
Using envelope math we can expect a food allergy death in a child every 7-20 years.
Risk for Fatal Food Reaction
Large majority of victims were adolescents or young adults
A prior history of allergy to the specific food is very common.
Asthma appears to be a strong risk factor. Epinephrine needs to be given in a timely
manner. From Sampson’s original 13 cases: “The six patients
who died had symptoms within 3 to 30 minutes of the ingestion of the allergen, but only two received epinephrine in the first hour. All the patients who survived had symptoms within 5 minutes of allergen ingestion, and all but one received epinephrine within 30 minutes.”
Peanut and tree nut caused 95% of fatalities.Fatal and near-fatal anaphylactic reactions to food in children and adolescents.Sampson HA - N Engl J Med - 6-AUG-1992; 327(6): 380-4
Epinephrine
Epinephrine is safe in children. It may cause pharmacologic adverse
effects such as anxiety, fear, restlessness, headache, dizziness, palpitations, pallor, and tremor.
Rarely, and especially after overdose, it may lead to ventricular arrhythmias, angina, myocardial infarction, pulmonary edema, sudden sharp increase in blood pressure, and intracranial hemorrhage.
There is, however, no absolute contraindication to epinephrine use in anaphylaxis.
F. Estelle R. Simons, J Allergy Clin Immunol 2004;113:837-44.)

Epinephrine
EpiPen Jr 0.15mg is optimally dosed for a 15kg child (50%ile 3 years old).
EpiPen 0.30mg is optimally dosed for a 30kg child (50%ile 12 years old).
Personally I switch up at 20 kg (45 pounds) (50%ile 6 years old).
The 5/8” length may be too short to ensure intramuscular injection of epinephrine in obese individuals.
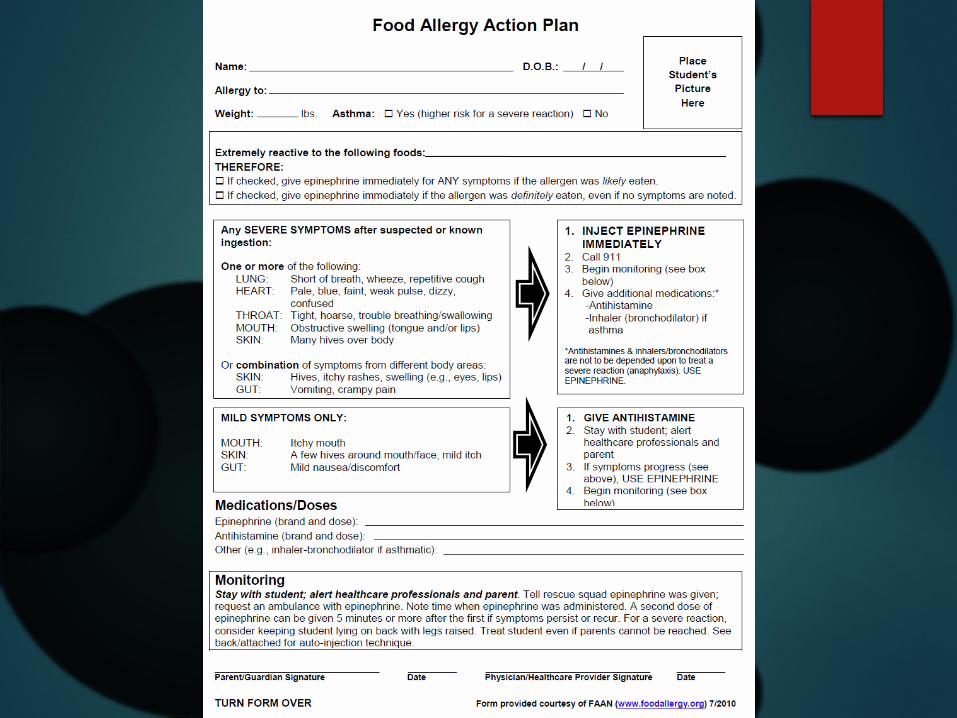
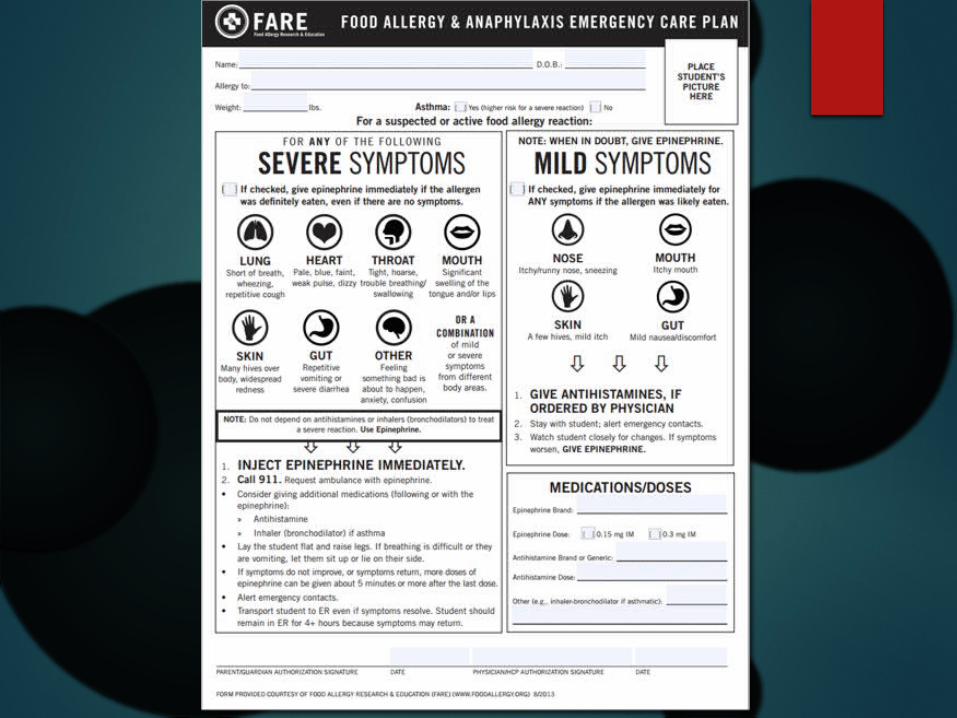
Practical tips about food allergy action plans
Low threshold for giving epinephrine: Pros:
Early administration for life threatening cases.
Low risk of significant side effects in children
Simpler decision making for non-medical personnel
Decreased liability?
Cons: Potential cost with ER/ambulance
Psychological burden of increased fear
High threshold for giving epinephrine: Pros:
Decreased inappropriate uses of epinephrine
Less “knee jerk”
Cost savings of used epi-pen
Cons:
Increased risk of delayed epi in life threatening case
More decision making required
Increased liability?
The LEAP studySHOULD IT HAVE BEEN CALLED THE “TURN THE WORLD UPSIDE DOWN STUDY”?
LEAP study
Current guidelines recommended avoiding allergenic foods such as peanut or shellfish until age three for siblings of allergic patients.
Is this the right advice? In the UK women were adviced to avoid eating
peanuts while pregnant and avoid giving peanuts to children until three yet the incidence of peanut allergy continued to climb.
Jewish mothers in the UK were more likely to have peanut allergic kids than Jewish mothers in Israel. One difference was kids in Israel have early exposure to peanut.

LEAP study
LEAP Study
640 infants between 4 and 11 months randomized to eat at least 6g peanut protein per week.
All had eczema, egg allergy or both.
Stratified between negative skin prick and positive skin prick.
LEAP Study
530 infants had negative skin prick result. 13.7% of avoidance group developed peanut
allergy.
1.9% of consumption group developed peanut allergy. (86% risk reduction)
98 infants had positive skin prick results. 35.3% in avoidance group
10.6% in consumption group (70% risk reduction)
Siblings of peanut allergic children
Prick test early
If negative, introduce peanut Practical issues with keeping peanut in house to
feed sibling while keeping it away from allergic child.
If positive, consider challenge in office or avoidance.
Oral immunotherapy
• The primary outcome, desensitisation, was recorded for 62% in the active group and none of the control group after six months. 84% of the active group tolerated daily ingestion of 800 mg protein (equivalent to roughly five peanuts).
Happening in Oregon
Tolerance vs. Desensitization? “bite proof”
Cost and coverage
Asthma
The September epidemic of asthma hospitalizations: School children as disease vectorsNeil W Johnston, MSc, Sebastian L. Johnston, MD, PhD, Geoff R. Norman, PhD, Jennifer Dai, MSc, and Malcolm R. Sears, MB, ChB
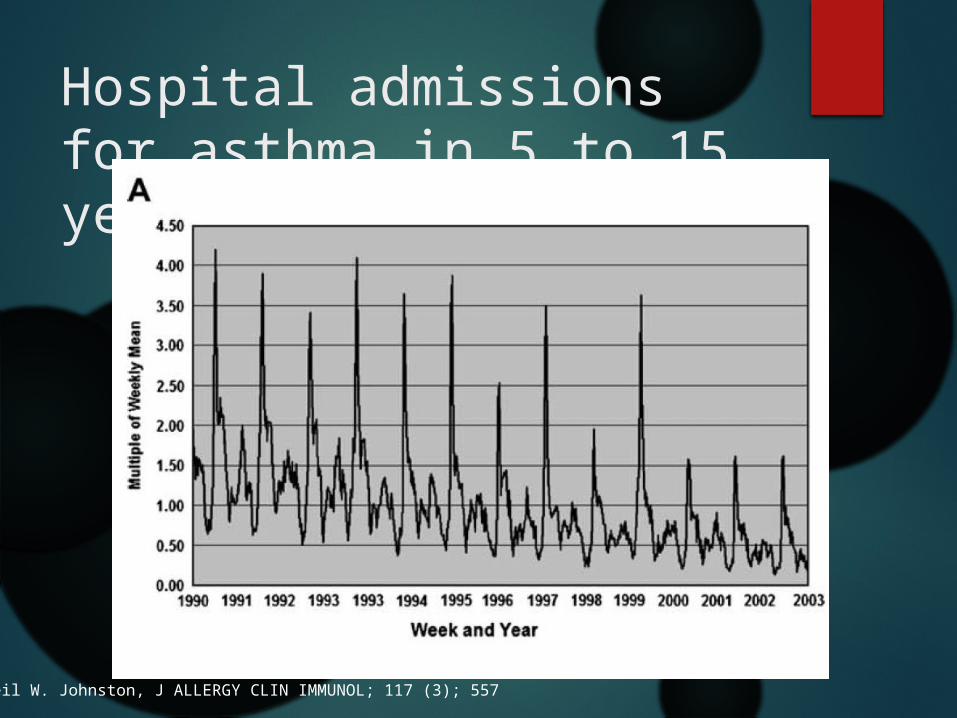
Hospital admissions for asthma in 5 to 15 year olds
Neil W. Johnston, J ALLERGY CLIN IMMUNOL; 117 (3); 557
Other Studies find the same thing
This effect has been noted across the northern hemisphere: Finland, Canada, United Kingdoms, United States,
Mexico, Israel, Trinidad.
A parallel post-summer vacation effect has been noted in the southern hemisphere as well: South Africa, Australia, New Zealand
Noncompliance?
Summer tends to have the fewest asthma admissions.
Schedules for school kids are much more chaotic making routines harder to keep.
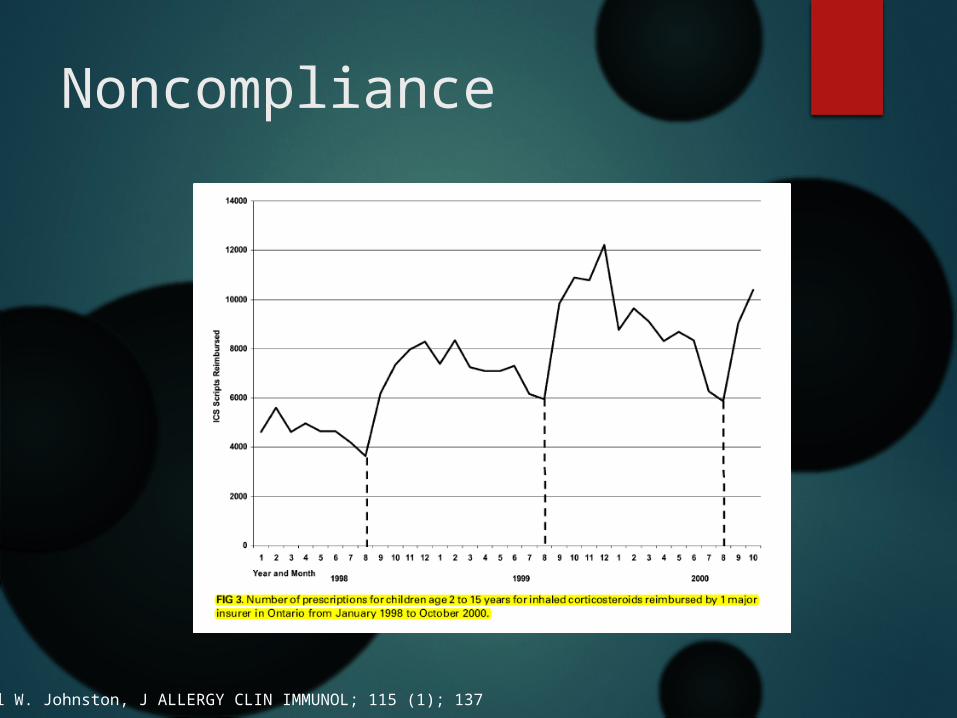
Noncompliance
Neil W. Johnston, J ALLERGY CLIN IMMUNOL; 115 (1); 137
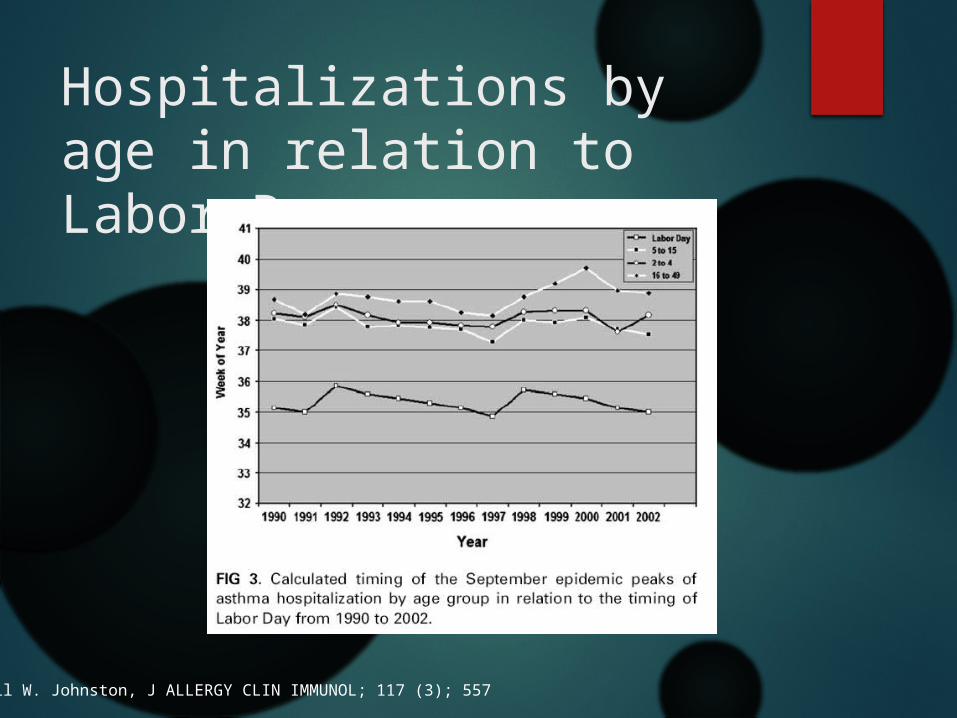
Hospitalizations by age in relation to Labor Day
Neil W. Johnston, J ALLERGY CLIN IMMUNOL; 117 (3); 557
Short-Course Montelukast for Intermittent Asthma in ChildrenA Randomized Controlled TrialColin F. Robertson, David Price, Richard Henry, Craig Mellis, Nicholas Glasgow,Dominic Fitzgerald, Amanda J. Lee, Jane Turner, and Melissa Sant
Methods
Double-blind, randomized, placebo-controlled trial comparing 7-20 days of montelukast at the first sign of a URI.
220 children age 2-14 randomized.
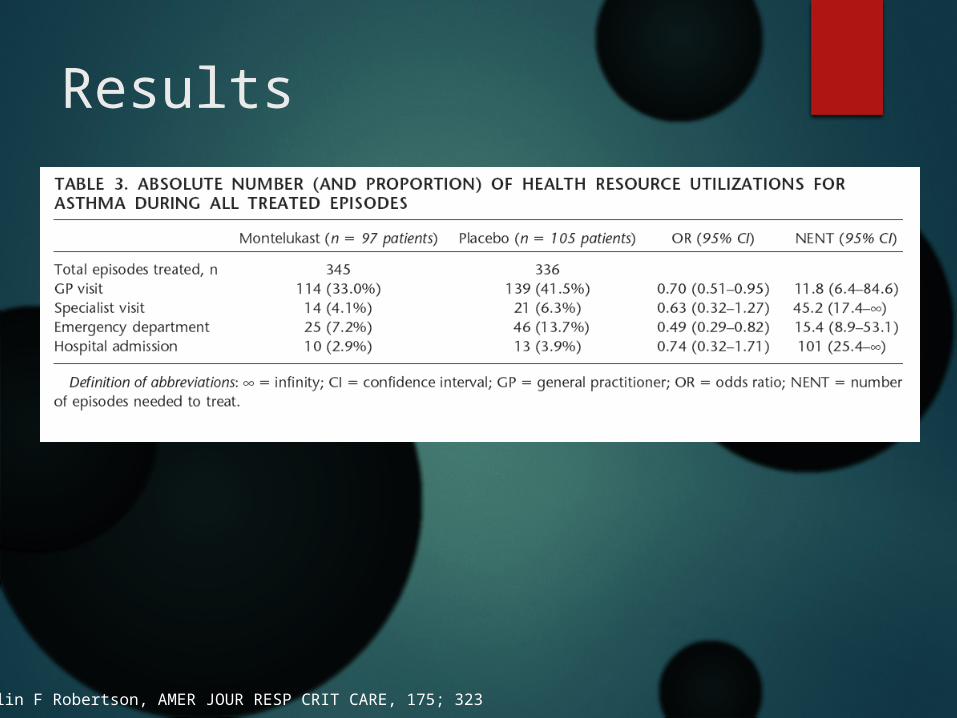
Results
Colin F Robertson, AMER JOUR RESP CRIT CARE, 175; 323
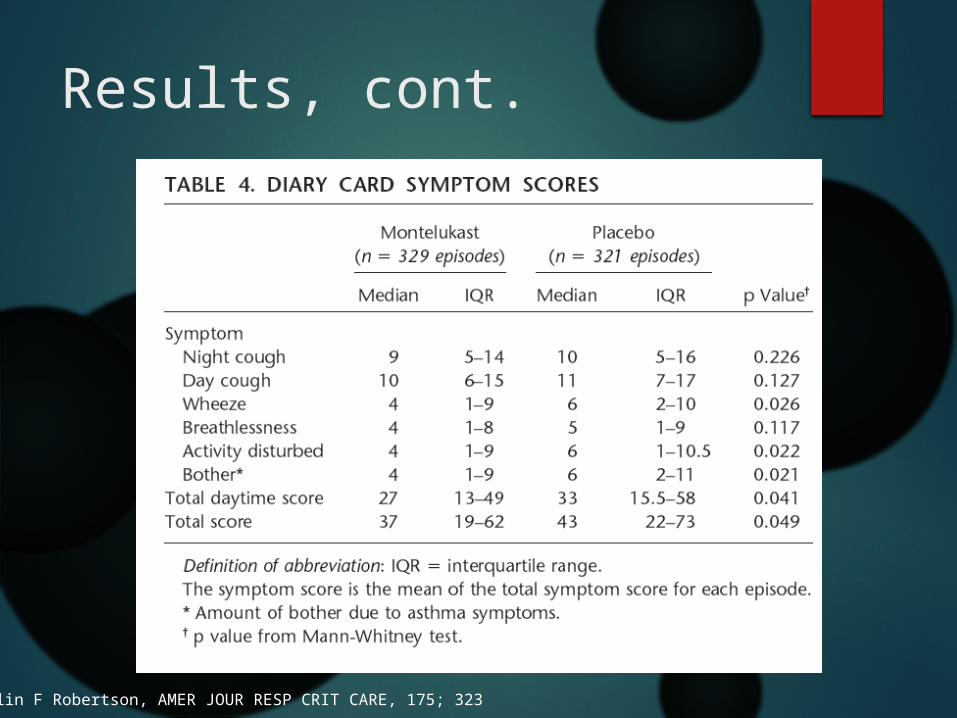
Results, cont.
Colin F Robertson, AMER JOUR RESP CRIT CARE, 175; 323
Conclusion
“For 100 patient episodes treated with montelukast, there would be an avoidance of one hospital admission, six emergency room attendances, two specialist consultations, and eight GP visits.”
Quadrupling the Dose of Inhaled Corticosteroid to Prevent Asthma Exacerbations: A Randomized, Double-blind, Placebo-controlled,Parallel-group Clinical Trial
Janet Oborne, Kevin Mortimer, Richard B. Hubbard, Anne E Tattersfield, and Tim WHarrison.University of Nottingham, Nottingham, United Kingdom
J Obonre, Am J Respir Crit Care Med Vol 180. pp 598–602, 2009
Results cont.
“Among the 94 participants who started the study inhaler, quadrupling the dose of inhaled corticosteroid led to a marked reduction in the need for oral corticosteroids (21 vs. 50%, relative risk reduction, 57%).”
Practical consideration: Running through a month’s worth of ICS in one week. Cost and insurance headache.

Conclusions
September asthma A real event
Occurs roughly three weeks after Labor Day.
Likely virally driven, although summer non-compliance may play a factor.
Having kids on their controller before Labor Day may be beneficial to avoiding an exacerbation.
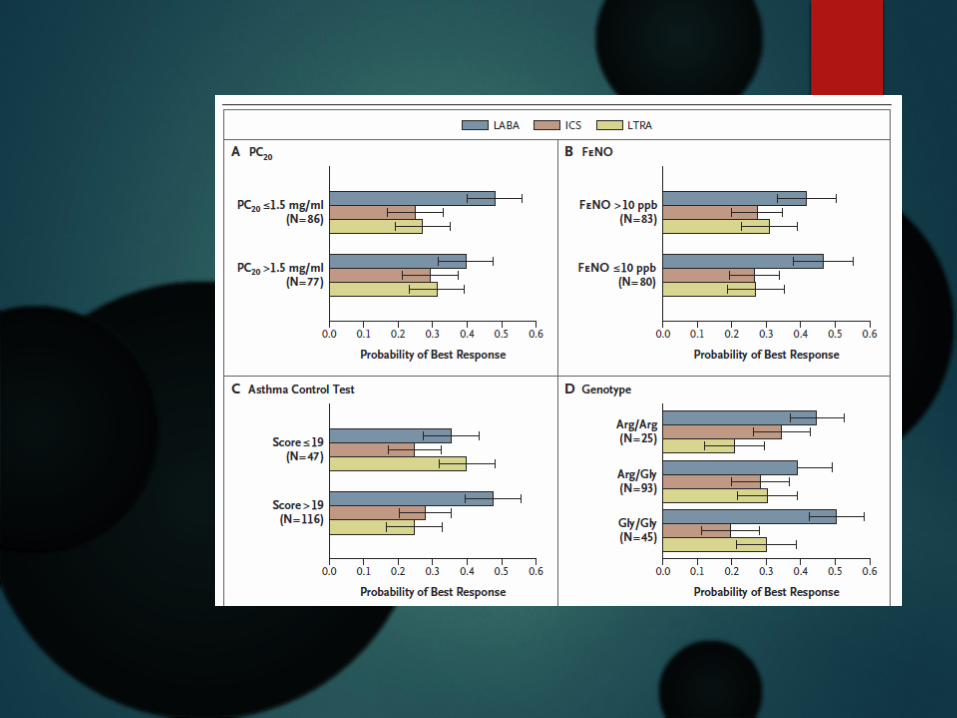
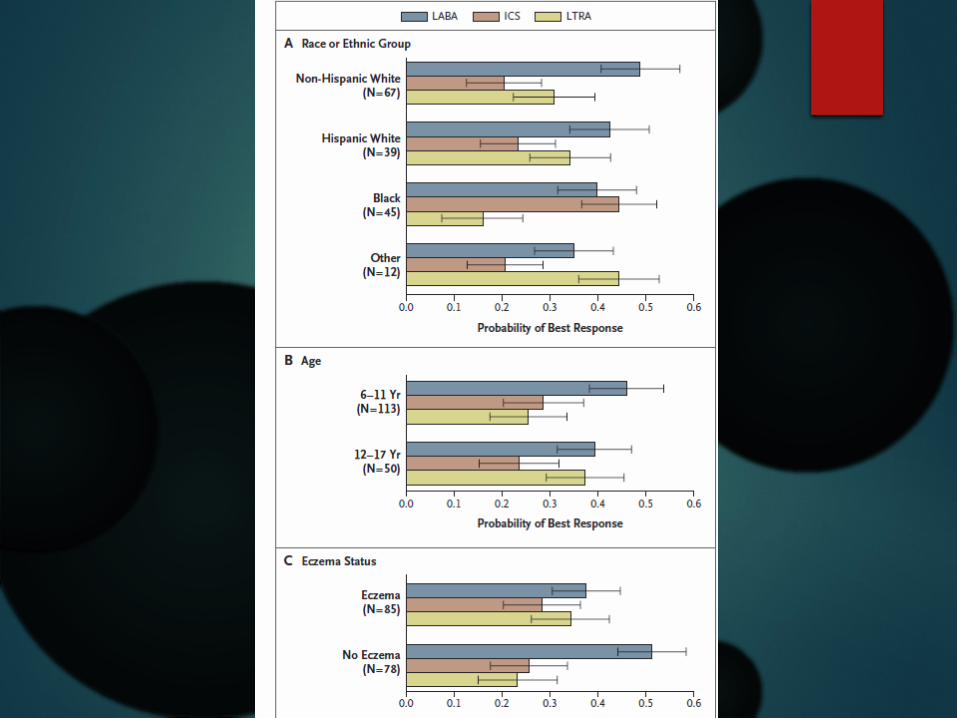
Asthma Phenotypes
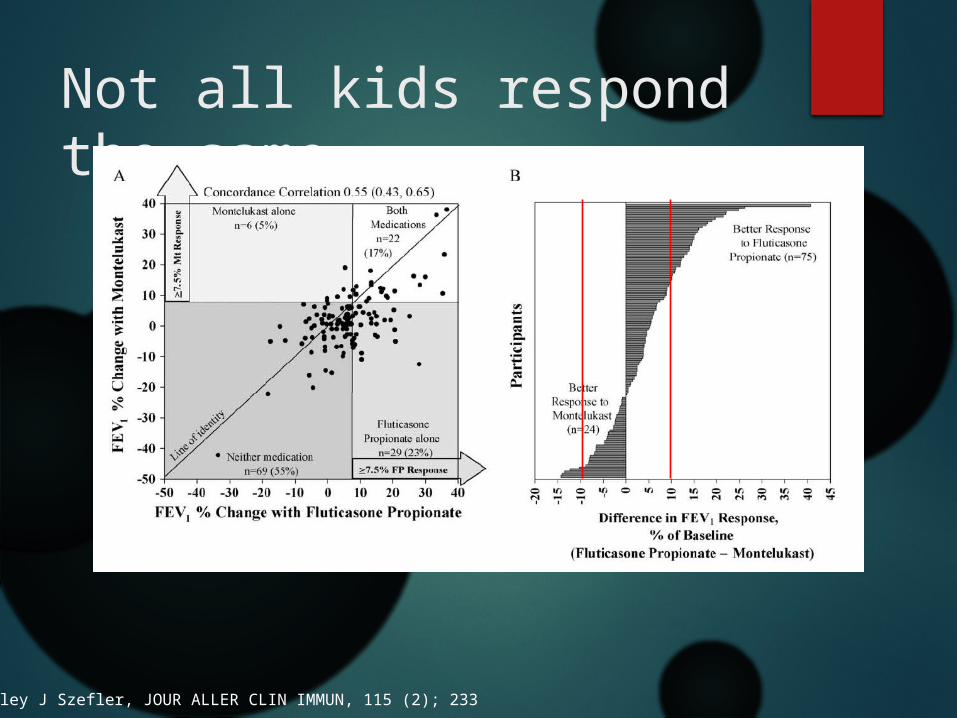
Not all kids respond the same
Stanley J Szefler, JOUR ALLER CLIN IMMUN, 115 (2); 233
Conclusions
Phenotypes of asthma An exciting horizon of research
Different phenotypes may respond to different modalities of medical therapy.
FeNO can help reveal kids who will most likely respond to inhaled steroids.
Step-up Therapy
Exercise asthma
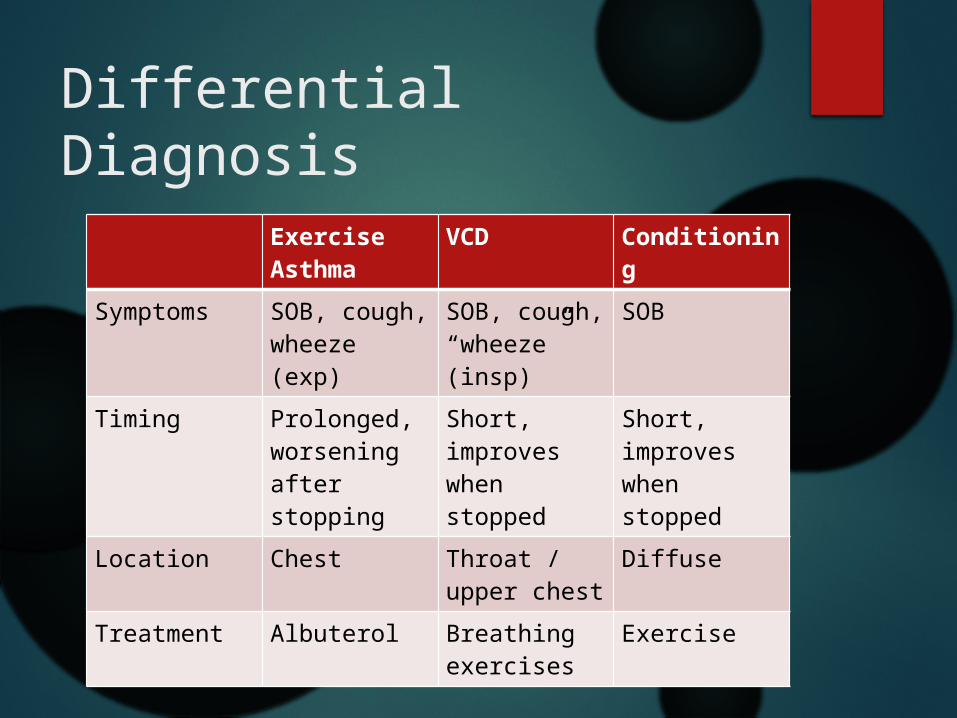
Differential Diagnosis
Exercise Asthma
VCD Conditioning
Symptoms SOB, cough, wheeze (exp)
SOB, cough, “wheeze” (insp)
SOB
Timing Prolonged, worsening after stopping
Short, improves when stopped
Short, improves when stopped
Location Chest Throat / upper chest
Diffuse
Treatment Albuterol Breathing exercises
Exercise

Using your inhaler
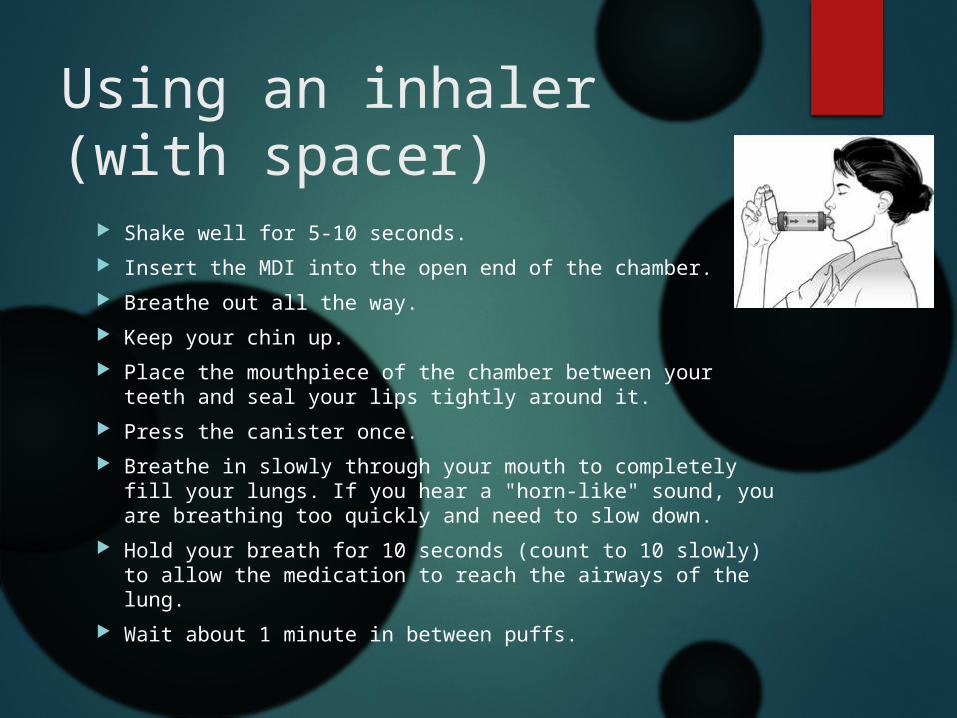
Using an inhaler (with spacer)
Shake well for 5-10 seconds.
Insert the MDI into the open end of the chamber.
Breathe out all the way.
Keep your chin up.
Place the mouthpiece of the chamber between your teeth and seal your lips tightly around it.
Press the canister once.
Breathe in slowly through your mouth to completely fill your lungs. If you hear a "horn-like" sound, you are breathing too quickly and need to slow down.
Hold your breath for 10 seconds (count to 10 slowly) to allow the medication to reach the airways of the lung.
Wait about 1 minute in between puffs.
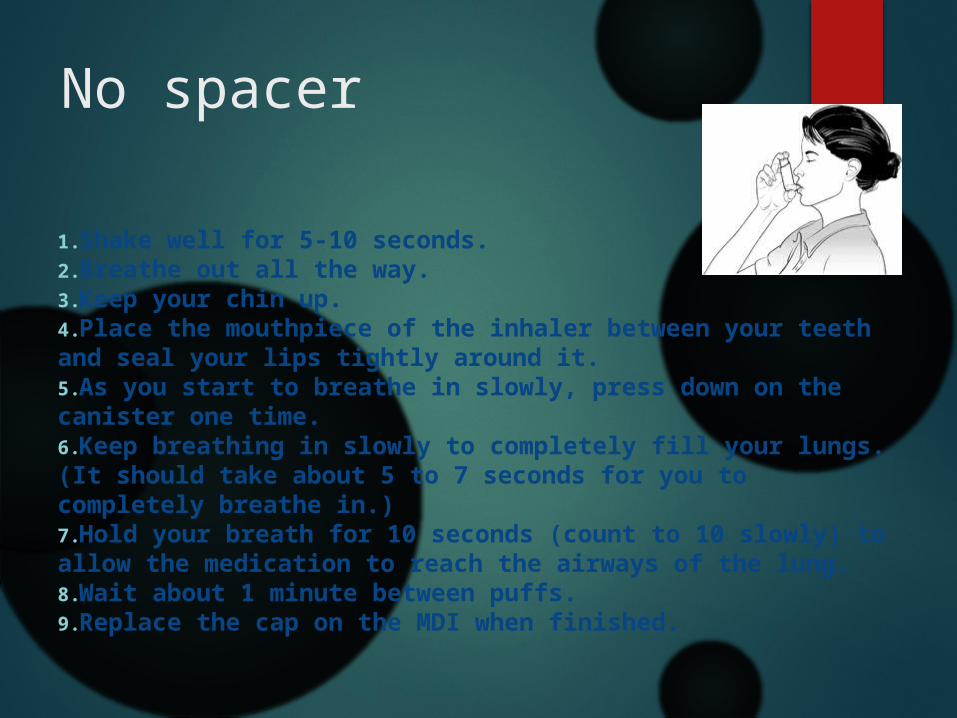
No spacer
1.Shake well for 5-10 seconds. 2.Breathe out all the way. 3.Keep your chin up. 4.Place the mouthpiece of the inhaler between your teeth and seal your lips tightly around it. 5.As you start to breathe in slowly, press down on the canister one time. 6.Keep breathing in slowly to completely fill your lungs. (It should take about 5 to 7 seconds for you to completely breathe in.) 7.Hold your breath for 10 seconds (count to 10 slowly) to allow the medication to reach the airways of the lung. 8.Wait about 1 minute between puffs. 9.Replace the cap on the MDI when finished.
Using an MDI without a chamber (figure 2)
New Therapies
Biologics Xolair
Mepolizumab
Generic Advair